Back to Journals » Journal of Pain Research » Volume 16
Opioid Initiation Within One Year After Starting a Digital Musculoskeletal (MSK) Program: An Observational, Longitudinal Study with Comparison Group
Authors Wang G, Lu L, Gold LS, Bailey JF
Received 24 March 2023
Accepted for publication 24 July 2023
Published 27 July 2023 Volume 2023:16 Pages 2609—2618
DOI https://doi.org/10.2147/JPR.S412081
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Timothy Atkinson
Grace Wang,1 Louie Lu,1 Laura S Gold,2 Jeannie F Bailey3
1Clinical Research, Hinge Health, Inc, San Francisco, CA, USA; 2Clinical Learning, Evidence and Research Center, University of Washington, Seattle, WA, USA; 3Orthopaedic Surgery, University of California, San Francisco, CA, USA
Correspondence: Grace Wang, Senior Director of Clinical Research, Hinge Health, Inc, 455 Market Street, Floor 7, San Francisco, CA, 94105-2437, USA, Tel +1 415 900-3997, Email [email protected]
Background: In-person, conservative care may decrease opioid use for chronic musculoskeletal (MSK) pain, but the impact of digitally delivered conservative care on opioid use is unknown. This study examines associations between a digital MSK program and opioid initiation and prescriptions among opioid naive adults with chronic MSK pain.
Methods: This observational study used commercial medical and pharmacy claims data to compare digital MSK program members to matched physical therapy (PT) patients. Outcomes were any opioid prescriptions and opioid prescriptions per 100 participants within the 12-months after starting a digital MSK program. After propensity-score matching, we conducted multivariate regression models that controlled for demographic, comorbidity, and baseline MSK healthcare use.
Results: The study included 4195 members and 4195 matched PT patients. For opioid initiation, 7.89% (95% Confidence Interval [CI]: 7.07%, 8.71%) of members had opioid prescriptions within 12 months after starting the digital MSK program versus 13.64% (95% CI: 12.60%, 14.67%) of matched PT patients (p < 0.001). Members had significantly fewer opioid prescriptions (16.73 per 100 participants; 95% CI: 14.11, 19.36) versus PT patients (22.36 per 100 participants; 95% CI: 19.99, 24.73). Members had lower odds (OR: 0.52, 95% CI: 0.45, 0.60) of initiating opioids and significantly fewer prescriptions per 100 participants (beta: − 6.40, 95% CI: − 9.88, − 2.93) versus PT patients after controlling for available confounding factors.
Conclusion: An MSK program that delivers conservative care digitally may be a promising approach for decreasing opioid initiation among individuals with chronic MSK pain given the limitations of the observational design and matching on only available covariates.
Keywords: musculoskeletal pain, telemedicine, telerehabilitation, opioid, claims analysis
Plain Language Summary
In-person conservative care is a best practice for managing chronic MSK pain and may help to prevent people from starting opioids (ie, opioid initiation). We did this study to see if conservative care delivered digitally might also lower opioid initiation. Using medical claims data, we identified people with MSK needs who did not have any opioid prescriptions one year before starting a digital MSK program or in-person physical therapy (PT). We found that 7.89% of members of a digital MSK program had new opioid prescriptions within one year of starting the program. In contrast, 13.64% of patients in PT had new opioid prescriptions within one year after PT.
Introduction
Musculoskeletal (MSK) disorders affected 127.4 million Americans in 2019 and greatly contributed to disability worldwide.1,2 MSK disorders were the third most prevalent diseases or injuries in the U.S in 2019 and have been the primary reasons for healthcare spending over time.3 In 2016, payers spent $380.9 billion on MSK disorders.4
To manage chronic MSK pain, clinical guidelines from several countries and professional associations recommend conservative care including physical activity, exercises, strengthening, and mobility.5,6 For example, guidelines covering osteoarthritis, low back pain, and neck pain recommend physical activity/exercise and activity maintenance with guidelines for osteoarthritis further recommending strengthening, mobility, and other activities specifically.6 Moderate to strong evidence has shown that these conservative care approaches result in improvements in pain and function.7,8
Opioids may also be used to manage MSK needs, but guidelines urge providers to assess the risks and benefits of opioid use and careful consideration of duration of use.5,6,9 The cautious tone in chronic MSK pain guidelines is the result of adverse event risks associated with opioid use and the potential for diversion and nonmedical use.10,11 Despite risks, opioid use for chronic MSK pain persists.12–16
By improving pain and function, guideline-adherent, in-person conservative care may curb opioid initiation and use.17,18 For example, PT is associated with decreases in opioid prescriptions. Privately insured adults with low back pain living in the northwestern United States had 87.6% lower probability of receiving an opioid prescription versus those with no PT.19 Similarly, Thackeray et al reported that taking part in PT versus not taking part significantly decreased the odds of receiving an opioid prescription (OR: 0.47; 95% CI: 0.24 to 0.92) among Medicaid covered patients with back pain in 2013.20
Although in-person conservative care decreases opioid initiation, the impact of digitally delivered conservative care on opioid use is unknown. Systematic reviews have shown that digital MSK programs resulted in statistically significant pain and functional improvement compared to waiting-list, usual care, or active controls (eg, health education).21–25 We also previously reported on significant improvements in self-reported pain and function in our specific digital MSK program.26–29 But, we have not conducted a study to examine the impact of the digital MSK program on opioid use among these same members. Therefore, this study’s objective is to examine the extent to which conservative care delivered digitally decreases opioid initiation and prescriptions among individuals with no opioid use in the past 12 months.
Materials and Methods
Study Design
We conducted an observational, cohort study using medical claims data, comparing digital MSK program members (herein, members) versus propensity-score matched nonparticipants who had physical therapy (herein, PT patients).
Supplementary Materials, Tables S1–S3 provides additional information about definitions used to identify and classify claims.
Digital MSK Program Description
The digital MSK program has been described in detail previously.26 In brief, the program was a health benefit for employees and dependents offered through 160 employers. The digital MSK program’s goal was to help participants manage chronic MSK pain. It provided members with tablet computers with a program app and wearable motion sensors (InvenSense MPU-6050, TDK Electronics, Tokyo, Japan). The program app used “playlists” to present exercises via animations and videos. Based on information from the sensors, the app provided feedback during exercises about repetitions and range of movement. After exercises, the app presented educational resources to members. Certified health coaches and physical therapists were available to guide members and support program adherence.
Study Participants
The study included two groups. Members were adults (18 to 64 years) who reported via the application that they had more than 12 weeks of back, knee, shoulder, hip, or neck pain. Members started the digital MSK program between January 2020 and October 2020.
PT patients were adults with a PT visit index event for chronic back, knee, shoulder, hip, or neck pain between January 2020 and October 2020, as identified in claims data. All members and PT patients had continuous employer-based medical and pharmacy benefit coverage for the 12 months before (herein, baseline) and 12 months after (herein, post period) starting the digital MSK program or PT index event.
Study exclusion criteria were as follows: any MSK surgery or opioid prescriptions during baseline; pregnancy, childbirth, or malignant cancer during the baseline or post period; missing demographics data; or total medical cost over $102,787.80 (99th percentile) during the baseline or post period.
Outcome Variables
The primary outcome was whether the study participant had any opioid prescriptions within 12 months after starting the digital MSK program or having PT (no/yes). A secondary outcome was the average number of opioid prescriptions in the post period per 100 participants.
Confounding Variables
The study included demographics (age, gender, census division) and comorbidities (hypertension, heart disease, diabetes, obesity, mental health needs, substance use disorders, autoimmune disorders, neurological disorders, respiratory disorders, additional MSK pain regions). We also identified MSK-related health care use during baseline. We included the per participant mean number of injections, emergency department (ED) visits, orthopedic surgeon visits, PT visits, and chiropractor visits. We included presence/absence of evaluation and management (E&M) services, imaging, tests (eg, laboratory), anesthesia, durable medical equipment (DME), and other invasive procedure (eg, vertebroplasty, destruction by neurolytic agent).
Data Source
We used de-identified, person-level enrollment, medical claims, and pharmacy claims data files from a commercial health plan aggregator. The database represents more than 100 million commercially insured lives across all states in the United States. Data with enrollment dates and dates of service between January 2019 and September 2021 were included in this study.
Statistical Methods
Within each pain region, we calculated a propensity score for each individual using a logit model with demographics, comorbidities and other concurrent pain region(s), and baseline MSK-related health care use. Then we matched PT patients in each respective pain region to members on propensity score, using full Mahalanobis matching with 1:1 nearest neighbor without replacement and without caliper (Stata command psmatch2). The final analytic sample included 4195 members and 4195 PT patients.
To characterize the study participants, we generated descriptive statistics and standardized mean difference (SMD) for the matched sample for baseline demographics, comorbidities, MSK-related health care use, and outcomes.
For main findings, we conducted unadjusted regression models and adjusted multivariate regression models that included all demographic, comorbidity, and baseline MSK healthcare use variables. We conducted logistic regression for opioid initiation and linear regression for prescription number. Finally, we used postestimation predictions to report outcomes as adjusted percentages or means for each group.
We used Stata statistical software (version 17.0, Stata Corp, College Station, Texas, USA) to conduct the analyses. A two-sided p < 0.05 was taken to indicate statistical significance. Data analysis was performed in October 2022.
Results
Descriptive results
Table 1 shows the demographics of the study participants in the propensity matched groups. Depending on pain region, between 38% and 62% of participants were female, and 52% to 82% of participants were in the 50 to 64 age range. After matching, the members and PT patients did not exhibit any significant differences in baseline demographics.
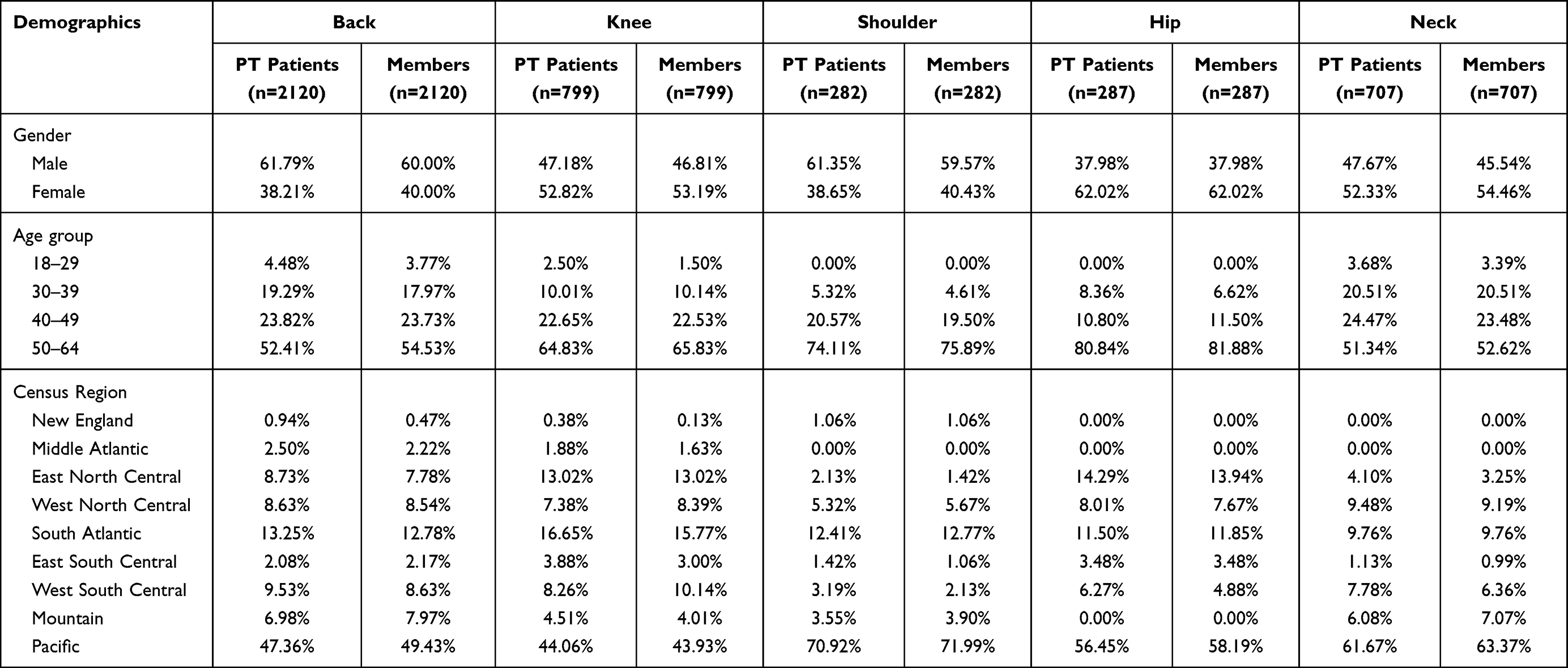 |
Table 1 Study Participant Demographics, by Pain Region, After Matching |
Table 2 shows study participants’ comorbidities. Across all pain regions, the most common comorbidities were hypertension, mental health needs, and diabetes. Less than 5% of study participants had medical claims related to other MSK pain regions. After matching, the members and PT patients did not exhibit any significant differences in baseline comorbidities.
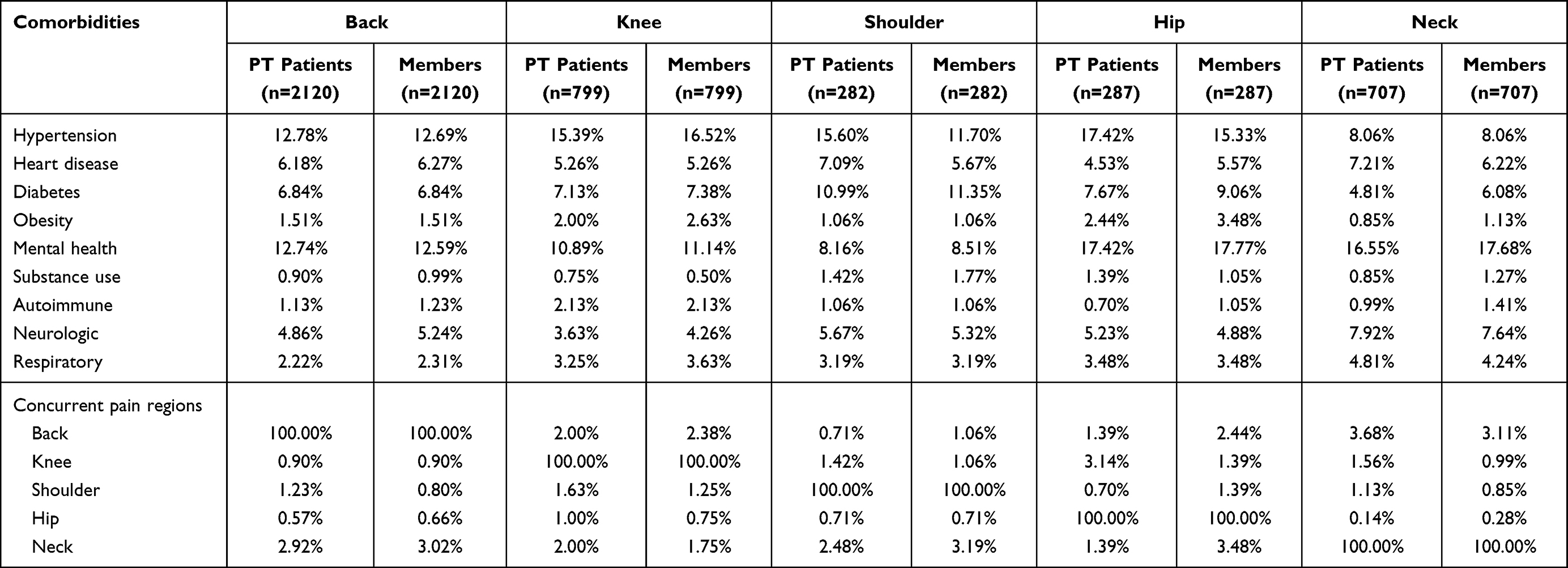 |
Table 2 Study Participant Comorbidities, by Pain Region, After Matching |
Table 3 shows MSK-related health care use in the 12 months before starting the digital MSK program or the PT index event. Among back pain participants, members had significantly more orthopedic surgeon visits and PT visits versus PT patients. Significantly more members had E&M visits and imaging. Among knee pain participants, significantly more members had E&M visits. Among neck pain participants, significantly more members had nonsurgical invasive procedures versus PT patients. We detected no other statistically significant differences in MSK-related health care use at baseline between groups.
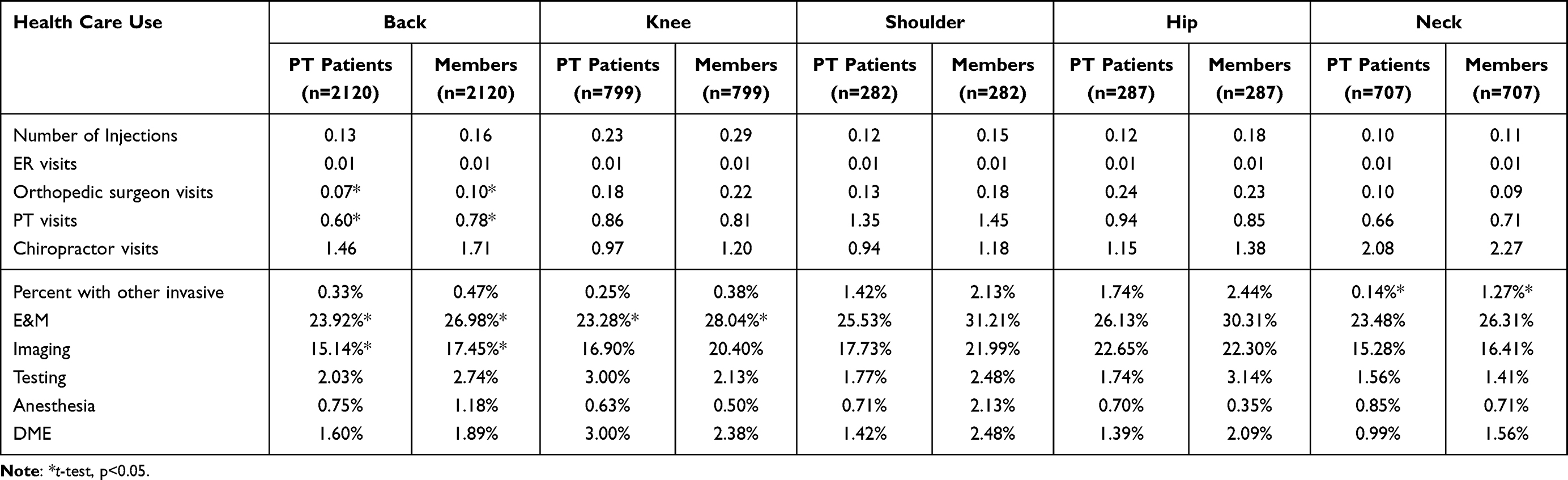 |
Table 3 Study Participant’s MSK Healthcare Use at Baseline, by Pain Region, After Matching |
The additional file reports standardized mean differences for these factors.
Table 4 shows descriptive results for members versus PT patients. For opioid initiation, 7.89% (95% Confidence Interval [CI]: 7.07%, 8.71%) of members had opioid prescriptions within 12 months of starting the digital MSK program versus 13.64% (95% CI: 12.60%, 14.67%) of matched PT patients (p < 0.001). Members had significantly fewer opioid prescriptions (16.73 per 100 participants; 95% CI: 14.11, 19.36) versus PT patients (22.36 per 100; 95% CI: 19.99, 24.73).
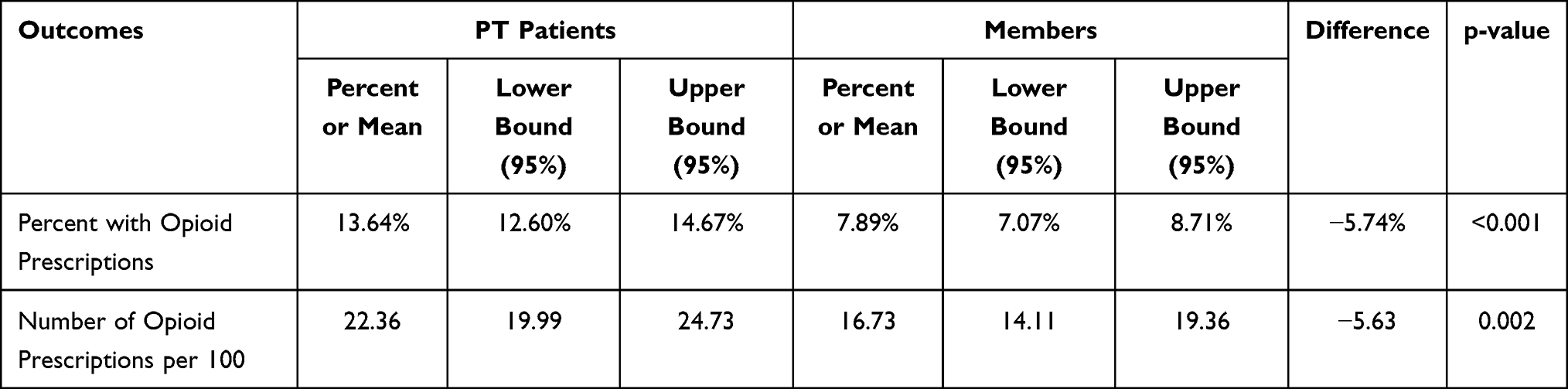 |
Table 4 Descriptive Results for Members versus PT Patients |
Main Findings
Table 5 shows results from unadjusted and adjusted regression models. Members had significantly lower odds (OR: 0.52, 95% CI: 0.45, 0.60) of initiating opioids within 12 months of starting the digital MSK program versus PT patients after controlling for available confounding variables. Members had significantly fewer prescriptions per 100 participants (beta: −6.40, 95% CI: −9.88, −2.93) in the post period versus PT patients after controlling for available confounding variables.
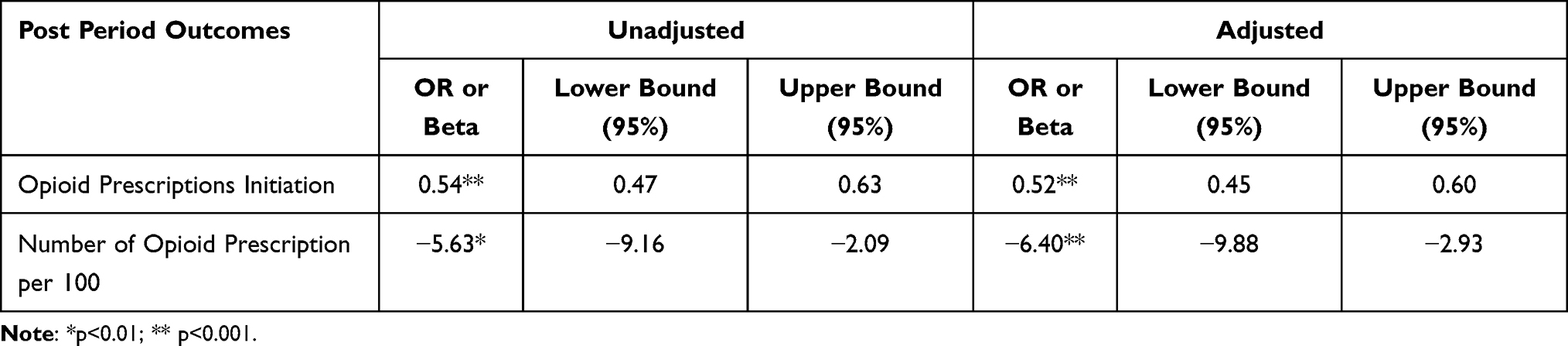 |
Table 5 Regression Model Results for Members versus PT Patients |
Discussion
This study shows the significant associations between digitally-delivered conservative care and decreased opioid initiation and prescribing. Among opioid naive participants with chronic MSK pain, significantly fewer digital MSK program members initiated opioids compared to PT patients during the 12 month follow-up period. In addition, members had significantly fewer prescriptions than PT patients after adjusting for confounders.
One possible reason for our findings is the effectiveness of conservative care on MSK pain and function. For example, a systematic review reported that exercise therapy has a larger effect on knee pain compared with NSAIDs, which have similar effects as opioids.30 Studies have also shown that conservative care delivered digitally improves clinical outcomes as well if not better than in-person care.21–25 Digital health utilization became especially pronounced during the spring and summer of 2020 when many people were unable to access in-person treatment for MSK pain due to the coronavirus pandemic. Therefore, digital MSK program members may have experienced improved pain and function, which may have prevented the need for new opioid prescriptions.
Study strengths are that the analysis includes a large sample size, and findings are generalizable to opioid naive adults with chronic MSK pain and employer-based medical and pharmacy coverage. To our knowledge, this is the first published study about a digital MSK program and opioid utilization.
The study had the following limitations. First, this is not a randomized controlled trial so we cannot establish causality of the digital MSK program’s effect on opioid initiation or prescriptions.
Second, our dataset is deidentified claims data that do not contain a number of variables that would greatly enhance the analysis. For example, the data do not include important confounding variables such as education and race/ethnicity, even though chronic MSK pain disproportionally affects underrepresented groups.31 The data do not include granular geographic indicators (eg, zip code, census tract), which prevented us from controlling for rurality or area deprivation. Furthermore, as a deidentified dataset, we are unable to link to our program’s engagement and clinical outcomes data. As a result, we do not account for baseline pain intensity or functional status, which are likely associated with opioid use. Our results may be overestimated if the digital MSK program included members with less pain or higher function.32 Without a data linkage, we are also unable to show in a single study that the digital MSK program improves pain and function, with subsequent decreases in opioid initiation and prescriptions.
Third, we cannot fully account for individual-level selection bias into the program. We do match members to PT patients drawn from the entire commercial health plan population rather than from just employers with the digital MSK program benefit to mitigate individual selection bias within the same employer. Finally, the PT patients had PT visit index events between January and October 2020 during COVID closures. It is unclear whether COVID restrictions had an effect on findings.
To address limitations, future research could include prospectively designed randomized controlled trials to further prove the efficacy of a digital MSK program on decreasing opioid use and amounts. Studies could also combine clinical outcomes and claims data to identify the range of factors associated with opioid use as well as the progression from improved clinical outcomes to changed medical care use.
Conclusions
An MSK program that delivers conservative care digitally may be a promising approach for decreasing opioid initiation among individuals with chronic MSK pain. The digital MSK program may effectively address pain, thereby preventing the need for opioids. By decreasing opioid initiation, the program may also help members avoid adverse events associated with opioid use.
Abbreviations
CDC, Centers for Disease Control and Prevention; CI, Confidence interval; DME, Durable medical equipment; ED, Emergency department; E&M, Evaluation and management; MSK, Musculoskeletal; PT, Physical therapy.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
Hinge Health contracts the independent entity WIRB-Copernicus Group® Institutional Review Board (OHRP/FDA IRB registration number IRB00000533) at WIRB-Copernicus Group® (1019 39th Avenue SE Suite 120, Puyallup, Washington 98374–2115) to conduct reviews. WIRB-Copernicus Group® Institutional Review Board reviewed this study, deemed it exempt, and waived informed consent.
WIRB-Copernicus Group® Institutional Review Board believes the study is exempt under 45 CFR § 46.104(d)(4), because information is recorded in such a manner that the identity of the human subjects cannot readily by ascertained directly or through identifiers linked to the subjects, the investigator does not contact the subjects, and the investigator will not re-identify subjects.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
Hinge Health, Inc., provided the digital MSK program to participants. Hinge Health, Inc. employees and manuscript authors GW and LL designed the study, interpreted results, and wrote the manuscript. Hinge Health, Inc. employees GW and LL analyzed data.
Disclosure
GW and LL are employed by and have equity interest in Hinge Health, Inc. LG and JB declare that they have no competing interests.
References
1. Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396(10258):1204–1222. doi:10.1016/S0140-6736(20)30925-9
2. Liu S, Wang B, Fan S, Wang Y, Zhan Y, Ye D. Global burden of musculoskeletal disorders and attributable factors in 204 countries and territories: a secondary analysis of the global burden of disease 2019 study. BMJ Open. 2022;12(6):e062183. doi:10.1136/bmjopen-2022-062183
3. McConaghy K, Klika AK, Apte SS, Erdemir A, Derwin K, Piuzzi NS. A call to action for musculoskeletal research funding: the growing economic and disease burden of musculoskeletal conditions in the United States is not reflected in musculoskeletal research funding. JBJS. 2023;105(6):492. doi:10.2106/JBJS.22.00693
4. Dieleman JL, Cao J, Chapin A, et al. US health care spending by payer and health condition, 1996–2016. JAMA. 2020;323(9):863–884. doi:10.1001/jama.2020.0734
5. Bichsel D, Liechti FD, Schlapbach JM, Wertli MM. Cross-sectional analysis of recommendations for the treatment of hip and knee osteoarthritis in clinical guidelines. Arch Phys Med Rehabil. 2022;103(3):559–569.e5. doi:10.1016/j.apmr.2021.07.801
6. Lin I, Wiles L, Waller R, et al. What does best practice care for musculoskeletal pain look like? Eleven consistent recommendations from high-quality clinical practice guidelines: systematic review. Br J Sports Med. 2020;54(2):79–86. doi:10.1136/bjsports-2018-099878
7. Bounds CL, Coppieters MW, Thomson HW, Larsen B, Evans K. Efficacy of conservative interventions for musculoskeletal conditions on pain and disability in active serving military personnel—a systematic review. Mil Med. 2023;usac409. doi:10.1093/milmed/usac409
8. Babatunde OO, Jordan JL, Van der Windt DA, Hill JC, Foster NE, Protheroe J. Effective treatment options for musculoskeletal pain in primary care: a systematic overview of current evidence. PLoS One. 2017;12(6):e0178621. doi:10.1371/journal.pone.0178621
9. Dowell D, Ragan KR, Jones CM, Baldwin GT, Chou R. CDC clinical practice guideline for prescribing opioids for pain — United States, 2022. MMWR Recomm Rep. 2022;71:1–95. doi:10.15585/mmwr.rr7103a1
10. Chou R, Hartung D, Turner J, et al. Opioid Treatments for Chronic Pain. Agency for Healthcare Research and Quality (US); 2020. Available from: http://www.ncbi.nlm.nih.gov/books/NBK556253/.
11. Centers for Disease Control and Prevention. Prescription opioid overdose death maps; 2022. Available from: https://www.cdc.gov/drugoverdose/deaths/prescription/maps.html.
12. Centers for Disease Control and Prevention. U.S. opioid dispensing rate maps; 2022. Available from: https://www.cdc.gov/drugoverdose/rxrate-maps/index.html.
13. Bandara S, Bicket MC, McGinty EE. Trends in opioid and non-opioid treatment for chronic non-cancer pain and cancer pain among privately insured adults in the United States, 2012–2019. PLoS One. 2022;17(8):e0272142. doi:10.1371/journal.pone.0272142
14. Feldman DE, Carlesso LC, Nahin RL. Management of patients with a musculoskeletal pain condition that is likely chronic: results from a national cross sectional survey. J Pain. 2020;21(7–8):869–880. doi:10.1016/j.jpain.2019.11.014
15. Groenewald CB, Murray CB, Battaglia M, Scaini S, Quinn PD. Prevalence of pain management techniques among adults with chronic pain in the United States, 2019. JAMA Netw Open. 2022;5(2):e2146697. doi:10.1001/jamanetworkopen.2021.46697
16. Mathieson S, Wertheimer G, Maher C, et al. What proportion of patients with chronic noncancer pain are prescribed an opioid medicine? Systematic review and meta-regression of observational studies. J Intern Med. 2020;287(5):458–474. doi:10.1111/joim.13026
17. Brown-Taylor L, Beckner A, Scaff KE, et al. Relationships between physical therapy intervention and opioid use: a scoping review. PM R. 2022;14(7):837–854. doi:10.1002/pmrj.12654
18. Thorlund JB, Roos EM, Goro P, Ljungcrantz EG, Grønne DT, Skou ST. Patients use fewer analgesics following supervised exercise therapy and patient education: an observational study of 16 499 patients with knee or hip osteoarthritis. Br J Sports Med. 2021;55(12):670–675. doi:10.1136/bjsports-2019-101265
19. Frogner BK, Harwood K, Andrilla CHA, Schwartz M, Pines JM. Physical therapy as the first point of care to treat low back pain: an instrumental variables approach to estimate impact on opioid prescription, health care utilization, and costs. Health Serv Res. 2018;53(6):4629–4646. doi:10.1111/1475-6773.12984
20. Thackeray A, Hess R, Dorius J, Brodke D, Fritz J. Relationship of opioid prescriptions to physical therapy referral and participation for Medicaid patients with new-onset low back pain. J Am Board Fam Med JABFM. 2017;30(6):784–794. doi:10.3122/jabfm.2017.06.170064
21. Xie SH, Wang Q, Wang LQ, Wang L, Song KP, He CQ. Effect of internet-based rehabilitation programs on improvement of pain and physical function in patients with knee osteoarthritis: systematic review and meta-analysis of randomized controlled trials. J Med Internet Res. 2021;23(1):e21542. doi:10.2196/21542
22. Du S, Liu W, Cai S, Hu Y, Dong J. The efficacy of e-health in the self-management of chronic low back pain: a meta analysis. Int J Nurs Stud. 2020;106:103507. doi:10.1016/j.ijnurstu.2019.103507
23. Seron P, Oliveros MJ, Gutierrez-Arias R, et al. Effectiveness of telerehabilitation in physical therapy: a rapid overview. Phys Ther. 2021;101(6):zab053. doi:10.1093/ptj/pzab053
24. Suso-Martí L, La Touche R, Herranz-Gómez A, Angulo-Díaz-Parreño S, Paris-Alemany A, Cuenca-Martínez F. Effectiveness of telerehabilitation in physical therapist practice: an umbrella and mapping review with meta–meta-analysis. Phys Ther. 2021;101:zab075. doi:10.1093/ptj/pzab075
25. Gava V, Ribeiro LP, Barreto RPG, Camargo PR. Effectiveness of physical therapy given by telerehabilitation on pain and disability of individuals with shoulder pain: a systematic review. Clin Rehabil. 2022;02692155221083496. doi:10.1177/02692155221083496
26. Wang G, Yang M, Hong M, Krauss J, Bailey JF. Clinical outcomes one year after a digital musculoskeletal (MSK) program: an observational, longitudinal study with nonparticipant comparison group. BMC Musculoskelet Disord. 2022;23:237. doi:10.1186/s12891-022-05188-x
27. Mecklenburg G, Smittenaar P, Erhart-Hledik JC, Perez DA, Hunter S. Effects of a 12-week digital care program for chronic knee pain on pain, mobility, and surgery risk: randomized controlled trial. J Med Internet Res. 2018;20(4):e156. doi:10.2196/jmir.9667
28. Shebib R, Bailey JF, Smittenaar P, Perez DA, Mecklenburg G, Hunter S. Randomized controlled trial of a 12-week digital care program in improving low back pain. Npj Digit Med. 2019;2(1):1–8. doi:10.1038/s41746-018-0076-7
29. Bailey JF, Agarwal V, Zheng P, et al. Digital care for chronic musculoskeletal pain: 10,000 participant longitudinal cohort study. J Med Internet Res. 2020;22(5):e18250. doi:10.2196/18250
30. Thorlund JB, Simic M, Pihl K, et al. Similar effects of exercise therapy, nonsteroidal anti-inflammatory drugs, and opioids for knee osteoarthritis pain: a systematic review with network meta-analysis. J Orthop Sports Phys Ther. 2022;52(4):207–216. doi:10.2519/jospt.2022.10490
31. Patel M, Johnson AJ, Booker SQ, et al. Applying the NIA health disparities research framework to identify needs and opportunities in chronic musculoskeletal pain research. J Pain. 2022;23(1):25–44. doi:10.1016/j.jpain.2021.06.015
32. Lentz TA, Beneciuk JM, George SZ. Prediction of healthcare utilization following an episode of physical therapy for musculoskeletal pain. BMC Health Serv Res. 2018;18(1):648. doi:10.1186/s12913-018-3470-6
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.