Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 12
Oral Health Knowledge, Attitudes, and Behaviors Among University Students in Jeddah, Saudi Arabia
Authors Farsi NJ ![]() , Merdad Y
, Merdad Y ![]() , Mirdad M
, Mirdad M ![]() , Batweel O
, Batweel O ![]() , Badri R, Alrefai H, Alshahrani S, Tayeb R
, Badri R, Alrefai H, Alshahrani S, Tayeb R ![]() , Farsi J
, Farsi J ![]()
Received 22 July 2020
Accepted for publication 27 October 2020
Published 17 November 2020 Volume 2020:12 Pages 515—523
DOI https://doi.org/10.2147/CCIDE.S272986
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Nada J Farsi,1 Yasser Merdad,2 Mohammed Mirdad,3 Omar Batweel,4 Rawan Badri,5 Hind Alrefai,6 Sultanah Alshahrani,7 Rawan Tayeb,8 Jamila Farsi9
1Department of Dental Public Health, Faculty of Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia; 2Department of Restorative and Aesthetic Dentistry, Faculty of Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia; 3Ministry of Health, Jeddah, Saudi Arabia; 4Ministry of Health, Makkah, Saudi Arabia; 5Department of Periodontics, Faculty of Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia; 6Faculty of Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia; 7Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia; 8Ministry of Health, Riyadh, Saudi Arabia; 9Department of Oral Biology, Faculty of Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia
Correspondence: Nada J Farsi
Department of Dental Public Health, Faculty of Dentistry, King Abdulaziz University, P.O. Box 80200, Jeddah 21589, Saudi Arabia
Tel +966126400000
Fax +966126952437
Email [email protected]
Purpose: This study aimed to evaluate oral health knowledge, attitudes, and behaviors among a sample of senior students at King Abdulaziz University (KAU), and to assess differences among these factors between genders.
Methods: A total of 1177 senior university students at KAU were included in this cross-sectional study. Participants were selected by stratified random sampling. KAU has three main streams categorized by field of study. One faculty was randomly selected from each stream. Information regarding oral health knowledge, attitudes, and behaviors was collected with a validated self-administered questionnaire. A knowledge score was calculated, and predictors of oral health knowledge were assessed by linear regression.
Results: In general, the mean oral health knowledge score of females (8.1 ± 1.8) was significantly higher than that of males (7.2 ± 2.1) out of 13. Relative to males, females reported a greater frequency of teeth cleaning and of using a toothbrush with proper technique (p < 0.001). Females were also more likely to have ever visited a dentist than males (95% and 86%, respectively). The linear regression model revealed that students in non-medical faculties and those who were not shown how to brush their teeth by a dentist had lower oral health knowledge scores, than their counterparts. Students older than 22 years and females were more likely to have higher oral health knowledge scores than were their counterparts.
Conclusion: Oral health knowledge was relatively low among the university students, but females showed better oral health knowledge and behaviors than males did.
Keywords: oral health, attitudes, behaviors, university students
Introduction
Oral health is an essential component of individuals’ general health and overall well-being, which is related to individuals’ oral health knowledge and healthy oral hygiene habits.1 Abstract knowledge of oral health practices alone does not ensure a subsequent change in individuals’ attitudes and behaviors, however, as they are usually acquired after conceptualizing oral health practices. Neglect of oral health, on the other hand, can lead to pain and suffering, which can affect individuals’ quality of life and hinder productivity at the workplace.2
According to the World Health Organization (WHO), oral health problems are still not well controlled globally despite the considerable improvements in oral health measures among populations. This state of oral health might be related to the rapid development of oral diseases following lifestyle changes such as consumption of a sugar-rich diet, lack of water fluoridation, and other socio-environmental factors.3,4 The high incidence and prevalence of oral diseases globally qualifies oral health as a serious public health issue. In addition, oral disease treatments are considered to be the fourth most expensive disease treatments in most industrial countries.3,4 That makes oral health a huge burden at both the individual and the community level. In 2003, the Fédération Dentaire Internationale World Dental Federation (FDI), WHO, and the International Association for Dental Research issued the document “Global Goals for Oral Health 2020,” which contains proposals for new goals, objectives, and targets for global oral health of increasing detail and complexity. That proposal aimed to provide an instrument for local and national health care planners to determine realistic goals and standards for oral health.3 Establishing a baseline of detailed information regarding oral health knowledge and healthy oral hygiene habits will help policymakers set attainable goals and track changes. Moreover, this baseline information will strengthen oral health programs through the implementation of effective prevention measures.
Studies on oral health knowledge, attitudes, and practices have been conducted among university students in different countries. In 2014, Peltzer and Pengpid investigated oral health behavior and associated factors among undergraduate university students from various disciplines in 26 low, middle-, and high-income countries. This study confirmed low rates of tooth brushing and dental attendance among university students in different cultures across Africa, Asia, and the Americas.5 In Nigeria, a study was conducted to compare oral health knowledge, attitudes, and behavior of medical, pharmacy, and nursing university students. The investigators found that students’ oral health knowledge, attitudes, and behavior were inadequate and needed to be improved.6 In 2017, Kumar et al studied and compared oral health knowledge, attitudes, and practices among dental and medical students at a university in Eastern India. They reported that oral health knowledge and practices among females was better than that in males.7
In Arab countries, several studies have been conducted to assess oral health knowledge, attitudes, and behaviors, especially among school students.1,8–13 Other studies assessed university dental undergraduate students and compared them with undergraduate students of other faculties. The findings of these studies are expected, as, compared with non-dental students, dental students had already received education on oral health in their undergraduate curriculum.14–18 Previous studies did not focus on senior students, however, which is important because the knowledge of senior students reflects the cumulative oral health knowledge and behaviors that students acquire during their years at university.14,16,18–26 Moreover, most of the previous studies did not focus on gender differences in oral health knowledge, attitudes, and behaviors. The studies that did focus on gender differences assessed the knowledge of dental students and compared students from different dental academic years.14,26 Therefore, the present study was performed to evaluate oral health knowledge, attitudes, and behaviors among senior students of King Abdulaziz University (KAU), and to assess gender-based differences among these factors.
Methods
Study Design
In this cross-sectional study, we used a stratified random sampling technique to select a sample of senior undergraduate students attending KAU. Data were collected from March 2017 to April 2017.
Sampling Procedure
KAU is divided into three main streams: Health (Medical) Science, Sciences, and Humanities. Each stream has several faculties and departments. There were 96,459 students in all faculties during the 2016/2017 academic year. In this study, we included only those faculties in which students of both genders were enrolled (26,109 students) to allow for comparisons between genders.
The Faculties of Pharmacy and Applied Medical Sciences from the Health Sciences stream, the Faculty of Sciences from the Sciences stream, and the Faculty of Economics and Administration from the Humanities stream were randomly selected by using the stratified random sampling technique (Table 1). Two faculties were chosen from the Health Sciences stream because of the small number of senior students enrolled in them.
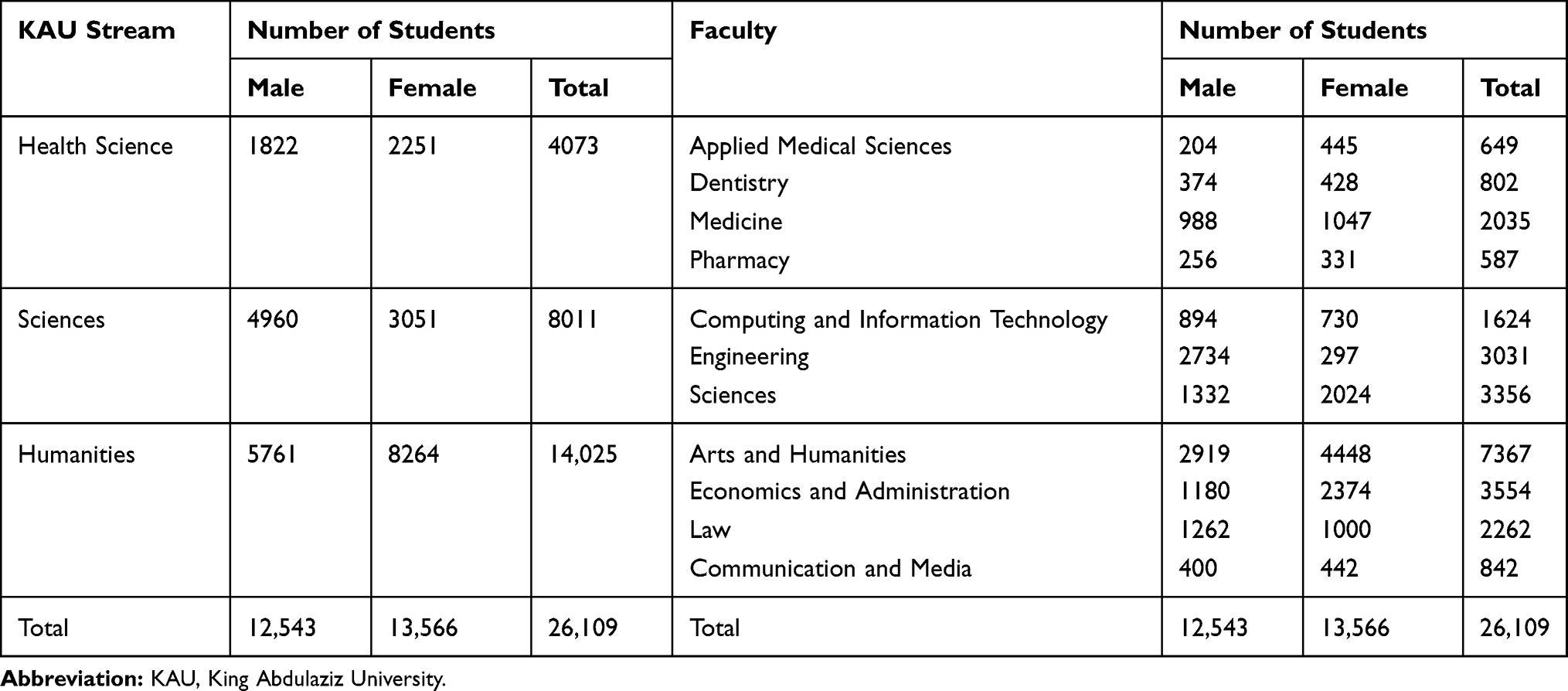 |
Table 1 Number of Students Enrolled in KAU in the 2016/2017 Academic Year |
All senior students from each faculty were invited to participate. Ethical approval was obtained from the Research Ethics Committee of the Faculty of Dentistry (Proposal number #092-16). Written permission was obtained from the vice dean of each of the selected faculties. Participants were assured of data confidentiality, and all provided informed consent.
Questionnaire
A validated Arabic questionnaire was administered that had been developed by Farsi et al in 2003.11 It consisted of 34 questions divided into three sections. The first section elicited demographic data: faculty, gender, age, parental education level, and monthly income. The second section contained questions that assessed the participants’ knowledge of oral health. The third section contained questions regarding oral health behavior and the attitudes of the participants: teeth cleaning; tooth and tongue brushing; frequency of tooth brushing; frequency of floss, miswak, and toothpick use; dental visits; and tooth brushing instructions received from a dentist.
Although the questionnaire was validated, some questions related to access to dental care were added for specific use in another study. A pilot questionnaire was administered to a sample of 20 recent KAU graduates from different specialties to ensure comprehensibility. The questionnaire was then slightly modified based on the responses, with only some words requiring modification. The questionnaire was then piloted again on another group of 20 recent graduates.
Questionnaire Distribution
Lists of all senior undergraduate male and female students were obtained from each faculty. The lists contained the number of classes, the locations of the classes, and the number of students enrolled in each class. Because classes overlapped and many were attended by the same students, a schedule was created to guarantee that the questionnaires reached all students. Graduation requisite classes were chosen, as only seniors can enroll in these classes and attendance is mandatory.
The questionnaire and a consent form were distributed by the investigation team. The consent form contained a brief description of the study, its aim, a disclaimer that their participation is optional and a data confidentiality statement. The questionnaires were distributed to 1280 students and were returned by 1177, yielding a 92% response rate. The administration and student affairs offices of the selected faculties were contacted to obtain permission to administer the questionnaire, to schedule a date, and to ask whether they preferred it to be distributed at the beginning or end of class. Most of the faculty members agreed to distribute the questionnaire in the last 7 minutes of their lecture.
Statistical Analysis
Descriptive statistics were calculated by using means and standard deviations for continuous variables and frequencies and percentages for categorical variables. The chi-square test was used to assess associations between categorical variables.
A knowledge score was calculated from the 13 knowledge questions; a score of 1 was given for correct answers and 0 for incorrect or “I don’t know” answers. By adding the scores of all knowledge questions, we calculated a total knowledge score for each participant, ranging from 0 to 13. Higher scores indicated better knowledge.
Linear regression was used to determine predictors of students’ knowledge scores. The predictors assessed were faculty, age, gender, mother’s education, father’s education, monthly income, and whether the dentist had shown the participants how to brush their teeth correctly; the outcome was the knowledge score. A forward stepwise technique was used to select variables for inclusion in the model, with an entry level p-value of 0.05 and a removal level p-value of 0.1.
Logistic regression was used to assess the predictors of students’ attitudes toward visiting the dentist. The predictors assessed were faculty, age, gender, mother’s education, father’s education, and monthly income; the outcome was having ever visited a dentist (never vs. ever). The same predictors were assessed in relation to the participants’ oral health behavior; the outcome was brushing frequency (less than twice daily vs. twice daily or more). The data were analyzed by using statistical analysis software (SPSS version 22, IBM, Armonk, NY, USA). A p-value of < 0.05 was considered statistically significant.
Results
A total of 1177 senior undergraduate students (482 males, 695 females), with a mean age of 22.4 ± 1.7 years were included in this study. The demographic characteristics of the study participants are presented in Table 2. Female participants comprised a significantly greater proportion of participants than male students in all chosen faculties, except in the sciences. Most participants reported that their parents had education levels above high school (19.37% for fathers, 30.75% for mothers). Female students’ mothers had higher education levels than did male students’ mothers (p < 0.05). Fathers’ education levels did not significantly differ between genders.
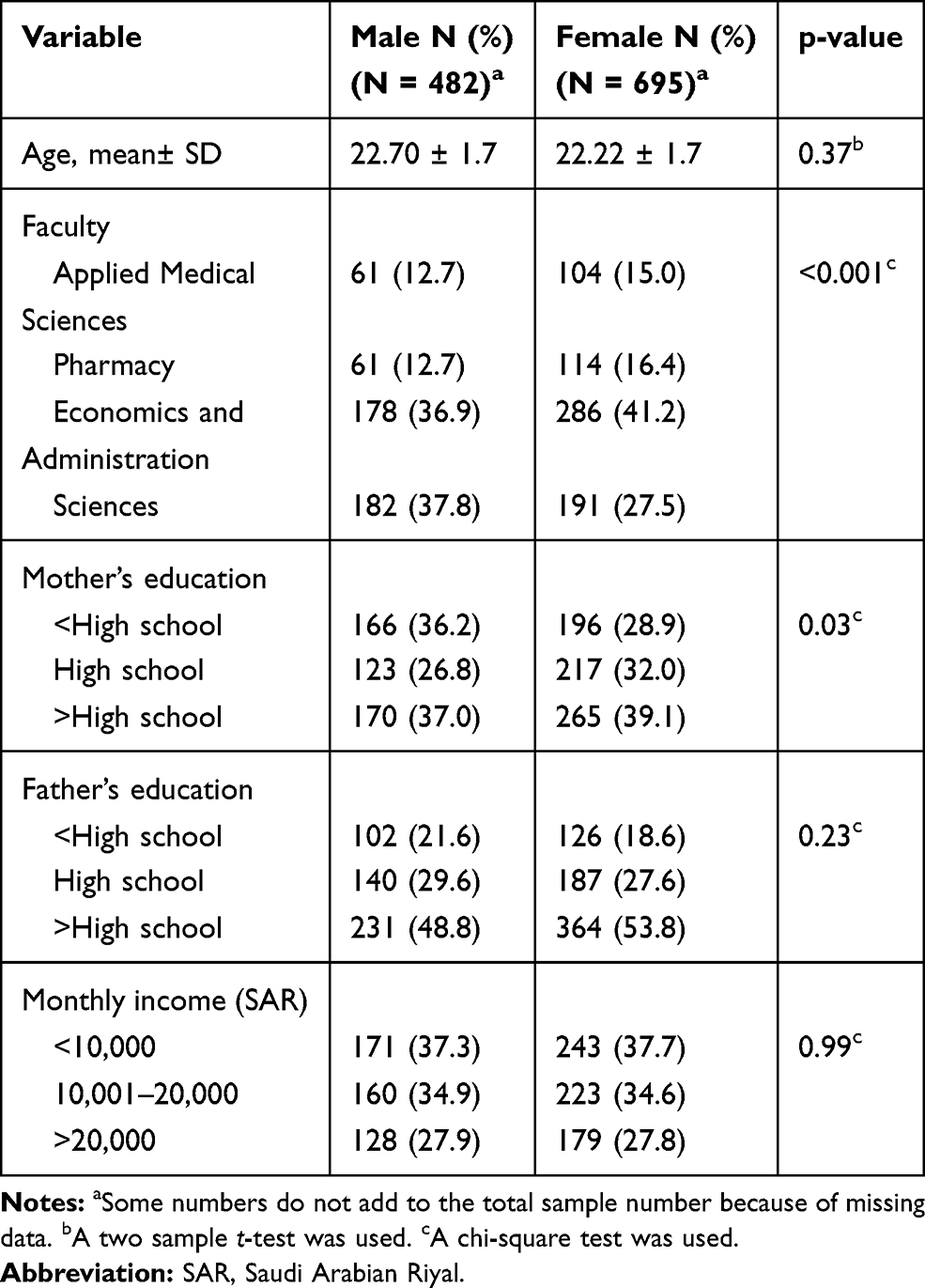 |
Table 2 Characteristics of Study Participants |
Table 3 illustrates the distribution of the participants with respect to oral health knowledge. The majority of participants of both genders agreed that tooth brushing prevents periodontal disease (94%); however, females were significantly more knowledgeable regarding the role of flossing in preventing gum problems (p < 0.001). A greater proportion of female students (70.2%) than male students (55.7%) (p < 0.001) knew that gum bleeding during brushing is a sign of early-stage inflammation. A high proportion of both genders did not exhibit an understanding of the relationship between oral disease and systemic problems; a significantly greater proportion of males (68.5%) than females (63.7%) (p < 0.001) exhibited a poor understanding of this relationship. Among the females, 96.8% knew that oral hygiene prevents halitosis versus 89.4% of the males (p < 0.001). Most male and female students knew what dental calculus is (85.6% and 96.5%, respectively; p < 0.001). However, the majority of both genders responded incorrectly regarding the nature of plaque. In general, the mean knowledge score (± SD) for females (8.1 ± 1.8) was significantly higher than that for males (7.2 ± 2.1) (p < 0.001).
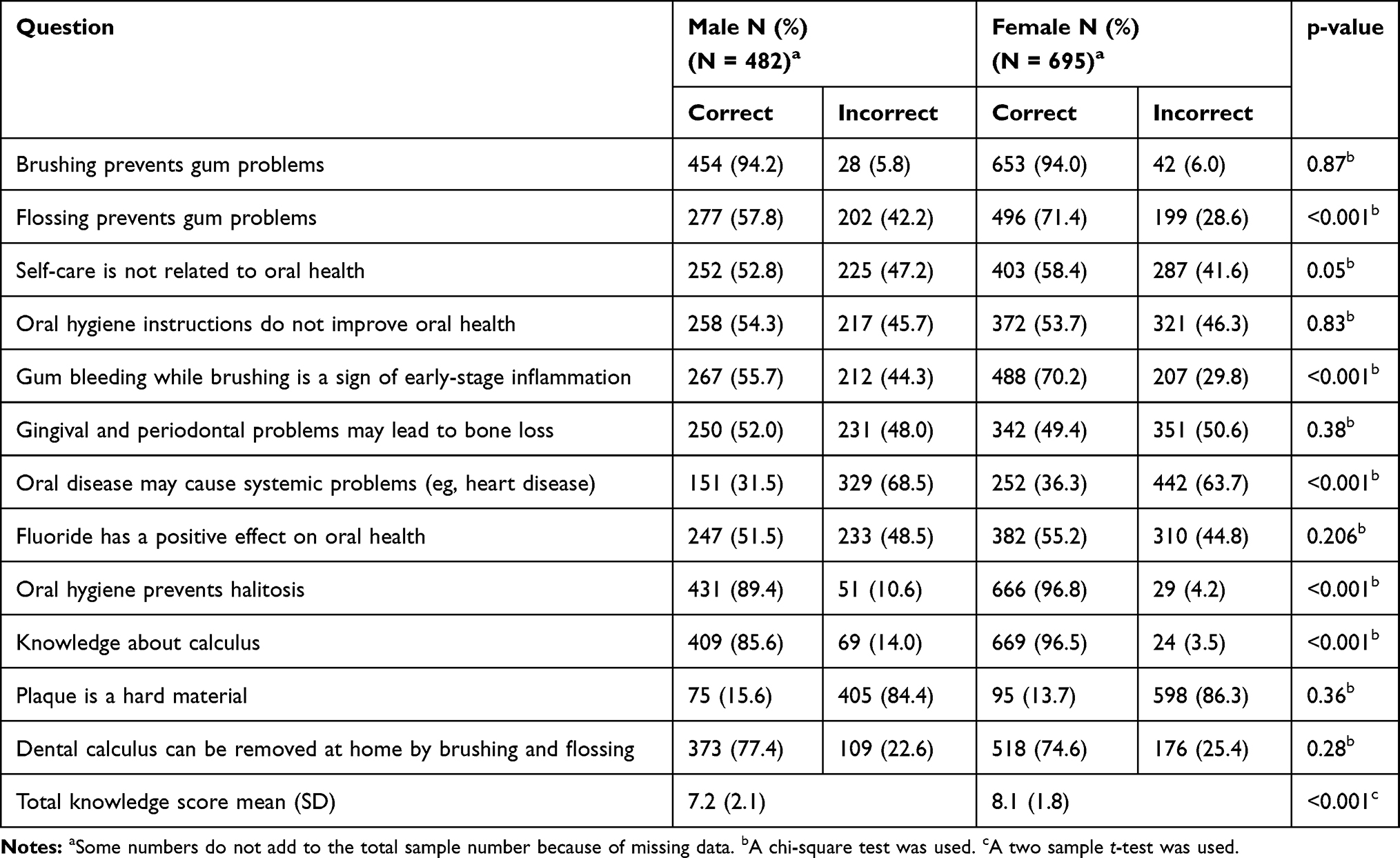 |
Table 3 Oral Health Knowledge Among Study Participants |
Oral health attitudes and behaviors among the study participants are presented in Table 4. Females visited the dentist and brushed their teeth more frequently than males did (p < 0.001). Furthermore, females reported a higher frequency of using a toothbrush with proper technique (outer and inner surfaces of all teeth) than males did (p < 0.001). A greater proportion of males reported using toothpaste during brushing rather than any other materials. Only 9.4% of females and 13% of males used electric toothbrushes.
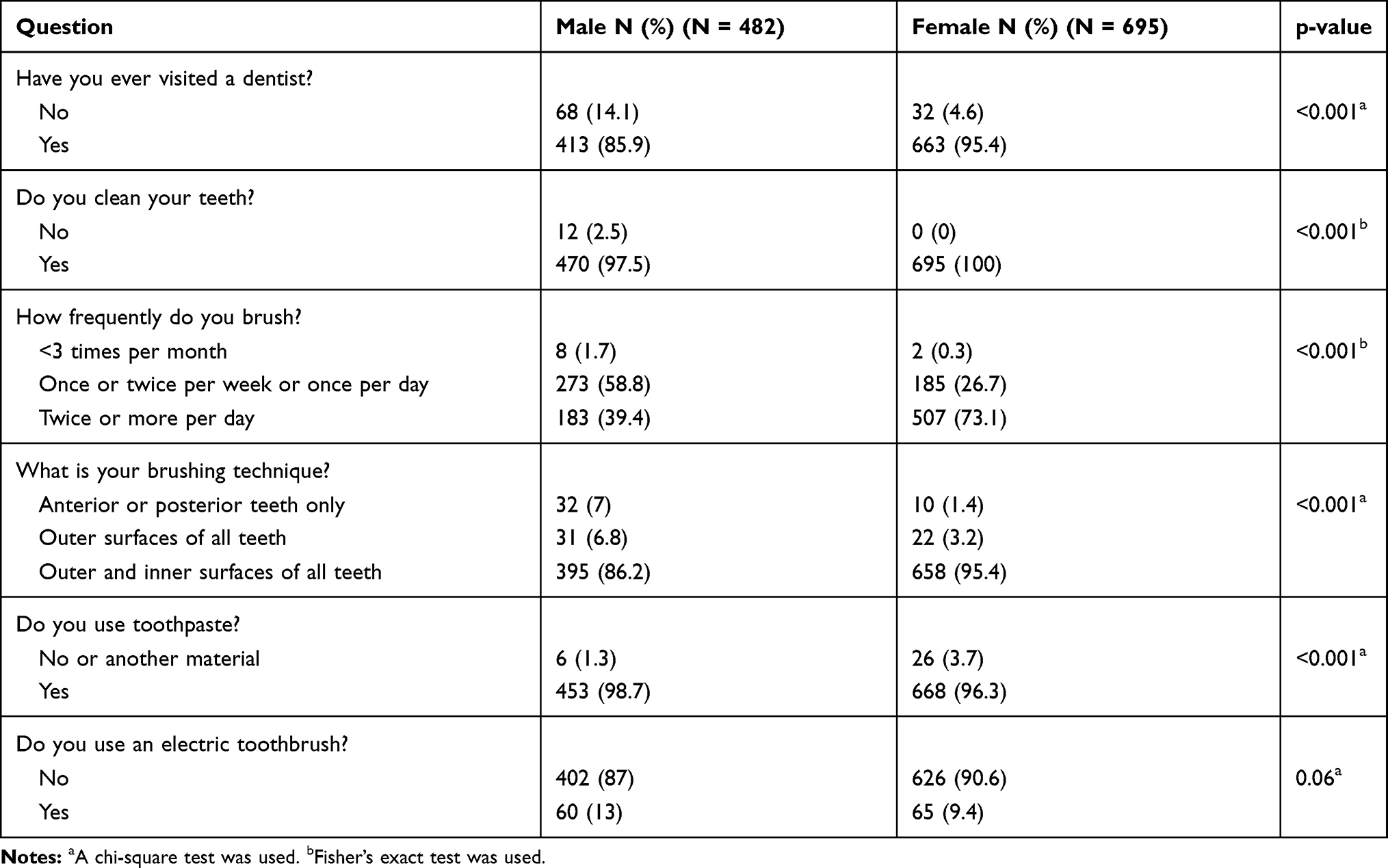 |
Table 4 Oral Health Attitudes and Behaviors Among Study Participants |
Table 5 demonstrates the results of the linear regression model that assessed predictors of the oral health knowledge score. Students in non-medical faculties tend to have lower scores than students in medical faculties. Significant positive relationships were shown between older age (>22 years vs. ≤22 years) and the knowledge score (coefficient = 0.42, 95% confidence interval (CI): 0.2–0.7). Furthermore, females showed better oral health knowledge than males (p < 0.001). A predictor of a lower knowledge score was the lack of learning about how to brush correctly from a dentist (p = 0.003).
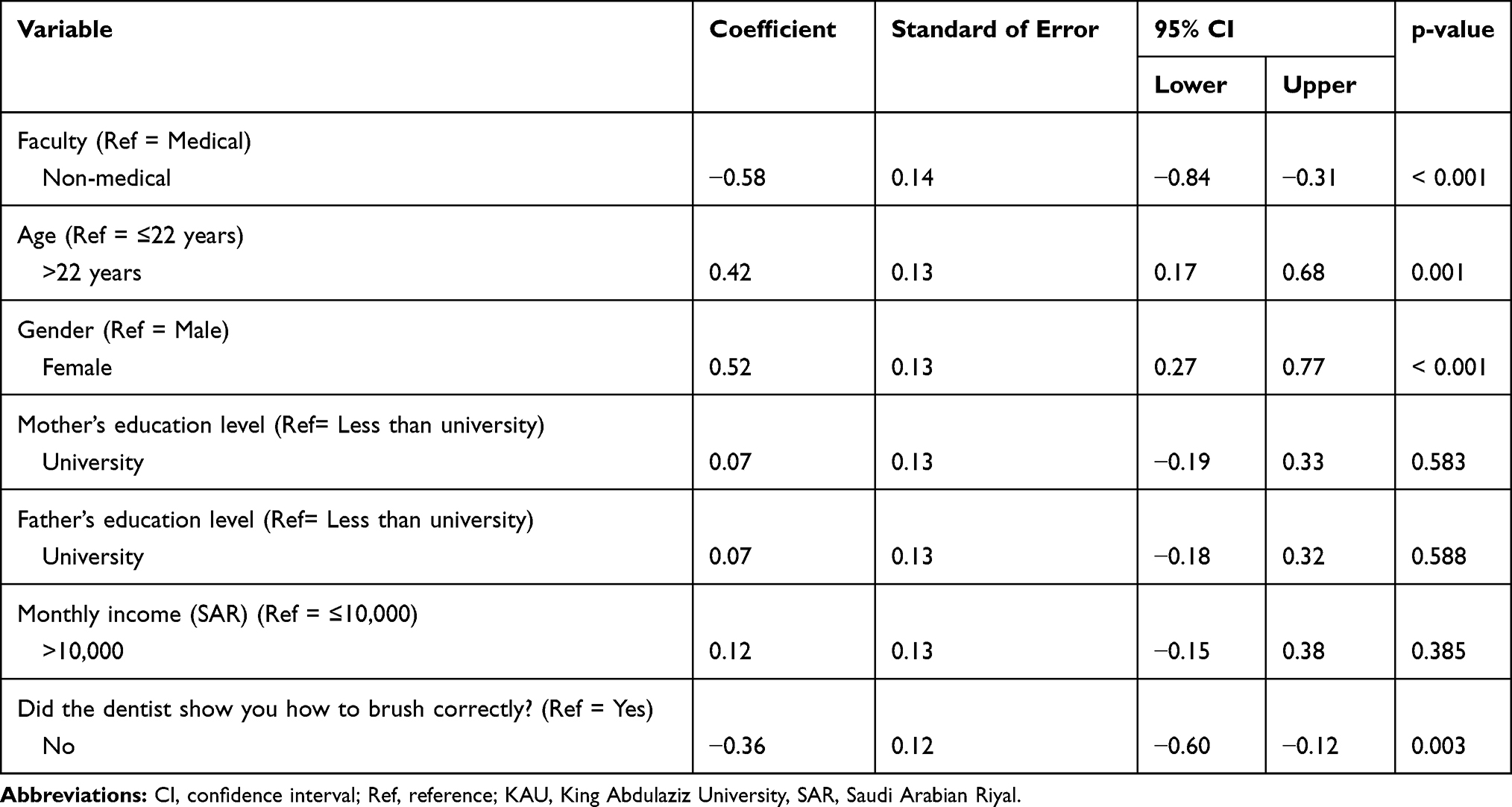 |
Table 5 Predictors of Oral Health Knowledge Score |
Logistic regression models were used to assess predictors of the participants’ attitudes toward visiting the dentist (ever vs. never visiting a dentist) (Supplementary Table 1) and another model was made to assess oral hygiene behavior (brushing less than twice daily vs brushing twice or more daily) (Supplementary Table 2). The same predictors from the previous model were assessed in these two models. The only predictor that affected dental visits and oral hygiene was gender. Females were more likely than males to brush twice daily or more (odds ratio [OR] = 4.5, 95% CI: 3.4–5.9), and were more likely to have ever visited a dentist (OR = 3.6, 95% CI: 2.2–5.8).
Discussion
This cross-sectional study assessed the oral health knowledge, attitudes, and behaviors of 1177 senior undergraduate students who were randomly selected from KAU. Results showed that female students demonstrated significantly better knowledge, attitudes, and behaviors than male students did.
Females were more knowledgeable than males with respect to bleeding as a sign of periodontal disease and the role of flossing as a preventive aid. In this study, our assessments of knowledge regarding flossing were consistent with the results of prior studies that reported that females showed better knowledge and attitudes regarding dental floss and other interdental aids.14–17,27 This finding may result from greater esthetic awareness among females. Thus, they might be more proactive with respect to visiting the dentist and might tend to receive more frequent dental health care, thereby providing them with greater exposure to oral health knowledge.17,27 In addition, attitudes regarding oral health are influenced by one’s own experiences, cultural/familial practices, religious beliefs, and other life situations. These attitudes are reflected in an individual’s oral health behavior.
In the present study, females exhibited better oral health behavior than males did with respect to the frequency of brushing and visiting the dentist. Female students also showed better brushing techniques, which involved cleaning of all outer and inner surfaces of the teeth, consistent with the results of previous studies.14,18,25,28 The positive oral health behaviors and attitudes of females could be explained in terms of females usually having a higher concern about their appearance. Thus, they would be more likely to visit a dentist and become educated about oral health. Periodic dental checkups are important in preventing oral disease, educating patients, and encouraging them to maintain good oral hygiene habits.6,29–32 For example, in 2020, Covello et al found that periodic follow-ups can even prevent oral piercing complications.33 Only a minority of our participants used electric toothbrushes, which is consistent with the results of previous studies that showed a low frequency of electric toothbrush users among students and adults.11,28 A previous study found that the majority of respondents did not consider electric toothbrushes to offer any greater advantage over manual toothbrushes.18
We found that parental education did not play a critical role in determining the extent of oral hygiene knowledge and behavior among participants. It could be expected that more educated parents would be more aware of their children’s’ oral health and more likely to supervise them while brushing. However, a previous study that assessed tooth brushing behavior in 32 countries reported that lack of parental supervision had an inconsistent effect on brushing behavior.34 School and media contributions have increased awareness in recent years, thereby potentially relieving a portion of the parental burden with regard to oral hygiene. Vozza et al concluded that oral health prevention programs in schools play an important role in students’ gaining knowledge and practicing skills.35 In contrast, numerous studies involving children have shown that parents play a significant role in overall oral hygiene.8,9,12 It was reported that the development of caries can be decreased with parental supervision in addition to tooth brushing.36,37 Our participants were university students, and thus parental guidance probably plays less of a role than it does for younger students. In addition, the participants’ monthly income did not seem to significantly contribute to oral hygiene knowledge or behavior. This result was unexpected and differs from the findings of previous studies, which have shown significant correlations between socioeconomic status and oral hygiene.35,36 This finding might be explained by a lack of oral health knowledge, which negatively affects participants’ behaviors. Furthermore, participants who frequently brushed and flossed had better oral health knowledge. In previous studies, this improved knowledge was correlated with good oral hygiene behavior.28,38,39 Dentists are regarded as an important source of oral health information, along with mass media, and have a considerable impact on their patients.13,40 In the present study, participants showed better oral hygiene knowledge if their dentists had shown them how to properly brush their teeth.
Our study has a few limitations. First, the research was performed on the basis of self-reported data. Thus, participants may have made errors in interpreting the questions.41 We believe that any such effect would be minimal, however, as the questionnaire was validated11 and piloted twice. Notably, previous studies found that self-reporting of daily flossing and annual checkups accurately predicted the incidences of plaque, calculus, gingivitis, and periodontal destruction.42,43 Second, a dental examination was not performed, which could have offered an objective assessment of oral health status along with the questionnaire-based subjective assessment of participants’ knowledge, attitudes, and practices.
The study also has notable strengths, in that we used an appropriate sampling strategy to select participants. We believe that the use of this sampling technique, in addition to the high response rate, minimized selection bias. A diverse group of senior students was randomly selected from the KAU, which makes the study results more generalizable to all senior students at KAU.
Conclusion
This study of a sample of senior students demonstrated that females had significantly better oral health knowledge, attitudes, and behaviors than males did. We recommend that oral health-related education be included and emphasized in university curricula with a greater focus on male students.
Data Sharing Statement
Data can be made available upon request.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Al Subait AA, Alousaimi M, Geeverghese A, Ali A, El Metwally A. Oral health knowledge, attitude and behavior among students of age 10–18 years old attending Jenadriyah festival Riyadh: a cross-sectional study. Saudi J Dental Res. 2016;7(1):45–50. doi:10.1016/j.sjdr.2015.05.001
2. Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye C. The global burden of oral diseases and risks to oral health. Bull World Health Organ. 2005;83(9):661–669.
3. Hobdell M, Petersen PE, Clarkson J, Johnson N. Global goals for oral health 2020. Int Dent J. 2003;53(5):285–288. doi:10.1111/j.1875-595X.2003.tb00761.x
4. Petersen PE. The World Oral Health Report 2003: continuous improvement of oral health in the 21st century–the approach of the WHO Global Oral Health Programme. Community Dent Oral Epidemiol. 2003;31(Suppl 1):3–23. doi:10.1046/j.2003.com122.x
5. Peltzer K, Pengpid S. Oral health behaviour and social and health factors in university students from 26 low, middle and high income countries. Int J Environ Res Public Health. 2014;11(12):12247–12260. doi:10.3390/ijerph111212247
6. Bashiru BO, Omotola OE. Oral health knowledge, attitude and behavior of medical, pharmacy and nursing students at the University of Port Harcourt, Nigeria. J Oral Res Rev. 2016;8(2):66. doi:10.4103/2249-4987.192209
7. Kumar H, Behura SS, Ramachandra S, Nishat R, Dash KC, Mohiddin G. Oral health knowledge, attitude, and practices among dental and medical students in Eastern India–a comparative study. J Int Soc Prevent Communit Dent. 2017;7(1):58–63. doi:10.4103/jispcd.JISPCD_30_17
8. Al-Omiri MK, Al-Wahadni AM, Saeed KN. Oral health attitudes, knowledge, and behavior among school children in North Jordan. J Dent Educ. 2006;70(2):179–187. doi:10.1002/j.0022-0337.2006.70.2.tb04074.x
9. Amin TT, Al-Abad BM. Oral hygiene practices, dental knowledge, dietary habits and their relation to caries among male primary school children in Al Hassa, Saudi Arabia. Int J Dent Hyg. 2008;6(4):361–370. doi:10.1111/j.1601-5037.2008.00310.x
10. Baghdadi Z. Improving oral health status of children in Tabuk, Saudi Arabia. Dent J. 2014;2(1):22–40. doi:10.3390/dj2010022
11. Farsi JM, Farghaly MM, Farsi N. Oral health knowledge, attitude and behaviour among Saudi school students in Jeddah city. J Dent. 2004;32(1):47–53. doi:10.1016/j.jdent.2003.08.002
12. Togoo RA, Yaseen SM, Al Zamzami M. Oral hygiene knowledge and practices among school children in a rural area of southern Saudi Arabia. Int J Contemp Dent. 2012;3:1.
13. Wyne AH, Chohan AN, Al-Dosariai K, Al-Dokheilai M. Oral health knowledge and sources of information among male Saudi school children. Odontostomatol Trop. 2004;27(106):22–26.
14. Al-Omari QD, Hamasha AA. Gender-specific oral health attitudes and behavior among dental students in Jordan. J Contemp Dent Pract. 2005;6(1):107–114. doi:10.5005/jcdp-6-1-107
15. Amran AG, Alhajj MN, Madfa AA. Social characteristics and oral self-care practices associated with periodontal health status among a sample of Yemeni dental students. J Dent Med Sci. 2015;14:28–35.
16. Halboub E, Dhaifullah E, Yasin R. Determinants of dental health status and dental health behavior among Sana’a University students, Yemen. J Investig Clin Dent. 2013;4(4):257–264. doi:10.1111/j.2041-1626.2012.00156.x
17. Kawamura M, Spadafora A, Kim KJ, Komabayashi T. Comparison of United States and Korean dental hygiene students using the Hiroshima University–Dental Behavioural inventory (HU-DBI). Int Dent J. 2002;52(3):156–162. doi:10.1111/j.1875-595X.2002.tb00621.x
18. Peker I, Alkurt MT. Oral health attitudes and behavior among a group of Turkish dental students. Eur J Dent. 2009;3(1):24–31. doi:10.1055/s-0039-1697402
19. Ahamed S, Moyin S, Punathil S, Patil NA, Kale VT, Pawar G. Evaluation of the oral health knowledge, attitude and behavior of the preclinical and clinical dental students. J Int Oral Health. 2015;7(6):65–70.
20. Al-Ansari J, Honkala E, Honkala S. Oral health knowledge and behavior among male health sciences college students in Kuwait. BMC Oral Health. 2003;3(1):2. doi:10.1186/1472-6831-3-2
21. Al-Zarea BK. Oral health knowledge of periodontal disease among university students. Int J Dent. 2013;2013:647397. doi:10.1155/2013/647397
22. Almas K, Al-Hawish A, Al-Khamis W. Oral hygiene practices, smoking habit, and self-perceived oral malodor among dental students. J Contemp Dent Pract. 2003;4(4):77–90. doi:10.5005/jcdp-4-4-77
23. Baseer MA, Rahman G, Al Kawaey Z, Al Awamy B, Al Manmeen Z, Al Shalaty F. Evaluation of oral health behavior of female dental hygiene students and interns of Saudi Arabia by using Hiroshima University Dental Behavioural Inventory (HU-DBI). Oral Health Dent Manag. 2013;12(4):255–261.
24. Doshi D, Baldava P, Anup N, Sequeira PS. A comparative evaluation of self-reported oral hygiene practices among medical and engineering university students with access to health-promotive dental care. J Contemp Dent Pract. 2007;8(1):68–75. doi:10.5005/jcdp-8-1-68
25. Kassak KM, Dagher R, Doughan B. Oral hygiene and lifestyle correlates among new undergraduate university students in Lebanon. J Am Coll Health. 2001;50(1):15–20. doi:10.1080/07448480109595706
26. Kateeb E. Gender-specific oral health attitudes and behaviour among dental students in Palestine. East Mediterr Health J. 2010;16(3):329–333. doi:10.26719/2010.16.3.329
27. Kawamura M, Iwamoto Y, Wright FA. A comparison of self-reported dental health attitudes and behavior between selected Japanese and Australian students. J Dent Educ. 1997;61(4):354–360. doi:10.1002/j.0022-0337.1997.61.4.tb03125.x
28. Peltzer K, Pengpid S. Dental health status and oral health behavior among university students from five ASEAN countries. Nagoya J Med Sci. 2017;79(2):123–133.
29. Al-Hussaini R, Al-Kandari M, Hamadi T, Al-Mutawa A, Honkala S, Memon A. Dental health knowledge, attitudes and behaviour among students at the Kuwait University health sciences centre. Med Princ Pract. 2003;12(4):260–265. doi:10.1159/000072295
30. Al-Qahtani SM, Razak PA, Khan SD. Knowledge and practice of preventive measures for oral health care among male intermediate schoolchildren in Abha, Saudi Arabia. Int J Environ Res Public Health. 2020;17(3):703. doi:10.3390/ijerph17030703
31. Al-wesabi AA, Abdelgawad F, Sasahara H, El Motayam K. Oral health knowledge, attitude and behaviour of dental students in a private university. BDJ Open. 2019;5(1):1–5. doi:10.1038/s41405-019-0024-x
32. Peker K, Uysal Ö, Bermek G. Dental training and changes in oral health attitudes and behaviors in Istanbul dental students. J Dent Educ. 2010;74(9):1017–1023. doi:10.1002/j.0022-0337.2010.74.9.tb04958.x
33. Covello F, Salerno C, Giovannini V, Corridore D, Ottolenghi L, Vozza I. Piercing and oral health: a study on the knowledge of risks and complications. Int J Environ Res Public Health. 2020;17(2):613. doi:10.3390/ijerph17020613
34. Maes L, Vereecken C, Vanobbergen J, Honkala S. Tooth brushing and social characteristics of families in 32 countries. Int Dent J. 2006;56(3):159–167. doi:10.1111/j.1875-595X.2006.tb00089.x
35. Vozza I, Capasso F, Calcagnile F, et al. School-age dental screening: oral health and eating habits. Clin Ter. 2019;170(1):e36–e40.
36. Calcagnile F, Pietrunti D, Pranno N, Di Giorgio G, Ottolenghi L, Vozza I. Oral health knowledge in pre-school children: a survey among parents in central Italy. J Clin Exp Dent. 2019;11(4):e327–e333.
37. Watanabe M, Wang D-H, Ijichi A, et al. The influence of lifestyle on the incidence of dental caries among 3-year-old Japanese children. Int J Environ Res Public Health. 2014;11(12):12611–12622. doi:10.3390/ijerph111212611
38. Holmes RD. Tooth brushing frequency and risk of new carious lesions. Evid Based Dent. 2016;17(4):98–99. doi:10.1038/sj.ebd.6401196
39. Kumar S, Tadakamadla J, Johnson NW. Effect of toothbrushing frequency on incidence and increment of dental caries: a systematic review and meta-analysis. J Dent Res. 2016;95(11):1230–1236. doi:10.1177/0022034516655315
40. Paik DI, Moon HS, Horowitz AM, Gift HC, Jeong KL, Suh SS. Knowledge of and practices related to caries prevention among Koreans. J Public Health Dent. 1994;54(4):205–210. doi:10.1111/j.1752-7325.1994.tb01216.x
41. Marquis KH, Marquis MS, Polich JM. Response bias and reliability in sensitive topic surveys. J Am Stat Assoc. 1986;81(394):381–389. doi:10.1080/01621459.1986.10478282
42. Lang WP, Farghaly MM, Ronis DL. The relation of preventive dental behaviors to periodontal health status. J Clin Periodontol. 1994;21(3):194–198. doi:10.1111/j.1600-051X.1994.tb00303.x
43. Lang WP, Ronis DL, Farghaly MM. Preventive behaviors as correlates of periodontal health status. J Public Health Dent. 1995;55(1):10–17. doi:10.1111/j.1752-7325.1995.tb02324.x
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.