Back to Journals » Journal of Pain Research » Volume 19
Optimizing Osteoarthritis Management – Therapeutic Efficacy and Evaluation of Intra-Articular Triamcinolone Acetonide Injection
Authors Wan Y, Kong L ![]() , Ning R
, Ning R
Received 29 September 2025
Accepted for publication 12 March 2026
Published 23 March 2026 Volume 2026:19 571167
DOI https://doi.org/10.2147/JPR.S571167
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Alaa Abd-Elsayed
Yongqing Wan, Lingchao Kong, Rende Ning
Department of Orthopedics, The Third Affiliated Hospital of Anhui Medical University (The First People’s Hospital of Hefei), Anhui Medical University, Hefei, Anhui, 230061, People’s Republic of China
Correspondence: Lingchao Kong, Email [email protected] Rende Ning, Email [email protected]
Abstract: Osteoarthritis (OA) is a common degenerative joint disease that often leads to pain and diminished quality of life in patients. For end-stage osteoarthritis, surgical intervention remains the only effective treatment. However, for the majority of patients, surgery is not the initial consideration. The management of osteoarthritis primarily focuses on alleviating associated clinical symptoms, and rational non-surgical conservative treatment is the recommended approach for patients in the early to middle stages. Intra-articular injection therapy represents one of the most effective non-surgical treatment options, second only to oral analgesics and anti-inflammatory medications, with a lower incidence of systemic complications. Compared to surgery, it is more cost-effective and less invasive. Among these, intra-articular corticosteroid injection is a widely adopted non-surgical treatment by rheumatologists for osteoarthritis. Numerous studies have demonstrated that intra-articular corticosteroid injections can provide short-term pain relief in osteoarthritis. Triamcinolone Acetonide (TA) is one of the commonly used corticosteroids, valued for its notable anti-inflammatory and analgesic effects. It is extensively applied in intra-articular injections for osteoarthritis to alleviate pain and potentially delay disease progression. The purpose of this paper is to review the mechanism of action of Triamcinolone Acetonide, its current applications and efficacy in osteoarthritis, safety profile, and future directions, thereby providing a theoretical foundation and practical guidance for clinical management strategies in osteoarthritis.
Keywords: osteoarthritis, intra-articular injection, pharmacology, triamcinolone acetonide, ultrasound
A Letter to the Editor has been published for this article.
Introduction
OA is a highly prevalent condition worldwide and represents one of the most common musculoskeletal disorders leading to disability. According to a 2019 Lancet study, approximately 250 million people globally were affected by OA. By 2025, new research has found that this number has increased to over 500 million. The high prevalence of OA imposes a substantial socioeconomic burden. On an individual level, the pain and functional impairment associated with the disease pose significant challenges to quality of life and healthcare expenditure.1–3 Historically, OA was regarded as a condition resulting merely from mechanical wear and tear. However, emerging evidence indicates that OA is a whole-joint disorder, characterized by structural damage involving the articular cartilage, subchondral bone, ligaments, joint capsule, synovium, and periarticular muscles. Previously considered a mere consequence of mechanical wear, osteoarthritis is now recognized as a whole-organ disease involving structural damage of the articular cartilage, subchondral bone, ligaments, joint capsule, synovium, and periarticular muscles.4 It’s pathogenesis also involves dysregulation of the innate immune system, cytokine networks (IL-1β, TNF-α), synovial inflammation, and an imbalance in cartilage metabolism.5,6 Corticosteroid have anti-inflammatory effects for systemic application and can act on the entire body, which is consistent with the multi-site and multi-structural onset of OA.
Previous studies have indicated that patients with OA may continue to experience pain symptoms even after undergoing joint replacement surgery.7,8 In addition, a series of complications may also arise. Firstly, periprosthetic fractures occur at a rate of 0.3% to 2.5% following arthroplasty. This is often due to improper prosthesis positioning, excessive bone resection during surgery, or excessive postoperative activity, leading to localized stress concentration and subsequent fracture. As more arthroplasty cases are included in research, an increasing number of postoperative periprosthetic fractures have been identified and reported.9,10 Secondly, patients may develop Metal deposition syndrome within a period ranging from 6 weeks to 26 years after the initial implantation, resulting from wear or dislocation of the metal components.11 Additionally, one case study reported postoperative septic metal intoxication.12 It has been observed that the majority of patients in clinical practice seek treatment only when the disease has reached an end-stage or when the pain symptoms become unbearable. At this point, surgical intervention often becomes the last resort. However, the aforementioned studies demonstrate that even after joint replacement surgery, pain relief may not be fully achieved, studies indicate that as high as 25% of patients still report pain and mobility difficulties one year after surgery,13,14 and a range of complications may still arise. Consequently, a growing number of researchers have focused on investigating the pathogenesis of OA to identify non-surgical interventions that may delay disease progression. It is now widely recognized that OA develops as a chronic, prolonged process, progressing through mild to moderate stages before reaching the end phase. With advances in research, increasing evidence indicates that the mild to moderate stages represent a critical window for therapeutic intervention. Targeting the early phases of OA with proactive and tailored non-surgical management is considered a first-line treatment strategy. Such approaches can alleviate the disease burden before OA progresses to severe osteophyte formation, joint space narrowing, cartilage destruction, significant functional impairment, and persistent chronic pain.15–18 Current non-surgical treatment strategies include foundational therapies, topical agents, oral medications, intra-articular injections, and biologics. Among these, intra-articular injections are widely utilized in early to moderate OA due to their low systemic adverse effects, potent localized action, cost-effectiveness compared to surgery, and minimal invasiveness. This modality has proven to be a highly effective approach for managing OA. Commonly injected agents include hyaluronic acid, stem cells, platelet-rich plasma (PRP), and corticosteroids.18
However, among the aforementioned therapies, hyaluronic acid has been demonstrated in studies to provide only a modest reduction in pain compared to placebo, while also increasing the risk of serious adverse events, suggesting that the perceived pain relief by patients lacks clinical significance,19,20 studies also suggest that intra-articular injection of corticosteroid not only provides short-term analgesic effects compared with intra-articular hyaluronic acid, but also demonstrates more pronounced efficacy in patients with severe pain.21,22 The European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO) working group recommends that intra-articular hyaluronic acid should be avoided when patients have contraindications to non-steroidal anti-inflammatory drugs (NSAIDs) or continue to experience symptoms despite NSAIDs use.23 PRP is limited by insufficient durability of efficacy, unclear advantages in safety, and low cost-effectiveness. Furthermore, it is not suitable for all OA patients or disease stages, and the definition of the optimal candidate population remains unclear.24 Stem cell therapy, as an emerging treatment modality, is constrained by high costs, uncertain therapeutic outcomes, and potential adverse effects such as pain, swelling, and immune reactions.25–28 In comparison, corticosteroid injections have the longest history of use,29 and intra-articular and periarticular glucocorticoid injections are common in sports medicine.30 According to the ESCEO 2019 algorithm, intra-articular corticosteroids serve as an effective alternative to oral NSAIDs and are particularly suitable for patients with knee joint effusion (though evidence remains limited).31 It is recommended that injections be administered no more than 2–3 times per year, with intervals between injections not shorter than 3–6 months.32 Studies have shown that intra-articular corticosteroid injections can rapidly alleviate pain within two weeks and exhibit a range of anti-inflammatory mechanisms. Their application is not only historically validated but also meets patients’ needs for symptomatic pain relief, while their anti-inflammatory effects align with the pathogenesis of OA. For OA patients, pain is often the most typical clinical symptom. Corticosteroids such as TA, methylprednisolone acetate, prednisolone acetate, and betamethasone are used in the treatment of OA patients and demonstrate favorable anti-inflammatory effects. However, studies indicate that TA is more effective and has a longer duration of action in terms of analgesia compared to other corticosteroids.33,34 Therefore, TA is frequently employed in OA management.
This article provides a systematic review of the pharmacodynamics, pharmacokinetics, clinical efficacy, and safety of TA and its sustained-release formulations in the treatment of systemic OA. It also explores the potential for their combination with other therapeutic agents, aiming to offer an evidence-based foundation for clinical practice.
Pharmacological Properties of Triamcinolone Acetonide
Chemical Structure
The molecular structure of TA is derived from hydrocortisone through several chemical modifications. These include the introduction of a fluorine atom at the C9α position, the formation of a double bond between C1 and C2, and the addition of a 16-α-hydroxyl group (Figure 1). The fluorine atom and hydroxyl group enhance the compound’s binding affinity to hormone receptors, while the double bond further strengthens receptor interaction and retards metabolic clearance.35,36 As a result of these structural modifications, TA exhibits prolonged anti-inflammatory and analgesic effects compared to other corticosteroids, which is attributed to its altered pharmacokinetic profile.33,34
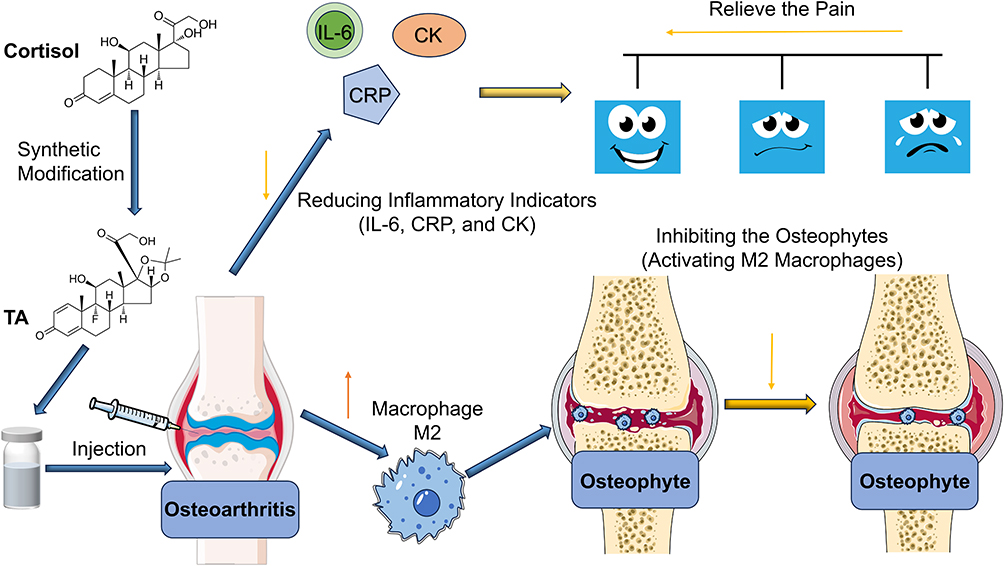 |
Figure 1 The molecular structure of triamcinolone acetonide is based on that of hydrocortisone, with specific chemical modifications. When formulated and injected into the human knee joint, it alleviates pain by reducing inflammatory indicators and also decreases osteophyte formation through increasing the population of M2 macrophages. |
Mechanism of Pharmacological Action
Anti-Inflammatory Effect: Inhibits Inflammatory Mediator Production and Reduces Inflammatory Cell Infiltration
The beneficial effects of glucocorticoid (GC) injections are thought to be primarily attributable to their anti-inflammatory properties.37 As a potent anti-inflammatory agonist, GCs act on immune cells by stimulating the bone marrow to increase granulocyte production, while simultaneously inhibiting neutrophil apoptosis and their migration through the vasculature to sites of inflammation or infection. Additionally, GCs suppress the activity of other immune cells such as monocytes, lymphocytes, and mast cells.36,38 In terms of inflammatory mediators, GCs inhibit phospholipase A2, thereby reducing the release of pro-inflammatory derivatives of arachidonic acid, including interleukin-1 (IL-1), IL-2, interferon-γ, and tumor necrosis factor (TNF). They also diminish the synthesis of prostaglandins and leukotrienes, contributing to their anti-inflammatory effects.36,39 As a synthetic glucocorticoid, TA exerts anti-inflammatory actions similar to those of other corticosteroids. Upon binding to and activating the glucocorticoid receptor, TA induces an anti-inflammatory response characterized by downregulation of pro-inflammatory cytokine expression, inhibition of prostaglandin and leukotriene synthesis, and suppression of arachidonic acid release. Concurrently, it activates anti-inflammatory transcription factors such as lipocortin-1.35,40 Previous studies have indicated that lipocortin-1 can be induced by glucocorticoids, suppresses the production of the inflammatory mediator nitric oxide in synovial macrophages, thereby alleviating arthritis inflammation, and plays a significant anti-inflammatory role in neutrophil-mediated joint inflammation by regulating their migration and activation. Moreover, lipocortin-1 is not only a key mediator of glucocorticoid action but also possesses intrinsic anti-inflammatory functions, its effect may be mediated through cellular surface receptors or external secretion signaling pathways.41,42 However, the cited studies are relatively dated, and recent research on the impact of lipocortin-1 on the pathophysiological mechanisms of osteoarthritis remains limited. We hope that future studies will provide further supplementation and more detailed explanations in this regard. TA exerts an inhibitory effect on synovial inflammation but does not significantly affect synoviocytes. Sherman was the first to systematically evaluate the response of synovial cells to pharmacological treatment by culturing synovial explants in medium containing TA. Observations at 1 and 7 days revealed no significant decrease in synovial explant viability, indicating that TA did not markedly influence synoviocyte viability or metabolic activity.43
Furthermore, TA exhibits analgesic effects through anti-inflammatory mechanisms. Previous studies have reported that OA can trigger the release of IL-6, leading to local inflammation at the injury site, along with elevated levels of C-reactive protein (CRP), a key inflammatory marker.44–46 Serum CRP levels have also been associated with the severity of pain in OA.47 Creatine kinase (CK), an energy-producing enzyme located in mitochondria and predominantly found in muscle tissue, has been demonstrated to increase in response to muscle inflammation or injury.48 A single-center retrospective cohort study revealed that patients treated with TA injections exhibited lower levels of CRP and CK compared to those who did not receive such treatment.49 Therefore, it can be concluded that TA, as a systemic therapeutic agent, alleviates OA-related pain and mitigates inflammatory progression by reducing these inflammatory biomarkers (Figure 1).
Immunosuppressive Effect: Inhibits Osteophyte Formation
Macrophages are critically involved in osteophyte formation, as studies have shown that selective depletion of synovial macrophages in two collagenase-induced mouse osteoarthritis models significantly reduces the formation of joint osteophytes.50,51 The polarization of synovial macrophage subtypes plays a critical role in the progression of OA.6 Studies have demonstrated that the three subtypes of M2 macrophages exhibit an anti-inflammatory phenotype and contribute to tissue repair and remodeling.52,53 Previous transgenic studies in mice with polarized M1 and M2 macrophages revealed that M1 macrophages accelerate OA progression, whereas M2 macrophages attenuate disease development.54 M1 macrophages secrete pro-inflammatory cytokines (such as TNF-α, IL-1β), exacerbating inflammation and cartilage destruction; whereas M2 macrophages promote tissue repair by secreting TGF-β, IL-10, and other factors. When macrophages are biased toward the M1 phenotype, it leads to an imbalance in polarization, resulting in persistent inflammation, cartilage degeneration, and osteophyte formation, thereby further exacerbating the symptoms and structural damage of osteoarthritis.55 In an in vitro study, Utomo demonstrated that corticosteroids suppress M1 macrophage polarization by downregulating pro-inflammatory cytokines such as interferon-γ and TNF-α, while promoting M2 macrophage polarization through the upregulation of anti-inflammatory cytokines including IL-4 and IL-10.56 In a combined in vivo and in vitro study, TA was shown to induce macrophage activation and differentiation, thereby inhibiting osteophyte formation. Siebelt quantified macrophage activation via intra-articular TA injection in a rat OA model and complemented these findings with in vitro assays characterizing M1 and M2 polarization through surface receptor expression. In vitro macrophage cultures demonstrated that TA strongly induces monocyte differentiation into CD163⁺ and FRβ⁺ regulatory macrophages. Furthermore, TA-stimulated M2 macrophages exhibited enhanced IL-10 expression at the mRNA level (Figure 2). Comparative analyses between TA-injected experimental groups, untreated healthy controls, and normal saline (NS)-injected groups indicated that only TA specifically activated M2 macrophages, leading to suppression of osteophyte formation.33
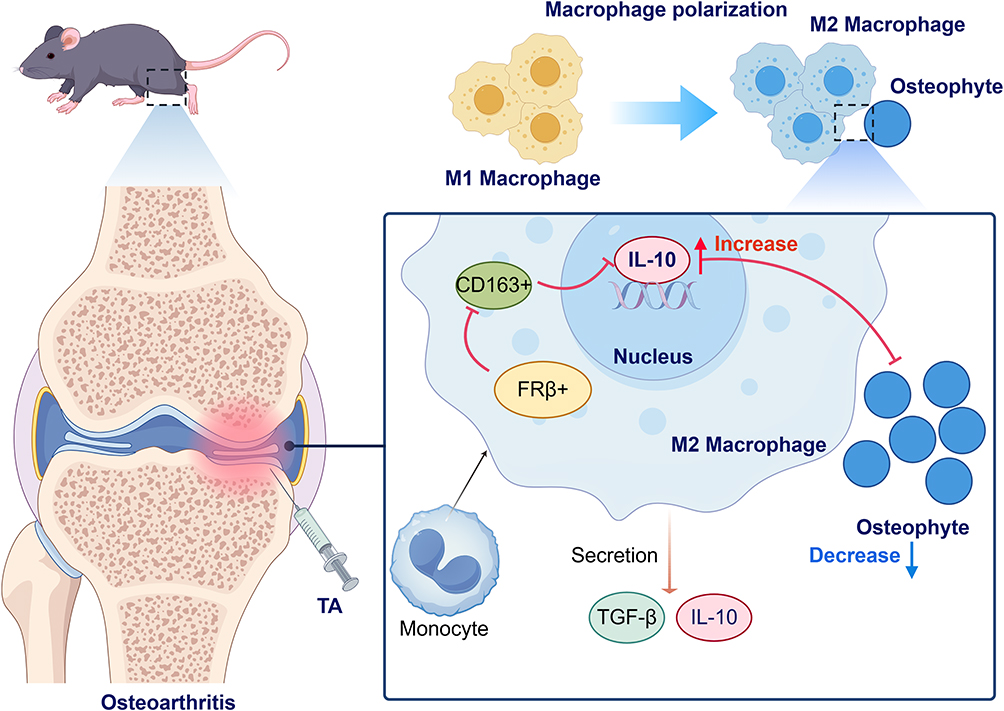 |
Figure 2 After intra-articular injection of triamcinolone acetonide into the mouse knee joint, a robust induction of monocyte differentiation into CD163+ and FRβ+ regulatory macrophages was observed. Furthermore, TA-stimulated M2 macrophages exhibited enhanced IL-10 expression at the mRNA level, and these M2 macrophages suppressed osteophyte formation. In addition, M2 macrophages promoted tissue repair through the secretion of TGF-β and IL-10. |
Analgesic Effect: Animal Studies
Preclinical studies conducted in both small and large animal models have demonstrated that TA exerts certain analgesic effects in animals with OA. In rats subjected to OA induced by medial meniscectomy, joint pain was characterized using a dynamic weight-bearing test during jumping. The right/left hind paw pressure ratio significantly decreased to approximately 66% beginning on postoperative day 7 and remained at this level through day 90. However, in the group of OA-induced rats treated with the triamcinolone acetonide extended-release microsphere formulation FX006 (Zilretta), the pressure ratio recovered to 96% at 15 days post-surgery (8 days post-administration), showing no significant difference compared with that of the healthy control group.57 These findings reveal its capacity to elicit analgesic effects within a short-term period. In a canine model of intra-articular hip injection, Alves observed that administration of TA (n=20) resulted in significantly greater improvements in weight-bearing, pain (with sustained relief lasting 118.6 days vs 8.4 days), and functional outcomes over a 6-month period compared with NS (n=20). The anti-inflammatory effect of TA was supported by a marked reduction in synovial fluid IL-1β levels at 8 days post-injection (P=0.04) and lower joint temperatures as measured by thermography (P<0.01). However, possibly due to the generally higher physical activity levels in dogs, the duration of therapeutic benefits—including weight-bearing capacity, pain relief, and joint function—was limited to 90 days in canines, in contrast to the sustained effects of up to 7 months reported in human studies.58 Despite these interspecies variations, the findings collectively indicate that intra-articular TA injection can ameliorate pain and improve joint function in both animal and human subjects. In horses with distal tarsal joint osteoarthritis, intra-articular administration of TA resulted in short-term improvement of lameness attributable to osteoarthritis.59,60 In another in vivo equine study, pain responses to passive flexion and joint effusion of the metacarpophalangeal joint were assessed using a 4-point grading scale (0 = none, 1 = mild, 2 = moderate, 3 = severe). Although TA was assigned to the control group in this study, intra-articular injection of TA into the metacarpophalangeal joint yielded significantly lower effusion scores at the one-week follow-up compared to baseline (p < 0.001), and passive flexion scores were significantly reduced at both one week (p < 0.001) and two weeks (p < 0.001) post-injection.61
Effects on Cartilage
Plasma serine protease-activated protein C (APC) has been demonstrated to be synthesized by human chondrocytes at sites of pathological cartilage fibrillation. In vitro studies have shown that APC acts synergistically with IL-1β to promote the degradation of articular cartilage, an effect that can be inhibited by corticosteroids.62 Porter and his team further corroborated these findings through in vivo experiments, in which cartilage was harvested from the femoral condyles and patellar groove of the knee joints of young healthy cattle (1–2 months old). IL-1β was employed to simulate acute or persistent inflammation, and the effects of physiological doses of TA (1 nM–200 μM) on cartilage metabolism were evaluated. The results indicated that, in the short term (2 days), TA did not affect chondrocyte viability or proliferation, irrespective of the presence of IL-1β. While short-term treatment with IL-1β alone reduced glycosaminoglycan (GAG) synthesis by 30% and collagen synthesis by 60%, treatment with any physiological dose of TA neither inhibited the rate of GAG synthesis nor accelerated it in inflamed cartilage. Instead, TA rescued IL-1β-induced GAG loss, thereby preventing degradation of the cartilage extracellular matrix. Even under long-term treatment (10–14 days), TA exhibited no effect on chondrocyte viability or the synthesis of GAG or collagen. This experiment demonstrates that, although physiological doses of TA are unable to restore cartilage synthesis, they can mitigate matrix degradation in an inflammatory environment through anti-catabolic mechanisms. Moreover, both short-term and long-term TA treatments are relatively safe, with no evident chondrotoxicity.63 In Klocke’s study, a cohort of 80 patients with symptomatic knee osteoarthritis (KOA) who received an intra-articular injection of 40 mg TA combined with 4 mL of 1% lidocaine, comparisons were made between baseline and 3-week post-injection levels of urinary C-terminal telopeptide of type II collagen (uCTX-II), a biomarker of cartilage metabolism, and serum cartilage oligomeric matrix protein (sCOMP), another cartilage metabolic marker. The results showed a significant reduction in uCTX-II at 3 weeks post-injection (349.9 vs 306.3 ng/mmol, p = 0.002), along with a downward trend in sCOMP. The decrease in these cartilage catabolic biomarkers suggests that intra-articular TA may potentially inhibit cartilage degradation in the short-term following injection.64
Previous studies have demonstrated that intra-articular application of TA exerts toxic effects on cartilage from three perspectives: chondrocyte viability, oxidative stress, and gene expression. TA was shown to reduce chondrogenic gene activity in a dose-dependent manner. Measurements taken at 7 and 14 days after injection of 1, 5, and 10 mg/mL of TA revealed cartilage viability rates of 75.43%/70.10%/66.07% and 78.30%/68.55%/66.05%, respectively. Furthermore, TA induced oxidative stress, as indicated by a significant increase in the ratio of oxidized glutathione to total glutathione with rising TA concentrations. In terms of gene expression, TA significantly upregulated the mRNA levels of P21, GDF15, and c-Fos, suggesting that its toxic effects may be mediated through pathways involving cell cycle regulation and apoptosis. However, when comparing the total glutathione levels measured with TA treatment alone versus those with additional vitamin C at concentrations of 0 mg/mL (0.087±0.025 vs 0.089±0.023), 1 mg/mL (0.394±0.12 vs 0.129±0.048), and 5 mg/mL (0.517±0.135 vs 0.123±0.031, P=0.025), it was found that the application of antioxidants such as vitamin C could ameliorate TA-induced cartilage damage.65 This provides insights that such an approach may potentially serve as a remedial measure, though further experimentation is required for comprehensive summarization and validation. Dragoo utilized a bioreactor equipped with a continuous infusion pump simulating synovial fluid metabolism to administer a single dose of 5 mg of TA to human chondrocytes in vitro. In an experimental setup where the duration of exposure was individually determined for TA and four other corticosteroid groups, TA exhibited a mean exposure time of 14 days. Compared to the 14-day medium control, this single TA dose resulted in a significantly reduced chondrocyte viability (10.2% ± 1.3% vs 4.8% ± 0.9%; P = 0.0049), demonstrating significant cytotoxic effects. To account for the potential influence of culture duration on cell survival, a subsequent experiment standardized the exposure time to 14 days for all five corticosteroid groups. Under these uniform conditions, TA showed only a trend towards cytotoxicity (9.2% ± 3.4% cell death vs 4.6% ± 2.4% cell death; P > 0.05), which was not statistically significant. The authors suggest that this lack of significance may be attributed to increased variability when comparing multiple drugs concurrently, potentially diluting the effect. Nevertheless, Dragoo’s findings indicate that, although the effect may be weaker under controlled conditions, the toxic effect of TA on chondrocytes is authentic.66 Taken together, the role of the agent in modulating chondrocytes remains contentious based on the aforementioned mechanistic studies, with dosage and duration of administration emerging as two critical factors underlying the controversy. However, discrepancies among study findings preclude a unified conclusion regarding the optimal dosing and timing, underscoring the need for further investigation.
Another study has reported an association between cartilage defects and joint pain. The researchers utilized magnetic resonance imaging (MRI) to observe cartilage morphological features in 294 participants initially free of radiographic knee osteoarthritis (KOA) over a six-year period. They assessed both full-thickness cartilage loss and loss of cartilage area, and correlated these findings with the Knee Injury and Osteoarthritis Outcomes Score (KOOS) questionnaire. The results indicated that each one-point increase in the score for full-thickness cartilage loss was associated with a 1.04-point decrease in the KOOS score. Full-thickness cartilage defects were found to be associated with joint pain, whereas cartilage area loss showed no significant correlation.67 Ishijima conducted molecular biomarker testing on serum and urine samples from 30 patients with Kellgren-Lawrence Grade (KL) 1 and 16 patients with KL grade 2 knee osteoarthritis. The serum biomarkers included the Serum Cartilage Type II Collagen Cleavage by Collagenase (sC2C, a marker of degradation) and the Serum Cartilage Type II Procollagen Carboxy Propeptide (sCPII, a marker of synthesis). Urinary biomarkers measured were uCTX-II (indicating cartilage degradation) and Urinary Bone N-terminal Crosslinking Telopeptide of Type I Collagen (uNTx, a marker of bone resorption). When patients were stratified by the presence of pain, irrespective of KL grade, levels of sC2C, sCPII, and uCTX-II were significantly elevated, suggesting that pain is associated with increased cartilage metabolism and enhanced bone resorption. Upon stratification by both KL grade and pain status, KL grade 1 patients with pain exhibited significantly higher sC2C and sCPII levels, whereas KL grade 2 patients with pain showed significantly elevated uCTX-II levels and an increased uCTX-II/sCPII, suggesting that pain at different stages of KOA may be associated with distinct patterns of tissue metabolic abnormalities. However, cartilage has no nerves, the authors propose that pain may arise indirectly through cartilage structural changes leading to alterations in joint mechanics and stress at the bone-cartilage interface, which subsequently stimulate nerve endings and result in pain perception.68 This provides us with new insights, suggesting that cartilage regeneration may be associated with pain relief, which could offer a novel therapeutic direction for OA pain management. However, more comprehensive trials are needed to provide evidence-based support for clinical application. Additionally, while the analgesic effect of TA is well-established, its potential chondrotoxicity remains controversial, indirectly indicating that its pain-relieving effect is primarily mediated through anti-inflammatory mechanisms rather than direct action on cartilage.
Pharmacokinetic Characteristics
Understanding the pharmacokinetics of intra-articular TA administration is crucial for assessing its efficacy and safety in OA treatment.
Blood Concentration and Time to Onset After Administration
In the equine intercarpal (IC) and sacroiliac (SI) joints, 18 mg of TA was administered respectively. It was observed that the peak plasma concentration in the IC group was significantly higher than that in the SI group (1.61 vs 0.70 ng/mL, p < 0.01), although both groups reached peak concentrations at 8 hours. Furthermore, TA concentrations in the IC group remained significantly higher than those in the SI group from 8 to 36 hours.69 Similarly, in equine studies conducted by Soma et al, it was demonstrated that TA exhibits distinct pharmacokinetic profiles depending on the route of administration—intravenous (IV), intramuscular (IM), and intra-articular (IA). The study indicated that TA follows a three-compartment model for both IM and IA administration, while a two-compartment model applies to IV administration. Regarding half-life: the median distribution half-life after IV administration was 0.50 hours (range: 0.24–0.67 hours), whereas the transfer half-life of TA from the joint to plasma following IA administration was 5.2 hours (range: 0.49–7.3 hours). In terms of elimination half-life, IA administration resulted in a significantly longer duration compared to IV administration (23.8 hours vs 6.1 hours). As for maximum plasma concentration (Cmax): the Cmax after IA administration was 2.0 ng/mL (range: 0.94–2.5 ng/mL), achieved at 10 hours (range: 8–12 hours), while IM administration yielded a Cmax of 0.34 ng/mL (range: 0.20–0.48 ng/mL), reached at 13.0 hours (range: 12–16 hours).70 These differences suggest that IA administration may result in a longer duration of action in the body compared to IV administration, while demonstrating a more potent concentration efficacy relative to IM injection. In light of these comparisons, IA administration is the more preferable approach for the treatment of OA. Although the experimental data presented above were not directly derived from human studies, findings from other mammalian species may still offer valuable translational insights.
Metabolism and Clearance within the Joint
Following intra-articular injection of 40 mg TA into the shoulder joint, a significant decrease in urinary TA concentration was observed starting 1week post-injection, becoming nearly undetectable by day 45.71 Triamcinolone Hexacetonide (THA), an ester of TA, is frequently administered via the intra-articular route. Even if a small fraction of the administered dose reaches the systemic circulation, plasma esterases are expected to rapidly hydrolyze THA into TA. Coll et al investigated the elimination of THA and its metabolites in human urine and plasma following a single intra-articular hip injection, with the detection of TA metabolites in urine representing a novel exploration. In OA patients (n=8) receiving a single 40 mg THA injection, urinary elimination of THA peaked at 48 hours and remained detectable until day 23; plasma concentrations peaked between 24 and 28 hours and were detectable until day 10. After intra-articular THA administration, only TA metabolites (not THA or new metabolites) were detected in urine, whereas both THA and TA were detected in plasma, leading to the consideration that plasma THA serves as direct evidence of intra-articular administration.72 When comparing plasma samples collected over the same timeframe after intra-articular injections of TA (10 mg, 20 mg, and 40 mg) and THA (20 mg and 40 mg), the terminal half-life of THA was determined to be 4.6 days, while that of TA ranged between 3.2 and 6.4 days. Regarding systemic clearance, the total clearance for TA at 10 mg, 20 mg, and 40 mg doses was 66.7 L/h, 38.8 L/h, and 62.9 L/h, respectively. For THA, the total clearance was 75.0 L/h and 67.5 L/h at the 20 mg and 40 mg doses, respectively. Both TA and THA were completely absorbed, albeit with slightly different absorption rates; approximately 35% to 40% of THA was absorbed from the joint within 3 days of intra-articular administration, compared to 58% to 67% for TA. The mean residence time within the joint also differed, being only 3.2–4.3 days for TA compared to 6 days for THA35,73 (Table 1). This longer intra-articular residence time of THA underscores its potential for intra-articular therapy in the management of osteoarthritis.
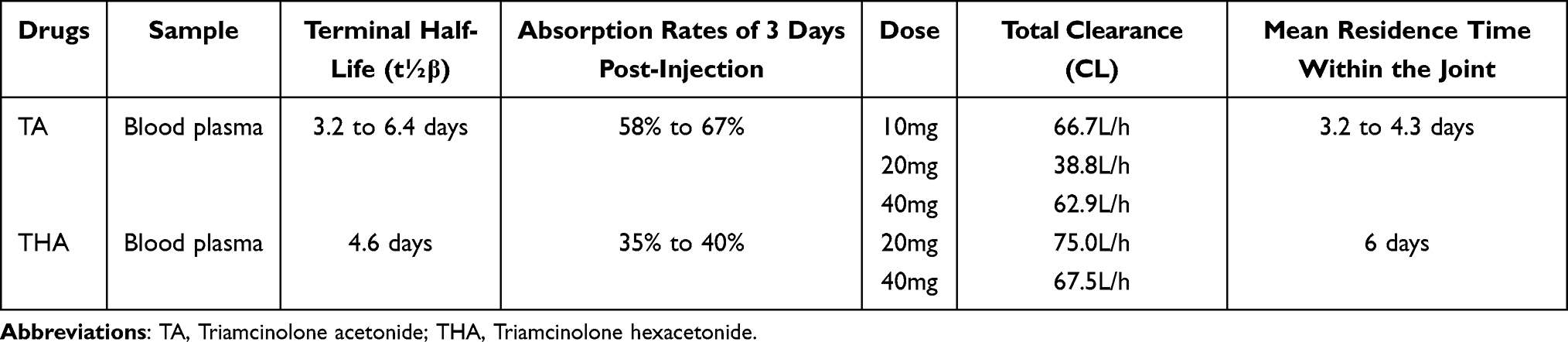 |
Table 1 Comparison of TA and THA Metabolism and Clearance Within the Joint |
Efficacy of Novel TA-Loaded Formulations
In recent years, there has been increasing exploration and application of novel formulations of TA. When FX006, an extended-release microsphere formulation of TA, was administered via intra-articular injection into the knee at doses of 16 mg and 32 mg, the median time to onset of analgesic effect was similar for both doses (Day 4) and occurred earlier than that observed with saline placebo (Day 8). The maximum analgesic effect for both FX006 16 mg and 32 mg was achieved at Weeks 4–5.74 In a Phase IIa clinical study, eligible patients with bilateral knee osteoarthritis received simultaneous unilateral injections of either TA extended-release (TA-ER) 32 mg or conventional TA 40 mg into each knee. The time to peak plasma concentration was 4.5 hours for TA compared to 6.5 hours for TA-ER. Furthermore, systemic exposure, as measured by the area under the concentration-time curve (AUC), was lower for TA-ER than for TA.75 Following intra-articular injection into the hip, the maximum plasma concentration of TA-ER was significantly lower than that of triamcinolone acetonide crystalline suspension (TAcs) (geometric mean: 890.4 pg/mL vs 5549.4 pg/mL). Systemic exposure (AUC) was also significantly lower for TA-ER compared to TAcs. TA-ER demonstrated a more stable plasma concentration profile and a longer mean residence time.76
FXOO6 was developed by Flexion Therapeutics in 2017 (development code: FX006, trade name: Zilretta) and received FDA approval for marketing (National Drug Code: 70801–003-01, Flexion Therapeutics, Burlington, MA, USA).57 However, the prescribing information (FDA-approved labeling) for FX006 (Zilretta) does not list Kellgren-Lawrence (KL) grade as an absolute restriction for its use. The sustained-release properties of the novel TA-loaded material prolong intra-articular drug retention, enabling longer-lasting symptomatic improvement, reduced injection frequency, and minimized systemic exposure, thereby supporting its potential as an optimized non-surgical therapeutic option for OA.
Clinical Application of TA in Osteoarthritis
Commonly Injected Joints (Hip, Knee, Hand, Shoulder) and Clinical Efficacy Assessment (Figure 3)
Efficacy of Hip Joint Intra-Articular Injection
In a six-month comparative trial conducted by Kigozi, patients with hip OA were allocated to either basic conservative treatment (BCT) alone (n=66) or BCT combined with ultrasound-guided intra-articular injection of 40 mg TA and 4 mL of 1% lidocaine (BCT+US-T) (n=67). The study revealed that the BCT group required a greater number of specialist consultations (+0.14 visits) and private physiotherapy sessions (+0.33 sessions), and underwent more hip surgeries (2 vs 0) compared to the BCT+US-T group. Additionally, the mean number of sick leave days due to hip pain was significantly higher in the BCT group than in the BCT+US-T group (6.25 days vs 1.39 days). The average cost of treatment interventions was also greater in the BCT group (£327.5) relative to the BCT+US-T group (£165.8).77 In conclusion, this trial demonstrates that the combined BCT and US-T approach resulted in superior therapeutic outcomes and lower costs, indicating that TA injection significantly improves pain relief and functional outcomes in patients with hip OA.
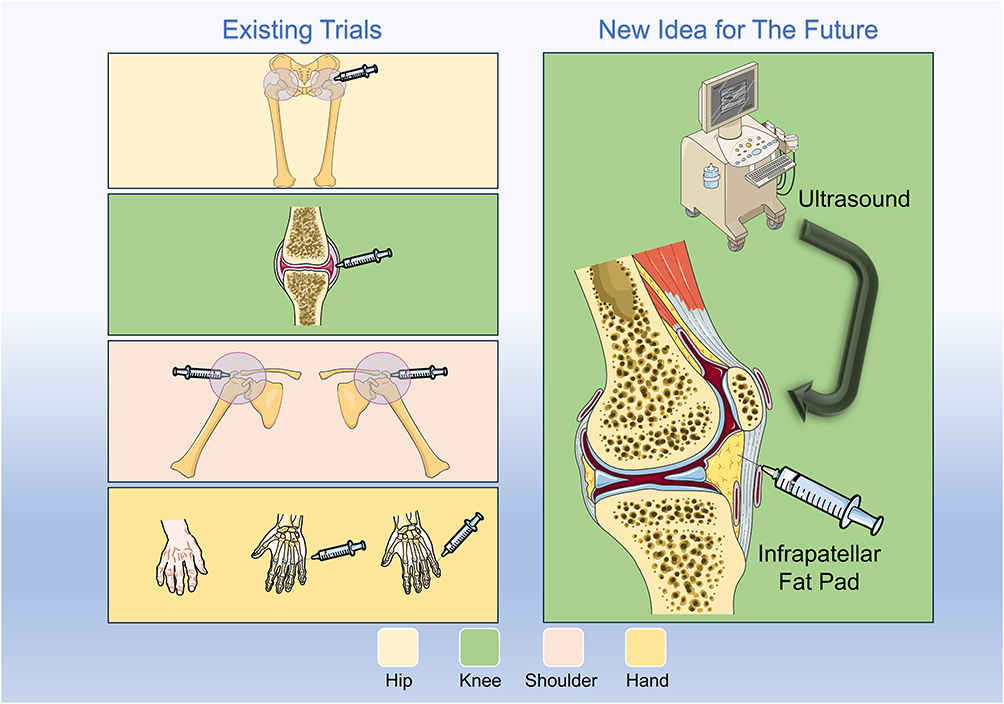 |
Figure 3 This article discusses the efficacy of triamcinolone acetonide injections in the Hip, knee, shoulder, and hand joints. Future research could explore ultrasound-guided injections into the infrapatellar fat pad for the knee joint. |
In addition to its ability to alleviate pain in patients with hip OA prior to surgery, a single-center retrospective cohort study has also highlighted the significance of TA administration during total hip arthroplasty.49 In the periarticular analgesic injection (PAI) group, a 41-mL mixture comprising 20 mL of 5 mg/mL levobupivacaine, 1 mL of 40 mg/mL TA, and 20 mL of NS was injected into 87 hip joints after prosthesis implantation and before wound closure. In contrast, 113 hip joints in the control group underwent total hip arthroplasty without PAI intervention. The PAI group exhibited significantly lower Numerical Rating Scale (NRS) scores than the control group on both the first and second postoperative days (3.8 vs 4.7 and 2.2 vs 2.3, respectively). Although the potential confounding effect of local anesthetics on pain reduction must be considered, previous studies have reported that PAI with levobupivacaine and/or epinephrine did not significantly reduce postoperative pain following total hip arthroplasty,78,79 underscoring TA’s role in rapid analgesia. Importantly, on postoperative day 7, D-dimer levels were significantly lower in the PAI group (3.9±1.8 vs 6.3±2.1), suggesting corticosteroid PAI might promote early mobilization, thereby prevent elevated D-dimer levels and potentially reduce deep vein thrombosis risk49 (Table 2).
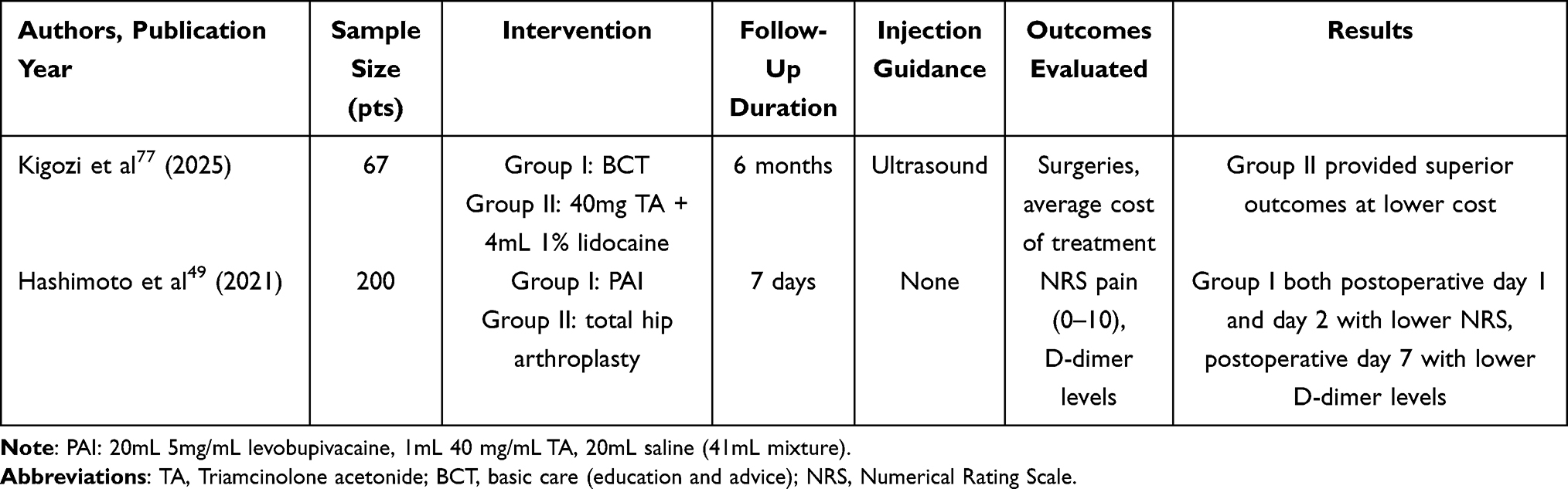 |
Table 2 Summary of the Efficacy of TA Hip Joint Intra-Articular Injection |
In reality, the actual cost of TA is relatively low. According to the analysis of Kigozi’s trial, the BCT+US-T group of patients maintained longer working periods while saving £450 in societal productivity costs.77 Hashimoto’s study demonstrated that the use of TA during total hip arthroplasty provides rapid postoperative analgesia and helps prevent thrombosis.49 Furthermore, the American Academy of Orthopaedic Surgeons (AAOS) and the American College of Rheumatology (ACR) support the use of intra-articular corticosteroid injections for the hip—preferably under ultrasound guidance.4 These findings represent highly positive outcomes: TA administration in hip osteoarthritis patients can improve their quality of life and reduce both societal and individual economic burdens.
Efficacy of Knee Joint Intra-Articular Injection
Theoretically, OA can affect any joint in the body; however, the knee joint is one of the most commonly involved sites, with KOA accounting for approximately 43% of all OA cases. The condition predominantly affects the elderly and obese populations, with an estimated prevalence of 10% to 13% among older adults, which may be associated with long-term mechanical loading and cumulative wear of the knee joint.1,16,80 In addition to the dietary and physical activity modifications recommended by clinical guidelines, we aim to experimentally demonstrate the therapeutic efficacy of intra-articular administration of TA in patients with KOA.
For patients with KOA, the administration of corticosteroids prior to exercise therapy provided no additional benefit, regardless of OA severity. No significant differences were observed between the intra-articular corticosteroid group (n=50) and the placebo group (n=50) in the Knee injury and Osteoarthritis Outcome Score (KOOS) (+13.6 vs +14.8, p=0.64). Similarly, lower extremity muscle strength, walking distance, and functional outcomes were comparable between the two groups.81 In contrast, the use of TA during total knee arthroplasty (TKA) was associated with reduced postoperative pain and a rapid onset of action by the second day after surgery. Compared with the control group, patients in the TA group achieved straight-leg-raising earlier (2.3 days vs 2.8 days) and demonstrated better knee function improvements within six months, along with greater range of motion.82
Conaghan first conducted a randomized, double-blind, placebo-controlled, multicenter phase IIb trial, in which patients were assigned to receive either 16 mg (n=102) or 32 mg (n=104) of the extended-release TA microsphere formulation (FX006), or a saline placebo (n=104). The 32 mg FX006 group exhibited a longer duration of analgesia compared to the 16 mg group (9 weeks vs 3 weeks). Although the reduction in average daily pain (ADP) at week 12 did not reach statistical significance between the 32 mg FX006 and placebo groups (−3.1 vs −2.5, p=0.08), the 32 mg FX006 group demonstrated significant improvements over placebo at most time points in the McMaster Universities Osteoarthritis Index (WOMAC) pain and function subscales, as well as in the Patient Global Impression of Change (PGIC) score. The incidence of adverse events was similar across groups, with the majority being mild to moderate in severity. This trial provided the basis for subsequent Phase III clinical trials.74 Subsequently, a phase III randomized controlled trial was conducted, where patients received an intra-articular injection of either 5 mL FX006 (n=161), 1 mL (40 mg) of standard TAcs (n=162), or 5 mL saline placebo (n=163). At week 12, the FX006 group showed a 50% improvement in ADP, which was significantly greater than that in the placebo group (−3.12 vs −2.14, p < 0.0001), but not significantly different from the TAcs group. However, according to the WOMAC and the KOOS, the FX006 group exhibited significantly greater improvements in pain and physical function compared to the TAcs group at 12 weeks post-injection (P < 0.05).83 In a study involving bilateral KOA patients who received TA-ER injections (n=70), significant pain improvement from baseline was observed: the NRS scores decreased by 4.7±0.3 at 6 weeks, 3.4±0.3 at 12 weeks (p < 0.0001), and 1.1±0.3 at 24 weeks (p < 0.0011)84 (Table 3).
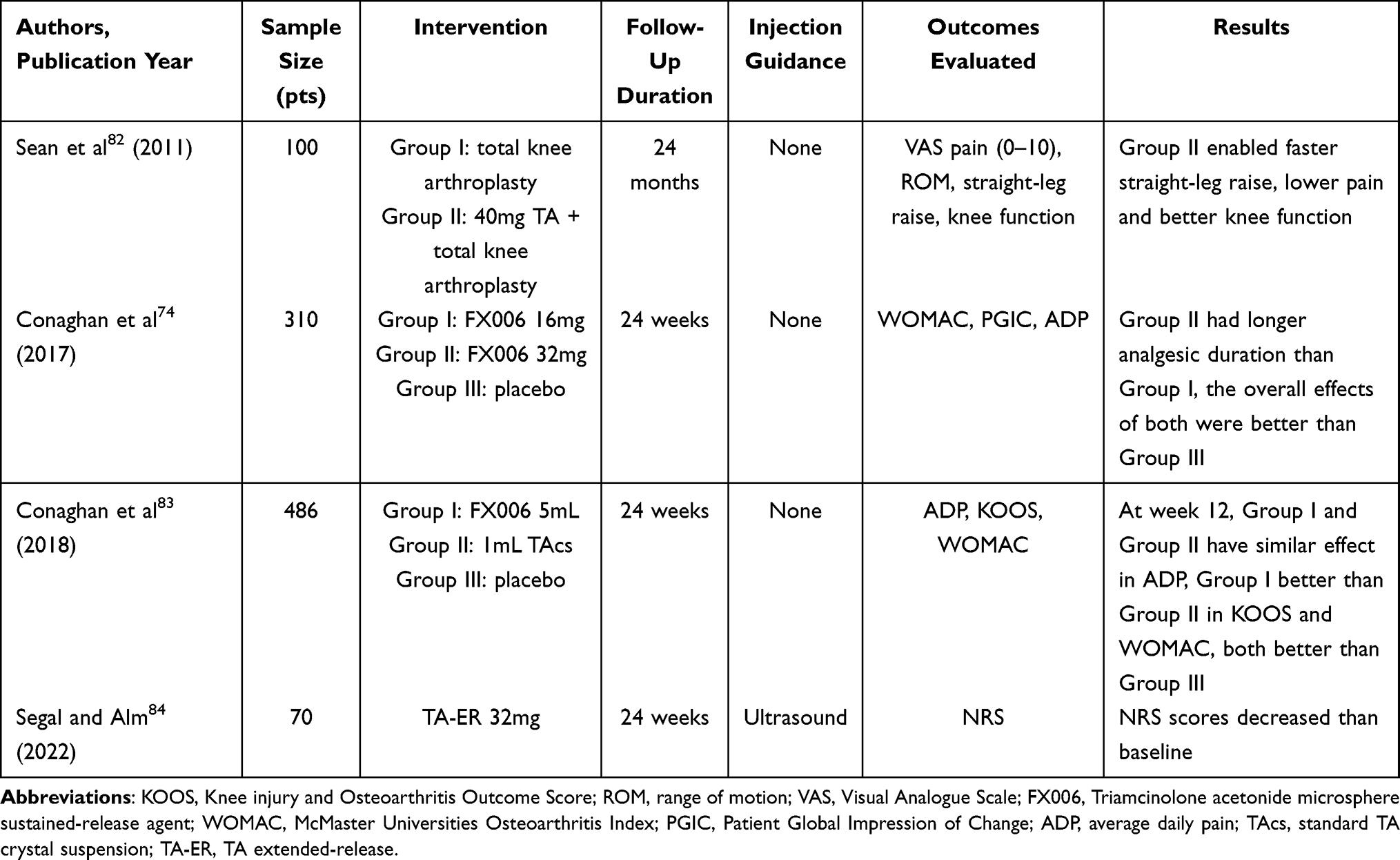 |
Table 3 Summary of The Efficacy of TA Knee Joint Intra-Articular Injection |
International associations have issued specialized guidelines on intra-articular corticosteroid injections for patients with KOA. Although the American Academy of Orthopaedic Surgeons (AAOS) maintains a neutral stance, several societies—such as the American College of Rheumatology (ACR), the European Alliance of Associations for Rheumatology (EULAR), and the Osteoarthritis Research Society International (OARSI)—support the use of intra-articular injections.4 In summary, evidence from specific clinical trials to guidelines issued by internationally recognized authorities indicates that intra-articular TA injection is an effective and acknowledged treatment for KOA patients. Moreover, TA-ER demonstrates superior efficacy compared to conventional TA formulations in the management of KOA. However, attention must be paid to the timing of administration: injection prior to exercise training appears to offer little benefit, in severe osteoarthritis, total knee arthroplasty remains an effective option for alleviating pain and functional symptoms. Beyond this, adjunctive intraoperative and postoperative therapeutic strategies can be explored; for instance, continuous cold flow (CCF) therapy has been proposed as an effective intervention by some researchers.85 The aforementioned findings in this study indicate that, analogous to hip arthroplasty, the application of TA in knee arthroplasty also ameliorates pain. Therefore, future consideration may be given to administering additional combined TA injections for patients with poor pain tolerance undergoing joint replacement surgery.
Efficacy of Shoulder Joint Intra-Articular Injection
OA affecting the shoulder joint has a reported prevalence ranging from 15% to 75%, which is comparable to that of the knee. The interplay among periarticular structures—including muscles, ligaments, tendons, and bursae—often contributes to the pathology, and these structures are frequently implicated as sources of pain in shoulder OA.1,86 This review summarizes three randomized controlled trials that evaluated the efficacy of intra-articular TA injections in the shoulder. Two of these trials were dose-comparison studies, designed as single-blind (n=61) or triple-blind (n=136), while the third investigated the effect of injection volume (n=90).
Carroll and Hong investigated the efficacy of intra-articular TA at doses of 20 mg and 40 mg in patients with shoulder pain (n=61 vs n=136). Despite differences in follow-up time points (3 days/3 weeks/6 weeks vs 2/4/8 weeks), both studies reported similar outcomes, indicating no significant differences in shoulder pain scores and functional improvement between the 20 mg and 40 mg TA groups. However, both doses demonstrated superior efficacy compared to placebo.86,87
In addition to the aforementioned trials using TA injection dosage as the independent variable, Klontzas also designed a study from a volumetric perspective, in which 40 mg of TA was administered in volumes of 1 mL and 10 mL, respectively, into the subacromial-subdeltoid bursae of two subject groups (n=90). At follow-up time points of 30 minutes, 3 weeks, 3 months, 6 months, and 1 year, the 10 mL TA injection group demonstrated significantly improved Visual Analogue Scale for Pain (VAS) pain scores compared to the 1 mL group (2.6 / 2.2 / 2.0 / 1.6 / 1.0 vs 7.3 / 4.7 / 3.2 / 2.5 / 1.8). This led to the conclusion that injection volume is the critical factor for achieving both early and long-term pain relief (Table 4). Hong suggested that these outcomes may be attributed to the 10 mL mixture (corticosteroid combined with anesthetic—the latter intended to mitigate irritation caused by high-volume triamcinolone acetonide injection) sufficiently distending the bursa, disrupting adhesions, and promoting uniform drug distribution, thereby facilitating early and sustained pain alleviation.88
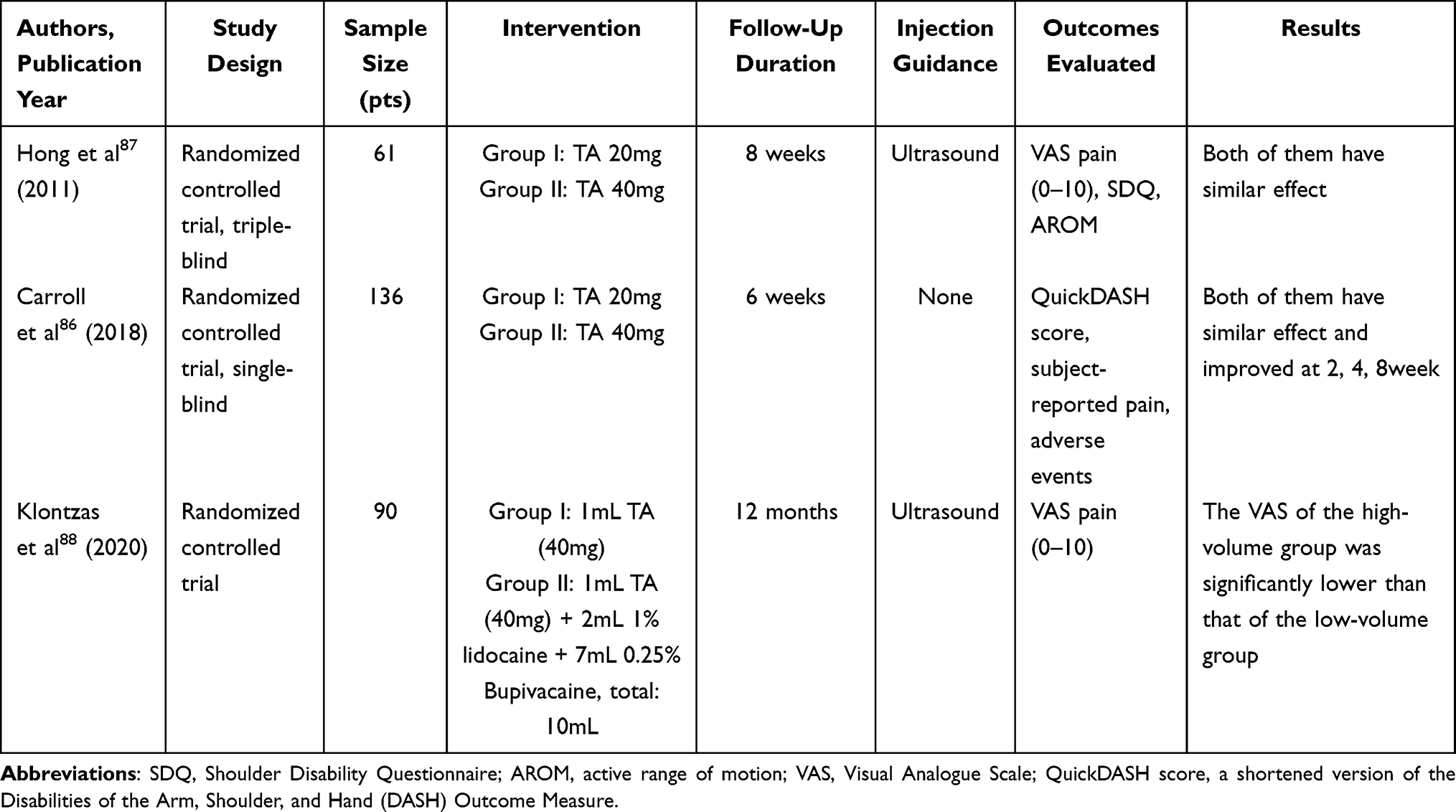 |
Table 4 Summary of the Efficacy of TA Shoulder Joint Intra-Articular Injection |
Based on the above trials, it can be concluded that TA is an extended-release formulation. However, its therapeutic efficacy is dose-independent, with 20 mg and 40 mg of TA demonstrating comparable effectiveness. This supports the selection of a lower dose for initial TA therapy to minimize unnecessary drug utilization in clinical practice.
Efficacy of Hand Joint Intra-Articular Injection
OA affecting the hand is relatively common and can be further categorized into radiographic OA (prevalence: 21–92%) and symptomatic OA (prevalence: 3–16%).1 Long-standing erosive hand osteoarthritis (EHOA) is considered a variant of hand OA, characterized by severe local inflammation and progressive joint degeneration.89
In a novel approach, Spolidoro administered intra-articular injections of THA 20 mg/mL combined with 2% lidocaine (LID) into the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints of the hand. A comparative analysis between the experimental group (THA + LID, n=30) and the control group (LID alone, n=30) revealed that at the 1-, 4-, 8-, and 12-week follow-ups, the experimental group showed significant improvements in movement-induced pain (VASm) (mean values: 3.9, 2.8, 1.8, 2.2 vs 4.1, 3.0, 4.0, 4.0; P=0.014) and joint swelling (VASs) (mean values: 2.0, 1.4, 0.7, 1.1 vs 2.1, 2.0, 1.8, 2.0; P=0.022). The treatment was well tolerated, with no between-group differences observed in transient discomfort or increased pain within 48 hours post-injection.90
In a study by Favero evaluating the efficacy of ultrasound-guided intra-articular injection of 40 mg/mL TA in 12 patients with EHOA, targeting both the DIP and PIP joints, significant reductions in joint effusion, capsular distension, and synovial hypertrophy were observed at 1-, 3- and 6-months post-injection. The proportion of joints achieving a VAS pain score of 0 was 48.38%, 42.86%, and 22.58% at 1-, 3- and 6-months, respectively. At the 6-month follow-up, the prevalence of joint effusion decreased from 66.7% at baseline to 19.4%; synovial thickening declined from 92.3% to 29.0%; and capsular distension was reduced from 96.6% to 41.9%. Regarding safety, Favero highlighted favorable post-injection outcomes with no reported serious adverse events. Following the 2018 EULAR recommendations, which support the consideration of intra-articular glucocorticoid injections for painful interphalangeal joints with clear inflammatory features, this study provides evidence for an effective localized treatment strategy utilizing ultrasonography to target inflammation in EHOA—a relatively uncommon disorder.91
Despite the relatively small sample size, the findings nevertheless demonstrate the local efficacy and tolerability of intra-articular TA injections at this specific anatomical site.
Exploring Standardized Use and Personalized Protocols in the Era of Precision Medicine
Common Doses
In a 12-week multicenter, double-blind, randomized controlled trial, Popma investigated the efficacy of intra-articular knee injections of 40 mg (n = 49) versus 80 mg (n = 48) of TA in patients with KOA. A significant reduction in the Likert burden score and VAS pain score was observed in both groups as early as the first week post-injection. However, no statistically significant difference was found between the 40 mg and 80 mg groups in terms of the rate of good response (defined as an improvement of ≥ 2 points on the Likert burden scale) over the 12-week period (49% vs 55%). Similarly, there were no significant differences in VAS pain scores, arthritis activity, swelling reduction, or functional improvement between the two doses.92 In line with these findings, studies by Carroll and Klontzas also reported no significant differences in pain relief or functional improvement between 20 mg and 40 mg TA injections in the shoulder joint.86,88 Additionally, it has been reported that the use of TA at doses exceeding recommended levels (> 40 mg per month) or with frequent administration may lead to adverse effects. For instance, a 34-year-old female developed typical iatrogenic Cushing’s syndrome following monthly injections of 100 mg TA.93
The aforementioned controlled trial indicates that intra-articular TA injection does not exhibit a dose-dependent effect in terms of clinical efficacy. A 20 mg dose of TA provides pain relief and functional improvement comparable to that of a 40 mg dose post-injection, and a similar relationship is observed between 40 mg and 80 mg doses. Moreover, long-term administration of higher doses may lead to adverse events such as iatrogenic Cushing’s syndrome. These findings offer critical insights for clinical practice: to minimize both pharmaceutical waste and the incidence of adverse reactions, it is estimated that the recommended dosage for intra-articular injection of TA is 20 to 40mg. Nevertheless, the precise optimal dose within this range warrants further investigation and validation in future studies.
Importance of Ultrasound Guidance for Accurate Injection
Ultrasound, as a well-established two-dimensional imaging technique, offers the advantages of being non-invasive, cost-effective, and capable of repeated examinations.94 It can be used both for localizing inflammatory sites and for guiding needle insertion, thereby enabling “precision-guided” drug delivery, which is of significant importance in facilitating intra-articular injections. In a study by Soh, the efficacy of ultrasound-guided versus blind corticosteroid shoulder injections was evaluated. At six weeks post-injection, the ultrasound-guided group demonstrated significant improvements in both pain and shoulder function, with a mean difference of 2.23 in the VAS pain score and 1.09 in the Constant-Murley shoulder score. Moreover, the ultrasound-guided group experienced fewer adverse events.37 In the treatment of OA, ultrasound guidance allows for precise localization and anti-inflammatory drug injection into the affected site, which can further delay disease progression and lead to improved therapeutic outcomes.
Efficacy Evaluation of Combination with Hyaluronic Acid (HA)
Intra-articular TA, as a monotherapy for OA, often proves insufficient for adequate symptom relief and quality-of-life improvement. Under these circumstances, combining TA with other pharmacotherapies, such as hyaluronic acid (HA), presents a viable therapeutic strategy. The superior efficacy of this combination approach will be demonstrated through references to three prospective clinical trials.
In a 26-week follow-up study of patients with KOA (n=98), Petrella found that combined intra-articular administration of TA (Hydros-TA, HA + 10 mg TA) provided more rapid pain relief compared to HA (Hydros, Hyaluronic acid-based hydrogen gel suspended in a hyaluronic acid solution) alone, with significant pain improvement observed within 2 weeks (WOMAC difference: 12.4 mm, p = 0.04). By week 26, the Hydros-TA group showed a 30.0 mm improvement in WOMAC function scores. Moreover, the tolerability of Hydros-TA was comparable to that of Hydros, with no additional adverse events reported.95 Tammachote et al evaluated knee pain, function, and range of motion over 6 months (n=99) and reported no statistically significant differences between the HA-only (cross-linked) and HA+TA groups at the 6-month endpoint. However, the HA+TA combination demonstrated superior pain relief at 1 week and functional improvement at 2 weeks.96 A prospective observational study investigated pain and functional outcomes as well as adverse events following intra-articular HA (cross-linked) +TA injection in the hip over 6 months (n=100). Among the 91 patients who completed follow-up, the mean VAS pain score improved by 19.2 points. Sixteen patients no longer required analgesic medication after treatment. Positive hip impingement test rates decreased from 85.3% to 62.8% for anterior impingement and from 56.8% to 30.8% for posterior impingement. All HOOS function subscales showed significant improvements (pain: 12.7 points; activities of daily living: 10.9 points; quality of life: 13.5 points; etc., p < 0.001). Hip flexion range improved from 103.3° to 115.4° in 78 patients with bilateral involvement. The adverse event rate was 9.5% (9/91), mostly transient pain (5.3% lasting <7 days). Serious events included three arthroplasty cases (1 fracture, 2 due to OA progression), deemed unrelated to the injection.29
The aforementioned three sets of trials demonstrate that, compared with HA injection alone, intra-articular injection of HA combined with TA provides enhanced short-term rapid analgesic effects in patients with osteoarthritis, with sustained improvements in joint pain and function lasting up to six months. Moreover, the combination therapy was associated with no serious adverse events, indicating a relatively safe treatment option. These findings may assist in the development of additional individualized non-surgical management strategies for OA patients, tailored to their specific needs. Clinicians can consider patients’ pain levels, functional status, and overall health status to design combined interventions that address individual requirements.
Previous studies have indicated that intra-articular injection of HA can reduce the concentration of matrix metalloproteinase (MMP)-9 in synovial fluid.97 Since MMPs can promote chondrocyte degradation, HA is considered to exert a chondroprotective effect.98 Although glucocorticoid injections exhibit potent anti-inflammatory properties, they may also cause some degree of cartilage damage. Therefore, it is hypothesized that the combination of HA and TA in intra-articular injections may allow HA to counteract the cartilage damage induced by TA, while TA could compensate for the limitations of HA in terms of pain relief and anti-inflammatory efficacy, thereby resulting in superior therapeutic outcomes. However, all three prospective trials discussed here are limited by small sample sizes and the absence of placebo-controlled groups. Moreover, the potential chondrotoxic effects of TA were not assessed. Thus, the proposed hypothesis has not been fully validated. Further studies with improved methodological rigor are warranted to substantiate these findings.
Safety and Adverse Reactions
Local Adverse Reactions
Intra-articular TA injection for the treatment of OA has been demonstrated to induce several localized dermatological adverse effects, with transient facial flushing being the most frequently reported.35 Case reports have described systemic allergic dermatitis manifesting as symmetrical drug-related intertriginous and flexural exanthema and erythema multiforme-like eruptions.99 Additionally, rare ischemic reactions in the feet have been observed in the absence of ischemia, temperature changes, or diminished pulses.100 Atrophic linear plaques accompanied by hyperpigmentation and cutaneous atrophy have also been documented; however, these must be differentiated from linear scleroderma, which requires immunosuppressive therapy.101
But the aforementioned studies indicate that these adverse effects subside spontaneously after drug discontinuation. This observation, to some extent, provides supporting evidence for the safety profile of intra-articular TA in the local treatment of OA, suggesting an absence of severe local adverse reactions.
Systemic Adverse Reactions
Transient Hyperglycemia
Following intra-articular injection of 18mg TA into either the intercarpal joint (n=10) or the sacroiliac joint (n=10), both groups exhibited significant elevations in blood glucose levels starting at 1-hour post-injection, which persisted for up to 72 hours.69 The rapid egress of corticosteroids from the joint space may lead to high systemic peak concentrations of TA after conventional TA (TAcs) injections in human joints, resulting in several days of hyperglycemia following administration. In contrast, the extended-release characteristics of TA-ER result in lower systemic exposure, with peak plasma concentrations approximately 80% lower than those observed with TAcs, thereby significantly attenuating glycemic fluctuations and minimizing the impact on blood glucose levels.102 Both animal studies and clinical trials have demonstrated transient acute hyperglycemia following intra-articular TA injection. Notably, approximately 30% of patients with type 2 diabetes also suffer from KOA.102 Consequently, particular attention to glycemic variability is warranted when performing intra-articular TA injections in OA patients with comorbid diabetes.
Hypothalamic-Pituitary-Adrenal Axis (HPAA) Suppression
A notable and potentially serious side effect associated with TA use is the suppression of the hypothalamic-pituitary-adrenal axis (HPAA), which may lead to secondary adrenal insufficiency (SAI).71,103 A systematic review encompassing 3753 patients found that intra-articular corticosteroid injections were associated with the highest incidence of SAI (52.2%) compared to other routes of administration.104 In a comparative study, 40 mg of methylprednisolone acetate (MA) and the same dose of TA were administered via intra-articular injection into the shoulder joint. Due to differences in pharmacokinetics, cortisol recovery was significantly slower in the TA group at 7 days post-injection compared to the MA group (P < 0.0001). Moreover, 24-hour urinary free cortisol levels remained below baseline at 45 days post-injection, indicating that TA-induced HPAA suppression persisted throughout the 45-day observation period. Although none of the patients in this trial exhibited clinical symptoms, the findings suggest that subclinical HPAA suppression is common.71 Therefore, caution is warranted when administering intra-articular TA injections in patients with OA.
Psychiatric Abnormalities
While the psychiatric impact of systemic corticosteroids may be more widely recognized, Malladi reported a particularly rare case of intra-articular corticosteroid injection inducing neuropsychiatric adverse effects. A 51-year-old female received three sequential intra-articular injections of 40mg TA for KOA. Following the first injection, she exhibited suicidal behavior requiring hospitalization within 10 days. The second injection precipitated extreme agitation, delusions, and suicidal ideation within 3 days, necessitating police intervention and involuntary psychiatric admission. After the third injection, the patient discontinued long-term psychiatric follow-up and was lost to follow-up. Notably, the patient maintained psychiatric stability prior to each episode, with no documented history of suicidality or prior psychiatric hospitalizations.105
Clinical Implications for Cartilage
Although debates persist regarding the toxicity of TA toward chondrocytes from a mechanistic perspective, its adverse effects on cartilage in clinical trials involving intra-articular injections are significant enough that clinicians cannot afford to overlook them.
According to clinical trial findings, six months after intra-articular TA injection in 12 patients with knee osteoarthritis (KOA), histological analysis of eight knee samples per patient revealed cartilage degeneration in 16.67% of the subjects, whereas no such degeneration was observed in the untreated control group.34 A randomized, double-blind, placebo-controlled trial was conducted in which the experimental group received intra-articular injections of TA (40 mg/1 mL) every 12 weeks over a period of 2 years (n = 70), while the control group received saline injections (1 mL) on the same schedule (n = 70). The results showed a greater reduction in the inter-space cartilage thickness index in the TA group compared to the control group, with a mean change of −0.21 mm versus −0.10 mm, respectively—a difference of 0.11 mm. This indicates that TA was associated with significantly greater cartilage loss compared to saline, suggesting that long-term use of TA may have adverse effects on cartilage integrity.106
Conclusion and Future Perspectives
This article provides a comprehensive review of the mechanism of action of triamcinolone acetonide, its current clinical applications in osteoarthritis, therapeutic efficacy, and post-administration safety profile (Figure 4). TA, as a long-acting glucocorticoid, continues to be a valuable agent in clinical practice. Despite being a well-established drug, it has garnered renewed widespread attention in the non-surgical management of OA due to its potent anti-inflammatory and immunomodulatory effects. Its ability to concurrently address both inflammation and analgesia allows it to achieve therapeutic goals for OA at two levels: targeting the underlying pathological mechanisms and alleviating clinical symptoms, making it an effective tool for OA symptom management. However, its use requires careful consideration. Firstly, because intra-articular injection can cause significant discomfort for patients, it often needs to be co-administered with a local anesthetic such as lidocaine. Secondly, although the overall post-injection efficacy profile of TA is generally safe, it can still induce certain adverse effects in patients, including rare dermatological and psychiatric symptoms, which clinicians must differentiate from other conditions. Furthermore, studies in both animal models and human trials have indicated that TA administration can impact the endocrine system, leading to transient hyperglycemia and suppressed cortisol levels. Therefore, clinical application must take into account the patient’s individual health status. Finally, the potential impact of TA on articular cartilage remains a subject of debate, necessitating further long-term, large-sample clinical studies to clarify its chondrotoxic safety profile. Recent studies have demonstrated that the introduction of slide-ring polyrotaxane and conductive polypyrrole esters into hydrogel microspheres through supramolecular engineering and microfluidic techniques, enabling the construction of stress-electrically coupled hydrogel microspheres, as well as the application of precise cellular electrical stimulation therapy using these electro-mechanically active hydrogel microspheres, can promote cartilage healing. These combined approaches can be utilized for the repair of cartilage injuries.107,108
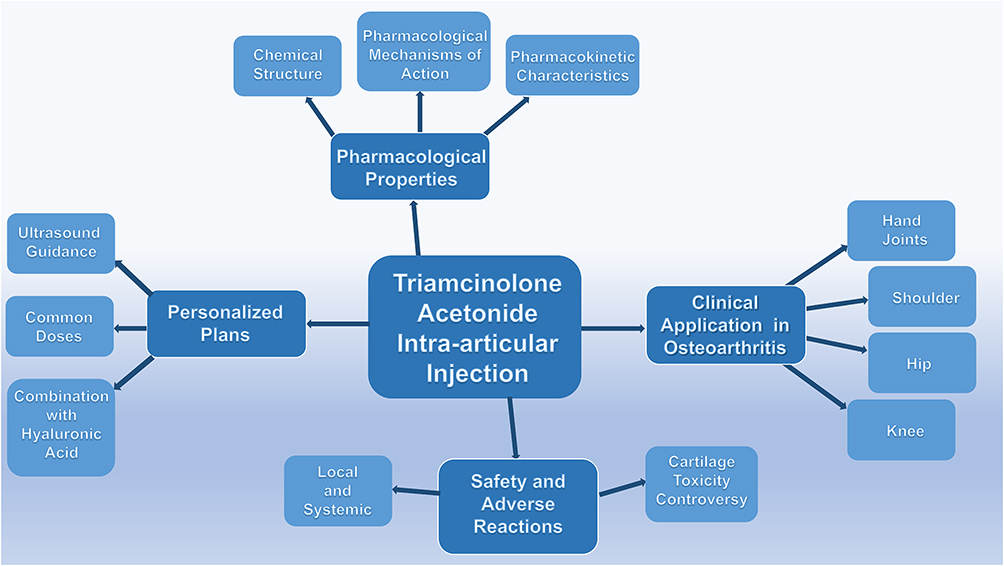 |
Figure 4 This article focuses on the intra-articular injection of triamcinolone acetonide, providing a detailed elaboration and discussion across four key aspects: pharmacological properties, personalized treatment plans, clinical application in osteoarthritis, and safety profile and adverse reactions. |
With the advancement of the era, ultrasound and other imaging technologies can provide targeted guidance for injections, which to some extent reduces the incidence of complications and improves therapeutic efficacy. The novel sustained-release material loaded with TA demonstrates lower systemic exposure and longer-lasting efficacy without inducing additional adverse events, making it worthy of promotion and application. Future studies may further explore treatment strategies involving TA in combination with drugs other than HA to investigate potential synergistic effects between therapeutic agents. Furthermore, another study has demonstrated that the application of ultrasound-responsive piezoelectric analgesic microspheres, constructed using ultrasound and piezoelectric nanomaterials in rats, can significantly improve pain-related behaviors and joint pathological damage. Further in-depth validation is warranted in the future to demonstrate their therapeutic efficacy for pain and joint damage associated with human osteoarthritis.109
For OA, emerging research advancements indicate that it is frequently associated with extensive effects on periarticular structures, including cartilage degradation, ligament injury, subchondral bone remodeling, and inflammatory manifestations involving the synovium.1 Due to their anatomical proximity and functional interconnections and interdependence, if one periarticular structure is traumatized or inflamed, others may also be affected. In the knee joint, the infrapatellar fat pad (IFP, also known as Hoffa’s fat pad) is a particularly important and unique anatomical structure compared to those in other joints throughout the body. Adjacent to the synovium, it serves specific mechanical roles by providing cushioning to protect the knee joint and is believed to contribute to the blood supply—via the genicular rete arteriosum—to the anterior cruciate ligament, patella, and patellar tendon. However, with ongoing research, the IFP has been found to play a dual role in the pathogenesis of OA,110 being closely associated with pain and inflammation in KOA. It involves not only immune cells, typically represented by mast cells, but also a range of cytokines including interleukins, natural killer cells, substance P, and calcitonin gene-related peptide, in addition to being richly innervated.18,111 Whether anti-inflammatory therapy targeting the IFP can alleviate KOA symptoms and disease progression is increasingly attracting researchers’ attention. This paper has already discussed the application and superior efficacy of TA in systemic OA. In the future, leveraging TA’s anti-inflammatory and analgesic mechanisms, ultrasound-guided injection of TA-loaded novel materials into the IFP could be utilized to explore whether this approach can effectively delay the progression of KOA (Figure 3).
With the application of novel biomaterials and precise targeting techniques, we believe that TA holds great promise in the future management of OA. It may serve as a non-surgical intervention to delay disease progression and alleviate symptoms, thereby reducing healthcare expenditures and optimizing medical resources for both patients and society, while simultaneously enhancing social satisfaction and workforce productivity.
Despite its contributions, this review has several limitations. First, from a methodological standpoint, our search strategy focused exclusively on peer-reviewed journals indexed in the PubMed, potentially excluding relevant findings from books and conference proceedings (methodological limitation). Second, this article, due to its focus on the use of TA in the treatment of osteoarthritis, predominantly highlights its therapeutic efficacy when compared to alternative treatments. However, many other therapies have also demonstrated positive outcomes through research, which, owing to space constraints, are not as prominently featured in this text—potentially leading to a subtle bias (theoretical limitation).
Abbreviations
APC, Serine Protease-activated Protein C; AUC, The Area Under the Concentration-time Curve; AAOS, the American Academy of Orthopaedic Surgeons; ACR, the American College of Rheumatology; ADP, Average Daily Pain; BCT, Basic Conservative Treatment; CRP, C-reactive Protein; CK, Creatine Kinase; DIP, Distal Interphalangeal; ESCEO, European Society for Clinical and Economic Aspects of Osteoporosis; EULAR, European Alliance of Associations for Rheumatology; EHOA, Erosive Hand Osteoarthritis; GC, Glucocorticoid; GAG, Glycosaminoglycan; HA, Hyaluronic Acid; HPAA, Hypothalamic-pituitary-adrenal Axis; IL, Interleukin; IC, Intercarpal; IV, Intravenous; IM, Intramuscular; IA, Intra-articular; KOA, Knee Osteoarthritis; KOOS, the Knee injury and Osteoarthritis Outcome Score; KL, Kellgren-Lawrence Grade; LID, Lidocaine; MRI, Magnetic Resonance Imaging; MMP, Matrix Metalloproteinase; MA, Methylprednisolone Acetate; NSAIDs, Non-Steroidal Anti-inflammatory Drugs; NS, Normal Saline; NRS, Numerical Rating Scale; OA, Osteoarthritis; OARSI, Osteoarthritis Research Society International; PRP, Platelet-rich Plasma; PAI, Periarticular Analgesic Injection; PGIC, Patient Global Impression of Change; PIP, Proximal Interphalangeal; sC2C, Serum Cartilage Type II Collagen Cleavage by Collagenase; sCPII, Serum Cartilage Type II Procollagen Carboxy Propeptide; SI, Sacroiliac; SAI, Secondary Adrenal Insufficiency; sCOMP, Serum Cartilage Oligomeric Matrix Protein; TA, Triamcinolone Acetonide; TNF, Tumor Necrosis Factor; THA, Triamcinolone Hexacetonide; TA-ER, TA Extended-release; TAcs, Triamcinolone Acetonide Crystalline Suspension; uCTX-II, Urinary C-terminal Telopeptide of Type II Collagen; uNTx, Urinary Bone N-terminal Crosslinking Telopeptide of Type I Collagen; US, Ultrasound; VAS, Visual Analogue Scale for Pain; WOMAC, McMaster Universities Osteoarthritis Index.
Ethics Approval
This narrative article contains no original data, so issues of ethics, informed consent, and patient confidentiality do not apply.
Acknowledgments
We would like to thank FigDraw (https://www.Figdraw.com/#/) for Figure 2.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from the Graduate Research and Practice Innovation Project Fund of Anhui Medical University (YJS20240110), the Key Project of Natural Science Foundation of Bengbu Medical University (2024byzd356), the Hefei Municipal Natural Science Foundation (HZR2444), the Key Project of Health Commission Applied Medical Research of Hefei (Hwk2024zd001), the Basic and Clinical Collaborative Research Promotion Initiative of the Third Affiliated Hospital of Anhui Medical University (2023sfy017), the Health Research Project of Health Commission of Anhui Province (No. AHWJ2024Aa30021) and the Anhui Medical University Foundation (2023xkj109).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tang S, Zhang C, Oo WM, et al. Osteoarthritis. Nat Rev Dis Primers. 2025;11(1):10. doi:10.1038/s41572-025-00594-6
2. Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. Lancet. 2019;393(10182):1745–23. doi:10.1016/s0140-6736(19)30417-9
3. Bedenbaugh AV, Bonafede M, Marchlewicz EH, Lee V, Tambiah J. Real-world health care resource utilization and costs among US patients with knee osteoarthritis compared with controls. Clinicoecon Outcomes Res. 2021;13:421–435. doi:10.2147/ceor.S302289
4. Guermazi A, Neogi T, Katz JN, et al. Intra-articular corticosteroid injections for the treatment of hip and knee osteoarthritis-related pain: considerations and controversies with a focus on imaging-radiology scientific expert panel. Radiology. 2020;297(3):503–512. doi:10.1148/radiol.2020200771
5. Pan F, Wang Y, Lim YZ, et al. Metformin for knee osteoarthritis in patients with overweight or obesity. JAMA. 2025;333(20):1804. doi:10.1001/jama.2025.3471
6. Zhang H, Cai D, Bai X. Macrophages regulate the progression of osteoarthritis. Osteoarthritis Cartilage. 2020;28(5):555–561. doi:10.1016/j.joca.2020.01.007
7. Devor M. An alternative perspective on the causes of pain in osteoarthritis of the knee and its persistence after total knee replacement surgery. Pain. 2024;165(9):2135. doi:10.1097/j.pain.0000000000003327
8. DeFrance MJ, Scuderi GR. Are 20% of patients actually dissatisfied following total knee arthroplasty? A systematic review of the literature. J Arthroplasty. 2023;38(3):594–599. doi:10.1016/j.arth.2022.10.011
9. Ebraheim NA, Kelley LH, Liu X, Thomas IS, Steiner RB, Liu J. Periprosthetic distal femur fracture after total knee arthroplasty: a systematic review. Orthop Surg. 2015;7(4):297–305. doi:10.1111/os.12199
10. Bengoa F, Neufeld ME, Howard LC, Masri BA. Periprosthetic fractures after a total knee arthroplasty. J Am Acad Orthop Surg. 2023;31(19):e746–e759. doi:10.5435/JAAOS-D-22-00701
11. Sahan I, Anagnostakos K. Metallosis after knee replacement: a review. Arch Orthop Trauma Surg. 2020;140(11):1791–1808. doi:10.1007/s00402-020-03560-x
12. Alayane A, Moussa MK, Boushnak MO, Boulazaib I, Nicolas N. Septic metallosis after unicompartmental knee replacement: a case report and literature review. J Orthop Case Rep. 2023;13(6):11–15. doi:10.13107/jocr.2023.v13.i06.3676
13. Singh JA, Lewallen D. Predictors of pain and use of pain medications following primary total hip arthroplasty (THA): 5707 THAs at 2-years and 3289 THAs at 5-years. BMC Musculoskelet Disord. 2010;11(1):90. doi:10.1186/1471-2474-11-90
14. Wylde V, Hewlett S, Learmonth ID, Dieppe P. Persistent pain after joint replacement: prevalence, sensory qualities, and postoperative determinants. Pain. 2011;152(3):566–572. doi:10.1016/j.pain.2010.11.023
15. Jang S, Lee K, Ju JH. Recent updates of diagnosis, pathophysiology, and treatment on osteoarthritis of the knee. Int J Mol Sci. 2021;22(5):2619. doi:10.3390/ijms22052619
16. Gelber AC. Knee Osteoarthritis. Ann Intern Med. 2024;177(9):Itc129–itc144. doi:10.7326/annals-24-01249
17. Mahmoudian A, Lohmander LS, Mobasheri A, Englund M, Luyten FP. Early-stage symptomatic osteoarthritis of the knee - time for action. Nat Rev Rheumatol. 2021;17(10):621–632. doi:10.1038/s41584-021-00673-4
18. Belluzzi E, Stocco E, Pozzuoli A, et al. Contribution of infrapatellar fat pad and synovial membrane to knee osteoarthritis pain. Biomed Res Int. 2019;2019:6390182. doi:10.1155/2019/6390182
19. Rutjes AWS, Jüni P, da Costa BR, Trelle S, Nüesch E, Reichenbach S. Viscosupplementation for osteoarthritis of the knee. Ann Internal Med. 2012;157(3):180–191. doi:10.7326/0003-4819-157-3-201208070-00473
20. Pereira TV, Juni P, Saadat P, et al. Viscosupplementation for knee osteoarthritis: systematic review and meta-analysis. BMJ. 2022;378:e069722. doi:10.1136/bmj-2022-069722
21. Van Middelkoop M, Arden NK, Atchia I, et al. The OA Trial Bank: meta-analysis of individual patient data from knee and Hip osteoarthritis trials show that patients with severe pain exhibit greater benefit from intra-articular glucocorticoids. Osteoarthritis Cartilage. 2016;24(7):1143–1152. doi:10.1016/j.joca.2016.01.983
22. Jüni P, Hari R, Rutjes AW, et al. Intra-articular corticosteroid for knee osteoarthritis. Cochrane Database Syst Rev. 2015;2015(10):Cd005328. doi:10.1002/14651858.CD005328.pub3
23. Bruyère O, Honvo G, Veronese N, et al. An updated algorithm recommendation for the management of knee osteoarthritis from the European society for clinical and economic aspects of osteoporosis, osteoarthritis and musculoskeletal diseases (ESCEO). Semin Arthritis Rheum. 2019;49(3):337–350. doi:10.1016/j.semarthrit.2019.04.008
24. Bennell KL, Paterson KL, Metcalf BR, et al. Effect of intra-articular platelet-rich plasma vs placebo injection on pain and medial tibial cartilage volume in patients with knee osteoarthritis: the RESTORE randomized clinical trial. JAMA. 2021;326(20):2021–2030. doi:10.1001/jama.2021.19415
25. Jones IA, Togashi R, Wilson ML, Heckmann N, Vangsness CT. Intra-articular treatment options for knee osteoarthritis. Nat Rev Rheumatol. 2019;15(2):77–90. doi:10.1038/s41584-018-0123-4
26. Riggle C, McLellan M, Bohlen H, Wang D. Complications of stem cell-based injections for knee osteoarthritis: a systematic review. Hss j. 2025;21(4):476–484. doi:10.1177/15563316241271058
27. Fan M, Tong P, Yan L, et al. Detrimental alteration of mesenchymal stem cells by an articular inflammatory microenvironment results in deterioration of osteoarthritis. BMC Med. 2023;21(1):215. doi:10.1186/s12916-023-02923-6
28. Carneiro DC, Araújo LT, Santos GC, et al. Clinical trials with mesenchymal stem cell therapies for osteoarthritis: challenges in the regeneration of articular cartilage. Int J Mol Sci. 2023;24(12):9939. doi:10.3390/ijms24129939
29. Bourgeault-Gagnon Y, Simunovic N, Heels-Ansdell D. Intra-articular injection of a cross-linked hyaluronic acid combined with triamcinolone hexacetonide improves pain at six months in patients with mild to moderate Hip osteoarthritis: a prospective observational study. J Isakos. 2025;10:100363. doi:10.1016/j.jisako.2024.100363
30. Allado E, Poussel M, Gambier N, et al. SporTRIA study-a multicentre trial protocol for excretion kinetics of triamcinolone acetonide following sport-related intra-articular injections in knees: definitions of the washout periods. BMJ Open. 2021;11(6):e047548. doi:10.1136/bmjopen-2020-047548
31. Yeap SS, Tanavalee A, Perez EC, et al. 2019 revised algorithm for the management of knee osteoarthritis: the Southeast Asian viewpoint. Aging Clin Exp Res. 2021;33(5):1149–1156. doi:10.1007/s40520-021-01834-x
32. Xia W, Cooper C, Li M, et al. East meets West: current practices and policies in the management of musculoskeletal aging. Aging Clin Exp Res. 2019;31(10):1351–1373. doi:10.1007/s40520-019-01282-8
33. Siebelt M, Korthagen N, Wei W, et al. Triamcinolone acetonide activates an anti-inflammatory and folate receptor-positive macrophage that prevents osteophytosis in vivo. Arthritis Res Ther. 2015;17(1):352. doi:10.1186/s13075-015-0865-1
34. Charnwichai P, Tammachote R, Tammachote N, Chaichana T, Kitkumthorn N. Histological features of knee osteoarthritis treated with triamcinolone acetonide and hyaluronic acid. Biomed Rep. 2023;18(6):40. doi:10.3892/br.2023.1623
35. Scherer J, Rainsford KD, Kean CA, Kean WF. Pharmacology of intra-articular triamcinolone. Inflammopharmacology. 2014;22(4):201–217. doi:10.1007/s10787-014-0205-0
36. Shahinfar S, Maibach H. Enigma of intramuscular triamcinolone acetonide (Kenalog((R))) efficacy. Clin Pharmacokinet. 2023;62(9):1189–1199. doi:10.1007/s40262-023-01297-5
37. Soh E, Li W, Ong KO, Chen W, Bautista D. Image-guided versus blind corticosteroid injections in adults with shoulder pain: a systematic review. BMC Musculoskelet Disord. 2011;12(1):137. doi:10.1186/1471-2474-12-137
38. Fauci AS, Dale DC, Balow JE. Glucocorticosteroid therapy: mechanisms of action and clinical considerations. Ann Intern Med. 1976;84(3):304–315. doi:10.7326/0003-4819-84-3-304
39. Jermak CM, Dellacroce JT, Heffez J, Peyman GA. Triamcinolone acetonide in ocular therapeutics. Surv Ophthalmol. 2007;52(5):503–522. doi:10.1016/j.survophthal.2007.06.004
40. Paik J, Duggan ST, Keam SJ. Triamcinolone acetonide extended-release: a review in osteoarthritis pain of the knee. Drugs. 2019;79(4):455–462. doi:10.1007/s40265-019-01083-3
41. Yang YH, Hutchinson P, Santos LL, Morand EF. Glucocorticoid inhibition of adjuvant arthritis synovial macrophage nitric oxide production: role of lipocortin 1. Clin Exp Immunol. 1998;111(1):117–122. doi:10.1046/j.1365-2249.1998.00438.x
42. Yang Y, Leech M, Hutchinson P, Holdsworth SR, Morand EF. Antiinflammatory effect of lipocortin 1 in experimental arthritis. Inflammation. 1997;21(6):583–596. doi:10.1023/a:1027330021479
43. Sherman SL, Khazai RS, James CH, Stoker AM, Flood DL, Cook JL. In vitro toxicity of local anesthetics and corticosteroids on chondrocyte and synoviocyte viability and metabolism. Cartilage. 2015;6(4):233–240. doi:10.1177/1947603515594453
44. Kuchálik J, Magnuson A, Tina E, Gupta A. Does local infiltration analgesia reduce peri-operative inflammation following total Hip arthroplasty? A randomized, double-blind study. BMC Anesthesiol. 2017;17(1):63. doi:10.1186/s12871-017-0354-y
45. Reikeras O, Borgen P, Reseland JE, Lyngstadaas SP. Changes in serum cytokines in response to musculoskeletal surgical trauma. BMC Res Notes. 2014;7(1):128. doi:10.1186/1756-0500-7-128
46. Kugisaki H, Sonohata M, Komine M, et al. Serum concentrations of interleukin-6 in patients following unilateral versus bilateral total knee arthroplasty. J Orthop Sci. 2009;14(4):437–442. doi:10.1007/s00776-009-1344-9
47. Stürmer T, Brenner H, Koenig W, Günther KP. Severity and extent of osteoarthritis and low grade systemic inflammation as assessed by high sensitivity C reactive protein. Ann Rheum Dis. 2004;63(2):200–205. doi:10.1136/ard.2003.007674
48. Iaccarino L, Pegoraro E, Bello L, et al. Assessment of patients with idiopathic inflammatory myopathies and isolated creatin-kinase elevation. Auto Immun Highlights. 2014;5(3):87–94. doi:10.1007/s13317-014-0063-1
49. Hashimoto A, Sonohata M, Hirata H, et al. Periarticular analgesic injection containing a corticosteroid after total Hip arthroplasty may prevent deep venous thrombosis: a retrospective comparative cohort study. BMC Musculoskelet Disord. 2021;22(1):19. doi:10.1186/s12891-020-03879-x
50. van Lent PL, Blom AB, van der Kraan P, et al. Crucial role of synovial lining macrophages in the promotion of transforming growth factor beta-mediated osteophyte formation. Arthritis Rheum. 2004;50(1):103–111. doi:10.1002/art.11422
51. Blom AB, van Lent PL, Holthuysen AE, et al. Synovial lining macrophages mediate osteophyte formation during experimental osteoarthritis. Osteoarthritis Cartilage. 2004;12(8):627–635. doi:10.1016/j.joca.2004.03.003
52. Shapouri-Moghaddam A, Mohammadian S, Vazini H, et al. Macrophage plasticity, polarization, and function in health and disease. J Cell Physiol. 2018;233(9):6425–6440. doi:10.1002/jcp.26429
53. Murray PJ, Allen JE, Biswas SK, et al. Macrophage activation and polarization: nomenclature and experimental guidelines. Immunity. 2014;41(1):14–20. doi:10.1016/j.immuni.2014.06.008
54. Zhang H, Lin C, Zeng C, et al. Synovial macrophage M1 polarisation exacerbates experimental osteoarthritis partially through R-spondin-2. Ann Rheum Dis. 2018;77(10):1524–1534. doi:10.1136/annrheumdis-2018-213450
55. Wu L, Cao X, Shen B. Development of a macrophage polarization-modulating therapeutic agent for osteoarthritis treatment. J Orthop Surg Res. 2025;20(1):279. doi:10.1186/s13018-025-05679-2
56. Utomo L, van Osch GJ, Bayon Y, Verhaar JA, Bastiaansen-Jenniskens YM. Guiding synovial inflammation by macrophage phenotype modulation: an in vitro study towards a therapy for osteoarthritis. Osteoarthritis Cartilage. 2016;24(9):1629–1638. doi:10.1016/j.joca.2016.04.013
57. Westhof A, Kleinschmidt-Doerr K, Michaelis M, Brenneis C. Dynamic weight-bearing test during jumping: a sensitive outcome measure of chronic osteoarthritis pain in rats. Heliyon. 2021;7(9):e07906. doi:10.1016/j.heliyon.2021.e07906
58. Alves JC, Santos A, Jorge P, Lavrador C, Carreira LM. The intra-articular administration of triamcinolone hexacetonide in the treatment of osteoarthritis. Its effects in a naturally occurring canine osteoarthritis model. PLoS One. 2021;16(1):e0245553. doi:10.1371/journal.pone.0245553
59. McIlwraith CW, Lattermann C. Intra-articular corticosteroids for knee pain-what have we learned from the equine athlete and current best practice. J Knee Surg. 2019;32(1):9–25. doi:10.1055/s-0038-1676449
60. Labens R, Mellor DJ, Voûte LC. Retrospective study of the effect of intra-articular treatment of osteoarthritis of the distal tarsal joints in 51 horses. Vet Rec. 2007;161(18):611–616. doi:10.1136/vr.161.18.611
61. Guidoni K, Chiaradia E, Pepe M, et al. The combined use of triamcinolone and platelet-rich plasma in equine metacarpophalangeal joint osteoarthritis treatments: an in vivo and in vitro study. Animals. 2024;14(24). doi:10.3390/ani14243645
62. Garvican ER, Vaughan-Thomas A, Redmond C, Gabriel N, Clegg PD. MMP-mediated collagen breakdown induced by activated protein C in equine cartilage is reduced by corticosteroids. J Orthop Res. 2010;28(3):370–378. doi:10.1002/jor.21001
63. Porter A, Newcomb E, DiStefano S, et al. Triamcinolone acetonide has minimal effect on short- and long-term metabolic activities of cartilage. J Orthop Res. 2024;42(11):2426–2436. doi:10.1002/jor.25913
64. Klocke R, Levasseur K, Kitas GD, Smith JP, Hirsch G. Cartilage turnover and intra-articular corticosteroid injections in knee osteoarthritis. Rheumatol Int. 2018;38(3):455–459. doi:10.1007/s00296-018-3988-2
65. Suntiparpluacha M, Tammachote N, Tammachote R. Triamcinolone acetonide reduces viability, induces oxidative stress, and alters gene expressions of human chondrocytes. Eur Rev Med Pharmacol Sci. 2016;20(23):4985–4992.
66. Dragoo JL, Danial CM, Braun HJ, Pouliot MA, Kim HJ. The chondrotoxicity of single-dose corticosteroids. Knee Surg Sports Traumatol Arthrosc. 2012;20(9):1809–1814. doi:10.1007/s00167-011-1820-6
67. Magnusson K, Turkiewicz A, Kumm J, Zhang F, Englund M. Relationship between magnetic resonance imaging features and knee pain over six years in knees without radiographic osteoarthritis at baseline. Arthritis Care Res. 2021;73(11):1659–1666. doi:10.1002/acr.24394
68. Ishijima M, Watari T, Naito K, et al. Relationships between biomarkers of cartilage, bone, synovial metabolism and knee pain provide insights into the origins of pain in early knee osteoarthritis. Arthritis Res Ther. 2011;13(1):R22. doi:10.1186/ar3246
69. Hallowell KL, Dembek K, Horne CR, Knych HK, Messenger KM, Schnabel LV. Systemic absorption of triamcinolone acetonide is increased from intrasynovial versus extrasynovial sites and induces hyperglycemia, hyperinsulinemia, and suppression of the hypothalamic-pituitary-adrenal axis. Front Vet Sci. 2024;11:1388470. doi:10.3389/fvets.2024.1388470
70. Soma LR, Uboh CE, You Y, Guan F, Boston RC. Pharmacokinetics of intra-articular, intravenous, and intramuscular administration of triamcinolone acetonide and its effect on endogenous plasma hydrocortisone and cortisone concentrations in horses. Am J Vet Res. 2011;72(9):1234–1242. doi:10.2460/ajvr.72.9.1234
71. Guaraldi F, Gori D, Calderoni P, et al. Comparative assessment of hypothalamic-pituitary-adrenal axis suppression secondary to intrabursal injection of different glucocorticoids: a pilot study. J Endocrinol Invest. 2019;42(9):1117–1124. doi:10.1007/s40618-019-01033-6
72. Coll S, Matabosch X, Llorente-Onaindia J, et al. Elimination profile of triamcinolone hexacetonide and its metabolites in human urine and plasma after a single intra-articular administration. Drug Test Anal. 2019;11(11–12):1589–1600. doi:10.1002/dta.2614
73. Derendorf H, Möllmann H, Grüner A, Haack D, Gyselby G. Pharmacokinetics and pharmacodynamics of glucocorticoid suspensions after intra-articular administration. Clin Pharmacol Ther. 1986;39(3):313–317. doi:10.1038/clpt.1986.45
74. Conaghan PG, Cohen SB, Berenbaum F, Lufkin J, Johnson JR, Bodick N. Brief report: a Phase IIb trial of a novel extended-release microsphere formulation of triamcinolone acetonide for intraarticular injection in knee osteoarthritis. Arthritis Rheumatol. 2018;70(2):204–211. doi:10.1002/art.40364
75. Kivitz A, Kwong L, Shlotzhauer T, Lufkin J, Cinar A, Kelley S. A randomized, phase IIa study to assess the systemic exposure of triamcinolone acetonide following injection of extended-release triamcinolone acetonide or traditional triamcinolone acetonide into both knees of patients with bilateral knee osteoarthritis. Ther Adv Musculoskelet Dis. 2019;11:1759720x19881309. doi:10.1177/1759720x19881309
76. Kivitz A, Mehra P, Hanson P, et al. A randomized, open-label, single-dose study to assess safety and systemic exposure of triamcinolone acetonide extended-release in patients with hip osteoarthritis. Rheumatol Ther. 2022;9(2):679–691. doi:10.1007/s40744-022-00430-3
77. Kigozi J, Oppong R, Paskins Z, et al. The cost-effectiveness of adding an ultrasound corticosteroid and local anaesthetic injection to advice and education for Hip osteoarthritis. Rheumatology. 2025;64(1):165–172. doi:10.1093/rheumatology/kead659
78. Dobie I, Bennett D, Spence DJ, Murray JM, Beverland DE. Periarticular local anesthesia does not improve pain or mobility after THA. Clin Orthop Relat Res. 2012;470(7):1958–1965. doi:10.1007/s11999-012-2241-7
79. Murphy TP, Byrne DP, Curtin P, Baker JF, Mulhall KJ. Can a periarticular levobupivacaine injection reduce postoperative opiate consumption during primary Hip arthroplasty? Clin Orthop Relat Res. 2012;470(4):1151–1157. doi:10.1007/s11999-011-2108-3
80. Messier SP, Beavers DP, Queen K, et al. Effect of diet and exercise on knee pain in patients with osteoarthritis and overweight or obesity: a randomized clinical trial. JAMA. 2022;328(22):2242–2251. doi:10.1001/jama.2022.21893
81. Henriksen M, Christensen R, Klokker L, et al. Evaluation of the benefit of corticosteroid injection before exercise therapy in patients with osteoarthritis of the knee: a randomized clinical trial. JAMA Intern Med. 2015;175(6):923–930. doi:10.1001/jamainternmed.2015.0461
82. Sean VW, Chin PL, Chia SL, Yang KY, Lo NN, Yeo SJ. Single-dose periarticular steroid infiltration for pain management in total knee arthroplasty: a prospective, double-blind, randomised controlled trial. Singapore Med J. 2011;52(1):19–23.
83. Conaghan PG, Hunter DJ, Cohen SB, et al. Effects of a single intra-articular injection of a microsphere formulation of triamcinolone acetonide on knee osteoarthritis pain: a double-blinded, randomized, placebo-controlled, multinational study. J Bone Joint Surg Am. 2018;100(8):666–677. doi:10.2106/jbjs.17.00154
84. Segal NA, Alm JC. The effect of intra-articular extended-release triamcinolone acetonide on OARSI-recommended physical performance measures in adults with bilateral symptomatic knee osteoarthritis. Osteoarthr Cartil Open. 2022;4(3):100268. doi:10.1016/j.ocarto.2022.100268
85. Coviello M, Abate A, Ippolito F, et al. Continuous cold flow device following total knee arthroplasty: myths and reality. Medicina. 2022;58(11). doi:10.3390/medicina58111537
86. Carroll MB, Motley SA, Smith B, Ramsey BC, Baggett AS. Comparing corticosteroid preparation and dose in the improvement of shoulder function and pain: a randomized, single-blind pilot study. Am J Phys Med Rehabil. 2018;97(6):450–455. doi:10.1097/PHM.0000000000000758
87. Hong JY, Yoon SH, Moon DJ, Kwack KS, Joen B, Lee HY. Comparison of high- and low-dose corticosteroid in subacromial injection for periarticular shoulder disorder: a randomized, triple-blind, placebo-controlled trial. Arch Phys Med Rehabil. 2011;92(12):1951–1960. doi:10.1016/j.apmr.2011.06.033
88. Klontzas ME, Vassalou EE, Zibis AH, Karantanas AH. The effect of injection volume on long-term outcomes of US-guided subacromial bursa injections. Eur J Radiol. 2020;129:109113. doi:10.1016/j.ejrad.2020.109113
89. Favero M, Ramonda R, Rossato M. Efficacy of intra-articular corticosteroid injection in erosive hand osteoarthritis: infrared thermal imaging. Rheumatology. 2017;56(1):86. doi:10.1093/rheumatology/kew333
90. Spolidoro Paschoal Nde O, Natour J, Machado FS, de Oliveira HA, Furtado RN. Effectiveness of triamcinolone hexacetonide intraarticular injection in interphalangeal joints: a 12-week randomized controlled trial in patients with hand osteoarthritis. J Rheumatol. 2015;42(10):1869–1877. doi:10.3899/jrheum.140736
91. Favero M, Hoxha A, Frallonardo P, et al. Efficacy and safety of ultrasound-guided intra-articular glucocorticoid injection in erosive hand osteoarthritis. Pain Med. 2021;22(5):1229–1232. doi:10.1093/pm/pnaa261
92. Popma JW, Snel FW, Haagsma CJ, et al. Comparison of 2 dosages of intraarticular triamcinolone for the treatment of knee arthritis: results of a 12-week randomized controlled clinical trial. J Rheumatol. 2015;42(10):1865–1868. doi:10.3899/jrheum.141630
93. Sukhumthammarat W, Putthapiban P, Sriphrapradang C. Local injection of triamcinolone acetonide: a forgotten aetiology of cushing’s syndrome. J Clin Diagn Res. 2017;11(6):Or01–or02. doi:10.7860/jcdr/2017/27238.10091
94. Mizuno Y, Takata Y, Shima Y, et al. Relationship between ultrasonographic findings and subscales of the knee injury and osteoarthritis outcome score in patients with early knee osteoarthritis: a multicenter study. J Med Ultrason. 2025;52(1):139–148. doi:10.1007/s10396-024-01498-w
95. Petrella RJ, Emans PJ, Alleyne J, Dellaert F, Gill DP, Maroney M. Safety and performance of Hydros and Hydros-TA for knee osteoarthritis: a prospective, multicenter, randomized, double-blind feasibility trial. BMC Musculoskelet Disord. 2015;16(1):57. doi:10.1186/s12891-015-0513-6
96. Tammachote N, Kanitnate S, Yakumpor T, Panichkul P. Intra-articular, single-shot hylan G-F 20 hyaluronic acid injection compared with corticosteroid in knee osteoarthritis: a double-blind, randomized controlled trial. J Bone Joint Surg Am. 2016;98(11):885–892. doi:10.2106/jbjs.15.00544
97. Shimizu M, Higuchi H, Takagishi K, Shinozaki T, Kobayashi T. Clinical and biochemical characteristics after intra-articular injection for the treatment of osteoarthritis of the knee: prospective randomized study of sodium hyaluronate and corticosteroid. J Orthop Sci. 2010;15(1):51–56. doi:10.1007/s00776-009-1421-0
98. Brun P, Zavan B, Vindigni V, et al. In vitro response of osteoarthritic chondrocytes and fibroblast-like synoviocytes to a 500-730 kDa hyaluronan amide derivative. J Biomed Mater Res B Appl Biomater. 2012;100(8):2073–2081. doi:10.1002/jbm.b.32771
99. Bianchi L, Marietti R, Tramontana M, Hansel K, Stingeni L. Systemic allergic dermatitis from intra-articular triamcinolone acetonide: report of two cases with unusual clinical manifestations. Contact Dermatitis. 2021;84(1):54–56. doi:10.1111/cod.13667
100. Rumsey DG, Temple M, Borschel G, Tse SM. Ischemic reaction secondary to corticosteroid injection of the joint. Arthritis Rheum. 2013;65(8):2189. doi:10.1002/art.37978
101. Call JE, Mann JA, Linos KD, Perry A, Yost J. Linear lipoatrophy following intra-articular triamcinolone acetonide injection mimicking linear scleroderma. Pediatr Dermatol. 2019;36(1):e56–e57. doi:10.1111/pde.13736
102. Russell SJ, Sala R, Conaghan PG, et al. Triamcinolone acetonide extended-release in patients with osteoarthritis and type 2 diabetes: a randomized, Phase 2 study. Rheumatology. 2018;57(12):2235–2241. doi:10.1093/rheumatology/key265
103. Crowley RK, Argese N, Tomlinson JW, Stewart PM. Central hypoadrenalism. J Clin Endocrinol Metab. 2014;99(11):4027–4036. doi:10.1210/jc.2014-2476
104. Broersen LH, Pereira AM, Jørgensen JO, Dekkers OM. Adrenal insufficiency in corticosteroids use: systematic review and meta-analysis. J Clin Endocrinol Metab. 2015;100(6):2171–2180. doi:10.1210/jc.2015-1218
105. Malladi AS, Gratton SB, Stone D, Scalapino KJ, Charles JF. Recurrent adverse psychiatric effects following intra-articular corticosteroid injection. J Clin Rheumatol. 2011;17(5):284–285. doi:10.1097/RHU.0b013e318227ab11
106. McAlindon TE, LaValley MP, Harvey WF, et al. Effect of intra-articular triamcinolone vs saline on knee cartilage volume and pain in patients with knee osteoarthritis: a randomized clinical trial. JAMA. 2017;317(19):1967–1975. doi:10.1001/jama.2017.5283
107. Wang F, Han X, Han Z, et al. Slide-ring structured stress-electric coupling hydrogel microspheres for low-loss transduction between tissues. Adv Mater. 2025;37(7):e2413156. doi:10.1002/adma.202413156
108. Han Z, Wang F, Xiong W, et al. Precise cell type electrical stimulation therapy via force-electric hydrogel microspheres for cartilage healing. Adv Mater. 2025;37(7):e2414555. doi:10.1002/adma.202414555
109. Li X, Wang F, Zhang X, et al. Ultrasound-responsive piezoelectric analgesic microspheres alleviate osteoarthritis pain. J Control Release. 2025;385:114049. doi:10.1016/j.jconrel.2025.114049
110. Yue S, Zhai G, Zhao S, et al. The biphasic role of the infrapatellar fat pad in osteoarthritis. Biomed Pharmacother. 2024;179:117364. doi:10.1016/j.biopha.2024.117364
111. Zhu Z, Han W, Lu M, et al. Effects of infrapatellar fat pad preservation versus resection on clinical outcomes after total knee arthroplasty in patients with knee osteoarthritis (IPAKA): study protocol for a multicentre, randomised, controlled clinical trial. BMJ Open. 2020;10(10):e043088. doi:10.1136/bmjopen-2020-043088
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Network Analysis of Osteoarthritis Progression Using a Steiner Minimal Tree Algorithm
Xie Y, Shao F, Ji Y, Feng D, Wang L, Huang Z, Wu S, Sun F, Jiang H, Miyamoto A, Wang H, Zhang C
Journal of Inflammation Research 2024, 17:3201-3209
Published Date: 18 May 2024