Back to Journals » ClinicoEconomics and Outcomes Research » Volume 15
Patient Characteristics and Clinical and Economic Outcomes Associated with Unplanned Medical and Surgical Intensive Care Unit Admissions: A Retrospective Analysis
Authors Khanna AK, Moucharite MA, Benefield PJ, Kaw R ![]()
Received 7 June 2023
Accepted for publication 13 September 2023
Published 25 September 2023 Volume 2023:15 Pages 703—719
DOI https://doi.org/10.2147/CEOR.S424759
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Ashish K Khanna,1– 3 Marilyn A Moucharite,4 Patrick J Benefield,5 Roop Kaw2,6
1Department of Anesthesiology, Section on Critical Care Medicine, Wake Forest University School of Medicine, Winston-Salem, NC, USA; 2Outcomes Research Consortium, Cleveland, OH, USA; 3Perioperative Outcomes and Informatics Collaborative, Winston-Salem, NC, USA; 4Healthcare Economics Outcomes Research, Medtronic, Mansfield, MA, USA; 5Healthcare Economics Outcomes Research, Medtronic, Boulder, CO, USA; 6Department of Hospital Medicine, Cleveland Clinic, Cleveland, OH, USA
Correspondence: Ashish K Khanna, Department of Anesthesiology, Section on Critical Care Medicine, Wake Forest University School of Medicine, Medical Center Boulevard, Winston-Salem, NC, 27106-1009, USA, Tel +1-336-716-4498, Fax +1-336-716-8190, Email [email protected]
Purpose: To characterize medical and surgical patient characteristics, as well as clinical and economic outcomes, associated with unplanned intensive care unit (ICU) admissions.
Patients and Methods: This was a retrospective matched cohort analysis that utilized the PINC AITM Healthcare Database, which collects deidentified data from 25% of United States (US) hospital admissions. Discharge records were assessed for medical and surgical admissions in 2021. An unplanned ICU admission was defined as direct transfer from a medical, surgical, or telemetry unit to the ICU. Patients with and without an unplanned ICU admission were 1:1 propensity score matched. Differences between patients with and without unplanned ICU admissions were assessed using two-sample t-tests for continuous measures and Chi-square tests for categorical measures.
Results: A total of 3,807,124 qualifying admissions were identified. Medical admissions with unplanned ICU transfers were more likely to be urgent/emergent (odds ratio [OR] 2.9, 95% confidence interval [CI 2.7– 3.0], p< 0.0001), with patient characteristics including male sex (1.4, [1.4– 1.4], p< 0.0001), obesity (1.7, [1.6– 1.7], p< 0.0001), and increased Charlson Comorbidity Index (CCI=1: 1.8, [1.8– 1.9], p< 0.0001; CCI≥ 5: 3.2, [3.1– 3.3], p< 0.0001). Surgical admissions with unplanned ICU transfers were more likely to be urgent/emergent (3.1, [2.9– 3.2], p< 0.0001) and with patients of higher CCI (2.5, [2.3– 2.6], p< 0.0001 to a CCI of≥ 5 (7.9, [7.4– 8.4], p< 0.0001). Between matched medical patients, mean differences in length of stay, cost, and mortality were 4.1 days (p< 0.0001), $13,424 (p< 0.0001), and 21% (p< 0.0001), respectively. Between matched surgical patients, mean differences in these outcomes were 6.4 days (p< 0.0001), $21,448 (p< 0.0001), and 14% (p< 0.0001), respectively.
Conclusion: Emergency care in patients with a higher co-morbid burden is more likely to lead to unplanned ICU admission, putting patients at a significantly increased chance of mortality, longer length of stay, and increased costs. Improving care and monitoring of patients outside the ICU may help detect early changes in pathophysiology and enable early intervention.
Plain Language Summary: Although unplanned intensive care unit (ICU) admissions from medical and surgical hospital units are common, the risk factors and outcomes associated with unplanned ICU admissions are not well-characterized. The purpose of this research was to examine the patient risk factors for unplanned ICU admissions and to calculate the impact of unplanned ICU transfers on patient length of stay, healthcare costs, and mortality. This research used a healthcare database that contains discharged patient data from 25% of United States (US) hospital admissions. The top risk factors for medical patients who had an unplanned ICU admission included emergency admissions (compared to pre-scheduled hospital admissions), male sex, obesity, and having one or more underlying disease. In surgical patients, the top risk factors for unplanned ICU admissions were emergency admissions (compared to pre-scheduled surgeries) and having one or more underlying disease. After risk adjustment, compared to medical patients without an unplanned ICU admission, medical patients with an unplanned ICU admission had significantly longer length of stay (4.1 days), higher cost ($13,424), and higher mortality (21%). Similarly, surgical patients with an unplanned ICU admission had longer length of stay (6.4 days), higher cost ($21,448), and higher mortality (14%) compared to surgical patients without unplanned ICU admission. Together, these results indicate that emergency care in patients with underlying disease is more likely to lead to an unplanned ICU admission. This puts patients at a higher chance of mortality, longer length of stay, and increased costs. Improving care and monitoring of patients outside of the ICU could enable clinicians to intervene early to reduce ICU transfers.
Keywords: healthcare costs, length of stay, mortality, comorbidity
Introduction
Unplanned admissions to the intensive care unit (ICU) are common, but the frequency reported in the current body of literature is wide, ranging from approximately <1% to 20% in surgical patients and 9% to 40% in medical patients.1–4 These events are associated with increased hospital and ICU lengths of stay, as well as mortality, particularly in cases where transfers occur from the hospital ward or are delayed.5,6
Respiratory and cardiac events are common reasons for ICU admission.6 Almost all mortality in the Vascular Events in Noncardiac Surgery Patients Cohort Evaluation occurred during the post-operative period following the non-cardiac surgical procedure.7 Nearly half of all these events were attributed to sepsis, major bleeding, and myocardial injury after non-cardiac surgery.7 These critical changes in pathophysiology put post-operative patients on a trajectory for unplanned ICU admissions. Several factors, both patient level and those involving the emergent nature of surgical intervention, have been associated with unplanned admissions to the surgical ICU.8 Some of these factors are modifiable, and therefore better pre-operative patient preparation and early proactive ICU admission on an elective basis in the post-surgical period may be occasionally necessary.9 The severity of sickness or injury and the burden of pre-existing illness are almost universally identified as risk factors for unplanned medical ICU admission. In some cases, age and the nature of underlying disease drive admission.6,10
Monitoring practices on hospital wards may be linked to unplanned ICU transfers. Spot check intermittent monitoring is the driver of most early warning scores. Early warning scores that trigger activation of rapid response teams are often delayed and lag the evolution of the critical event. As little as a 15-minute delay of the ‘afferent limb’ of the rapid response arc is associated with an increased risk of transfer to the ICU and subsequent mortality.11 Understanding early indicators of patient deterioration on hospital wards with risk scores and prediction models may be necessary to reduce unplanned ICU admissions.12
Detailed patient risk profiles and outcomes of unplanned ICU admissions remain poorly characterized, especially when compared to planned ICU admissions and to patients who do not undergo ICU transfer. In addition, there is a paucity of cost data. The purpose of this retrospective analysis was to identify patient characteristics associated with unplanned ICU admissions during surgical and medical hospital admissions. Secondarily, we describe detailed clinical and health economic outcomes associated with unplanned ICU admissions.
Materials and Methods
This retrospective analysis was conducted using the PINC AI™ Healthcare Database (Premier Inc, Charlotte, NC, USA), hereafter referred to as “the healthcare database”, which is compliant with the Health Insurance Portability and Accountability Act (HIPAA) per 45 Code of Federal Regulations (CFR) 164.514(b)(1) through the “Expert Determination” method. Institutional Review Board (IRB) approval was not required because the study was not classified as human subject research under IRB guidelines. Moreover, due to its de-identified and retrospective nature, this analysis was exempt from the patient informed consent process.
Dataset
The healthcare database used for this analysis contains de-identified data representing approximately 25% of all United States (US) inpatient admissions. It houses discharge information for inpatient admissions including patient demographics, Medicare severity-diagnosis related groups (MS-DRG), International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) primary and secondary diagnosis and procedure codes, department-level billing and cost data, hospital characteristics, and payer information. Sixty percent of the hospitals report costs to the healthcare database based on the hospital accounting system, and 40% of hospitals submit charges, which the healthcare database uses to estimate costs based on the submitted charges and cost:charge ratios that hospitals provide to Centers for Medicare and Medicaid Services (CMS).13 The cost data include both fixed and variable costs and reflect actual costs for patient treatment. Discharge records that included admission in the year 2021 were assessed. Costs were reported in 2021 US dollars. This cost analysis took the perspective of the hospital.
Objectives
The objective of this analysis was to identify the demographic and clinical characteristics associated with unplanned ICU admissions of patients admitted to a medical/surgical general or telemetry care unit. Complete lists of the demographic and clinical characteristics evaluated are provided in Table 1 and Table 2 for medical and surgical patients, respectively. A secondary objective was to describe the clinical and economic outcomes associated with unplanned ICU admissions, including total cost of admission, cost of ICU admission, total hospital length of stay, and ICU length of stay. Refer to Table 3 and Table 4 for complete lists of the clinical and economic outcomes evaluated for medical and surgical patients, respectively.
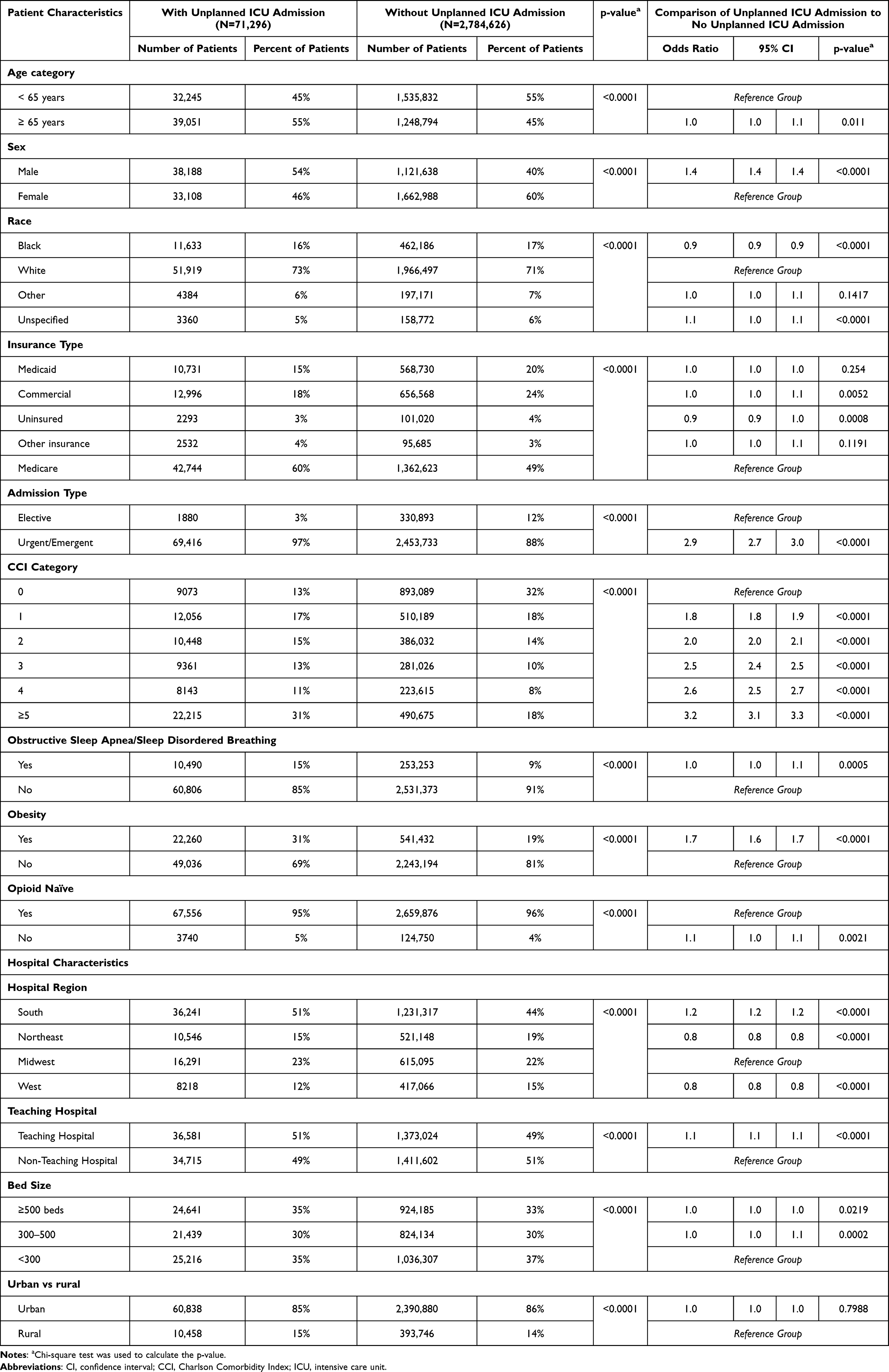 |
Table 1 Medical Patient and Hospital Characteristics Prior to Risk Adjustment Matching |
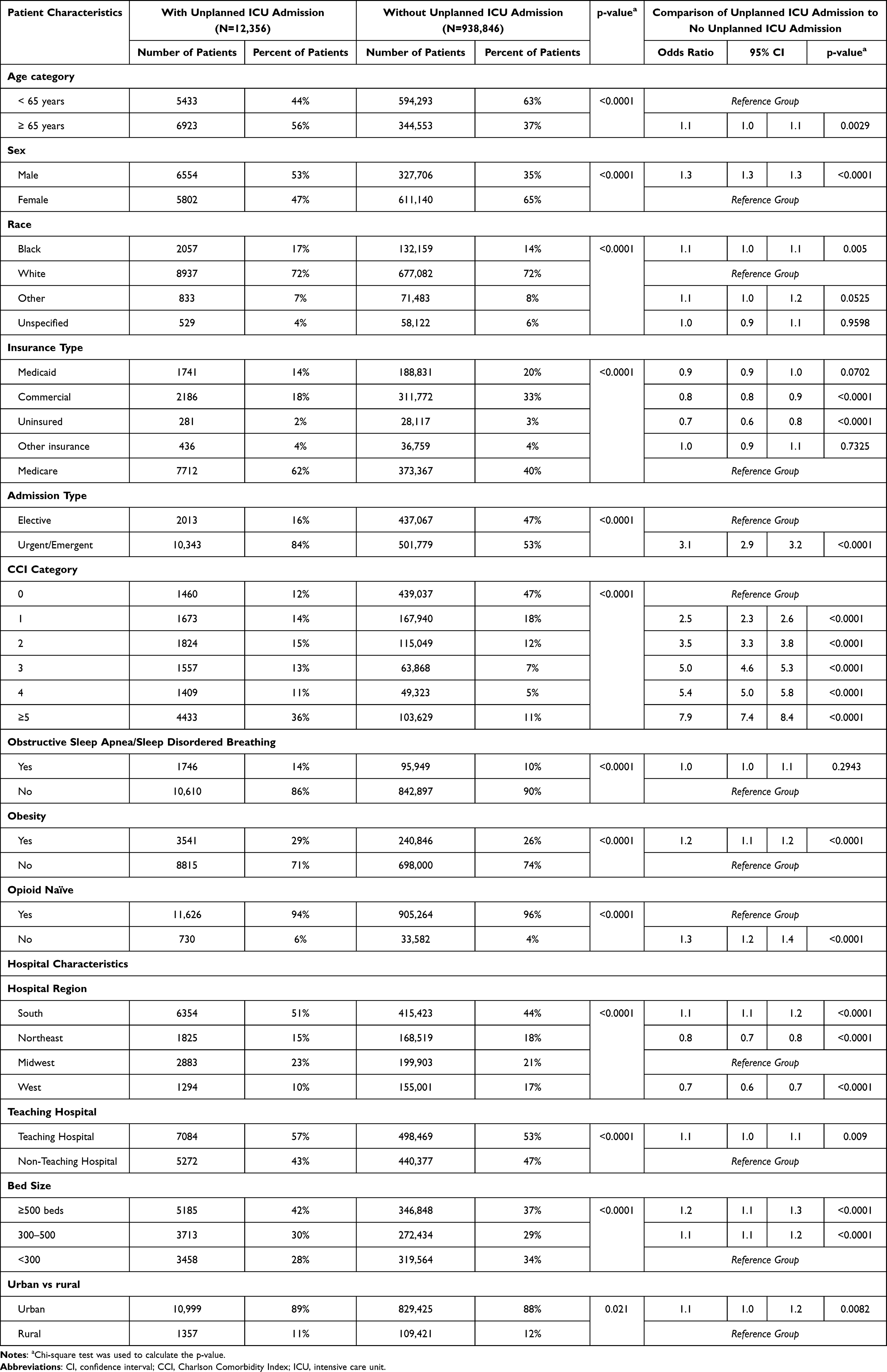 |
Table 2 Surgical Patient and Hospital Characteristics Prior to Risk Adjustment Matching |
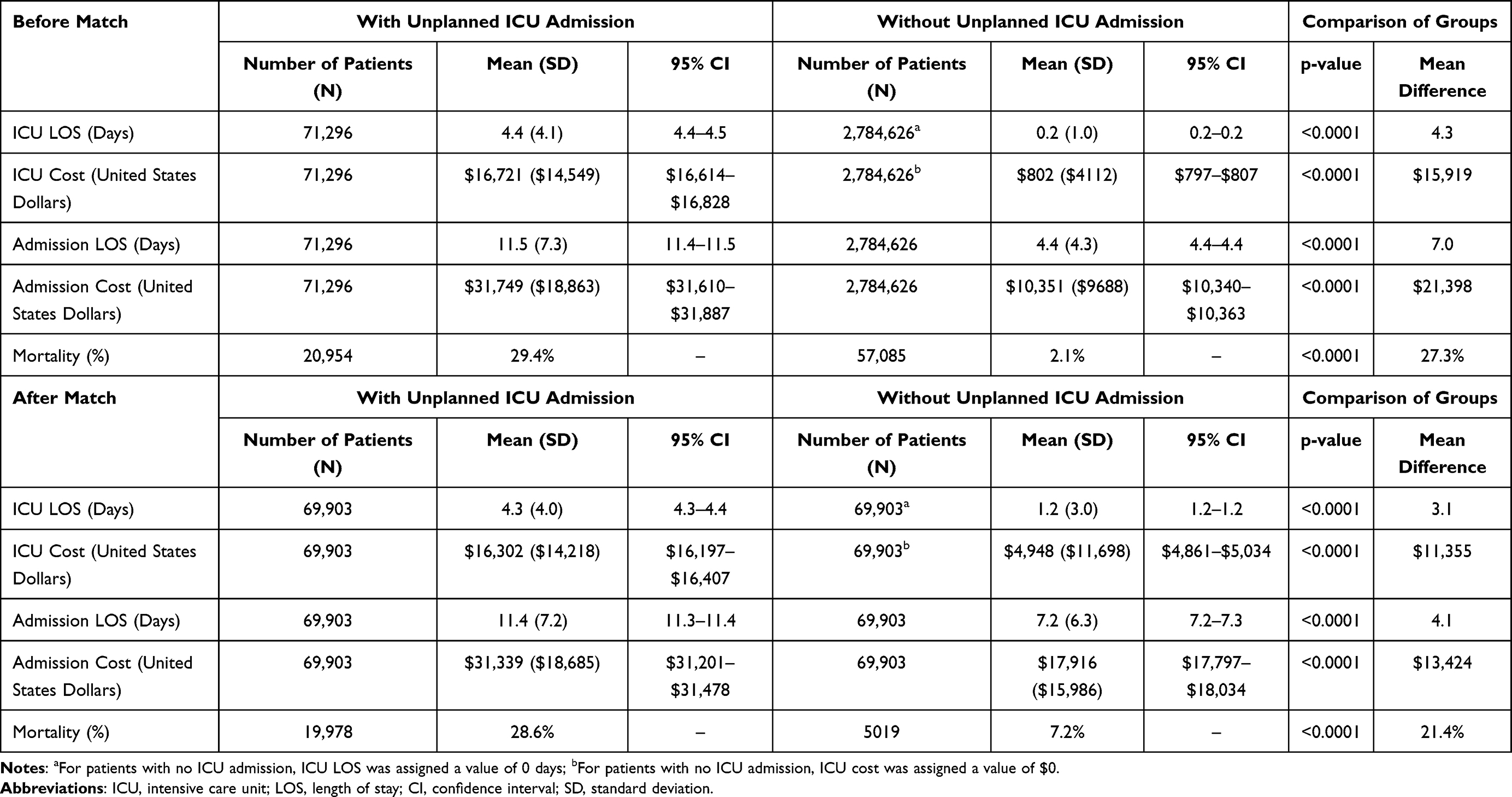 |
Table 3 Economic and Clinical Outcomes Associated with Unplanned ICU Admissions in Medical Patients Before and After Risk Adjustment |
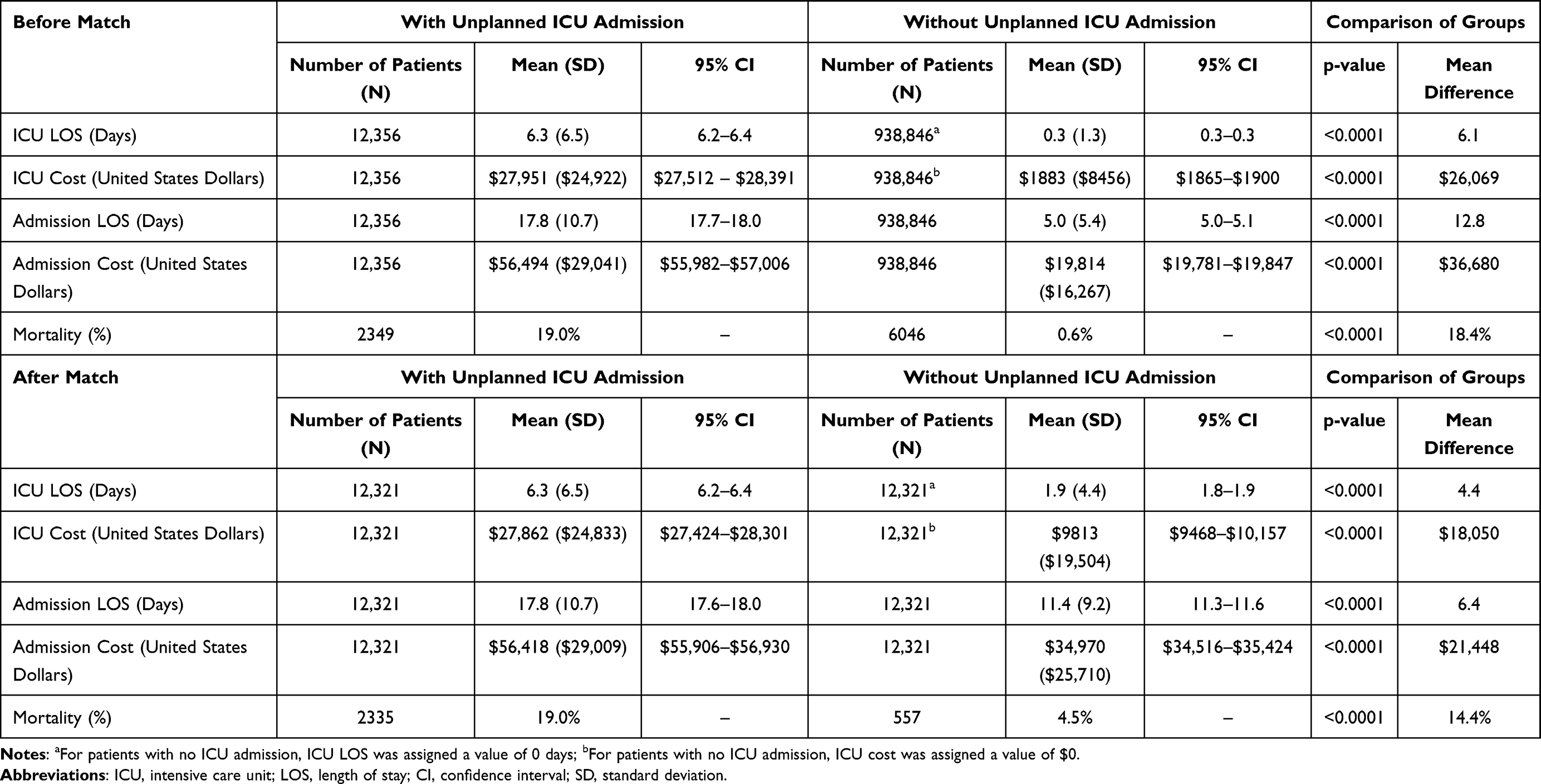 |
Table 4 Economic and Clinical Outcomes Associated with Unplanned ICU Admissions in Surgical Patients Before and After Risk Adjustment |
Analysis Cohort
All admissions occurring in the year 2021 were assessed, and patients aged ≥18 years with medical/surgical or telemetry care floor utilization were selected. Admissions with MS-DRG values that were not classified as medical or surgical by CMS were excluded. Admission records with missing cost data, including records with care floor utilization and admission cost of $0 or ICU utilization and ICU cost of $0, were excluded. Due to the presence of specialized care pathways, admissions involving any cardiac surgical procedure were excluded. Unplanned ICU admission was defined as a direct transfer from a medical, surgical, or telemetry floor to the medical or surgical ICU, including any patients experiencing an ICU bounceback (Tables S1 and S2). Other types of ICU admission, for example, directly from the emergency room (ER) or surgery, were treated as planned ICU admissions. Patients were classified as surgical if they had a timed surgery operating room billing line or a billing line for cesarean section. The sequence of surgery time in relation to the room and board billing day it falls on is inconclusive in the database, resulting in an ambiguous patient pathway. As a result, the analysis required a surgical patient to have one full general ward or telemetry billing day after the surgery billing date to be included in the unplanned ICU transfer cohort. Medical and surgical patients were analyzed as separate cohorts.
Within each cohort, patients with and without an unplanned ICU admission were propensity score matched 1:1 within each MS-DRG using a greedy algorithm and the nearest available neighbor matching method. The propensity score was calculated using multivariable logistic regression with the following predictor variables: age group, sex, race, insurance type, admission type, Charlson Comorbidity Index (CCI) category, obstructive sleep apnea (OSA) or sleep disordered breathing, obesity, opioid naivety, hospital region, teaching or non-teaching hospital, hospital bed size, and urban or rural hospital. Admission type was defined as either elective, in which the patient’s condition permitted adequate time to schedule care, or urgent/emergent, in which the patient required immediate attention for the care and treatment of a physical or mental disorder. CCI is an established measure of long-term mortality risk and assesses the following 19 comorbidities:14,15 AIDS, metastatic solid tumor, moderate or severe liver disease, lymphoma, leukemia, non-metastatic cancer, diabetes with end organ damage, moderate or severe renal disease, hemiplegia, diabetes, mild liver disease, ulcer disease, connective tissue disease, chronic pulmonary disease, dementia, cerebrovascular disease, peripheral vascular disease, congestive heart failure, and myocardial infarction.15
Propensity score matching required an exact match on the MS-DRG value. Admissions for which there were no corresponding records with the same MS-DRG value were excluded. Post matching covariate balance was validated separately for the medical and surgical patient cohorts using the standardized difference of predictor variables between the unplanned ICU admissions group and the comparison group, with threshold value for each variable <0.1.16
Statistics
Data were summarized by descriptive statistics (for continuous variables) or frequencies and percentages (for categorical variables). Statistical tests, including two-sample t-tests for continuous measures and Chi-square tests for categorical measures, were 2-sided. Statistical significance was accepted at p<0.05. Analyses were performed using SAS® Version 9.4 for UNIX (SAS Institute Inc, Cary, NC).
Admission records with total costs below the 1st and above the 99th percentiles across admissions in both the ICU admissions group and the comparison group were excluded from the analysis to minimize the impact of extreme outliers. The cost percentiles for medical and surgical cohorts were calculated independently.
Results
Analysis Cohort
Among the 6,514,189 admissions in 2021 within the healthcare database, 3,807,124 admissions met all inclusion criteria and no exclusion criteria (Figure 1). This included 2,855,922 medical patients and 951,202 surgical patients. Within the medical patient cohort, 71,296 patients (2.5%) had an unplanned ICU admission. Within the surgical patient cohort, 12,356 (1.3%) surgical patients had an unplanned ICU admission. Propensity matched medical and surgical patient cohorts included 69,903 and 12,321 patients, respectively (Figure 1).
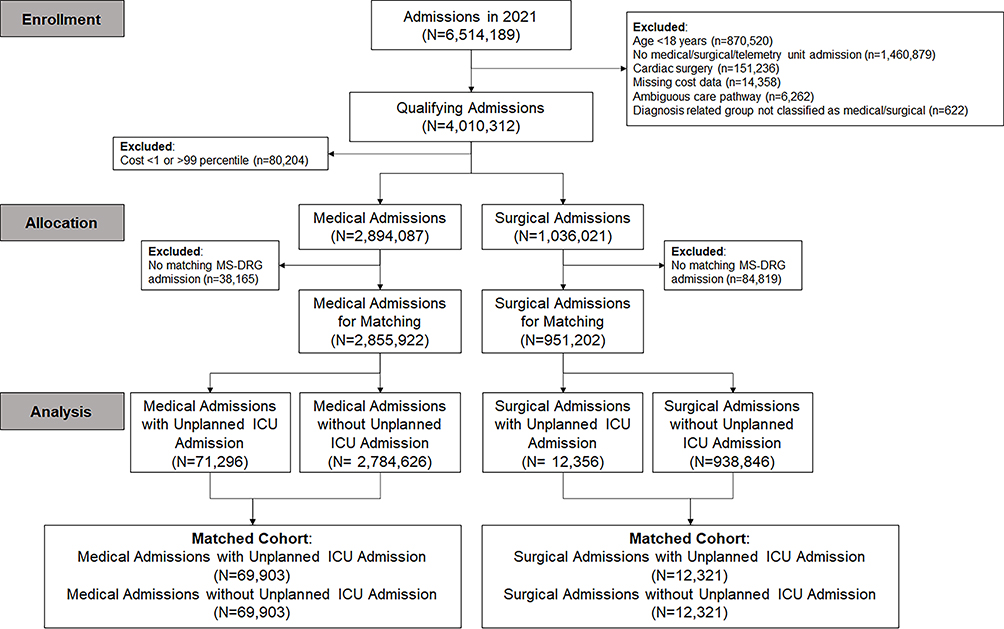 |
Figure 1 Patient selection criteria for inclusion in the analysis cohort. |
Patient Care Pathways and Primary Diagnoses
For medical patients with an unplanned ICU admission, the most common patient care pathway was from the ER to the medical/surgical unit, to the ICU, to the medical/surgical unit, and discharged (Table S1). For medical patients either with or without an unplanned ICU admission, the most common primary diagnoses were COVID-19 and sepsis (Table S2).
For surgical patients with an unplanned ICU admission, the most common patient care pathway was the ER to the medical/surgical unit, to the ICU, to surgery, to the ICU, and discharged (Table S3). Surgical patients with either unplanned ICU admission or no unplanned ICU admission most frequently had a primary diagnosis of either sepsis or COVID-19 (Table S4).
Characteristics of Medical Cohorts Before Propensity Score Matching
Among medical patients, 55% of patients with unplanned ICU admission were ≥65 years of age, compared to 45% of patients without unplanned ICU admission. Fifty four percent and 40% of patients with and without unplanned ICU admission were male, respectively (Table 1). Most admissions were urgent or emergent, comprising 97% and 88% of patients with and without unplanned ICU admission, respectively.
The odds of unplanned ICU admission were significantly higher in patients with urgent or emergent admission (odds ratio [OR] 2.9, 95% confidence interval [CI] 2.7–3.0, p<0.0001), in male patients (OR 1.4, 95% CI 1.4–1.4, p<0.0001) and in patients with obesity (OR 1.7, 95% CI 1.6–1.7, p<0.0001). In addition, compared to patients with a CCI of 0, the odds of unplanned ICU admission increased as the CCI increased from 1 (OR 1.8, 95% CI 1.8–1.9, p<0.0001) to ≥5 (OR 3.2, 95% CI 3.1–3.3, p<0.0001) (Table 1, Figure 2A). The odds of unplanned ICU admission for any of the individual comorbidities within the CCI ranged from 0.939 (95% CI 0.9–1.0, p<0.0001) for dementia, to 2.5 (95% CI 2.4–2.6, p<0.0001) for moderate/severe liver disease (Table S5). Patient and hospital characteristics after risk adjustment matching are provided in Table S6. Post-match covariate balance was validated using standardized mean difference of predictor variables (Figure 3).
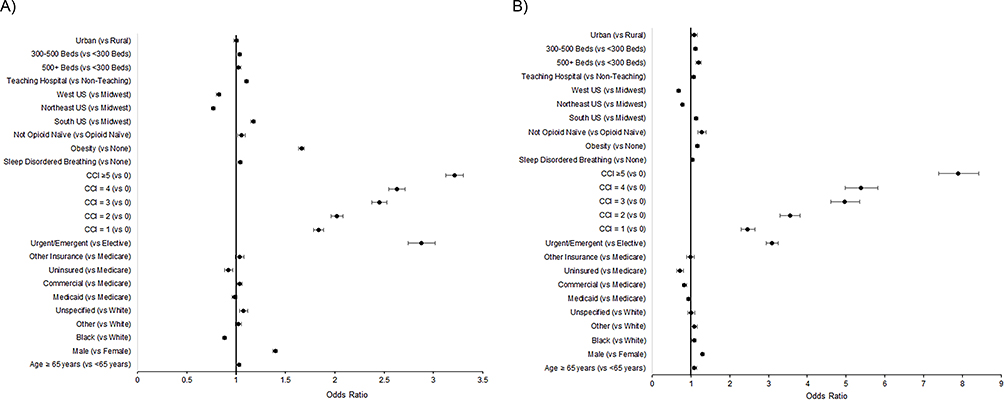 |
Figure 2 Patient demographic and clinical characteristics associated with unplanned ICU admissions, compared to admissions without unplanned ICU admissions, in (A) medical and (B) surgical patients. Points represent odds ratio and bars represent 95% confidence intervals. Abbreviations: OSA, obstructive sleep apnea; CCI, Charlson Comorbidity Index; US, United States. |
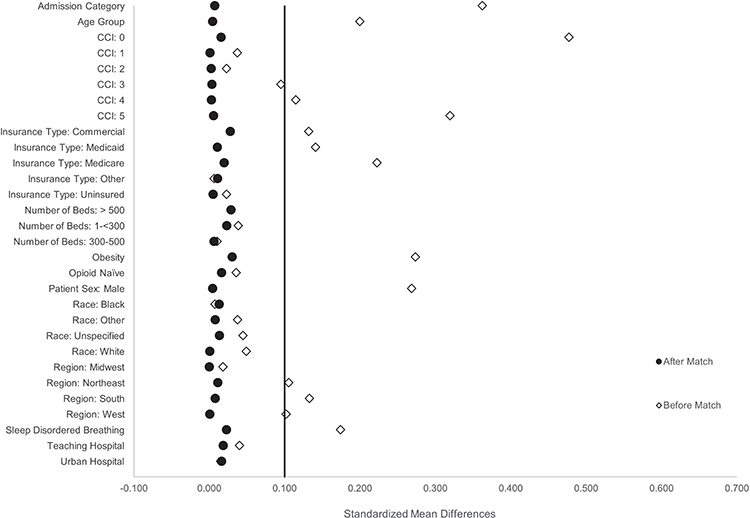 |
Figure 3 Results of the post-match covariate balance validation for predictor variables, medical admissions. Points represent standardized mean differences before matching (white diamonds) and after matching (black circles). Abbreviation: CCI, Charlson Comorbidity Index. |
Characteristics of Surgical Cohorts Before Propensity Score Matching
Among surgical patients, 56% of patients with an unplanned ICU admission and 37% of patients without an unplanned ICU admission were ≥65 years of age (Table 2). Fifty three percent and 35% of patients with and without an unplanned ICU admission were male. Most surgical patients with or without an unplanned ICU admission had no history of OSA or sleep disordered breathing (86% and 90%, respectively), were not obese (71% and 74%, respectively), and were opioid naïve (94% and 96%, respectively).
Surgical patients with an unplanned ICU admission were more likely to have urgent/emergent admissions (OR 3.1, 95% CI 2.9–3.2, p<0.0001), and the odds for unplanned ICU admission increased in a stepwise manner as the CCI increased, from a CCI of 1 (OR 2.5, 95% CI 2.3–2.6, p<0.0001) to a CCI of ≥5 (OR 7.9, 95% CI 7.4–8.4, p<0.0001) (Table 2, Figure 2B). The odds of unplanned ICU admission for any of the individual comorbidities within the CCI ranged from 1.0 (95% CI 1.0–1.1, p=0.3452) for diabetes with complications, to 3.3 (95% CI 3.0–3.6, p<0.0001) for moderate or severe liver disease (Table S7). Patient and hospital characteristics after risk adjustment matching are provided in Table S8. Post-match covariate balance was validated using standardized mean difference of predictor variables (Figure 4).
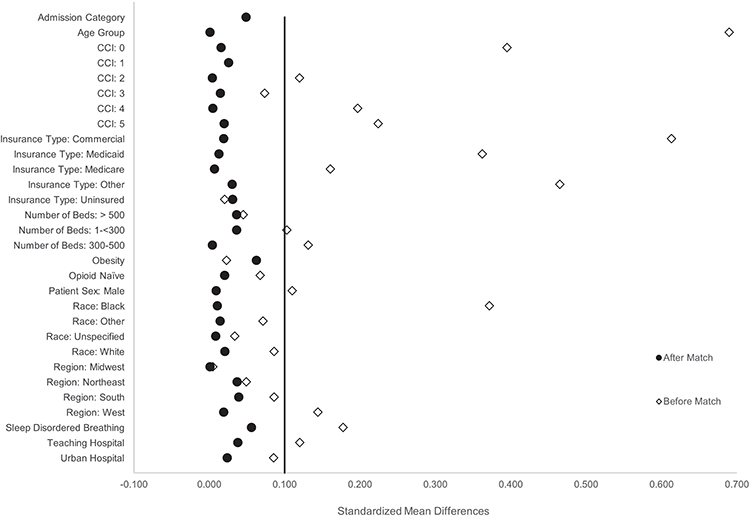 |
Figure 4 Results of the post-match covariate balance validation for predictor variables, surgical admissions. Points represent standardized mean differences before matching (white diamonds) and after matching (black circles). Abbreviation: CCI, Charlson Comorbidity Index. |
Clinical and Economic Outcomes Associated with Unplanned ICU Admissions in Medical Patients
Table 3 provides a brief summary of the main results for clinical and economic outcomes associated with unplanned ICU admissions in medical patients.
In the medical cohort, the mean difference in total admission length of stay between matched patients with and without an unplanned ICU admission was 4.1 days (11.4 ± 7.2 vs 7.2 ± 6.3; p<0.0001), and the mean difference in total admission cost was $13,424 ($31,339 ± $18,685 vs $17,916 ± $15,986; p<0.0001) (Table 3). Similarly, the mean difference in ICU length of stay between matched patients with and without unplanned ICU admission was 3.1 days (4.3 ± 4.0 vs 1.2 ± 3.0; p<0.0001), and the mean difference in ICU cost was $11,355 ($16,302 ± $14,218 vs $4,948 ± $11,698; p<0.0001). In the unmatched population, mortality rates were 29% and 2% in patients with and without an unplanned ICU admission, respectively (p<0.0001). After matching, mortality rates in patients with or without unplanned ICU admission were 29% and 7%, respectively (p<0.0001).
Clinical and Economic Outcomes Associated with Unplanned ICU Admissions in Surgical Patients
Table 4 provides a brief summary of the main results for clinical and economic outcomes associated with unplanned ICU admissions in surgical patients.
Before matching surgical patients, mortality rates for admissions with or without an unplanned ICU transfer were 19% and 1%, respectively (p<0.0001). After matching, the mortality rate in surgical patients with an unplanned ICU admission was 19%, compared to 5% in patients without an unplanned ICU admission (p<0.0001) (Table 4). Between matched patients with and without unplanned ICU admissions, the mean total admission length of stay was 6.4 days longer (17.8 ± 10.7 vs 11.4 ± 9.2; p<0.0001), the mean ICU length of stay was 4.4 days longer (6.3 ± 6.5 vs 1.9 ± 4.4; p<0.0001), the mean total admission cost was $21,448 higher ($56,418 ± $29,009 vs $34,970 ± $25,710; p<0.0001), and the mean ICU cost was $18,050 higher ($27,862 ± $24,833 vs $9,813 ± $19,504; p<0.0001) (Table 4).
Discussion
Our analysis confirms that predominantly males, ≥65 years of age, and with higher CCI scores were more likely to experience unplanned ICU transfers from medical and surgical floors.17–20 Although most patients transferred to the ICU happen to be unplanned, our findings compare well to a large (non-US) multicenter prospective cohort.17 Besides requiring a higher level of care, these patients also carry higher in-hospital mortality, hospital length of stay, and higher mean admission and ICU costs than those who did not need an ICU transfer or went to the ICU directly from the ER, surgery, or the Telemetry unit, which is also consistent with prior literature.17,21–27 For example, Hillman et al reported that patients from the general wards had greater severity of illness (APACHE II) than patients from the ER or surgery, and a greater percentage of those patients died (47.6%) than from the ER (31.5%) and surgery (19.3%).23 Our analysis confirms the significant human toll of patient decline on the general ward, as patients in our cohort who experienced unplanned transfer had a 3 to 4 fold increase in mortality and significantly greater lengths of stay.
Age is known to be an important and independent patient characteristic determining unplanned transfer to medical and surgical ICUs and consequent higher mortality.18 Although our analysis accounted for age, it did not adjust for frailty and decreased physiological reserve, which are known to be important contributors.19,28 Whether systematic prophylactic ICU admission of the critically ill elderly leads to reduction in mortality is a matter of debate, but this was outside the scope of our study.20 Co-morbid burden is a well-recognized factor associated with unplanned ICU transfers, but it is also a formidable patient attribute to plan for. Given the timing of the study period, COVID-19 and sepsis were the most common primary diagnoses among both medical and surgical patients with unplanned transfer to the ICU, and moderate to severe liver disease was the most predictive comorbidity for unplanned ICU transfer. Our findings call for further studies to focus on better planning and triage for ICU transfers to decrease in-hospital mortality and cost of care for patients admitted with moderate to severe liver disease. This study also confirms a higher rate of ICU transfers among patients admitted with a diagnosis of sleep disordered breathing.29 This was reported among both medical and surgical cohorts. This finding calls for the screening of all inpatients for both OSA and obesity-hypoventilation syndrome, and this is particularly important for the obesity-hypoventilation syndrome group because of the need for higher levels of care, as well as postoperative complications.30,31 Overall, these comorbidities are expected to continue to be common reasons for patient transfer to the ICU.
The above examples of underlying co-morbid states make the case for potential earlier transfer to the ICU when the co-morbid load in a clinically deteriorating patient is higher, given that it has consistently been shown that patients transferred from the medical/surgical floors have higher mortality compared to patients admitted directly from the ER, from surgery, or the telemetry unit. In particular, this may be possible for patients in the non-academic setting where ICU bed availability may be less strained. Alternatively, future studies need to develop criteria for identification of patients with a greater co-morbid load and allow clinicians to evaluate the need for better monitoring and proactive intervention on the hospital floors. This is particularly true in the current hospital setting, where ICU bed availability is scarce. Several studies have shown that continuous vital sign monitoring in general hospital wards is associated with reduced ICU transfer and length of stay.32–35 In one study before and after optimization of a continuous monitoring system, Dykes et al found 367.11 avoided ICU days, with an estimated cost savings of 2.3 million.34 Establishing a continuous monitoring system that articulates with an early warning score and decreases time for the afferent response arm of the rapid response team may be an important intervention to decrease unplanned ICU admissions.
To the best of our knowledge this analysis is the first study examining the economic impact of unplanned ICU transfers from medical and surgical wards using a large US database. ICU costs stand at approximately 1% of the US gross domestic product.36 With increasing age and acuity of hospitalized patients, the need for ICU care is likely to grow. At a time when hospital budgets are strained with high inflation and labor shortages, our finding that unplanned ICU transfers result in over 60% greater costs is significant. This analysis illustrates the significant economic burden of escalation of care, allowing hospitals to better understand the financial impact of mitigation strategies aimed at reducing avoidable ICU admissions. Our data are derived from one of the largest US administrative databases, and we analyzed medical and surgical patients separately. All patients identified as unplanned transfers to the ICU represent those that deteriorated on the medical or surgical floors, including telemetry unit patients.
Limitations
This retrospective cohort study, although large, is limited by the use of hospital administrative data. The propensity score calculation was limited to the data available, including patient demographics, comorbidity load, and hospital characteristics. Unplanned ICU admissions were identified using patient care pathways, which rely on the accuracy of billing records. Although higher in-hospital mortality was reported in the unplanned ICU transfer group, the data do not directly compare patients who deteriorated on the medical/surgical floors to patients directly admitted to the ICU from the ER or from surgery. In our study, the three major groups of patients in the cohort without unplanned transfer to ICU were patients directly admitted from the ER to the general medical or surgical floor, ICU, and telemetry floors. Previous smaller studies have reported higher mortality in patients admitted from general wards to the ICU, compared to those admitted from the ER, surgery or the recovery room, sometimes even independent of APACHE scores.25 This further calls for equal emphasis on the underlying co-morbid burden of a deteriorating patient over the adverse clinical event necessitating higher level of care. Our study also does not give us any information about what antecedent adverse events, types of surgery, intra-operative events, surgical complications, vital sign abnormalities, or hospital-level factors such as bed availability and staffing triggered the transfer to the ICU, and whether rapid response teams were involved. COVID-19 patients were a substantial portion of our unplanned ICU cohort. This 2021 data set followed the most disruptive period of 2020 at the beginning of the COVID-19 pandemic. We believe the results are applicable and generalizable to periods with no or lower COVID-19 burden, as our large sample also includes many patients without COVID-19.
Conclusion
In an analysis of >3 million medical and surgical admissions, age and comorbidity burden are the biggest drivers of unplanned medical and surgical ICU admissions. These led to increased ICU mortality and length of stay, which resulted in significantly higher healthcare costs. Early identification of these patients on the hospital wards and proactive measures to prevent decline will be necessary to reduce these critical events and burden on ICU systems.
Abbreviations
CCI, Charlson Comorbidity Index; CI, Confidence Interval; CMS, Centers for Medicare and Medicaid Services; ER, Emergency Room; HIPAA, Health Insurance Portability and Accountability Act; ICD-10-CM, International Classification of Diseases, 10th Revision, Clinical Modification; ICU, Intensive Care Unit; IRB, Institutional review board; MS-DRG, Medicare severity-diagnosis related groups; OR, Odds Ratio; OSA, Obstructive Sleep Apnea; SD, Standard Deviation; US, United States.
Data Sharing Statement
The data supporting the conclusions of this article are included within the article and Supplementary Information.
Ethics Approval and Informed Consent
Not applicable. IRB review and informed consent were not required because the study was not classified as human subject research under IRB guidelines.
Acknowledgments
Medical writing support was provided by Katherine E. Liu, PhD and Alyssa K. Eakley, MS of Medtronic (Minneapolis, MN). A portion of this research was submitted to the Society of Hospital Medicine 2023 Annual Meeting and to the Society of Critical Care Anesthesiologists 2023 Annual Meeting.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The research was funded by Medtronic, which was involved in the design, analysis, interpretation, and manuscript preparation. The authors had access to study data and final responsibility for the decision to submit for publication.
Disclosure
Roop Kaw reports consulting fees from Medtronic. Marilyn A. Moucharite and Patrick Benefield report full time employment with Medtronic. Ashish K. Khanna reports consulting fees from Medtronic, Edwards Lifesciences, Philips Research North America, GE Healthcare, Caretaker Medical, Retia Medical, Baxter, Trevena Pharmaceuticals and support via an NIH/NCATS KL2 award for a trial of continuous portable monitoring on hospital general care floors. The Department of Anesthesiology at Wake Forest School of Medicine is funded by Edwards Lifesciences, Masimo, and Medtronic. The authors report no other conflicts of interest in this work.
References
1. Peixoto SG, Wolf JM, Glaeser AB, Maccari JG, Nasi LA. Longer length of stay, days between discharge/first readmission, and pulmonary involvement >/=50% increase prevalence of admissions in ICU in unplanned readmissions after COVID-19 hospitalizations. J Med Virol. 2022;94(8):3750–3756. doi:10.1002/jmv.27792
2. Peng L, Luo Z, Liang L, et al. Comparison of the performance of 24 early warning scores with the updated National Early Warning Score (NEWS2) for Predicting Unplanned Intensive Care Unit (ICU) admission in postoperative brain tumor patients: a retrospective study at a single center. Med Sci Monit. 2021;27:e929168. doi:10.12659/MSM.929168
3. Cao Q, Fan C, Li W, Bai S, Dong H, Meng H. Unplanned post-anesthesia care unit to ICU transfer following cerebral surgery: a retrospective study. Biol Res Nurs. 2023;25(1):129–136. doi:10.1177/10998004221123288
4. Grimshaw KS, Fan K, Mullins A, Parkosewich J. Using quality improvement methods to understand incidence, timing, and factors associated with unplanned intensive care unit transfers of patients with end-stage liver disease. Prog Transplant. 2019;29(4):361–363. doi:10.1177/1526924819888132
5. Katori N, Yamakawa K, Yagi K, Kimura Y, Doi M, Uezono S. Characteristics and outcomes of unplanned intensive care unit admission after general anesthesia. BMC Anesthesiol. 2022;22(1):191. doi:10.1186/s12871-022-01729-y
6. Mulvey HE, Haslam RD, Laytin AD, Diamond CA, Sims CA. Unplanned ICU admission is associated with worse clinical outcomes in geriatric trauma patients. J Surg Res. 2020;245:13–21. doi:10.1016/j.jss.2019.06.059
7. Spence J, LeManach Y, Chan MTV, et al. Association between complications and death within 30 days after noncardiac surgery. Cmaj. 2019;191(30):E830–e837. doi:10.1503/cmaj.190221
8. Onwochei DN, Fabes J, Walker D, Kumar G, Moonesinghe SR. Critical care after major surgery: a systematic review of risk factors for unplanned admission. Anaesthesia. 2020;75(Suppl 1):e62–e74. doi:10.1111/anae.14793
9. Pecorelli N, Turi S, Salvioni MT, et al. Development of a predictive model for unplanned intensive care unit admission after pancreatic resection within an enhanced recovery pathway. Surg Endosc. 2022;37(4):2932.
10. Laytin AD, Sims CA. Risk factors for unplanned ICU readmission among trauma patients: age matters. Crit Care Explor. 2022;4(10):e0778. doi:10.1097/CCE.0000000000000778
11. Chen J, Bellomo R, Flabouris A, Hillman K, Assareh H, Ou L. Delayed emergency team calls and associated hospital mortality: a multicenter study. Crit Care Med. 2015;43(10):2059–2065. doi:10.1097/CCM.0000000000001192
12. Veldhuis LI, Woittiez NJC, Nanayakkara PWB, Ludikhuize J. Artificial intelligence for the prediction of in-hospital clinical deterioration: a systematic review. Crit Care Explor. 2022;4(9):e0744. doi:10.1097/CCE.0000000000000744
13. PINC AI™ healthcare data white paper: data that informs and performs, September 14, 2021. PINC AI™ Applied Sciences, Premier Inc. Available from: https://offers.premierinc.com/rs/381-NBB-525/images/Premier-Healthcare-Database-Whitepaper-Final.pdf.
14. Austin SR, Wong YN, Uzzo RG, Beck JR, Egleston BL. Why summary comorbidity measures such as the Charlson comorbidity index and elixhauser score work. Med Care. 2015;53(9):e65–72. doi:10.1097/MLR.0b013e318297429c
15. Charlson ME, Carrozzino D, Guidi J, Patierno C. Charlson comorbidity index: a critical review of clinimetric properties. Psychother Psychosom. 2022;91(1):8–35. doi:10.1159/000521288
16. Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat Med. 2009;28(25):3083–3107. doi:10.1002/sim.3697
17. Grieve R, O’Neill S, Basu A, Keele L, Rowan KM, Harris S. Analysis of benefit of intensive care unit transfer for deteriorating ward patients: a patient-centered approach to clinical evaluation. JAMA Network Open. 2019;2(2):e187704–e187704. doi:10.1001/jamanetworkopen.2018.7704
18. Flaatten H, de Lange DW, Artigas A, et al. The status of intensive care medicine research and a future agenda for very old patients in the ICU. Intensive Care Med. 2017;43(9):1319–1328. doi:10.1007/s00134-017-4718-z
19. Bagshaw SM, Webb SA, Delaney A, et al. Very old patients admitted to intensive care in Australia and New Zealand: a multi-centre cohort analysis. Crit Care. 2009;13(2):R45. doi:10.1186/cc7768
20. Guidet B, Leblanc G, Simon T, et al. Effect of systematic intensive care unit triage on long-term mortality among critically ill elderly patients in France: a randomized clinical trial. JAMA. 2017;318(15):1450–1459. doi:10.1001/jama.2017.13889
21. Gabler NB, Ratcliffe SJ, Wagner J, et al. Mortality among patients admitted to strained intensive care units. Am J Respir Crit Care Med. 2013;188(7):800–806. doi:10.1164/rccm.201304-0622OC
22. Simchen E, Sprung CL, Galai N, et al. Survival of critically ill patients hospitalized in and out of intensive care units under paucity of intensive care unit beds. Crit Care Med. 2004;32(8):1654–1661. doi:10.1097/01.CCM.0000133021.22188.35
23. Hillman KM, Bristow PJ, Chey T, et al. Duration of life-threatening antecedents prior to intensive care admission. Intensive Care Med. 2002;28(11):1629–1634. doi:10.1007/s00134-002-1496-y
24. Goldhill DR, Sumner A. Outcome of intensive care patients in a group of British intensive care units. Crit Care Med. 1998;26(8):1337–1345. doi:10.1097/00003246-199808000-00017
25. Escarce JJ, Kelley MA. Admission source to the medical intensive care unit predicts hospital death independent of APACHE II score. JAMA. 1990;264(18):2389–2394. doi:10.1001/jama.1990.03450180053028
26. Lundberg JS, Perl TM, Wiblin T, et al. Septic shock: an analysis of outcomes for patients with onset on hospital wards versus intensive care units. Crit Care Med. 1998;26(6):1020–1024. doi:10.1097/00003246-199806000-00019
27. Sax FL, Charlson ME. Medical patients at high risk for catastrophic deterioration. Crit Care Med. 1987;15(5):510–515. doi:10.1097/00003246-198705000-00012
28. McIsaac DI, Beaule PE, Bryson GL, Van Walraven C. The impact of frailty on outcomes and healthcare resource usage after total joint arthroplasty: a population-based cohort study. Bone Joint J. 2016;98(6):799–805. doi:10.1302/0301-620X.98B6.37124
29. Kaw R, Chung F, Pasupuleti V, Mehta J, Gay PC, Hernandez AV. Meta-analysis of the association between obstructive sleep apnoea and postoperative outcome. Br J Anaesth. 2012;109(6):897–906. doi:10.1093/bja/aes308
30. Chebib N, Nesme P, Freymond N, et al. Acute respiratory failure in obesity-hypoventilation syndrome managed in the ICU. Respir Care. 2019;64(12):1545. doi:10.4187/respcare.06901
31. Kaw R, Bhateja P, Paz YMH, et al. Postoperative complications in patients with unrecognized obesity hypoventilation syndrome undergoing elective noncardiac surgery. Chest. 2016;149(1):84–91. doi:10.1378/chest.14-3216
32. Eddahchouri Y, Peelen RV, Koeneman M, Touw HRW, van Goor H, Bredie SJH. Effect of continuous wireless vital sign monitoring on unplanned ICU admissions and rapid response team calls: a before-and-after study. Br J Anaesth. 2022;128(5):857–863. doi:10.1016/j.bja.2022.01.036
33. Vroman H, Mosch D, Eijkenaar F, et al. Continuous vital sign monitoring in patients after elective abdominal surgery: a retrospective study on clinical outcomes and costs. J Comp Eff Res. 2023;12(2):e220176. doi:10.2217/cer-2022-0176
34. Dykes PC, Lowenthal G, Lipsitz S, et al. Reducing ICU utilization, length of stay, and cost by optimizing the clinical use of continuous monitoring system technology in the hospital. Am J Med. 2022;135(3):337–341.e331. doi:10.1016/j.amjmed.2021.09.024
35. Sun L, Joshi M, Khan SN, Ashrafian H, Darzi A. Clinical impact of multi-parameter continuous non-invasive monitoring in hospital wards: a systematic review and meta-analysis. J R Soc Med. 2020;113(6):217–224. doi:10.1177/0141076820925436
36. Halpern NA, Pastores SM. Critical care medicine beds, use, occupancy, and costs in the United States: a methodological review*. Crit Care Med. 2015;43(11):2452–2459. doi:10.1097/CCM.0000000000001227
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Preadmission Insulin-Treated Type 2 Diabetes Mellitus Patients Had Increased Mortality in Intensive Care Units
Fan R, Xie L, Peng X, Yu B, Zou H, Huang J, Yu X, Wang D, Yang Y
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2135-2148
Published Date: 22 July 2022
Comorbid Heart Disease in Patients with COPD is Associated with Increased Hospitalization and Mortality – A 15-Year Follow-Up
Giezeman M, Sundh J, Athlin Å, Lisspers K, Ställberg B, Janson C, Montgomery S, Kisiel MA, Nager A, Sandelowsky H, Hasselgren M
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:11-21
Published Date: 9 January 2023
In-Hospital Outcomes of Heart Failure Patients with Valvular Heart Disease: Insights from Real-World Claims Data

Izumi C, Matsuyama R, Yamabe K, Iwasaki K, Takeshima T, Murphy SME, Teng L, Igarashi A
ClinicoEconomics and Outcomes Research 2023, 15:349-360
Published Date: 18 May 2023
Association Between the Emergency Department Length of Stay and in-Hospital Mortality: A Retrospective Cohort Study
Habib H, Sudaryo MK
Open Access Emergency Medicine 2023, 15:313-323
Published Date: 13 September 2023
Risk Factors of Gastrointestinal Perforation with a Poor Prognosis
Yuan W, Zhou X, Cai Z, Qiu J, Li X, Tong G
International Journal of General Medicine 2023, 16:4637-4647
Published Date: 16 October 2023