Back to Journals » Journal of Pain Research » Volume 16
Pain Education and Knowledge (PEAK) Consensus Guidelines for Neuromodulation: A Proposal for Standardization in Fellowship and Training Programs
Authors Pritzlaff SG ![]() , Goree JH
, Goree JH ![]() , Hagedorn JM
, Hagedorn JM ![]() , Lee DW, Chapman KB
, Lee DW, Chapman KB ![]() , Christiansen S, Dudas A, Escobar A, Gilligan CJ
, Christiansen S, Dudas A, Escobar A, Gilligan CJ ![]() , Guirguis M, Gulati A
, Guirguis M, Gulati A ![]() , Jameson J, Mallard CJ
, Jameson J, Mallard CJ ![]() , Murphy MZ, Patel KV, Patel RG
, Murphy MZ, Patel KV, Patel RG ![]() , Sheth SJ, Vanterpool S, Singh V
, Sheth SJ, Vanterpool S, Singh V ![]() , Smith G
, Smith G ![]() , Strand NH
, Strand NH ![]() , Vu CM
, Vu CM ![]() , Suvar T, Chakravarthy K, Kapural L
, Suvar T, Chakravarthy K, Kapural L ![]() , Leong MS, Lubenow TR
, Leong MS, Lubenow TR ![]() , Abd-Elsayed A, Pope JE, Sayed D
, Abd-Elsayed A, Pope JE, Sayed D ![]() , Deer TR
, Deer TR ![]()
Received 7 June 2023
Accepted for publication 23 August 2023
Published 13 September 2023 Volume 2023:16 Pages 3101—3117
DOI https://doi.org/10.2147/JPR.S424589
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Andrea Tinnirello
Scott G Pritzlaff,1 Johnathan H Goree,2 Jonathan M Hagedorn,3 David W Lee,4 Kenneth B Chapman,5 Sandy Christiansen,6 Andrew Dudas,7 Alexander Escobar,8 Christopher J Gilligan,9 Maged Guirguis,10 Amitabh Gulati,11 Jessica Jameson,12 Christopher J Mallard,13 Melissa Z Murphy,14 Kiran V Patel,15 Raj G Patel,16 Samir J Sheth,17 Stephanie Vanterpool,18 Vinita Singh,19 Gregory Smith,2 Natalie H Strand,20 Chau M Vu,21 Tolga Suvar,22 Krishnan Chakravarthy,23 Leonardo Kapural,24 Michael S Leong,25 Timothy R Lubenow,22 Alaa Abd-Elsayed,26 Jason E Pope,21 Dawood Sayed,27 Timothy R Deer28
1Department of Anesthesiology and Pain Medicine, University of California, Davis, Sacramento, CA, USA; 2Department of Anesthesiology, University of Arkansas for Medical Sciences, Little Rock, AR, USA; 3Department of Anesthesiology and Perioperative Medicine, Mayo Clinic, Mayo Clinic, Rochester, MN, USA; 4Fullerton Orthopedic Surgery Medical Group, Fullerton, CA, USA; 5The Spine & Pain Institute of New York, New York, NY, USA; 6Department of Anesthesiology and Perioperative Medicine, Oregon Health & Science University, Portland, OR, USA; 7Mays & Schnapp Neurospine and Pain, Memphis, TN, USA; 8Department of Anesthesiology, University of Toledo, Toledo, OH, USA; 9Division of Pain Medicine, Brigham and Women’s Hospital Harvard Medical School, Boston, MA, USA; 10Division of Pain Management, Ochsner Health, New Orleans, LA, USA; 11Department of Anesthesiology and Critical Care, Memorial Sloan Kettering Cancer Center, New York, NY, USA; 12Axis Spine Center, Coeur D’Alene, ID, USA; 13Department of Anesthesiology, University of Kentucky, Lexington, KY, USA; 14North Texas Orthopedics and Spine Center, Grapevine, TX, USA; 15Department of Anesthesiology and Pain Medicine, Donald and Barbara Zucker School of Medicine at Hofstra/Northwell, Northwell Health, Hempstead, NY, USA; 16Capitol Pain Institute, Austin, TX, USA; 17Interventional Pain Management, Sutter Health, Roseville, CA, USA; 18Department of Anesthesiology, University of Tennessee, Knoxville, TN, USA; 19Department of Anesthesiology, Emory University, Atlanta, GA, USA; 20Interventional Pain Management, Mayo Clinic, Scottsdale, AZ, USA; 21Evolve Restorative Center, Santa Rosa, CA, USA; 22Department of Anesthesiology and Pain Medicine, Rush University Medical Center, Chicago, IL, USA; 23Coastal Pain and Spinal Diagnostics Medical Group, San Diego, CA, USA; 24Carolinas Pain Institute, Winston-Salem, NC, USA; 25Department of Anesthesiology, Perioperative and Pain Medicine, Stanford University, Stanford, CA, USA; 26Department of Anesthesiology, University of Wisconsin School of Medicine and Public Health, Madison, WI, USA; 27Department of Anesthesiology, Pain and Perioperative Medicine, University of Kansas, Kansas City, KS, USA; 28The Spine and Nerve Center of the Virginias, Charleston, WV, USA
Correspondence: Scott G Pritzlaff, University of California, Davis, 4860 Y Street, Suite 3020, Sacramento, CA, 95817, USA, Tel +1 916 734-6824, Fax +1 916 734-6827, Email [email protected]
Abstract: The need to be competent in neuromodulation is and should be a prerequisite prior to completing a fellowship in interventional pain medicine. Unfortunately, many programs lack acceptable candidates for these advanced therapies, and fellows may not receive adequate exposure to neuromodulation procedures. The American Society of Pain and Neuroscience (ASPN) desires to create a consensus of experts to set a minimum standard of competence for neurostimulation procedures, including spinal cord stimulation (SCS), dorsal root ganglion stimulation (DRG-S), and peripheral nerve stimulation (PNS). The executive board of ASPN accepted nominations for colleagues with excellence in the subject matter of neuromodulation and physician education. This diverse group used peer-reviewed literature and, based on grading of evidence and expert opinion, developed critical consensus guides for training that all accredited fellowship programs should adopt. For each consensus point, transparency and recusal were used to eliminate bias, and an author was nominated for evidence grading oversight and bias control. Pain Education and Knowledge (PEAK) Consensus Guidelines for Neuromodulation sets a standard for neuromodulation training in pain fellowship training programs. The consensus panel has determined several recommendations to improve care in the United States for patients undergoing neuromodulation. As neuromodulation training in the United States has evolved dramatically, these therapies have become ubiquitous in pain medicine. Unfortunately, fellowship programs and the Accreditation Council for Graduate Medical Education (ACGME) pain program requirements have not progressed training to match the demands of modern advancements. PEAK sets a new standard for fellowship training and presents thirteen practice areas vital for physician competence in neuromodulation.
Keywords: neuromodulation, pain education, spinal cord stimulation, dorsal root ganglion stimulation, peripheral nerve stimulation, fellowship training
Introduction
Growth of Neuromodulation/Need for Guidelines
The International Neuromodulation Society (INS) defines neuromodulation as “the alteration of nerve activity through targeted delivery of a stimulus, such as electrical stimulation or chemical agents, to specific neurological sites in the body”.1 Specifically, electrical stimulation of the central or peripheral nervous system is used to treat intractable trunk or limb pain for patients that fail to respond to more conservative measures. Bioelectric technologies have rapidly advanced with the rise in patients affected by debilitating chronic pain. With this accelerated growth of neuromodulation, it is imperative that training programs also update and modernize training curricula.
As with any medical procedure, using neuromodulatory techniques requires proper training. Clinical guidelines promote patient safety, and many examples of safe implementation during medical training exist. For instance, the Accreditation Council for Graduate Medical Education (ACGME) has established program requirements for pain fellowships in the United States that require residents to demonstrate competence in specific procedures before they can perform them unsupervised.2 Similarly, the World Health Organization (WHO) has developed guidelines for safe surgery that have been implemented in many countries worldwide, leading to improved patient outcomes.3
In the context of ACGME-accredited fellowships or NASS (North American Spine Society) fellowships, the term “pain fellows” refers to physicians undergoing specialized training in pain medicine. These fellows are postgraduate physicians who have completed residency training in specialties such as Anesthesiology, Physical Medicine and Rehabilitation (PM&R), Neurology, or Psychiatry. As the field of pain medicine has grown, other specialties have become eligible to complete pain fellowships, including Emergency Medicine, Radiology, and Family medicine.
Unfortunately, the requirements around neuromodulation, including spinal cord stimulation (SCS), are nebulous and non-specific. No consensus guidelines to date have addressed the need for standardization across training programs. While outcomes rely on the technical aspects of implanting these devices to treat chronic pain, standardization of pain education and knowledge is equally important to optimize the efficacy of neuromodulation. In the most recent ACGME program requirements (2022), discussion around newer neuromodulation techniques like dorsal root ganglion stimulation (DRG-S) and peripheral nerve stimulation (PNS) is notably absent (Box 1).
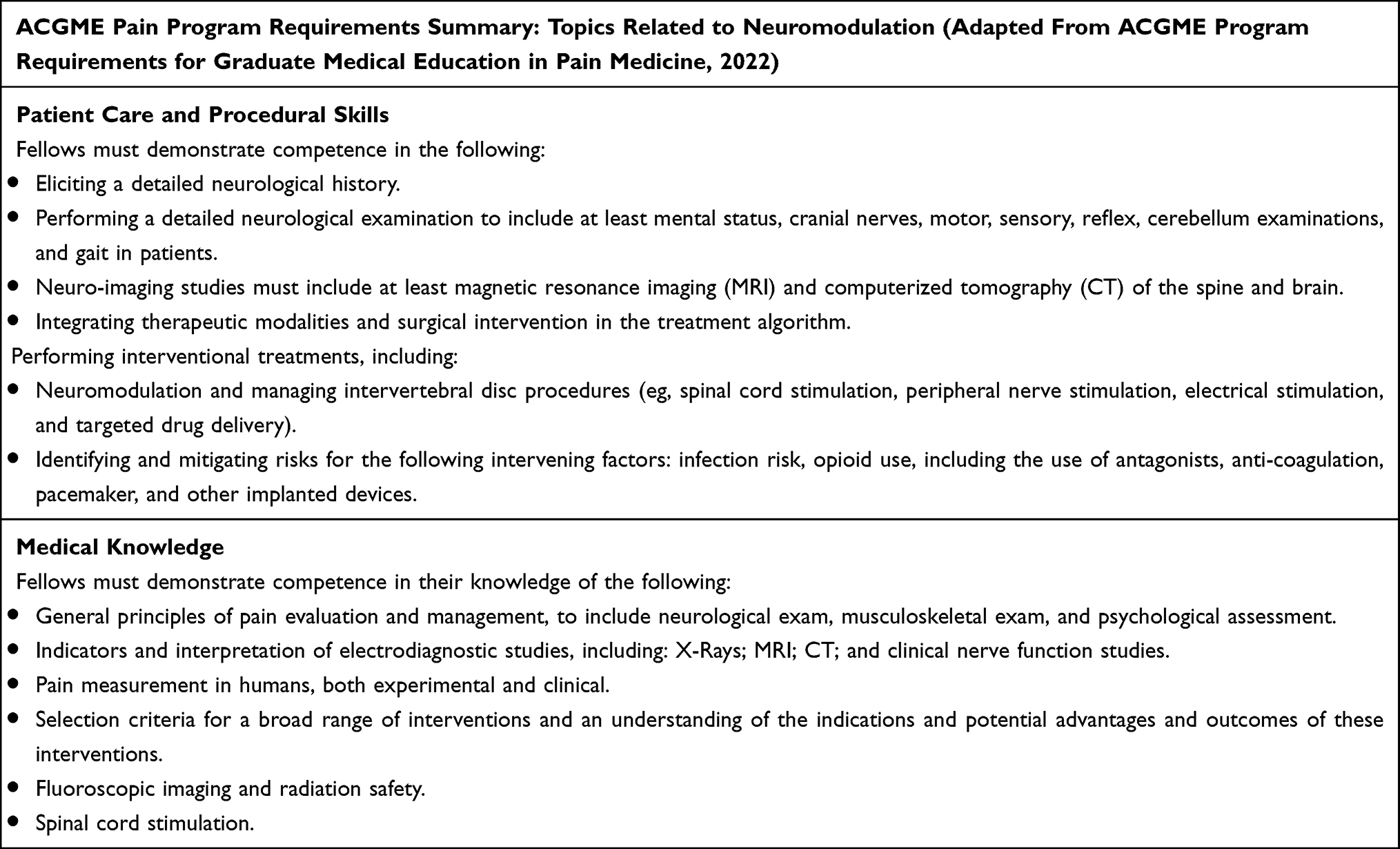 |
Box 1 Summary of ACGME Pain Program Requirements Relevant to Neuromodulation Training |
Statements in Other Interventional/Surgical Specialties (Cardiology, Laparoscopic and Robotic Surgery)
Several societies have issued guidelines to establish minimum standards for advanced training. These guidelines form a framework within training programs to meet standards and ensure training consistency. For instance, the American College of Cardiology published an advanced training statement on Interventional Cardiology interventions in 2023, which guided fellowship directors and faculty, didactic programs, clinical experience, patient selection, and hands-on clinical experience.4
Similarly, The British Journal of Urology published a consensus statement for standardized training for robotic surgery in 2015. The authors of this manuscript highlighted the need for a universally standardized training curriculum, assessment of training of trainers, and set requirements for certification.5 In 2018, the International Journal of Surgery published a Delphi study on the optimal training curriculum for advanced minimally invasive surgery. The study involved fifty-seven international experts in advanced minimally invasive surgery across multiple specialties who completed a three-round survey. The study concluded that trainers must demonstrate competencies via a “train the trainer” course, multi-step coursework including basic and advanced skill training, and technical evaluation tests via recorded surgical videos before accreditation.6
Examples of Interventional Consensus Training
In the case of neuromodulation, clinical guidelines are necessary to help ensure that trainees receive the training required to perform the procedures safely and effectively. The Neuromodulation Appropriateness Consensus Committee (NACC) has provided guidelines for the preoperative assessment, intraoperative techniques, and post-operative care of implantable neuromodulation therapies.7,8 The North American Neuromodulation Society (NANS) has also created educational curricula for PNS, SCS, and intrathecal drug delivery (IDDS) per ACGME pain fellowship program requirements.9–11 However, consensus guidelines must address the need for standardization across training programs. While outcomes rely on the technical aspects of safely delivering implantable electroceuticals to treat chronic pain, standardization of pain education and knowledge is equally important to optimize the efficacy of neuromodulation. Therefore, we aim to provide a standardized set of guidelines for fellowship and training programs across the international chronic pain medicine community, the United States, and the international community to improve trainee confidence, safety, and patient outcomes.
Methods
The Pain Education and Knowledge (PEAK) Consensus Guidelines for Neuromodulation were carefully designed to ensure a comprehensive and diverse perspective. To achieve this, a diverse group of authors was assembled, comprising experts from academia, private practice, and pain program directors, all of whom possess extensive experience in the field of neuromodulation. ASPN members and board members nominated authors, or they were self-nominated. The final list of authors was vetted and selected by the ASPN executive board. This diverse group was chosen deliberately to incorporate a broad range of viewpoints, enhancing the guidelines’ overall applicability and relevance.
A comprehensive literature review was undertaken to develop the guidelines despite the need for more current research in certain areas. Despite the challenge, we aimed to include the most up-to-date evidence complemented by the authors’ expertise in neuromodulation. A key strength of our approach lies in the achievement of unanimous consensus among all the authors regarding each of the 13 statements presented in the guidelines. This level of agreement signifies a robust foundation for the recommendations and ensures that the final guidelines are founded on a strong collective expert opinion. By combining diverse perspectives, the most current evidence, and unanimous consensus, our neuromodulation education guidelines for pain fellows aspire to be an authoritative and invaluable resource for the field, fostering excellence in pain management and patient care.
The consensus statements were created by thoroughly reviewing and analyzing the literature on neuromodulation education. Due to the breadth of new information around neurostimulation, the committee decided to focus its recommendations on SCS, DRG-S, and PNS. The authors carefully considered the available evidence and incorporated their experiences and expertise to develop statements reflecting current knowledge and best practices in the field.
A systematic consensus-building process ensured that all authors’ final recommendations were based on unanimous feedback. The authors engaged in multiple rounds of discussion and review to refine the statements and achieve consensus. The authors were encouraged to provide input and voice their concerns, and any disagreements were resolved through dialogue and compromise until a consensus was reached.
Despite a lack of high-quality evidence describing best practices in neuromodulation education, the authors tried to incorporate the most up-to-date data available. The recommendations were grounded in the best available evidence, and the authors used their clinical experience and judgment to fill in any gaps in the literature. By bringing together an experienced, diverse group of authors and using a consensus-building approach, the paper represents a consensus of the most current knowledge and best practices in the field, providing valuable guidance to educators, clinicians, and researchers. Additionally, bias control for consensus points was implemented by several factors, including recusal, transparency, and an author serving as a bias referee. A summary of the PEAK Consensus Committee recommendations is shown in Box 2.
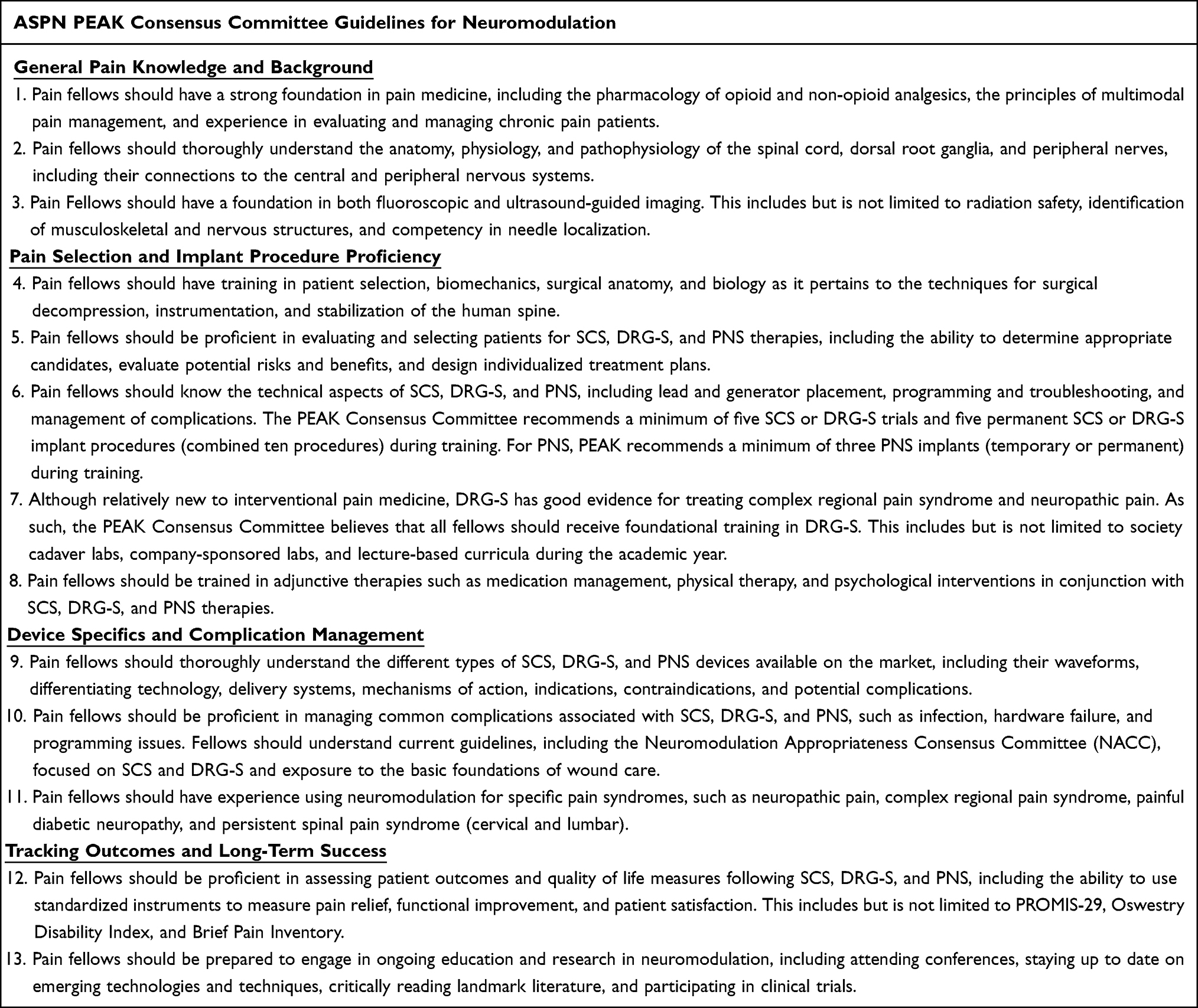 |
Box 2 Summary of PEAK Guidelines |
Results: Consensus Statements and Evidence
Consensus Statement 1: Pain fellows should have a strong foundation in pain medicine, including the pharmacology of opioid and non-opioid analgesics, the principles of multimodal pain management, and experience in evaluating and managing chronic pain patients.
Understanding the foundations of pain diagnosis and the nuances of multimodal pain treatment is key to effectively treating pain and improving function. Fellows should be proficient in identifying pain states and mechanisms, anatomic sources of pain, functional limitations and contributors, and psychological confounders. Standardizing the core concepts of pain assessment and treatment taught during pain fellowship ensures that trainees are best equipped with the knowledge to safely and effectively provide advanced pain management care.
The first step in treating chronic pain is to assess and identify the causes of pain accurately. Therefore, history taking, physical examination, and test interpretation abilities are fundamental during pain fellowship training.2 The overall goal of multimodal pain treatment should be to treat the underlying cause of pain to provide relief while optimizing patient function.
Selecting effective, non-opioid medications for pain treatment requires understanding the mechanisms by which pain signals are transmitted. Vardeh et al describe five pain mechanisms and the types of medications that target them--nociceptive transduction, peripheral sensitization, ectopic activity, central sensitization, and central disinhibition.12 Different pharmacologic agents can target each of these mechanisms of pain transmission.
Opioids (both natural and synthetic) are among the most effective pain medications available.13 However, while opioids tend to be predictably effective in acute pain, the use of opioids for chronic pain is more complicated. Prolonged use of opioids is associated with a high risk of side effects, dependence, opioid use disorder, and overdose.14,15 As a result, the Centers for Disease Control and Prevention (CDC) has released updated guidelines and recommendations when using opioids for pain management.16 Understanding these guidelines is vital to understand the proper multimodal treatment.
Multiple non-pharmacologic options help reduce pain and restore function in treating pain patients. First-line therapies involve non-invasive interventions and can instill powerful psychological and physical tools when addressing underlying chronic pain issues. To that end, physical therapy and psychological interventions are effective for chronic pain patients.17,18 Introducing these modalities early in the therapy pathway is important for patients and can help supplement other modalities or prevent the need for pharmacological or invasive non-pharmacological options.
Not all people will respond to non-invasive or pharmacological modalities, and presenting interventional pain modalities may be an option in these patients. With appropriate diagnosis and patient selection, interventional pain management can be very effective regarding pain intensity, interference, and quality of life. As per recent comprehensive guidelines developed by the United States Department of Health and Human Services, an individualized stepwise interventional approach carried out by fellowship-trained pain physicians is paramount in providing successful and safe patient care.19 Setting a solid foundation for diagnosing pain generators will lead to better patient selection and outcomes with various pain modalities and interventions. A stepwise, individualized approach is essential when treating pain patients. Using multiple modalities simultaneously (ie, cognitive behavioral therapy combined with epidural steroid injections) may aid a swifter recovery and return to function.
Consensus Statement 2: Pain fellows should thoroughly understand the anatomy, physiology, and pathophysiology of the spinal cord, dorsal root ganglia, and peripheral nerves, including their connections to the central and peripheral nervous systems.
The PEAK consensus recommends that pain fellows thoroughly understand the anatomy, physiology, and pathophysiology of the spinal cord, dorsal root ganglia, and peripheral nerves. This also includes the connection between the central and peripheral nervous systems. Given the increasing prevalence of chronic pain, this knowledge is essential for understanding pain mechanisms and developing effective multimodal pain management strategies. Multiple pain societies have content outlines for the recommended fundamentals, including the International Neuromodulation Society (INS) and the International Association for the Study of Pain (IASP).
While spinal cord and dorsal root ganglion stimulation can be an effective pain management tool, it does carry some risks. Thus, pain physicians need expert knowledge of the relevant anatomy to decrease the risk of neurologic injury.20–23
Integration of the relevant anatomy to determine optimal candidates for SCS, DRG-S, or PNS is imperative before performing procedures. This also includes a review of the appropriate MR imaging to evaluate for significant spinal or foraminal stenosis where these space-occupying leads can result in neurologic injury. For PNS, scanning the target area with ultrasound can assist with preprocedural planning and identify the area of optimal lead placement.
Consensus Statement 3: Pain fellows should have a foundation in both fluoroscopic and ultrasound-guided imaging. This includes but is not limited to radiation safety, identification of musculoskeletal and nervous structures, and competency in needle localization.
Fluoroscopy and ultrasound are the two most common imaging modalities used in interventional pain management. In general, fluoroscopy is superior for visualizing bony structures of the spine, while ultrasound is used to visualize soft tissue, vessels, and nerves.24 As such, Pain Medicine fellowships must establish a strong foundation of best practices in competency and safety that will carry forward in independent practice.
Fluoroscopic guidance uses a fluoroscope, which includes the X-ray generator and tube, collimator, and image intensifier. To minimize radiation exposure, practitioners should apply the principle of “as low as reasonably achievable” (ALARA) by reducing exposure time, maximizing distance from the radioactive sources, and using lead shielding.25 Hence, programs should educate trainees on the importance of wearing dosimeters, image collimation, pulsed or “low dose” fluoroscopy, intermittent image capture during needle advancement, and removing radio-dense objects (such as metal instruments) during live fluoroscopy to limit radiation exposure risk.26
Furthermore, fellows should know the factors that lead to higher radiation exposure levels. When the clinical scenario necessitates higher dose radiation, the care team should maximize the distance between themselves and the fluoroscope. For example, the majority of radiation exposure for the team comes from scatter radiation, which is reduced by up to 90% by stepping back one meter from the source.25 Trainees must also be comfortable applying directional terms, such as cephalad, caudal, ventral, dorsal, medial, lateral, anterior-posterior (AP), and oblique when discussing needle movements or imaging equipment.
With ultrasound guidance, successful utilization requires knowledge of appropriate frequency, probe selection, depth, gain, and Doppler settings.27
Lastly, to competently carry out a procedure, trainees must arrange patient and equipment positioning, identify normal and abnormal structures on imaging, recognize surrounding critical structures, relay required views for safe multiplanar needle advancement, and ultimately produce ideal final needle placement. With ultrasound, both in-plane and out-of-plane needle approaches are described for various ultrasound-guided procedures. Notably, the out-of-plane approach does not maintain a direct view of the needle tip during advancement.27
Consensus Statement 4: Pain fellows should have training in patient selection, biomechanics, surgical anatomy, and biology as it pertains to the techniques for surgical decompression, instrumentation, and stabilization of the human spine.
Fellowship affords the opportunity to create collaborative partnerships in the ever-changing world of pain and spine care. No other technique exemplifies this more than neuromodulation of the spine, as paddle and percutaneous techniques can be utilized with similar safety profiles.28 A comprehensive understanding of surgical candidacy, including surgical technique and instrumentation considerations, alongside biomechanics (pelvic incidence, sagittal balance, spine lordosis, and kyphosis), will improve patient outcomes and the durability of neuromodulation care.29 In addition, these skills promote improved treatment selection, broaden patient access, and strengthen the treatment algorithm for using neuromodulation or instrumentation, fixation, stabilization, or decompression to manage disorders of the human spine and beyond.30
Consensus Statement 5: Pain fellows should be proficient in evaluating and selecting patients for SCS, DRG-S, and PNS therapies, including the ability to determine appropriate candidates, evaluate potential risks and benefits, and design individualized treatment plans.
Fellows should be directly involved in patient discussions in an office setting regarding neuromodulation options, including SCS, DRG-S, and PNS. Fellowship programs should include a series of didactic lectures, seminars, and cadaver training sessions delineating appropriate patient selection for neuromodulation techniques. This should be accomplished by defining the characteristics of optimal patients, including the currently approved indications for SCS, DRG-S, and PNS.20,31,32 Ideal patients should have pathology consistent with approved indications for the selected neuromodulation modality. Instruction should also focus on comorbidities that increase the risk of infection (obese, smokers, diabetics, immunodeficiencies) and complications (significant spinal pathology or concurrent medical problems).7,33–36 Fellows must also understand the psychological risk factors associated with poor procedural outcomes, including uncontrolled mood disorder, addiction, and underlying psychosocial stressors.
Finally, delineating factors that make patients more appropriate for one therapy modality versus another should be explicitly included. Informed consent is vital to any advanced procedural intervention. Trainees should be able to conduct a detailed risk and benefit discussion with any patient before a procedure they will perform.
Consensus Statement 6: Pain fellows should know the technical aspects of SCS, DRG-S, and PNS, including lead and generator placement, programming and troubleshooting, and management of complications. The PEAK Consensus Committee recommends a minimum of five SCS or DRG-S trials and five permanent SCS or DRG-S implant procedures (combined ten procedures) during training. For PNS, PEAK recommends a minimum of three PNS implants (temporary or permanent) during training.
After learning indications and appropriate patient selection (as discussed in the previous section), it is paramount that pain fellows develop an understanding of the technical aspects of SCS, DRG-S, and PNS. Unfortunately, these skills have not been emphasized in many pain fellowship programs. Additionally, ACGME program requirements only state that fellows should demonstrate competence in “neuromodulation and managing intervertebral disc procedures (eg, spinal cord stimulation, peripheral nerve stimulation, electrical stimulation, and targeted drug delivery).” ACGME does not define how competence is measured or how many procedures should be required.2
The need for increased access and standardized education due to unmet training needs has been previously identified in multiple publications.37–39 Pak et al identified deficiency in SCS case volume as one of the most common barriers (38.5%). The deficiency of neuromodulation education can be attributed to various reasons, including lack of infrastructure to support neuromodulation, attendings with variable training and comfort level with neuromodulation therapies, and limited resources dedicated to neuromodulation. ASPN PEAK Consensus Committee recommends that education should include but not be limited to lead and generator placement, programming and troubleshooting, and management of complications.
The number of procedures required to obtain true proficiency remains in question and is somewhat arbitrary. Historically, consensus recommendations have been to guide the standardization of fellowship-based SCS training, though detailed requirements have yet to be agreed upon.9,11 For example, Henderson et al previously recommended the participation of at least ten electrode arrays in the epidural space as the primary operator under the direct supervision of a recognized mentor.40 Unfortunately, these recommendations were proposed over a decade ago without any significant follow-up or means of implementation.
ASPN PEAK Consensus Committee recommends that trainees have at least ten SCS and/or DRG-S neuromodulation procedures during their fellowship year (five trials and five permanent implants). The recommendation of ten procedures amounts to an average of one neuromodulation case per month, which the committee felt was relatively overall low but realistically attainable for nearly all existing fellowship training programs. Conversely, given the unique nature of PNS and the placement of these devices in the peripheral nervous system, the committee recommends that fellows complete three implants (temporary or permanent) during their training year to be considered competent in PNS.
Neuromodulation cases should be supervised by a fellowship director or qualified attending, appropriately trained in either SCS, DRG-S, or PNS. Physicians who are qualified to teach fellows on neuromodulation procedures should possess the following attributes: a comprehensive understanding of the evidence supporting the procedure, expertise in patient selection for the intervention, verified proficiency accredited by a credentialing body or a specialized training program, and extensive knowledge pertaining to post-operative care and effective management of potential complications. These qualifications ensure the dissemination of accurate and up-to-date information, fostering the development of competent practitioners in neuromodulation. Trainee participation during each case should be substantial enough to count towards one’s proficiency. At a minimum, the trainee should be the first assistant, which includes direct involvement with 1) Epidural access (SCS and DRG-S), 2) Utilization and understanding of image guidance (whether fluoroscopy or ultrasound), and 3) Lead placement.
The rationale behind this decision by the PEAK Consensus Committee to include specific implant procedure numbers is due to the growing expectations for pain physicians to implant various types of neuromodulation systems. This is particularly relevant with advancements in minimally invasive spine procedures and ongoing improvements in neuromodulation implantation tools and techniques. Furthermore, direct involvement in implant procedures provides training and experiences that are not attainable with trials alone. Implant cases are more detailed and thus require more planning pre-operatively, increased understanding perioperatively, and additional patient care post-operatively. Based on the educational advantages, implant training should be required for all pain fellows, regardless of whether they intend to do their implants in the future.
Consensus Statement 7: Although relatively new to interventional pain medicine, DRG-S has good evidence for treating complex regional pain syndrome and neuropathic pain. As such, the PEAK Consensus Committee believes that all fellows should receive foundational training in DRG-S. This includes but is not limited to society cadaver labs, company-sponsored labs, and lecture-based curricula during the academic year.
Although relatively new to interventional pain medicine, DRG-S has robust and growing evidence in treating complex regional pain syndrome and neuropathic pain. The ACCURATE study demonstrated that DRG-S yields a higher treatment success rate for complex regional pain syndrome and causalgia at 3 and 12 months, compared to traditional spinal cord stimulation.41 Since this time, there has been increasing data highlighting the uses of DRG-S. For example, DRG-S for refractory, chronic neuropathic knee pain has significantly improved pain scores and quality of life and reduced opioid usage.42 Similarly, DRG-S for treating chronic pelvic pain has been shown to improve pain scores and reduce opioid usage significantly.43 DRG-S has also been reported to successfully treat neuropathic groin pain, foot/ankle pain, and phantom limb pain.44,45
A pooled analysis of 217 patients with DRG-S for CRPS type I, causalgia, and back pain found a 63% responder rate (defined as greater than 50% relief) at 12-month follow-up.46 Groin and foot pain (areas that are historically more challenging to treat with traditional SCS) had a responder rate of 80% with DRG-S. Complication rates in this study were comparable to those observed for other neurostimulation therapies.
Long-term results have also demonstrated the durability of this therapy. A single-center prospective study of 62 patients with chronic neuropathic pain of multiple types treated with DRG-S reported significant pain reduction and improved functionality sustained through a 3-year follow-up period.47
Given this growing body of evidence supporting DRG-S, all fellows in interventional pain medicine must receive foundational training in this technique. This training should include both lecture-based and practical components. Since 2019, guidelines and best practices for DRG-S have been published by multiple groups, including the NACC and ASPN. These foundational papers provide evidence-based recommendations on patient selection, procedural techniques, and post-operative care, ensuring pain fellows receive comprehensive and standardized training. By adhering to these guidelines, pain fellows can develop a solid foundation in DRG-S, enabling them to offer safe and effective treatment options for patients suffering from chronic pain.32,48
Concepts of particular importance in the lecture curriculum include the anatomy and physiology of the DRG, its role in the chronic pain state, and the mechanisms by which stimulation of the DRG relieves pain. The lecture material should also review the techniques of safe DRG-S lead placement and implantation. Fellows should also receive education on the existing clinical data for DRG-S and a review of the appropriate levels to target based on the site of pathology. This material should be supplemented with case reviews to highlight real-world use examples of DRG-S.
Practical components include hands-on training in society cadaver labs and company-sponsored labs. Other considerations would be the establishment of partnerships with institutions performing a higher volume of DRG-S cases for fellows to visit as an away rotation.
Consensus Statement 8: Pain fellows should be trained in adjunctive therapies such as medication management, physical therapy, and psychological interventions in conjunction with SCS, DRG-S, and PNS therapies.
Conservative management, including pharmacologic and non-pharmacologic interventions, should be done before and in conjunction with advanced neuromodulation therapies. Pain fellows should understand common non-opioid analgesics such as topical medications, acetaminophen, non-steroidal anti-inflammatory medications (NSAIDs), muscle relaxants, gabapentinoids, and antidepressants. Antidepressants and gabapentinoids should be considered first-line agents for neuropathic pain.49 Opioids have been shown to perform similarly to NSAIDs, gabapentinoids, and antidepressants for various chronic pain conditions;50 however, they may be considered in select patients, especially for cancer-related pain.51 Therefore, pain fellows should be trained in opioid management as well. The analgesic medications should be carefully selected based on the severity of pain, type of pain, comorbidities, potential drug interactions, and side effects.
Physical therapy (PT) has been proven beneficial for many musculoskeletal and post-surgical indications. Neuromodulation in combination with PT is more cost-effective than PT alone.52 However, the percentage of pain relief determines success in many neuromodulation studies. Nevertheless, pain impacts the quality of life, work status, and sleep by causing physical and psychological distress.53 Cognitive, affective, behavioral, and psychophysiological interventions such as cognitive behavioral therapy (CBT) and biofeedback have improved outcomes in patients with chronic pain.54 Some recent studies suggested neuromodulation’s effect on directly impacting pain’s affective and emotional components.55
Consensus Statement 9: Pain fellows should thoroughly understand the different types of SCS, DRG-S, and PNS devices available on the market, including their waveforms, differentiating technology, delivery systems, mechanisms of action, indications, contraindications, and potential complications.
In the past two decades, significant advancements in spinal cord stimulation led to various modern waveforms and hardware development. To understand waveforms, SCS uses three primary parameters: amplitude, pulse width, and frequency. The amount of charge delivered is dependent on amplitude and pulse width. Conventional stimulation was the primary waveform utilized in the first four decades since SCS was adopted. It is characterized by low frequency (40–100Hz), high amplitude (3.6–8.5mA), and pulse width of 300–600 µs—the high charge per pulse results in perceived “paresthesia” by patients.56
In the mid-2010s, new waveforms were introduced to the market. High frequency (HF) the frequency of 10khz characterizes SCS with a pulse width of 30 µs and amplitude between 1–5mA. The SENZA randomized control trial (RCT) showed improved low back pain and leg pain relief compared to tonic stimulation.57
Burst SCS uses a series of five 1000 µs pulses delivered at 500 Hz followed by a repolarization pulse with each series repeated at 40 Hz, mimicking the natural firing pattern of endogenous neurons.58 The SUNBURST study59 demonstrated the efficacy of burst stimulation compared to tonic stimulation.
Similarly, High-dose (HD) stimulation is frequently used as an alternative to tonic stimulation to treat low back and leg pain. The efficacy of using the Evolve workflow involving stimulating at 1 kHz with a pulse width from 90–220 µs was demonstrated in the Vectors study.60 Differential Target Multiplexed (DTM) SCS uses electrical signals and multiple anatomical targets to target neurons and glial cells differently to balance neuro-glial interaction and optimize neuromodulation outcomes. The DTM RCT61 showed a superior effect on back pain and leg pain treatment using DTM SCS versus tonic stimulation.
Most recently, closed-loop SCS measures individual evoked compound action potential (ECAP) and uses it as a feedback control mechanism to maintain desired dorsal column fiber activation to deliver more consistent therapy. This development can mitigate unpleasant side effects from postural changes. The Evoke study showed that an ECAP-controlled closed-loop stimulation could provide significantly greater relief for up to 12 months than open-loop SCS.62
In addition, there is active research around pulsed radiofrequency ultrahigh frequency stimulation up to 500kHz63 to provide analgesic relief.64
There are multiple delivery platforms. Currently, most implanted neuromodulation devices are spinal cord stimulators. However, the popularity of DRG-S and PNS has allowed the delivery of the waveform at both the cell body and the peripheral nervous system.31,41
SCS systems are available in rechargeable and recharge-free platforms. The rechargeable devices are typically smaller, with more extended battery longevity than recharge-free devices. However, the explant rate is higher for rechargeable devices at 22% compared to recharge-free stimulators at 19.2%.65
It is vital to understand the MRI conditionality of each neuromodulation system. Most devices are MRI conditional, with some restrictions for various imaging requirements.
Consensus Statement 10: Pain fellows should be proficient in managing common complications associated with SCS, DRG-S, and PNS, such as infection, hardware failure, and programming issues. Fellows should understand current guidelines, including the Neuromodulation Appropriateness Consensus Committee (NACC), focused on SCS and DRG-S and exposure to the basic foundations of wound care.
To effectively plan neuromodulatory care for patients, fellows must understand how to manage common complications associated with the procedures and implants. Current guidance from the ACGME is nebulous, stating that fellows should demonstrate competence in recognizing risks and complications related to interventional procedures. SCS, DRG-S, and PNS are considered advanced pain procedures; therefore, understanding the potential complications of implantable devices is paramount. The first significant complication for fellows to be proficient in managing is infections. The incidence ranges from 4–10% and is a common reason for explant.21 Fellows should be trained in the strategies to decrease identified risk factors for implantation in their patients. They should be able to identify the signs and symptoms associated with superficial infections and understand the utility of lab tests and appropriate antibiotics. Each fellow should be familiar with the NACC for Infection Prevention and Management and be able to apply the recommendations at all stages of neuromodulatory procedures.35 Fellows need to have exposure to wound management to understand the basic tenets of wound healing. In addition, fellows should be able to identify and manage device hardware failures, including lead migration, fracture, malfunction, battery failure, and pain related to the device components. Fellowship training should include education around the basic parameters of programming each device and understanding the proposed mechanisms of action for the various techniques used. In addition, they should practice SAFE guidelines outlined by Krames et al to ensure good clinical decision-making is done based on device selection, therapy adoption, and safety perspective.66
Consensus Statement 11: Pain fellows should have experience using neuromodulation for specific pain syndromes, such as neuropathic pain, complex regional pain syndrome, painful diabetic neuropathy, and persistent spinal pain syndrome (cervical and lumbar).
Because neuromodulation primarily affects neuropathic pain, correctly diagnosing and differentiating neuropathic pain syndromes is essential. This is critical to appropriate patient selection and, ultimately, good outcomes. According to the International Association for the Study of Pain (IASP), neuropathic pain can be divided into central and peripheral pain.67 It is also crucial to differentiate neuropathic and nociceptive pain since patients present with a combination of these pain generators. Patients should understand that neurostimulation therapy is primarily utilized for neuropathic pain, as expectation management is crucial in successfully adopting neuromodulation.
Several screening tools can be used to delineate neuropathic pain, including the Leeds assessment of neuropathic symptoms and signs (LANSS), Neuropathic Pain Questionnaire (NPQ), Douleur Neuropathique 4 questions (DN4), ID-Pain, and painDETECT. These can be used with a comprehensive history and physical exam. Additional testing can include imaging, electrodiagnostics, quantitative sensory testing, laser-evoked action potentials, skin biopsy, laboratory studies, or diagnostic injections.68 Familiarity with common neuropathic pain syndromes amenable to SCS therapy can help practitioners determine the appropriate treatment.
Complex Regional Pain Syndrome: CRPS is a complex pain syndrome causing debilitating neuropathic pain with autonomic and inflammatory symptoms, including sensory, motor, sudomotor, and vasomotor changes. CRPS Type 1 occurs without specific nerve injury, whereas CRPS Type 2 occurs following nerve injury. When CRPS is suspected, fellows should refer to the revised 2012 IASP Criteria, aka the “Budapest Criteria”, to aid in diagnosis.69 In patients with focal neuropathic pain, DRG-S should be considered.
Diabetic Peripheral Neuropathy (DPN): DPN should be suspected in diabetic patients who develop distal symmetric polyneuropathy, particularly in a “stocking and glove” distribution, first affecting the distal hands and feet and progressing proximally. Several SCS therapies have been FDA-approved in the treatment of DPN.70 Since this patient population is prone to infection and poor healing, fellows should refer to the NACC guidelines to decrease the potential for perioperative complications, including optimization of hemoglobin A1c, before implantation.35
Persistent Spine Pain Syndrome (PSPS): PSPS refers to patients with persistent pain despite surgical intervention. Neuromodulation is an effective treatment for cervical and lumbar PSPS.71 North et al demonstrated in an RCT that SCS was more cost-effective and had better outcomes when compared to reoperation and, therefore, should be considered before repeat surgery.72 In addition, efforts should be taken to rule out nociceptive causes of pain, ie, facet or SI joint pain.
Vascular Disorders: Spinal cord stimulation effectively treats ischemic pain related to refractory angina and peripheral vascular disease. Additionally, SCS has been shown to cause vasodilation, improving blood flow.73
Focal Neuropathic Pain: PNS or DRG-S should also be considered in focal neuropathic pain, where individual nerves can be isolated or targeted. Moderate-strong evidence supports PNS in treating migraine, postamputation pain, chronic pelvic pain, and chronic low back and lower extremity pain.74
Consensus Statement 12: Pain fellows should be proficient in assessing patient outcomes and quality of life measures following SCS, DRG-S, and PNS, including the ability to use standardized instruments to measure pain relief, functional improvement, and patient satisfaction. This includes but is not limited to PROMIS-29, Oswestry Disability Index, and Brief Pain Inventory.
Physicians who wish to perform advanced neuromodulation procedures not only must meet the minimum qualifications deemed appropriate to provide safe and effective care but must also recognize that capturing a patient’s unique, physical, and emotional pain experience is complex. Given that pain is shaped by biochemical, psychosocial, and behavioral factors, a clinician must have the proper tools to optimize decision-making.75 The current ACGME program requirements mandate that fellows demonstrate competence in pain assessment, including patient pain measurement. Although numerical rating scales (NRS) or visual analog scales (VAS) have been used historically, these measures can lead to an unhealthy focus on pain scores alone. As a result, the NRS and VAS scales alone can underestimate pain reduction.76
Nearly every major consensus panel including the US Department of Health and Human Services (HHS), the National Institutes of Health (NIH) Research Task Force for Chronic Low Back Pain, the Institute of Medicine (IOM), and the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT) recommends a multidimensional approach toward patient-reported outcomes.19,77–79 It was suggested that using the Patient-Reported Outcomes Measurement Information System (PROMIS)-29 is preferred for studies investigating chronic low back pain.19,77–80 It was also concluded that legacy measures could be substituted if desired. There are several legacy indexes aspiring pain physicians should be familiar with, including the following: the Oswestry Disability Index (ODI), Roland Morris Disability Questionnaire, Brief Pain Inventory (BPI)-Pain Interference domain, the EuroQol Research Foundation five-dimension, the Health Utilities Index Mark 3 quality-adjusted life year (QALY) calculations, and the Short-Form McGill Pain Questionnaire. Thankfully, several studies validate the comparison between the above legacy indexes and the PROMIS-29. Many indexes measure relevant domains, including pain, mood, sleep, social participation, and function. These patient-reported outcome measures are helpful not only in the context of the clinical research trial but also clinically relevant to track patient progress and treatment efficacy, allowing the clinician to “alter the course of care” when necessary.75
Great care must be taken when choosing which “fit-for-purpose” outcome measurement to utilize, or else the physician can introduce a degree of detection bias and measurement inconsistency.81 Synthesizing the extent of the literature for chronic pain is burdensome due to the heterogeneity in outcome measures applied, even when the studies are similar. Common language is needed to decide which intervention is appropriate for a clinical scenario. These domains help the physician better understand a well-rounded picture of the patient in which therapy is utilized while keeping a common language that allows congruence among clinical trials and in clinical practice.
Consensus Statement 13: Pain fellows should be prepared to engage in ongoing education and research in neuromodulation, including attending conferences, staying up to date on emerging technologies and techniques, critically reading landmark literature, and participating in clinical trials.
Fellowship training is intended to bridge the gaps and provide master skills while receiving further mentorship. These experiences will help transition the trainee to independent practice and help coincide personal interests with future practice goals.82 Some factors associated with further training reside within the institutional parameters, while others are secondary to influences outside training. With the ever-changing landscape of interventional pain medicine, pain fellows are encouraged and required to stay current. This can be accomplished through the foundation of fellowship, mentorship, industry-sponsored cadaver training, and national conferences. It is recommended that trainees consider joining at least two pain societies that have a strong neuromodulation focus (Box 3). The foundation of interventional pain medicine should also include understanding landmark literature and current evidence in neuromodulation (Table 1).
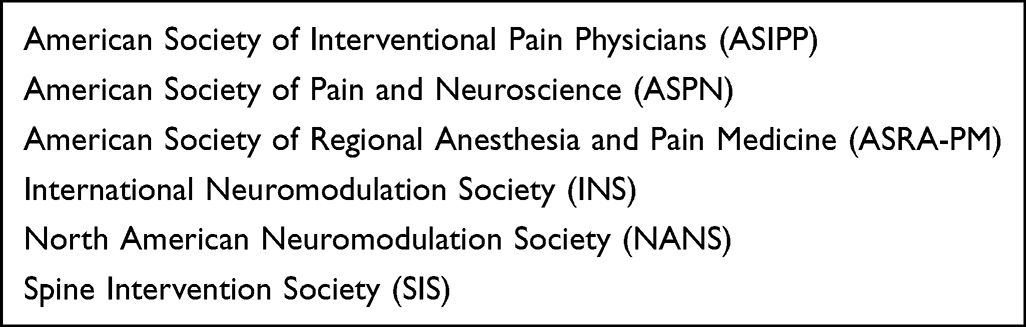 |
Box 3 Recommended Pain Societies with Neuromodulation Focus |
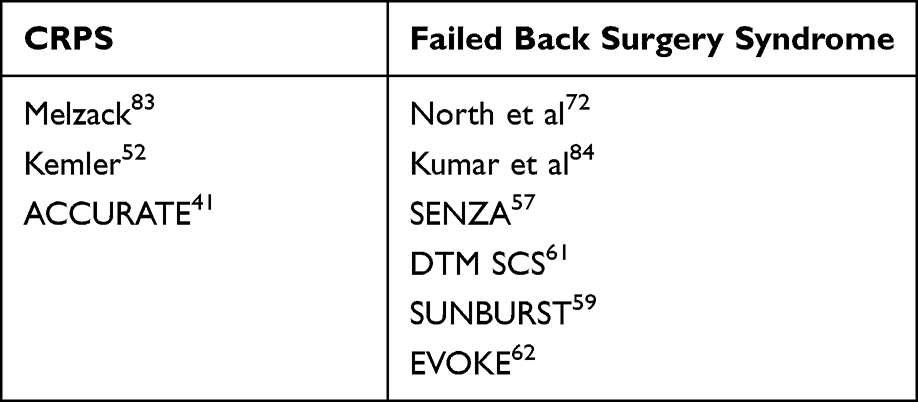 |
Table 1 Landmark Studies in Neuromodulation |
Cadaver training is supplemental to the ACGME Pain fellowship training, which about 77.5% of fellows attend in industry-sponsored workshops.38 Therefore, it is recommended that fellows attend at least three cadaver courses in the form of society-sponsored or industry-sponsored cadaver training courses during the fellowship. In addition, not all ACGME-accredited fellowships provide the surgical skills needed to implant a spinal cord stimulator device safely. In these scenarios, it is paramount for the pain fellow to attend cadaver training or seek additional practical instruction throughout the fellowship to ensure competency before graduation.
Discussion
Pain medicine is rapidly evolving, with neuromodulation techniques emerging as effective therapies for various pain syndromes. In this journal article, we summarize the key consensus points identified by the PEAK Consensus Committee regarding the essential knowledge and skills that pain fellows should acquire during their training in neuromodulation.
First and foremost, pain fellows should possess a strong foundation in pain medicine, encompassing an understanding of the pharmacology of opioid and non-opioid analgesics, multimodal pain management principles, and experience in evaluating and managing chronic pain patients. This comprehensive knowledge base forms the bedrock for effective patient care and optimizing pain management outcomes.
Additionally, pain fellows should develop a thorough understanding of the anatomical and physiological aspects relevant to neuromodulation. This includes a detailed grasp of the spinal cord, dorsal root ganglia, and peripheral nerves, as well as their intricate connections to the central and peripheral nervous systems. A robust comprehension of these structures and their pathophysiology enables pain fellows to accurately diagnose and target specific pain pathways for intervention.
Furthermore, pain fellows should receive comprehensive training in fluoroscopic and ultrasound-guided imaging techniques to accurately access this anatomy in a minimally invasive manner. Proficiency in radiation safety, identification of musculoskeletal and nervous structures, and precise needle localization are essential skills for successful neuromodulation procedures. This emphasis on imaging ensures the accurate and safe placement of leads and generators during SCS, DRG-S, and PNS implant procedures.
In conclusion, this article presents a concise summary of the PEAK Consensus Committee’s recommendations on the core competencies required for pain fellows in the field of neuromodulation. It highlights the importance of a strong foundation in pain medicine, a thorough understanding of relevant anatomy and physiology, proficiency in imaging techniques, selection and management of patients for neuromodulation therapies, technical expertise in device placement and troubleshooting, knowledge of adjunctive treatments, familiarity with different devices and potential complications, and a commitment to ongoing education and research. By adhering to these recommendations, pain fellows can become well-equipped practitioners capable of providing optimal care and improving patient outcomes in neuromodulation.
Acknowledgments
The American Society of Pain and Neuroscience (ASPN) would like to thank the PEAK Committee and its members for supporting this project and improving pain education worldwide.
Disclosure
Alaa Abd-Elsayed, MD, MPH, has had a financial agreement or affiliation with the following commercial interests in the form of Consultant: Medtronic, Curonix, Avanos, Averitas, SPR Therapeutics. Krishnan Chakravarthy, MD, PhD, has had a financial agreement or affiliation with the following commercial interests in the form of Consultant: Vertos Medical, Medtronic, Mainstay Medical; Stock Options: Neuronoff, Higgs Boson Health, Rune Labs; Owner: NXTSTIM INC., Accufix Medical. Kenneth B. Chapman, MD, has had a financial agreement or affiliation with the following commercial interest in the form of Research: Abbott. Sandy Christiansen, MD, has had a financial agreement or affiliation with the following commercial interest in the form of Research: Sorrento, GLG, Pacific Spine and Pain Society. Timothy R. Deer, MD, has had a financial agreement or affiliation with the following commercial interests in the form of Consultant: Abbott, Vertos, SpineThera, Saluda, Nalu, CornerLoc, Ethos, SPR Therapeutics, Medtronic, Boston Scientific, PainTEQ, Tissue Tech, Spinal Simplicity, Biotronik; Advisory Board: Biotronik, Abbott, Nalu, SPR Therapeutics, Tissue Tech; Stock Options: Vertos, SpineThera, Ethos, Saluda, Nalu, CornerLoc, SPR Therapeutics, PainTeq, Spinal Simplicity; Pending Patent: Abbott; Research: Abbott, Vertos, Saluda, Mainstay, SPR Therapeutics, Boston Scientific, PainTEQ, Avanos. Alexander Escobar, MD, has had a financial agreement or affiliation with the following commercial interests in the form of Consultant: Abbott, Boston Scientific Vertiflex, PainTEQ; Advisory Board: Medtronic, Nevro, Vertos Medical; Speaker’s Bureau: Medtronic, Nevro. Christopher J. Gilligan, MD, has had a financial agreement or affiliation with the following commercial interests in the form of consultant: Mainstay Medical, Saluda, Persica, Iliad Lifesciences. Johnathan H. Goree, MD, has had a financial agreement or affiliation with the following commercial interests in the form of Consultant: Abbott, Saluda Medical, Stratus Medical. Maged Guirguis, MD, has had a financial agreement or affiliation with the following commercial interests in the form of consultant: Nevro, Boston Scientific, Abbott, Avertis pharmaceutical, Saluda, Avanos, Omnia, SPR Therapeutics; Research: Nevro, Boston Scientific, Saluda, Avanos. Amitabh Gulati, MD, has had a financial agreement or affiliation with the following commercial interests in the form of Consultant: Medtronic, Inc., SPR Therapeutics, Nalu Medical, Averitas Medical; Advisory Board: AIS Healthcare, Hinge Health, Tersera Medical, Neurovasis. Jonathan M. Hagedorn, MD, has had a financial agreement or affiliation with the following commercial interests in the form of Consultant: Abbott, Boston Scientific, Nevro Corp, Saluda Medical. Jessica Jameson MD, FASA, has had a financial agreement or affiliation with the following commercial interests in the form of Research/Consultant: Nevro, Abbott, SPR, Vertos, SI Bone, Boston Scientific, Medtronic, Saluda Medical. Leonardo Kapural, MD, PhD, has had a financial agreement or affiliation with the following commercial interests in the form of Advisory Board: Avanos, Biotronik, Gimer, Medtronic, Neuralace, Neuros, PainTEQ, Nevro, Presidio; Research: Avanos, Neuros, Nevro, FUS Mobile, Nalu, Saluda. David W. Lee, MD, has had a financial agreement or affiliation with the following commercial interests in the form of Consultant: Abbott, Medtronic, Mainstay Medical, Biotronik, Boston Scientific, Petal Surgical. Michael S. Leong, MD, has had a financial agreement or affiliation with the following commercial interests in the form of Consultant: Sorrento Therapeutics; Research: Wex Pharmaceuticals. Timothy R. Lubenow, MD, has had a financial agreement or affiliation with the following commercial interests in the form of Consultant: Abbott, Boston Scientific, Nevro, Medtronic, PainTEQ, PenTec. Chris J. Mallard, MD, has had a financial agreement of affiliation with the following commercial interest in the form of consultant: Zavation. Melissa Z Murphy, MD, MPH, has had a financial agreement or affiliation with the following commercial interest in the form of Consultant: Medtronic, Relievant; Researcher: Medtronic; Advisor/Speaker: Medtronic. Kiran V. Patel, MD, has had a financial agreement or affiliation with the following commercial interest in the form of Consultant: Abbott Neuromodulation. Jason E. Pope, MD, has had a financial agreement or affiliation with the following commercial interest in the form of Consultant: Abbott, Medtronic, Saluda, Flowonix, SpineThera, Painteq, Vertos, Vertiflex, SPR Therapeutics, Tersera, Aurora, Spark, Ethos, Biotronik, Mainstay, WISE, Boston Scientific, Thermaquil; Grant/Research Support: Abbott, Flowonix, Saluda, Aurora, Painteq, Ethos, Muse, Boston Scientific, SPR Therapeutics, Mainstay, Vertos, AIS, Thermaquil; Shareholder: Painteq, Vertos, SPR Therapeutics, Aurora, Spark, Celeri Health, Neural Integrative Solutions (NIS), Pacific Research Institute, Saluda, Thermaquil and Anesthetic Gas Reclamation. In addition, he also has a patent Neuro monitoring DRG issued to NIS. Scott G. Pritzlaff, MD, CIPS, FIPP, has had a financial agreement or affiliation with the following commercial interest in the form of Consultant: Bioness, Bioventus, SPR Therapeutics, Nalu Medical, EBT Medical; Royalties: Oxford University Press, Wolters Kluwer; Research Grants; Medtronic, Nevro Corp, Abbott. Dawood Sayed, MD, has had an agreement or affiliation with the following commercial interests in the form of Consultant: PainTEQ, Saluda, Abbott, Nevro, Vertos, Surgentec. Samir J Sheth, MD has had a financial agreement or affiliation with the following commercial interest in the form of Consultant: Boston Scientific, Medtronic, Nevro, SPR Therapeutics, Vertos. Vinita Singh, MD, has no financial relationships to disclose. Tolga Suvar, MD, has had a financial agreement or affiliation with the following commercial interests in the form of Consultant: Nalu, Medtronic, Nevro. Chau M. Vu, MD, has had a financial agreement or affiliation with the following commercial interests in the form of Consultant/Research: Saluda Medical, PainTEQ. The authors report no other conflicts of interest in this work.
References
1. INS website. Available from: https://www.neuromodulation.com/about-neuromodulation.
2. Accreditation Council for Graduate Medical Education. ACGME program requirements for graduate medical education in pain medicine; 2022. Available from: https://www.acgme.org/globalassets/pfassets/programrequirements/530_painmedicine_2022.pdf.
3. World Health Organization. Safe surgery saves lives. Available from: https://www.who.int/teams/integrated-health-services/patient-safety/research/safe-surgery.
4. Committee W, Bass TA, Abbott JD, et al. 2023 ACC/AHA/SCAI advanced training statement on interventional cardiology (coronary, peripheral vascular, and structural heart interventions): a report of the ACC competency management committee. J Am Coll Cardiol. 2023;81(14):1386–1438. doi:10.1016/j.jacc.2022.11.002
5. Ahmed K, Khan R, Mottrie A, et al. Development of a standardised training curriculum for robotic surgery: a consensus statement from an international multidisciplinary group of experts. BJU Int. 2015;116(1):93–101. doi:10.1111/bju.12974
6. Awad M, Awad F, Carter F, et al. Consensus views on the optimum training curriculum for advanced minimally invasive surgery: a delphi study. Int J Surg. 2018;53:137–142. doi:10.1016/j.ijsu.2018.03.039
7. Deer TR, Russo MA, Grider JS, et al. The Neurostimulation Appropriateness Consensus Committee (NACC): recommendations for surgical technique for spinal cord stimulation. Neuromodulation. 2022;25(1):1–34. doi:10.1016/j.neurom.2021.10.015
8. Deer TR, Russo M, Grider JS, et al. The Neurostimulation Appropriateness Consensus Committee (NACC): recommendations on best practices for cervical neurostimulation. Neuromodulation. 2022;25(1):35–52. doi:10.1016/j.neurom.2021.10.013
9. Abd-Elsayed A, Abdallah R, Falowski S, et al. Development of an educational curriculum for spinal cord stimulation. Neuromodulation. 2020;23(5):555–561. doi:10.1111/ner.13142
10. Chaiban G, Abdallah RT, Abd-Elsayed A, et al. North American neuromodulation society educational curriculum for intrathecal drug delivery systems implantation and management. Neuromodulation. 2022;26(6):SS1094–2. doi:10.1016/j.neurom.2021.11.012
11. Kalia H, Abd-Elsayed A, Malinowski M, et al. Educational curriculum for peripheral nerve stimulation developed by the North American Neuromodulation Society. Neuromodulation. 2023;26(3):483–489. doi:10.1016/j.neurom.2022.09.015
12. Vardeh D, Mannion RJ, Woolf CJ. Toward a mechanism-based approach to pain diagnosis. J Pain. 2016;17(9 Suppl):T50–T69. doi:10.1016/j.jpain.2016.03.001
13. Vearrier D, Grundmann O. Clinical pharmacology, toxicity, and abuse potential of opioids. J Clin Pharmacol. 2021;61(Suppl 2):S70–S88. doi:10.1002/jcph.1923
14. Chou R, Turner JA, Devine EB, et al. The effectiveness and risks of long-term opioid therapy for chronic pain: a systematic review for a national institutes of health pathways to prevention workshop. Ann Intern Med. 2015;162(4):276–286. doi:10.7326/M14-2559
15. Scher C, Meador L, Van Cleave JH, Reid MC. Moving beyond pain as the fifth vital sign and patient satisfaction scores to improve pain care in the 21st century. Pain Manag Nurs. 2018;19(2):125–129. doi:10.1016/j.pmn.2017.10.010
16. Dowell D, Ragan KR, Jones CM, Baldwin GT, Chou R. CDC clinical practice guideline for prescribing opioids for pain - United States, 2022. MMWR Recomm Rep. 2022;71(3):1–95. doi:10.15585/mmwr.rr7103a1
17. Hayden JA, Ellis J, Ogilvie R, Malmivaara A, Van Tulder MW. Exercise therapy for chronic low back pain. Cochrane Back and Neck Group, ed. Cochrane Database Syst Rev. 2021;2021(10). doi:10.1002/14651858.CD009790.pub2
18. de Williams ACDC, Fisher E, Hearn L, et al. Psychological therapies for the management of chronic pain (excluding headache) in adults. Cochrane Database Syst Rev. 2020;8(8):CD007407. doi:10.1002/14651858.CD007407.pub4
19. Pain management best practices inter-agency task force report; 2018. Available from: https://www.hhs.gov/sites/default/files/pmtf-final-report-2019-05-23.pdf.
20. Deer TR, Mekhail N, Provenzano D, et al. The appropriate use of neurostimulation of the spinal cord and peripheral nervous system for the treatment of chronic pain and ischemic diseases: the neuromodulation appropriateness consensus committee: appropriate use of neurostimulation. Neuromodulation. 2014;17(6):515–550. doi:10.1111/ner.12208
21. Eldabe S, Buchser E, Duarte RV. Complications of spinal cord stimulation and peripheral nerve stimulation techniques: a review of the literature. Pain Med. 2016;17(2):325–336. doi:10.1093/pm/pnv025
22. Kumar K, Hunter G, Demeria D. Spinal cord stimulation in treatment of chronic benign pain: challenges in treatment planning and present status, a 22-year experience. Neurosurgery. 2006;58(3):481–496. doi:10.1227/01.NEU.0000192162.99567.96
23. North RB, Kidd DH, Farrokhi F, Piantadosi SA. Spinal cord stimulation versus repeated lumbosacral spine surgery for chronic pain: a randomized, controlled trial. Neurosurgery. 2005;56(1):98–106; discussion 106–107. doi:10.1227/01.neu.0000144839.65524.e0
24. Wang D. Image guidance technologies for interventional pain procedures: ultrasound, fluoroscopy, and CT. Curr Pain Headache Rep. 2018;22(1):6. doi:10.1007/s11916-018-0660-1
25. Centers of Disease Control and Prevention. ALARA – as low as reasonably achievable. Available from: https://www.cdc.gov/nceh/radiation/alara.html#:~:text=ALARA%20stands%20for%20“as%20low,time%2C%20distance%2C%20and%20shielding.
26. Miller DC, Patel J, Smith CC. Spine intervention society’s patient safety committee. Fact finders for patient safety: radiation safety for interventional spine procedures. Pain Med. 2018;19(3):629–630. doi:10.1093/pm/pnx302
27. Narouze SN. Atlas of Ultrasound-Guided Procedures in Interventional Pain Management. Springer; 2011.
28. Petraglia Iii FW, Farber SH, Gramer R, et al. The incidence of spinal cord injury in implantation of percutaneous and paddle electrodes for spinal cord stimulation. Neuromodulation. 2016;19(1):85–90. doi:10.1111/ner.12370
29. Kapural L, Jameson J, Johnson C, et al. Treatment of nonsurgical refractory back pain with high-frequency spinal cord stimulation at 10 kHz: 12-month results of a pragmatic, multicenter, randomized controlled trial. J Neurosurg Spine. 2022;37(2):188–199. doi:10.3171/2021.12.SPINE211301
30. Naidu RK, Chaturvedi R, Engle AM, et al. Interventional spine and pain procedure credentialing: guidelines from the American society of pain and neuroscience. JPR. 2021;14:2777–2791. doi:10.2147/JPR.S309705
31. Strand N, D’Souza RS, Hagedorn JM, et al. Evidence-based clinical guidelines from the American society of pain and neuroscience for the use of implantable peripheral nerve stimulation in the treatment of chronic pain. J Pain Res. 2022;15:2483–2504. doi:10.2147/JPR.S362204
32. Deer TR, Pope JE, Lamer TJ, et al. The neuromodulation appropriateness consensus committee on best practices for dorsal root ganglion stimulation. Neuromodulation. 2019;22(1):1–35. doi:10.1111/ner.12845
33. Bendersky D, Yampolsky C. Is spinal cord stimulation safe? A review of its complications. World Neurosurg. 2014;82(6):1359–1368. doi:10.1016/j.wneu.2013.06.012
34. Deer TR, Lamer TJ, Pope JE, et al. The Neurostimulation Appropriateness Consensus Committee (NACC) safety guidelines for the reduction of severe neurological injury: NACC NEUROLOGICAL SAFETY GUIDELINES. Neuromodulation. 2017;20(1):15–30. doi:10.1111/ner.12564
35. Deer TR, Provenzano DA, Hanes M, et al. The Neurostimulation Appropriateness Consensus Committee (NACC) recommendations for infection prevention and management. Neuromodulation. 2017;20(1):31–50. doi:10.1111/ner.12565
36. Meints SM, Edwards RR. Evaluating psychosocial contributions to chronic pain outcomes. Prog Neuropsychopharmacol Biol Psychiatry. 2018;87(Pt B):168–182. doi:10.1016/j.pnpbp.2018.01.017
37. Fanciullo GJ, Rose RJ, Lunt PG, Whalen PK, Ross E. The state of implantable pain therapies in the United States: a nationwide survey of academic teaching programs. Anesth Analg. 1999;88(6):1311–1316. doi:10.1097/00000539-199906000-00021
38. Pak DJ, Gruber J, Deer T, et al. Spinal cord stimulator education during pain fellowship: unmet training needs and factors that impact future practice. Reg Anesth Pain Med. 2019;44(3):407–414. doi:10.1136/rapm-2018-100065
39. Gharibo C, Laux G, Forzani BR, Sellars C, Kim E, Zou S. State of the field survey: spinal cord stimulator use by academic pain medicine practices. Pain Med. 2014;15(2):188–195. doi:10.1111/pme.12264
40. Henderson JM, Levy RM, Bedder MD, et al. NANS training requirements for spinal cord stimulation devices: selection, implantation, and follow-up. Neuromodulation. 2009;12(3):171–174. doi:10.1111/j.1525-1403.2009.00211.x
41. Deer TR, Levy RM, Kramer J, et al. Dorsal root ganglion stimulation yielded higher treatment success rate for complex regional pain syndrome and causalgia at 3 and 12 months: a randomized comparative trial. Pain. 2017;158(4):669–681. doi:10.1097/j.pain.0000000000000814
42. Martin SC, Macey AR, Raghu A, et al. Dorsal root ganglion stimulation for the treatment of chronic neuropathic knee pain. World Neurosurg. 2020;143:e303–e308. doi:10.1016/j.wneu.2020.07.102
43. Hunter CW, Yang A. Dorsal root ganglion stimulation for chronic pelvic pain: a case series and technical report on a novel lead configuration. Neuromodulation. 2019;22(1):87–95. doi:10.1111/ner.12801
44. Morgalla MH, Bolat A, Fortunato M, Lepski G, Chander BS. Dorsal root ganglion stimulation used for the treatment of chronic neuropathic pain in the groin: a Single-Center Study with long-term prospective results in 34 cases. Neuromodulation. 2017;20(8):753–760. doi:10.1111/ner.12713
45. Eldabe S, Burger K, Moser H, et al. Dorsal Root Ganglion (DRG) stimulation in the treatment of Phantom Limb Pain (PLP). Neuromodulation. 2015;18(7):610–616; discussion 616–617. doi:10.1111/ner.12338
46. Huygen FJPM, Kallewaard JW, Nijhuis H, et al. Effectiveness and safety of dorsal root ganglion stimulation for the treatment of chronic pain: a pooled analysis. Neuromodulation. 2020;23(2):213–221. doi:10.1111/ner.13074
47. Morgalla MH, Fortunato M, Lepski G, Chander BS. Dorsal Root Ganglion Stimulation (DRGS) for the treatment of chronic neuropathic pain: a Single-Center Study with long-term prospective results in 62 cases. Pain Physician. 2018;21(4):E377–E387. doi:10.36076/ppj.2018.4.E377
48. Chapman KB, Sayed D, Lamer T, et al. Best practices for dorsal root ganglion stimulation for chronic pain: guidelines from the American society of pain and neuroscience. JPR. 2023;16:839–879. doi:10.2147/JPR.S364370
49. Finnerup NB, Attal N, Haroutounian S, et al. Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. Lancet Neurol. 2015;14(2):162–173. doi:10.1016/S1474-4422(14)70251-0
50. Busse JW, Wang L, Kamaleldin M, et al. Opioids for chronic noncancer pain: a systematic review and meta-analysis. JAMA. 2018;320(23):2448–2460. doi:10.1001/jama.2018.18472
51. Paice JA, Bohlke K, Barton D, et al. Use of opioids for adults with pain from cancer or cancer treatment: ASCO guideline. JCO. 2023;41(4):914–930. doi:10.1200/JCO.22.02198
52. Kemler MA, Furnée CA. Economic evaluation of spinal cord stimulation for chronic reflex sympathetic dystrophy. Neurology. 2002;59(8):1203–1209. doi:10.1212/01.wnl.0000028686.74056.e3
53. IsHak WW, Wen RY, Naghdechi L, et al. Pain and depression: a systematic review. Harv Rev Psychiatry. 2018;26(6):352–363. doi:10.1097/HRP.0000000000000198
54. Hofmann SG, Asnaani A, Vonk IJJ, Sawyer AT, Fang A. The efficacy of cognitive behavioral therapy: a review of meta-analyses. Cogn Ther Res. 2012;36(5):427–440. doi:10.1007/s10608-012-9476-1
55. Goudman L, De Groote S, Linderoth B, et al. Exploration of the supraspinal hypotheses about spinal cord stimulation and dorsal root ganglion stimulation: a systematic review. JCM. 2021;10(13):2766. doi:10.3390/jcm10132766
56. Deer TR, Jain S, Hunter C, Chakravarthy K. Neurostimulation for intractable chronic pain. Brain Sci. 2019;9(2):23. doi:10.3390/brainsci9020023
57. Kapural L, Yu C, Doust MW, et al. Novel 10-kHz High-frequency Therapy (HF10 Therapy) is superior to traditional low-frequency spinal cord stimulation for the treatment of chronic back and leg pain: the SENZA-RCT randomized controlled trial. Anesthesiology. 2015;123(4):851–860. doi:10.1097/ALN.0000000000000774
58. De Ridder D, Plazier M, Kamerling N, Menovsky T, Vanneste S. Burst spinal cord stimulation for limb and back pain. World Neurosurg. 2013;80(5):642–649.e1. doi:10.1016/j.wneu.2013.01.040
59. Deer T, Slavin KV, Amirdelfan K, et al. Success using neuromodulation with BURST (SUNBURST) study: results from a prospective, randomized controlled trial using a novel burst waveform. Neuromodulation. 2018;21(1):56–66. doi:10.1111/ner.12698
60. Hatheway JA, Mangal V, Fishman MA, et al. Long-term efficacy of a novel spinal cord stimulation clinical workflow using kilohertz stimulation: twelve-month results from the Vectors Study. Neuromodulation. 2021;24(3):556–565. doi:10.1111/ner.13324
61. Fishman M, Cordner H, Justiz R, et al. Twelve-month results from multicenter, open-label, randomized controlled clinical trial comparing differential target multiplexed spinal cord stimulation and traditional spinal cord stimulation in subjects with chronic intractable back pain and leg pain. Pain Pract. 2021;21(8):912–923. doi:10.1111/papr.13066
62. Mekhail N, Levy RM, Deer TR, et al. Long-term safety and efficacy of closed-loop spinal cord stimulation to treat chronic back and leg pain (Evoke): a double-blind, randomised, controlled trial. Lancet Neurol. 2020;19(2):123–134. doi:10.1016/S1474-4422(19)30414-4
63. Wen YR, Shyu BC, Yang CT. O002 / #954 A NOVEL ULTRAHIGH FREQUENCY SCS REDUCES NEUROPATHIC PAIN AND BRAIN HYPERACTIVITIES IN THE RATS. Neuromodulation. 2022;25(7):S32–S33. doi:10.1016/j.neurom.2022.08.039
64. ClnicalTrials.gov. A prospective, multi-site, randomized, sham-controlled, double-blind trial with one-way crossover designed to assess the effectiveness and safety of the gimer NeuroBlock SCS trialing system for the treatment of chronic back pain and/or lower limb pain. Available from: https://clinicaltrials.gov/ct2/show/NCT04693650.
65. Deer TR, Pope JE, Falowski SM, et al. Clinical longevity of 106,462 rechargeable and primary cell spinal cord stimulators: real World Study in the medicare population. Neuromodulation. 2023;26(1):131–138. doi:10.1016/j.neurom.2022.04.046
66. Krames E, Poree L, Deer T, Levy R. Implementing the SAFE principles for the development of pain medicine therapeutic algorithms that include neuromodulation techniques. Neuromodulation. 2009;12(2):104–113. doi:10.1111/j.1525-1403.2009.00197.x
67. Scholz J, Finnerup NB, Attal N, et al. The IASP classification of chronic pain for ICD-11: chronic neuropathic pain. Pain. 2019;160(1):53–59. doi:10.1097/j.pain.0000000000001365
68. Haanpää M, Attal N, Backonja M, et al. NeuPSIG guidelines on neuropathic pain assessment. Pain. 2011;152(1):14–27. doi:10.1016/j.pain.2010.07.031
69. Harden RN, McCabe CS, Goebel A, et al. Complex regional pain syndrome: practical diagnostic and treatment guidelines, 5th edition. Pain Med. 2022;23(Suppl 1):S1–S53. doi:10.1093/pm/pnac046
70. Wang EJ, Berninger LE, Komargodski O, Smith TJ. Painful diabetic neuropathy - spinal cord stimulation, peripheral nerve stimulation, transcutaneous electrical nerve stimulation, and scrambler therapy: a narrative review. Pain Physician. 2022;25(8):E1163–E1173.
71. Kapural L, Peterson E, Provenzano DA, Staats P. Clinical evidence for spinal cord stimulation for Failed Back Surgery Syndrome (FBSS): systematic review. Spine. 2017;42(Suppl 14):S61–S66. doi:10.1097/BRS.0000000000002213
72. North RB, Kidd D, Shipley J, Taylor RS. Spinal cord stimulation versus reoperation for failed back surgery syndrome: a cost effectiveness and cost utility analysis based on a randomized, controlled trial. Neurosurgery. 2007;61(2):361–368; discussion 368–369. doi:10.1227/01.NEU.0000255522.42579.EA
73. Deer TR, Raso LJ. Spinal cord stimulation for refractory angina pectoris and peripheral vascular disease. Pain Physician. 2006;9(4):347–352.
74. Xu J, Sun Z, Wu J, et al. Peripheral nerve stimulation in pain management: a systematic review. Pain Physician. 2021;24(2):E131–E152.
75. Pope JE, Fishman MA, Gunn JA, Cotten BM, Hill MM, Deer TR. Cross-validation of the foundation pain index with PROMIS-29 in chronic pain patients. J Pain Res. 2021;14:2677–2685. doi:10.2147/JPR.S314021
76. Pope JE, Fishman M. Redefining success: longitudinal patient reported outcome measures and the importance of psychometric testing for optimization in neuromodulation. Neuromodulation. 2019;22(1):119–120. doi:10.1111/ner.12907
77. Pope JE, Fishman M, Chakravarthy K, et al. A retrospective, multicenter, quantitative analysis of patients’ baseline pain quality (PROMIS-29) entering into pain and spine practices in the United States (ALIGN). Pain Ther. 2021;10(1):539–550. doi:10.1007/s40122-021-00238-z
78. Deyo RA, Dworkin SF, Amtmann D, et al. Report of the NIH task force on research standards for chronic low back pain. J Pain. 2014;15(6):569–585. doi:10.1016/j.jpain.2014.03.005
79. Institute of Medicine (US) Committee on Advancing Pain Research, Care, and Education. Relieving pain in America: a blueprint for transforming prevention, care, education, and research. National Academies Press (US); 2011. Available from: http://www.ncbi.nlm.nih.gov/books/NBK91497/.
80. Herman PM, Edelen MO, Rodriguez A, Hilton LG, Hays RD. A protocol for chronic pain outcome measurement enhancement by linking PROMIS-29 scale to legacy measures and improving chronic pain stratification. BMC Musculoskelet Disord. 2020;21(1):671. doi:10.1186/s12891-020-03696-2
81. Chiarotto A, Terwee CB, Ostelo RW. Choosing the right outcome measurement instruments for patients with low back pain. Best Pract Res Clin Rheumatol. 2016;30(6):1003–1020. doi:10.1016/j.berh.2017.07.001
82. Grover BT, Kothari SN. Fellowship training: need and contributions. Surg Clin North Am. 2016;96(1):47–57. doi:10.1016/j.suc.2015.09.003
83. Melzack R and Wall PD. (1965). Pain Mechanisms: A New Theory. Sci, 150(3699), 971–979. 10.1126/science.150.3699.971
84. Kumar K, Taylor RS, Jacques L, et al. Spinal cord stimulation versus conventional medical management for neuropathic pain: a multicentre randomised controlled trial in patients with failed back surgery syndrome. Pain. 2007;132(1–2):179–188. doi:10.1016/j.pain.2007.07.028
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.