Back to Journals » Journal of Asthma and Allergy » Volume 19
A Patient Education Intervention to Address Allergic Anaphylaxis-Related Quality-of-Life and Self-Efficacy
Received 4 November 2025
Accepted for publication 29 January 2026
Published 13 February 2026 Volume 2026:19 573932
DOI https://doi.org/10.2147/JAA.S573932
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Caroline Belin,1,2 Cecília Tomori1,2
1Johns Hopkins School of Nursing, Baltimore, MD, USA; 2Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA
Correspondence: Cecília Tomori, Johns Hopkins School of Nursing, 525 N Wolfe St, Baltimore, MD, 21205, USA, Email [email protected]
Introduction: Allergic anaphylaxis diagnoses can impact quality of life and self-efficacy, which in turn can lead to poor outcomes. Patient education can help empower patients but may be inadequately implemented in clinical settings.
Methods: This quality improvement study utilized a retrospective pretest-posttest brief educational intervention design and retrospective chart review over 12 weeks in an allergy specialty practice. Adult-Anaphylaxis-QoL (A-QoL) and New General Self-Efficacy (NGSE) scales were analyzed with SPSS using Wilcoxon Sign Rank tests.
Results: Sixty-six patients received the intervention. A-QoL was slightly, but statistically significantly, higher overall post intervention, 3.88 pre-test median, (IQR = 2.85, 4.81) vs post-intervention 3.95 median (IQR = 3.38, 4.68), (Z = − 2.77, p < 0.01, d = − 0.73). Significant improvements in social, emotional, and limitation subscales were found (p< 0.01), with the largest improvement in the emotional subscale. A small, statistically significant, increase was also found in self-efficacy, 3.94 pretest median (IQR 3.25, 4.28), vs 4.13 post-test median (IQR 4.12, 4.75, p < 0.01), (Z = − 4.43, p < 0.01, d = − 1.30).
Discussion: The implementation of evidence-based prevention-focused patient education was associated with modest but statistically significant increases in anaphylaxis-related quality of life and small, significant improvements in self-efficacy. This intervention was successfully implemented in a specialty allergy clinic to improve these outcomes and can be part of broader efforts to enhance patient education to reduce delays and improve appropriate use of epinephrine auto-injector.
Conclusion: Brief, evidence-based patient education can modestly improve quality of life and self-efficacy for severely allergic patients. More comprehensive interventions in diverse settings are needed to ensure that patient-centered education is coupled with linkage to epinephrine auto-injector carriage to ensure improved anaphylaxis outcomes.
Plain Language Summary: Why was the study done?
Many people have severe allergic reactions. These can be prevented with immediate first aid use of medication, but often there are delays. We know that there are many reasons for this delay, including how people feel about their illness, along with other factors. This study was done to see if patient education based on best available evidence can help make a positive difference for how people at risk for severe allergic reactions feel about their illness, which may help reduce these delays in the future.
What did the researchers do and find?
We developed and implemented a patient education intervention over the course of 12 weeks in an allergy clinic. The patient education was based on best practices in the field. We found that patient education made a small but important difference for patients’ quality of life, especially for their emotional health. The intervention also made a small difference for their confidence.
What do these results mean?
Patient education is an important part of improving care for people who have severe allergic reactions. We need high-quality patient education to be part of larger changes in clinical care so that all patients can have information about how to prevent severe allergic reactions and that they can access necessary medication to do so.
Keywords: anaphylaxis, allergy, epinephrine, patient education, quality of life, self-efficacy, health equity
Introduction
Anaphylaxis is a severe, acute, potentially life-threatening allergic health emergency brought on by an allergy to insect stings, food, medication, and immunotherapy.1,2 Global guidelines urge prompt medication administration in the hospital setting, as epinephrine is universally available worldwide. In the United States, the incidence rate of anaphylaxis is 42 per 100,000 person-years with an estimated lifetime prevalence between 1.6% and 5.1%,2–4 the condition is under-treated and underdiagnosed in both community and hospital settings. Underuse of epinephrine in the prehospital setting for the initial treatment of anaphylaxis is a known barrier to patient outcomes.3,4
Symptoms of anaphylaxis can present within minutes of exposure, leading to basophil and mast cell cytokine release in an immune-mediated systemic response.1,5 Epinephrine, an alpha/beta-agonist, is the current medication of choice for all-cause anaphylaxis first aid treatment.6,7 Early immediate management with epinephrine auto-injectors (EAI) can prevent complications including respiratory arrest, cardiac arrest, and death.5–7 Delayed treatment of anaphylaxis is associated with higher mortality and higher risk of complication with lower responsiveness to medical treatment.5,7
Early intervention for anaphylaxis treatment has the greatest ability to improve outcomes and reduce health complications; therefore, initial management in the community setting is an urgent public health concern. At present, national guidelines specifically address barriers to care with timely referral, diagnosis, and patient health literacy as positive associations to prompt care and early EAI use, however these guidelines are not often adequately implemented in clinical practice.5,7,8 National and international guidelines underscore the necessity of early use of EAIs and comprehensive patient education to improve outcomes and prevent morbidity and mortality.5,7 These guidelines reflect the strong body of existing research, which demonstrates a positive relationship between evidence-based patient education and improved adherence to emergency care plans, specifically the timely administration of EAIs in pre-hospital and community settings.3,4,9,10 Research has shown that when patients and caregivers receive targeted, evidence-informed instruction on anaphylaxis management, there is a greater likelihood of prompt EAI use during allergic emergencies.3,4,10 This early intervention is critical, as it can significantly reduce morbidity and mortality associated with anaphylactic reactions outside the clinical environment.5,7 Multiple studies support the idea that equipping at-risk individuals with the knowledge and skills to recognize symptoms and act quickly translates to better emergency outcomes.4,6,9 However, studies consistently demonstrate that patient education is inconsistent.4,5,9 This disconnect between best practice guidance and real-world healthcare delivery highlights the need for more effective, system-level strategies to ensure that evidence-based recommendations are enacted in practice.5,7
Previous studies have found that a severe allergy diagnosis has a substantial impact on quality of life and can lead to reduced self-efficacy.11,12 A diagnosis of anaphylaxis can be a significant, unexpected, life-changing event associated with adverse medical experiences and can induce anxiety and increased distress.11,12 Because of diagnosis and symptomatology, patients can exhibit heightened avoidance, lower self-efficacy and delay medical care-seeking behaviors, increasing overall negative healthcare outcomes related to anaphylaxis prompt care treatment.12–14 These impacts are compounded by structural inequities, but they affect patients across socioeconomic groups. Effective patient education can help to counter these impacts, but remains inadequately implemented.5,7 This quality improvement initiative built on this literature to develop, implement and evaluate an evidence-based intervention that followed guidelines on health literacy and patient education.8,15,16 In the West Coast practice setting for this study, patients did not face insurance coverage barriers. However, prior to this intervention, patient education was limited and unevenly implemented in this busy clinic setting – a common concern across many clinical outpatient settings. Despite a relatively privileged setting, the care team noted opportunities to improve the quality of care based on reports of patients lacking an understanding of anaphylaxis and appropriate use of EAIs.5–7 The objective of this study was to evaluate whether this brief evidence-based intervention could improve anaphylaxis-related quality of life and self-efficacy, and whether it can be successfully incorporated into practice.
Materials and Methods
Intervention Development
The intervention combined nursing and public health approaches to patient education. The study team identified evidence-based patient education as a means to address health disparities to support anaphylaxis-diagnosed patients with the information necessary to recognize signs and symptoms of anaphylaxis.8,15,17 According to Schultz et al, “high levels of health literacy without a corresponding high degree of patient empowerment creates an unnecessary dependence of patients on health professionals, while a high degree of empowerment without a corresponding degree of health literacy poses the risk of dangerous health choices”.16 When empowerment is paired with health literacy, patients report improved quality of life and increased self-efficacy, which can lead to improved health outcomes.8,13,16
First, an educational pamphlet was developed following best practice guidance. The primary objective of the pamphlet “Anaphylaxis: a Big Word for a Big Problem” (Figure 1) was to help patients achieve the following competencies:
Figure 1 Continued. Figure 1 Anaphylaxis Educational Trifold Brochure “Anaphylaxis: a Big Word for a Big Problem”.
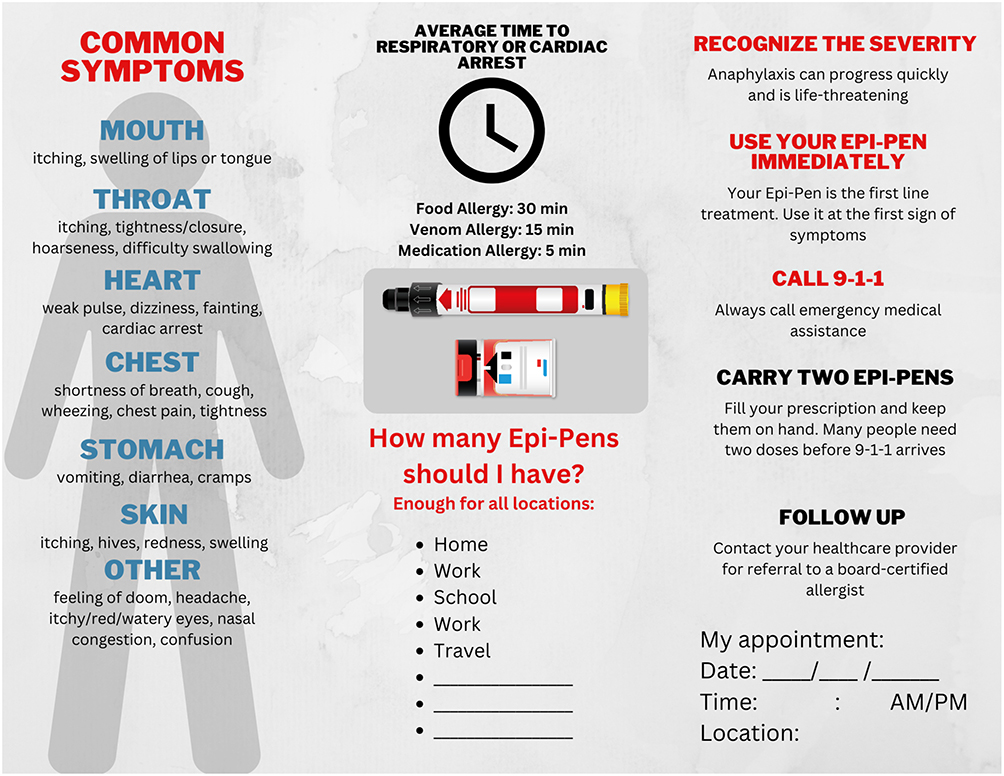
- Understand common causes of severe allergy: anaphylaxis.
- Know how many epinephrine auto-injectors a person should have.
- Seek appropriate care, including follow-up and when to call 9-1-1.
The purpose of selecting instructional strategies and a trifold pamphlet for the intended lay public audience was to maximize engagement. Relevance and usability are essential for the adult learner.15 The information visually addressed the behavioral needs of the adult patient audience in plain language. The purpose of the trifold was to serve as a guide to avoid misinformation: website resources provided a collection of trusted, reliable resources to help the patient make informed decisions. Best practice guidance also indicates that active teaching and teach-back strategies are most effective.16 Therefore, these strategies were paired in the intervention with using the pamphlet with the objective that this approach would enable the patient to participate in shared decision-making and use the assembled resources in the pamphlet to prevent delayed use of EAI.16
Study Design
The quality improvement study utilized a retrospective pretest-posttest intervention design and retrospective chart review.
Ethical Approval
Ethical approval was obtained by the Johns Hopkins School of Nursing DNP Scholarly Project Ethical Review Committee (#394). This study was carried out as the first author’s doctoral work and was determined to be a quality improvement study. As such, it did not constitute human subjects research under the US Department of Health and Human Services or Federal Drug Administration regulations and Johns Hopkins University institutional guidelines. Therefore, individual informed consent was not required. The study was in compliance with the Declaration of Helsinki by undergoing institutional ethical review, was determined to be of minimal risk to the study site’s patients, and followed all required ethical standards for quality improvement studies that engaged a clinical practice setting.
Setting
The practice setting for this project was an allergy specialty private practice site in greater Los Angeles. The practice site for implementation included two outpatient clinics led by the owner-operator physician. In total, this practice serves approximately 2000 insured new patients annually, with a service unit of approximately 8000 empaneled insured established patients annually. The practice included a direct care physician provider and a nurse practitioner (NP), for the treatment, diagnosis, and prevention of allergy, asthma, and immune-related diseases.
Sample
A convenience sample of adults aged 18 years and older who had a diagnosis of anaphylaxis or allergic angioedema, or allergy reaction were eligible to participate. A total of 66 respondents participated in the study.
Inclusion/Exclusion Criteria
Criteria for inclusion was defined by privately insured, established current patient individuals with a diagnosis of food, hymenopteran, or medication allergy with or without previous presentation to the emergency care hospital or urgent care setting. Hereditary angioedema patients and pediatric patients were excluded from the sample. The sample measure was obtained from a single practice group setting comprised of two physical clinics located in the greater Los Angeles area between October 3, 2023, and December 19, 2023.
Implementation and Recruitment
The physician, nurse practitioner, and staff at the location participated in the implementation of the project. A chart review audit was conducted for all established adult patients over the age of 18 to obtain a sufficiently large sample who met the inclusion criteria. No identifying information was extracted or recorded. Data did not contain PHI. Data were stored on password and 2FA secure servers on OneDrive compliant with all information technology policies.
Baseline Data and Study Instruments/Measures
A retrospective chart review of the EPIC electronic health record for the service unit population for specialty practice was conducted. Data collection included established patients age 18 and older with International Classification of Diseases (ICD-10) diagnosis codes of allergic reaction and anaphylaxis, excluding in-hospital coding, and hereditary angioedema. A known problem related to the predictive use of ICD-10 algorithms is that despite acceptable validity, the positive predictive value of the algorithm will underestimate absolute risk by up to one-third.18,19 Therefore, as a requirement for this quality improvement project, an additional manual review of the chart was conducted to identify and evaluate the suspected history of allergic anaphylactic reactions before intervention implementation. Diagnosis codes, linkage to primary care, appointment completion, and prescription renewal were assessed for baseline data in the chart review.13,14
Since data suggest that individuals with poor anaphylaxis related quality of life may need psychological support in addition to medical management of the anaphylactic condition, the study employed the Anaphylaxis Quality of Life for Adults scale (A-QoL), a reliable 21-item measure of the effects of anaphylaxis’ impact on three different health domains: the emotional domain; the social domain; and on the limitations on life domain.12,14 Each domain is assessed by a different subscale, which together can be added up for an overall A-QoL score. The A-QoL scale demonstrates excellent internal reliability, Cronbach alpha = 0.96.14 The response options were scored 5 = Never, 1 = Always, with higher scores meaning greater quality of life. This is a reverse scoring from the original scale in order to be consistent with the direction of change in the New General Self-Efficacy Scale below.14
Self-efficacy was assessed using the 8-item New General Self-Efficacy Scale (NGSE), which has been previously found to be superior to earlier general self-efficacy scales.13 This measure provides a reliable assessment of an individual’s belief in their ability to achieve goals and their orientation towards learning and change. The Cronbach’s alpha = 0.87, 0.88, and 0.85, respectively. The responses options were 5 = Strongly Agree, 1 = Strongly Disagree, with higher scores meaning greater self-efficacy.
Intervention Implementation
The intervention occurred over the duration of 12 weeks, including a 15-minute educational session using the developed pamphlet reviewing EAI prescription renewal, EAI use, and signs and symptoms of anaphylaxis (Figure 1). Language translation was provided for Limited English Proficiency patients identified in the chart review and accommodations were also provided for any disability or impairment, such as mobility access and extended visit time.20,21 A single NP, the study lead, implemented the intervention to ensure fidelity. During the pre-implementation phase, sample data was collected in a retrospective chart review for diagnoses, appointment completion, prescription renewal, and follow-up appointment scheduling. During the intervention phase, patients were provided with Signs and Symptoms of Anaphylaxis handout (Figure 1), EAI demonstration with patient EAI and teach back method, and safety plan assessment. During the post-intervention phase, the NGSE and AQOL scales were administered and analyzed for the 66 participants.
Results
Data Analysis
There was no missing data in the dataset. Data were analyzed using SPSS Version 29.0.0. Descriptive statistics were used to report patient demographics, linkage to primary care, diagnoses, and prescription renewal. For evaluating quality of life and self-efficacy, data collected did not show normal distribution as evaluated by Normal Q-Q Plot. Because the data did not show normal distribution, a Wilcoxon Sign Rank (nonparametric) test was used to evaluate improvements in NGSE and AQOL.
Participant Characteristics
Most participants (51.5%) were aged 30–49. Three quarters (75%) were female, two thirds (66.7%) were white, and nearly half (43.9%) attained a 4-year college degree, and nearly half (53.0%) of participants reported an annual individual income level of $100,000 to $149,999 (Table 1). All patients reported linkage to a primary care health provider (Table 2). Even though all patients had an ICD-10 diagnosis for severe anaphylaxis allergy, only half of the respondents reported a diagnosis of severe anaphylaxis allergy, indicating a gap in understanding prior to the intervention. Less than half (42.9%) of respondents had carriage and current prescriptions for epinephrine auto-injectors. Additionally, despite the high level of insurance coverage for this patient population, approximately half of the respondents of all incomes reported difficulty or challenges filling their prescriptions, which is a known barrier to positive health outcomes.
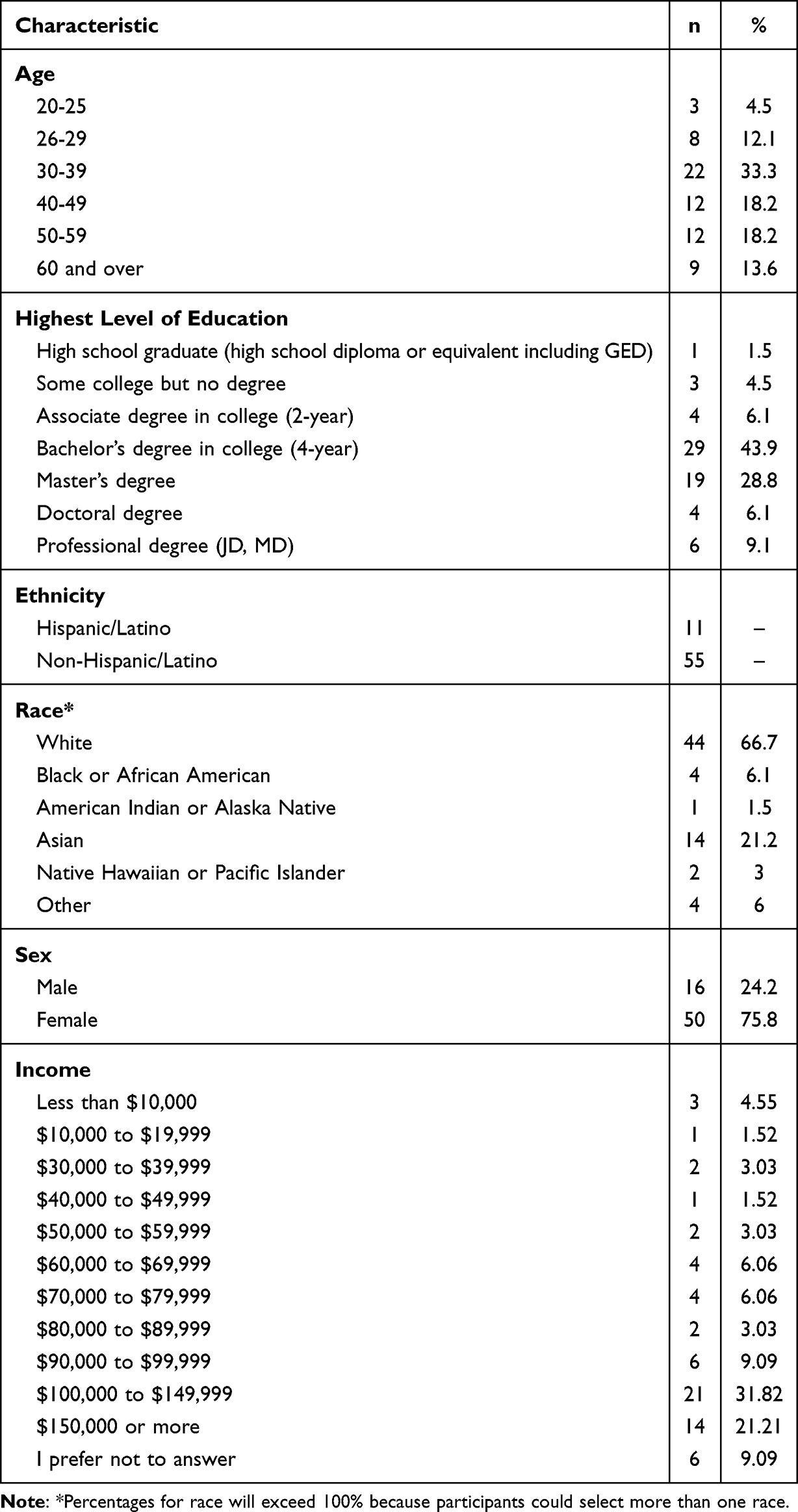 |
Table 1 Demographic Characteristics of the Sample |
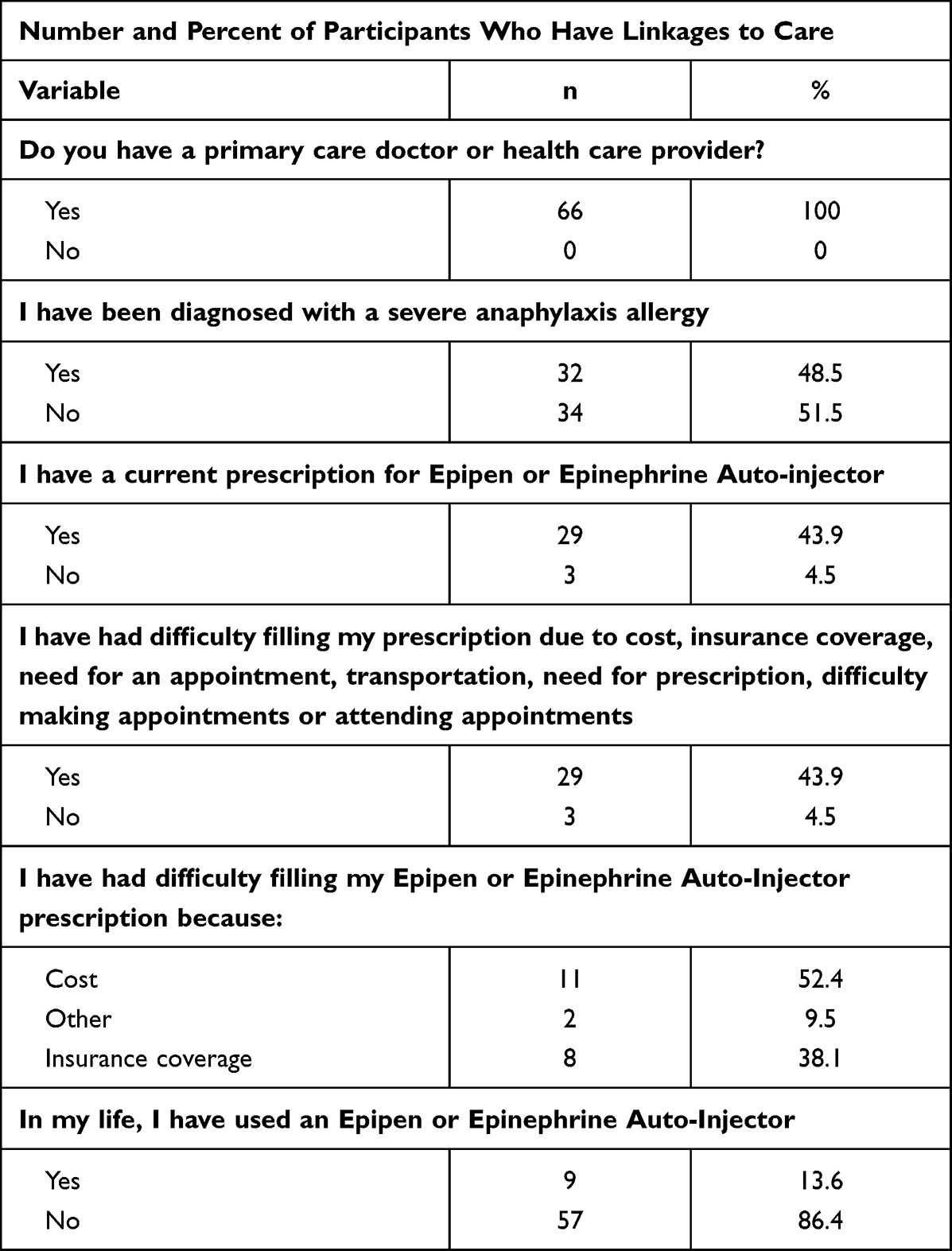 |
Table 2 Anaphylaxis-Related Background Characteristics |
The general Anaphylaxis Quality of Life pretest median for participants (n=66) was 3.88 (IQR = 2.85, 4.81) and the post-test median was 3.95 (IQR = 3.38, 4.68) (Table 3 and Figure 2). There was a median 0.07-point increase in scores, indicating a slight overall improvement in patient self-rating of the quality of life. Since the data were not normally distributed, Wilcoxon Sign Rank test was used to evaluate this difference, which was statistically significant, (Z = −2.77, p < 0.01, d = −0.73). Higher scores indicate a better QoL, suggesting the intervention had a small but statistically significant impact in improving anaphylaxis-related QoL.
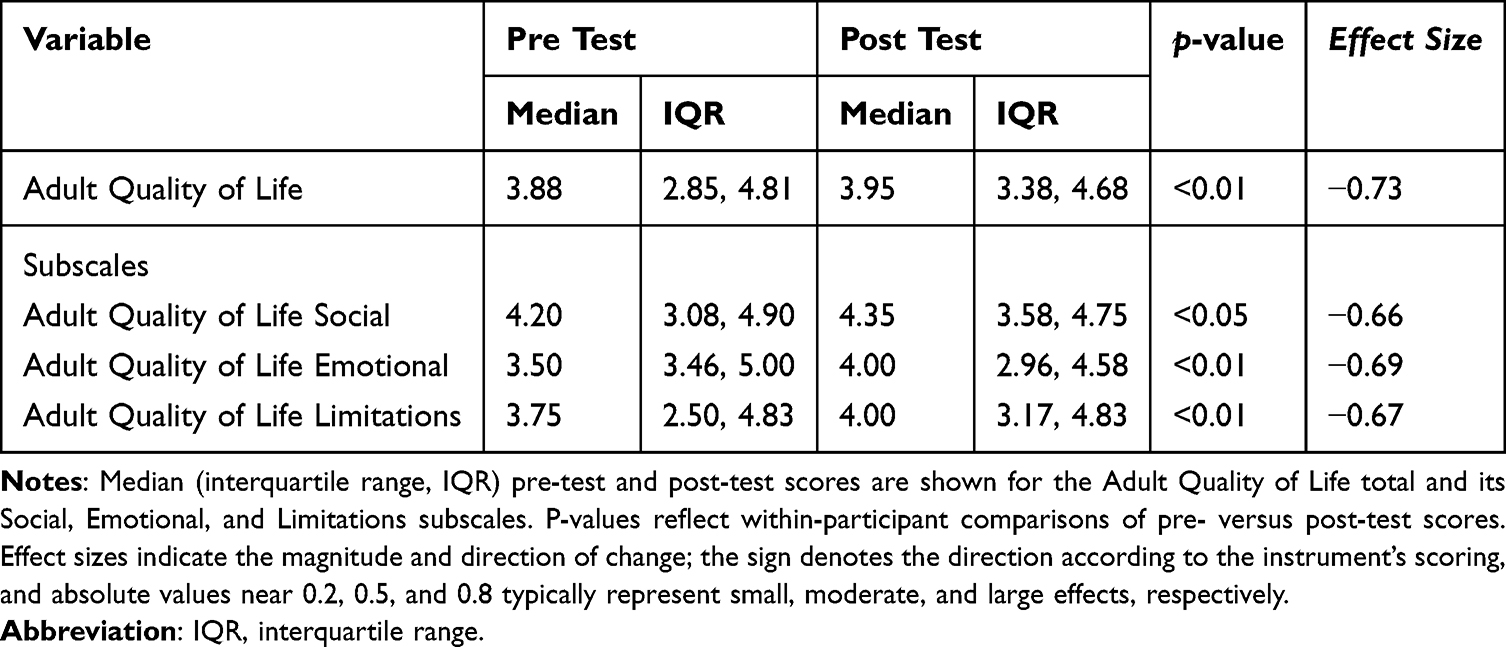 |
Table 3 Anaphylaxis-Related Quality of Life (n = 66) |
 |
Figure 2 Anaphylaxis Quality of Life Retrospective Pretest Posttest. |
Subscale scores for the AQOL scale were also evaluated separately and demonstrated significant improvements after the intervention as assessed by the Wilcoxon Sign Rank test (see Table 3). The AQOL Social subscale pretest median improved slightly from 4.20 (IQR = 3.08, 4.90) to a post-test median of 4.35 (IQR = 3.58, 4.75) and this improvement was statistically significant with an intermediate effect size (Z = −2.53, p < 0.05, d = −0.66). The AQOL Emotional subscale post-test median was 4.00 (IQR = 2.96, 4.58), a 0.5 point improvement from a median pretest score of 3.50 (IQR = 3.46, 5.00), which was also statistically significant with an intermediate effect size (Z = −2.64, p < 0.01, d = −0.69). Finally, the AQOL Limitations subscale post median also increased from pretest score of 3.75 (IQR = 2.50, 4.83) to 4.00 (IQR = 3.17, 4.83), which was another statistically significant improvement with an intermediate effect size (Z = −2.6, p < 0.01, d = −0.67). Together, the subscales show an overall median improvement of patient-rated subjective experience in all three domains, with the greatest improvement in the emotional subscale, and a modest positive effect of the total AQOL, all with an intermediate effect size. Pre-post-test findings on the New General Self-Efficacy scale were also evaluated with a Wilcoxon Sign Rank test due to non-normal distribution of the data (Table 4 and Figure 3). The post-test median score of 4.13 (IQR = 4.12, 4.75) was higher than the pre-test median of 3.94 with an (IQR = 3.25, 4.28), and this change was statistically significant with a large effect size (Z = −4.43, p < 0.01, d = −1.30). Higher scores suggest greater patient self-rating of self-efficacy, indicating that the intervention had a small, statistically significant positive impact.
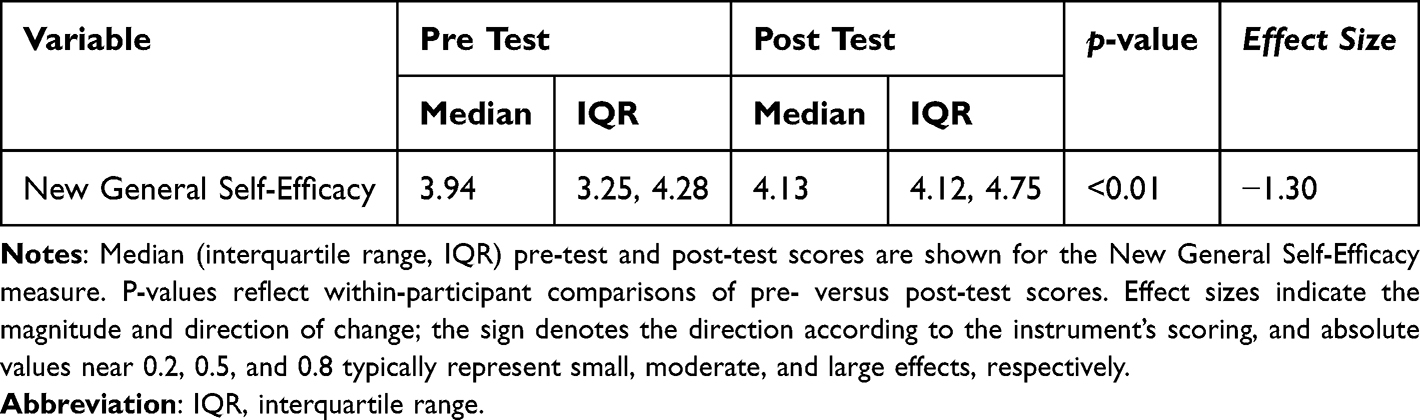 |
Table 4 New General Self-Efficacy (n = 66) |
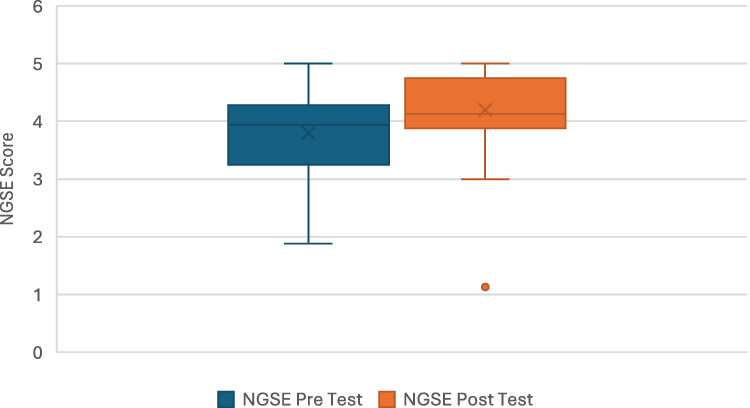 |
Figure 3 New General Self Efficacy scale. |
Discussion
This study employed evidence-based, best-practice guidance for patient education in an allergy specialty clinical setting to improve patient quality of life and self-efficacy, with the ultimate goal to improve appropriate use of EAI in the future. Patient baseline data indicated large gaps in understanding of their diagnosis of severe anaphylaxis allergy despite confirmed ICD-10 codes, poor EAI carriage, and difficulties refilling EAI prescriptions even in this relatively privileged population. Small, statistically significant, improvements were found for A-QoL, including its three subscales, with intermediate effect sizes as well as for self-efficacy with a large effect size (Figures 2 and 3, Tables 3 and 4). The emotional domain of the A-QoL demonstrated the largest improvement; however, all changes demonstrated at least an intermediate effect size, suggesting small but meaningful improvements. As neither scale has established MCID criteria, future work will need to explore the importance of these improvements for clinical significance. Nevertheless, the results of this quality improvement study demonstrate that evidence-based education as part of an empowering patient environment can modestly improve anaphylaxis-related quality of life and self-efficacy for patients diagnosed with or at risk for anaphylaxis. Integration of this intervention into a broader set of clinical practice outcomes for patient-centered care may provide an opportunity to improve patient wellbeing. Although the brief study period prevented collection of long-term behavioral data, since both quality of life and self-efficacy are associated with better care-seeking and utilization behaviors, these improvements may also lead to increases in appropriate EAI carriage and use that could be investigated in future studies.2–4
The findings of this study are consistent with the existing literature, which highlights the impact of patient education to improve quality of life and self-efficacy for patients with severe allergies.8,12,14 A diagnosis of anaphylaxis can be a significant, unexpected, life changing event associated with adverse medical experiences, can induce anxiety, and increase distress, whereas patient empowerment is associated with higher quality of life.11,12 Additionally, because of diagnosis and symptomatology, patients can exhibit heightened avoidance and delay of medical care seeking behaviors increasing overall negative healthcare outcomes related to anaphylaxis prompt care treatment.12,14 The fact that the greatest improvement in this study was in the emotional domain of the A-QoL suggests that this dimension of QoL can be influenced by a brief educational intervention. Additional work should be undertaken to ensure that other domains are also addressed, and that improvements are sustained. Additionally, there have been numerous calls to collect patient-reported outcome measures (PROMs) for allergic disease in an effort to personalize and improve quality of care.22 This intervention takes up these calls to build on best practice evidence and collect PROMs, such as A-QoL and NGSE, to help improve patient-centered care.
Patient education can improve anaphylaxis-related outcomes in multiple ways. Previous work has demonstrated that evidence-based patient education can help provide an empowering environment and improve timely administration of EAIs in pre-hospital and community settings.3,4,9,10 Patient education is also generally a cost-effective first step in improving quality of care since it is less expensive compared to hospital intervention, does not cause harm to the patient, and can facilitate early patient recognition of signs of anaphylaxis.5,23 At the same time, patient education and EAI carriage should be emphasized as part of a comprehensive plan of care for anaphylaxis because the cause of delay in epinephrine administration is multifactorial. A brief educational intervention on its own is not sufficient to achieve needed improvement. Patients likely require ongoing support and face additional structural and social barriers, which also impact their A-QoL and self-efficacy. For instance, it is known that patient education related to EAI device use and obtaining renewal of prescription may present immediate financial hurdles.9,10 Even in this relatively privileged clinical setting, with an insured sample, nearly half (43.9%) in this study had difficulties with prescription renewal (Table 2). Therefore, patient education should be coupled with additional structural changes to ensure that all patients have access to EAI, regardless of insurance status.7,23
Future Research Opportunities
Future research could build on this study to effectively integrate patient education into clinical practice, and address the entire process from diagnosis to ensuring that each patient has a current EAI prescription and EAI carriage. A comprehensive intervention that encompasses multiple points of patient education and incorporates all dimensions of A-QoL and self-efficacy coupled with removing structural barriers for EAI carriage (eg by linking each patient to coverage for EAI or free EAI) may be most effective.10,12,14,16 This intervention would ideally be tested in a larger RCT, with a diverse population. Importantly, interventions in the future should provide information to patients free of commercial influence from EAI manufacturers.
Limitations
This study design, like all quality improvement studies, involved only a single group without a control group. As a result, the data does not separate the effects of the intervention from other potential confounding variables.24 Additionally, a key limitation of the retrospective pretest-posttest study design is recall bias.25 Participants are asked to reflect and rate their previous knowledge, skills, or attitudes after the intervention has occurred, which can lead to inaccurate or biased responses because their memories or perceptions may have changed over time. This can affect the reliability of the results, as participants might unintentionally overestimate or underestimate their initial status. Another limitation was the duration of the intervention and the lack of ability to collect behavioral data on EAI use following the intervention, due to the limited time period available for data collection for this study. A longer period would be necessary to be able to assess appropriate EAI use in real time. Finally, the study population was relatively privileged; therefore, work in more diverse settings is needed to ensure applicability of the findings. However, even with compounding structural issues, many impacts on quality of life and self-efficacy affect broad groups of patients with anaphylaxis, and a wide range of practice settings struggle with implementing best practices in patient education. Creating an empowering environment is a shared goal across these settings.
Conclusions
This quality improvement study demonstrates that a brief, evidence-based patient education intervention can make modest improvements in anaphylaxis-related quality of life and self-efficacy and can be effectively incorporated in a busy clinical practice setting. This intervention could be integrated into broader efforts that may lead to more appropriate and timely use of EAI. As a cornerstone of best practice, patient education is necessary for initial and ongoing clinical intervention and improvement of anaphylaxis outcomes.6,7 By devoting greater attention to integrating evidence-based patient education as part of patient-centered care, healthcare practitioners can enact a treatment strategy that can improve patient wellbeing and may ultimately contribute to improving other anaphylaxis-related health outcomes.
Acknowledgment
An abstract based on the work in the manuscript has been presented at and uploaded to the online server for the American Public Health Association 2024 Annual Meeting and Expo https://apha.confex.com/apha/2024/meetingapp.cgi/Paper/550207.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lieberman P. Epidemiology of anaphylaxis. Curr Opin Allergy Clin Immunol. 2008;8(4):316–12. doi:10.1097/aci.0b013e3283036a69
2. Turner PJ, Campbell DE, Motosue MS, Campbell RL. Global trends in anaphylaxis epidemiology and clinical implications. J Allergy Clin Immunol. 2020;8(4):1169–1176. doi:10.1016/j.jaip.2019.11.027
3. Dami F, Enggist R, Comte D, Pasquier M. Underuse of epinephrine for the treatment of anaphylaxis in the prehospital setting. Emerg Med Int. 2022;2022:1–7. doi:10.1155/2022/5752970
4. Prince BT, Mikhail I, Stukus DR. Underuse of epinephrine for the treatment of anaphylaxis: missed opportunities. J Asthma Allergy. 2018;11:143–151. doi:10.2147/jaa.s159400
5. Shaker MS, Wallace DV, Golden DBK, et al. Anaphylaxis—a 2020 practice parameter update, systematic review, and grading of recommendations, assessment, development and evaluation (GRADE) analysis. J Allergy Clin Immunol. 2020;145(4):1082–1123. doi:10.1016/j.jaci.2020.01.017
6. Fromer L. Prevention of anaphylaxis: the role of the epinephrine auto-injector. Am J Med. 2016;129(12):1244–1250. doi:10.1016/j.amjmed.2016.07.018
7. Cardona V, Ansotegui IJ, Ebisawa M, et al. World allergy organization anaphylaxis guidance 2020. World Allergy Organ J. 2020;13(10):100472. doi:10.1016/j.waojou.2020.100472
8. Nutbeam D, Lloyd JE. Understanding and responding to health literacy as a social determinant of health. Ann Rev Public Health. 2021;42(1):159–173. doi:10.1146/annurev-publhealth-090419-102529
9. Glassberg B, Nowak-Wegrzyn A, Wang J. Factors contributing to underuse of epinephrine autoinjectors in pediatric patients with food allergy. Ann Allergy Asthma Immunol. 2021;126(2):175–179.e3. doi:10.1016/j.anai.2020.09.012
10. Warren CM, Zaslavsky JM, Kan K, Spergel JM, Gupta RS. Epinephrine auto-injector carriage and use practices among US children, adolescents, and adults. Ann Allergy Asthma Immunol. 2018;121(4):479–489.e2. doi:10.1016/j.anai.2018.06.010
11. Emre E, Kan A. Evaluation anxiety levels of adult patients and parents of adolescent patients with anaphylaxis. Harran Üniversitesi Tip Fakültesi Dergisi. 2022;19(3):515–519. doi:10.35440/hutfd.1122524
12. Knibb RC, Huissoon AP, Baretto R, et al. The impact of anaphylaxis on the quality of life and mental health of adults. Clin Exp Immunol. 2022;53(1):121–125. doi:10.1111/cea.14249
13. Chen G, Gully SM, Eden D. Validation of a new general self-efficacy scale. Organizational Res Methods. 2001;4(1):62–83. doi:10.1177/109442810141004
14. Knibb RC, Huissoon AP, Baretto R, et al. Development and validation of the anaphylaxis quality of life scale for adults. J Allergy Clin Immunol. 2022;10(6):1527–1533.e3. doi:10.1016/j.jaip.2022.02.023
15. Jordan K, Lofton S, Richards EA. Strategies for embedding population health concepts into nursing education. Nursing Forum. 2020;56(1):208–213. doi:10.1111/nuf.12498
16. Schulz PJ, Nakamoto K. Health literacy and patient empowerment in health communication: the importance of separating conjoined twins. Patient Educ Couns. 2013;90(1):4–11. doi:10.1016/j.pec.2012.09.006
17. Palmer RC, Ismond D, Rodriquez EJ, Kaufman JS. Social determinants of health: future directions for health disparities research. Am J Public Health. 2019;109(S1):S70–S71. doi:10.2105/ajph.2019.304964
18. Pourang D, Batech M, Sheikh J, Samant S, Kaplan M. Anaphylaxis in a health maintenance organization: international classification of diseases coding and epinephrine auto-injector prescribing. Ann Allergy Asthma Immunol. 2017;118(2):186–190.e1. doi:10.1016/j.anai.2016.10.027
19. de Sordi D, Kappen S, Otto‐Sobotka F, et al. Validity of hospital ICD‐10‐GM codes to identify anaphylaxis. Pharmacoepidemiol Drug Saf. 2021;30(12):1643–1652. doi:10.1002/pds.5348
20. Agaronnik ND, Pendo E, Campbell EG, Ressalam J, Iezzoni LI. Knowledge of practicing physicians about their legal obligations when caring for patients with disability. Health Affairs. 2019;38(4):545–553. doi:10.1377/hlthaff.2018.05060
21. Iezzoni LI, Rao SR, Ressalam J, et al. US physicians’ knowledge about the Americans with disabilities act and accommodation of patients with disability. Health Affairs. 2022;41(1):96–104. doi:10.1377/hlthaff.2021.01136
22. Anagnostou A, Warren C, Dantzer J, et al. Patient-reported outcome measures in food and drug allergy. J Allergy Clin Immunol. 2024;12(10):2591–2598. doi:10.1016/j.jaip.2024.04.053
23. Westermann-Clark E, Pepper AN, Lockey RF. Economic considerations in the treatment of systemic allergic reactions. J Asthma Allergy. 2018;11:153–158. doi:10.2147/jaa.s159851
24. Linden A. Conducting interrupted time-series analysis for single- and multiple-group comparisons. Stata J. 2015;15(2):480–500. doi:10.1177/1536867x1501500208
25. Hill LG, Betz DL. Revisiting the retrospective pretest. Am J Eval. 2005;26(4):501–517. doi:10.1177/1098214005281356
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Anaphylaxis in Chinese Children with Pollen Sensitization: Triggers, Clinical Presentation, and Acute Management
Jiang N, Xu W, Huang H, Hou X, Xiang L
Journal of Asthma and Allergy 2022, 15:633-643
Published Date: 16 May 2022
Anaphylaxis in Chinese Children: Different Clinical Profile Between Children with and without a History of Asthma/Recurrent Wheezing
Jiang N, Xu W, Huang H, Hou X, Xiang L
Journal of Asthma and Allergy 2022, 15:1093-1104
Published Date: 18 August 2022
Phenotypic Distinctions Between Omega-5-Gliadin Allergy and Peanut Allergy: Clinical Profile, Reaction Rates and Triggers, and Quality of Life
Zubrinich CM, Puy RM, O'Hehir RE, Hew M
Journal of Asthma and Allergy 2022, 15:1823-1830
Published Date: 22 December 2022
Best Evidence Summary of Home Enteral Tube Feeding Care Management in the Elderly
Zhu H, Liu A, Han Z, Yang Y, Ma X, Shi H
Patient Preference and Adherence 2025, 19:49-63
Published Date: 7 January 2025