Back to Journals » Breast Cancer: Targets and Therapy » Volume 15
Optimized Radiomics Nomogram Based on Automated Breast Ultrasound System: A Potential Tool for Preoperative Prediction of Metastatic Lymph Node Burden in Breast Cancer
Authors Li N, Song C ![]() , Huang X, Zhang H, Su J, Yang L, He J, Cui G
, Huang X, Zhang H, Su J, Yang L, He J, Cui G
Received 5 December 2022
Accepted for publication 27 January 2023
Published 5 February 2023 Volume 2023:15 Pages 121—132
DOI https://doi.org/10.2147/BCTT.S398300
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Ning Li,1,* Chao Song,2 Xian Huang,3,* Hongjiang Zhang,1 Juan Su,4 Lichun Yang,5 Juhua He,6 Guihua Cui1
1Department of Ultrasound, Anning First People’s Hospital, Kunming City, People’s Republic of China; 2Department of Radiology, Anning First People’s Hospital, Kunming City, People’s Republic of China; 3Department of Ultrasound, Kunming City Maternal and Child Health Hospital, Kunming City, People’s Republic of China; 4Department of Ultrasound, Yulong People’s Hospital, Lijiang City, People’s Republic of China; 5Department of Ultrasound, Yunnan Cancer Hospital, Kunming City, People’s Republic of China; 6Department of Function Examination, Yunnan Provincial Hospital of Traditional Chinese Medicine, Kunming City, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chao Song, Department of Radiology, Anning First People’s Hospital, Ganghe South Road, Anning City, Kunming City, Yunnan Province, 650302, People’s Republic of China, Tel + 86-13908848395, Email [email protected] Hongjiang Zhang, Department of Ultrasound, Anning First People’s Hospital, Ganghe South Road, Anning City, Kunming City, Yunnan Province, 650302, People’s Republic of China, Tel +86- 13308809792, Email [email protected]
Background: Axillary lymph node dissection (ALND) can be safely avoided in women with T1 or T2 primary invasive breast cancer (BC) and one to two metastatic sentinel lymph nodes (SLNs). However, cancellation of ALND based solely on SLN biopsy (SLNB) may lead to adverse outcomes. Therefore, preoperative assessment of LN tumor burden becomes a new focus for ALN status.
Objective: This study aimed to develop and validate a nomogram incorporating the radiomics score (rad-score) based on automated breast ultrasound system (ABUS) and other clinicopathological features for evaluating the ALN status in patients with early-stage BC preoperatively.
Methods: Totally 354 and 163 patients constituted the training and validation cohorts. They were divided into ALN low burden (< 3 metastatic LNs) and high burden (≥ 3 metastatic LNs) based on the histopathological diagnosis. The radiomics features of the segmented breast tumor in ABUS images were extracted and selected to generate the rad-score of each patient. These rad-scores, along with the ALN burden predictors identified from the clinicopathologic characteristics, were included in the multivariate analysis to establish a nomogram. It was further evaluated in the training and validation cohorts.
Results: High ALN burdens accounted for 11.2% and 10.8% in the training and validation cohorts. The rad-score for each patient was developed based on 7 radiomics features extracted from the ABUS images. The radiomics nomogram was built with the rad-score, tumor size, US-reported LN status, and ABUS retraction phenomenon. It achieved better predictive efficacy than the nomogram without the rad-score and exhibited favorable discrimination, calibration and clinical utility in both cohorts.
Conclusion: We developed an ABUS-based radiomics nomogram for the preoperative prediction of ALN burden in BC patients. It would be utilized for the identification of patients with low ALN burden if further validated, which contributed to appropriate axillary treatment and might avoid unnecessary ALND.
Keywords: axillary lymph node, sentinel lymph node biopsy, invasive breast cancer, radiomics, nomogram, automated breast ultrasound system, tumor burden
Introduction
Accurate assessment of axillary lymph node (ALN) status is of great significance for clinical staging, treatment strategies, and prognosis evaluation in patients with breast cancer (BC).1,2 Since 2017, the American Society of Clinical Oncology has updated the clinical practice guidelines based on the results of the Z0011 trials. Declares that axillary lymph node dissection (ALND) is no longer necessary for women with T1 or T2 primary invasive BC and one to two metastatic sentinel lymph nodes (SLNs) who are planning to undergo breast-conserving surgery with whole-breast radiotherapy.3,4 However, SLN biopsy (SLNB) has a false-negative rate of roughly 10% to diagnose the metastatic LNs,5,6 which means relying solely on the results of SLNB increases the risk of recurrence. Therefore, preoperative assessment of LN tumor burden rather than metastasis has become a new focus for ALN status.
Ultrasound (US) is currently one of the primary non-invasive imaging modalities for determining ALN status.7 However, studies have already proved that the diagnosis of ALN metastasis (ALNM) only by ultrasound is insufficient.8,9 According to the latest meta-analysis, 43.2% of US-positive patients had a low-risk nodal burden and could safely avoid ALND.10 This implies that the non-invasive identification of nodal burden by axillary US alone is inadequate, and more efficient methods are desired. Radiomics is an emerging tool that transfers digital medical images into mineable data based on machine-learning-based algorithms to improve the accuracy of disease diagnosis and prognosis prediction.11,12 Recently, the application of nomograms that combined radiomics signatures and clinicopathological characteristics has suggested improvement in predicting ALNM.13–15 Nevertheless, these previous works mainly focused on the radiomics features derived from magnetic resonance imaging (MRI) or dynamic contrast-enhanced MRI, which are quite costly and time-consuming. As an emerging US technology, automated breast ultrasound system (ABUS) can also provide reconstructed three-dimensional images of the breast lesion volumes,16,17 which has been approved by US Food and Drug Administration since 2012 to distinguish benign and malignant breast lesions.18 The updated studies supported the use of ABUS data for radiomics analysis in the diagnosis of BC.19 Additionally, a nomogram including ABUS features was constructed for effectively predicting metastatic ALN burden.20 Thus, whether ABUS-based radiomics contributes to the prediction of ALN tumor burden is an interesting topic, but there are currently few investigations on this subject.
Here, we investigated the potential use of the ABUS-based radiomics score (rad-score) as a predictive biomarker for high-risk nodal burden, and to develop and validate a nomogram incorporating a combination of the rad-score and other clinicopathological features for evaluating the ALN status in patients with early-stage BC.
Materials and Methods
This retrospective study was performed following the declaration of Helsinki and approved by the Institutional Review Boards at Yunnan Cancer Hospital (hospital A) (KYLX2022181) and Anning First People’s Hospital (hospital B) (2022-034-01), which waived the requirement for informed consent due to the retrospective nature of this study. We declared that patient data was maintained with confidentiality.
Patients
Between January 2015 and July 2022, after searching the medical databases from hospital A and hospital B, 843 patients who were confirmed to have primary invasive BC by postoperative pathological examination were reviewed. Patients in the study met the following inclusion criteria: 1) unifocal mass ≤ 5cm in diameter (stages T1 and T2) without palpable axillary adenopathy, 2) underwent breast US examination before biopsy, neoadjuvant chemotherapy, ablation, or radiotherapy, and 3) pathologically verified ALN status by SLNB / ALND. Patients with a history of ipsilateral axillary surgery, distant metastasis, poor-quality US or ABUS images, and incomplete clinical or pathological information were excluded. Ultimately, 354 patients from hospital A comprised the training cohort while 163 patients from hospital B made up the independent external validation cohort. All the excised ALNs were histologically examined and classified as metastatic (including macrometastasis and micrometastasis) and nonmetastatic nodes. The enrolled patients were defined as ALN low burden (< 3 metastatic LNs) and high burden (≥3 metastatic LNs) according to the final histopathological diagnosis.4 Figure 1 describes the study design and the patients’ screening pathway.
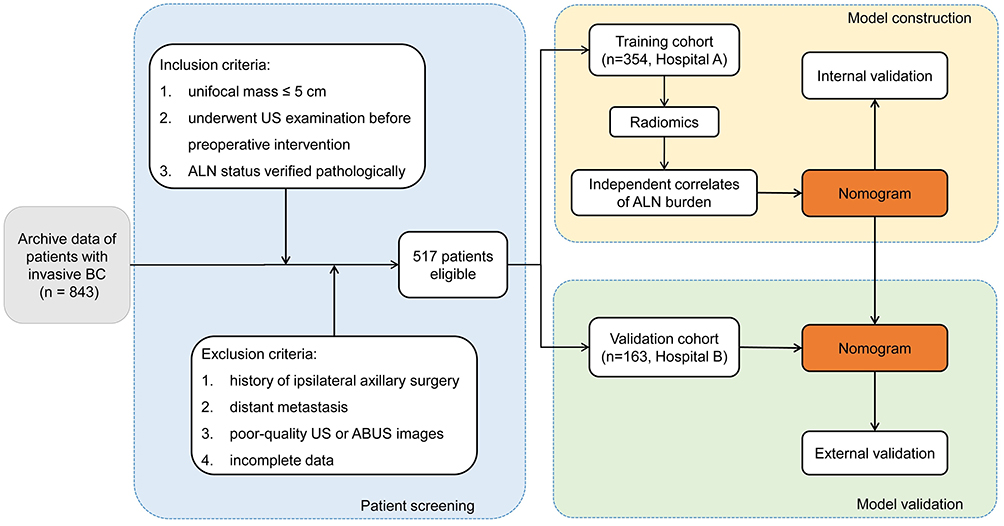 |
Figure 1 Workflow of necessary steps for patients’ screening pathway and model construction and validation. Abbreviations: BC, breast cancer; US, ultrasound; ABUS, automated breast ultrasound system; ALN, axillary lymph node; Hospital A, Yunnan Cancer Hospital; Hospital B, Anning First People’s Hospital. |
Preoperative Clinicopathologic Characteristics
The demographic information (age and BC family history), clinical data [tumor size (the maximum diameter measured on the grayscale US image) and clinical T stage], and pathological data of US-guided core-needle biopsy specimens [histologic type, estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor-2 (HER-2), and Ki-67 status] were retrieved from the medical records and pathologic systems. Preoperative ALN status was determined by axillary US, and US abnormal morphological features to identify metastatic LN were as follows: (1) cortical thickness ≥3 mm; (2) longitudinal axis-to-transverse axis ratio < 2; or (3) absence of fatty hilum.21
ABUS Acquisition for Radiomics
ABUS examinations at both medical centers were performed using Invenia™ ABUS (GE Healthcare, Sunnyvale, CA, USA) with the same setting. After the patient lying in a supine position with a gentle breath, the instrument progressively scanned the median, lateral, and medial positions of the breast sequentially and, when necessary, other planes. If a mass was found during the examination, the imaging feature of the mass “retraction phenomenon” in the coronal view (negative / positive) was recorded, and the axial, sagittal, and coronal images displaying the mass were exported for further radiomics analysis.
Lesion Segmentation and Feature Extraction
Utilizing ITK-SNAP software (version 3.8.0; http://www.itksnap.org/pmwiki/pmwiki.php), each breast lesion was manually segmented by two trained ultrasonographers with more than 10 years of experience in breast US who were blinded to the final histopathological diagnosis. To extract radiomics features, the region of interest (ROI) for each patient’s breast lesion was manually delineated on axial, sagittal, and coronal ABUS images, avoiding the inclusion of adjacent normal tissue. Contouring was drawn within the lesion boundary, and the adjacent tissue was carefully avoided. In total, 6 image types, 7 feature classes, and wavelet transform were automatically extracted using the PyRadiomics toolkit (v3.0.1) (Supplementary Figure S1).
Feature Selection and Rad-Score Development
All features extracted from the primary breast tumors were rescaled via Z-score normalization to facilitate the subsequent statistical analysis. The reproducibility of the extracted features was evaluated based on the inter-operator findings. The interclass correlation coefficients (ICCs) > 0.8 were considered satisfied agreement. Then, each feature was compared between patients with low and high ALN burden using a Student’s t-test. Finally, the least absolute shrinkage and selection operator (LASSO) logistic regression with 10-fold cross validation, which was suitable for removing the redundant or irrelevant features without much loss of information in machine learning,22 was utilized to select ALN burden related features with nonzero coefficients from those features with P-values < 0.05 in the t-test. The radiomics score (rad-score) of each patient was generated using a linear combination of the chosen features weighted by the LASSO algorithm. The flowchart of radiomics analysis workflow is outlined in Figure 2.
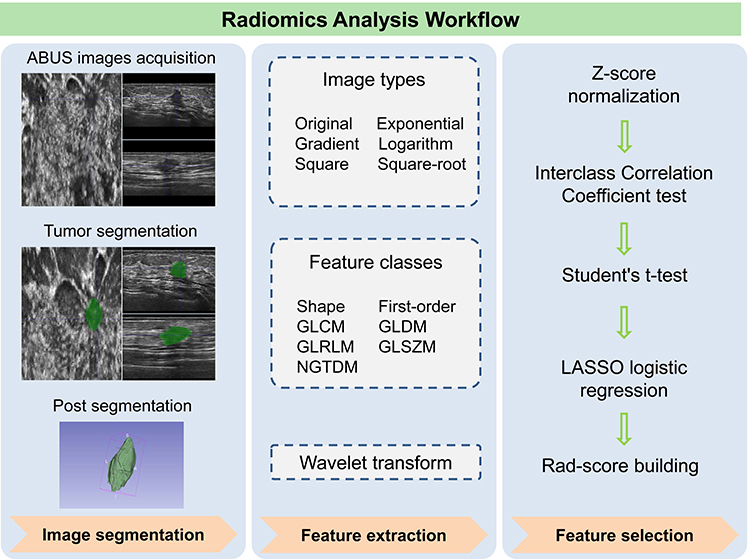 |
Figure 2 Workflow of the key steps in constructing an ABUS imaging-based rad-score for a BC patient. Breast tumor is first manually segmented on axial, sagittal, and coronal ABUS images to extract radiomics features. After normalization, a three-step feature selection method (Interclass Correlation Coefficient test, Student’s t-test, and LASSO logistic regression) was used to identify the key radiomics features related to metastatic LN burden and incorporate them into the rad-score. Abbreviations: BC, breast cancer; GLCM, gray-level co-occurrence matrix; GLDM, gray-level dependence matrix; GLRLM, gray-level run length matrix; GLSZM, gray-level size zone matrix; NGTDM, neighbouring grey tone difference matrix; LASSO, least absolute shrinkage and selection operator; rad-score, radiomics score. |
Construction and Validation of the Radiomics Nomogram
To develop a radiomics nomogram, the preoperative clinical characteristics, features identified by US and ABUS, and rad-scores were initially assessed using the univariate logistic analysis to investigate the predictors associated with the ALN burden. A multivariate logistic regression analysis was performed subsequently on all statistically significant variables in the univariate analysis. Then, a radiomics nomogram was developed by including all of the predictors and their related regression coefficients, and was evaluated in both the training and validation cohorts.
Statistical Analysis
Statistical analyses were conducted with IBM SPSS Statistics (version 22.0, SPSS Inc.), MedCalc software (version 19.2.1), R statistical software (version 4.2.1), and Python programming software (version 3.7.1). A two-sided P < 0.05 was used as the standard of statistically significant difference. Differences in characteristics between the training and validation cohorts were compared using independent sample t-test, Chi-square test, and Mann–Whitney U-test, as appropriate. In the validation and clinical utility of the radiomics nomogram, the receiver operating characteristic (ROC) curve was utilized to evaluate the discrimination of the nomogram. Through bootstrapping with 1000 resamples, the calibration was evaluated using a calibration curve, and the Hosmer-Lemeshow (HL) test was used to determine the goodness-of-fit. The clinical usefulness of the model was assessed with the calculation of the net benefits determined by a decision curve analysis (DCA).
Results
Patient Summary
The medical records of 354 patients in the training cohort and 163 patients in the validation cohort were analyzed. High ALN burdens (≥3 metastatic LNs) accounted for 11.2% (95/354) and 10.8% (47/163) in the training and validation cohorts, respectively. There were no statistically significant differences in ALN burden distribution, preoperative clinicopathologic characteristics, and rad-scores between the two cohorts (all P values > 0.05). Details of the two cohorts are listed in Supplemental Table S1.
Radiomics Analyses for Rad-Score
In the training cohort, a total of 1316 radiomics features from each ABUS image were extracted and normalized. Their ICCs ranged from 0.5 to 0.99, and 1109 (84.3%) features with intra-observer ICC ≥ 0.8 were selected for subsequent Student’s t-test. Finally, seven ALN status related features with nonzero coefficients were selected using a LASSO logistic regression model (Figures 3A and B). The rad-score for each patient was developed based on these features and their weights, which were the correlation between the features and ALN burden status (Figure 3C). Its calculation formula is presented in Supplemental Appendix 1. There was a significant difference in rad-score between patients with and without high ALN burden (0.282±0.038 vs 0.263±0.037; P < 0.001). ROC curve analysis showed that the rad-score had a moderate predictive efficacy predicting ALN status, with the AUC of 0.764 [95% confidence interval (CI): 0.717–0.808] (Figure 3D).
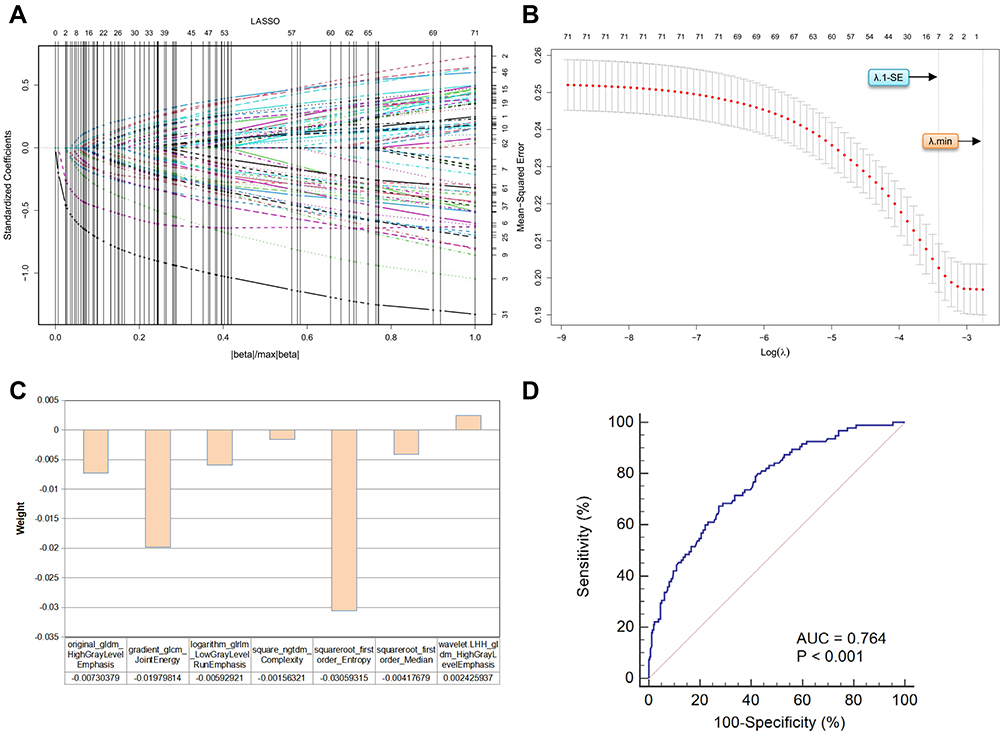 |
Figure 3 Radiomics feature selection using LASSO logistic regression for establishing the rad-score. (A) LASSO coefficient distribution of the 71 radiomics features. (B) Selection of the tuning parameter (λ) using 10-fold cross validation via the minimum criteria (λ.min) and the 1-standard error of the minimum criteria (λ.1-SE). The optimal λ results in 7 features with nonzero coefficients. (C) The weights of the selected radiomics features. (D) ROC curve of the rad-score for predicting high ALN burden. Abbreviations: LASSO, least absolute shrinkage and selection operator; λ, penalty regularization parameter; AUC, area under the curve. |
Radiomics Nomogram Development
To develop the radiomics nomogram, the clinicopathologic characteristics and rad-scores were assessed using univariate logistic regression followed by multivariate logistic regression (Table 1). The result revealed that high ALN burden was independently associated with tumor size, US-reported LN status, ABUS retraction phenomenon, and rad-score (all P < 0.05). High ALN burden was more prevalent in patients who had US-reported metastatic ALN, larger tumor size, higher rad-score, and negative ABUS retraction phenomenon [odds ratio (OR): 1.853, 1.602, 4.159, and 0.456, respectively]. The radiomics nomogram was built with these selected predictors to preoperatively visualize the likelihood of high ALN burden in BC patients (Figure 4).
 |
Table 1 Univariate and Multivariate Logistic Regression Analyses for the Independent Correlates of High ALN Burden |
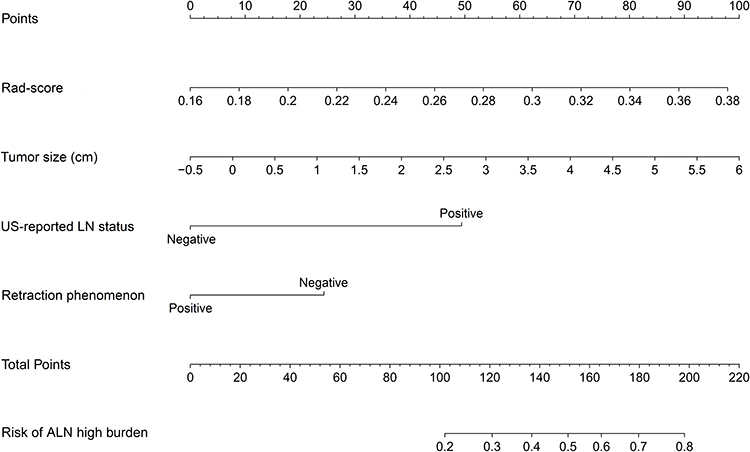 |
Figure 4 Radiomics nomogram for preoperatively assessing the likelihood of high ALN burden in BC patients. It is developed by combining tumor size, US-reported LN status, ABUS retraction phenomenon, and rad-score with weights equal to the OR values. Abbreviations: Rad-score, radiomics score; OR, odds ratio; US, ultrasound; LN, lymph node; ABUS, automated breast ultrasound system. |
Model Validation
The discriminations of the radiomics nomogram and the clinical nomogram (building without the rad-score) were tested with the ROC curves, as indicated in Figure 5A and B. In the training cohort, the AUC of the radiomics nomogram was 0.924 (95% CI: 0.891 to 0.949), which denoted an outstanding performance in discrimination.23 After applying the original model to the validation cohort, its discrimination was still pretty good even with reductions [AUC: 0.812 (95% CI: 0.767 to 0.851)].
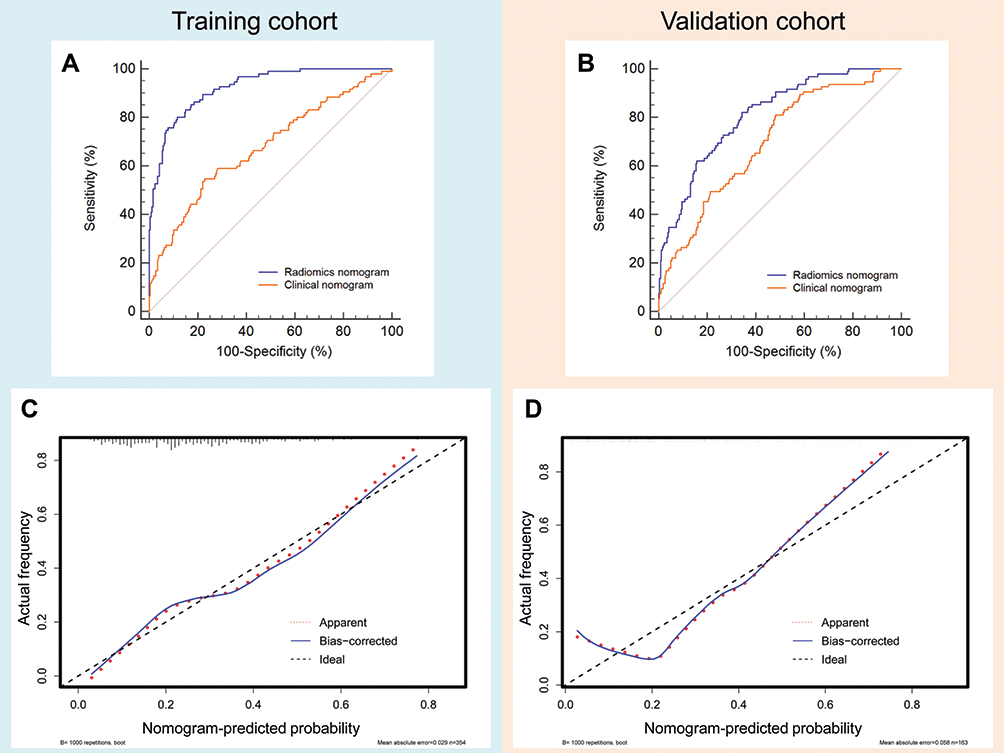 |
Figure 5 Evaluation of the discrimination and calibration in training and validation cohorts. (A and B) show the ROC curves in the training and validation cohorts, respectively, for comparing the discrimination of radiomics nomogram and clinical nomogram (building without the rad-score). The discrimination of the radiomics nomogram is higher than that of the clinical nomogram in both cohorts. (C and D) show the calibration curves of the radiomics nomogram in the training and validation cohorts, respectively. The bias curve for the training cohort is close to the ideal line, indicating good agreement. The curve for the validation cohort presents underestimation when the predicted risk is ≥ 60%, but the overall agreement remains good. Abbreviations: ROC, receiver operating characteristic; rad-score, radiomics score. |
Compared with the radiomics nomogram, the discrimination of the clinical nomogram was significantly lower both in the training [AUC: 0.699 (95% CI: 0.649 to 0.747); P < 0.001 for DeLong test] and validation cohort [AUC: 0.677 (95% CI: 0.625 to 0.725); P < 0.001 for DeLong test]. It indicated that the radiomics nomogram achieved better predictive efficacy than the nomogram without the rad-score in both cohorts.
The calibration curves of the radiomics nomogram revealed good agreement between the nomogram-predicted and the observed ALN status in the training and validation cohorts (Figures 5C and D). The HL test yielded a nonsignificant P value of 0.538 and 0.374 in both cohorts, suggesting the good calibration capability of the radiomics nomogram.
Clinical Use of the Model
Figure 6 summarizes the clinical application of the radiomics nomogram by means of DCA. The plots showed that using the radiomics nomogram to predict the ALN burden adds more net benefit than the treat-all or treat-none scheme, with a threshold probability ranging from 10 to 80% in the training cohort and 20 to 90% in the validation cohort.
 |
Figure 6 DCA of the radiomics nomogram for predicting the high ALN burden in the training and validation cohorts. Both (A) (training cohort) and (B) (validation cohort) reveal that using the radiomics nomogram to predict the ALN burden adds more net benefit than the treat-all or treat-none scheme. Abbreviations: DCA, decision curve analysis; ALN, axillary lymph node. |
Example of the Radiomics Nomogram
For example, patient A was a 55-year-old female. She was diagnosed with a 2.5-cm-sized breast lesion with positive US-reported ALN and negative retraction phenomenon. Her rad-score was 0.29. The corresponding scores were: 58 points for rad-score, 45 points for tumor size, 50 points for positive US-reported LN status, and 22 points for negative ABUS retraction phenomenon. Her total score was 175 points, and the risk of a high ALN burden exceeded 65%. Pathology confirmed 4 metastatic ALNs in this patient. Patient B was a 50-year-old female. She was diagnosed with a 2-cm-sized breast lesion with negative US-reported ALN and retraction phenomenon. Her rad-score was 0.26. Her total score was calculated to be approximately 110 (25% of predicted risk), implying that this patient had a low ALN burden. Pathology confirmed that she had only one ALN micrometastasis.
Discussion
In the present study, an ABUS-based radiomics nomogram incorporating the ALN status related rad-score and preoperative clinicopathologic features was developed and validated as a novel method for the prediction of ALN burden in patients with early-stage invasive BC. It outperformed the clinical nomogram that was built without the rad-score and exhibited favorable discrimination, calibration, and clinical utility in both training and validation cohorts. If further validated, it may contribute to the determination of BC surgical options.
According to the Z0011 trial, ALND provided no benefit in patients with one to two metastatic SLNs.3 This means SLNB should be performed to determine the status of ALN burden regardless of whether clinically positive LNs are present or absent. However, a meta-analysis by Pesek et al6 revealed that the false-negative rate of SLNB is conservatively estimated to be around 10%. Canceling ALND based only on SLNB results may lead to adverse outcomes, including inadequate cancer staging and increased risk of recurrence. Therefore, there is an urgent need to develop a non-invasive protocol to predict the presence of multiple metastatic ALNs. It helps to increase the confidence of surgeons to omit ALND in BC patients with low ALN burden.
In this study, we developed a nomogram that integrated the ABUS rad-score with preoperative clinicopathological features to further improve its predictive accuracy for ALN burden status. Although various predictive models have been constructed to assess the likelihood of ALN status, they are beyond clinical implication because some predictors in their models are available postoperatively.24–26 Comparatively, predictive models developed using only preoperative imaging data, clinical details, and pathological information obtained from biopsies may be preferable in clinical practice. With the development of radiomics, some studies have explored the application of radiomics in predicting ALN status and achieved good performance.13,27–29 However, most studies are designed based on MRI, which is detrimental to being popularized in clinical practice because it is expensive and time-consuming. Similar to MRI, the ABUS utilized in this study could provide three-dimensional images of the breast without depending on the sonographers’ experience. The nomogram incorporating the ABUS rad-score allowed non-invasive assessment of the ALN status before surgery, which is convenient for clinical promotion.
It is well known that intra-tumoral heterogeneity, which cannot be objectively evaluated by visual interpretation, can be analyzed by radiomics.30 Although radiomics has been successfully applied to MRI and CT, its application to US or ABUS is somewhat behind schedule. Recently, radiomics has demonstrated the potential in differentiating benign and malignant tumors using ABUS images.19,31,32 According to the investigation of the radiomics biological mechanisms by Panth et al33 radiomics was also linked to tumor phenotype and genotype. By measuring the intra-tumoral heterogeneity, radiomics features may consequently be able to assess the status of lymph nodes. In our study, the rad-score was developed based on 6 image types, 7 feature classes, and wavelet transform extracted from ABUS images, which demonstrated that it was related to the status of ALN burden. To further improve the predictive performance of rad-score, the clinicopathologic features of BC were also assessed and incorporated to build an integrative radiomics-based nomogram. Besides the rad-score, we found larger tumor size, US-reported metastatic ALN, and negative ABUS retraction phenomenon were the independent predictors for high ALN burden. Among these, ABUS retraction phenomenon is a special predictor, which has been an effective feature in the diagnosis of BC.16 However, its appearance may also prevent early ALNM in a sense, because it is caused by a desmoplastic response around the malignant lesion, which prevents the rapid invasion and metastasis of BC cells.34
The ABUS-based radiomics nomogram established in this study showed good performance for the risk of high ALN burden in BC patients. However, we have to acknowledge the limitations of this study. First, due to the retrospective nature, the number of abnormal LNs was not purposefully determined in some axillary US examinations. Therefore, the value of US assessment of ALN burden requires further investigation. Second, despite the consideration of reproducibility from an inter-observer perspective, potential vendor variabilities in ABUS assessments may affect the performance of subsequent radiomics analysis. Third, patients with multifocal and non-mass-like tumors were excluded, which might lead to selection bias and limited generalizability of our results. However, accurately delineating the boundaries of non-mass-like lesions is a challenge. It is also difficult to determine which lesion is responsible for the metastatic ALN and should be selected for multifocal radiomics analysis. Finally, despite our satisfaction with the model’s performance, the prediction results should be interpreted with caution. In fact, we do not think this radiomics nomogram can replace SLNB results, and it is suitable for facilitating surgical recommendations (For example, recommending reassessment when there is a disagreement between SLNB and nomogram, or increasing confidence when they are identical). Further multicenter studies with a larger sample size are needed in future studies for the clinical application of our radiomics nomogram.
Conclusion
We developed an ABUS-based radiomics nomogram for the preoperative prediction of ALN burden status in patients with early-stage BC. This model was shown to have a favorable prediction performance, demonstrating its potential to assist decision-making for appropriate axillary treatment and avoid unnecessary invasive operations, such as ALND, in BC patients with low ALN burden.
Data Sharing Statement
The data during the current study are available from the corresponding author on reasonable request.
Ethical Approval
Ethical approvals for the study were obtained from the Institutional Review Boards at Yunnan Cancer Hospital (KYLX2022181) and Anning First People’s Hospital (2022-034-01).
Informed Consent
Informed consents were waived due to the retrospective nature of this study. We declared that patient data was maintained with confidentiality.
Acknowledgments
The authors wish to thank all the study participants, research staff and students who participated in this work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Study design: Ning Li, Chao Song, Hongjiang Zhang, and Xian Huang.
Data collection and analysis: Ning Li, Chao Song, Hongjiang Zhang, Xian Huang, Juhua He, Juan Su, Lichun Yang, and Guihua Cui.
Supervision: Chao Song and Hongjiang Zhang.
Statistics: Ning Li, Juhua He, Chao Song, Xian Huang, and Hongjiang Zhang.
Manuscript writing: Ning Li, Chao Song, Hongjiang Zhang, and Xian Huang.
Manuscript revision: Ning Li, Chao Song, Hongjiang Zhang, and Xian Huang.
Approval of the manuscript: all authors.
Funding
Supported by Kunming Health Talents Training Project [2021-SW(reserve)-78] and Yunnan Academician Expert Workstation (202105AF150087).
Disclosure
The authors declare that they have no conflict of interest.
References
1. Park KU, Caudle A. Management of the axilla in the patient with breast cancer. Surg Clin North Am. 2018;98(4):747–760. doi:10.1016/j.suc.2018.04.001
2. Chang JM, Leung JWT, Moy L, Ha SM, Moon WK. Axillary nodal evaluation in breast cancer: state of the art. Radiology. 2020;295(3):500–515. doi:10.1148/radiol.2020192534
3. Giuliano AE, Ballman KV, McCall L, et al. Effect of axillary dissection vs no axillary dissection on 10-year overall survival among women with invasive breast cancer and sentinel node metastasis: the ACOSOG Z0011 (Alliance) randomized clinical trial. JAMA. 2017;318(10):918–926. doi:10.1001/jama.2017.11470
4. Lyman GH, Somerfield MR, Bosserman LD, Perkins CL, Weaver DL, Giuliano AE. Sentinel lymph node biopsy for patients with early-stage breast cancer: American Society of clinical oncology clinical practice guideline update. J Clin Oncol. 2017;35(5):561–564. doi:10.1200/jco.2016.71.0947
5. Krag DN, Anderson SJ, Julian TB, et al. Technical outcomes of sentinel-lymph-node resection and conventional axillary-lymph-node dissection in patients with clinically node-negative breast cancer: results from the NSABP B-32 randomised Phase III trial. Lancet Oncol. 2007;8(10):881–888. doi:10.1016/s1470-2045(07)70278-4
6. Pesek S, Ashikaga T, Krag LE, Krag D. The false-negative rate of sentinel node biopsy in patients with breast cancer: a meta-analysis. World J Surg. 2012;36(9):2239–2251. doi:10.1007/s00268-012-1623-z
7. Marino MA, Avendano D, Zapata P, Riedl CC, Pinker K. Lymph node imaging in patients with primary breast cancer: concurrent diagnostic tools. Oncologist. 2020;25(2):e231–e242. doi:10.1634/theoncologist.2019-0427
8. Patani NR, Dwek MV, Douek M. Predictors of axillary lymph node metastasis in breast cancer: a systematic review. Eur J Surg Oncol. 2007;33(4):409–419. doi:10.1016/j.ejso.2006.09.003
9. Du LW, Liu HL, Gong HY, et al. Adding contrast-enhanced ultrasound markers to conventional axillary ultrasound improves specificity for predicting axillary lymph node metastasis in patients with breast cancer. Br J Radiol. 2021;94(1118):20200874. doi:10.1259/bjr.20200874
10. Ahmed M, Jozsa F, Baker R, Rubio IT, Benson J, Douek M. Meta-analysis of tumour burden in pre-operative axillary ultrasound positive and negative breast cancer patients. Breast Cancer Res Treat. 2017;166(2):329–336. doi:10.1007/s10549-017-4405-3
11. Lambin P, Leijenaar RTH, Deist TM, et al. Radiomics: the bridge between medical imaging and personalized medicine. Nat Rev Clin Oncol. 2017;14(12):749–762. doi:10.1038/nrclinonc.2017.141
12. Gillies RJ, Kinahan PE, Hricak H. Radiomics: images are more than pictures, they are data. Radiology. 2016;278(2):563–577. doi:10.1148/radiol.2015151169
13. Qiu Y, Zhang X, Wu Z, et al. MRI-based radiomics nomogram: prediction of axillary non-sentinel lymph node metastasis in patients with sentinel lymph node-positive breast cancer. Front Oncol. 2022;12:811347. doi:10.3389/fonc.2022.811347
14. Song D, Yang F, Zhang Y, et al. Dynamic contrast-enhanced MRI radiomics nomogram for predicting axillary lymph node metastasis in breast cancer. Cancer Imaging. 2022;22(1):17. doi:10.1186/s40644-022-00450-w
15. Cui X, Wang N, Zhao Y, et al. Preoperative prediction of axillary lymph node metastasis in breast cancer using radiomics features of DCE-MRI. Sci Rep. 2019;9(1):2240. doi:10.1038/s41598-019-38502-0
16. Zheng FY, Yan LX, Huang BJ, et al. Comparison of retraction phenomenon and BI-RADS-US descriptors in differentiating benign and malignant breast masses using an automated breast volume scanner. Eur J Radiol. 2015;84(11):2123–2129. doi:10.1016/j.ejrad.2015.07.028
17. Vourtsis A, Kachulis A. The performance of 3D ABUS versus HHUS in the visualisation and BI-RADS characterisation of breast lesions in a large cohort of 1886 women. Eur Radiol. 2018;28(2):592–601. doi:10.1007/s00330-017-5011-9
18. U.S. Food and Drug Administration. Medical Devices: Somo-v Automated Breast Ultrasound System (ABUS): P110006 [Internet]. Silver Spring, MD: U.S. Food and Drug Administration; 2012. Available from: http://wayback.archive-it.org/7993/20170112091556/http://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/DeviceApprovalsandClearances/Recently-ApprovedDevices/ucm320724.htm.
19. Wang H, Yang X, Ma S, Zhu K, Guo S. An optimized radiomics model based on automated breast volume scan images to identify breast lesions: comparison of machine learning methods: comparison of machine learning methods. J Ultrasound Med. 2022;41(7):1643–1655. doi:10.1002/jum.15845
20. Zhao F, Cai C, Liu M, Xiao J. Identification of the lymph node metastasis-related automated breast volume scanning features for predicting axillary lymph node tumor burden of invasive breast cancer via a clinical prediction model. Front Endocrinol. 2022;13:881761. doi:10.3389/fendo.2022.881761
21. Koelliker SL, Chung MA, Mainiero MB, Steinhoff MM, Cady B. Axillary lymph nodes: US-guided fine-needle aspiration for initial staging of breast cancer--correlation with primary tumor size. Radiology. 2008;246(1):81–89. doi:10.1148/radiol.2463061463
22. Muthukrishnan R, Rohini R. LASSO: a feature selection technique in predictive modeling for machine learning.
23. Mandrekar JN. Receiver operating characteristic curve in diagnostic test assessment. J Thorac Oncol. 2010;5(9):1315–1316. doi:10.1097/JTO.0b013e3181ec173d
24. Bevilacqua JL, Kattan MW, Fey JV, Cody HS 3rd, Borgen PI, Van Zee KJ. Doctor, what are my chances of having a positive sentinel node? A validated nomogram for risk estimation. J Clin Oncol. 2007;25(24):3670–3679. doi:10.1200/jco.2006.08.8013
25. Pal A, Provenzano E, Duffy SW, Pinder SE, Purushotham AD. A model for predicting non-sentinel lymph node metastatic disease when the sentinel lymph node is positive. Br J Surg. 2008;95(3):302–309. doi:10.1002/bjs.5943
26. Kohrt HE, Olshen RA, Bermas HR, et al. New models and online calculator for predicting non-sentinel lymph node status in sentinel lymph node positive breast cancer patients. BMC Cancer. 2008;8:66. doi:10.1186/1471-2407-8-66
27. Zhang X, Yang Z, Cui W, et al. Preoperative prediction of axillary sentinel lymph node burden with multiparametric MRI-based radiomics nomogram in early-stage breast cancer. Eur Radiol. 2021;31(8):5924–5939. doi:10.1007/s00330-020-07674-z
28. Han L, Zhu Y, Liu Z, et al. Radiomic nomogram for prediction of axillary lymph node metastasis in breast cancer. Eur Radiol. 2019;29(7):3820–3829. doi:10.1007/s00330-018-5981-2
29. Liu Y, Li X, Zhu L, et al. Preoperative prediction of axillary lymph node metastasis in breast cancer based on intratumoral and peritumoral DCE-MRI radiomics nomogram. Contrast Media Mol Imaging. 2022;2022:6729473. doi:10.1155/2022/6729473
30. Aerts HJ, Velazquez ER, Leijenaar RT, et al. Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nat Commun. 2014;5:4006. doi:10.1038/ncomms5006
31. Wang S-J, Liu H-Q, Yang T, et al. Machine learning based on automated breast volume scanner (ABVS) radiomics for differential diagnosis of benign and malignant BI-RADS 4 lesions. Int J Imaging Syst Technol. 2022;32(5):1577–1587. doi:10.1002/ima.22724
32. Wang SJ, Liu HQ, Yang T, et al. Automated breast volume scanner (ABVS)-based radiomic nomogram: a potential tool for reducing unnecessary biopsies of BI-RADS 4 lesions. Diagnostics. 2022;12(1). doi:10.3390/diagnostics12010172
33. Panth KM, Leijenaar RT, Carvalho S, et al. Is there a causal relationship between genetic changes and radiomics-based image features? An in vivo preclinical experiment with doxycycline inducible GADD34 tumor cells. Radiother Oncol. 2015;116(3):462–466. doi:10.1016/j.radonc.2015.06.013
34. Jiang J, Chen YQ, Xu YZ, et al. Correlation between three-dimensional ultrasound features and pathological prognostic factors in breast cancer. Eur Radiol. 2014;24(6):1186–1196. doi:10.1007/s00330-014-3135-8
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Predictive Clinical-Radiomics Nomogram for Differentiating Tuberculous Spondylitis from Pyogenic Spondylitis Using CT and Clinical Risk Factors
Wu S, Wei Y, Li H, Zhou C, Chen T, Zhu J, Liu L, Wu S, Ma F, Ye Z, Deng G, Yao Y, Fan B, Liao S, Huang S, Sun X, Chen L, Guo H, Chen W, Zhan X, Liu C
Infection and Drug Resistance 2022, 15:7327-7338
Published Date: 13 December 2022
Radiomics Nomogram Model Based on TOF-MRA Images: A New Effective Method for Predicting Microaneurysms
Kong D, Li J, Lv Y, Wang M, Li S, Qian B, Yu Y
International Journal of General Medicine 2023, 16:1091-1100
Published Date: 27 March 2023
Integration of Multimodal Computed Tomography Radiomic Features of Primary Tumors and the Spleen to Predict Early Recurrence in Patients with Postoperative Adjuvant Transarterial Chemoembolization
Chen C, Liu J, Gu Z, Sun Y, Lu W, Liu X, Chen K, Ma T, Zhao S, Zhao H
Journal of Hepatocellular Carcinoma 2023, 10:1295-1308
Published Date: 8 August 2023
Shear-Wave Elastography-Based Radiomics Nomogram for the Prediction of Cardiovascular Disease in Patients with Diabetic Kidney Disease
Meng F, Wu Q, Zhang W, Hou S
Diabetes, Metabolic Syndrome and Obesity 2023, 16:2705-2716
Published Date: 7 September 2023
Deep-Learning-Based Radiomics to Predict Surgical Risk Factors for Lumbar Disc Herniation in Young Patients: A Multicenter Study
Fan Z, Wu T, Wang Y, Jin Z, Wang T, Liu D
Journal of Multidisciplinary Healthcare 2024, 17:5831-5851
Published Date: 7 December 2024