Back to Journals » Infection and Drug Resistance » Volume 19
Oxidative Stress, Glutathione System Activity, and Zinc/Selenium Imbalance in Adult Measles of Varying Severity According to Vaccination Status
Authors Matviiuk O ![]() , Pryshliak O, Boichuk O, Vaskul N, Ersteniuk A, Domina N
, Pryshliak O, Boichuk O, Vaskul N, Ersteniuk A, Domina N
Received 5 January 2026
Accepted for publication 20 March 2026
Published 3 April 2026 Volume 2026:19 589101
DOI https://doi.org/10.2147/IDR.S589101
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Oliver Planz
Olha Matviiuk,1 Oleksandra Pryshliak,1 Oleksandr Boichuk,1 Nadiia Vaskul,1 Anna Ersteniuk,2 Nataliia Domina3
1Department of Infectious Diseases and Epidemiology, Ivano-Frankivsk National Medical University, Ivano-Frankivsk, Ukraine; 2Center for Bioelementology, Ivano-Frankivsk National Medical University, Ivano-Frankivsk, Ukraine; 3Municipal Non-Commercial Enterprise “Center for Infectious Diseases”, Ivano-Frankivsk, Ukraine
Correspondence: Olha Matviiuk, Department of Infectious Diseases and Epidemiology, Ivano-Frankivsk National Medical University, Ivano-Frankivsk, Ukraine, Email [email protected]
Background: Adult measles is increasingly associated with severe clinical manifestations, particularly among unvaccinated individuals. Oxidative stress and micronutrient depletion may contribute to disease severity; however, integrated data evaluating oxidative protein damage, glutathione system activity, and zinc/selenium status in adult measles remain limited. This study assessed oxidative stress markers, glutathione-dependent enzymes, and trace element levels according to vaccination status.
Methods: Eighty adults with laboratory-confirmed measles were stratified into vaccinated (n=40) and unvaccinated (n=40) groups. Oxidative protein modification was quantified spectrophotometrically at 356, 370, 430, and 530 nm. GPx and GR activities were measured using standard assays. Serum zinc and selenium concentrations were determined by atomic absorption spectrophotometry. Statistical analyses included distribution testing, group comparisons with Holm correction, and standardized effect size estimation.
Results: Unvaccinated patients demonstrated higher protein carbonyl levels at 356 nm (1.474 ± 0.148 vs 1.266 ± 0.041; p=0.005) and 370 nm (p< 0.01), along with lower GR activity (0.048 ± 0.007 vs 0.061 ± 0.003; p=0.035). Effect size analysis showed a large between-group difference for GR activity (Hedges g≈0.89) and moderate effects for oxidative indices. Zinc levels were reduced by 24% in unvaccinated and 13% in vaccinated patients (78.7 ± 0.72 vs 89.5 ± 0.78 μg/dL; p< 0.001). Selenium levels were decreased by 55% and 49%, respectively (61.3 ± 0.49 vs 69.8 ± 0.56 μg/L; p< 0.001).
Conclusion: Adult measles was associated with oxidative protein modification, impaired glutathione system activity, and reduced zinc and selenium levels, particularly in unvaccinated patients. These findings are associative and require confirmation in prospective longitudinal studies.
Plain Language Summary: Measles remains a clinically significant viral infection in adults and can lead to severe complications, particularly in individuals who have not been vaccinated. In addition to its well-known symptoms, measles can disrupt the body’s antioxidant defenses and alter the balance of essential trace elements in the blood.
In this study, we compared vaccinated and unvaccinated adults hospitalized with measles. We examined laboratory markers of oxidative stress, including protein damage caused by excessive oxidative reactions, the activity of key antioxidant enzymes, and blood levels of zinc and selenium—two trace elements important for immune function.
We found that unvaccinated patients showed higher levels of oxidative stress and lower concentrations of zinc, selenium, and glutathione reductase activity than vaccinated patients. These biochemical changes were associated with a more severe course of the disease. Vaccinated individuals demonstrated a milder biochemical response, suggesting partial protection not only against infection but also against harmful oxidative processes.
These findings may contribute to understanding biochemical mechanisms linked to disease severity and suggest that certain laboratory markers could assist in early clinical assessment. Further prospective studies are needed to confirm these observations and clarify their potential clinical implications.
Keywords: measles, adults, vaccination status, oxidative stress, micronutrient imbalance, zinc, selenium, glutathione system
Introduction
Over the past decade, measles incidence has increased both globally and in Ukraine, affecting not only children but also a growing proportion of adults, largely due to declining vaccination coverage.1–6 Adult measles is frequently associated with a more severe clinical course, higher complication rates, and prolonged hospitalization, underscoring the need to identify early biochemical predictors of disease severity that may support clinical risk stratification and management.1–6
One of the key processes associated with viral infections is oxidative stress (OS), which arises from the excessive production of reactive oxygen species (ROS) during viral replication and inflammatory immune responses.7,8 When antioxidant defense mechanisms are overwhelmed, ROS contribute to cellular damage, activation of inflammatory cascades, and induction of apoptosis, thereby aggravating tissue injury and disease progression.7–9 Oxidative stress plays a central role in the pathogenesis of multiple viral infections, including influenza, COVID-19, respiratory syncytial virus infection, and other acute respiratory viral diseases.9–14 However, the contribution of oxidative imbalance to the clinical course of measles, particularly in adults, remains insufficiently studied.9 However, integrated data simultaneously evaluating oxidative protein modification, glutathione system activity, and trace element status in adult measles, particularly in relation to vaccination status, are lacking.
Protein oxidative modification is considered an early and sensitive marker of oxidative stress. Carbonyl derivatives formed during oxidative protein damage reflect irreversible structural changes that impair enzymatic activity, receptor function, and membrane integrity, ultimately affecting cellular metabolism and organ function.15–23 Monitoring oxidative protein modification, therefore, provides valuable insight into the severity of inflammatory and infectious processes and has been proposed as a laboratory indicator of tissue injury in critical conditions.17–22
In parallel, the acute phase response is associated with pronounced alterations in trace element metabolism. Zinc (Zn) and selenium (Se) play essential roles in immune regulation and antioxidant defense, serving as cofactors for enzymes of the glutathione system and other redox-regulating pathways.24–28 During systemic inflammation, redistribution of Zn and Se results in decreased serum concentrations, which may exacerbate oxidative stress, impair immune responses, and contribute to adverse clinical outcomes in infectious and critical illnesses.29–37
The Ivano-Frankivsk region belongs to a biogeochemical zone characterized by chronic deficiencies of several trace elements, including zinc and selenium, due to soil and water composition.38 Notably, this region experienced a high burden of measles during recent outbreaks, raising the possibility that pre-existing micronutrient imbalance may influence disease severity in adult patients.1–6,38 Despite accumulating evidence linking Zn and Se status to outcomes in acute infectious and inflammatory conditions, data specifically addressing their role in adult measles—particularly in relation to vaccination status—remain limited.29,30
Importantly, trace element deficiencies are not limited to specific regions but represent a global public health concern, particularly in populations with suboptimal nutritional status, which increases the broader relevance of these findings.
Vaccination against measles is well established as an effective measure for preventing infection and reducing disease severity.29 Beyond its role in adaptive immune protection, vaccination may also modulate the intensity of systemic inflammation and oxidative stress during infection, thereby influencing metabolic and redox homeostasis.29,37 However, the extent to which vaccination history affects oxidative stress markers, glutathione system activity, and trace element status in adults with measles has not been sufficiently explored.
Therefore, this study addresses an important gap by providing an integrated assessment of oxidative protein damage, glutathione system function, and micronutrient balance in adult measles patients stratified by vaccination status.
A graphical abstract summarizing the proposed pathogenic model of oxidative stress, glutathione system impairment, and Zn/Se imbalance in adult measles patients depending on vaccination status is providedin the Supplementary Materials.
Aim
This study aimed to assess the degree of oxidative protein modification, glutathione system activity, and zinc and selenium status in adult patients with measles, and to evaluate their association with disease severity according to vaccination history.
Materials and Methods
Study Design and Participants
This observational study included 80 adult patients with laboratory-confirmed measles who were hospitalized at the Center for Infectious Diseases of the Ivano-Frankivsk Regional Council, Ukraine. Patients were enrolled during the acute phase of the disease and stratified into two groups according to vaccination history: vaccinated (n=40) and unvaccinated (n=40). Vaccination status was confirmed by official immunization records (preventive vaccination cards, form No. 063/o). Patients with an undocumented vaccination history were classified as unvaccinated.
The study groups were comparable in terms of age, sex, and presence of comorbid conditions. All laboratory parameters were compared with internationally accepted reference values. Medical and diagnostic procedures were performed after obtaining written informed consent from all participants.
All biochemical measurements were performed according to standardized laboratory protocols routinely used in clinical biochemical research. Commercially available reagents and assay kits were used for all analyses in accordance with manufacturers’ instructions.
Serum zinc and selenium concentrations were determined by flame atomic absorption spectrophotometry using a Shimadzu AA-7000 series atomic absorption spectrophotometer (Model GFA-7000A; Shimadzu Corporation, Kyoto, Japan).
Calibration was performed for each analytical session using certified reference standard solutions within the working concentration range (0–20 ppb). Multi-point calibration curves were generated prior to sample analysis and verified for linearity before measurement.
For selenium, the calibration curve was constructed using linear regression analysis according to the equation: A = 0.00264 × C − 0.00446 (R² = 0.965).
For zinc, the corresponding regression equation was: A = 0.00479 × C − 0.00016 (R² = 0.990) where A represents absorbance and C represents element concentration (ppb). Sample concentrations were calculated by back-calculation from the respective regression equations. Instrument performance and analytical stability were monitored using internal quality control samples analyzed within each batch.
All biochemical assays were performed as single measurements in accordance with standardized protocols. Laboratory personnel conducting the biochemical analyses were blinded to patients’ vaccination status in order to minimize potential analytical bias.
Diagnostic Criteria
The diagnosis of measles was established based on epidemiological history, characteristic clinical manifestations, and laboratory confirmation. Specific IgM antibodies to measles virus were detected in serum samples using an enzyme-linked immunosorbent assay (ELISA). Diagnostic results were documented in standardized hospital medical records (form No. 003/o).
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki (1964–2013), International Council for Harmonisation Good Clinical Practice (ICH GCP, 1996), EEC Directive No. 609/86 (24 November 1986), and Order No. 690 of the Ministry of Health of Ukraine (23 September 2009). The study protocol was approved by the Local Ethics Committee of Ivano-Frankivsk National Medical University. All participants provided written informed consent before inclusion in the study.
Assessment of Oxidative Protein Modification
Oxidative modification of plasma proteins was assessed using spectrophotometric analysis based on the detection of carbonyl derivatives formed during oxidative damage. Protein carbonyl groups were quantified following derivatization with 2,4-dinitrophenylhydrazine (DNPH). Absorbance of the resulting hydrazones was measured at wavelengths of 356, 370, 430, and 530 nm, corresponding to early and late products of oxidative protein degradation. Oxidative protein modification was assessed spectrophotometrically by determining protein carbonyl derivatives at wavelengths of 356, 370, 430, and 530 nm using established methods.
The intensity of oxidative protein modification was expressed as optical density units per gram of protein or per milliliter of serum. Blood samples (0.05–0.1 mL) were centrifuged at 1500 rpm for 10 minutes to obtain serum. Serum samples were stored at −20 °C and were not subjected to repeated freeze–thaw cycles. Sample transportation and storage conditions complied with standard laboratory requirements.39
Assessment of Glutathione System Enzyme Activity
Glutathione reductase (GR) activity (nmol/min·mg protein) was determined by measuring the rate of NADPH oxidation spectrophotometrically at 340 nm. Glutathione peroxidase (GPx) activity (µmol/min·mg protein) was assessed by monitoring the rate of reduced glutathione (GSH) oxidation, based on changes in optical density at 270 nm during the enzymatic reaction.
Determination of Zinc and Selenium Concentrations
Serum zinc and selenium concentrations were determined by flame atomic absorption spectrophotometry using a Shimadzu AA-7000 series atomic absorption spectrophotometer (Model GFA-7000A; Shimadzu Corporation, Kyoto, Japan).
Calibration was performed for each analytical session using certified reference standard solutions. Multi-point calibration curves were generated prior to sample analysis within the working concentration range (0–20 ppb), and linearity was verified before measurements.
For selenium, the calibration curve was constructed using linear regression analysis according to the equation: A = 0.00264 × C − 0.00446 (R² = 0.965).
For zinc, the corresponding regression equation was: A = 0.00479 × C − 0.00016 (R² = 0.990) where A represents absorbance and C represents element concentration (ppb). Sample concentrations were calculated by back-calculation from the respective regression equations.
All measurements were performed under optimized analytical conditions according to the manufacturer’s technical specifications for each element (including wavelength, slit width, lamp current, and flame parameters). Instrument stability and analytical accuracy were monitored using internal quality control samples analyzed within each batch.
Laboratory personnel conducting biochemical analyses were blinded to patients’ vaccination status to minimize potential analytical bias.
Inclusion and Exclusion Criteria
Inclusion criteria were: age ≥18 years; clinical signs consistent with measles (fever, cough, coryza, conjunctivitis, oral enanthema, and characteristic exanthema); hospitalization within 1–5 days of disease onset; moderate or severe disease course; positive ELISA IgM test for measles virus; and absence of concurrent acute viral infections of other etiology.
Exclusion criteria included: hospitalization later than 6 days after disease onset; mild measles; negative ELISA results; and intake of dietary supplements or multivitamin preparations containing zinc or selenium within 3 months prior to enrollment.
Statistical Analysis
All data were recorded in standardized individual case report forms. Statistical analysis was performed using IBM SPSS Statistics software (version 28). Data distribution was assessed using the Shapiro–Wilk test. Normally distributed variables were compared using Welch’s t-test, while non-normally distributed data were analyzed using the Mann–Whitney U-test. Multiple comparisons were adjusted using Holm’s correction. Correlation analyses were conducted using Pearson’s or Spearman’s coefficients, as appropriate. A p-value <0.05 was considered statistically significant.
A sensitivity analysis was additionally performed to estimate the minimal detectable effect size given the study sample. With 40 participants per group, the study had 80% power to detect a standardized between-group difference of approximately Cohen’s d=0.63 at a two-sided α=0.05. Therefore, the study was adequately powered to detect moderate-to-large effects but may have been underpowered for small effect sizes. Standardized effect sizes (Hedges g with 95% confidence intervals) were calculated for all primary between-group comparisons.
Results
Clinical Characteristics of the Study Population
Patients were admitted to the Center for Infectious Diseases at a mean of 3.77 ± 0.11 days after disease onset. The age of enrolled participants ranged from 18 to 61 years, with a mean age of 27.59 ± 0.40 years. Overall, 54 patients (67.5%) were admitted by emergency medical services due to moderate or severe clinical conditions at presentation. A history of contact with individuals presenting catarrhal symptoms 10–14 days before disease onset was reported by 56 patients (70.0%).
In the vaccinated group (Group I), the mean age was 31.9 ± 2.02 years; 23 patients (57.5%) were male and 17 (42.5%) were female. Severe disease was documented in 2 patients (5.0%), moderate disease with complications in 25 patients (62.5%), and moderate disease without complications in 13 patients (32.5%). The most frequent complications included acute catarrhal non-obstructive bronchitis (62.5%) and reactive hepatitis (47.5%). Less frequent complications were viral-bacterial community-acquired pneumonia (2.5%), mild iron-deficiency anemia (7.5%), and bacterial conjunctivitis (5.0%). The mean length of hospital stay in this group was 8.74 ± 0.51 days.
In the unvaccinated group (Group II), the mean age was 28.6 ± 1.38 years; 21 patients (52.5%) were male, and 19 (47.5%) were female. Severe disease was observed in 9 patients (22.5%), while moderate disease with complications was recorded in 31 patients (77.5%). Complications were more frequent and included acute catarrhal non-obstructive bronchitis (60.0%), reactive hepatitis (65.0%), viral-bacterial community-acquired pneumonia (40.0%), mild to moderate iron-deficiency anemia (32.5%), otitis media (5.0%), pleurisy (5.0%), and bacterial conjunctivitis (15.0%). The mean duration of hospitalization in this group was longer than in vaccinated patients.
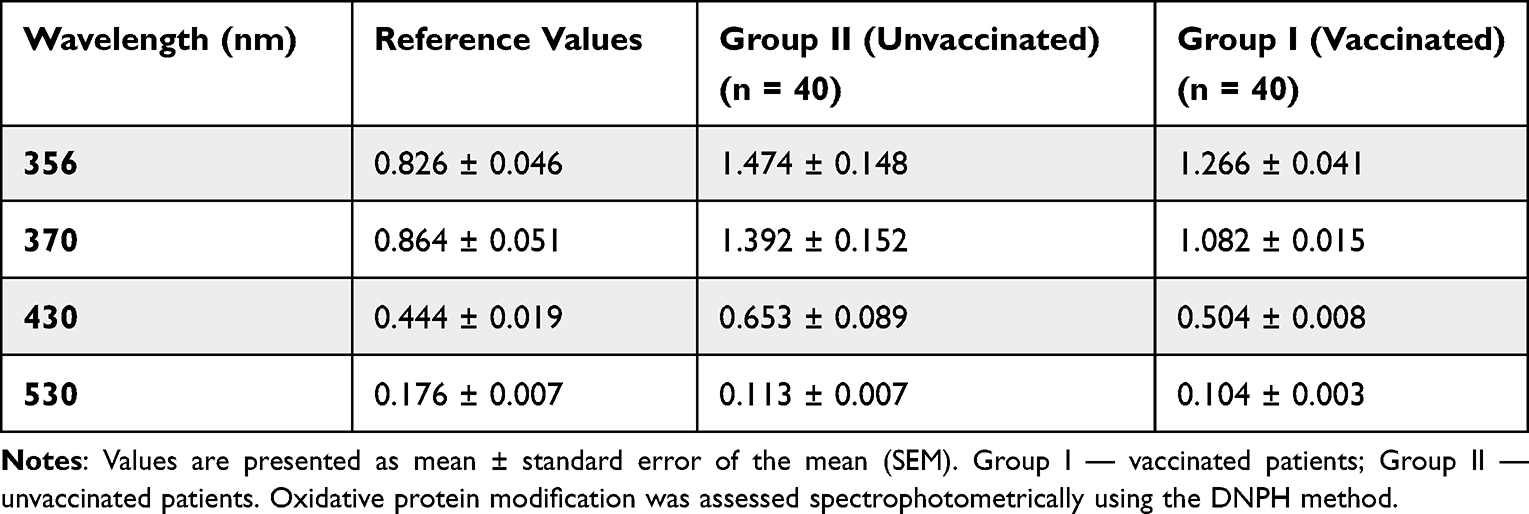 |
Table 1 Levels of Oxidative Protein Modification in Adult Patients with Measles at the Time of Hospital Admission (M ± SEM) (Arbitrary Units of Optical Density per mL of Serum) |
Oxidative Modification of Proteins
At the time of hospital admission, statistically significant differences in oxidative protein modification were observed between vaccinated and unvaccinated patients (Table 1 and Table 2). For all analyzed spectral ranges (356, 370, 430, and 530 nm), unvaccinated patients demonstrated higher levels of oxidative modification of proteins compared with reference values.
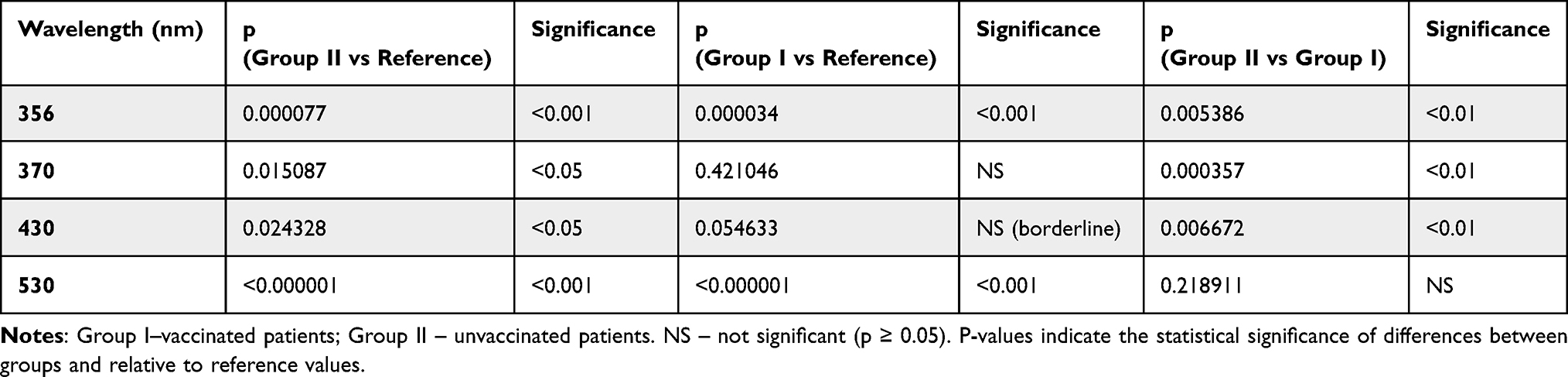 |
Table 2 Statistical Significance of Differences in Oxidative Protein Modification Parameters Between Study Groups (p-values for Intergroup and Reference Comparisons) |
At 356 nm, which reflects early products of oxidative protein damage, unvaccinated patients exhibited significantly higher values compared with both reference values (p < 0.001) and vaccinated patients (p < 0.01). At 370 nm, oxidative modification indices were also significantly increased in unvaccinated individuals relative to reference data (p < 0.01), whereas vaccinated patients demonstrated values close to the reference range.
At 430 nm, unvaccinated patients showed significantly elevated protein carbonyl levels compared with both reference values (p < 0.05) and vaccinated patients (p < 0.01). At 530 nm, oxidative modification indices in unvaccinated patients remained significantly higher than reference values (p < 0.001); however, no statistically significant difference was observed between vaccinated and unvaccinated groups at this wavelength (p > 0.2).
Overall, higher levels of oxidative protein modification at 356, 370, and 430 nm were consistently observed in unvaccinated patients at hospital admission (Figure 1).
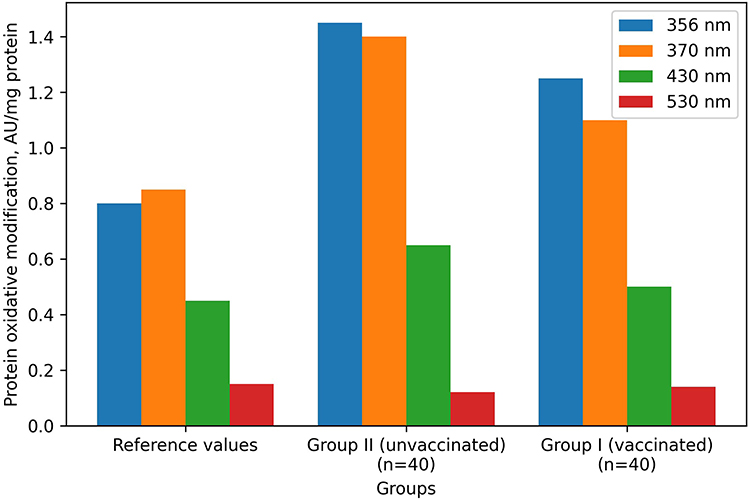 |
Figure 1 Level of oxidative modification of proteins in adult patients with measles at hospital admission depending on vaccination status (mean ± SEM). Protein oxidative modification was assessed at wavelengths of 356 nm, 370 nm, 430 nm, and 530 nm. Data are shown for reference values, unvaccinated patients (Group II, n=40), and vaccinated patients (Group I, n=40). |
Activity of Glutathione System Enzymes
Analysis of antioxidant enzyme activity revealed no statistically significant differences in glutathione peroxidase (GPx) activity between vaccinated and unvaccinated patients; values in both groups remained within the reference range (Table 3 and Table 4).
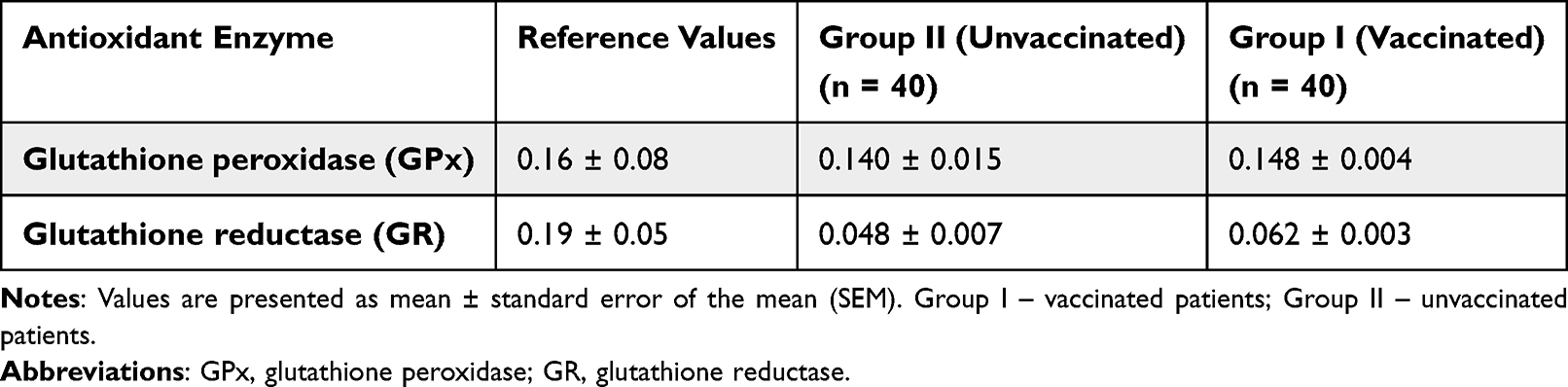 |
Table 3 Activity of Antioxidant Enzymes in Adult Patients with Measles (M ± SEM) (µmol/Min·mg Protein for GPx; nmol/Min·mg Protein for GR) |
 |
Table 4 Statistical Comparison of Antioxidant Enzyme Activity Between Study Groups and Reference Values |
In contrast, glutathione reductase (GR) activity was significantly reduced in both groups compared with reference values, with a more pronounced decrease observed in unvaccinated patients. GR activity was significantly lower in Group II compared with Group I (p < 0.05), indicating a greater degree of impairment of glutathione regeneration in unvaccinated individuals (Figure 2).
 |
Figure 2 Activity of antioxidant defense enzymes in adult patients with measles at hospital admission. Glutathione peroxidase and glutathione reductase activities are shown for reference values, vaccinated patients (Group I, n=40), and unvaccinated patients (Group II, n=40). Data are presented as mean ± SEM. |
Effect size analysis demonstrated a large between-group difference in GR activity (Hedges g=−0.89), a small-to-negligible effect for GPx activity (g=0.11), and moderate effects for selected oxidative protein modification indices (g ranging from −0.38 to −0.59). Effect size estimates for all between-group comparisons are presented in Supplementary Table S1. GR activity demonstrated a large effect size, whereas GPx showed a negligible effect. Oxidative protein modification indices demonstrated small-to-moderate effects.
Serum Zinc and Selenium Levels
Serum zinc concentrations were significantly lower in both vaccinated and unvaccinated patients compared with reference values (Table 5). A clear gradient was observed, with the lowest zinc levels detected in unvaccinated patients (Figure 3). Zinc concentrations in vaccinated patients were approximately 13% lower than reference values, whereas unvaccinated patients demonstrated a reduction of approximately 24%. The difference between the two groups was statistically significant (p < 0.001) (Table 6).
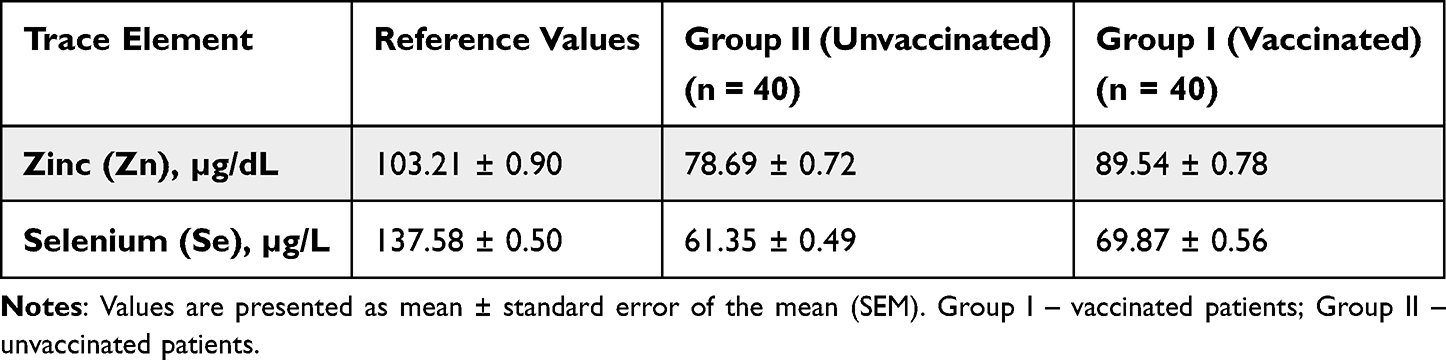 |
Table 5 Serum Zinc and Selenium Levels in Adult Patients with Measles at the Time of Hospital Admission (M ± SEM) |
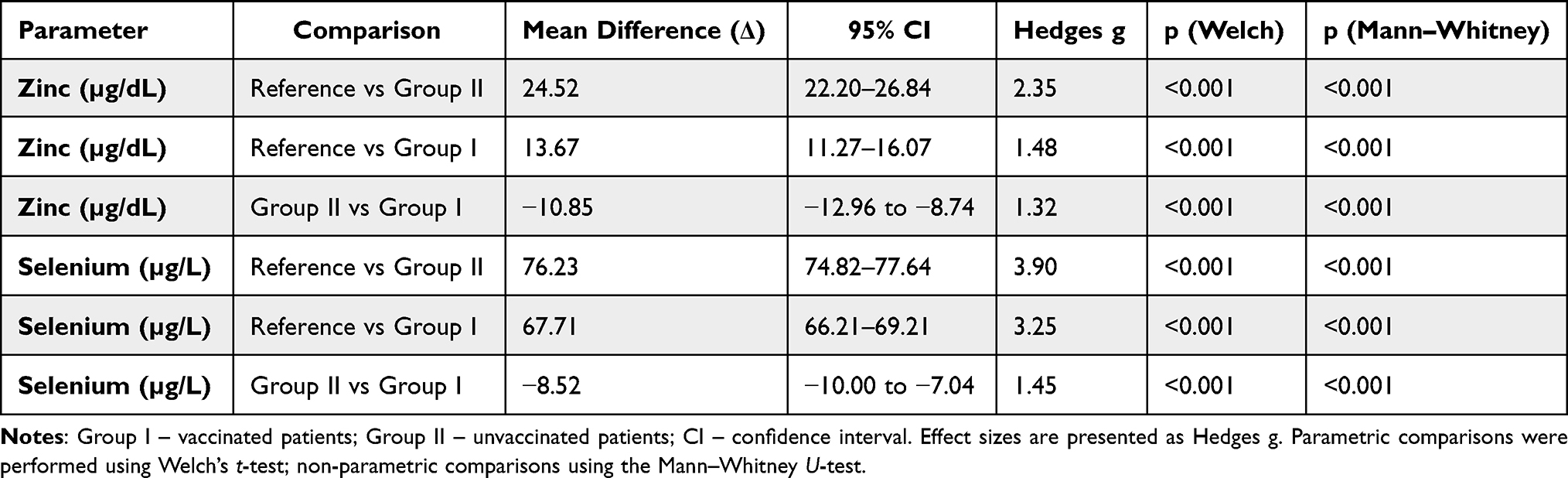 |
Table 6 Differences in Serum Zinc and Selenium Levels Between Study Groups and Reference Values |
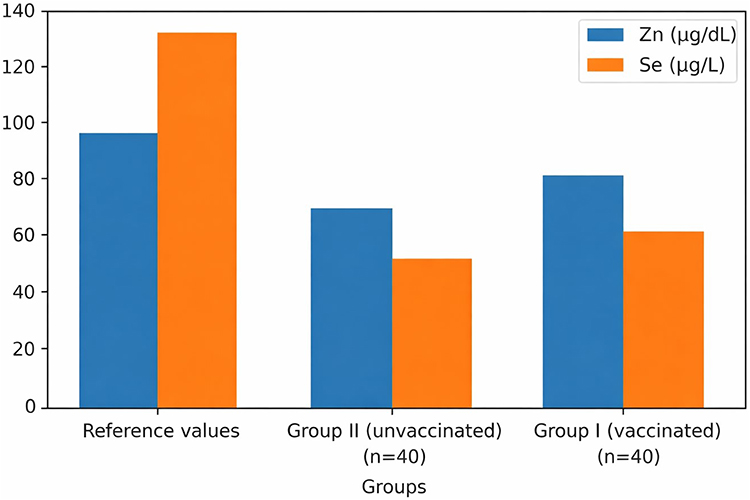 |
Figure 3 Serum zinc (Zn) and selenium (Se) levels in adult patients with measles at hospital admission. Data are shown for reference values, unvaccinated patients (Group II, n=40), and vaccinated patients (Group I, n=40). Values are expressed in μg/L and presented as mean ± SEM. |
Similarly, serum selenium concentrations were significantly reduced in both groups relative to reference values. Vaccinated patients exhibited a decrease of approximately 49%, while unvaccinated patients showed a reduction of approximately 55% (Figure 3). Selenium levels were significantly lower in unvaccinated patients compared with vaccinated individuals (p < 0.001) (Table 5 and Table 6).
Across all comparisons, differences in zinc and selenium concentrations between vaccinated and unvaccinated patients remained statistically significant after adjustment for multiple testing (Table 7).
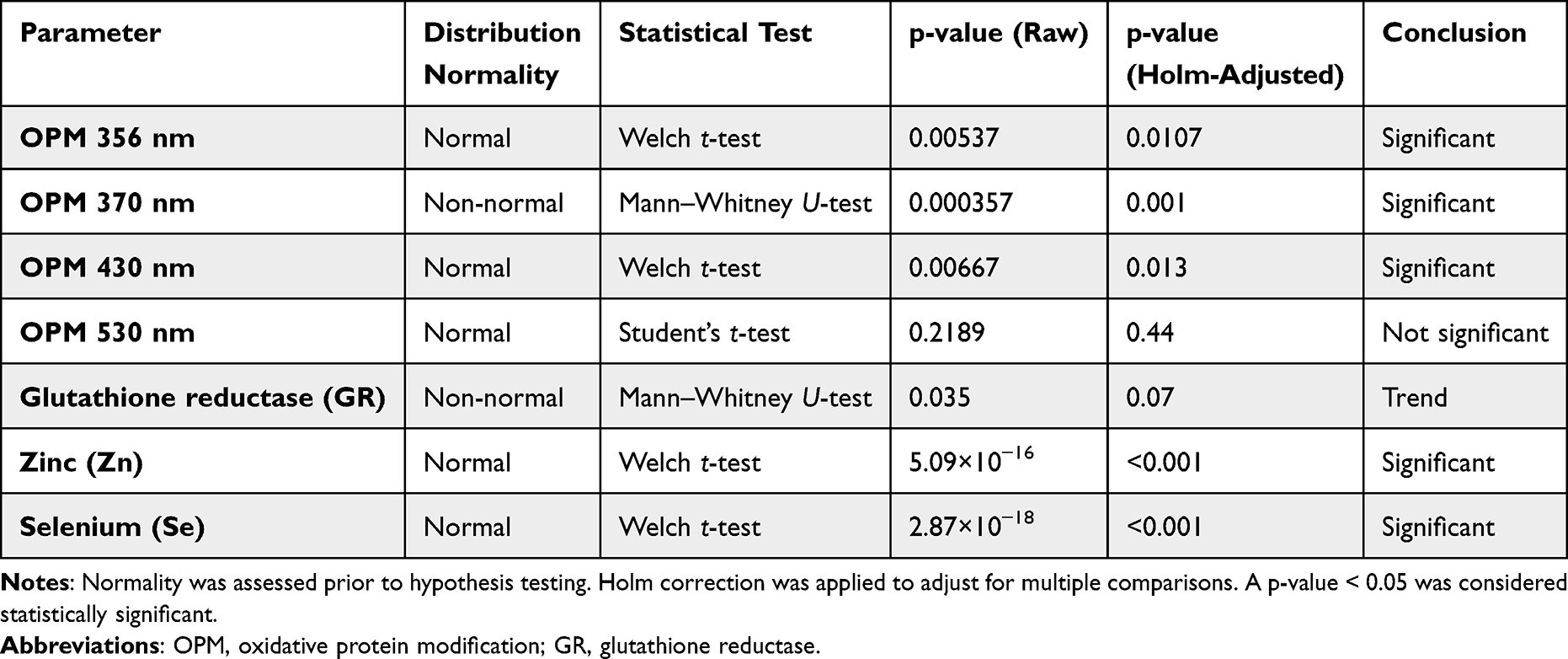 |
Table 7 Normality Assessment and Statistical Testing of Oxidative Stress Markers, Antioxidant Enzymes, and Trace Elements |
Discussion
This study provides a comprehensive biochemical characterization of adult measles, demonstrating that disease severity is closely associated with the intensity of oxidative stress, dysfunction of the glutathione antioxidant system, and disturbances in zinc and selenium homeostasis. Importantly, these alterations were consistently more pronounced in unvaccinated patients, indicating that vaccination status modifies not only the clinical course of measles but also the underlying biochemical response to infection (Conceptual schematic model Figure 4).
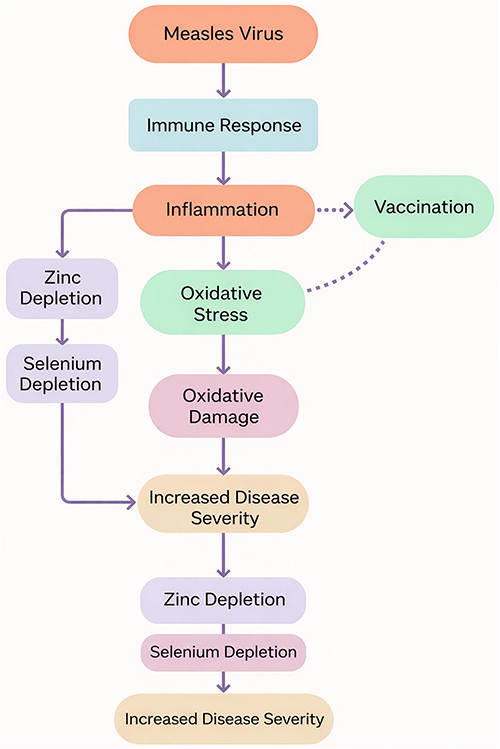 |
Figure 4 Conceptual model of oxidative stress and micronutrient imbalance in adult measles according to vaccination status. This schematic presents a conceptual model of the potential interactions between measles infection, inflammatory response, oxidative stress, zinc and selenium depletion, and clinical severity. The relationships shown are based on observed biochemical associations in the present study and existing literature and should be interpreted as hypothesis-generating rather than causal. |
The present analysis was based on biochemical assessments performed at a single time point during the acute phase of measles at hospital admission. Some oxidative modification indices demonstrated distributional asymmetry and variability differences between groups; therefore, effect estimates should be interpreted with caution and confirmed in larger cohorts. While this approach is appropriate for capturing early oxidative and micronutrient-related alterations associated with disease severity, it does not allow evaluation of temporal dynamics, recovery patterns, or causal relationships, which would require longitudinal follow-up.
Oxidative modification of proteins represents an early and irreversible consequence of excessive reactive oxygen species generation during viral infection. Elevated levels of protein carbonyl derivatives reflect structural damage to proteins, leading to impaired enzymatic activity, altered receptor signaling, and compromised membrane integrity.15–23 In the present study, unvaccinated patients exhibited significantly higher protein carbonyl levels, particularly at wavelengths corresponding to early oxidative damage (356 and 370 nm), indicating more intense oxidative protein degradation at the time of hospitalization. It should be noted that the assessment of protein carbonyl derivatives using the 2,4-dinitrophenylhydrazine (DNPH) method has certain methodological limitations. Classical acid-based protocols may overestimate carbonyl content due to incomplete removal of excess DNPH and potential interference, whereas modified neutral pH protocols improve the specificity and reproducibility of measurements.40–43 Similar mechanisms of oxidative injury have been described in other viral infections, including influenza, COVID-19, and respiratory syncytial virus infection.9–14 Our findings extend these observations to adult measles and highlight vaccination status as an important modifier of oxidative stress intensity.
The glutathione system is a central component of cellular antioxidant defense. While glutathione peroxidase activity remained largely preserved in both study groups during early hospitalization, glutathione reductase activity was significantly reduced, especially in unvaccinated patients. Glutathione reductase is essential for maintaining adequate levels of reduced glutathione, and its suppression limits the capacity of cells to neutralize reactive oxygen species, thereby amplifying oxidative stress.17,18,34 The observed pattern—preserved GPx activity with reduced GR activity—suggests early depletion of glutathione regeneration rather than primary failure of peroxide detoxification, a phenomenon previously described in systemic inflammatory and septic conditions.17,19–21
Trace element redistribution during acute infection represents a key component of the inflammatory response. In this study, both zinc and selenium concentrations were significantly reduced in adult patients with measles, with a clear gradient favoring vaccinated individuals. Hypozincemia during acute inflammation is largely mediated by interleukin-6–dependent upregulation of the hepatic ZIP14 transporter, resulting in rapid zinc sequestration in hepatocytes as part of the nutritional immunity response.29,31 Selenium depletion reflects reduced synthesis and secretion of selenoprotein P during systemic inflammation, redistribution of selenium to target tissues, and impaired hepatic function.30,32,33 These mechanisms are more pronounced in severe inflammatory states and have been associated with adverse outcomes in infectious and critical illnesses.33,34,44,45
Importantly, the observed reductions in serum zinc and selenium levels should be interpreted with caution. Given the absence of baseline micronutrient assessment and the known regional prevalence of trace element deficiency, it is not possible to fully distinguish infection-related acute-phase redistribution from pre-existing deficiency.
Zinc and selenium play complementary roles in immune regulation and redox balance.40,43 Zinc modulates innate and adaptive immune responses and regulates pro-inflammatory signaling pathways, including NF-κB activation.24,35–37 Selenium is an essential cofactor for selenoproteins such as glutathione peroxidases, which protect cells from oxidative damage and regulate inflammatory responses.25–27,32–34 The combined depletion of Zn and Se observed in unvaccinated patients may therefore exacerbate oxidative stress by simultaneously reducing antioxidant capacity and enhancing inflammatory signaling. This synergistic effect provides a plausible mechanistic explanation for the higher oxidative protein damage and more pronounced glutathione system impairment identified in this group.
The observed biochemical differences between vaccinated and unvaccinated patients expand the current understanding of the protective effects of measles vaccination. Beyond preventing infection or reducing viral replication, vaccination appears to attenuate the magnitude of systemic inflammation and oxidative stress, thereby limiting secondary metabolic and redox disturbances.29,37 This observation is consistent with epidemiological data demonstrating reduced complication rates and improved outcomes among vaccinated individuals and adds a mechanistic dimension to the concept of vaccine-mediated protection.
From a clinical perspective, the combination of elevated protein carbonyl levels, reduced glutathione reductase activity, and decreased serum zinc and selenium concentrations constitutes a coherent panel of early biochemical markers associated with disease severity. These parameters are measurable using routine laboratory techniques and may support early risk stratification in hospitalized adult patients with measles, particularly among unvaccinated individuals who appear more vulnerable to rapid oxidative and metabolic deterioration.
Several limitations of this study should be acknowledged. The single-center design and assessment of biochemical parameters at a single time point limit the evaluation of dynamic changes during disease progression and recovery. Cytokine profiling was not performed, which would have provided additional insight into inflammatory drivers of micronutrient redistribution and oxidative stress. In addition, baseline nutritional status was not assessed and may have influenced trace element levels. Nevertheless, the consistency and statistical robustness of the observed intergroup differences support the validity and clinical relevance of the findings.
These interpretations should be considered in light of the study limitations, including the observational design, absence of baseline micronutrient data, and lack of longitudinal follow-up.
Limitations
This study has several limitations that should be considered when interpreting the findings. First, the single-center, observational design limits the generalizability of the results to populations with different epidemiological, nutritional, or healthcare settings and precludes causal inference.
Second, baseline zinc and selenium status prior to measles infection was not assessed. Given the regional prevalence of micronutrient deficiencies, it is not possible to fully distinguish infection-related acute-phase redistribution from pre-existing deficiency.
Third, potential confounding factors such as detailed dietary intake, inflammatory cytokine profiles, and antioxidant supplementation history beyond predefined exclusion criteria were not systematically evaluated.
Finally, biochemical parameters were assessed at a single time point during the acute phase of disease, which does not allow evaluation of temporal dynamics, recovery patterns, or long-term associations. Longitudinal studies are required to confirm the persistence and clinical relevance of the observed biochemical alterations.
No formal a priori power calculation was performed, as the study was designed as an exploratory observational analysis. However, sensitivity analysis indicated adequate power to detect moderate-to-large between-group effects, whereas small effect sizes may have remained undetected. Nevertheless, the sample size was sufficient to detect moderate between-group differences across multiple independent biochemical parameters. These findings should be interpreted within the context of the study design and warrant confirmation in larger, prospective studies.
Conclusions
In conclusion, adult measles was associated with pronounced oxidative protein modification, impaired glutathione system activity, and reduced serum zinc and selenium levels, particularly among unvaccinated patients. Vaccination status was associated with a more favorable oxidative and micronutrient profile at hospital admission.
These biochemical alterations may reflect early pathophysiological processes related to disease severity; however, given the observational design and the absence of baseline and longitudinal data, causal inferences cannot be made. The identified markers should therefore be considered hypothesis-generating and warrant further investigation in larger, prospective studies with longitudinal follow-up.
The combined assessment of oxidative stress markers and micronutrient status may contribute to improved understanding of disease severity patterns and could potentially inform future risk stratification approaches pending further confirmation.
Novelty Statement
For the first time in Ukraine, a comprehensive clinical and laboratory study of adult patients with measles was conducted, comparing the degrees of oxidative stress, the intensity of oxidative modification of proteins, the activity of glutathione system enzymes, and the microelement balance (Zn, Se) depending on the vaccination status of patients. Our data show that vaccination against measles not only modifies the clinical course of the disease but also has a pronounced protective effect on the intensity of oxidative imbalance, reducing the levels of protein modification and the degree of depletion of antioxidant systems. The identified biochemical markers (Zn↓, Se↓, OMP↑, GR↓) form a new diagnostic panel for early prediction of the severity of measles and can be used in personalised approaches to patient management.
Clinical Implications
The results obtained indicate that simultaneous assessment of Zn and Se levels, protein oxidative modification indicators, and glutathione reductase activity at the time of hospitalisation may be useful for:
- Early risk stratification in adult patients with measles;
- Identifying patients who are at increased risk of complications and severe disease;
- Identifying a group of patients who require enhanced monitoring or correction of micronutrient imbalance;
- Developing personalised treatment strategies, especially in unvaccinated patients;
- Optimising the management of measles outbreaks among the adult population.
Zn, Se, GR and OMP markers can be considered as accessible early biomarkers of severity, which adds practical value to the study.
Strengths and Limitations
Strengths of the Study
- Comprehensive biochemical analysis covering several levels of oxidative stress: protein carbonylation, the enzymatic link of the glutathione system, and micronutrient status.
- Comparison by vaccination status, which allowed us to assess the protective effect of vaccination on the course of measles.
- Use of standardised methods of spectrophotometry and atomic absorption analysis.
- Clear inclusion/exclusion criteria, which reduces the risk of confounding factors.
- Homogeneity of the cohort in terms of age and comorbidities.
Limitations
- Lack of data on the dynamics of indicators at different stages (only the initial hospitalisation point).
- The study was conducted in a single centre, which may limit the generalisability of the results.
- Cytokine levels (IL-6, TNF-α) were not studied, which could further confirm the mechanisms of micronutrient redistribution.
- No analysis of nutritional status and past nutritional deficiencies.
- Some of the 2,4-DNFG methods have potential variability characteristic of the classic protocol.
Data Sharing Statement
All data used in this study are stored on secure servers at Ivano-Frankivsk National Medical University. A set of anonymised data is available upon reasonable request to the corresponding author for scientific or educational use. The data are not publicly available due to confidentiality and medical privacy requirements.
Ethical Approval Statement
The study was conducted in accordance with the Helsinki Declaration (1964–2013), ICH GCP (1996), EEC Directive No. 609/86, and Order No. 690 of the Ministry of Health of Ukraine dated 23 September 2009.
The study protocol was reviewed and approved by the Local Ethics Committee of Ivano-Frankivsk National Medical University (protocol No. 111/19 dated 19 November 2019). All patients provided written informed consent to participate in the study and to the processing of their personal data.
Author Contributions
All authors made a substantial contribution to the work; participated in drafting or critically revising the article; approved the final version for publication; agreed on the journal to which the manuscript was submitted; and accept responsibility for all aspects of the work.
Funding
The research was conducted without external funding. Laboratory analyses were performed at Ivano-Frankivsk National Medical University, the Centre for Bioelementology of IFNMU, and the Centre for Infectious Diseases as part of routine medical and diagnostic work.
Disclosure
The authors declare that there is no conflicts of interest regarding the materials presented in the article.
References
1. Ducomble T, Gignoux E. Learning from a massive epidemic: measles in DRC. Lancet Infect Dis. 2020;20(5):542. doi:10.1016/S1473-3099(20)30265-6
2. Mathis AD, Raines K, Filardo TD, et al. Measles update — US, 2025. MMWR Morb Mortal Wkly Rep. 2025;74(14):232–16. doi:10.15585/mmwr.mm7414a1
3. Pryshliak OY, Dykyi BM, Matviiuk OY, et al. Peculiarities of measles in adults in the Ivano-Frankivsk region. Wiad Lek. 2020;73(4):782–785. doi:10.36740/WLek202004130
4. Matviiuk OY. Hematological markers in adult measles. Buk Med Herald. 2024;28(4):53–60. doi:10.24061/2413-0737.28.4.112.2024.9
5. Pryshliak O, Matviiuk O, Boichuk O, Nedostup U. Measles course and RNA-based medicine. Pharma Innov J. 2022;11(10):147–150. doi:10.22271/tpi.2022.v11.i10b.16893
6. Hryzhak I, Pryshliak O, Gryb V, et al. Subacute sclerosing encephalitis in adult with HIV. Prague Med Rep. 2025;126(2):86–91. doi:10.14712/23362936.2025.14
7. Valko M, Leibfritz D, Moncol J, Cronin MT, Mazur M, Telser J. Free radicals and antioxidants in normal physiological functions and human disease. Int J Biochem Cell Biol. 2007;39(1):44–84. doi:10.1016/j.biocel.2006.07.001
8. Sies H. Oxidative stress: a concept in redox biology and medicine. Redox Biol. 2015;4:180–183. doi:10.1016/j.redox.2015.01.002
9. Erel O, Erdoğan S. Thiol-disulfide homeostasis as a marker of oxidative stress in patients with measles. Turk J Med Sci. 2020;50(Suppl 2):1728–1738. doi:10.3906/sag-2004-53
10. Delgado-Roche L, Mesta F. Oxidative stress as key player in SARS-CoV infection. Arch Med Res. 2020;51(5):384–387. doi:10.1016/j.arcmed.2020.04.015
11. Cecchini R, Cecchini AL. SARS-CoV-2 infection pathogenesis is related to oxidative stress as a response to aggression. Med Hypotheses. 2020;143:110102. doi:10.1016/j.mehy.2020.110102
12. Moskaliuk V, Pudyak K, Balaniuk I, et al. Hemostasis and inflammation in COVID-19. Med Perspekt. 2025;30(3):59–67. doi:10.26641/2307-0404.2025.3.340589
13. Karkhanei B, Pincemail J, van Eijk L, et al. Redox collapse in COVID-19. Redox Exp Med. 2022;1:1–15. doi:10.1016/j.redox.2022.102465
14. Yang X, Liu X, Nie Y, Zhan F, Zhu B. Oxidative stress in RSV infection. Virol J. 2023;20(1):224. doi:10.1186/s12985-023-02189-4
15. Santus P, Danzo F, Zuffi A, et al. Oxidative stress and viral infections: rationale, experiences, and perspectives on N-acetylcysteine. Eur Rev Med Pharmacol Sci. 2022;26(22):8582–8590. doi:10.26355/eurrev_202211_30395
16. Kurutas EB. The importance of antioxidants in the cellular response against oxidative/nitrosative stress. Nutr J. 2016;15(1):71. doi:10.1186/s12937-016-0186-5
17. Galley HF. Oxidative stress and mitochondrial dysfunction in sepsis. Br J Anaesth. 2011;107(1):57–64. doi:10.1093/bja/aer093
18. Litvinets YEA, Balabanyk VR. Dynamics of oxidative modification of plasma proteins in acute epididymitis. Ukr Sci Pract J Urol Androl Nephrol. 2018;3:65–70.
19. Andrades ME, Ritter C, Moreira JC, Dal-Pizzol F. Oxidative parameters in non-lethal and lethal sepsis. J Surg Res. 2005;123(2):254–260. doi:10.1016/j.jss.2004.07.251
20. Lin Y, Alhaskawi A, Chen L, et al. Recent advances in understanding oxidative stress in sepsis: pathogenic roles and antioxidant therapeutic prospects. Front Pharmacol. 2025;16:1695992. doi:10.3389/fphar.2025.1695992
21. Yang XR, Wen R, Yang N, et al. Role of oxidative stress in sepsis: mechanisms, pathways, and therapeutic strategies. J Pharm Anal. 2025:101452. doi:10.1016/j.jpha.2025.101452
22. Lushchak VI. Free radicals, reactive oxygen species and oxidative stress classification. Chem Biol Interact. 2014;224:164–175. doi:10.1016/j.cbi.2014.10.016
23. Dalle-Donne I, Rossi R, Colombo R, Giustarini D, Milzani A. Protein carbonyl groups as biomarkers of oxidative stress. Clin Chim Acta. 2003;329(1–2):23–38. doi:10.1016/S0009-8981(03)00003-2
24. Prasad AS. Zinc in human health: effect on immune cells. Mol Med. 2008;14(5–6):353–357. doi:10.2119/2008-00033.Prasad
25. Huang Z, Rose AH, Hoffmann PR. Selenium in inflammation and immunity. Antioxid Redox Signal. 2012;16(7):705–743. doi:10.1089/ars.2011.4145
26. Steinbrenner H, Speckmann B, Sies H. Understanding selenium in cancer prevention. Antioxid Redox Signal. 2013;19(2):181–191. doi:10.1089/ars.2012.4600
27. Nelson HK, Shi Q, Van Dael P, et al. Nutritional selenium and influenza mutations. FASEB J. 2001;15(10):1846–1848. doi:10.1096/fj.00-0872fje
28. Li Z, Xu X, Leng X, et al. Reactive oxygen species in viral infections. Int J Mol Sci. 2021;23(1):119. doi:10.3390/ijms23010119
29. Leung J, Munir NA, Mathis AD, et al. Vaccination status and measles severity in the US, 2001–2022. Clin Infect Dis. 2025;80(3):663–672. doi:10.1093/cid/ciae470
30. Cemek M, Dede S, Bayiroğlu F, et al. Oxidant and non-enzymatic antioxidant status in measles. J Trop Pediatr. 2007;53(2):83–86. doi:10.1093/tropej/fml068
31. Liuzzi JP, Lichten LA, Rivera S, et al. IL-6 regulates zinc transporter Zip14. Proc Natl Acad Sci U S A. 2005;102(19):6843–6848. doi:10.1073/pnas.0502257102
32. Sherlock LG, Polewski MD, Lahner E, et al. Endotoxemia reduces selenoenzymes. Front Immunol. 2020;11:595282. doi:10.3389/fimmu.2020.595282
33. Braunstein M, Kusmenkov T, Zuck C, et al. Selenium deficiency and trauma outcome. Shock. 2020;53(1):63–70. doi:10.1097/SHK.0000000000001344
34. Bierl C, Voetsch B, Jin RC, Handy DE, Loscalzo J. Determinants of plasma GPx-3. J Biol Chem. 2004;279(25):26839–26845. doi:10.1074/jbc.M401907200
35. Prasad AS. Zinc: immunity and inflammation. Curr Opin Clin Nutr Metab Care. 2009;12(6):646–652. doi:10.1097/MCO.0b013e3283312956
36. Prasad AS, Bao B. Zinc as antioxidant mediator. Antioxidants. 2019;8(8):164. doi:10.3390/antiox8080164
37. Wessels I, Haase H, Rink L. Zinc as gatekeeper of immune function. Nutrients. 2017;9(12):1286. doi:10.3390/nu9121286
38. Івано-Франківська обласна державна адміністрація. Звіт про стратегічну екологічну оцінку Програми економічного і соціального розвитку Івано-Франківської області на 2024 рік. Івано-Франківськ; 2024. Ukrainian. Available from: https://www.if.gov.ua/storage/app/sites/24/documentu-2024/Zvit%20SEO%20proektu%20prohramy%20ekonomichnoho%20ta%20sotsial%CA%B9noho%20rozvytku%20Iv-Fr.%20oblasti%20na%202024%20rik-2.docx.
39. Ukrainian Blood Service. Rules for storage of blood components. Available from: https://bloodservice.org.ua/likarnyanij-bank-krovi/pravila-zberigannya-komponentiv-ta-pr.html.
40. Mohammadi H, Asadi S, Nilashi M, et al. Zinc supplementation meta-analysis. J Trace Elem Med Biol. 2021;67:126789. doi:10.1016/j.jtemb.2021.126789
41. Georgiou CD, Zisimopoulos D, Argyropoulou V, et al. Carbonyl assay using DNPH. Redox Biol. 2018;17:128–142. doi:10.1016/j.redox.2018.04.010
42. Weber D, Davies MJ, Grune T. Determination of protein carbonyls. Redox Biol. 2015;5:367–380. doi:10.1016/j.redox.2015.06.005
43. Mahmoodpoor A, Shadvar K, Ghamari AA, et al. Selenium supplementation review. SN Appl Sci. 2022;4:173. doi:10.1007/s42452-022-05208-4
44. Alexander J, Colzani R, Ferrari P, et al. Circulating GPx-3 in elderly. Antioxidants. 2024;13(4):680. doi:10.3390/antiox13040680
45. Júnior EL, Leite HP, Konstantyner T, et al. Selenium and endothelial activation. Clin Nutr ESPEN. 2022;47:223–229. doi:10.1016/j.clnesp.2021.12.017
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Relationship Between Plasma Selenium, Antioxidant Status, Inflammatory Responses and Ischemic Cardiomyopathy: A Case-Control Study Based on Matched Propensity Scores
Luo Y, He X, Hu L, Zhao J, Su K, Lei Y, Li Y
Journal of Inflammation Research 2022, 15:5757-5765
Published Date: 10 October 2022
The Association Between Psoriasis and Trace Element Serum Levels and Dietary Intake: Results from USA National Health and Nutrition Examination Survey 2011–2014
Ding RL, Fu C, Zheng Y, Bu J, Shen EX
Clinical, Cosmetic and Investigational Dermatology 2024, 17:1449-1458
Published Date: 18 June 2024
Study on the Effects of Cadmium Exposure on Zinc Metabolism and FOXO3a Expression in the Preeclampsia Maternal-Fetal System
Ding A, Cao Y, Li F, Yang Q, Zhou D, Dong X
International Journal of Women's Health 2025, 17:2551-2559
Published Date: 15 August 2025