Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Oral Health Assessment Tools for Elderly Adults: A Scoping Review
Authors Yang H ![]() , Xiao J
, Xiao J ![]() , Cui S, Zhang L, Chen L
, Cui S, Zhang L, Chen L ![]()
Received 3 October 2023
Accepted for publication 18 December 2023
Published 22 December 2023 Volume 2023:16 Pages 4181—4192
DOI https://doi.org/10.2147/JMDH.S442439
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Heng Yang,1 Jiechenming Xiao,2 Shaomei Cui,1 Liyan Zhang,1 Lixia Chen1
1Department of Nursing, the Fourth Affiliated Hospital, Zhejiang University School of Medicine, Yiwu, Zhejiang, People’s Republic of China; 2Department of Nursing, Huangyan Hospital, Wenzhou Medical University, Taizhou, Zhejiang, People’s Republic of China
Correspondence: Lixia Chen, Department of Nursing, the Fourth Affiliated Hospital, Zhejiang University School of Medicine, N1 Shangcheng Avenue, Yiwu, Zhejiang, People’s Republic of China, Tel +1 596 882 9886, Email [email protected]
Purpose: The aim of this study was to synthesize the Oral Health Assessment Tool for elderly adults and determine its psychosocial properties.
Methods: We conducted a scoping review. The Arkey and O’Malley methodology was employed to conduct scoping reviews involving the exploration of both national and international databases, as well as a manual search of the reference lists of the selected studies. We focused on oral health assessment tools for elderly adults (> 60 years). The review report adhered to the standards outlined in the PRISMA-ScR guidelines. The study protocol was officially filed with the Open Science Framework.
Results: A total of 19 documents were included. The literature search included a time frame ranging from 1995 to 2023 and covered a diverse range of 13 countries. Of the 19 assessment tools examined, it was found that only the Oral Assessment Sheet had multidimensional characteristics, while the remaining tools were unidimensional in nature. The evaluation of oral health assessment tools was conducted across several contexts, including nursing homes, geriatric facilities, communities, and hospitals. A total of eleven studies underwent reliability testing, whereas two studies were alone validated for validity and did not undergo reliability testing. Additionally, seven studies were exclusively validated for reliability and did not undergo validity testing.
Conclusion: Multidimensional oral health assessment tools for elderly adults that integrate social and psychological aspects need to be developed and validated. It is necessary to develop oral health assessment tools based on hospitalized elderly patients to meet the oral and dental health needs of elderly patients.
Keywords: assessment tools, elderly adults, oral health, reliability, scoping review, validity
Introduction
Life expectancy has increased worldwide because of improvements in the prevention, diagnosis, and treatment modalities. The World Health Organization (WHO) predicts that by 2050, individuals aged 60 years and over will make up 21.3% of the world’s population.1 According to the data from China’s seventh population census, there are approximately 191 million individuals aged 65 years and over, accounting for 13.5% of the total population, and China’s population is expected to age at a rate of 18.7% by 2020.2 Worldwide, there has been a notable acceleration in the process of population aging, characterized by a rising number of elderly individuals. Consequently, the health of the elderly has emerged as a key concern within aging societies. Oral health is part of the overall health of elderly adults, and the World Report on Aging and Health suggests that oral health is a key and often neglected area of healthy aging.3 Oral health has emerged as a major health challenge for the elderly population.
According to the WHO, oral health includes the condition of the mouth, teeth, and oral-facial structures, which facilitate essential functions such as eating, breathing, and speaking. Additionally, it involves psychosocial aspects, such as self-confidence, well-being, and the ability to socialize and work without pain, discomfort, and embarrassment.4 Elderly adults commonly exhibit diminished oral health sometimes presenting with prevalent oral conditions, such as dental caries, periodontal disease, and oral cancer. Poor oral health is prevalent among elderly adults and is associated with general health and chronic diseases.5,6 Poor oral health may threaten the general health of these adults and influence the development of chronic disorders, such as stroke, diabetes, and dementia.7 The incidence of chronic diseases and the utilization of multiple medications frequently increase with advancing age, hence intensifying the susceptibility to oral health degradation.8,9 Hakeem et al discovered a substantial association between dental health and age-related frailty in a systematic review, indicating that oral health might be a predictor of age-related frailty.10,11 Poor oral health can exacerbate physiological burdens in elderly adults, such as tooth loss and pain, as well as increased risk of local and systemic infections, leading to impaired oral function and reduced quality of life.12,13 In addition, the presence of dental imperfections and halitosis negatively impacts an individual’s mental welfare and hinders their ability to integrate into social settings. Maintaining optimal overall health is dependent upon the imperative nature of oral health for elderly individuals.
Proactive oral health assessment and intervention can prevent poor oral health and deterioration. Studies have shown that when nurses follow standardized oral care routines, the oral health of elderly patients improves.14 In the context of nursing homes or intensive care units, the implementation of effective oral hygiene practices and the provision of professional oral care have been shown to mitigate the incidence or advancement of respiratory diseases among elderly individuals who are particularly susceptible to such conditions.12 Hence, the evaluation of the oral health condition among elderly individuals becomes advantageous in terms of identifying oral diseases and monitoring the risk of chronic inflammation and systemic disorders.15 Healthcare professionals, nursing facilities, and community providers concerned about the oral health of older adults should encourage the development of strategies to maximize oral health and prevent complications.16
Currently, the more widely used scales for the assessment of oral health in elderly adults include the Brief Oral Health Status Examination (BOHSE), the Oral Health Assessment Tool (OHAT), and the Oral Assessment Sheet (OAS). Rodrigues et al conducted a systematic review with the aim of ascertaining the progression and assessing the measuring features of oral health assessment tools used by non-dental practitioners for elderly individuals residing in facilities that provide long-term care.17 However, this study only considered the application of oral health assessment tools by non-dental professionals in long-term care facilities. In addition, since new studies on oral health assessment tools have been published, it is necessary to update the review of assessment tools in a timely manner. Meanwhile, none of the previous studies have reviewed Chinese-related oral health assessment tools. The absence of a globally acknowledged and standardized oral health evaluation tool for the elderly necessitates the development of a reliable and efficient assessment tool.
To this aim, we conducted a scoping review to systematically characterize research in this area and identify existing knowledge gaps. A scoping review helps organize and summarize the scope and characteristics of the existing literature on a specific topic, as well as identify gaps in research on a particular topic to aid in the planning of future studies.18,19 Unlike a systematic review, a scoping review does not focus on the quality of inclusion but rather supports the identification of a broader body of the literature.20 This study aimed to collect a comprehensive collection of oral health assessment tools for elderly adults and synthesize their psychometric properties, in order to provide healthcare professionals with scientific and valid tools when screening and assessing oral health.
Materials and Methods
The purpose of this study was to perform a scoping review of the literature to identify current tools for assessing the state of oral health in the elderly. The methodology employed in this investigation adhered to the reporting criteria outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMAR-ScR), as detailed in Supplementary File PRISMA-ScR Checklist. The PRISMAR-ScR framework is derived from the recommendations established by the EQUATOR Network.21 The scoping review follows the five phases outlined in Arksey and O’Malley’s methodological framework.22 The methodological framework has a broad conceptual scope that can account for a wide range of relevant studies and is therefore suitable.20 The scoping review protocol has been published in the Open Science Framework (OSF: https://OSF.io/s89qb/) registration.
Stage I: Identifying the Research Question
The research questions of interest in this scoping review are as follows: (1) What are the current oral health assessment tools applied to elderly adults both domestically and internationally? (2) What are the reliability and validity of various oral health assessment tools used on the elderly population? (3) Identification of research gaps and guiding future research.
Stage II: Identifying Relevant Studies
A comprehensive search was conducted across five databases, namely CNKI, Wanfang, PubMed, Embase, and Web of Science Core Collection. The search covered the period from the inception of the databases to August 30, 2023. Additionally, a final search was performed on September 23, 2023. A complete and detailed search strategy was formulated by a graduate student in nursing who had received systematic training. The approach was subsequently presented to the team for further development. In addition, a snowballing technique was employed for citation tracking; however, gray literature was not included in the retrieval process. The results of the Chinese literature search were imported into NoteExpress (V 3.7.0.9296), and the English literature was imported into EndNote X9.3.3. The search strategy for selected databases is shown in Table 1.
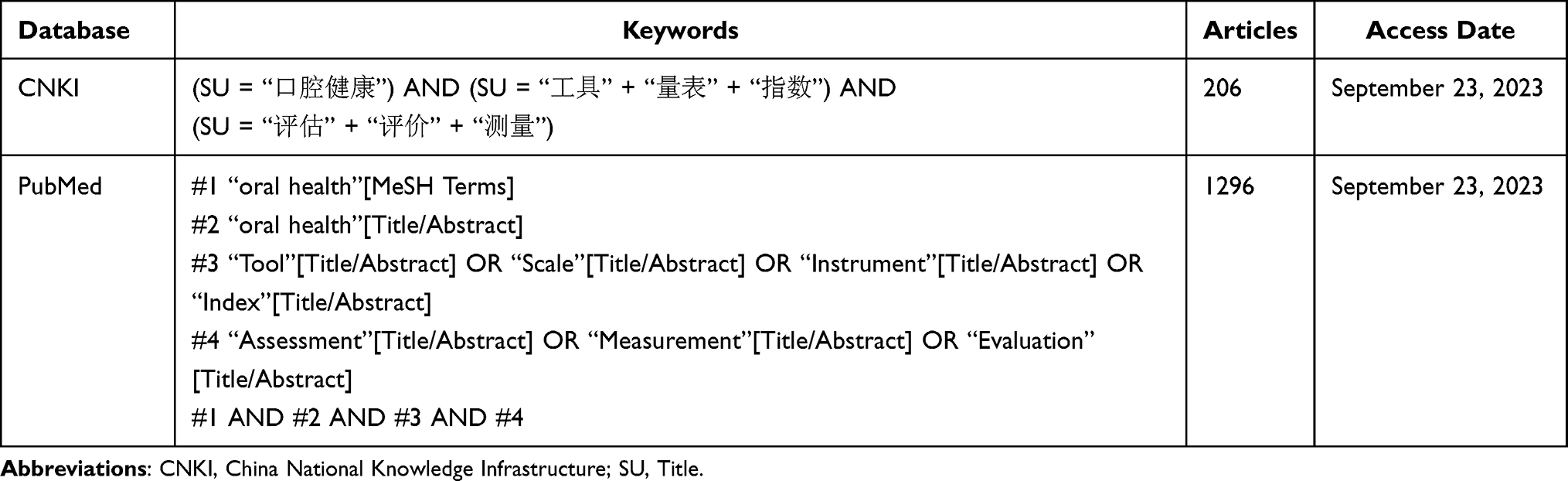 |
Table 1 Partial Search Strategy and Results |
Stage III: Study Selection
Literature inclusion criteria: (1) Subjects in the research were over 60 years old, and included elderly hospitalized patients, community elders, and elderly individuals in nursing homes; (2) The research content pertained to the primary literature about the development, testing, revision, localization, and application of oral health assessment tools; (3) The study types included cross-sectional, longitudinal, cohort, and case-control studies; and (4) The sources of information included scholarly publications published in academic journals. The exclusion criteria were: (1) duplicates; (2) the unavailability of the full-text version of the article; (3) non-Chinese and English literature; (4) conference abstracts, dissertations, editorials, letters, books; and (5) comprehensive assessment tools containing oral health assessment. The process of literature screening involved the use of automated methods to identify duplicate articles. Additionally, two authors independently assessed the titles, abstracts, and full texts of the identified articles. Any discrepancies in their evaluations were resolved by consensus among the study team.
Stage IV: Charting the Data
The full-text versions of collected articles were imported into EndNote for management, and a data extraction form was created to help answer the research questions, including an assessment tool, developer, publication date, country/region, study population, study setting, the number of dimensions, the number of items, characteristics, as well as reliability and validity. Two authors independently extracted the relevant information, and disagreements were negotiated by the research team, and the data were compared and summarized when the extraction was completed.
Stage V: Collating, Summarizing and Reporting Results
The included studies were descriptively outlined, providing a basic overview of their key characteristics. The findings were then classified to facilitate a systematic understanding of the study results. Additionally, a narrative summary was provided to elucidate the nature of the Oral Health Assessment Tool for Older Adults and identify any existing gaps in the current body of research.
Results
Search results
A total of 65,856 records were obtained through a comprehensive search of the databases described earlier. Following a meticulous screening process based on the predetermined inclusion and exclusion criteria, 16 relevant literature sources were ultimately included in the study. Retrospective references were obtained from 3 literature sources. Also, 19 literature sources were finally included in this study. The literature screening process is shown in Figure 1.
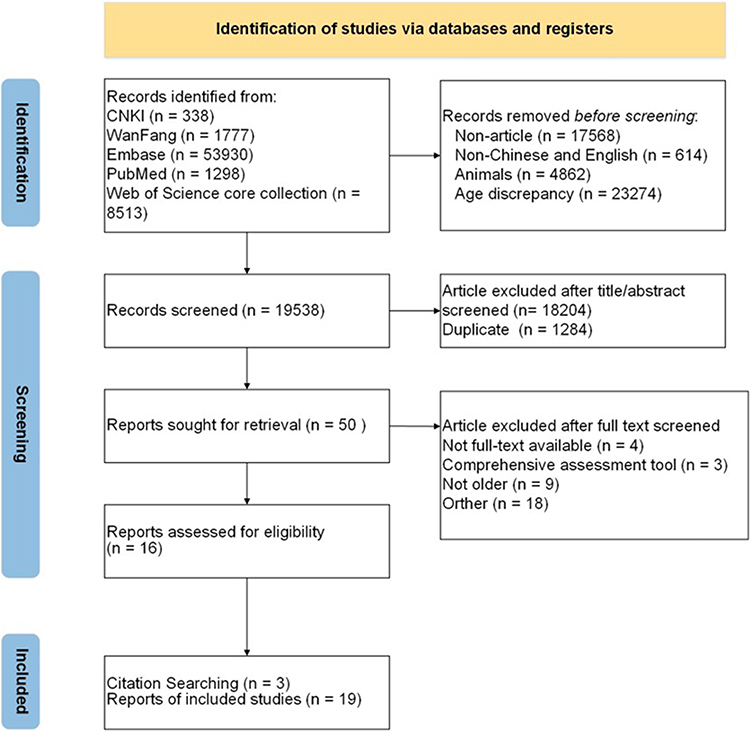 |
Figure 1 PRISMA flow diagram for the scoping review process. Notes: Adapted from Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. Creative Commons.23 |
Basic Characteristics of the Included Studies
The literature published during the years 1995–2023 in the field of oral health assessment consisted of a total of 19 papers. Among these, three papers were published in 2017, while two papers each were published in 2016, 2019, 2020, and 2023. Additionally, one paper each was published in the years 1995, 1999, 2002, 2005, 2007, 2014, 2021, and 2022. Geographically, the studies were primarily conducted in Belgium (n = 3), with two papers each originating from China, the United States, Norway, and Japan. Furthermore, one paper each was conducted in Brazil, Australia, Sweden, Germany, Italy, Portugal, Turkey, and the Netherlands. BOHSE, mucosal-plaque index (MPS), OHAT, A Single-Item for Oral Health Assessment, dental hygiene registration (DHR), the oral health-related section of the Resident Assessment Instrument (ohr-interRAI), OAS, and oral health screening tool were developed as scales. The remaining studies involved scale revision, localization, and application (Table 2).
 |
Table 2 Chronological Overview of Oral Health Assessment Tools |
Dimensional Characteristics of Oral Health Assessment Tools for Older Adults
Among the 19 assessment tools included, only the oral assessment sheet (OAS) is a multidimensional assessment tool that contains three dimensions: oral hygiene, oral function, as well as biting and chewing, while the rest are unidimensional. Chen et al devised a singular-entry evaluation tool for assessing the oral health status of elderly people, specifically focusing on the question, “Do you have regular dental checkups?”.28 The number of unidimensional entries varied from 8 to 12, with a predominant number of research utilizing 8 items to evaluate oral health. Henriksen developed the Mucosal Plaque Index as a means of evaluating oral hygiene in elderly individuals, with the intention of having it administered by a dentist. Simpelaere et al subsequently conducted a study to confirm the reliability of this oral health assessment tool when used by speech pathologists. In contrast, the remaining oral health assessment tools were evaluated by professionals from non-dental backgrounds. A total of nineteen studies were carried out, comprising five studies in nursing homes, two studies in hospitals, six studies in care setting, four studies in the community, one study performed in both a nursing home and care setting, and one study performed in both a nursing home and community. (See Supplementary File: Basic Characteristics of Oral Health Assessment Tool).
Reliability of Oral Health Assessment Tools for Older Adults
The oral health assessment tools used in this study were developed, localized for use in the elderly population, and validated for reliability. Eight studies had a small sample size of less than 100 participants. A total of eleven studies underwent assessment to determine their reliability and validity. Among these, two studies were only evaluated for validity, while their reliability was not assessed. Conversely, seven studies were solely examined for reliability, without undergoing validity testing. Simpelaere et al conducted a series of reliability validation studies, including inter-rater agreement, test-retest reliability, and internal-rater agreement assessments.30 A total of 17 inter-rater reliability tests were undertaken, while 7 research focused on test-retest reliability and another 7 studies examined intra-rater reliability. Validity tests were not conducted in six studies, and the detailed information is shown in Table 3.
 |
Table 3 Reliability and Validity of Included Studies |
Discussion
The development of aging is often accompanied by many chronic diseases, which, together with the cumulative nature of oral diseases, increases the risk of rapid deterioration of oral health in elderly adults. Studies have shown that low levels of oral health are associated with poor health outcomes, and the WHO has suggested that oral health is an essential determinant of quality of life, overall health, and well-being.43 The present study conducted a comprehensive analysis of oral health assessment tools for older individuals by including 19 research via a scoping review. The primary objective was to elucidate the psychosocial characteristics of these tools, therefore establishing a theoretical foundation for the evaluation of oral health in the elderly population.
This review found that scholars from 13 countries have conducted studies on oral health assessment tools for elderly adults, covering a wide range of geographic areas, suggesting that scholars around the world are becoming more involved in managing the oral health of these individuals. This study demonstrates that the Oral Health Assessment Tool (OHAT), as revised by Chalmers et al, is the most often utilized instrument for evaluating oral health among elderly people.27 This tool was developed by elaborating the Brief Oral Health Status Examination (BOHSE) originally developed by Kayser-Jones et al.24 OHAT has been cross-culturally adapted by scholars from multiple countries, including China, Germany, Italy, Portugal, Turkey, the Netherlands, Belgium, and Japan.
Oral health assessment tools for elderly individuals are unidimensional, and multidimensional oral health assessment for the elderly is required. The study comprised 19 oral health assessment tools for the elderly, 18 of which were unidimensional, with the most often appearing items being lips, tongue, gingiva and tissues, saliva, masticatory posture, oral hygiene, and denture. The WHO suggests that oral health in elderly individuals primarily includes oral problems, such as tooth loss, dental caries, periodontal disease, dry mouth, denture-related disease, and inflammatory periodontal disease. These concerns are consistent with the current components of the Oral Health Assessment Tool for elderly individuals.44 The WHO has broadened the scope of health by incorporating the notion of well-being and integrating social well-being into its definition. Consequently, this expansion has also covered the elements of oral health.45 Oral health, as part of overall health, should not be focused solely on oral health issues. The socio-environmental paradigm has been introduced to acknowledge the state of health as including optimal functioning, as well as social and psychological well-being.46 Oral health may be described as the state of having a dentition that is both pleasant and functional, enabling individuals to maintain their intended social responsibilities without hesitation.47 Single-dimensional oral health assessment tools for the elderly have overemphasized physiological elements while ignoring social and psychological dimensions. Yanagisawa et al developed an Oral Health Assessment Form that contains three dimensions of oral hygiene, namely biting, chewing, and oral function, but does not address the social and psychological dimensions.32 Therefore, there is a need to develop multidimensional oral health assessment tools for elderly individuals to comprehensively assess their oral health status.
The Oral Health-Related Quality of Life Assessment Scale is a tool to assess the impact of oral health status on daily life in elderly individuals. The Oral Health Impact Profile (OHIP) is the most widely used oral health-related quality of life scale, which is based on Locker’s conceptual model and consists of seven dimensions, including functional limitations, physical pain, psychological discomfort, physical disability, psychological disability, social disability, and handicap.48 When designing a comprehensive assessment tool for oral health in the elderly population, it is important to differentiate it from the Oral Health-Related Quality of Life Assessment Scale specifically designed for elderly individuals.
This study highlights the potential use of current oral health assessment tools in evaluating the oral health of elderly individuals. However, it emphasizes the need for more rigorous assessments to establish their reliability and validity. Reliability pertains to the extent to which a measurement lacks errors, whereas validity refers to the extent to which scores on a scale accurately depict the construct it intends to assess. To effectively evaluate the oral health status of older individuals, it is imperative to employ assessment tools that exhibit favorable levels of reliability and validity.49 The reliability of the 19 studies was evaluated by measures such as inter-rater agreement, retest reliability, and intra-rater agreement. In terms of validity, most of the research employed content validity and structural validity as assessment methods. Seven studies conducted scale development, and only BOHSE, OHAT, OAS and DHR were validated for validity and reliability. However, it is important to note that BOHSE was not validated for intra-rater consistency and was only validated for content validity. Similarly, OHAT, OAS, and DHR were not validated for retest reliability. Lastly, DHR was solely validated for calibration validity. In the process of scale development, the validity of the MPS was not assessed, while the inter-rater agreement and intra-rater agreement of the MPS were examined. The validity of the A Single-Item for Oral Health Assessment, which constitutes the oral health-related portion of the Resident Assessment Instrument, was exclusively evaluated, while the reliability of the assessment tool was not subjected to testing. Retest reliability is a response to the stability and consistency of a test across time and can respond to the stability of the assessment results.50 This review found that only seven studies assessed the retest reliability of the Oral Health Assessment Tool for elderly individuals, and the stability of the Oral Health Assessment Tool for Older Adults needs further validation. The validity of calibration is determined by the correlation coefficient between the assessment tool and other measurement criteria. A higher correlation coefficient indicates a stronger validity of the assessment tool.51 However, it is worth noting that out of the 18 studies analyzed in this review, only 5 were able to establish calibration validity. In these cases, the dentist’s diagnosis was commonly used as the gold standard. This choice might be attributed to the absence of a widely accepted assessment instrument specifically designed for evaluating oral health in elderly individuals. Only five studies validated construct validity, which is an essential indicator for evaluating the amount to which an assessment tool’s measurement dimensions conform to the construct dimensions examined.52 Future studies need to focus on the validation of retest reliability, calibration validity, and structural validity of oral health assessment tools for elderly individuals.
However, the research found significant gaps and limitations, insufficient psychometric testing of current assessment tools in hospital settings and demographics, and the fact that none of the oral health assessment tools were designed in inpatient settings for elderly patients. In geriatric wards and outside the dental department, oral health assessments are not routinely performed, and the low priority of oral care hinders nurses from delivering desirable oral care.53 Studies have shown that poor oral health in elderly patients increases the risk of aspiration of oral bacteria into the lungs as well as local and systemic inflammation, increasing the risk of hospital-acquired pneumonia. In turn, hospital-acquired pneumonia and inflammation affect morbidity, mortality, length of stay, and hospitalization costs.54 According to a systematic review, there is evidence to show that the oral health of elderly individuals tends to decline following hospitalization.9 Maeda et al demonstrated that poor oral health on admission was an independent predictor of death during hospitalization in elderly patients and that oral health care interventions stratified according to oral health status deserve further investigation.55 Current problem-oriented medical practices largely discourage preventive care, and oral health screening should be integrated into the inpatient process to improve clinical decision-making and promote secondary and tertiary prevention of oral health and related systemic diseases.43 The Oral Assessment Guide (OAG), which was created by Anderson for the evaluation of patients undergoing chemotherapy for malignant hematological oncology, underwent testing within a hospital setting. However, it is important to note that the sample size for this tool was limited to 16 cases, with a mean age of 60.7 years. Furthermore, it is worth mentioning that the testing of the OAG focused solely on inter-rater reliability and did not include an assessment of its validity.56 Given the importance of assessing elderly hospitalized patients’ oral health and the inadequacy of current assessment tools, future research should develop a clinically applicable, psychometrically tested assessment tool. The assessment tool could then be used for patient safety management, such as oral care and medical decision-making in elderly hospitalized patients.
This review found that most of the oral health assessment tools for elderly adults in China were introduced from abroad. Zhao conducted a study on the Chinese adaptation of the BOHSE, focusing on its reliability in assessing oral health among elderly patients in the fields of respiratory medicine and cardiology.31 Similarly, Wang examined the Chinese adaptation of the OHTA, specifically targeting elderly individuals in community settings.35 Both studies concluded that the Chinese versions of the BOHSE and the OHAT are appropriate tools for evaluating the oral health status of elderly individuals in China.31,35 However, no locally developed oral health assessment tools for older adults were found during the search. In light of the variations in cultural backgrounds and living habits among elderly individuals both domestically and internationally, it is imperative to develop localized oral health assessment tools concurrently with the introduction of foreign scales. Furthermore, efforts should be made to create a multidimensional assessment tool that holistically evaluates oral health. Additionally, it is crucial to consider the specificity of the target population and conduct comprehensive reliability testing in Chinese hospitals, communities, and nursing homes for the elderly. This will ensure the development of a reliable and appropriate oral health assessment tool. The inclusion of population specificity and the implementation of a comprehensive reliability test across various healthcare settings, such as hospitals, communities, nursing homes, and other elderly groups in China, are crucial considerations. These measures are necessary to systematically develop an appropriate assessment tool for evaluating the oral health of the elderly population. By doing so, robust evidence can be generated to effectively support the management and maintenance of their oral health.
Our review also has some limitations. First, only Chinese and English literature was included, and articles in other languages were excluded. To enhance the comprehensiveness of future research, it is imperative to incorporate studies conducted in a wider range of languages. Furthermore, our research specifically concentrated on assessment tools utilized for assessing oral health in the elderly population, with a deliberate exclusion of studies pertaining to younger age groups. Additional research might be conducted on oral health evaluation techniques for children and adolescents, taking into consideration the varying study aims.
Conclusion
The maintenance of oral health is of paramount importance in relation to general health and well-being. The primary objective of this review is to examine the existing oral health assessment tools specifically designed for older adults. The findings of this study indicate that future advancements in tool development should strive to integrate social and psychological aspects. By incorporating these dimensions, it is anticipated that the overall effectiveness and precision of oral health assessment tools can be enhanced on a wider scale. The existing Oral Health Assessment Tool for Older Adults is utilized for the evaluation of oral health in the elderly population. However, it is imperative for forthcoming research endeavors to augment the sample size and integrate modeling theory to carry out meticulous assessments of reliability and validity. Moreover, there is a pressing need for the advancement of oral health assessment tools specifically tailored for elderly individuals in hospital settings to effectively cater to their oral health requirements.
Abbreviations
BOHSE, Brief Oral Health Status Examination; MPS, Mucosal-plaque Index; ROAG, The Revised Oral Assessment Guide; OHAT, The Oral Health Assessment Tool; OAS, Oral Assessment Sheet; OHSTNP, Oral Health Screening Tool for Nursing Personnel; DHR, Dental Hygiene Registration; ohr‐interRAI, the oral health‐related section of the Resident Assessment Instrument; OHAT-EP, European Portuguese version of the OHAT; OHATE, Oral Health Assessment Tool for the Elderly; OHAT-NL, The Dutch version of the Oral Health Assessment Tool; PRISMAR-ScR, the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews; CNKI, China National Knowledge Infrastructure; OSF: Open Science Framework.
Data Sharing Statement
The original contributions presented in the study are included in the article and Supplementary Material, further inquiries can be directed to the corresponding authors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Ministry of Civil Affairs. China: 2021 statistical bulletin on development of civil affairs. Available from: https://www.mca.gov.cn/n152/n166/c45021/content.html.
2. World Health Organization. Ageing and health. Available from: http://www.who.int/zh/health-topics/ageing#tab=tab_1.
3. World Health Organization. World Report on Ageing and Health. Geneva: World Health Organization; 2015. Available from. http://iris.who.int/bitstream/handle/10665/186463/9789245565048_chi.pdf?sequence=9.
4. World Health Organization. Global Oral Health Status Report: Towards Universal Health Coverage for Oral Health by 2030. Geneva: World Health Organization; 2022.
5. Murray Thomson W. Epidemiology of oral health conditions in older people. Gerodontology. 2014;31 Suppl 1:9–16. doi:10.1111/ger.12085
6. Ahmadi B, Alimohammadian M, Yaseri M, et al. Multimorbidity: epidemiology and Risk Factors in the Golestan Cohort Study, Iran: a Cross-Sectional Analysis. Medicine. 2016;95(7):e2756. doi:10.1097/MD.0000000000002756
7. Scannapieco FA, Cantos A. Oral inflammation and infection, and chronic medical diseases: implications for the elderly. Periodontol. 2016;72(1):153–175. doi:10.1111/prd.12129
8. Afshar S, Roderick PJ, Kowal P, Dimitrov BD, Hill AG. Multimorbidity and the inequalities of global ageing: a cross-sectional study of 28 countries using the World Health Surveys. BMC Public Health. 2015;15:776. doi:10.1186/s12889-015-2008-7
9. Terezakis E, Needleman I, Kumar N, Moles D, Agudo E. The impact of hospitalization on oral health: a systematic review. J Clin Periodontol. 2011;38(7):628–636. doi:10.1111/j.1600-051X.2011.01727.x
10. Hakeem FF, Bernabé E, Sabbah W. Association between oral health and frailty: a systematic review of longitudinal studies. Gerodontology. 2019;36(3):205–215. doi:10.1111/ger.12406
11. Kang MG, Jung HW. Association Between Oral Health and Frailty in Older Korean Population: a Cross-Sectional Study. Clin Interv Aging. 2022;17:1863–1872. doi:10.2147/CIA.S384417
12. Kossioni AE, Hajto-Bryk J, Maggi S, et al. An Expert Opinion from the European College of Gerodontology and the European Geriatric Medicine Society: European Policy Recommendations on Oral Health in Older Adults. J Am Geriatr Soc. 2018;66(3):609–613. doi:10.1111/jgs.15191
13. Almirall J, Serra-Prat M, Bolíbar I, Balasso V. Risk Factors for Community-Acquired Pneumonia in Adults: a Systematic Review of Observational Studies. Respiration. 2017;94(3):299–311. doi:10.1159/000479089
14. Gibney JM, Wright FA, D’Souza M, Naganathan V. Improving the oral health of older people in hospital. Australas J Ageing. 2019;38(1):33–38. doi:10.1111/ajag.12588
15. Tavares M, Lindefjeld Calabi KA, San Martin L. Systemic diseases and oral health. Dent Clin North Am. 2014;58(4):797–814. doi:10.1016/j.cden.2014.07.005
16. Chantaraboot Y, Sermsuti-Anuwat N. Factors Associated with Self-reported Oral Health Among Community-Dwelling Older Adults in a Rural Province of Thailand. J Multidiscip Healthc. 2022;15:2111–2119. doi:10.2147/JMDH.S386993
17. Rodrigues LG, Sampaio AA, da Cruz CAG, Vettore MV, Ferreira RC. A systematic review of measurement instruments for oral health assessment of older adults in long-term care facilities by nondental professionals. Gerodontology. 2023;40(2):148–160. doi:10.1111/ger.12648
18. Tricco AC, Lillie E, Zarin W, et al. A scoping review on the conduct and reporting of scoping reviews. BMC Med Res Methodol. 2016;16:15. doi:10.1186/s12874-016-0116-4
19. Canadian Institutes of Health Research. A guide to knowledge synthesis: a knowledge synthesis chapter. 2010. Accessed from: www.cihr-irsc.gc.ca/e/41382.html.
20. Tricco AC, Lillie E, Zarin W, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and Explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
21. Moher D, Schulz KF, Simera I, Altman DG. Guidance for developers of health research reporting guidelines. PLoS Med. 2010;7(2):e1000217. doi:10.1371/journal.pmed.1000217
22. Arksey H, O’malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616
23. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021:
24. Kayser-Jones J, Bird WF, Paul SM, Long L, Schell ES. An instrument to assess the oral health status of nursing home residents. Gerontologist. 1995;35(6):814–824. doi:10.1093/geront/35.6.814
25. Henriksen BM, Ambjørnsen E, Axéll TE. Evaluation of a mucosal-plaque index (MPS) designed to assess oral care in groups of elderly. Spec Care Dentist. 1999;19(4):154–157. doi:10.1111/j.1754-4505.1999.tb01378.x
26. Andersson P, Hallberg IR, Renvert S. Inter-rater reliability of an oral assessment guide for elderly patients residing in a rehabilitation ward. Spec Care Dentist. 2002;22(5):181–186. doi:10.1111/j.1754-4505.2002.tb00268.x
27. Chalmers JM, King PL, Spencer AJ, Wright FA, Carter KD. The oral health assessment tool--validity and reliability. Aust Dent J. 2005;50(3):191–199. doi:10.1111/j.1834-7819.2005.tb00360.x
28. Chia-Hui Chen C, Chyun DA, Li CY, McCorkle R. A single-item approach to screening elders for oral health assessment. Nurs Res. 2007;56(5):332–338. doi:10.1097/01.NNR.0000289504.30037.d8
29. Ribeiro MT, Ferreira RC, Vargas AM. Validity and reproducibility of the revised oral assessment guide applied by community health workers. Gerodontology. 2014;31(2):101–110. doi:10.1111/ger.12014
30. Simpelaere IS, Van Nuffelen G, Vanderwegen J, Wouters K, De Bodt M. Oral health screening: feasibility and reliability of the oral health assessment tool as used by speech pathologists. Int Dent J. 2016;66(3):178–189. doi:10.1111/idj.12220
31. Zhao CJ, Ding F. Translation and psychometric evaluation of the Kayser-Jones Brief Oral Health Status Examination. Chin Nurs Manage. 2016;16(1):38–41. doi:10.3969/j.issn.1672-1756.2016.01.011
32. Yanagisawa S, Nakano M, Goto T, Yoshioka M, Shirayama Y. Development of an Oral Assessment Sheet for Evaluating Older Adults in Nursing Homes. Res Gerontol Nurs. 2017;10(5):234–239. doi:10.3928/19404921-20170621-04
33. Tsukada S, Ito K, Stegaroiu R, Shibata S, Ohuchi A. An oral health and function screening tool for nursing personnel of long-term care facilities to identify the need for dentist referral without preliminary training. Gerodontology. 2017;34(2):232–239. doi:10.1111/ger.12255
34. Fjeld KG, Eide H, Mowe M, Hove LH, Willumsen T. Dental hygiene registration: development, and reliability and validity testing of an assessment scale designed for nurses in institutions. J Clin Nurs. 2017;26(13–14):1845–1853. doi:10.1111/jocn.13452
35. Wang JQ, Zhu SZ, Zhan Y, Li J. Reliability and validity test of Chinese version of the Oral Health Assessment Tool. Chin J Mod Nurs. 2019;25(28):3607–3610. doi:10.3760/cma.j.issn.1674-2907.2019.28.010
36. Krausch-Hofmann S, De Almeida Mello J, Declerck D, et al. The oral health-related section of the interRAI: evaluation of test content validity by expert rating and assessment of potential reasons for inaccurate assessments based on focus group discussions with caregivers. Gerodontology. 2019;36(4):382–394. doi:10.1111/ger.12421
37. Klotz AL, Zajac M, Ehret J, Hassel AJ, Rammelsberg P, Zenthöfer A. Development of a German version of the Oral Health Assessment Tool. Aging Clin Exp Res. 2020;32(1):165–172. doi:10.1007/s40520-019-01158-x
38. Finotto S, Bertolini G, Camellini R, et al. Linguistic-cultural validation of the oral health assessment tool (OHAT) for the Italian context. BMC Nurs. 2020;19:7. doi:10.1186/s12912-020-0399-y
39. Krausch-Hofmann S, Tran TD, Janssens B, et al. Assessment of oral health in older adults by non-dental professional caregivers-development and validation of a photograph-supported oral health-related section for the interRAI suite of instruments. Clin Oral Investig. 2021;25(6):3475–3486. doi:10.1007/s00784-020-03669-8
40. Cerveira FR, Matos MAC, Sa-Couto P. Development of the European Portuguese version of the oral health assessment tool: content validity and reliability study in an elderly population. Spec Care Dentist. 2022;42(6):623–629. doi:10.1111/scd.12724
41. Genç FZ, Cingil D, Hisar F. Development of the Turkish version of the oral health assessment tool: methodological study. Spec Care Dentist. 2023;43(4):416–424. doi:10.1111/scd.12775
42. van Noort HHJ, Harderwijk A, Everaars B, Akkermans R, van der Putten GJ, Waal GH. The Dutch version of the Oral Health Assessment Tool: translation and inter-rater reliability among community nurses. Int J Dent Hyg. 2023. doi:10.1111/idh.12678
43. Noetzel N, Meyer AM, Siri G, et al. The impact of oral health on prognosis of older multimorbid inpatients: the 6-month follow up MPI oral health study (MPIOH). Eur Geriatr Med. 2021;12(2):263–273. doi:10.1007/s41999-020-00427-7
44. Petersen PE, Yamamoto T. Improving the oral health of older people: the approach of the WHO Global Oral Health Programme. Oral Epidemiol. 2005;33(2):81–92. doi:10.1111/j.1600-0528.2004.00219.x
45. Baiju RM, Peter E, Varghese NO, Sivaram R. Oral Health and Quality of Life: current Concepts. J Clin Diagn Res. 2017;11(6):ZE21–ZE26. doi:10.7860/JCDR/2017/25866.10110
46. Nettleton S. The Sociology of Health and Illness. Cambridge: polity press; 1995.
47. Dolan TA. Identification of appropriate outcomes for an aging population. Spec Care Dentist. 1993;13(1):35–39. doi:10.1111/j.1754-4505.1993.tb01451.x
48. Locker D. Measuring oral health: a conceptual framework. Community Dent Health. 1988;5(1):3–18.
49. Kamper SJ. Reliability and Validity: linking Evidence to Practice. J Orthop Sports Phys Ther. 2019;49(4):286–287. doi:10.2519/jospt.2019.0702
50. Polit DF. Getting serious about test-retest reliability: a critique of retest research and some recommendations. Qual Life Res. 2014;23(6):1713–1720. doi:10.1007/s11136-014-0632-9
51. Özel Aslıyüce Y, Fanuscu A, Aslıyüce A, Ülger Ö. Tele-Assessment of Functional Capacity: validity, Intra- and Inter-rater Reliability. Workplace Health Saf. 2023;71(10):476–483. doi:10.1177/21650799231180780
52. Clark LA, Watson D. Constructing validity: new developments in creating objective measuring instruments. Psychol Assess. 2019;31(12):1412–1427. doi:10.1037/pas0000626
53. Jordan RA, Bodechtel C, Hertrampf K, et al. The Fifth German Oral Health Study (Fünfte Deutsche Mundgesundheitsstudie, DMS V) - rationale, design, and methods. BMC Oral Health. 2014;14:161. doi:10.1186/1472-6831-14-161
54. Bail K, Goss J, Draper B, Berry H, Karmel R, Gibson D. The cost of hospital-acquired complications for older people with and without dementia; a retrospective cohort study. BMC Health Serv Res. 2015;15:91. doi:10.1186/s12913-015-0743-1
55. Maeda K, Mori N. Poor oral health and mortality in geriatric patients admitted to an acute hospital: an observational study. BMC Geriatr. 2020;20(1):26. doi:10.1186/s12877-020-1429-z
56. Andersson P, Persson L, Hallberg IR, Renvert S. Testing an oral assessment guide during chemotherapy treatment in a Swedish care setting: a pilot study. J Clin Nurs. 1999;8(2):150–158. doi:10.1046/j.1365-2702.1999.00237.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Validation of the Connor-Davidson Resilience Scale-10 in South Africa: Item Response Theory and Classical Test Theory
Pretorius TB, Padmanabhanunni A
Psychology Research and Behavior Management 2022, 15:1235-1245
Published Date: 16 May 2022
Validity and Reliability of the Thai Version of the 19-Item Compliance-Questionnaire-Rheumatology
Panichaporn S, Chanapai W, Srisomnuek A, Thaweeratthakul P, Katchamart W
Patient Preference and Adherence 2022, 16:2149-2158
Published Date: 17 August 2022
Psychometric Properties of the Montreal Cognitive Assessment (MoCA) to Detect Major Neurocognitive Disorder Among Older People in Ethiopia: A Validation Study
Daniel B, Agenagnew L, Workicho A, Abera M
Neuropsychiatric Disease and Treatment 2022, 18:1789-1798
Published Date: 22 August 2022
Development and Initial Validity of the Patients’ Literacy Scale Among Outpatients in Hangzhou City, China
Jiang D, Sang T, Xiao X, Wu Z, Wang H, Yang Q
Patient Preference and Adherence 2022, 16:2483-2496
Published Date: 7 September 2022
Research and Evaluation of a Cyberchondria Severity Scale in a Chinese Context
Wang D, Sun L, Shao Y, Zhang X, Maguire P, Hu Y
Psychology Research and Behavior Management 2023, 16:4417-4429
Published Date: 1 November 2023