Back to Journals » Advances in Medical Education and Practice » Volume 13
Orientation of Healthcare Educators Towards Using an Effective Medical Simulation-Based Learning: A Q-Methodology Study
Authors Alotaibi FZ ![]() , Agha S, Masuadi E
, Agha S, Masuadi E ![]()
Received 19 February 2022
Accepted for publication 29 April 2022
Published 13 May 2022 Volume 2022:13 Pages 507—519
DOI https://doi.org/10.2147/AMEP.S363187
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Feras Zeyad Alotaibi,1– 3 Sajida Agha,1,2 Emad Masuadi1,2
1Department of Medical Education, College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 2King Abdullah International Medical Research Centre, Riyadh, Saudi Arabia; 3Excellence Center for Simulation and Medical Education, Emergency Department, Prince Sultan Military Medical City, Riyadh, Saudi Arabia
Correspondence: Feras Zeyad Alotaibi, Department of Medical Education, College of Medicine, King Saud bin Abdulaziz University for Health Sciences, P. O. Box 3660, Riyadh 11481, Internal Mail Code 3118, Riyadh, Saudi Arabia, Tel +966597-555462, Email [email protected]
Purpose: This study explores the healthcare educators’ orientations about medical simulation in clinical skills training —its benefits, needs, challenges, and implications for proper implementation and integration into curricula.
Methods: The study used a Q-sort technique, allowing quantitative and qualitative representation of the participants’ orientations and was conducted at King Saud bin Abdulaziz University for Health Sciences in Riyadh, Saudi Arabia. A total of 22 healthcare educators from different roles were included. Participants pre-sorted into three categories and then ranked statements related to medical simulation, by level of agreement, and they answered open-ended and demographic questions. Data was uploaded to Ken-Q Analysis application to conduct Q-factor analysis.
Results: A total of 22 healthcare educators participated in the study. Q-factor analysis was performed with principal component analysis and varimax rotation, identifying three factors. Most educators shared a similar orientation regarding the benefits of using simulation-based learning. Most participants considered medical simulation a simple, effortless, and beneficial method of learning. However, challenges in scheduling sessions and obtaining the necessary resources, such as human resources and funds, and lack of training had a negative impact on some participants’ motivation to use medical simulation.
Conclusion: Healthcare educators shed light on the influence of multiple factors on using medical simulation. The possibility for students to learn practical and clinical skills was a leading factor. Financial resources, funds, and faculty training were identified as challenges and needs. It is important for institutions and leaders to be aware of the variations in faculty perceptions and to provide resources and training to improve the current use of medical simulation.
Keywords: medical education, by-person factor analysis, simulation-based training, educators’ perception, Q-sort study
Introduction
Simulation is a practical methodology for creating a learning-by-imitation experience modeled after real-life scenarios. Simulation-based learning has been widely used, examined, and studied for over six decades in many professional fields like management, engineering, nursing, and medicine.1 It was first introduced in aviation by Edwin Link’s invention in 1929 of the first flight simulator, which was named the “Blue Box”.2,3
In medicine and education, medical simulation—with models and computerized manikins that look like the human body —is commonly used to train and educate healthcare providers and students.4 In ancient times, medical simulation models originated with the use of clay and stones. In the 18th century, an obstetrical manikin of a human pelvis and a dead infant allowed obstetricians to teach delivery on simulators, lowering mortality rates.5
Simulation-based medical education provides a safe, controlled environment, where problem-based learning can prosper, and interprofessional competencies are examined.6 In addition, simulation helps in the practice and sharpening of procedural, diagnostic, and communication skills, and the development of self-confidence.7 Simulation-based learning has been proven to be beneficial in many studies among undergraduate medical students. For example, Agha8 investigated the effectiveness of simulation-based learning for medical students and concluded that it is a helpful and successful learning approach. Moreover, it is a useful learning tool from the perspective of not only educators but also students.7 In Poland, a survey of undergraduate satisfaction with the use of high-fidelity simulations in a nephrology course found that it improved their clinical reasoning and decision-making skills.9 However, in Saudi Arabia, the orientation of healthcare educators in using effective simulation-based learning has not been examined substantially.
Simulation is increasingly being used in medical education to teach individuals and groups cognitive, psychomotor, and affective skills. It is imperative first to determine the outcomes of using medical simulation and examine the challenges and needs seen by the educators, using it as a learning method, to achieve a fruitful integration into the curriculum. There are many simulation centers in Saudi Arabia, but most are not fully exploited for medical simulation. Previous studies have reported that effective use of medical simulation contributes to improving patients’ safety.10 While literature presents several challenges in the use of simulation, one of the main challenges of simulation-based medical education is the educator’s lack of experience in simulation teaching strategies.11 Therefore, this study aims to contribute to the integration of medical simulation into health professions education programs through the orientation of healthcare educators. Using Q-sort method to capture subjective views, this study therefore explores the healthcare educators’ orientations about medical simulation in clinical skills training —its benefits, needs, challenges, and implications for proper implementation and integration into curricula.
Materials and Methods
General Overview of Q Methodology
Q-methodology (Q-sort) has been used in academic psychology, communication, political science, and behavioral and health sciences.12 The mixed methods approach of Q-methodology is suitable for analytically exploring and illuminating patterns and diversity in a subjective experience. In Q-methodology, the participants engage in a Q-sorting where they rank a set of items (statements) on a pre-determined grid according to their level of agreement or disagreement (Figure 1). Usually, participants pre-sort the statements into three piles (agree, neutral, and disagree) before ranking them on the grid to break the task down and make it easier. Quantitative data are gathered in the form of Q-sorts (participants’ patterns of organizing the statements on the grid) and their subsequent intercorrelation merged in a by-person factor analysis.13 In a by-person factor analysis, participants are analyzed as the variables of the study. Then, qualitative data are commonly collected by asking the participants to elaborate on why they placed the items at the two extreme ends of the grid or by conducting a post-sort interview to reinforce the researcher’s interpretations. Q-methodology is recognized by Watts and Stenner13 as an extremely robust method for holistically exploring subjective opinions on any given topic, as it invites participants to actively shape their perspectives on a set of items, drawing on the “effort after meaning” theory.14 Using Q-methodology aims to identify shared orientations and then to generalize the findings’ concept at the population-level.
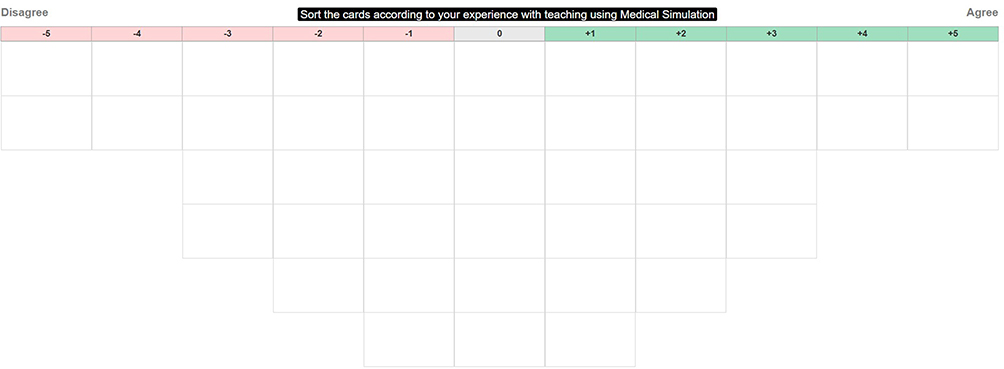 |
Figure 1 Q-sorting grid of the 44 statements. |
Q-Set Design and Content
A Q-study comprises a set of items (Q-set or “concourse”) that participants are asked to sort and rank. For this study, we initially collected 54 statements covering all aspects of medical simulation from a literature review and informal interviews (developing the “concourse”). Some of the statements were adopted with permission from Landeen et al15 but were modified for the purpose of the study. Subsequently, the 54 statements were piloted and reviewed for relevance and validation by two content experts in medical simulation. Having consulted a Q-methodology expert, we revised and reduced the statements to a total of 44 statements (Figure 2). The Q-set (44 items) in this study meets the standard number of items (40–80) proposed by Curt.16 The research team structured the statements under three themes; benefits, needs, and challenges to have a balanced set of statements. Further, the statements were categorized based on relevance to students, facilitators, resources, and usage to represent all aspects of medical simulation. The participants were not informed about the themes nor the categories to avoid influencing participants’ orientations. However, the 44 statements were designed to be controversial to engage the participants actively and elicit different reactions, as suggested by Watts and Stenner.13
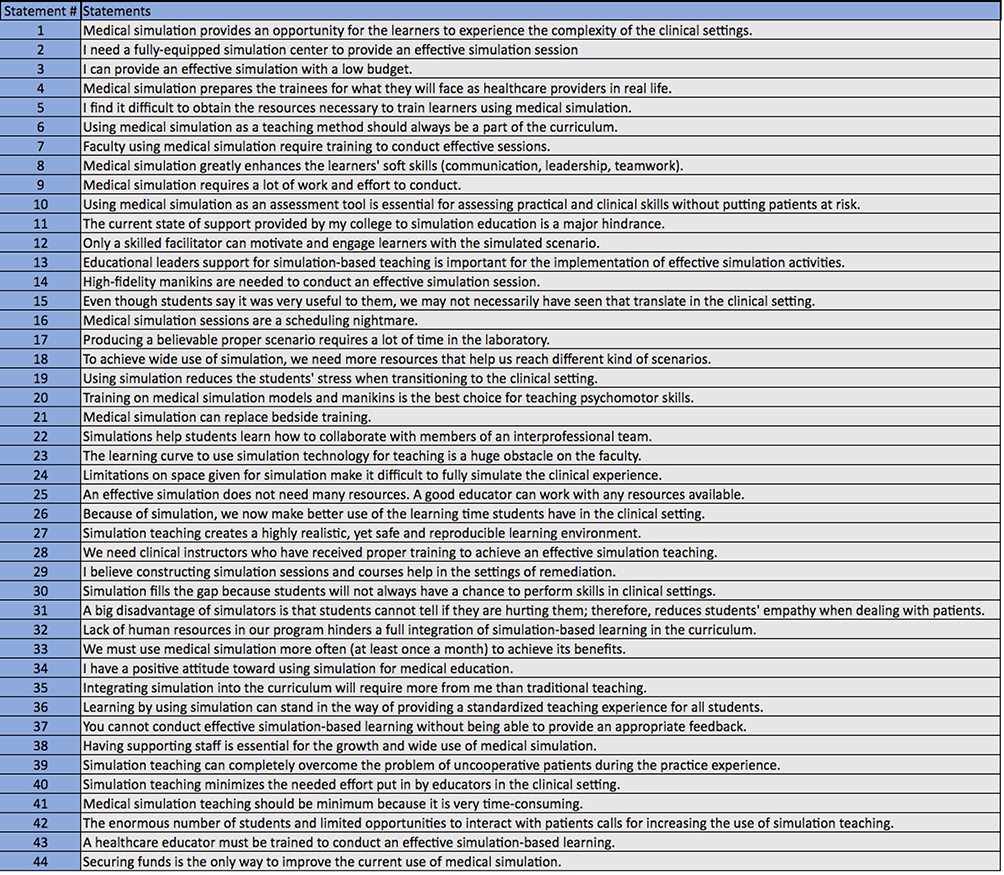 |
Figure 2 The list of 44 statements (Q-set) used in this study for the participants to place on the grid. |
Settings and Participants
The study was conducted at King Saud bin Abdulaziz University for Health Sciences (KSAU-HS) in Riyadh, Saudi Arabia. The university has a fully equipped Clinical Simulation Center hosting medical simulation sessions to educate health professions students. The participants were health professionals who are involved in simulation-based learning at KSAU-HS. Brown17 emphasized that the aim of Q-methodology is to reach, understand, and explain the existing orientations and compare them; therefore, it can be applied to very few participants. As each participant acts as a variable, it is recommended to have a limited number of variables. We purposively recruited 22 participants for this study with a ratio of one participant for every two statements, as suggested by Kline.18 We recruited both male and female participants of various ages and with varying levels of experience with medical simulation. We also recruited from various specialties in medicine and surgery (Radiology, Hematology, Neurology, Transplant, Obstetrics and Gynecology), applied medical sciences (Respiratory Therapy, Emergency Medical Services), and nursing to ensure diversity in views (Table 1). In addition, those who were from the same department were recruited through snowball sampling technique. Healthcare educators who frequently conduct medical simulation sessions were included.
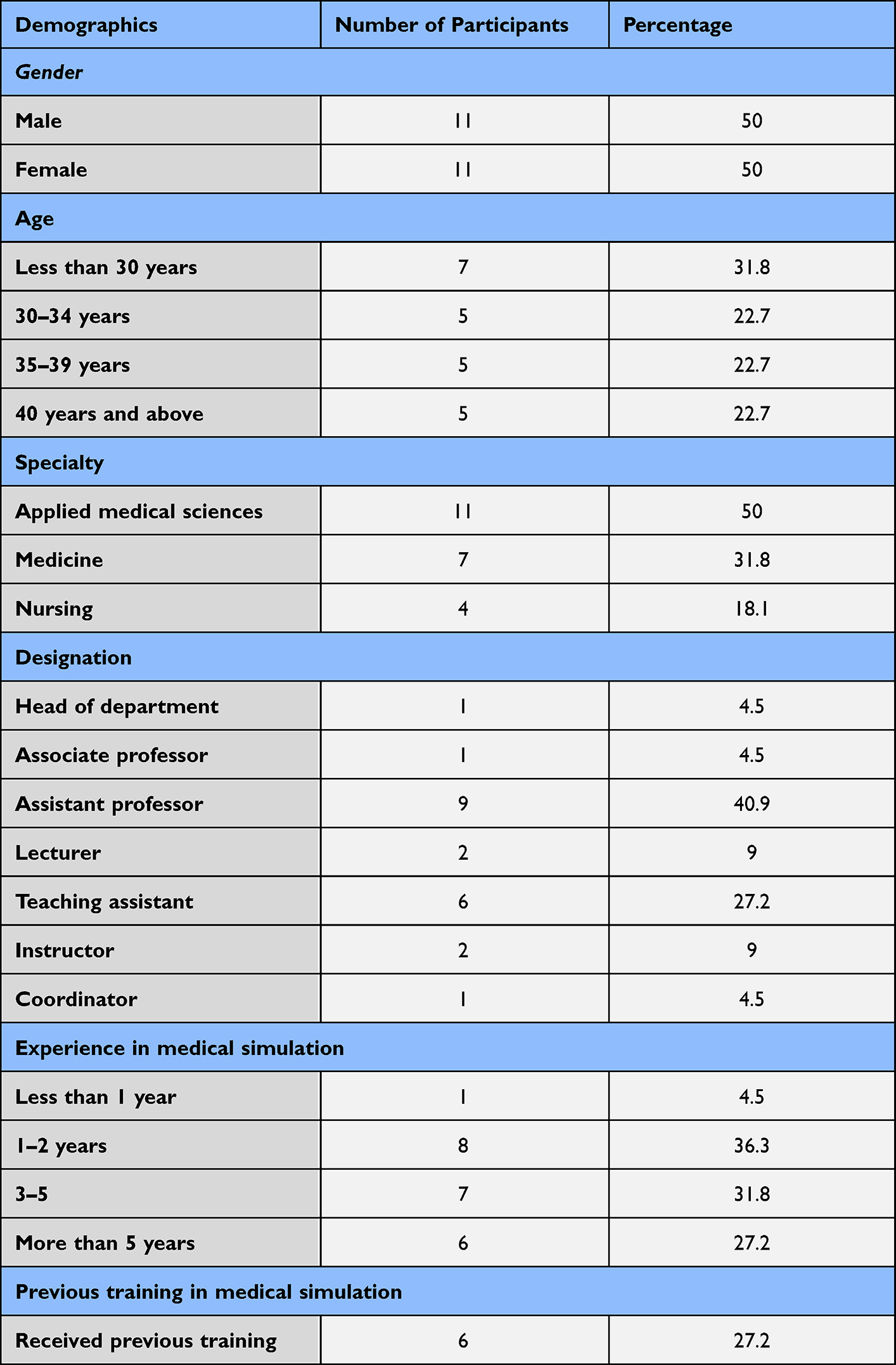 |
Table 1 Demographic Information of the Participants (N = 22) |
Implementation
After receiving approval from the Institutional Review Board (IRB), each participant was asked to provide informed consent online. The anonymity and confidentiality of the information were ensured. The participants were asked to access a webpage developed using Easy HTMLQ and pre-sort and rank the set of statements along a quasi-normal continuum on a fixed grid from (+5) to (−5) (Figure 1). The rank ordering was instructed as follows: first, participants were asked to read all statements and categorize them in three piles: agree, disagree, and neutral. Next, they were asked to read the statements in the “agree” pile once again and select the two statements with which they strongly agreed and place these in the two spots on the right-hand side of the score sheet (+5). Then, they were asked to read the remaining statements of the pile, select the next most agreeable items, and place them in the next column (+4). This process was repeated until no statements remained in the pile. A similar procedure was followed for the “disagree” pile (then ordering from left to right), and for the “neutral” pile (placed in the remaining open spots in the middle). After completing the ranking of the statements, participants were asked open-ended questions to explain their ranking of the statements at the extreme ends (+5) and (−5). This narrative information supported the interpretation of the quantitative findings and was used for elucidation of the results. Finally, the participants answered some demographic and background questions on the same webpage as an online-based questionnaire.
Data Analysis
Ken-Q Analysis web application was used to analyze quantitative data (https://shawnbanasick.github.io/ken-q-analysis/). The application identified the correlation between the participants (ie, variables). Then, a total of 22 Q-sorts were intercorrelated and analyzed through a Q-factor analysis, a by-person factor analysis. Principal Component Analysis (PCA) was conducted to formulate (factors) representing the shared orientations from the participants’ Q-sorts that were highly correlated together. Next, Varimax rotation was applied to maximize the study variance, as recommended for exploratory studies.19 We identified factors that met the 4 selection criteria: simplicity, clarity, distinctness, and stability.20 Therefore, we identified three such factors (orientations), which explained 56% of the study variance with eigenvalues greater than 1. All 22 Q-sorts were significantly associated with (loaded on) at least one of the three extracted factors; however, we removed 6 Q-sorts because they were loading on more than one factor (confounded Q sorts). Participants’ Q-sorts that had a similar pattern were loaded and flagged in the same factor [factor loading of ±0.4 or above were significant at p < 0.01 level] (Table 2). Participants with the flagged Q-sorts in one factor had a similar orientation on the use of medical simulation. By a calculated weight average procedure, the flagged Q-sorts were merged into one best possible Q-sort per factor called factor array, ie, each factor array is the combination of the flagged Q-sorts associated with one factor. The three factor arrays were then interpreted to represent the shared orientation held by the participants loaded on each factor, respectively.
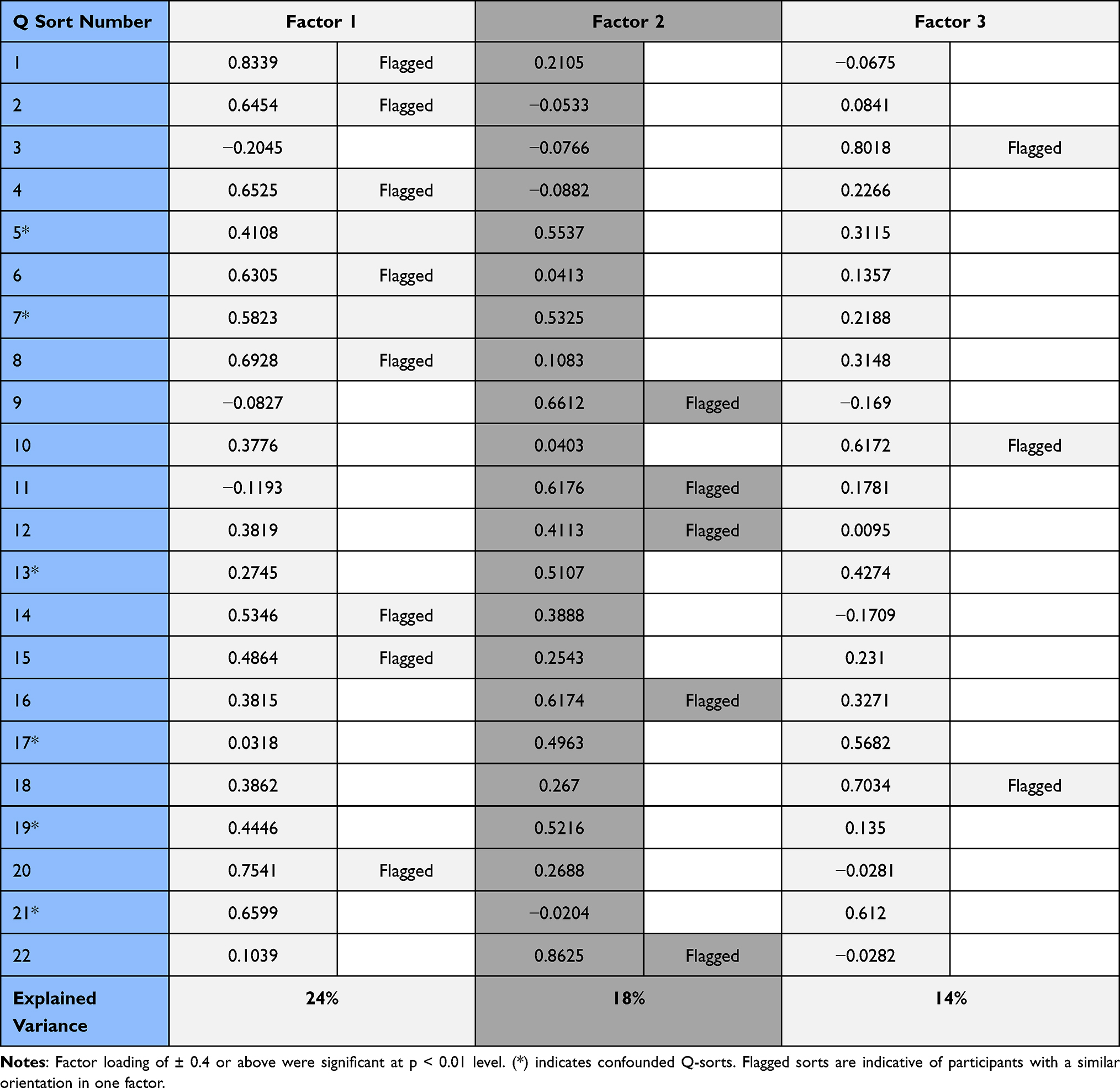 |
Table 2 Factor Matrix with Defining Sorts Flagged |
The analysis and interpretation of the factor arrays is a crucial step in Q-studies. Therefore, we followed the guidance of Watts & Stenner13 to maintain the holistic nature of Q-methodology.21 The interpretation was done by thoroughly and carefully examining patterns within the scores of the statements per factor array. We interpreted each factor based on the statements that were ranked highest and lowest. We included statements with scores significantly higher and lower positively and negatively in a factor array compared with the other factor arrays (distinguishing statements). In addition, we used participants’ qualitative comments to support and clarify the interpretation of the factors. We assigned a name that captures the essence of the participants’ shared orientation represented by each factor in line with the statements that distinguish factors from one another.
Results
The findings of the factors’ interpretations are described separately. The relevant statements are provided with their numbers and ranking scores between parentheses below (and Table 3) with the distinguishing statements significant at P< 0.05 marked with (*) and at P< 0.01 marked with (**).
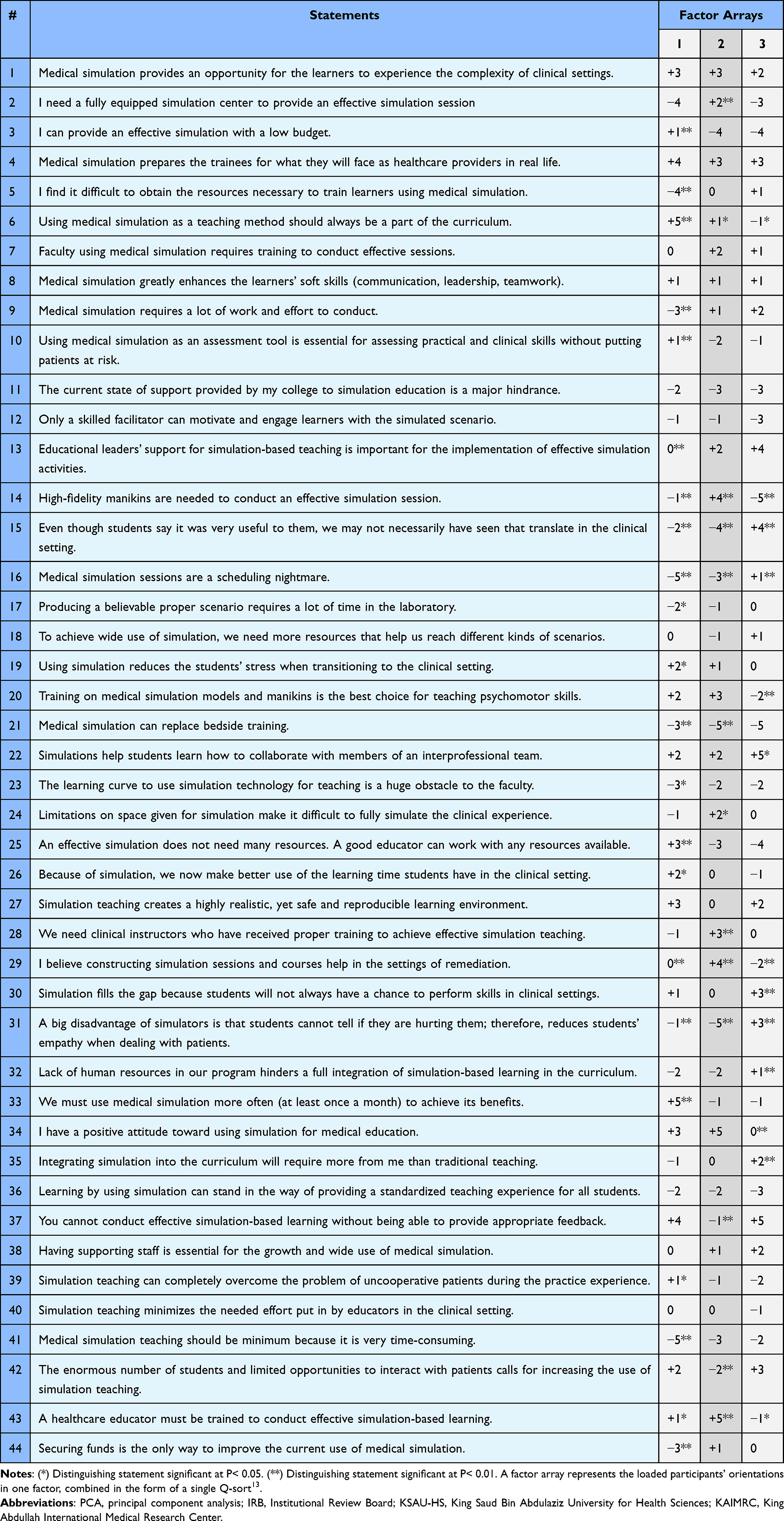 |
Table 3 Scores of the 44 Statements in Each Factor |
Factor 1 Interpretation (Minimalists)
Factor 1 sheds light on faculty members who consider medical simulation a simple, effortless, and beneficial method of teaching and learning. They reported that medical simulation sessions did not require a lot of effort or time to properly produce a scenario (9: −3**; 17: −2*). In comparison with traditional teaching, they expressed that integrating medical simulation into the curriculum does not require additional effort on their part (35: −1). Therefore, they not only strongly disagreed with minimizing medical simulation due to time constraints (41: −5**) but also opposed referring to scheduling the sessions as a nightmare (16: −5**) as some mentioned:
- “Simulation sessions can deliver information and knowledge to the students faster than traditional,”
- “I don’t think it will be a nightmare if you schedule properly and early,”
- “No, when we have properly trained personnel and passionate personnel it is NOT a nightmare.”
They did not perceive resource allocation as a challenge because “the college provides everything,” as one participant stated (5: −4**). The participants loading on this factor seemed to view medical simulation as an uncomplicated method as one participant suggested,
“It is a simple task to perform, organize and prepare with very simple resources. Any healthcare educator can provide it without sophisticated equipment or manikins.”
Factor 1 represented the belief that any good educator could produce an effective session without requiring a lot of resources (25: +3**); as one said, “I could run a well effective session with tiny resource and improvisation”. The participants loading on this factor did not consider securing funds as the only way to improve the current use of medical simulation (44: −3**). They also agreed that running simulation sessions did not necessarily require clinical instructors who had received proper training in its utilization (28: −1), nor did it require a fully equipped center (2: −4). To them, the learning curve for using simulation technology, a low budget, or limited space were not obstacles to providing an effective simulation of the clinical experience (23: −3*; 3: +1**; 24: −1); as one participant stated, “simulation sessions can effectively be achieved with low budget in the out of hospital care practice (EMS)”. Therefore, the participants strongly supported consistent incorporation of medical simulation in the curriculum (6: +5**), and a more frequent application to achieve its benefits (33: +5**).
The orientation represented by Factor 1 showed that participants loading on this factor valued the benefits of medical simulation. As some participants stated, “It’s necessary nowadays, it will keep students oriented more about their objectives. Also, it would be easier for them to apply the skills in real life,” “there are no other ways to training the students for these skills without harming the patient,” “it’s a beneficial method for students to apply what they have learned.” They agreed that medical simulation was an essential assessment tool to measure practical and clinical skills (10: +1**). Further, they perceived it beneficial in overcoming the problem of uncooperative patients and in reducing students’ stress and making better use of students’ time in the clinical setting (39: +1*; 19: +2*; 26: +2*).
Factor 2 Interpretation (Optimistic Worriers)
Factor 2 depicted an optimistic view of medical simulation outcomes, but one that was concerned about the resources, and the facilitator capabilities. Participants loading on factor 2 showed a positive attitude toward using medical simulation because they reported it was helpful for remediation and was the best choice for learning psychomotor skills (34: +5; 29: +4**; 20: +3):
Overall, Factor 2 participants recognized the positive impact of medical simulation on students in clinical settings (15: −4**) as one compared, “Students who have been trained by simulation are different than those who haven’t in the clinical”. They strongly disagreed with the claim that medical simulation reduces students’ empathy when dealing with patients; however, they described that medical simulation was a supplement to bedside training rather than a replacement for it (31: +5**; 21: −5**). One participant summarized this point,
“we must prepare the students on how to examine and what they should do in the simulation center, then they have to go to the patient. The student must see and be trained on a patient but as a second step.”
Nevertheless, they do not regard medical simulation as a key assessment tool, nor do they believe that using medical simulation more often is necessary to reap its benefits (10: −2; 33: −1).
To conduct an effective simulation session, the participants loading on factor 2 emphasized the need for a fully equipped simulation center, with high-fidelity manikins. As one said, “they help mimic the real situation,” but require enough space to simulate the clinical experience completely, “we need enough space to mimic real-life scenarios and high-fidelity cases.” (2: +2**; 44: +1;24: +2*). In addition, factor 2 participants reported that providing effective simulation with low budget was a challenge and that funds and the support of educational leaders could improve the current use of medical simulation (3: −4; 44: +1; 13: +2); “without support of stakeholders and having enough budget, clinical simulation will not be efficient or deliver its message,” a participant commented. However, the lack of human resources in their programs was not an obstacle to the integration of simulation-based learning (32: −2) but rather the facilitators’ competence.
They agreed that there was a need for professionally trained clinical instructors and emphasized that educators using medical simulation must be trained on how to conduct a complete simulation session and give constructive feedback (28: +3**; 43: +5**; 37: −1**); “Training is important so they can produce effective scenarios.” and “without qualification, the educator cannot perform a beneficial stimulation session”, some stated.
Factor 3 Interpretations (Reluctant Skeptics)
Factor 3 captured the view of those who seemed to struggle with medical simulation and were unenthusiastic about its benefits. They expressed that scheduling sessions and obtaining the necessary resources, such as human resources and funds, could be barriers to using medical simulation (16: +1**; 5: +1; 32: +1**). They even reported that a tutor’s potential could be debilitated by the lack of resources; as one participant reflected, “although the educators’ skills play a vital role in education, their skills will be limited if there are limited resources” (25: −4). However, they agreed that providing an effective simulation session was achievable without high-fidelity manikins or a fully equipped center (14: −5**; 2: −3), as two participants explained:
- “One can manage and improvise with available resources”
- “The fidelity of the situation is much more important than the fidelity of the manikins”
Furthermore, they believed that medical simulation required more work and effort than traditional teaching when integrating it into the curriculum (9: +2; 35: +2**); thus, most agreed that the support of both staff and educational leaders was essential for its implementation (38: +2;13: +4).
The participants loading on this factor appreciated some of the benefits of medical simulations but doubted others. They strongly agreed that, with proper feedback, a simulation session could be effective in teaching interprofessional collaboration and allowing the students to practice what they could not in clinical settings. As one elaborated, “appropriate feedback is the key to improve the students’ skills as they will know their mistakes and how to improve them” (37: +5; 22: +5*; 30: +3**). However, they had not necessarily seen the positive impact of medical simulation on students in clinical settings, and they doubted that it made better use of the students’ learning time (15: +4**; 26: −1). Even though they were unanimous in increasing the use of simulation teaching (42: +3), they did not describe medical simulation as a solution for the problem of uncooperative patients or effective for remediation (39: −2; 29: −2**). They even expressed that simulators could reduce students’ empathy when dealing with patients (31: +3**). Consequently, participants loading on Factor 3 had a neutral attitude towards medical simulation and did not perceive it as the best method for teaching psychomotor skills or as a replacement for bedside training (20: −2**; 21; −5). This attitude was encapsulated in the following comment:
“Even though the simulation provides a realistic environment, it is still not a real-life experience with a real patient. Stress and other emotions that novices will feel in their training when they face a real patient do not exist (to some degree) in the simulation environment. These feelings have the potential to influence their performance; therefore, integrating bedside training with simulation would be a much better training option.”
Discussion
If appropriately employed, simulation-based learning has several advantages that may enhance the healthcare professionals’ competencies, improve patient safety, and reduce healthcare costs. We identified three factors representing orientations of medical simulation among healthcare educators in Saudi Arabia: one that highlights the simplicity of the method “Minimalists,” a second that emphasizes the positive outcomes of medical simulation despite some concerns “Optimistic Worriers,” and a third that is more inclined to the potential benefits and challenges of medical simulation “Reluctant Skeptics.”
The first factor represented an enthusiastic orientation of medical simulation, which concurs with the labeled factor “Positive Enthusiasts” reported in Landeen et al.15 Participants were positive about the learning opportunities medical simulation provides, which corresponds with previous studies.22,23 Other studies on the effectiveness of medical simulation have reported that the use of medical simulation increased patient safety, enhanced students and healthcare instructors’ skills, and improved healthcare providers’ performance by reducing medical errors.5,24–28
In the second factor, learning from experienced faculty was of major importance. Medical educators with an “optimistic” orientation to simulation expressed a primary need for support from both staff and leadership to effectively implement simulation-based learning. In addition, training on high-fidelity simulators and incorporating real patients’ interaction with medical simulation were emphasized much more than other aspects. Participants in this factor recognized the importance of scenarios and experienced facilitators to achieve effective simulation-based learning. To address the need for highly qualified and trained instructors, educational institutions should provide opportunities for training in the use of medical simulation conducted by well-trained instructors who also assist in the development of case scenarios.29
We notice that the orientation of the participants representing factor 2 combined seeking help with acquiring resources and training. Moreover, participants loading on factor 3 were critical of medical simulation similar to the two factors labeled “Help Seekers” and “Traditionalists” in Akhtar-Danesh et al.22
Participants loading on factor 3 were more traditional and preferred using bedside training. The educators in this factor stressed the importance of support and resources, which may have lowered their motivation to use medical simulation; satisfaction of the educators’ needs correlates positively with their intrinsic motivation.30 Additionally, educators loading on factor 3 believed that medical simulation was unsuitable for teaching empathy; however, medical simulation can be helpful for learning empathy and developing empathetic behaviors, especially when learners act as patients in the simulation.31
Limitations and Implications
The study has certain limitations. Although our data collection technique was to identify distinct orientations, the selection process of participants might have overlooked important simulation-based learning orientations among healthcare educators from different programs. Furthermore, the study was conducted in a short period at a single Saudi university. Nevertheless, the results of the study have some implications. Our findings can be used to address the issues raised by participants and to plan strategically for integrating medical simulation and bedside training into the curriculum to achieve the benefits discussed in the participants’ orientations. Unlike the previously mentioned Q-studies on the same subject,15,22,23 our study revealed three different factors instead of one or two, which might be due to the various roles and backgrounds of our participants. Even though the data collection method was extensive, we managed to capture the orientations of those with different roles in the academic setting. The statements sorting exercise might be an effective method to help educators self-reflect because participants had to think about the different aspects of medical simulation and its effectiveness. Last, participants appreciated the uniqueness of the data collection in their additional comments.
Conclusion
We identified three orientations towards medical simulation among healthcare educators in Saudi Arabia that are important in the context of the benefits, needs, and challenges of simulation-based learning. We highlighted the importance of faculty training, curriculum integration, and staff and leadership support to successfully make medical simulation effective. Participants were more positive about using simulation to support clinical learning and embraced the accompanying challenges. In addition, faculty awareness of the importance of learning simulation, training in using the method, and providing constructive feedback was noticeable in the participants’ orientations. Furthermore, lack of resources, institutional support, and faculty training were identified as challenges to effective integration of medical simulation. For future work, we propose expanding the study across multiple institutions with varying levels of expertise in simulation-based learning, which may provide additional insights that can be employed to compare the data. We also recommend using alternative methodologies, such as combining Q-methodology with surveys and other qualitative studies, to capture the general perceptions of a larger proportion of faculty, students, and higher management. In addition, health profession institutions should consider the role of faculty, availability of resources, and opportunities for continuous training programs to enhance the effectiveness of medical simulation.
Acknowledgments
The ethics committee at King Abdullah International Medical Research Center (KAIMRC) approved this study (SP21R/160/04). The research did not receive any funding or financial support, and this work has not been submitted for publication anywhere else.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hallinger P, Wang R. The evolution of simulation-based learning across the disciplines, 1965–2018: a science map of the literature. Simul Gaming. 2019;51(1):9–32. doi:10.1177/1046878119888246
2. Aebersold M. The history of simulation and its impact on the future. AACN Adv Crit Care. 2016;27(1):56–61. doi:10.4037/aacnacc2016436
3. The National Aviation Hall of Fame. Edwin Link; 2020, Available from: https://www.nationalaviation.our-enshrinees/link-edwin/.
4. Kunkel ME. Medical Simulations. Salem Press Encyclopedia of Science; 2019.
5. Jones F, Passos-Neto C, Braghiroli OM. Simulation in medical education: brief history and methodology. Princ Pract Clin Res J. 2015;1(2):56–63. doi:10.21801/ppcrj.2015.12.8
6. Paige JT, Garbee DD, Brown KM, Rojas JD. Using simulation in interprofessional education. Surg Clin. 2015;95(4):751–766. doi:10.1016/j.suc.2015.04.004
7. Nuzhat A, Salem RO, Shehri FNA, Hamdan NA. Role and challenges of simulation in undergraduate curriculum. Med Teach. 2014;36(sup1):S69–73. doi:10.3109/0142159x.2014.886017
8. Agha S. Effect of simulation based education for learning in medical students: a mixed study. J Pak Med Assoc. 2019;69(4):545–554.
9. Pawłowicz E, Kulesza M, Szymańska A, Masajtis-Zagajewska A, Bartczak M, Nowicki M. ‘I hear and I forget. I see and I remember. I do and I understand.’– incorporating high-fidelity medical simulation into the undergraduate nephrology course. Ren Fail. 2020;42(1):1184–1191. doi:10.1080/0886022x.2020.1847722
10. Sollid SJM, Dieckman P, Aase K, Søreide E, Ringsted C, Østergaard D. Five topics health care simulation can address to improve patient safety: results from a consensus process. J Patient Saf. 2019;15(2):111–120. doi:10.1097/pts.0000000000000254
11. Ahmed S, Al-Mously N, Al-Senani F, Zafar M, Ahmed M. Medical teachers’ perception towards simulation-based medical education: a multicenter study in Saudi Arabia. Med Teach. 2016;38(sup1):S37–44. doi:10.3109/0142159x.2016.1142513
12. Brown SR The history and principles of Q methodology in Psychology and the Social Sciences. Department of Political Science, Kent State University, Kent, OH; 1997. Available from: http://facstaff.uww.edu/cottlec/Qarchive/Bps.htm.
13. Watts S, Stenner P. Doing Q Methodological Research: Theory, Method and Interpretation. Sage Publications Limited; 2012.
14. Rogers RS. Q methodology. In: Smith JA, Harré R, Langenhofe LV, editors. Rethinking Methods in Psychology.
15. Landeen J, Pierazzo J, Akhtar-Danesh N, Baxter P, van Eijk S, Evers C. Exploring student and faculty perceptions of clinical simulation: a Q-sort study. J Nurs Educ. 2015;54(9):485–491. doi:10.3928/01484834-20150814-02
16. Curt BC. Textuality and Tectonics: Troubling Social and Psychological Science. Open University Press; 1994.
17. Brown SR. Political Subjectivity: Applications of Q Methodology in Political Science. New Haven, CT: Yale University Press; 1980.
18. Kline P. An Easy Guide to Factor Analysis. New York: Routledge; 1994.
19. Akhtar-Danesh N. A comparison between major factor extraction and factor rotation techniques in Q-methodology. Open J Appl Sci. 2017;07(04):147–156. doi:10.4236/ojapps.2017.74013
20. Damio SM. The analytic process of Q methodology. Asian J Uni Educ. 2018;1:59–75.
21. Stephenson W. The inverted factor technique. British J Psychol. 1936a;26(4):344–361.
22. Akhtar-Danesh N, Baxter P, Valaitis RK, Stanyon W, Sproul S. Nurse faculty perceptions of simulation use in nursing education. West J Nurs Res. 2009;31:312–329. doi:10.1177/0193945908328264
23. Baxter P, Akhtar-Danesh N, Landeen J, Norman G. Teaching critical management skills to senior nursing students: videotaped or interactive hands- on instruction. Nurs Educ Perspect. 2012;33:106–110. doi:10.5480/1536-5026-33.2.106
24. AlHarbi WM. Simulation-based medical education: theory and practice. Int J Sci Eng Res. 2016;7(5):249–253.
25. Chacko T. Simulation-based medical education: using best practices and curriculum mapping to maximize educational benefits in the context of shift toward competency-based medical education. Arch Med Health Sci. 2017;5(1):9–15.
26. Phrampus PE. Simulation and integration into Patient Safety Systems. Simul Healthc. 2018;13(4):225–226. doi:10.1097/sih.0000000000000332
27. Sørensen JL, Østergaard D, LeBlanc V, et al. Design of simulation-based medical education and advantages and disadvantages of in situ simulation versus off-site simulation. BMC Med Educ. 2017;17(1):20. doi:10.1186/s12909-016-0838-3
28. Al Kuwari KM. Simulation - based medical education. Bahrain Medical Bull. 2018;40(1):9–10. doi:10.12816/0047451
29. Yeun EJ, Bang HY, Ryoo EN, Ha EH. Attitudes toward simulation-based learning in nursing students: an application of Q methodology. Nurse Educ Today. 2014;34(7):1062–1068. doi:10.1016/j.nedt.2014.02.008
30. Utomo HB. Teacher motivation behavior: the importance of personal expectations, need satisfaction, and work climate. Int J Pedagog Teach Educ. 2018;2(2):333. doi:10.20961/ijpte.v2i2.24036
31. Bearman M, Palermo C, Allen LM, Williams B. Learning empathy through simulation. Simul Healthc. 2015;10(5):308–319. doi:10.1097/sih.0000000000000113
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.