Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Parkinson’s Disease and Subjective Prospects for the Future in Different Life Domains. Findings of a Nationally Representative Sample
Authors Hajek A ![]() , Grupp K, Aarabi G, Kretzler B, König HH
, Grupp K, Aarabi G, Kretzler B, König HH ![]()
Received 11 April 2023
Accepted for publication 25 July 2023
Published 16 August 2023 Volume 2023:19 Pages 1791—1798
DOI https://doi.org/10.2147/NDT.S412366
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Roger Pinder
André Hajek,1 Katharina Grupp,2 Ghazal Aarabi,3 Benedikt Kretzler,1 Hans-Helmut König1
1Department of Health Economics and Health Services Research, University Medical-Center Hamburg-Eppendorf, Hamburg, Germany; 2Division of Plastic, Reconstructive and Aesthetic Surgery, University Medical Center Hamburg-Eppendorf, Hamburg, Germany; 3Department of Periodontics, Preventive and Restorative Dentistry, Center for Dental and Oral Medicine, University Medical Center Hamburg Eppendorf, Hamburg, Germany
Correspondence: André Hajek, Department of Health Economics and Health Services Research, University Medical-Center Hamburg-Eppendorf, Martinistr. 52, Hamburg, 20246, Germany, Tel +49 40 7410 52877, Fax +49 40 7410 40261, Email [email protected]
Purpose: To analyze the link between Parkinson’s disease and perceived prospects for the future.
Patients and Methods: Data were taken from the German Ageing Survey (year 2021; n=4296 individuals, thereof 33 individuals with Parkinson’s disease) were used. This is a nationally representative sample of community-dwelling individuals ≥ 40 years in Germany. Perceived prospects for the future in different life domains (ie, living standard, health and general optimism) were used as outcomes. Physician-diagnosed Parkinson’s disease served as key independent variable . It was adjusted for several covariates.
Results: Individuals with Parkinson’s disease had a markedly worse (Cohen’s d=0.65) general optimism compared to individuals without Parkinson’s disease. After adjusting for various factors, these differences disappeared in multiple linear regressions (β=− 0.04, p=0.72). Moreover, multiple ordered logistic regressions showed that individuals with Parkinson’s disease had a worse future self-rated health (OR: 4.10, 95% CI: 1.99– 8.47, p< 0.001) compared to individuals without Parkinson’s disease.
Conclusion: Our study first showed that general optimism may be lower among individuals with Parkinson’s disease (bivariate analysis). However, this association disappeared when it was adjusted for health-related factors in regression analysis. In sum, our findings indicate that more general future-related factors did not significantly differ between individuals with and without Parkinson’s disease. However, there were significant differences in future self-rated health.
Keywords: perceived longevity, outlook, optimism, health, living standard, Parkinson, Parkinson’s disease
Introduction
Parkinson’s disease is a progressive neurodegenerative disorder which is mainly characterized by, among other things, multisystem involvement and non-motor symptoms (eg, sleep disorder, constipation or hyposmia).1 As also outlined by Schapira et al1
The diagnosis of PD is currently dependent on the presence of motor deficits including bradykinesia, rigidity and tremor, usually manifesting unilaterally or at least asymmetrically. (p. 435)
A lot of studies have shown that Parkinson’s disease is associated with worse physical functioning2 or depressive symptoms3 – or more generally with lower health-related quality of life.4 However, only very few studies examined less clinically-oriented outcomes such as general optimism or life satisfaction. For example, a former longitudinal study showed that the incidence of Parkinson’s disease can lead to lower satisfaction with life.5 Moreover, another recent study6 reported a strong bivariate association between Parkinson’s disease and lower general optimism which, however, vanished in multiple linear regression analysis, after adjusting for various covariates.
Due to the limited knowledge, particularly related to perceived prospects for the future in different life domains, our aim was to examine the association between Parkinson’s disease and the aforementioned perceived prospects for the future in different life domains – based on nationally representative data of middle-aged and older community-dwelling adults. Such knowledge may help to underline the relevance of Parkinson’s disease for future-oriented psychological outcomes. Such outcomes are of great importance. We assume that outcomes such as poor future self-rated health may also (at least partly) reflect a potential powerlessness in the face of Parkinson’s disease. Moreover, we assume that individuals may therefore feel helpless and may think that Parkinson’s disease is progressing inevitably, regardless of their behavior regarding the disease. This may lead to a self-fulfilling prophecy where individuals may develop bad lifestyle habits (eg, start smoking, increase alcohol intake or drug use or sedentary behavior) and ultimately bad health.7–10 Moreover, this is important because favorable lifestyle habits can have a positive impact on physical capacities among individuals with Parkinson’s disease.11 Moreover, we assume that adherence to treatment (ie, behavior of the person with medical or health advice) may also change among individuals with Parkinson’s disease when the future is perceived as hopeless and without prospects. For these reasons, we think that it is important to examine the associations of interest.
With regard to government restrictions during the time of data collection: In mid-March 2020, a series of nationwide actions were taken to address the spread of COVID-19 in Germany, which involved, among other things, temporarily shutting down schools. Subsequently, in mid-April 2020, certain limitations were eased, enabling schools to resume operations in May 2020. Nevertheless, as infection rates started to surge once more during the autumn of 2020, additional measures were enforced. Finally, in May 2021, specific restrictions were lifted to facilitate a phased transition towards resuming normal activities.
Materials and Methods
Sample
We employed data from wave 7 of the German Ageing Survey (DEAS, “Deutscher Alterssurvey”) – a representative sample of community-dwelling middle-aged and older adults in Germany. We have focused on the most recent data collection in order to get as up-to-date a picture as possible of the associations of interest. The German Ageing Survey is funded by the Federal Ministry for Family Affairs, Senior Citizens, Women and Youth (BMFSFJ). Fieldwork was done by the infas Institute for Applied Social Sciences from November 2020 to March 2021. A CAPI-per-phone survey (with accompanying written drop-off questionnaire for self-completion which included sensitive questions such as well-being) was used. The average interview duration was about 75 minutes in wave 7. The DEAS study covers main topics in later life such as labor force participation, retirement, media consumption, well-being, health or ageism.
In general, the DEAS study has a cohort-sequential design. However, a new baseline sample could not be introduced in the most recent wave because a survey under the conditions of the COVID-19 pandemic could not be conducted in a face-to-face interview and only address data, but no telephone numbers, were available for the baseline sample.
Thus, in wave 7, the sample was based on all participants of the baseline samples 1996 to 2014 who were still available and who were willing to participate in the panel. The gross sample equaled 8379 individuals. In total, valid interviews were available for 5402 individuals aged 46 to 100. Moreover, about 82% (4419 individuals) of the participants filled out the additional written drop-off questionnaire. Due to a few missing values, the analytical sample equaled n=4296 individuals.
In wave 7, the response rate equaled approximately 65%. One main reason for non-participation was the fundamental refusal to take part, and thus the accompanying withdrawal of willingness to participate in the panel. The probability of participation was positively associated with younger age, higher educational level and good health status, whereas it was mostly not associated with income category, marital status, living situation or community size.12 Klaus et al13 gave further details about the DEAS study.
Before the interview, each participant signed a formal waiver of informed consent. An ethical statement was not required because the criteria for such a statement were not met (eg, examination of patients, risk to respondents, lack of information about the aims of the study, or use of invasive methods). This is in accordance with the guidelines of the German Research Foundation. The DEAS study is organized by the German Center for Gerontology (DZA), which decided that an ethical statement was not needed. The DEAS study has a standing advisory board that received detailed information about the sampling procedure, consent to participate, and instruments used in the DEAS study before each wave of data collection. This standing advisory board concluded that the DEAS study does not require approval by an ethics committee. The procedure described is in accordance with local guidelines. The study also follows the recommendations of the Declaration of Helsinki on Ethical Principles.
Dependent Variables
Different future-related outcomes were used: standard of living in the future, health prospects for the future and general optimism.
To quantify the living standard in the future, individuals were asked: “And if you think about the future, how do you expect your standard of living to change in the future?” [“will improve greatly”; “will improve somewhat”; “will remain the same”; “will worsen somewhat”; “will get much worse”].
To quantify health prospects for the future, individuals were asked: “How often do you deal with the topic death and dying?” [never; seldom; sometimes; often; very often]. Additionally, individuals were asked: “How do you expect your state of health to change in the future?” [“will improve greatly”; “will improve somewhat”; “will remain the same”; “will worsen somewhat”; “will get much worse”]. Furthermore, individuals were asked: “What age do you think you will live to?” [years]. With regard to perceived longevity, we removed four (quite) implausible values (two times: expected longevity was lower than their actual current chronological age; two times: expected longevity was 200 years).
Lastly, general optimism was quantified using a tool developed by Brandtstädter and Wentura.14 This tool has five items (each ranging from 1 = strongly agree to 4 = strongly disagree). An example is: “I am looking forward to the life ahead of me”. Four items were recoded. Subsequently, a final score was built by averaging the items. The final score ranges from 1 to 4 with higher values corresponding to higher optimism.
Key Independent Variable: Parkinson’s Disease
From a list of various chronic conditions, individuals were asked to identify which chronic conditions they had been formally diagnosed with by their doctor. One of these chronic conditions was Parkinson’s disease (no; yes). This item served as key independent variable. Such an assessment was also used in former studies5,6 and is a common way of quantifying Parkinson’s disease in large cohort studies such as the Survey of Health, Ageing, Retirement in Europe (SHARE) – or the DEAS study. It should be noted that the age of diagnosis and the severity of Parkinson’s disease was not quantified in the DEAS study (please see the limitations section for further details).
Covariates
Following prior research and based on theoretical considerations,15,16 several covariates were included in regression analysis: With regard to sociodemographic factors, age, sex (men; women), marital situation (married, living together with spouse; married, living separated from spouse; divorced; widowed; single), and educational level (which distinguished between low (0–2), medium (3–4), and high (5–6) education according to the ISCED-classification17) were included. With regard to lifestyle factors, we included: Current smoker status (daily; sometimes; not anymore; never been smoker), frequency of sports activities and alcohol intake (in both cases: six categories from daily to never).
With regard to health-related covariates, we included: Self-rated health (single item, from 1 (very good) to 5 (very bad)), physical functioning (SF-36 subscale “physical functioning”, ranging from 0 (worst) to 100 (best)),18 depressive symptoms (Center for Epidemiologic Studies Depression Scale;19 15-item version, ranging from 0 (no depressive symptoms) to 45 (severe depressive symptoms)) and a sum score for chronic conditions (0 to 11 chronic conditions; for example: cardiac and circulatory disorders, cancer or diabetes).
Statistical Analysis
For our analytical sample, sample characteristics stratified by Parkinson’s disease (ie, absence or presence of Parkinson’s disease) are shown. The effect sizes between Parkinson’s disease and the outcomes (Cramer’s V or Cohen’s d, as appropriate) are also given. Then, we conducted ordered logistic or linear regressions (as appropriate) to examine the association between Parkinson’s disease and the outcomes. A full-information maximum likelihood (FIML) approach was used to address missing values in sensitivity analyses for linear regressions.20 For example, when general optimism served as outcome measure, the average variance inflation factor (VIF) was 2.21, with most VIFs being very low. This suggests that multicollinearity is not a threat. To deal with serial correlation, cluster-robust standard errors were calculated.
P<0.05 was used to define the statistical significance level. The analyses were done with Stata 16.1 (StataCorp, College Station, TX, USA).
Results
Sample Characteristics and Bivariate Analysis
Sample characteristics for our analytical sample (additionally stratified by Parkinson’s disease) are shown in Table 1. In the total sample, average age was 68.8 years (SD: 10.2 years), ranging from 46 to 98 years. About 51% of the individuals were female and about 78% of the individuals thought that the living standard will remain the same in the future. Moreover, 48% of the individuals “somewhat” dealt with death and dying, and 60% of the individuals thought that their future self-rated health will remain the same. The average perceived longevity equaled 85.5 years (SD: 7.3) and average general optimism was 3.0 (SD: 0.6).
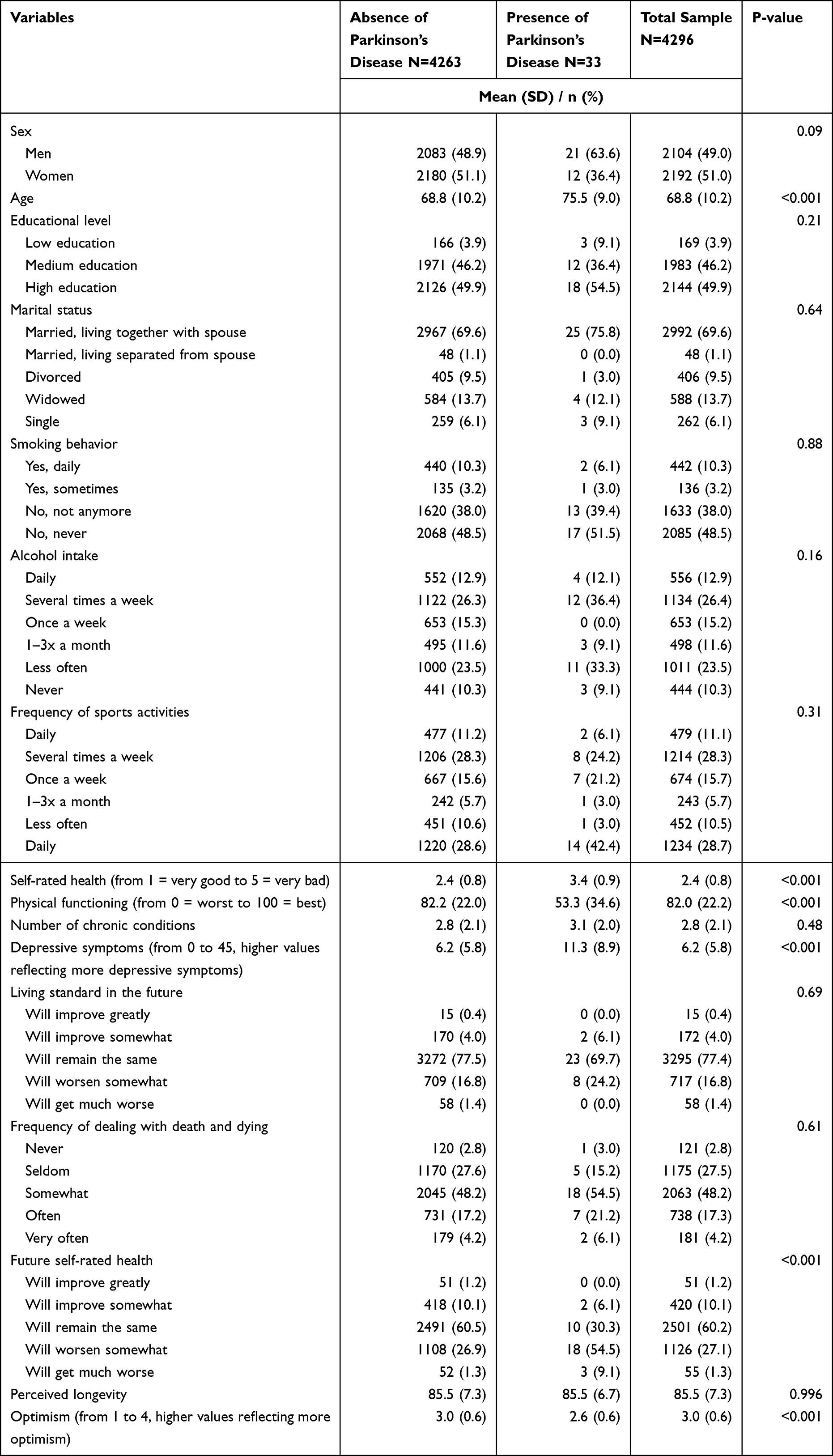 |
Table 1 Sample Characteristics |
Parkinson’s disease was significantly associated with age, self-rated health, physical functioning, depressive symptoms, future self-rated health and general optimism (with the expected signs). Further details are shown in Table 1.
Cohen’s d for the association between Parkinson’s disease and general optimism equaled 0.65. Moreover, Cohen’s d for the association between Parkinson’s disease and perceived longevity equaled −0.07.
We also calculated Cramer’s V (link between Parkinson’s disease and standard of living in the future). It was 0.02. Furthermore, Cramer’s V for the association between Parkinson’s disease and future self-rated health was 0.10. Moreover, Cramer’s V for the association between Parkinson’s disease and frequency of dealing with death and dying was 0.02.
Regression Analysis
Findings of regression analyses are shown in Table 2. It was adjusted for sex, age, family status, education, smoking behavior, alcohol intake, physical activity, depressive symptoms, physical functioning, self-rated health, and chronic diseases in all regressions (a full model displaying all covariates is shown in Supplementary Table 1).
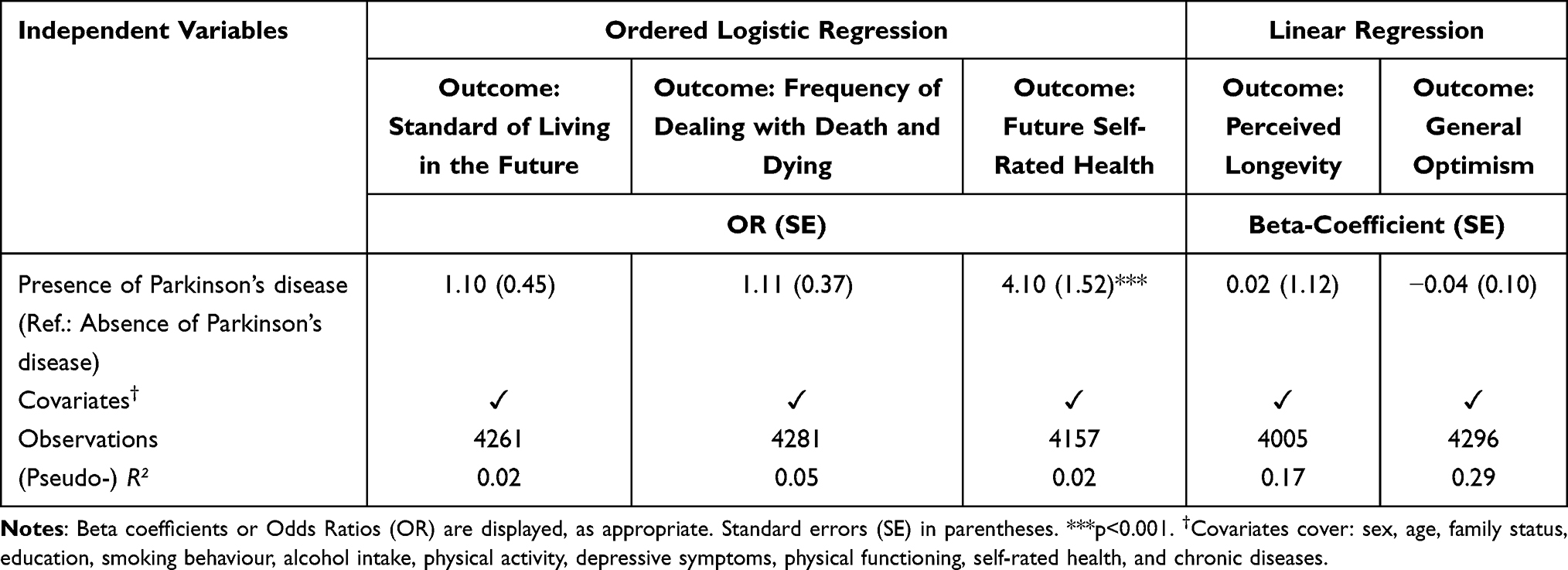 |
Table 2 Parkinson’s Disease and Perceived Prospects for the Future in Different Life Domains. Findings of Multiple Linear and Ordered Logistic Regressions (as Appropriate) |
Multiple ordered logistic regressions showed that individuals with Parkinson’s disease had a worse future self-rated health (OR: 4.10, 95% CI: 1.99–8.47, p<0.001) compared to individuals without Parkinson’s disease. However, the presence of Parkinson’s disease was not significantly associated with the other outcomes after adjusting for covariates.
Our robustness checks with FIML (in case of linear regressions) to address missing data also showed that the presence of Parkinson’s disease is neither significantly associated with perceived longevity (β=0.66, p=0.59) nor with general optimism (β=0.03, p=0.79).
Moreover, in another robustness check, physical functioning was removed as a covariate because Parkinson’s disease manifests itself primarily through a loss of function. However, compared with our main results presented in Table 2, our results remained nearly the same (ie, only the association with future self-rated health was significant: OR: 3.96, 95% CI: 1.95–8.05, p<0.001).
Discussion
The objective was to analyze the association between Parkinson’s disease and perceived prospects for the future in different life domains. In bivariate analysis, particularly individuals with Parkinson’s disease had a markedly lower general optimism compared to individuals without Parkinson’s disease. After adjusting for sociodemographic, lifestyle- and health-related factors, these differences disappeared in multiple linear regressions. Moreover, multiple ordered logistic regressions showed that individuals with Parkinson’s disease had a worse future self-rated health compared to individuals without Parkinson’s disease. Our findings are difficult to compare with previous studies due to the lack of studies examining the association between Parkinson’s disease and perceived prospects for the future in different life domains. Thus, our study adds very first evidence in this research field and may serve as a basis for upcoming studies.
At first glance, it was surprising to see that Parkinson’s disease was not significantly associated with four out of five outcomes. It seems that community-dwelling individuals having Parkinson’s disease are not generally pessimistic (general and in terms of perceived longevity, thoughts about death and in terms of living standard) about their future life. Particularly the perception of the standard of living in the future may partly reflect confidence in the German long-term care insurance. As discussed in a recent study,6 the general optimism of individuals with Parkinson’s disease may reflect a general trust in the treatment of Parkinson’s disease. Furthermore, they may have developed strong coping skills to face their diagnosis of Parkinson’s disease.21 These factors may also explain why individuals with Parkinson’s disease had no significant differences in the outcomes “frequency of dealing with death and dying” and general “perceived longevity” - compared to individuals without Parkinson’s disease. Other possible explanations for the aforementioned results may be the wide array of (health-related) covariates included and the potential lack of statistical power – which clearly highlights the need for upcoming research in this field using data from very large, representative samples.
In contrast, individuals with Parkinson’s disease reported a worse future self-rated health compared to individuals without Parkinson’s disease. Looking at the other results (and their possible explanations), this may sound contradictory at first. However, future self-rated health may more strongly reflect emerging functional limitations – or factors such as the perception of low mental energy, tremor or feeling dependent on others in the future (compared with the older general population without Parkinson’s disease). A former qualitative study also showed that individuals with Parkinson’s disease often fear further losses of functioning.21
With regard to strengths and limitations of our current study: Data were taken from a large, population-based sample. For example, a valid tool was used to quantify general optimism – and the other outcomes had a high face validity. Various covariates was included in regression analysis and FIML was used in sensitivity analysis (in case of linear regressions). However, we cannot rule out the possibility that other factors may affect the outcomes (such as other family-related factors). Moreover, it should be noted that our study was limited to community-dwelling individuals (which may explain the small number of individuals with Parkinson’s disease). It may be the case that the effect sizes are more pronounced among individuals living in institutionalized settings. Future research in this area is therefore needed. Additionally, the actual severity of the disease and the time of diagnosis remain unknown. If data are available in future studies, these factors should be incorporated in upcoming studies. Lastly, some sample selection bias of the DEAS study in general should be taken into consideration.13 For example, it may be the case, that individuals scoring lower in optimism may have a higher likelihood of non-participation.
Individuals were asked if they had received a formal diagnosis of Parkinson’s disease from their doctor. This was not additionally backed up by an official diagnosis on the part of the doctors. In this respect, we cannot completely exclude the possibility that the information provided by the participants is incorrect. However, we assume that the participants can correctly remember an official diagnosis by the doctors and also state this as such. Additionally, factors which may be important for Parkinson’s disease such as anxiety symptoms or dementia were not quantified in the DEAS study.
Conclusion and Future Research
In conclusion, our study first showed that particularly general optimism may be markedly lower among individuals with Parkinson’s disease (bivariate analysis). However, this association disappeared when it was adjusted for health-related factors in regression analysis. In sum, our findings indicate that more general future-related factors did not significantly differ between individuals with and without Parkinson’s disease. However, there were significant differences in future self-rated health between individuals with and without Parkinson’s disease.
With regard to future research: Exploring this association in different countries could yield intriguing results and shed light on how geographical location and the availability of health facilities in different settings affect outcomes. For example, a comparison between the UK and the US, for example, where access to healthcare is very different, would also provide potentially valuable insights.
Funding
We acknowledge financial support from the Open Access Publication Fund of UKE - Universitätsklinikum Hamburg-Eppendorf and DFG – German Research Foundation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Schapira AH, Chaudhuri KR, Jenner P. Non-motor features of Parkinson disease. Nat Rev Neurosci. 2017;18(7):435–450. doi:10.1038/nrn.2017.62
2. Dural A, Atay M, Akbostanci C, et al. Impairment, disability, and life satisfaction in Parkinson’s disease. Disabil Rehabil. 2003;25(7):318–323. doi:10.1080/0963828021000043761
3. Cong S, Xiang C, Zhang S, et al. Prevalence and clinical aspects of depression in Parkinson’s disease: a systematic review and meta‑analysis of 129 studies. Neurosci Biobehav Rev. 2022;141:104749. doi:10.1016/j.neubiorev.2022.104749
4. Zhao N, Yang Y, Zhang L, et al. Quality of life in Parkinson’s disease: a systematic review and meta-analysis of comparative studies. CNS Neurosci Ther. 2021;27(3):270–279. doi:10.1111/cns.13549
5. Buczak-Stec EW, König -H-H, Hajek A. Impact of incident Parkinson’s disease on satisfaction with life. Front Neurol. 2018;9:589. doi:10.3389/fneur.2018.00589
6. Vardanyan R, König HH, Hajek A. Association between Parkinson’s disease and psychosocial factors: results of the nationally representative German ageing survey. J Clin Med. 2022;11(15):4569. doi:10.3390/jcm11154569
7. Rappange DR, Brouwer WB, van Exel J. A long life in good health: subjective expectations regarding length and future health-related quality of life. Eur J Health Econ. 2016;17:577–589. doi:10.1007/s10198-015-0701-1
8. Palgi Y, Shrira A, Ben-Ezra M, et al. Age-related and death-related differences in emotional complexity. Psychol Aging. 2014;29(2):284. doi:10.1037/a0036302
9. Keyes CL, Westerhof GJ. Chronological and subjective age differences in flourishing mental health and major depressive episode. Aging Ment Health. 2012;16(1):67–74. doi:10.1080/13607863.2011.596811
10. Griffin B, Loh V, Hesketh B. A mental model of factors associated with subjective life expectancy. Soc Sci Med. 2013;82:79–86. doi:10.1016/j.socscimed.2013.01.026
11. Lauzé M, Daneault J-F, Duval C. The effects of physical activity in Parkinson’s disease: a review. J Parkinsons Dis. 2016;6(4):685–698. doi:10.3233/JPD-160790
12. Schiel S, Marcos JR, Schulz S, et al. Methodenbericht. Deutscher Alterssurvey (DEAS): Durchführung der 7. Erhebungswelle 2020/2021. Bonn: Infas; 2021.
13. Klaus D, Engstler H, Mahne K, et al. Cohort profile: the German ageing survey (DEAS). Int J Epidemiol. 2017;46(4):1105–1105g. doi:10.1093/ije/dyw326
14. Brandtstädter J, Wentura D. Veränderungen der Zeit- und Zukunftsperspektive im Übergang zum höheren Erwachsenenalter: entwicklungspsychologische und differentielle Aspekte. [Changes in time perspectives and attitudes toward the future during the transition to later adulthood: developmental psychology and differential aspects]. Zeitschrift für Entwicklungspsychologie und Pädagogische Psychologie. 1994;26:2–21. German.
15. Hajek A, Buczak-Stec E, König HH. Do sexually satisfied individuals think that they live longer? Results from the German Ageing Survey Healthcare. 2022;10(12):2482.
16. Hajek A, König HH. Do lonely and socially isolated individuals think they die earlier? The link between loneliness, social isolation and expectations of longevity based on a nationally representative sample. Psychogeriatrics. 2021;21(4):571–576. doi:10.1111/psyg.12707
17. UNESCO. International Standard Classification of Education. ISCED 1997.
18. Ware JJ, Sherbourne C. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30(6):473–483. doi:10.1097/00005650-199206000-00002
19. Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1(3):385–401. doi:10.1177/014662167700100306
20. Enders CK. The performance of the full information maximum likelihood estimator in multiple regression models with missing data. Educ Psychol Meas. 2001;61(5):713–740. doi:10.1177/0013164401615001
21. Charlton GS, Barrow CJ. Coping and self-help group membership in Parkinson’s disease: an exploratory qualitative study. Health Soc Care Community. 2002;10(6):472–478. doi:10.1046/j.1365-2524.2002.00385.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.