Back to Journals » Journal of Pain Research » Volume 18
Pain Knowledge, Attitudes, and Beliefs Among Final-Year Physiotherapy and Occupational Therapy Students in Jordan: A Cross-Sectional Study
Authors Muhsen A ![]() , Madi M
, Madi M ![]() , Wshah A
, Wshah A ![]() , Obaidat SM, Bin Sheeha B
, Obaidat SM, Bin Sheeha B ![]() , Shallan A
, Shallan A ![]() , Yabroudi MA, Altubasi I
, Yabroudi MA, Altubasi I ![]() , Altaim TA
, Altaim TA ![]()
Received 19 September 2025
Accepted for publication 16 November 2025
Published 22 November 2025 Volume 2025:18 Pages 6243—6257
DOI https://doi.org/10.2147/JPR.S565885
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ryan D'Souza
Ahmad Muhsen,1 Mohammad Madi,1 Adnan Wshah,1 Sakher M Obaidat,1 Bodor Bin Sheeha,2 Amjad Shallan,1 Mohammad A Yabroudi,3 Ibrahim Altubasi,4 Thamer A Altaim1
1Department of Physical Therapy, Faculty of Applied Medical Sciences, The Hashemite University, Zarqa, Jordan; 2Department of Rehabilitation Sciences, College of Health and Rehabilitation Sciences, Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia; 3Department of Rehabilitation Sciences, Faculty of Applied Medical Sciences, Jordan University of Science and Technology, Irbid, Jordan; 4Department of Physiotherapy, School of Rehabilitation Sciences, The University of Jordan, Amman, Jordan
Correspondence: Ahmad Muhsen, Department of Physical Therapy, Faculty of Applied Medical Sciences, The Hashemite University, P.O. Box 330127, Zarqa, 13133, Jordan, Tel +962 5 3903333, Ext: 5550, Fax +962 5 3903368, Email [email protected]
Background: Despite the global burden of chronic pain, gaps in pain education persist in healthcare programs. This study evaluated pain knowledge, attitudes, and beliefs among final-year physiotherapy (PT) and occupational therapy (OT) students in Jordan, compared these competencies between disciplines, examined the relationship between pain knowledge and beliefs, and explored significant predictors of pain knowledge.
Methods: A descriptive, cross-sectional study was conducted using an online survey of final-year PT and OT students from three public universities in Jordan. Pain knowledge was assessed using the Revised Neurophysiology of Pain Questionnaire (RNPQ), and attitudes and beliefs toward pain and disability were measured with the modified Health Care Providers’ Pain and Impairment Relationship Scale (HC-PAIRS). Students also reported perceived sources of pain knowledge. Data analysis involved non-parametric tests for group comparisons, Spearman correlations to assess the RNPQ-HC-PAIRS association, and multiple linear regression to identify predictors of RNPQ scores.
Results: A total of 216 students completed the survey (PT: n=149; OT: n=67). PT students demonstrated higher RNPQ scores and lower HC-PAIRS scores than OT students (both p< 0.001), indicating a better understanding of pain neurophysiology and more adaptive pain beliefs. Across the total sample, RNPQ and HC-PAIRS scores were inversely correlated (ρ = – 0.334, p< 0.001). Regression analysis identified discipline (PT vs OT), endorsing university courses as a primary pain knowledge source, and HC-PAIRS scores as significant predictors of RNPQ scores (adjusted R2 = 0.855, p< 0.001). A significant interaction showed that PT students derived greater pain knowledge gains from university courses than OT students.
Conclusion: Final-year PT and OT students in Jordan exhibited limited pain knowledge and persistent biomedical beliefs, with PT students outperforming OT students. University courses were the strongest predictor of pain knowledge, underscoring the need for integrating evidence-based pain curricula with a biopsychosocial focus in both disciplines.
Plain Language Summary: Chronic pain is a common problem worldwide. Future health care providers such as physiotherapists and occupational therapists need to have a sound understanding of modern pain concepts to provide care to people with pain. A key point is that pain is affected by our body, mind, and surroundings, not just tissue injury.
In our study, we surveyed 216 physiotherapy and occupational therapy students in their final year of training in Jordan. We also assessed their pain knowledge and attitudes and beliefs when caring for people with chronic pain.
We found that physiotherapy students had better knowledge and more positive beliefs about pain than occupational therapy students. We also found that students who viewed their university courses as a main source of pain knowledge tended to have higher scores on pain knowledge assessment. This connection was strongest for physiotherapy students.
Our findings show a clear opportunity to better prepare future health professionals for modern pain care by updating pain education curricula, especially occupational therapy programs. Improving pain education now will eventually lead to more effective and empathetic care in future.
Keywords: pain neuroscience education, biopsychosocial model, curricular assessment, health professional students
Introduction
Pain is one of the most common reasons patients seek healthcare globally.1,2 When pain persists or recurs beyond 3 months, it is classified as chronic.3 Chronic pain represents a significant global burden, affecting between 20% and 50% of the world’s population,4,5 and is a leading cause of disability and reduced quality of life.6,7 Low back pain remains one of the top contributors to years lived with disability (YLDs) worldwide,8,9 with a significant proportion of cases progressing to chronicity through dynamic biopsychosocial mechanisms.10,11
This understanding has driven a global shift towards a biopsychosocial model of pain,12 integrating patient-centered, multidisciplinary, and psychosocially informed care.13,14 Nevertheless, biomedical beliefs and limited knowledge of modern pain science persist among health professionals15 and students.16 These biomedical beliefs may negatively influence clinical decisions, reduce adherence to evidence-based treatment guidelines, and reinforce maladaptive pain beliefs among patients, ultimately contributing to greater disability and poorer outcomes.17–19
In this setting, two interrelated competencies are essential: knowledge of pain neurophysiology and beliefs toward pain-related function and disability. Collectively, these factors influence clinical decisions and behaviors and may be modified through educational interventions, although their effect on clinical behaviors is unclear.19,20 Despite growing consensus on the need for standardized, evidence-based pain education, most undergraduate curricula remain misaligned with the International Association for the Study of Pain (IASP) guidelines.21,22 This gap impedes implementation of biopsychosocial care, and thus, demands targeted interventions.
Pain neuroscience education (PNE) has demonstrated efficacy in improving pain knowledge and modifying maladaptive beliefs among students, clinicians and patients.23–27 Integrating PNE within IASP-aligned undergraduate curricula and biopsychosocial frameworks may enhance students’ clinical competencies in contemporary pain management.28
While evidence is growing in high-income countries,20 limited data exist on pain knowledge and beliefs among physiotherapy (PT) and occupational therapy (OT) students in the Arab region. In Saudi Arabia, for example, a study identified a significant pain knowledge gap in PT programs, indicating a need for curriculum reform.16 Despite cultural and educational similarities with neighboring Arab countries, no comparable investigations into pain education have been conducted in Jordan. Furthermore, since 1999, three leading public Jordanian universities: The Hashemite University (HU), The University of Jordan (JU), and Jordan University of Science and Technology (JUST), have offered physiotherapy and occupational therapy programs, making this context particularly relevant.29
To our knowledge, no prior studies in Jordan have assessed pain knowledge and beliefs among final-year PT and OT students. Specifically, this study aimed to: (1) assess students’ pain neurophysiology knowledge and attitudes toward pain-related disability using validated questionnaires; (2) examine the relationship between pain knowledge and beliefs; and (3) evaluate whether a priori candidate predictors (demographic factors, pain-related beliefs, and agreement with educational sources) were associated with pain knowledge. By establishing baseline data on pain knowledge and beliefs, this study provides a benchmark to guide curriculum development, support the integration of evidence-based pain neuroscience education, and encourage alignment with IASP guidelines.
Materials and Methods
Study Design and Setting
This descriptive, cross-sectional study was conducted using an online survey between February and June 2023 to evaluate the knowledge of pain neurophysiology among final year physiotherapy (PT) and occupational (OT) students enrolled at three major public universities in Jordan.
Ethics
Ethical approval was granted by the Institutional Review Board of The Hashemite University (HU-IRB No. 29/9/2021/2022) prior to study commencement. This approval covered recruitment at the three participating universities; institutional acknowledgment and support were obtained at each site. The survey was conducted anonymously online, and electronic informed consent was obtained from all students before participation. Students were assured that their responses would remain confidential, would not affect their academic standing or grades, and that participation was entirely voluntary. All data were anonymized, and the study adhered to the principles of the Declaration of Helsinki.
Participants
All final year Bachelor of Science (BSc) pre-registration PT and OT students from three major public Jordanian Universities were invited to participate. Inclusion required (1) active enrollment in the final year of a PT or OT program and (2) the ability to provide informed consent. Exclusion criteria were: enrollment in earlier academic years, current internship or graduation status, or being on academic leave at the time of data collection. An invitation letter, including study key information and a secure, anonymous Google Forms survey link, was distributed via social media platforms (WhatsApp and Facebook groups). After completing the electronic informed consent, students proceeded to complete the online questionnaires, which required an estimated 15 minutes to complete.
For multiple linear regression with 12 candidate predictors, sample size guidelines recommend a minimum of N ≥ 116 to test the overall model R2 and N ≥ 146 to adequately estimate individual predictors.30 The final analyzed sample of N = 216 exceeded these thresholds, supporting the stability and adequacy of the regression analyses.
Questionnaires
The survey was administered in English, as this is the medium of instruction in PT and OT programs in Jordan. It comprised a brief demographic questionnaire (gender, age, university, and discipline) and three other questionnaires as follows:
The Revised Neurophysiology of Pain Questionnaire (RNPQ)
The Revised Neurophysiology of Pain Questionnaire (RNPQ) is a validated 12-item instrument used to assess pain neurophysiological knowledge.31 The RNPQ consists of 12 closed-ended questions (true, false, undecided). Scoring for the RNPQ follows a binary system, where only correct responses receive 1 point, while incorrect or undecided responses scored as 0. The maximum possible score for the RNPQ is 12, with higher scores reflecting better understanding of pain neurophysiology.
The RNPQ was developed from the original Neurophysiology of Pain Questionnaire (NPQ) by Moseley.32 The RNPQ demonstrates robust psychometric properties. It shows excellent test-retest reliability (ICC=0.97; 95% CI, 0.93–0.99) and good internal consistency (Cronbach’s α = 0.84).31 These features support the validity of the RNPQ for evaluating understanding of pain neurophysiology in health professional populations.
The 13‑Item Modified Health Care Providers Pain and Impairment Relationship Scale (HC‑PAIRS)
The modified Health Care Providers Pain and Impairment Relationship Scale (HC-PAIRS) was used to assess students’ attitudes and beliefs towards individuals with chronic pain and their ability to function despite pain.33 It has 13 items rated on a 7-point Likert scale (strongly disagree=1; strongly agree =7). Total scores range from 13 to 91, with lower scores indicating more positive attitudes towards patients with chronic pain. HC-PAIRS has shown strong psychometric properties, including excellent internal consistency (Cronbach’s α = 0.92) and good test–retest reliability (ICC=0.84; 95% CI, 0.78–0.89).34
Assessment of Pain Neurophysiology Knowledge Sources
To assess pain knowledge sources, a research team-developed tool was used, grounded in the pain education literature.16,35 Students were asked to rate their level of agreement with five statements using a 5-point Likert scale (1=Strongly Disagree, 5=Strongly Agree). Each statement started with: “The majority of my pain neurophysiology knowledge came from…” followed by one of the five source categories: university courses, clinical training, internet (eg, podcasts, YouTube), self-study (eg books, journals), and other (workshops, peer discussion, conference talk). Further, students were asked to identify one source they considered their main source of pain knowledge by selecting just one. These items were developed specifically for this study and reviewed internally for content relevance. However, they have not undergone formal psychometric validation.
Data Quality Control Procedures
Data were screened using prespecified quality-control procedures. Duplicates, identified by identical timestamps and response patterns, were removed. To identify low-quality responses, we implemented a multi-step protocol: questionnaires with >10% missing data were excluded; page-time tracking was used to flag responses with improbably short completion times (<5th percentile); and attention was assessed through both patterned responding (eg, invariant selections) and embedded attention-check items. Entries failing these quality criteria were excluded. Only complete, valid cases were retained for analysis.
Statistical Analysis
Data were analyzed using Stata/SE (version 17, StataCorp LLC). For all analyses, two-sided tests with p<0.05 were considered statistically significant. Continuous variables were evaluated for normality using Shapiro–Wilk tests and graphical review.
Descriptive statistics were based on frequency distributions and percentages for categorical data (gender, discipline (PT vs OT), university affiliation (HU, JU, JUST), and main source of pain knowledge) and means and standard deviations (SD) or medians and interquartile ranges (IQR) for continuous/non-normally distributed (age, RNPQ, HC-PAIRS) or ordinal variables (Likert-type agreement variables).
Between-group comparisons included χ2 and Fisher exact tests for categorical comparisons, and nonparametric tests (Mann–Whitney U, Kruskal–Wallis H) for non-normally distributed or ordinal outcomes. Effect sizes (r) were reported where applicable.
To assess the relationships between RNPQ and HC-PAIRS, Spearman’s rank correlation coefficients (ρ) were calculated for the total sample and stratified by discipline. The strength of the correlations was interpreted according to the guidelines defined by Mukaka:36
(negligible, 0.00 ≤ ρ< 0.30; low, 0.30 ≤ ρ < 0.50; moderate, 0.50 ≤ ρ < 0.70; high, 0.70 ≤ ρ < 0.90; very high, 0.90 ≤ ρ < 1.00).
To determine predictors of RNPQ, multiple linear regression was used with RNPQ as the dependent variable. Based on theoretical relevance and prior literature,16,35 the following predictors (independent variables) were included in the model: five 5-point Likert-type items reflecting perceived agreement with sources of knowledge (university courses, clinical training, internet, self-study, other), HC-PAIRS, demographic and institutional variables (age, gender, discipline, university affiliation). Categorical variables (gender, discipline, university) were dummy coded before modeling with the following reference groups: female (Gender), OT (Discipline), HU (University).
An initial model was fitted with all candidate predictors. A backward elimination approach was then applied to derive a parsimonious model while retaining theoretically meaningful variables. This was done by iteratively removing the independent variable with the largest p-value > 0.05. After identification of the final main effects model, an interaction term between discipline and agreement with university courses (discipline x university courses) was added to test for potential effect modification. Model fit was assessed using the coefficient of determination (R2)/adjusted R2, F-statistic and its corresponding p-value.
All regression models were estimated using Ordinary Least Squares (OLS) regression with HC3 heteroskedasticity-consistent (robust) standard errors (SEs). Coefficient tests used robust two-sided t statistics (coefficient/SE) with the model’s residual degrees of freedom. Regression assumptions (linearity, homoscedasticity, normality of residuals, and multicollinearity) were assessed via visual inspection of residual plots, normal Q–Q plots, and Variance Inflation Factors (VIFs) scores.
Results
There were 277 respondents from the 3 universities. Following data quality screening and removal of duplicate or incomplete entries, 216 complete questionnaires were retained and included in the analysis. This represents a 36% response rate from the eligible population (N=600), as reported by faculty collaborators affiliated with the participating universities. Characteristics of all participants are summarized in Table 1.
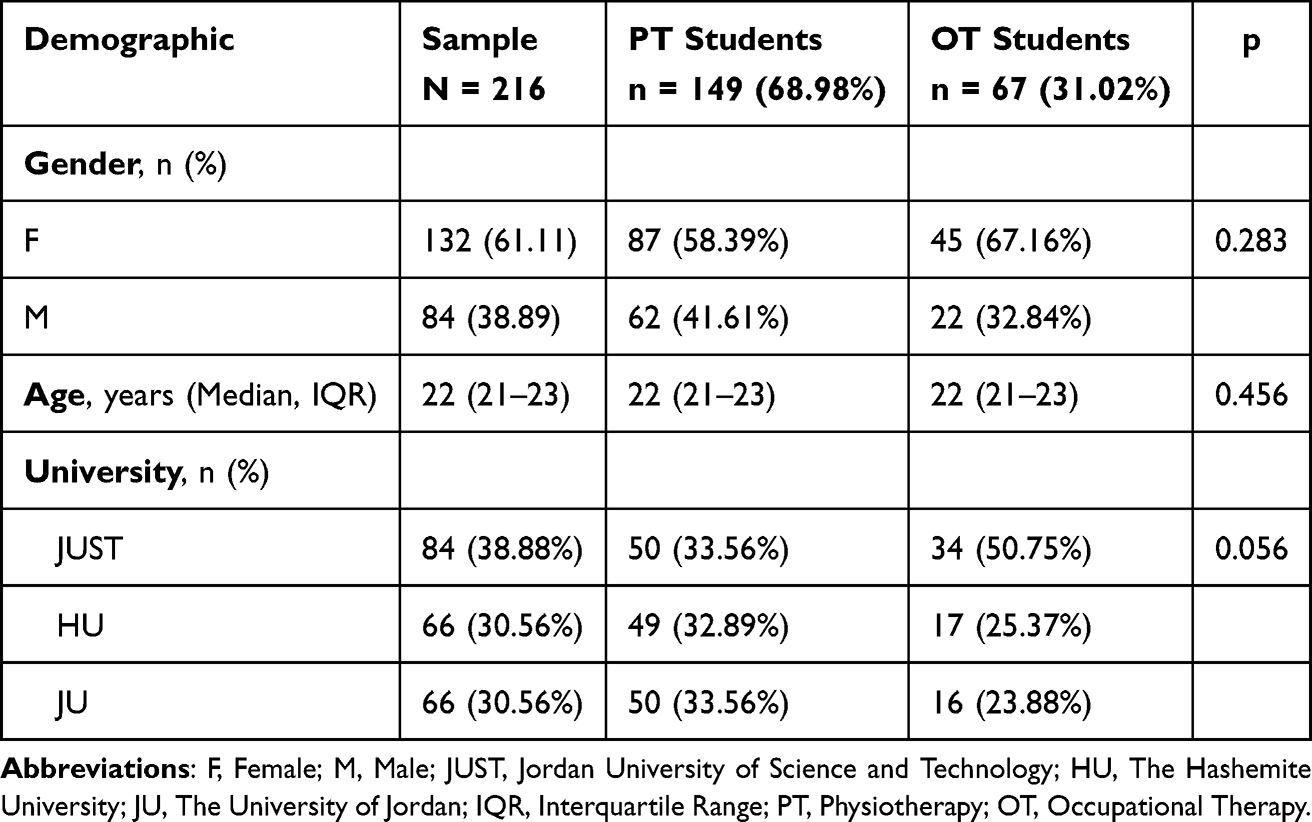 |
Table 1 Descriptive Characteristics of the Sample by Discipline |
Demographics
Final year PT students represented the majority of the sample (n=149, 68.98%). While the overall sample was dominated by females (n=132, 61.11%), there was no statistically significant difference in gender distribution between PT and OT students (p=0.283). Both student groups demonstrated no significant difference (p=0.456) in age, with median age of 22.0 years (IQR = 21.0–23.0) reported for the whole sample.
There was a relatively balanced university affiliation across the three institutions (HU, JU, JUST) for the overall sample (p=0.056). Although this result was not statistically significant, a higher proportion of OT students were from JUST (50.75%). However, PT students showed a more even distribution across the three universities (JUST: 33.56%, HU: 32.89%, JU: 33.56%).
As shown in Figure 1, PT and OT students identified similar distributions of main pain knowledge sources (p=0.898), with university courses (37.50%) being the most frequently reported source for the whole sample, followed by clinical training (23.61%) and the internet (15.14%). While both groups reported university courses as the predominant source of pain knowledge (PT: 39.60%, OT: 32.84%), they less frequently reported self-study and “other”.
 |
Figure 1 Main sources of pain neurophysiology knowledge (%) by discipline. Purple bars represent the whole sample, green bars represent physiotherapy (PT) students, and peach bars represent occupational therapy (OT) students. |
Between-Group Differences
There were significantly higher RNPQ scores reported for PT students (Median = 8.0, IQR = 7.0–8.0) compared to OT students (Median = 6.0, IQR = 6.0–7.0), with a large effect size (r)=0.66, p<0.001. In addition, HC-PAIRS scores were significantly lower for PT students (Median = 45.0, IQR = 38.0–52.0) than OT students (median=57.0, IQR=49.0–60.0), with a moderate effect size (r=0.42, p<0.001). This indicates more positive attitudes towards pain among PT students (Table 2).
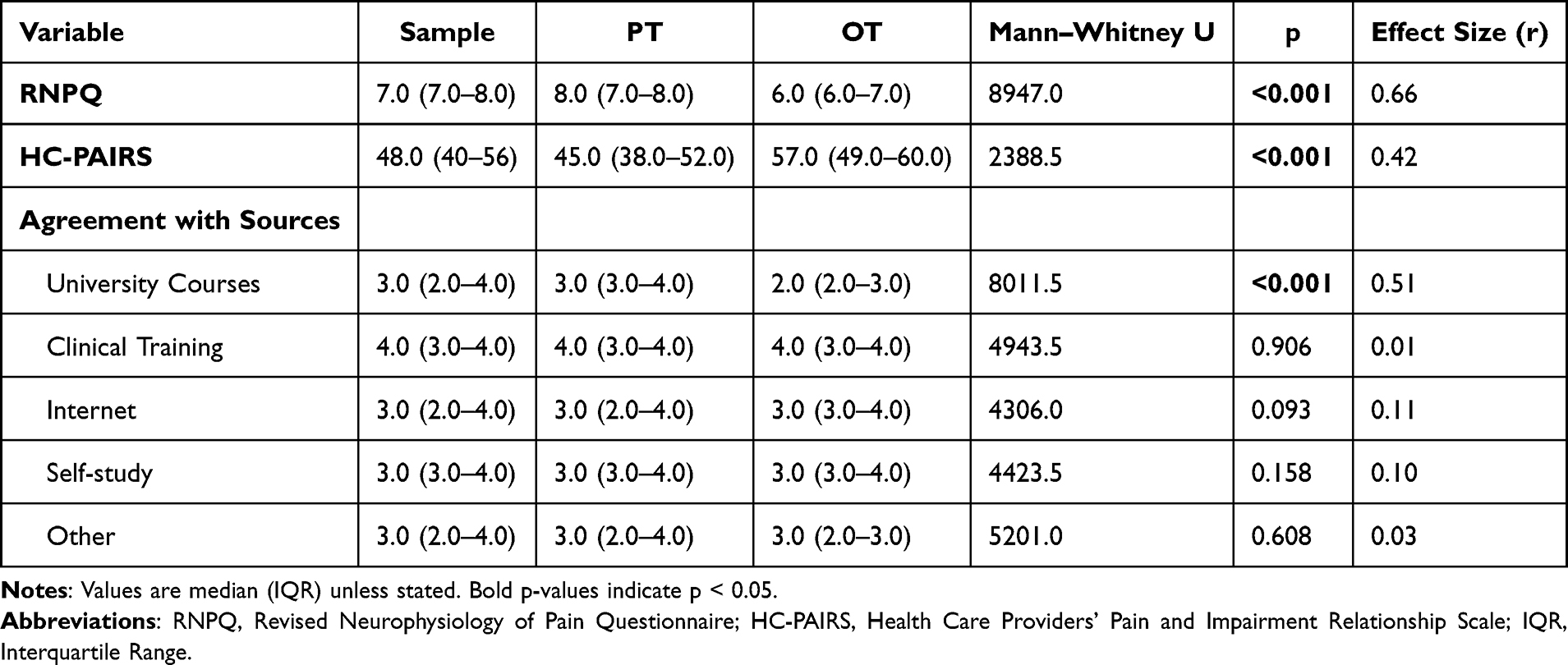 |
Table 2 Between-Group Comparison of RNPQ, HC-PAIRS, and Agreement with Pain Knowledge Sources |
Levels of agreement with different sources of pain knowledge are illustrated in Table 2. There was only a significant between-group difference found for university courses, where PT students showed higher agreement scores (Median = 3.0, IQR = 3.0–4.0), than OT students (Median = 2.0, IQR = 2.0–3.0), with a moderate effect size (r=0.51), p<0.001. No between-group differences in agreement level scores were reported with other sources of pain (p>0.05). These between-group differences are further reinforced in boxplots (Figure 2), where the most evident gap is shown for university courses (p<0.001) as opposed to all other sources across disciplines (p>0.05). There were no statistical differences between universities in RNPQ (p=0.516), HC-PAIRS (p=0.380), or agreement with different sources of pain knowledge (p>0.05) (Table 3).
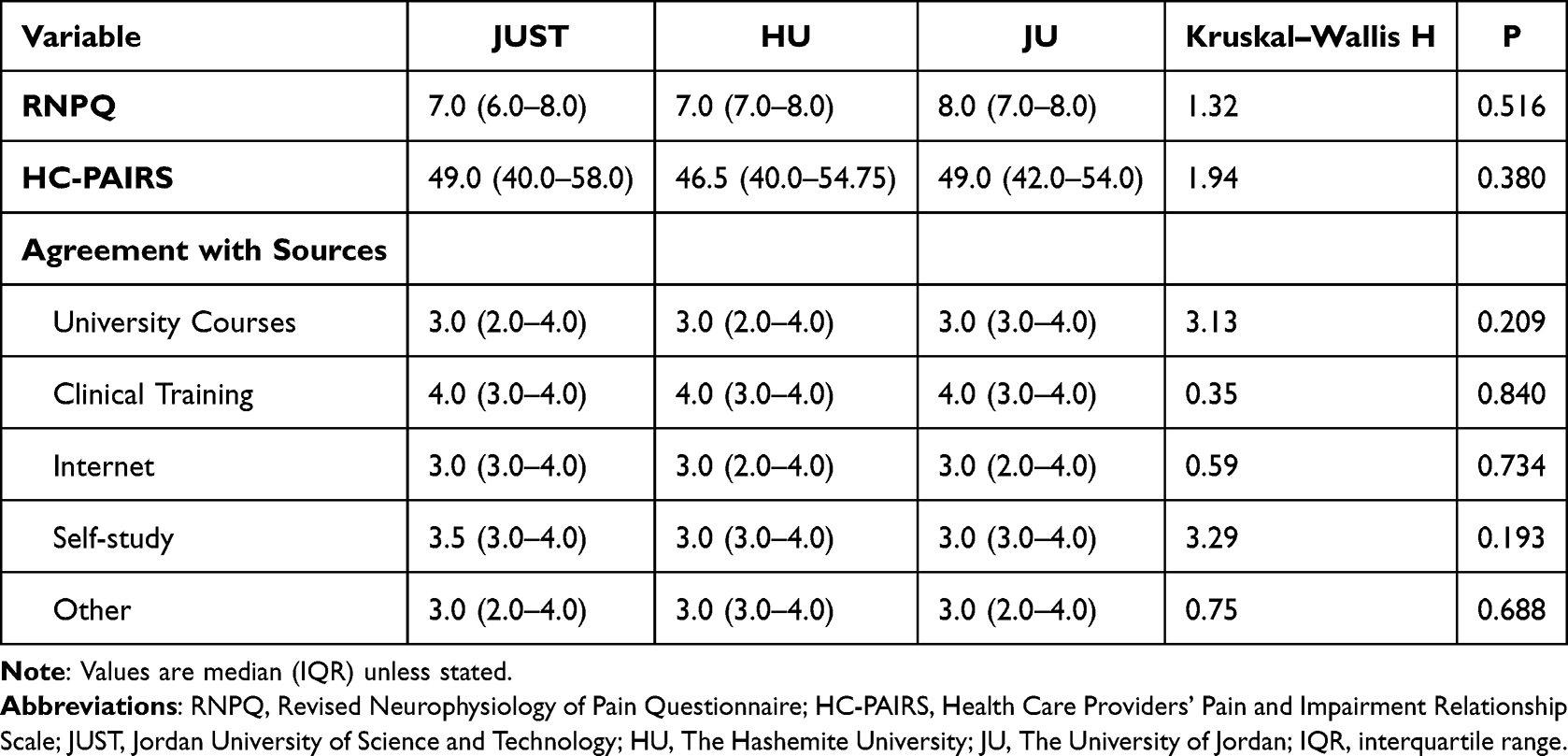 |
Table 3 University-Level Comparisons of RNPQ, HC-PAIRS, and Agreement with Pain Knowledge Sources |
 |
Figure 2 Agreement with different sources of pain knowledge by discipline (Likert scale 1–5). Boxplots display median and interquartile range (IQR). Green represents physiotherapy (PT) students and peach represents occupational therapy (OT) students. |
The Correlation Between RNPQ and HC-PAIRS
The correlations between RNPQ and HC-PAIRS assessed by Spearman’s rank correlation are presented in Table 4. The overall sample showed a statistically significant weak correlation between RNPQ and HC-PAIRS ((ρ = –0.334, 95% CI=–0.448, –0.208, p<0.001), indicating that better understanding of pain neurophysiology was associated with a more positive attitude towards pain. In contrast, there was no significant correlation in RNPQ and HC-PAIRS within PT (ρ= –0.067, p= 0.416) or within OT (ρ = –0.228, p= 0.064). The lack of statistically significant subgroup correlations may be due to limited statistical power, and these findings should therefore be interpreted with caution.
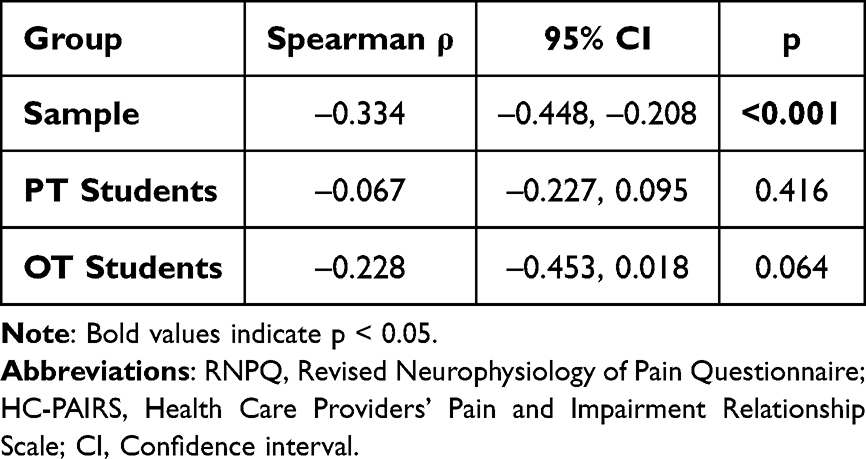 |
Table 4 Correlations Between the RNPQ and HC-PAIRS by Student Group |
A LOWESS (Locally Weighted Scatterplot Smoothing) scatterplot was created to visually assess the relationship between RNPQ and HC-PAIRS scores for the total sample (Figure 3). Overall, the LOWESS line demonstrated a non-linear mainly negative association between RNPQ and HC-PAIRS scores, with a more noticeable drop in RNPQ scores as HC-PAIRS scores increased beyond the midpoint, supporting the negative correlation observed for the total sample.
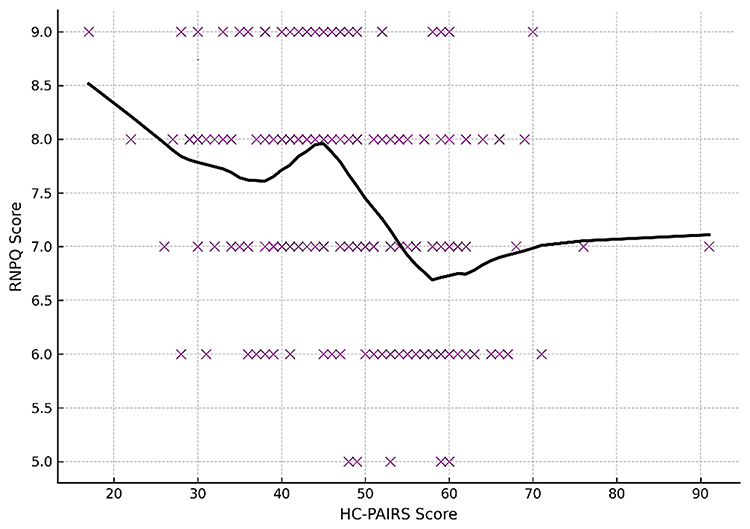 |
Figure 3 LOWESS scatterplot illustrating the relationship between Health Care Providers’ Pain and Impairment Relationship Scale (HC-PAIRS) scores and Revised Neurophysiology of Pain Questionnaire (RNPQ) scores in the total sample. Purple markers represent individual participants, and the solid line represents the locally weighted scatterplot smoothing (LOWESS) trend. |
Regression Modeling
Multiple linear regression (MLR) with backward elimination (α = 0.05) was used to build the most parsimonious model. The initial MLR model included all explanatory variables (predictors): age, gender, discipline, university, HC-PAIRS score, and five items reflecting agreement with different knowledge sources, to predict the RNPQ score (ie dependent variable).
The reduced model included three significant predictors (p<0.05): discipline (PT vs OT), agreement with university courses and HC-PAIRS (Table 5). The model demonstrated high predictive power, with 85.5% of the variance in the RNPQ score explained by the predictors (adjusted R2 = 0.855, F(3176)= 363.73, p< 0.001). Analyses showed a positive association between agreement with university courses and RNPQ scores (B = 0.91, p<0.001), while HC-PAIRS scores demonstrated a negative association (B= –0.027, p<0.001). Further, PT students achieved significantly higher scores in RNPQ than OT students (B= 0.34, p<0.001).
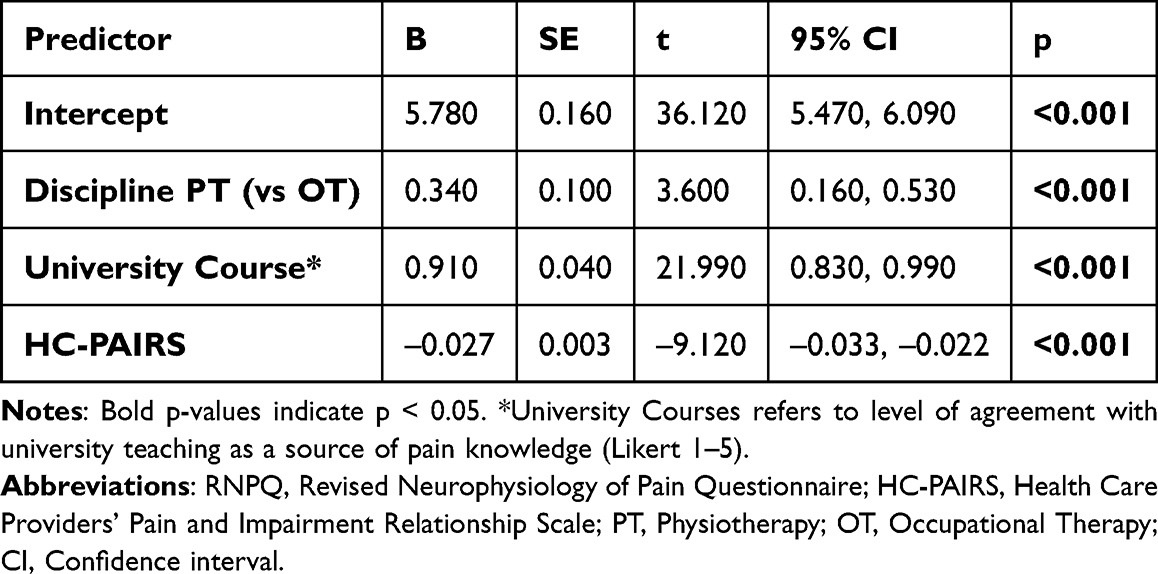 |
Table 5 Reduced Regression Model Predicting RNPQ Score |
To assess whether the association between agreement with university courses and RNPQ scores differed by discipline, an interaction term (discipline x university courses) was included (Table 6). The interaction model demonstrated improved model fit (adjusted R2 = 0.865) compared to the reduced model (adjusted R2 = 0.855; Table 7). The analysis demonstrated a statistically significant interaction term (B= 0.320, p= 0.026), with PT students exhibiting a stronger positive association between agreement with university courses and RNPQ scores than OT students (Figure 4). Further, with the interaction included, the main effect of agreement with university courses and HC-PAIRS scores remained statistically significant (p<0.001). The main effect of discipline was no longer statistically significant (p=0.135), indicating that the discipline differences in RNPQ scores depend on agreement with university courses (ie moderation).
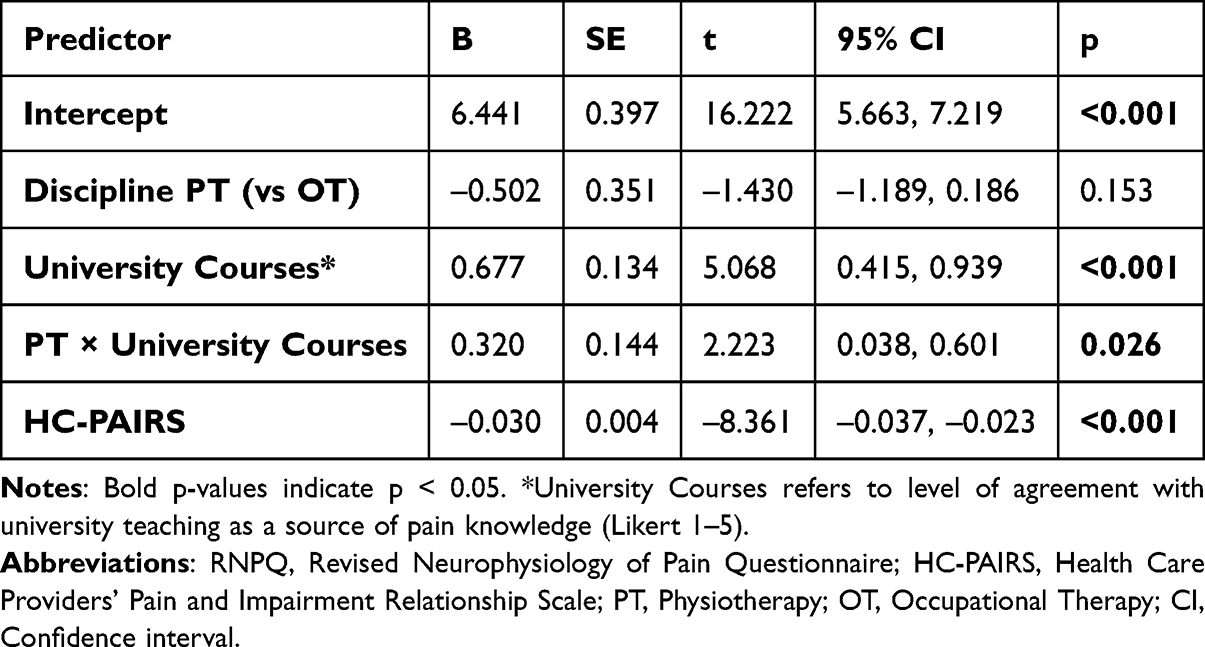 |
Table 6 Interaction Regression Model Predicting RNPQ Score |
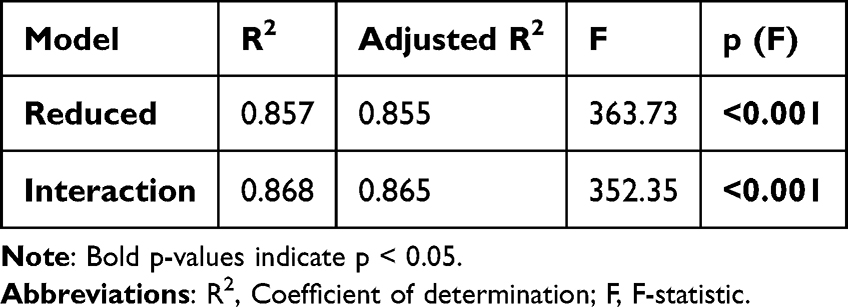 |
Table 7 Model Fit Comparison for Reduced and Interaction Models Predicting RNPQ Score |
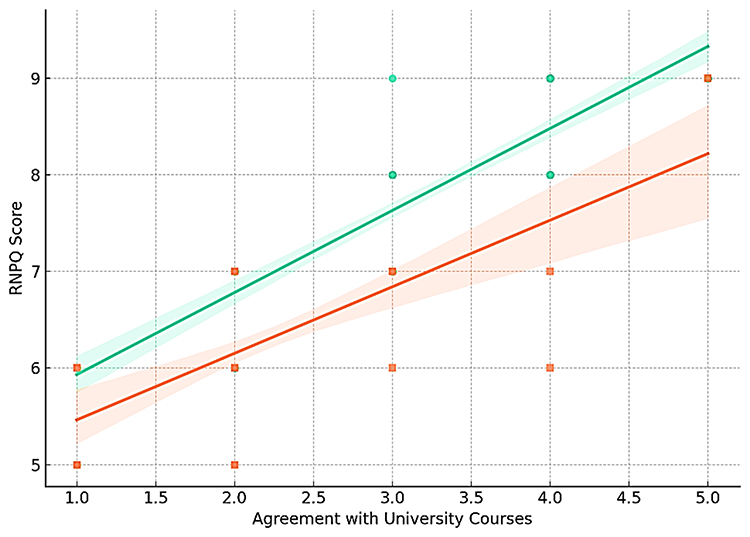 |
Figure 4 Interaction plot showing the effect of agreement with university courses on Revised Neurophysiology of Pain Questionnaire (RNPQ) scores by discipline. Lines show model-predicted means with 95% confidence intervals from the interaction model (agreement rated 1–5). The green line represents physiotherapy (PT) students and the peach line represents occupational therapy (OT) students; shaded areas represent 95% confidence intervals. |
Sensitivity analysis was conducted to evaluate the robustness of the findings by testing a full covariate model (Table S1, Supplementary materials). The full model showed a comparable adjusted R2 (0.864) to the interaction model and no meaningful change in the magnitude, direction, or significance of the key predictors. These results support the robustness and parsimony of the final interaction model (Table S2, Supplementary materials).
Diagnostic tests verified model validity. Residuals exhibited no significant violations of normality or homoscedasticity. Variance inflation factors (VIFs) were < 2.5, ruling out multicollinearity. Full diagnostics are provided in Figures S1, S2 and Table S3 (Supplementary materials).
Discussion
This study showed that final-year PT and OT students demonstrated limited to moderate levels of pain neurophysiology knowledge (as measured by RNPQ) and mixed attitudes and beliefs towards pain (as measured by HC-PAIRS). PT students exhibited a better understanding of pain neurophysiology and more positive attitudes towards pain compared to OT students. University courses and clinical training were the most frequently reported sources of pain knowledge. Further, levels of agreement with university courses as a primary source of pain knowledge positively associated with RNPQ scores, whereas higher HC-PAIRS scores (reflecting more maladaptive beliefs about pain and disability) negatively associated with lower RNPQ scores. The association between the agreement with university courses and RNPQ was stronger for PT students than OT students.
This study identified a significant difference in pain neurophysiology knowledge between final year PT students and their OT counterparts. This is evident by a higher RNPQ score of 8.0 (IQR: 7.0–8.0; 66.7%) for PT students than 6.0 (IQR: 6.0–7.0; 50%) for OT students. This represents a gap of 16.7 percentage points, resembling research findings from Mukoka et al,37 who reported a mean RNPQ scores of 58.08% and 43.42%, for South African PT and OT students, respectively. Similarly, Mankelow et al35 showed that international PT students surpassed OT students (75.8% vs 53.3%) on RNPQ. This disparity likely stems from structural discrepancies in curriculum design between the programs, particularly a greater emphasis on pain education in PT curricula. In support of this notion, Briggs et al21 demonstrated that PT curricula dedicated more formal teaching hours and more structured pain content than OT or medical curricula. This likely explains the superior pain related knowledge observed among PT students in our study.
Internationally, Jordanian PT students demonstrated a higher median RNPQ score 8 (IQR: 7.0–8.0; 66.7%) than that reported for Saudi qualified PTs (55.8%),38 South African PT students (58.1%),37 Japanese PT students (54.2%),39 and Portuguese PT students (62.5%).40 However, the RNPQ score for Jordanian PT students is slightly lower than that reported for Spanish PT students (68.9%)41 and well below baseline RNPQ scores for US-Doctor of Physical Therapy (DPT) students (76.9%) prior to pain neuroscience education intervention.42 These comparisons suggest that final-year status alone does not ensure advanced pain knowledge. In contrast, the RNPQ performance of Jordanian OT students (50%) remains below most comparable samples (43.42%)37 and (53.3%),35 consistent with reports of lower baseline pain knowledge among OT cohorts. Notably, pain knowledge among OT student cohorts remains remarkably understudied, which significantly limits comparative analysis and warrants further investigations.
In our study, PT students demonstrated a median HC-PAIRS score of 45.0 (IQR: 38.0–52.0; 49.5%), compared to a markedly higher HC-PAIRS score reported for OT students at 57.0 (IQR: 49.0–60.0; 62.6%), reflecting more biomedical- or disability-oriented beliefs for OT students. These findings align with international trends where OT students exhibit more biomedical oriented pain related beliefs than PT students. For example, in Australia, Briggs et al43 reported HC-PAIRS scores of 44.2% among PT students compared to 54.6% for OT students. Similar trends were observed for South African: 59.0% (PT) vs 62.5% (OT)37 and international (PT: 41.2% and OT: 58.0%) cohorts.35 These discipline-specific orientations likely stem from differences in curricular emphasis, where pain-focused content is historically under-emphasized in OT compared to PT programs.21
When benchmarked internationally, HC-PAIRS scores for PT students demonstrate substantial variability with our cohort (49.5%). Our PT students’ HC-PAIRS scores closely aligned with their final year Scottish (54.7%)44 and Australian (49.5%)45 PT counterparts. Conversely, our PT cohort’s scores were markedly lower than those observed in Saudi Arabia (67.1%)46 and Brazil (63.2%).47 Further, the elevated HC-PAIRS scores observed in our OT cohort (62.6%) are particularly concerning, as they consistently mirror OT global trends of more persistent biomedical biases in OT education.35,37,43 These observed cross-regional benchmarking disparities likely originate from cultural, institutional or curricular factors that frame students’ understanding of pain and disability.
The study found a significant inverse relationship between pain neurophysiology knowledge (RNPQ) and pain-related beliefs (HC-PAIRS) across the total sample (ρ = –0.334, p< 0.001). Students who demonstrated greater understanding of pain neurophysiology tended to report more positive pain-related beliefs; however, this cross-sectional design does not allow assumptions regarding directionality. The lack of significant between-discipline subgroup correlations could be explained by underpowered subgroup sample sizes rather than a true absence of correlations. Our findings align with previous research of significant moderate negative correlations between RNPQ and HC-PAIRS among final year PT students (r = –0.30)37 and across the entire PT cohort (r = –0.342).19 Springer et al19 reported stronger associations after clinical placements (r = –0.42), suggesting a progressive training effect. Furthermore, in our regression analyses, HC-PAIRS remained a significant predictor of RNPQ scores (B = −0.030, p< 0.001) after covariate adjustment, confirming a significant association between pain-related knowledge and attitudes.
Our findings suggest the need for further improvements in pain education within Jordanian PT and OT curricula. PT and OT students across all three universities (HU, JU, JUST) demonstrated limited pain knowledge with consistently persistent biomedical attitude trends. This suggests curricular rather than institutional limitations.
We found that university courses were one of the most frequently cited sources of pain knowledge (37.50%) and the strongest predictor of RNPQ scores (β = 0.677, p< 0.001). This association was significantly stronger among PT students than OT students, reflecting between-discipline differences in curricular pain education. These findings align with Alodaibi et al,16 who demonstrated that university courses were the primary source of pain knowledge among Saudi PT students. Similarly, Mankelow et al35 observed that the number of pain education teaching hours significantly predicted pain knowledge (RNPQ) and attitudes (HC-PAIRS) across international health professional students. These findings collectively highlight the primary influence that the curricular content exerts on students’ pain education knowledge, emphasizing the imperative for inclusion of standardized evidence-based neuroscience pain education within PT and particularly OT programs in Jordan.
Our findings provide multi-institutional data on pain curricula within physical and occupational therapy programs in Jordan, illuminating discipline-specific patterns to guide future curriculum reform. However, these discipline differences are descriptive rather than causal, as this study design did not include a formal audit of curricular content or instructional methods that might explain them; therefore, their interpretation requires caution. The modest effect sizes align with established educational research, which indicates that meaningful changes in knowledge and beliefs can evolve progressively through structured and sustained instructional and experiential learning. The observed association between university courses and pain knowledge scores suggests a potential educational driver and highlights practical opportunities to enhance pain curricula. Such enhancements could foster a more biopsychosocial approach in clinical practice and, ultimately, improve care for individuals with chronic pain.
Our study revealed a significant inverse relationship between pain knowledge (RNPQ) and maladaptive beliefs (HC-PAIRS). These findings highlight the relevance of addressing both knowledge and beliefs concurrently within educational approaches. This is consistent with meta-analytic evidence that biopsychosocially focused pain education improves both pain knowledge and attitudes among healthcare professionals and students.20 Remarkably, a brief (70-min) pain neuroscience education (PNE) session significantly enhanced students’ pain knowledge and attitudes.23 Similarly, Mankelow et al27 reported immediate - and sustained improvements after PNE, supporting the IASP - aligned scalable pain education approach. Overall, these findings emphasize the importance of embedding contemporary pain science education across both PT and OT training programs to better align graduate competencies with evidence-based practice.
Limitations
Several limitations should be considered when interpreting these findings. First, the cross-sectional design precludes causal inference; therefore, relationships between educational exposure, pain knowledge, and beliefs should be interpreted as associative rather than directional. Second, voluntary online recruitment may have introduced self-selection bias, and the 36% response rate may limit representativeness. Although the survey was widely disseminated with reminders, the sample may not fully reflect all final-year PT and OT students in Jordan. Third, the instrument used to assess perceived sources of pain knowledge was developed internally for this study and has not undergone formal psychometric validation. Fourth, self-reported agreement with learning sources may be subject to recall or social desirability bias; however, such measures remain informative for understanding perceived educational influences.
Fifth, RNPQ and HC-PAIRS data were summarized using medians and IQRs due to non-normality, while score percentage conversions were used to facilitate comparison with previous literature. This approach may reduce distributional detail but enhances interpretability and benchmarking relevance. Sixth, although students were recruited from three major universities, we did not conduct a systematic audit of curricular content; however, the lack of between-university differences suggests shared structural limitations in pain education nationally.
Seventh, although an a priori power calculation was not performed, the sample exceeded recommended thresholds for regression with multiple predictors; nonetheless, subgroup comparisons—particularly those involving OT students—may have been underpowered to detect smaller effects. Future studies should consider stratified sampling or oversampling of smaller subgroups. Eighth, chronic pain history and analgesic use were not assessed; these personal factors may influence pain knowledge and beliefs. Finally, findings may not generalize to students in earlier years of training or to other health professions programs. Future research should address these limitations.
Conclusion
This study provides the first multi-institutional data on pain-related knowledge and beliefs among final-year PT and OT students in Jordan. Although PT students demonstrated comparatively better understanding of pain and more favourable beliefs than their OT peers, both groups displayed significant gaps in pain neurophysiology knowledge and a tendency towards biomedical beliefs. University courses emerged as the dominant source of pain knowledge, particularly among PT students, and were positively associated with higher pain knowledge scores. The inverse relationship between pain knowledge and maladaptive beliefs confirms the interdependence of both domains, highlighting the importance of addressing both through curricular reform.
Collectively, these findings suggest a clear need for structured, biopsychosocially oriented pain education within undergraduate curricula. Implementing evidence-based pain neuroscience education (PNE) may enhance both pain knowledge and attitudes. Potential enhancements, aligned with the International Association for the Study of Pain (IASP) guidelines, could include increasing dedicated teaching hours on contemporary pain science, incorporating interprofessional and case-based learning, and fostering biopsychosocial reasoning during clinical training. Future longitudinal and interventional studies are warranted to examine curricular effectiveness and guide large-scale reforms across PT and OT education in Jordan.
Abbreviations
Participant groups & institutions: BSc, Bachelor of Science; DPT, Doctor of Physical Therapy; HU, Hashemite University; JU, University of Jordan; JUST, Jordan University of Science and Technology; OT, occupational therapy; PT, physiotherapy.
Measures & instruments: HC-PAIRS, Health Care Providers’ Pain and Impairment Relationship Scale; IASP, International Association for the Study of Pain; NPQ, Neurophysiology of Pain Questionnaire; PNE, pain neuroscience education; RNPQ, Revised Neurophysiology of Pain Questionnaire.
Study conduct & ethics: IRB, Institutional Review Board.
Statistical terms & reporting: CI, confidence interval; df, degrees of freedom; HC3, heteroskedasticity-consistent covariance estimator, type 3; ICC, intraclass correlation coefficient; IQR, interquartile range; LOWESS, locally weighted scatterplot smoothing; OLS, ordinary least squares; R2, coefficient of determination; SD, standard deviation; SE, standard error; VIF, variance inflation factor.
Epidemiology terms: GBD, Global Burden of Disease; YLDs, years lived with disability.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
Ethical approval was obtained from the Institutional Review Board of The Hashemite University (HU-IRB No. 29/9/2021/2022) before study commencement. This approval covered recruitment at the three participating universities; institutional acknowledgment and support were obtained at each site. The survey was administered anonymously online (no identifiable data were collected). Participation was voluntary, responses were confidential and had no bearing on academic standing or grades, and electronic informed consent was obtained prior to participation. The study adhered to the principles of the Declaration of Helsinki.
Acknowledgments
The authors express their gratitude for the support received from Princess Nourah bint Abdulrahman University Researchers Supporting Project (PNURSP2025R422), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia. The authors would also like to gratefully acknowledge all of the final year physiotherapy and occupational students who contributed their time to support the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Princess Nourah bint Abdulrahman University Researchers Supporting Project (PNURSP2025R422), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Disclosure
Ahmad Muhsen reports grants from Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia, non-financial support from The Hashemite University, during the conduct of the study. The authors report no conflicts of interest in this work.
References
1. Finley CR, Chan DS, Garrison S, et al. What are the most common conditions in primary care? A systematic review. Can Fam Physician. 2018;64(11):832–840.
2. Lim YZ, Chou L, Au RTM, Seneviwickrama KLMD, Cicuttini FM, Briggs AM. People with low back pain want clear, consistent and personalised information on prognosis, treatment options and self-management strategies: a systematic review. J Physiother. 2019;65(3):124–135. doi:10.1016/j.jphys.2019.05.010
3. Treede RD, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain. 2019;160(1):19–27. doi:10.1097/j.pain.0000000000001384
4. Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D. Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain. 2006;10(4):287–333. doi:10.1016/j.ejpain.2005.06.009
5. Fayaz A, Croft P, Langford RM, Donaldson LJ, Jones GT. Prevalence of chronic pain in the UK: a systematic review and meta-analysis of population studies. BMJ Open. 2016;6(6):e010364. doi:10.1136/bmjopen-2015-010364
6. Mills SE, Nicolson KP, Smith BH. Chronic pain: a review of its epidemiology and associated factors in population-based studies. Br J Anaesth. 2019;123(2):e273–e283. doi:10.1016/j.bja.2019.03.023
7. Pagé MG, Fortier M, Ware MA, Choinière M. As if one pain problem was not enough: prevalence and patterns of coexisting chronic pain conditions and their impact on treatment outcomes. J Pain Res. 2018;11:237–254. doi:10.2147/JPR.S149262
8. Hoy D, March L, Brooks P, et al. Measuring the global burden of low back pain. Best Pract Res Clin Rheumatol. 2010;24(2):155–165. doi:10.1016/j.berh.2009.11.002
9. Steiner TJ, Stovner LJ, Jensen R, Uluduz D, Katsarava Z. Migraine remains second among the world’s causes of disability, and first among young women: findings from GBD2019. J Headache Pain. 2020;21(1):137. doi:10.1186/s10194-020-01208-0
10. Zhao X, Xu M, Jorgenson K, Kong J. Neurochemical changes in patients with chronic low back pain detected by proton magnetic resonance spectroscopy: a systematic review. Neuroimage Clin. 2017;13:33–38. doi:10.1016/j.nicl.2016.11.006
11. O’Sullivan P. It’s time for change with the management of non-specific chronic low back pain. Br J Sports Med. 2012;46(4):224–227. doi:10.1136/bjsm.2010.081638
12. Gatchel RJ, Peng YB, Peters ML, Fuchs PN, Turk DC. The biopsychosocial approach to chronic pain: scientific advances and future directions. Psychol Bull. 2007;133(4):581–624. doi:10.1037/0033-2909.133.4.581
13. Kamper SJ, Apeldoorn AT, Chiarotto A, et al. Multidisciplinary biopsychosocial rehabilitation for chronic low back pain. Cochrane Database Syst Rev. 2014;2014(9):CD000963. doi:10.1002/14651858.CD000963.pub3
14. Scascighini L, Toma V, Dober-Spielmann S, Sprott H. Multidisciplinary treatment for chronic pain: a systematic review of interventions and outcomes. Rheumatology. 2008;47(5):670–678. doi:10.1093/rheumatology/ken021
15. Dwyer CP, McKenna-Plumley PE, Durand H, et al. Factors influencing the application of a biopsychosocial perspective in clinical judgement of chronic pain: interactive management with medical students. Pain Physician. 2017;20(6):E951–E960.
16. Alodaibi F, Alhowimel A, Alsobayel H. Pain neurophysiology knowledge among physical therapy students in Saudi Arabia: a cross-sectional study. BMC Med Educ. 2018;18(1):228. doi:10.1186/s12909-018-1329-5
17. Darlow B, Fullen BM, Dean S, Hurley DA, Baxter GD, Dowell A. The association between health care professional attitudes and beliefs and the attitudes and beliefs, clinical management, and outcomes of patients with low back pain: a systematic review. Eur J Pain. 2012;16(1):3–17. doi:10.1016/j.ejpain.2011.06.006
18. Gardner T, Refshauge K, Smith L, McAuley J, Hübscher M, Goodall S. Physiotherapists’ beliefs and attitudes influence clinical practice in chronic low back pain: a systematic review of quantitative and qualitative studies. J Physiother. 2017;63(3):132–143. doi:10.1016/j.jphys.2017.05.017
19. Springer S, Gleicher H, Hababou H. Attitudes and beliefs about musculoskeletal pain and its association with pain neuroscience knowledge among physiotherapy students in Israel. Isr J Health Policy Res. 2018;7(1):67. doi:10.1186/s13584-018-0266-4
20. Mankelow J, Ryan C, Taylor P, Atkinson G, Martin D. A systematic review and meta-analysis of the effects of biopsychosocial pain education upon health care professional pain attitudes, knowledge, behavior and patient outcomes. J Pain. 2022;23(1):1–24. doi:10.1016/j.jpain.2021.06.010
21. Briggs EV, Carr ECJ, Whittaker MS. Survey of undergraduate pain curricula for healthcare professionals in the United Kingdom. Eur J Pain. 2011;15(8):789–795. doi:10.1016/j.ejpain.2011.01.006
22. Briggs EV, Battelli D, Gordon D, et al. Current pain education within undergraduate medical studies across Europe: advancing the provision of pain education and learning (APPEAL) study. BMJ Open. 2015;5(8):e006984. doi:10.1136/bmjopen-2014-006984
23. Colleary G, O’Sullivan K, Griffin D, Ryan CG, Martin DJ. Effect of pain neurophysiology education on physiotherapy students’ understanding of chronic pain, clinical recommendations and attitudes towards people with chronic pain: a randomised controlled trial. Physiotherapy. 2017;103(4):423–429. doi:10.1016/j.physio.2017.01.006
24. Clarke CL, Ryan CG, Martin DJ. Pain neurophysiology education for the management of individuals with chronic low back pain: a systematic review and meta-analysis. Man Ther. 2011;16(6):544–552. doi:10.1016/j.math.2011.05.003
25. Fitzgerald K, Vaughan B, Fleischmann M, Austin P. Pain knowledge, attitudes and beliefs of Australian osteopaths drawn from a nationally representative sample. J Bodyw Mov Ther. 2020;24(4):43–50. doi:10.1016/j.jbmt.2020.06.022
26. Louw A, Diener I, Butler DS, Puentedura EJ. The effect of neuroscience education on pain, disability, anxiety, and stress in chronic musculoskeletal pain. Arch Phys Med Rehabil. 2011;92(12):2041–2056. doi:10.1016/j.apmr.2011.07.198
27. Mankelow J, Ryan C, Taylor P, Martin D. The effect of pain neurophysiology education on healthcare students’ knowledge, attitudes and behaviours: a mixed-methods randomized controlled trial. Musculoskelet Sci Pract. 2020;50:102249. doi:10.1016/j.msksp.2020.102249
28. Watt-Watson J, Hunter J, Pennefather P, et al. An integrated undergraduate pain curriculum for six health science faculties. Pain. 2004;110(1–2):140–148. doi:10.1016/j.pain.2004.03.019
29. Maayah MF, Al-Jarrah M, Mysore S, et al. The perception of physical therapy students towards their profession in Jordan. Healthcare. 2022;10(5):849. doi:10.3390/healthcare10050849
30. Green SB. How many subjects does it take to do a regression analysis? Multivariate Behav Res. 1991;26(3):499–510. doi:10.1207/s15327906mbr2603_7
31. Catley MJ, O’Connell NE, Moseley GL. How good is the neurophysiology of pain questionnaire? A Rasch analysis of psychometric properties. J Pain. 2013;14(8):818–827. doi:10.1016/j.jpain.2013.03.003
32. Moseley L. Unraveling the barriers to reconceptualization of the problem in chronic pain: the actual and perceived ability of patients and health professionals to understand the neurophysiology. J Pain. 2003;4(4):184–189. doi:10.1016/S1526-5900(03)00654-5
33. Houben RMA, Vlaeyen JWS, Peters M, Ostelo RWJG, Wolters PMJC, Stomp-van den Berg SGM. Health care providers’ attitudes and beliefs towards common low back pain: factor structure and psychometric properties of the HC-PAIRS. Clin J Pain. 2004;20(1):37–44. doi:10.1097/00002508-200401000-00006
34. Moran RW, Rushworth WM, Mason J. Investigation of four self-report instruments—FABT, TSK-HC, Back-PAQ, HC-PAIRS—to measure healthcare practitioners’ attitudes and beliefs toward low back pain: reliability and convergent validity. Musculoskelet Sci Pract. 2017;32:44–50. doi:10.1016/j.msksp.2017.07.005
35. Mankelow J, Ryan CG, Taylor PC, et al. International, multi-disciplinary, cross-sectional study of pain knowledge and attitudes in nursing, midwifery and allied health professions students. BMC Med Educ. 2022;22(1):547. doi:10.1186/s12909-022-03488-3
36. Mukaka MM. A guide to appropriate use of correlation coefficient in medical research. Malawi Med J. 2012;24(3):69–71.
37. Mukoka G, Olivier B, Ravat S. Level of knowledge, attitudes and beliefs towards patients with chronic low back pain among final year school of therapeutic sciences students at the University of the Witwatersrand—A cross-sectional study. S Afr J Physiother. 2019;75(1):683. doi:10.4102/sajp.v75i1.683
38. Alhowimel A, Alodiabi F, Alamam D, Alotaibi M, Fritz J. Current understanding of pain neurophysiology among physiotherapists practicing in Saudi Arabia. Healthcare. 2021;9(9):1242. doi:10.3390/healthcare9091242
39. Mikamo Y, Takasaki H. Pain neurophysiology knowledge enhances attitudes toward biopsychosocial management of low back pain among Japanese physical therapists. Prog Rehabil Med. 2021;6:20210039. doi:10.2490/prm.20210039
40. Marques ES, Xarles T, Antunes TM, et al. Evaluation of physiologic pain knowledge by physiotherapy students. Rev Dor. 2016;17(1):29–33.
41. Adillón C, Lozano È, Salvat I. Comparison of pain neurophysiology knowledge among health sciences students: a cross-sectional study. BMC Res Notes. 2015;8(1):592. doi:10.1186/s13104-015-1570-7
42. Bareiss SK, Nare L, McBee K. Evaluation of pain knowledge and attitudes and beliefs from a pre-licensure physical therapy curriculum and a stand-alone pain elective. BMC Med Educ. 2019;19(1):375. doi:10.1186/s12909-019-1820-7
43. Briggs AM, Slater H, Smith AJ, Parkin-Smith GF, Watkins K, Chua J. Low back pain-related beliefs and likely practice behaviours among final-year cross-discipline health students. Eur J Pain. 2013;17(5):766–775. doi:10.1002/j.1532-2149.2012.00246
44. Ryan C, Murphy D, Clark M, Lee A. The effect of a physiotherapy education compared with a non-healthcare education on the attitudes and beliefs of students towards functioning in individuals with back pain: an observational, cross-sectional study. Physiotherapy. 2010;96(2):144–150. doi:10.1016/j.physio.2009.09.010
45. Latimer J, Maher C, Refshauge K. The attitudes and beliefs of physiotherapy students to chronic back pain. Clin J Pain. 2004;20(1):45–50. doi:10.1097/00002508-200401000-00009
46. Alshami AM, Albahrani YA. A comparison of the attitudes toward chronic low back pain in Saudi, Australian and Brazilian physical therapy students. J Taibah Univ Med Sci. 2015;10(2):181–187. doi:10.1016/j.jtumed.2014.11.004
47. Ferreira PH, Ferreira ML, Latimer J, et al. Attitudes and beliefs of Brazilian and Australian physiotherapy students towards chronic back pain: a cross-cultural comparison. Physiother Res Int. 2004;9(1):13–23. doi:10.1002/pri.296
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.