Back to Journals » Infection and Drug Resistance » Volume 19
Pathogen-Specific Hypoalbuminemia in Patients with Sepsis: A Retrospective Study with Propensity Score Analysis
Authors Shao S, Yang J, Yin H, Zheng Y, Yu X, Zhou D, Feng J, Wang J
Received 29 October 2025
Accepted for publication 24 January 2026
Published 3 February 2026 Volume 2026:19 577402
DOI https://doi.org/10.2147/IDR.S577402
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Shasha Shao,1,2,* Jiale Yang,1,2,* Huimei Yin,3 Yan Zheng,1,2 Xi Yu,1,2 Daixing Zhou,1,2 Jun Feng,1,2 Junshuai Wang1,2
1Department of Emergency Medicine, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China; 2Department of Critical Care Medicine, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China; 3Department of Emergency Medicine, Peoples Hospital of Bortala Mongol Autonomous Prefecture, Bole, Xinjiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jun Feng, Department of Critical Care Medicine, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, 1095 JieFang Avenue, Wuhan, 430030, People’s Republic of China, Tel +8627 83665204, Email [email protected] Junshuai Wang, Department of Critical Care Medicine, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, 1095 JieFang Avenue, Wuhan, 430030, People’s Republic of China, Tel +8627 83665204, Email [email protected]
Background: Hypoalbuminemia has been proven to be an independent risk factor for poor prognosis in sepsis. This study attempts to provide a better understanding of the differences in sepsis-related hypoalbuminemia to facilitate efficient identification of high-risk patients by clinicians.
Methods: We collected and analyzed data on 1827 patients with sepsis from the intensive care unit (ICU) retrospectively. Based on their serum albumin levels, the patients were classified into two groups: hypoalbuminemia (n=1405) and non-hypoalbuminemia (n=422). The pathogens were identified based on the results of the blood cultures. We conducted propensity score matching (PSM) to balance baseline characteristics across pathogen groups and minimize confounding factors.
Results: Fourteen species of the most frequently detected pathogens were identified based on blood culture results from patients with sepsis. Eight species of pathogens, including Candida, Klebsiella, Acinetobacter baumannii, Staphylococcus, Pseudomonas, Streptococcus, Enterococcus, and Escherichia coli, caused a significantly higher risk of developing hypoalbuminemia than other pathogen infections, all with statistical differences (p< 0.05). Restricted cubic spline (RCS) analysis showed a U- or L-shaped relationship between serum albumin levels and 28-day all-cause mortality, with critical values that differed across the different species of pathogens. The L-shaped forms of Candida, Staphylococcus, Enterococcus, and Escherichia coli had albumin cut-off values of 30.36 g/L, 32.27 g/L, 30.46 g/L, and 30.95 g/L, respectively. While Bacteroides fragilis exhibited a U-shaped relationship with albumin cut-off values of 33.41 g/L and 39.42 g/L.
Conclusion: Our findings highlight the significance of meticulous surveillance of serum albumin levels in septic patients exposed to different species of pathogens. It is essential to pay attention to the pathogen-specific albumin threshold, not only for the efficient identification of high-risk patients, but also for prompt therapeutic interventions that can improve patient prognosis.
Keywords: sepsis, pathogen infection, hypoalbuminemia, propensity score method
Background
Sepsis, as defined by the 2016 update to the International Consensus Definitions for Sepsis (Sepsis-3.0), is characterized as a dysregulated host response to infection resulting in life-threatening tissue hypoperfusion and organ dysfunction, and it is one of the most common critical diseases in intensive care unit(ICU), with high morbidity and mortality.1,2 It is a well-established fact that albumin is the most abundant circulating protein, accounting for approximately 70% of the plasma’s oncotic power. This molecule also participates in many other biological functions, including binding, transport, and detoxification of endogenous and exogenous compounds, antioxidation, and modulation of inflammatory and immune responses.3 In critical illnesses, such as sepsis and severe trauma, the permeability of the vascular wall increases. The transendothelial escape of serum albumin contributes to hypoalbuminemia and edema formation.4 Hypoalbuminemia, whether direct or indirect, will weaken the protective effects on the body, aggravate the condition of patients with sepsis, increase the risk of complications, such as multiple organ dysfunction syndrome, and then result in poor prognosis of patients. As studies have demonstrated that critically ill patients with hypoalbuminemia upon admission have a significantly longer ICU length of stay and higher mortality.5,6 In clinical practice, hypoalbuminemia was defined as serum albumin levels of less than 35 g/L. Increasing or decreasing serum albumin levels are adequate indicators, respectively, of improvement or deterioration of the clinical state.7,8 Thus, serum albumin level serves as a key prognostic biomarker in sepsis, enabling early identification of high-risk patients and timely intervention, thereby improving patient prognosis.
However, there is still controversy in albumin administration as a therapeutic option for sepsis. This is largely due to a lack of research on hypoalbuminemia caused by specific pathogen species, which is an important gap in knowledge. In regard to the present clinical concern, we conducted this study retrospectively to explore the association between hypoalbuminemia and the most frequently detected pathogens in our local area. Of the total fourteen species of pathogens, eight species of pathogens, including Candida, Klebsiella, Acinetobacter baumannii (A. baumannii), Staphylococcus, Pseudomonas, Streptococcus, Enterococcus, and Escherichia coli exhibited a considerably higher risk of developing hypoalbuminemia compared to those caused by other pathogens. Subsequently, propensity-matched populations were analyzed to investigate the relationship between various pathogens and hypoalbuminemia, with distinct models and threshold values established for hypoalbuminemia caused by each specific pathogen. For this scenario, this study provides sufficient microbial species, establishing a foundation for examining pathogen-specific albumin alterations. We also endeavor to address this part of the research gap by evaluating hypoalbuminemia across different pathogens, with the objective of optimizing albumin therapy for septic patients infected with different pathogens.
Patients and Methods
Study Design and Population
We collected patients diagnosed with sepsis in the intensive care unit (ICU) of Wuhan Tongji Hospital between January 2008 and June 2025, adhering to the STROBE guidelines. The study was approved by the Ethics Committee of Tongji Hospital (No. TJ-IRB20250057). All procedures were performed in accordance with the Declaration of Helsinki. The flow chart for patient enrollment is shown in Figure 1.
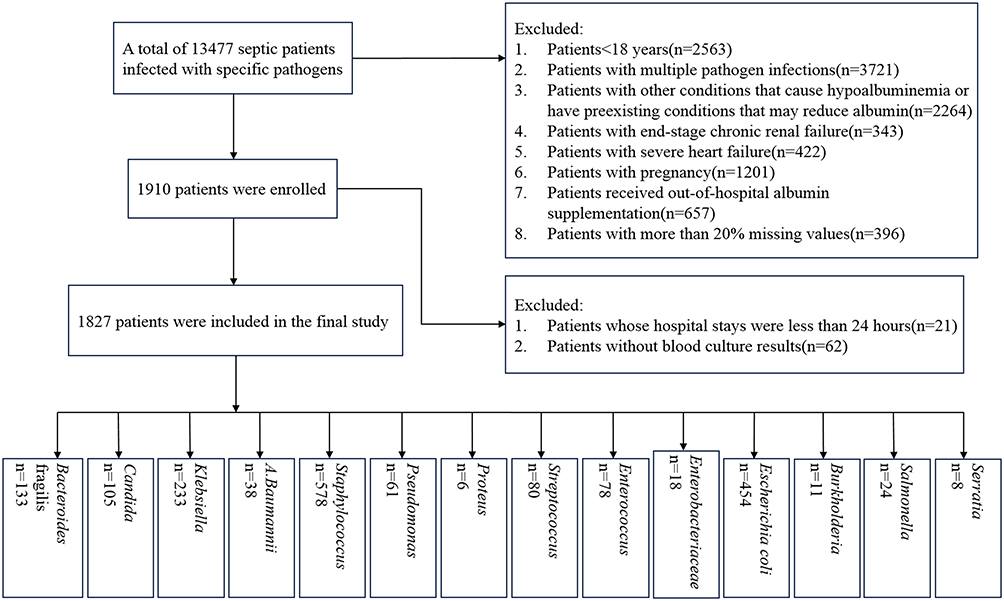 |
Figure 1 A flow diagram of patient enrollment. |
Data Collection
Clinical information was obtained from all patients, including baseline characteristics (age, sex, medical status), vital signs, and laboratory indicators, as well as SOFA (Sequential Organ Failure Assessment) scores on admission to the ICU. Hypoalbuminemia was defined as serum albumin content<35g/L. Based on their serum albumin levels, the patients were classified into two groups: hypoalbuminemia (n=1405) and non-hypoalbuminemia (n=422). The pathogens were identified based on the results of the blood cultures in this study.
Definition
The diagnosis of sepsis was determined according to the “Third International Consensus Definition for Sepsis and Septic Shock” (ie, sepsis-3.0). Sepsis is defined as life-threatening organ dysfunction resulting from a dysregulated host response to infection. An increase in the SOFA score of ≥2 was defined as organ dysfunction. Septic shock was defined as severe circulatory and cellular metabolic abnormalities in addition to sepsis requiring the use of vasoactive agents to maintain mean arterial pressure ≥65mmHg and blood lactate>2mmol/L despite adequate fluid resuscitation.1 The inclusion criteria were: (1) age ≥18 years; (2) The presence of pathogenic pathogens was confirmed by blood culture; (3) hospital stay ≥24 hours.
Patients were excluded according to the following exclusion criteria: (1) infection with multiple pathogens or the results of microbial culture were contaminated by other microorganisms;9 (2) other conditions that cause hypoalbuminemia or have preexisting conditions that may reduce albumin, including liver diseases (acute and chronic hepatitis, severe hepatitis, cirrhosis, liver cancer, etc)., protein loss (including nephrotic syndrome, gastrointestinal ulcer, inflammatory bowel disease, extensive burns, trauma, etc)., chronic wasting diseases (malignant tumor, tuberculosis, etc.) and autoimmune diseases (systemic lupus erythematosus, etc.) or hyperthyroidism and radiotherapy or chemotherapy within the previous three months; (3) end-stage chronic renal failure; (4) severe heart failure; (5) pregnant patients; (6) out-of-hospital albumin supplementation; (7) more than 20% missing values.
Outcome
The primary outcome was the incidence of hypoalbuminemia across various pathogens. The secondary outcome was 28-day all-cause mortality.
Statistical Analysis
SPSS 25.0 and R 4.4.2 were used to perform the statistical analysis of the data in this study. Data following a normal distribution were expressed as the mean ± standard deviation (mean ± SD) and analyzed using one-way ANOVA or Student’s t-test. The measurement data for the non-normal distribution were expressed as median (interquartile range) [M(IQR)] and the rank-sum test (Mann–Whitney U-test) was used to analyze the data. Qualitative data were expressed as examples or percentages and analyzed by chi-square test. Statistical significance was indicated by p<0.05 (two-sided).
To rule out other potential causes of hypoalbuminemia, we used the nearest neighbor matching method from propensity score matching (PSM) to match the baseline data of groups infected with different pathogens. We used a caliper value of 0.2 to determine the association between different pathogens and hypoalbuminemia. Kaplan-Meier curves were used to create survival plots. Multivariate Cox proportional hazards models were applied to assess the relationship between hypoalbuminemia and 28-day mortality. Restricted cubic splines (RCS) were constructed to assess the association between albumin content and 28-day all-cause mortality.
Results
Demographic and Baseline Characteristics
A total of 13,477 patients with confirmed sepsis and a specific pathogen were collected on the basis of inclusion criteria, 11,650 patients were excluded on the basis of exclusion criteria, and finally, 1827 patients were included. Figure 1 shows the flow chart for patient enrollment.
Of the 1827 patients with sepsis, 1405 had hypoalbuminemia (serum albumin <35g/L), while 422 had non-hypoalbuminemia (serum albumin ≥35g/L). We found that patients with hypoalbuminemia were older, more susceptible to congestive heart failure and diabetes, and more likely to progress to septic shock with higher mortality rates (p<0.001, respectively).
The five most commonly detected pathogens were Staphylococcus (578 cases), Escherichia coli (454 cases), Klebsiella (233 cases), Bacteroides fragilis (133 cases) and Candida (105 cases). However, the most frequent incidence of hypoalbuminemia was associated with infections caused by A. baumannii 92.1% (p=0.025), followed by Candida (87.6%, p=0.007), Klebsiella (87.6%, p<0.001), Serratia (87.5%, p<0.001), Escherichia coli (81.9%, p=0.003), Staphylococcus (69.6%, p<0.001) and Bacteroides fragilis (58.6%, p<0.001)(Table 1). Baseline characteristics of the septic patients including age, gender, disease severity and clinical outcomes based on serum albumin level are shown in Table 1.
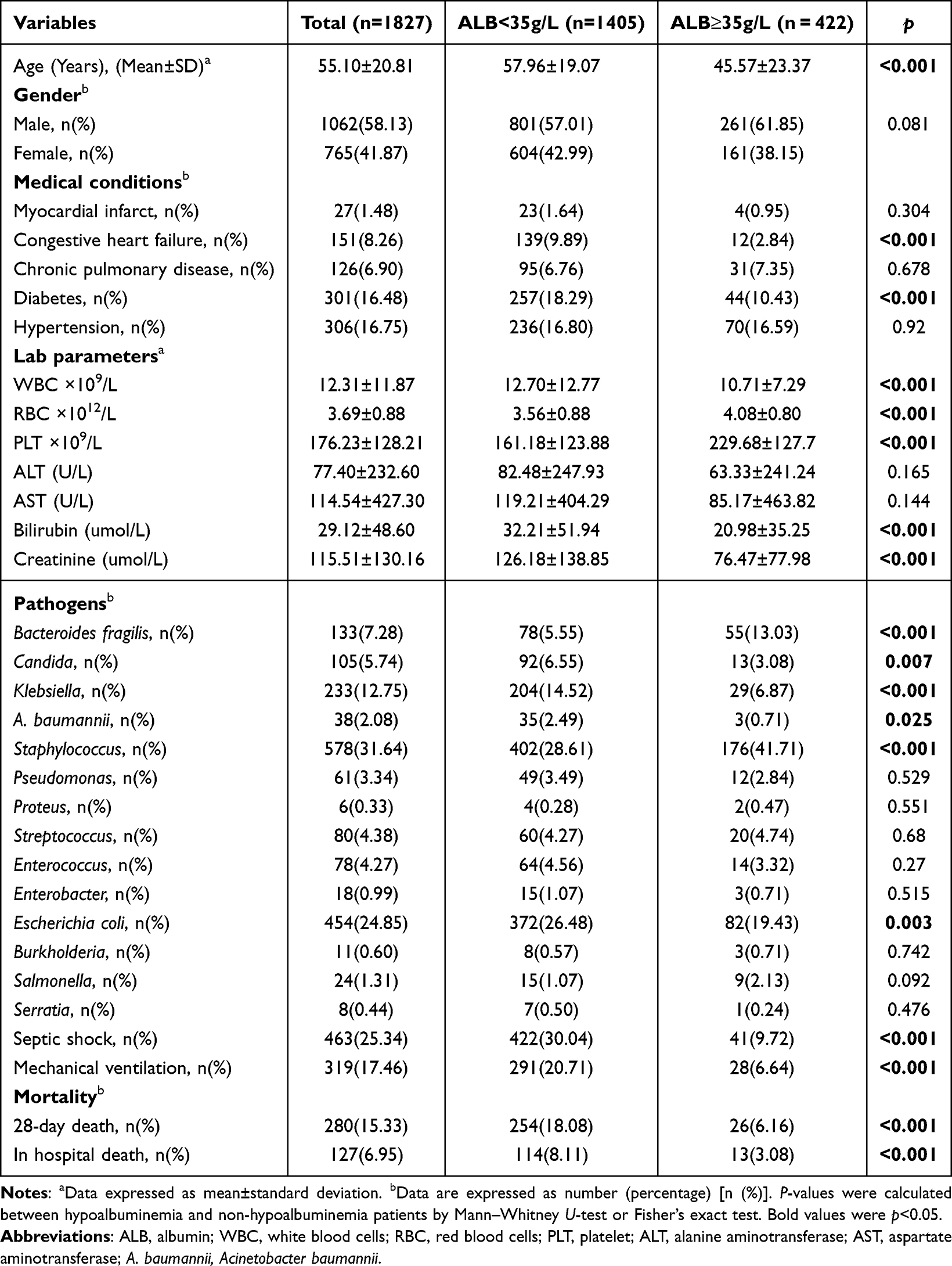 |
Table 1 Demographic and Clinical Characteristics of Patients with Sepsis |
Hypoalbuminemia Is an Independent Risk Factor for Sepsis-Related Mortality
Both univariate and multivariate analyses were performed to identify risk factors associated with 28-day all-cause mortality. As shown in Table 2, there was a significant difference between the hypoalbuminemia group and the non-hypoalbuminemia group (p<0.001). To investigate the association between serum albumin content and 28-day all-cause mortality, Cox proportional hazards models were used to analyze the association between hypoalbuminemia and 28-day all-cause mortality in all patients. Multivariate Cox regression analysis revealed that hypoalbuminemia was an independent risk factor for 28-day mortality (hazard ratio [HR]=1.72, 95% confidence interval [CI]=1.14–2.61, p=0.01; Table 2).
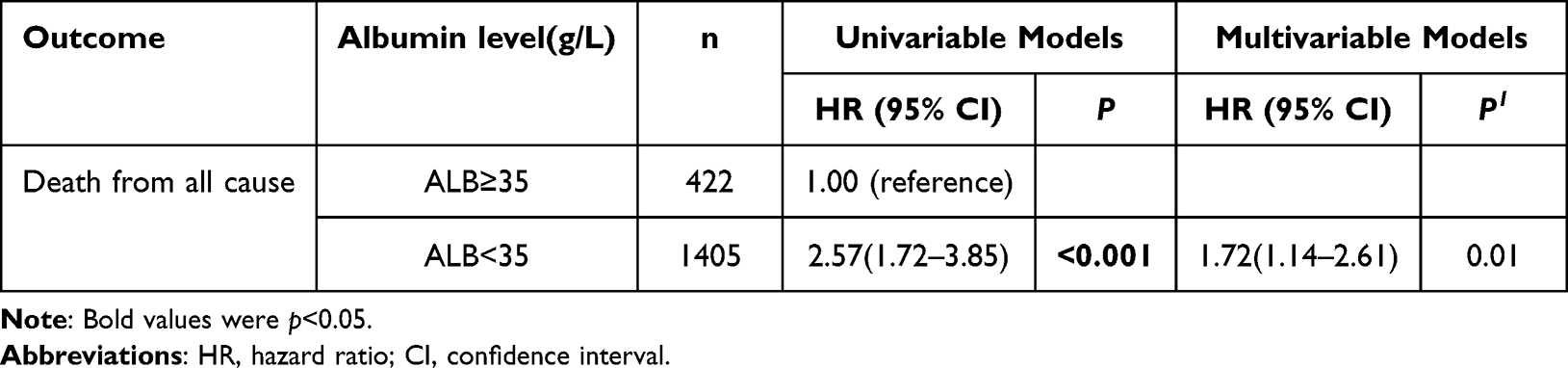 |
Table 2 Univariate and Multivariate Associations of Hypoproteinemia with 28-Day All-Cause Mortality in All Patients |
A subsequent Kaplan-Meier analysis of the patients showed a significantly increased risk of 28-day mortality among patients with hypoalbuminemia as compared with those without hypoalbuminemia (log-rank p<0.001, Figure 2).
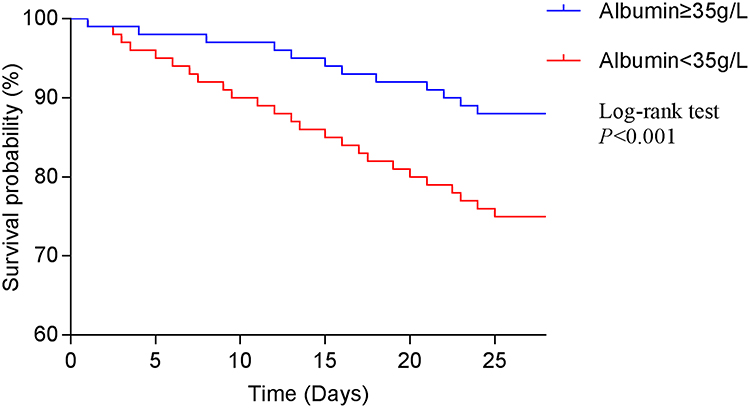 |
Figure 2 The 28-day survival rate of sepsis patients with and without hypoalbuminemia. Accumulated survival probabilities were compared between the hypoalbuminemia and non-hypoalbuminemia groups. A significant difference in survival rates was observed between the two groups at the end of the 28-day period (p<0.001). |
The Incidence of Hypoalbuminemia Differs Among Different Species of Pathogen Infections
We analyzed the proportion of hypoalbuminemia in sepsis patients infected with different pathogens. Multivariate logistic regression was utilized to evaluate the independent impact of particular pathogens on serum albumin in patients with sepsis. The incidence of hypoalbuminemia in patients infected with fourteen different species of pathogens was as follows: A. baumannii (92.1%), Candida (87.6%), Klebsiella (87.6%), Serratia (87.5%), Enterobacter (83.3%), Enterococcus (82.1%), Escherichia coli (81.9%), Pseudomonas (80.3%), Streptococcus (75.0%), Burkholderia (72.7%), Staphylococcus (69.6%), Proteus (66.7%), Salmonella (62.5%), and Bacteroides fragilis (58.6%), respectively. As shown in Figure 3, there were significant differences in the proportion of patients with hypoalbuminemia among patients infected with different pathogens.
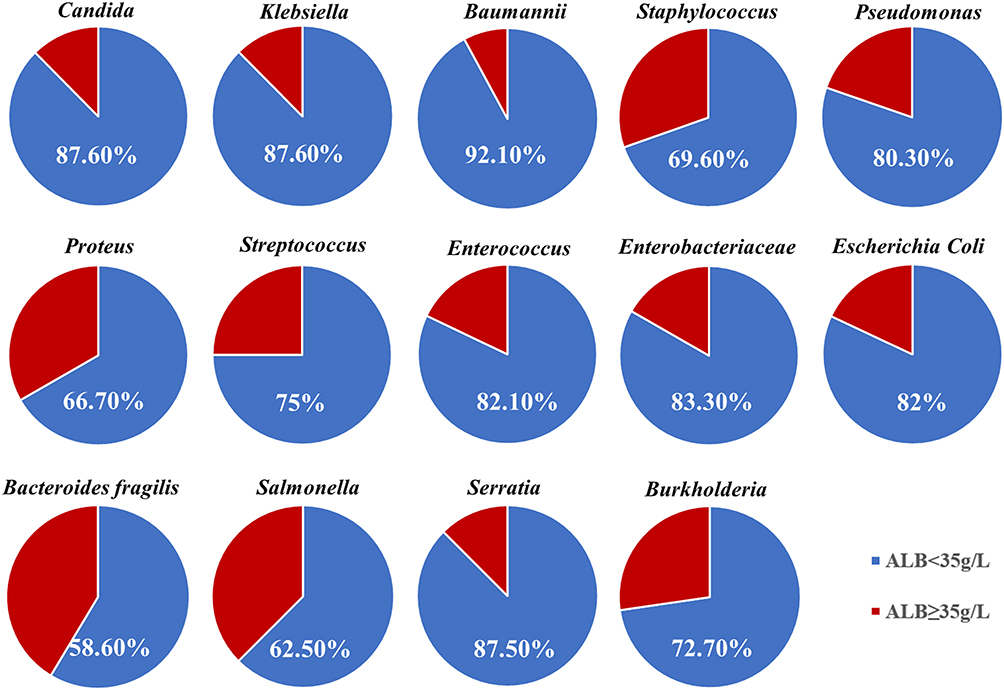 |
Figure 3 The incidence of hypoalbuminemia varies among patients with sepsis caused by different pathogens. The pie charts illustrated a significant variation in the incidence of hypoalbuminemia among patients infected with 14 different pathogens. |
A Mann–Whitney U-test was performed to determine whether 14 different species of pathogens could cause different levels of serum albumin. The serum albumin levels differ across the different pathogens, as shown in Table 3 (p<0.001).
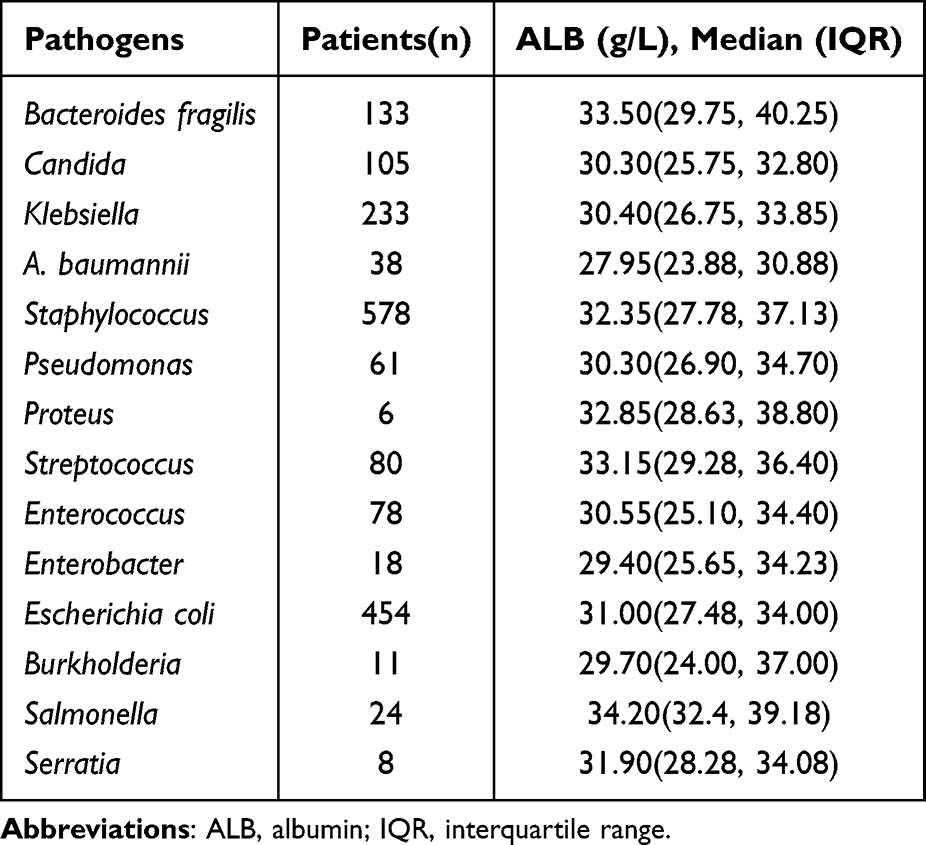 |
Table 3 The Ranges of Hypoalbuminemia Induced by Different Pathogens |
Eight Species of Pathogen Infections Significantly Predict the Risk of Hypoalbuminemia
We used a multivariate binary logistic regression model to figure out the risk of hypoalbuminemia. After adjusting for confounding factors, such as age, comorbidities, septic shock, and the use of mechanical ventilation, we found that eight species of pathogens, including Candida (OR, 4.07; 95% CI, 2.00–8.27; p<0.001), Klebsiella (OR, 3.76; 95% CI, 2.17–6.51; p<0.001), A. baumannii (OR, 4.73; 95% CI, 1.33–16.82; p=0.016), Staphylococcus (OR, 1.88; 95% CI, 1.24–2.85; p=0.003), Pseudomonas (OR, 2.63; 95% CI, 1.22–5.66; p=0.013), Streptococcus (OR, 2.04; 95% CI, 1.08–3.88; p=0.029), Enterococcus (OR, 2.64; 95% CI, 1.30–5.39; p=0.007), Escherichia coli (OR, 2.22; 95% CI, 1.41–3.49; p=0.001) had a significantly increased risk of hypoalbuminemia (Figure 4). Additional potential confounders were added by stepwise selection.
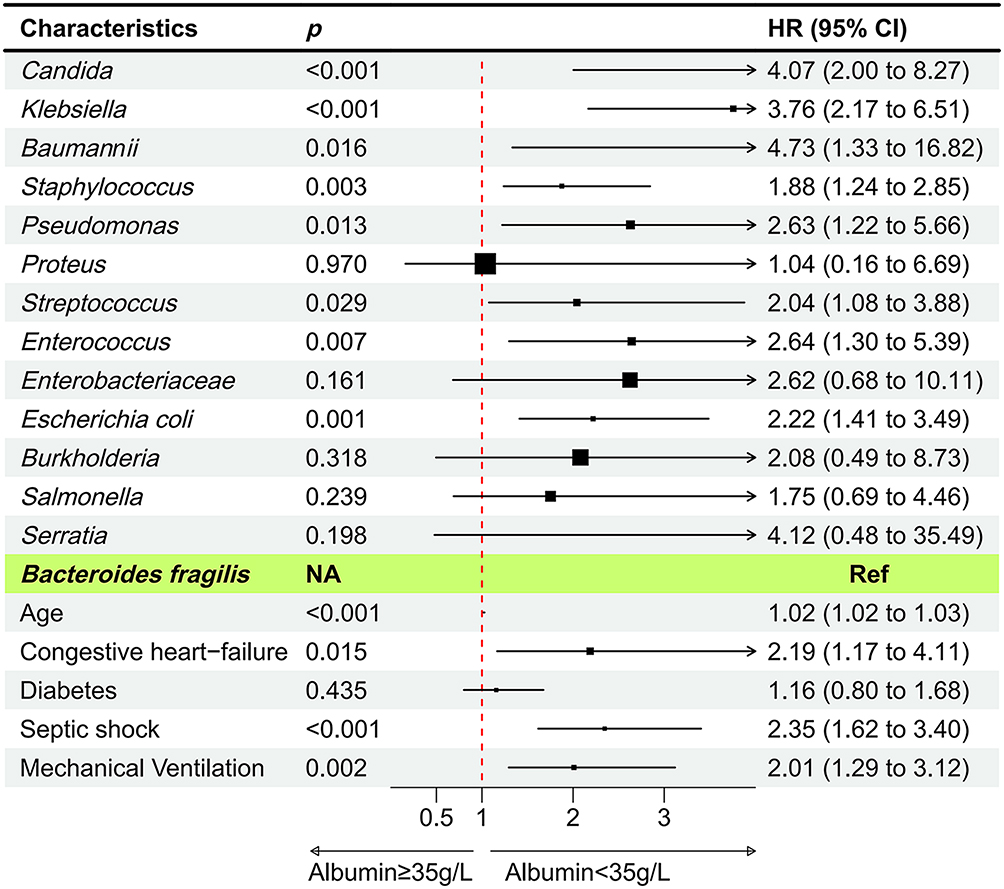 |
Figure 4 The multivariate-adjusted correlation between specific pathogens and the incidence of hypoalbuminemia. Bacteroides fragilis was set as the reference pathogen indicated in the colored context. Abbreviations: CI, confidence interval; OR, odds ratio; NA, not available; Ref, reference. |
To rule out the possibility of hypoalbuminemia due to other factors during infection, we used propensity-matched populations (as detailed in the statistical analysis) to predict the risk of hypoalbuminemia for different pathogen species (Table 4).
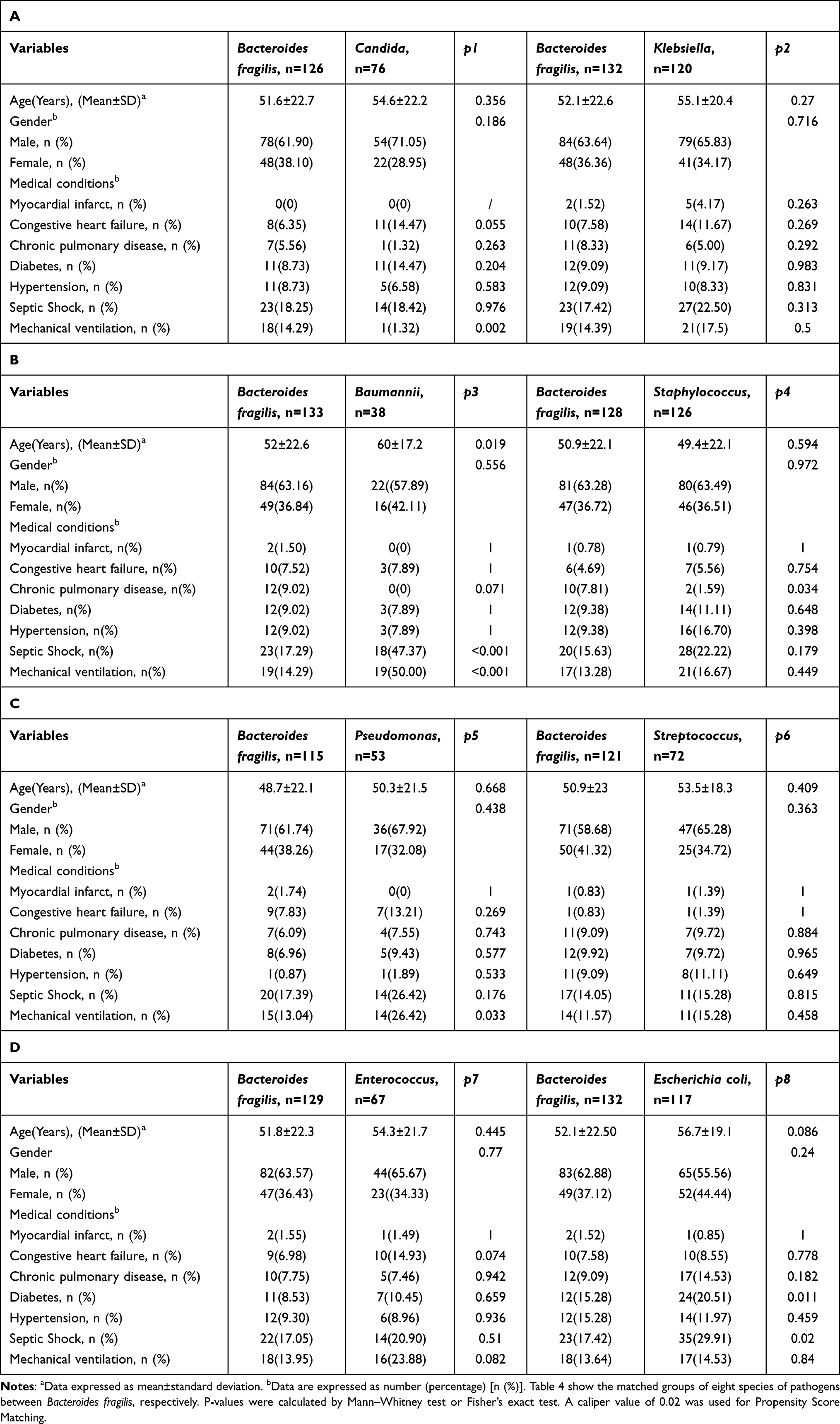 |
Table 4 The Characteristics of Patients in the Propensity-Matched Population |
Analysis of a multivariate binary logistic regression model confirmed that the following eight species of pathogens had a higher risk of hypoalbuminemia than others: Candida, Klebsiella, A. baumannii, Staphylococcus, Pseudomonas, Streptococcus, Enterococcus, and Escherichia coli (Table 5).
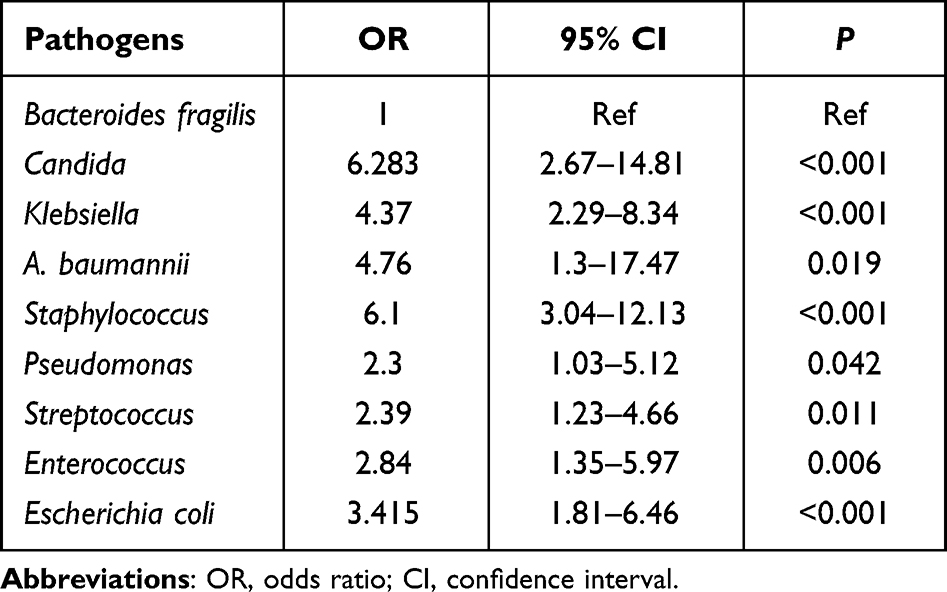 |
Table 5 Multivariate Analysis of Hypoalbuminemia by Propensity-Matched Methods |
Pathogen-Specific Hypoalbuminemia Leads to Distinct Models of Mortality Hazard Ratios
Based on RCS of the multivariate Cox proportional hazards model, we further examined the specific relationship between hypoalbuminemia and 28-day all-cause mortality among patients with different pathogens. After adjusting for age and other confounding factors, RCS analysis revealed that Candida, Staphylococcus, Enterococcus, and Escherichia coli exhibited an L-shaped curve. The albumin cut-off values were 30.36 g/L, 32.27 g/L, 30.46 g/L, and 30.95 g/L, suggesting that the mortality risk decreased with increasing albumin levels. The slope was steep when the albumin level was extremely low and was stable when the albumin level was increased. Whereas Bacteroides fragilis showed a U-shaped relationship with albumin cut-off values of 33.41 g/L and 39.42 g/L, indicating that the mortality hazard ratio decreased with increasing albumin levels and then increased with continued increases in albumin levels (Figure 5).
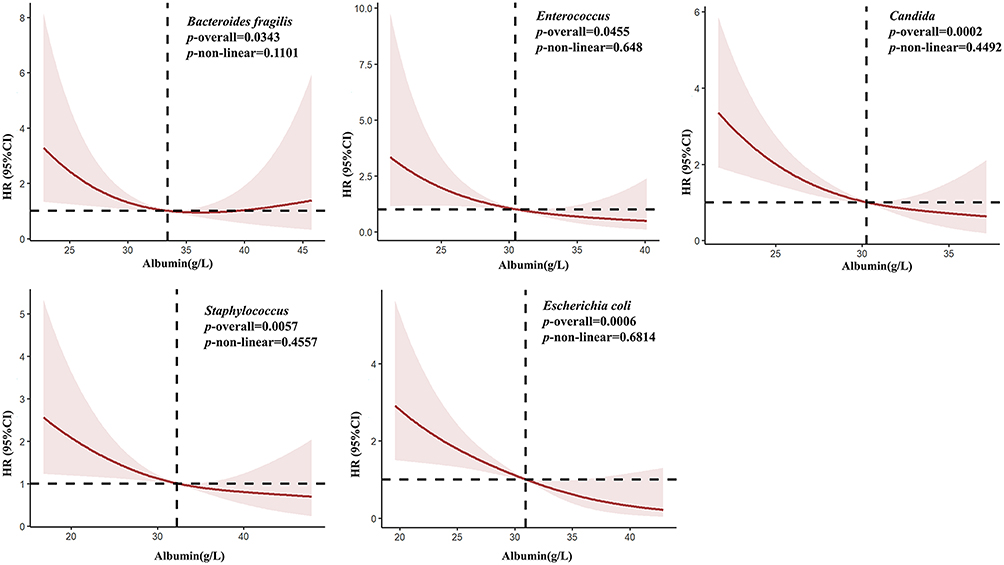 |
Figure 5 Correlation between albumin level and 28-day all-cause mortality in pathogen-specific RCS models. L-shaped: mortality hazard ratios decreased as albumin level increased. U-shaped: mortality hazard ratios decreased with increasing albumin level and then increased with continued increases in albumin level. Albumin (g/L). Abbreviation: RCS, restricted cubic spline. |
Discussion
This is the first study to explore distinctions in sepsis-related hypoalbuminemia across different species of pathogens. On the one hand, albumin can bind to and neutralize bacterial toxins, thereby reducing the damage they would otherwise cause to the host body.10–12 On the other hand, its antioxidant and anti-inflammatory effects help alleviate oxidative stress and an excessive inflammatory response in sepsis, thus protecting tissues and organs.13,14 Whether directly or indirectly, the mechanism behind infection-induced hypoalbuminemia is complex and involves a dysregulated inflammatory response triggered by specific microbial components15 (such as endotoxin, exotoxin, or pathogen-associated molecular patterns), vascular leakage,16,17 and an imbalance between albumin synthesis and degradation.8,18 This suggests that a variety of pathogens can interfere with albumin metabolism through different pathways. However, it is unclear whether the incidence and severity of hypoalbuminemia differ among different pathogen species.
The present study is the largest to date to address the impact of specific pathogens on hypoalbuminemia in sepsis, which was designed to investigate the relationship between clinical microbial infections and albumin levels, as well as their impact on prognosis. Our study, as expected, revealed specific variations in serum albumin levels associated with different microbial infections. The results showed that patients with sepsis infection were more likely to have significant hypoalbuminemia if they had infections caused by Candida, Klebsiella, A. baumannii, Staphylococcus, Pseudomonas, Streptococcus, Enterococcus, or Escherichia coli. We also found that for patients infected with Candida, Staphylococcus, Enterococcus, Escherichia coli, and Bacteroides fragilis, a particular association exists between serum albumin levels and 28-day mortality, which appears as an L-shaped or U-shaped curve relationship with different cut-off values. These data suggest that different pathogens have different effects on albumin metabolism in the host. These findings are consistent with previous studies.19,20 These different impacts are likely due to pathogen-specific mechanisms: (1) specific exotoxins directly damage the endothelium or consume albumin; (2) different microbial components, such as lipopolysaccharide (LPS) and peptidoglycan, can trigger various degrees of systemic inflammation and endothelial injury; and (3) the inflammatory cascade has the capacity to selectively reduce the synthesis of hepatic albumin. This mechanistic diversity suggests that hypoalbuminemia in sepsis is not a uniform condition, but rather a state of pathogen heterogeneity. Clinicians should be alert to hypoalbuminemia that may accompany an infection with these pathogens because hypoalbuminemia is an important indicator of poor prognosis. Thus, a management scheme for pathogen-specific hypocholesterolemia may improve microcirculation disorders and alleviate organ function impairment, thereby reducing the risk of sepsis-related complications.
Through an in-depth analysis, this study identified the most common pathogens associated with hypoalbuminemia are A. baumannii (92.1%), Candida (87.6%), Klebsiella (87.6%), Serratia (87.5%), Enterobacter (83.3%), Enterococcus (82.1%), Escherichia coli (81.9%), Pseudomonas (80.3%), Streptococcus (75.0%), Burkholderia (72.7%), Staphylococcus (69.6%), Proteus (66.7%), Salmonella (62.5%), and Bacteroides fragilis (58.6%), respectively. In the pathological process of sepsis, hypoalbuminemia is primarily associated with capillary leakage, impaired liver synthesis, and metabolic disorders resulting from a systemic inflammatory response.21,22 Previous studies have demonstrated that various pathogen infections can result in distinctive alterations in albumin metabolism. Additionally, a dose-response relationship has been observed between serum albumin levels and patient mortality.18,23,24 In consideration of this mechanism, it merits exploration whether the combination of vascular permeability-regulating drugs and precise anti-infection treatment in the early intervention stage can improve the prognosis of patients with sepsis. The treatment strategy for patients with sepsis should include actively maintaining serum albumin levels in the physiological range through nutritional support, albumin infusion, and other means. Furthermore, given the distinct effects of various pathogen infections on albumin metabolism and their evident correlation with sepsis prognosis, targeted interventions are warranted in clinical treatment to ensure that serum albumin levels remain within the physiological range, thereby reducing the risk of complications associated with hypoalbuminemia.
Pre-existing research has demonstrated that hypoalbuminemia is associated with the progression and severity of infectious diseases, and that intact innate and adaptive immune responses are contingent on albumin. Serum albumin levels are prognostic for complications of viral, bacterial, and fungal infections, as well as for infectious complications of non-infective chronic conditions.25,26 In addition, the pharmacokinetics and pharmacodynamics of antimicrobials are affected by non-oncotic properties of albumin. Low serum albumin has been associated with inadequate antimicrobial treatment, and a dose-response relationship has been identified between serum albumin levels and patient mortality.23,24 In randomized controlled trials, the infusion of a human albumin solution has been shown to effectively support antimicrobial therapy by supplementing endogenous albumin in patients with cirrhosis of the liver.27 These findings not only underscored the prognostic significance of hypoalbuminemia for clinical outcomes, including mortality, but also pointed to the potential salutary effects of albumin administration for targeted microcirculation therapy in septic patients.
We made even deeper, more valuable progress in our exploration of the impact of hypoalbuminemia induced by specific pathogens on clinical outcomes. Ultimately, we discovered an L- or U-shaped relationship between serum albumin levels and 28-day mortality in septic patients infected with different pathogens, with varied cutoff values. Candida, Staphylococcus, Enterococcus, and Escherichia coli exhibited an L-shaped curve, and the albumin cut-off values were 30.36 g/L, 32.27 g/L, 30.46 g/L, and 30.95 g/L. A steep slope was observed when albumin levels were low, and a stable slope was observed when albumin level was increased, indicating that the mortality risk decreased with increasing albumin level. Whereas Bacteroides fragilis showed a U-shaped curve with the albumin cut-off values of 33.41 g/L and 39.42 g/L, indicating that the mortality hazard ratio decreased with increased albumin levels and then increased with continued increased in albumin levels. This perspective differed from previous approaches because it was not only pathogen-specific; it also took into account the albumin thresholds of different conditions. Rather than merely serving as observational prognostic indicators, these albumin thresholds could be used to identify high-risk patients, inform dynamic monitoring, and enable precise interventions. Therefore, the pathogen-specific albumin thresholds identified in our study may provide a new basis to the precise management of sepsis. Yet, caution is warranted, particularly for pathogens with smaller sample sizes in our study (such as A. baumannii, Serratia), and these thresholds should be validated in larger, independent cohorts.
Propensity score matching (PSM) is a useful, novel, and creative statistical method for evaluating the effects of interventions using non-experimental or observational data. Paul Rosenbaum and Donald Rubin first proposed this method in 1983. It is used to process data from observational studies. Due to various reasons, observational studies have many data biases and confounding variables. The propensity score matching method is designed to reduce the influence of these biases and confounding variables to allow for a more reasonable comparison between the experimental and control groups.28,29 In this study, we selected Bacteroides fragilis as the reference pathogen for two reasons: (1) B. fragilis is representative of an anaerobic bacterial infection in clinical sepsis, and (2) the distribution of albumin levels in patients with B. fragilis infection differed significantly from those of other pathogens, making B. fragilis a suitable reference for comparison. Although our study is a retrospective study, we used PSM method to exclude patients with exposure to known risk factors at the time of enrollment, including previous conditions that cause hypoalbuminemia, end-stage chronic renal failure, or severe heart failure, in order to minimize the effect of confounding.
This study has the following limitations: First, this is a single-center study that can only represent our local pathogen constitution and not the spectrum of pathogens in other places around the world. And the sample of some pathogen species was relatively small, which might cause bias. Second, this is a retrospective study, even if we try to eliminate the interference of confounding factors by multivariate Cox regression and PSM as much as possible, it is still difficult to account for all confounding factors that may affect the effect of pathogens on hypoalbuminemia. Last but not the least, although we excluded patients who received an albumin infusion outside the hospital, it is difficult to assess the impact of those medications on albumin levels; therefore, to minimize the potential impact of treatment, we selected albumin level at the time of admission to the ICU for our analyses. In this regard, the prospective studies are necessary to determine the most effective approach for optimizing albumin therapy in cases of sepsis-related hypoalbuminemia.
Conclusions
Albumin plays a key role in the host immune and metabolic response to infection, and reduced albumin levels typically indicate disruption of host homeostatic mechanisms. Various pathogens engage in hypoalbuminemia through diverse and complex mechanisms, and the response of albumin to different pathogens may differ during sepsis, which may result in pathogen-specific variations in serum albumin levels. Therefore, clinicians should take into account the albumin thresholds associated with different pathogens when administering albumin treatment to sepsis patients to ensure its appropriate use. As controversy goes, future prospective studies should be designed with multiple centers and larger data platforms to enable more detailed investigation of the impacts, whether direct or indirect, of pathogens on serum albumin levels in patients with sepsis.
Data Sharing Statement
Data for this study are available from the Jun Feng.
Ethics Approval and Consent to Participate
The study was approved by the Ethics Committee of Tongji Hospital (NO. TJ-IRB20250057). Consent to Participate was waived by the Tongji Hospital Research Institutional Review Board due to the retrospective nature of this study. Data collection and analysis were undertaken in compliance with the approval and supervision of the Tongji Hospital Research Institutional Review Board.
Consent for Publication
The complete anonymization of personal information was accomplished during data collection, and the identification of individual patients was impossible. Thus, the requirement for informed consent by each patient was waived by our Ethics Committee.
Acknowledgments
We would like to thank our colleagues for all their collaboration and dedication to enhance patient safety and improve patient survival. We thank all the patients who participated in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was financed by This research was supported by the Fund of Central Government Guides Local Science and Technology Development, China (grant no. 20225EIA053 to J.F) and the Natural Science Foundation of Xinjiang Uygur Autonomous Region, China (grant no. 2022D01F65 to HM.Y).
Disclosure
The authors declare no conflict of interest.
References
1. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–14.
2. Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Crit Care Med. 2021;49(11):e1063–e1143.
3. Pompili E, Zaccherini G, Baldassarre M, Iannone G, Caraceni P. Albumin administration in internal medicine: a journey between effectiveness and futility. Eur J Intern Med. 2023;117:28–37. doi:10.1016/j.ejim.2023.07.003
4. Wiedermann CJ. Moderator effect of hypoalbuminemia in volume resuscitation and plasma expansion with intravenous albumin solution. Int J Mol Sci. 2022;23(22):14175. doi:10.3390/ijms232214175
5. Padkins M, Breen T, Anavekar N, Barsness G, Kashani K, Jentzer JC. Association between albumin level and mortality among cardiac intensive care unit patients. J Intensive Care Med. 2021;36(12):1475–1482. doi:10.1177/0885066620963875
6. Ari HF, Turanli EE, Yavuz S, et al. Association between serum albumin levels at admission and clinical outcomes in pediatric intensive care units: a multi-center study. BMC Pediatric. 2024;24(1):844. doi:10.1186/s12887-024-05331-8
7. Li ZQ, Liu XX, Wang XF, et al. Synergistic impact of plasma albumin and cognitive function on all-cause mortality in Chinese older adults: a prospective cohort study. Front Nutr. 2024;11:1410196. doi:10.3389/fnut.2024.1410196
8. Soeters PB, Wolfe RR, Shenkin A. Hypoalbuminemia: pathogenesis and clinical significance. JPEN J Parenter Enteral Nutr. 2019;43(2):181–193. doi:10.1002/jpen.1451
9. Doern GV, Carroll KC, Diekema DJ, et al. Practical guidance for clinical microbiology laboratories: a comprehensive update on the problem of blood culture contamination and a discussion of methods for addressing the problem. Clin Microbiol Rev. 2019;33(1). doi:10.1128/CMR.00009-19
10. Di Masi A, Leboffe L, Polticelli F, et al. Human serum albumin is an essential component of the host defense mechanism against clostridium difficile intoxication. J Infect Dis. 2018;218(9):1424–1435. doi:10.1093/infdis/jiy338
11. Austermeier S, Pekmezović M, Porschitz P, et al. Albumin neutralizes hydrophobic toxins and modulates candida albicans pathogenicity. mBio. 2021;12(3):e0053121. doi:10.1128/mBio.00531-21
12. Rombauts A, Abelenda-Alonso G, Simonetti AF, et al. Effect of albumin administration on outcomes in hypoalbuminemic patients hospitalized with community-acquired pneumonia (ALBUCAP): a prospective, randomized, Phase III clinical controlled trial-a trial protocol. Trials. 2020;21(1):727. doi:10.1186/s13063-020-04627-1
13. Povoa P, Coelho L, Dal-Pizzol F, et al. How to use biomarkers of infection or sepsis at the bedside: guide to clinicians. Intensive Care Med. 2023;49(2):142–153. doi:10.1007/s00134-022-06956-y
14. Cusack RAF, Rodriguez A, Cantan B, et al. Microcirculation properties of 20 % albumin in sepsis; a randomised controlled trial. J Crit Care. 2025;87:155039. doi:10.1016/j.jcrc.2025.155039
15. Fajgenbaum DC, June CH. Cytokine Storm. New Engl J Med. 2020;383(23):2255–2273. doi:10.1056/NEJMra2026131
16. Gradel KO, Vinholt PJ, Magnussen B, et al. Hypoalbuminaemia as a marker of trans-capillary leakage in community-acquired bacteraemia patients. Epidemiol Infect. 2018;146(5):648–655. doi:10.1017/S0950268818000274
17. Omiya K, Sato H, Sato T, et al. Albumin and fibrinogen kinetics in sepsis: a prospective observational study. Critical Care. 2021;25(1):436. doi:10.1186/s13054-021-03860-7
18. Ahmad M, Aduru SV, Smith RP, Zhao Z, Lopatkin AJ. The role of bacterial metabolism in antimicrobial resistance. Nat Rev Microbiol. 2025;23(7):439–454. doi:10.1038/s41579-025-01155-0
19. Gatta A, Verardo A, Bolognesi M. Hypoalbuminemia. Int Emerg Med. 2012;7(Suppl 3):S193–199. doi:10.1007/s11739-012-0802-0
20. Kim S, McClave SA, Martindale RG, Miller KR, Hurt RT. Hypoalbuminemia and clinical outcomes: what is the mechanism behind the relationship? Am Surg. 2017;83(11):1220–1227. doi:10.1177/000313481708301123
21. Castro R, Khanna AK, Schreiber M, Bakker J. Endothelial dysfunction in critically ill patients with sepsis and COVID-19 using the albumin transudation rate: a pilot study. J Crit Care. 2025;91:155237. doi:10.1016/j.jcrc.2025.155237
22. Wang M, Feng J, Zhou D, Wang J. Bacterial lipopolysaccharide-induced endothelial activation and dysfunction: a new predictive and therapeutic paradigm for sepsis. Eur. J. Med. Res. 2023;28(1):339. doi:10.1186/s40001-023-01301-5
23. Zhang L, Deng T, Zeng G, Chen X, Wu D. The association of serum albumin with 28 day mortality in critically ill patients undergoing dialysis: a secondary analysis based on the eICU collaborative research database. Eur. J. Med. Res. 2024;29(1):530. doi:10.1186/s40001-024-02127-5
24. Nelson JJ, Liao D, Sharrett AR, et al. Serum albumin level as a predictor of incident coronary heart disease: the atherosclerosis risk in communities (ARIC) study. Am J Epidemiol. 2000;151(5):468–477. doi:10.1093/oxfordjournals.aje.a010232
25. Wiedermann CJ. Hypoalbuminemia as surrogate and culprit of infections. Int J Mol Sci. 2021;22(9):4496. doi:10.3390/ijms22094496
26. Li J, Ding J, Chen L, et al. Epidemiological and clinical characteristics of three family clusters of COVID-19 transmitted by latent patients in China. Epidemiol Infect. 2020;148:e137.
27. China L, Freemantle N, Forrest E, et al. A randomized trial of albumin infusions in hospitalized patients with cirrhosis. New Engl J Med. 2021;384(9):808–817. doi:10.1056/NEJMoa2022166
28. Austin PC. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm Stat. 2011;10(2):150–161. doi:10.1002/pst.433
29. Austin PC. The use of propensity score methods with survival or time-to-event outcomes: reporting measures of effect similar to those used in randomized experiments. Stat Med. 2014;33(7):1242–1258. doi:10.1002/sim.5984
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Decrease in Hb and Hypoproteinemia: Possible Predictors of Complications in Neonates with Late-Onset Sepsis in a Developing Country
Cai N, Liao W, Chen Z, Tao M, Chen S
International Journal of General Medicine 2022, 15:6583-6589
Published Date: 13 August 2022