Back to Journals » Advances in Medical Education and Practice » Volume 11
Online Synchronous Clinical Communication Training During the Covid-19 Pandemic
Authors Junod Perron N, Dominicé Dao M ![]() , Rieder A, Sommer J, Audétat MC
, Rieder A, Sommer J, Audétat MC ![]()
Received 13 October 2020
Accepted for publication 21 November 2020
Published 24 December 2020 Volume 2020:11 Pages 1029—1036
DOI https://doi.org/10.2147/AMEP.S286552
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Noelle Junod Perron, 1 Melissa Dominicé Dao, 2 Arabelle Rieder, 3 Johanna Sommer, 3 Marie-Claude Audétat 1, 3
1Unit of Development and Research in Medical Education, Geneva Faculty of Medicine and Institute of Primary Care, Geneva University Hospitals, Geneva, Switzerland; 2Department of Primary Care, Geneva University Hospitals, Geneva, Switzerland; 3Unit of Primary Care, Geneva Faculty of Medicine, Geneva, Switzerland
Correspondence: Noelle Junod Perron
Unit of Development and Research in Medical Education, Faculty of Medicine, Geneva University and Institute of Primary Care, Geneva University Hospitals, Geneva, Switzerland
Tel +41 22 372 96 76
Email [email protected]
Purpose: As the COVID-19 pandemic outbreak occurred, most structured clinical communication training were transformed from in-person to remote seminars. The aim of our study was to evaluate the usefulness and feasibility of online synchronous clinical communication training from both students’ and tutors’ perspectives.
Patients and Methods: We conducted a cross-sectional study. Geneva Faculty of Medicine’ 3rd year medical students and tutors involved in clinical communication were asked to respond to an online survey.
Results: Eighty-five of 149 students and 15/16 tutors responded. Students highly valued both online seminars and reported little technical difficulty. They felt that tutors were well prepared and actively involved them in experiential learning. Tutors globally reported little technical difficulty and felt rather well prepared to do so online. Although both students and tutors preferred the in-person format, half of them could still consider using an online format in the future outside the pandemic but mentioned it required specific rules.
Conclusion: Our results suggest that clinical communication can be taught and practiced online and that tutors can quickly adapt to such changes.
Keywords: clinical communication, online, synchronous, training, teaching
A Letter to the Editor has been published for this article.
Introduction
Traditionally, structured clinical communication training activities in undergraduate education include in-person small group discussions, video observations, and role plays (with or without simulated patients).1 In the workplace setting, optimal methods of teaching and learning communication skills are direct observations of the student’s performance or videotaped clinical interaction, followed by feedback from an experienced tutor and role modeling preceded by observation tasks.2
Online learning, often called internet-based learning, has increased in medical education. It encompasses a wide variety of technological forms such as simulation, digital teaching aid, online teaching, serious games, massive open online courses, and augmented reality (virtual reality/patients and/or learning environments), hosted or not by learning management systems.3,4 The advantages of online learning are irrelevance of physical distance, cost savings once online tutorials have been developed, flexibility in time of participation, and individualizing learning through self-adjustment or automated adaptation.5 Disadvantages include costs related to the development of online learning, technical difficulties, and sense of isolation.5 A systematic review showed that online learning works as well as offline learning, but the conditions under which it can be used must be further clarified.6 Blended learning, the combination of both online and offline teaching methods, is presented as the best option in medical education.5
Regarding clinical skills, online education is considered to offer an attractive alternative because it is self-directed, flexible, and offers opportunities to simulate and rehearse different clinical situations.7 Online teaching of communication skills usually supplements learning in the workplace and is often part of blended learning programs in the context of continuous professional education.7,8 The online part of the courses usually emphasizes theoretical knowledge, video, and exercises/quizzes. It is recognized as an effective way to enhance and individualize self-directed learning while in-person learning aligns with collaborative and socialization goals. However, its impact on patient outcomes has not been well assessed,8 and further research is still needed to identify what makes virtual teaching of communication skills effective.7
As the COVID pandemic outbreak occurred, most medical schools were not equipped with effective online digital education regarding clinical communication training. Training activities were either suppressed or quickly converted from in-person to remote learning activities such as remote formative OSCEs or remote seminars via a videoconference platform. The challenge was to effectively teach and practice communication skills during synchronous online seminars and train available tutors to use new IT tools in a very short timeframe. Little is known about how such changes occurred and what lessons can be learned from such a shift in teaching practices.9,10
As in many countries, our medical school closed its doors mid-March 2020. Forty-eight hours later, all tutors involved in clinical communication small group training attended an online training session on how to effectively use a videoconference platform, to facilitate interactive seminars using virtual white board, videos, role play, and rooms for small group discussions. We relied on the online manual instruction developed by the University IT pedagogical team.11 The following week, all clinical communication seminars were converted from in-person to remote seminars, which took place during the following 4 weeks, with 3rd year medical students in groups of 8–14 students. These seminars included small group discussions, observation of videos, and role plays with the tutor (playing the role of a patient or a supervisor).
The aim of the study was to explore students’ and tutors’ perceptions regarding the feasibility, usefulness, and advantages/disadvantages of online synchronous clinical communication training activities.
Participants and Methods
Setting
We conducted a cross-sectional study at the Geneva Faculty of Medicine, Switzerland. We invited all 3rd year students and tutors involved in one or both of two clinical communication skills training/teaching sessions during March and April 2020 to respond to an online survey on the usefulness, feasibility, and advantages/disadvantages of online CS training seminars. Sixty-one of 117 students attended seminar 1 (S1 “how to prescribe a medication” in order to optimize patient compliance) and 100/149 students attended seminar 2 (S2 “how to present a clinical case”). The difference in the total number of students expected to attend S1 and S2 is explained by the fact the the Geneva Faculty of medicine allows medical students to unregister from one unit out of six during their 3rd year. Several students grasped this opportunity during the 4th unit, during which S1 is given, while S2 is given during the fifth unit. The low rate of attendance is explained under the result section. All 16 tutors answered the call to teach these seminars. These two seminars end the structured experiential communication skills training (8x2 hour seminars and five formative OSCEs) given during years 2 and 3. Table 1 describes the chronological sequences of both seminars.
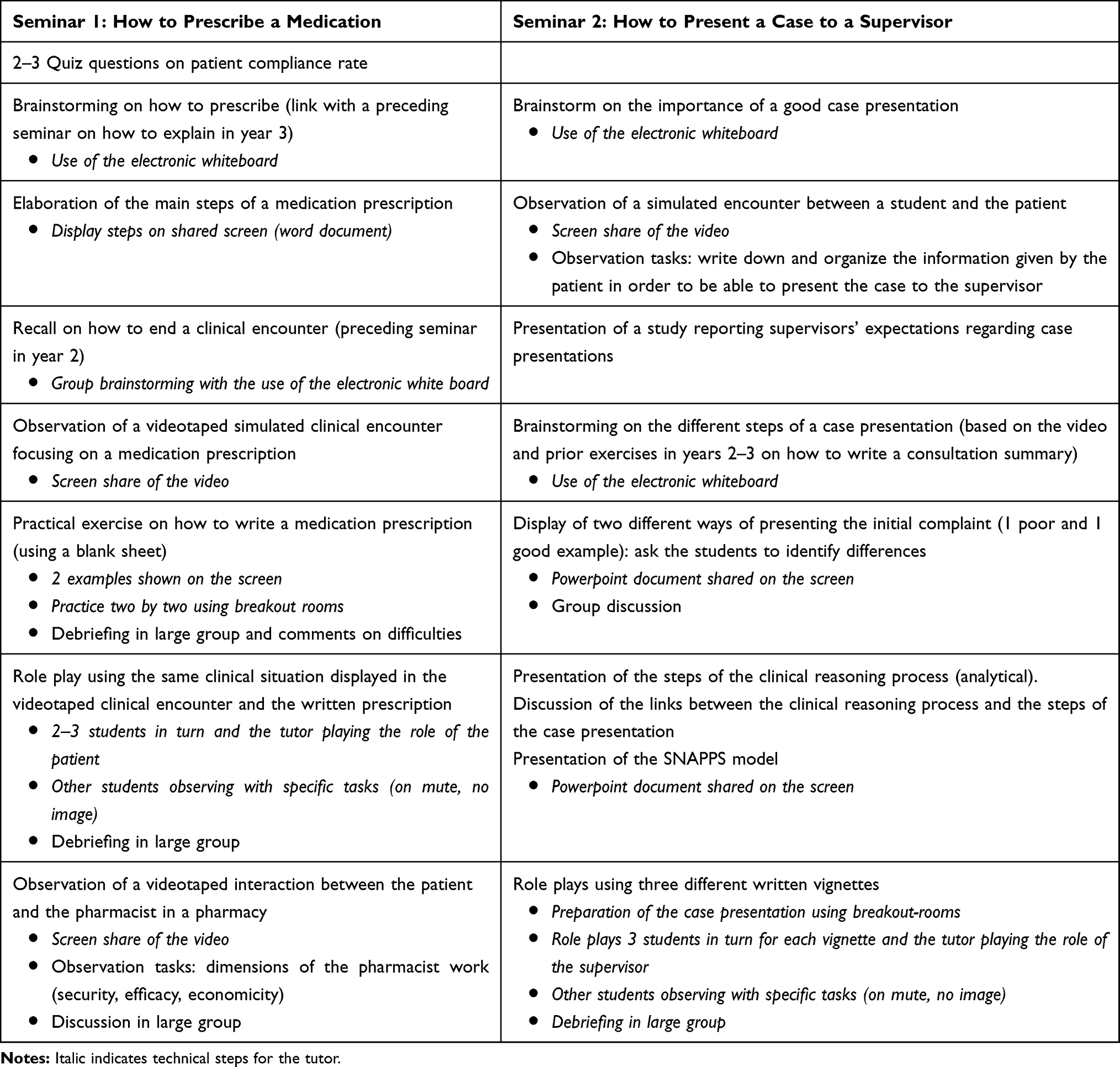 |
Table 1 Short Description of the Different Phases of the Seminars |
Questionnaire
We developed a 15-item online questionnaire using Qualtrics software.12 It was based on questionnaires used in our Faculty of medicine to evaluate participants’ satisfaction regarding experiential training activities, as well as dimensions we wanted to specifically explore (feasibility, technical difficulty, advantages/disadvantages of online vs in presence experiential teaching/training) since the literature is scarce on online synchronous experiential learning. This questionnaire was however not formally validated. Because of time constraints, we did not conduct any pilot testing of the survey. Students’ and tutors’ perspectives were explored using a Likert scale (1–5, 1=totally disagree to 5=totally agree) and three open-ended questions. The link to the online questionnaire was sent by email to all 3rd year medical students (n=149) and involved tutors (n=16) on April 25, 2020 and two reminders were sent 1 and 2 weeks later.
The study was granted a waiver from approval by the Ethical Committee of Geneva since it did not fall under the scope of the Swiss Evaluation of Human Research Act (no patients included).13 However, in the introduction of the survey, participants were informed about the goals of the study and that by answering the survey, they gave their consent to publish anonymized responses.
Analysis
SPSS software version was used for the analysis. Participants’ responses were analyzed descriptively using percentages, median, interquartile range, means and standard deviations. Responses to open-ended questions (advantages, disadvantages, suggestions) were analyzed thematically by four investigators. They first read all the written comments and identified themes that were compared and discussed. Once a consensus was achieved, themes were combined into main categories (Table 4).14
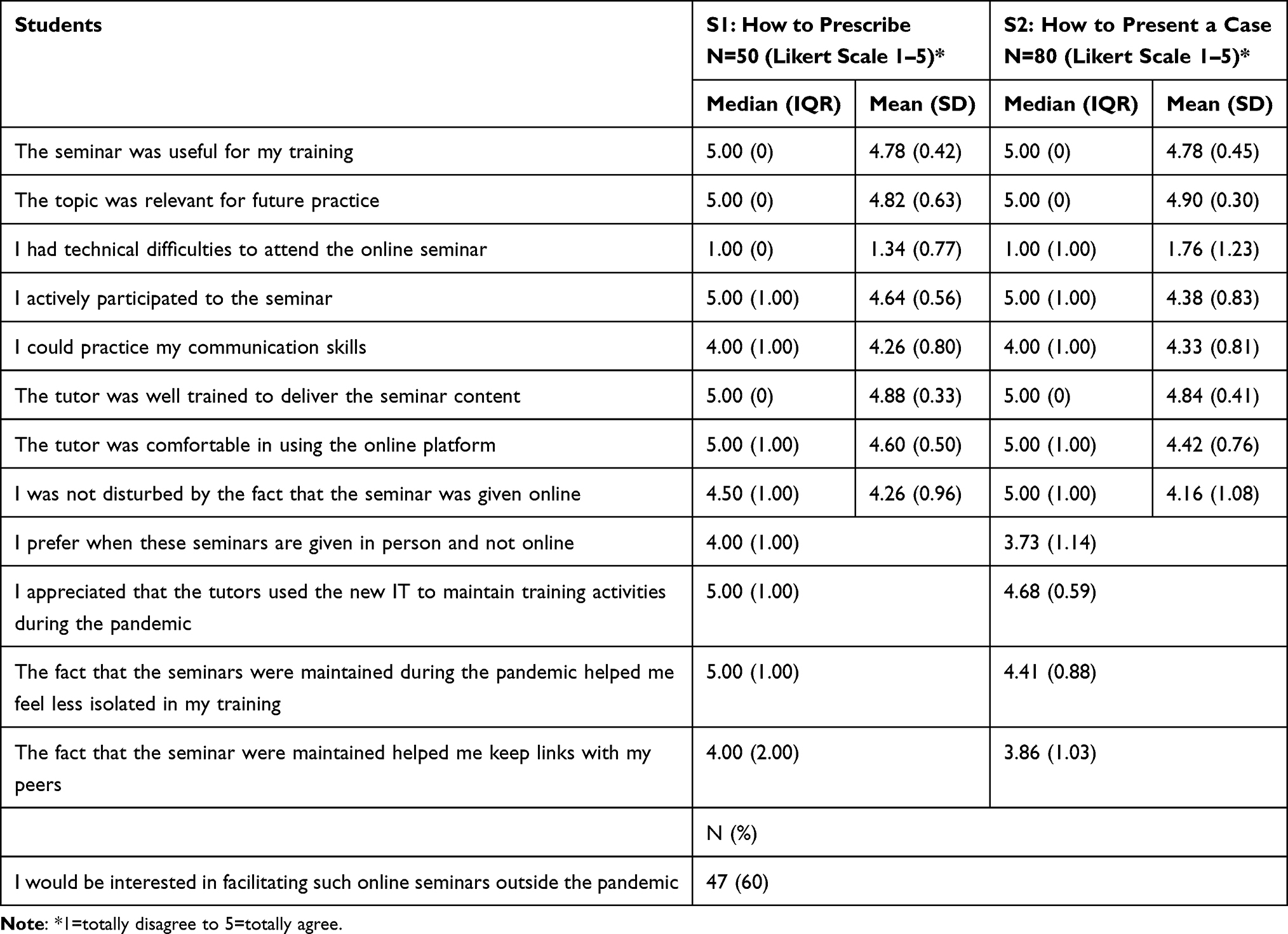 |
Table 2 Students’ Perceptions Regarding Online Synchronous Clinical Communication Training |
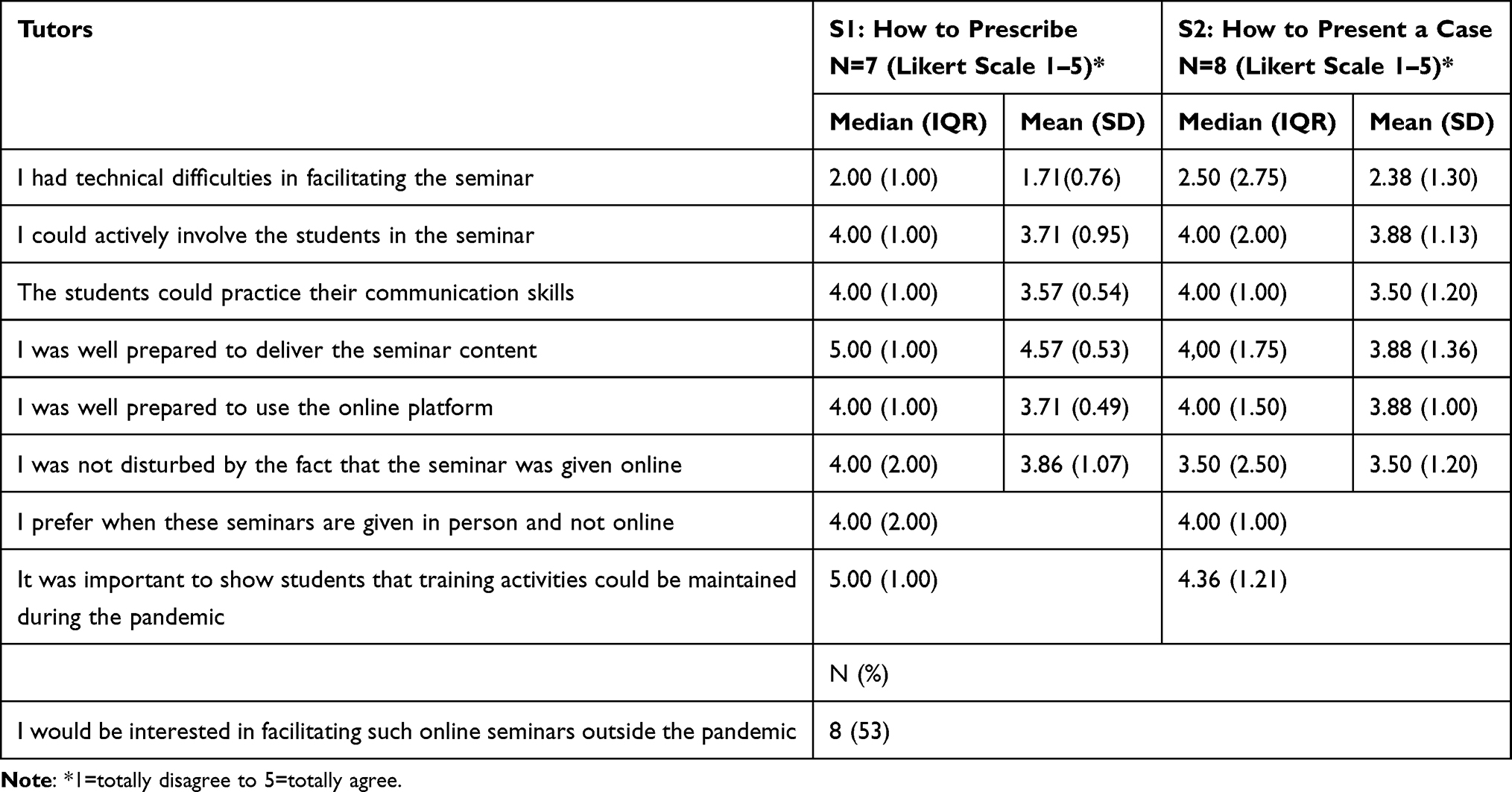 |
Table 3 Tutors’ Perceptions Regarding Online Synchronous Clinical Communication Training |
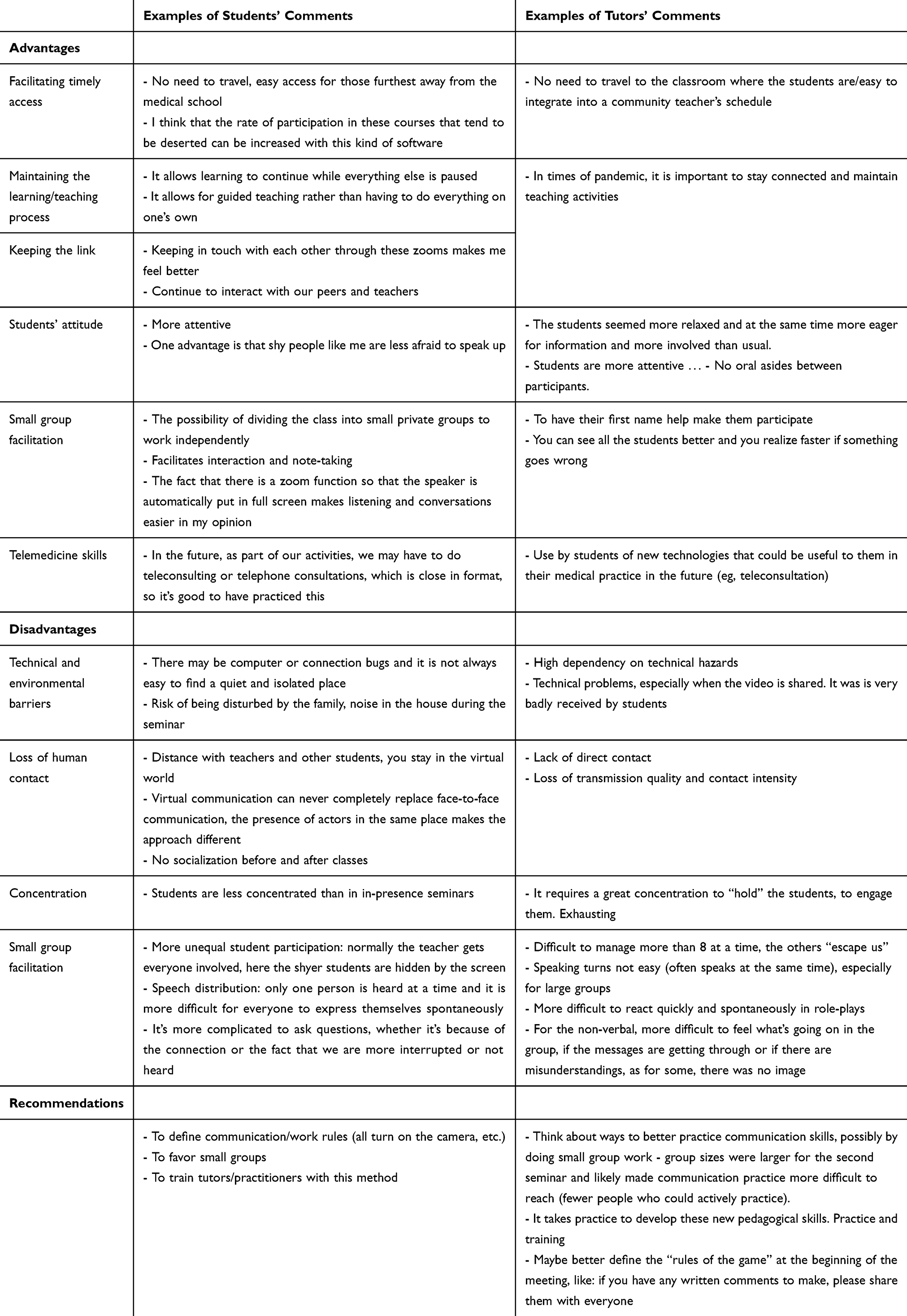 |
Table 4 Students’ and Tutors’ Comments Regarding Advantages, Disadvantages, and Suggestions Regarding Online Synchronous Clinical Communication Training/Teaching |
Results
Eighty-five students (50 attended S1 and 80 attended S2: 49 attended both) and 15/16 tutors (five facilitated both) responded. The main reasons reported by students for not attending the seminars were overseeing the email invitation or being involved as volunteers in the COVID crisis management.
Table 2 shows that students highly valued both online seminars in terms of usefulness and relevance to their practice and did not make a distinction between patient communication (S1) and professional communication (S2). They reported little technical difficulty. They felt that tutors were well trained, comfortable while using the online platform (median 5 (IQR=0 and 1)), and actively involved them in experiential learning (median=4–5 (IQR=1)). They highly valued the fact that these training activities were maintained during the pandemic (median=5 (IQR=1)). Tutors globally reported little technical difficulty in facilitating the seminar and felt rather well prepared to do so online (median=4 (IQR=1) for S1 and median=4 (IQR=1.5) for S2) (Table 3). However, their self-perceptions were less positive than students’ perceptions regarding tutors’ degree of comfort and preparedness. Although both students and tutors preferred the in-person format, half of them could still consider using such an online format in the future outside the pandemic (60% and 53%).
Analysis of participants’ answers to open-ended questions indicated that students particularly enjoyed keeping contact with peers and tutors when most learning activities were cancelled. In this context, online seminars also boosted their motivation to learn and decreased their sense of isolation. Several tutors felt that the students were more engaged, motivated, and attentive, and that it helped them and the students to be more focused than during in-person seminars. Students valued the interactive techniques used by tutors such as the electronic white board and the breakout rooms. Both tutors and students valued not needing to travel. For tutors, this new format mirrored the needed skills for telemedicine, while students considered on-line role play to be a first experience for their future practice in telemedicine. Some students felt less inhibited during on-line seminars, while others considered that shy students tended to hide behind the screen. Disadvantages included loss of social and human contact with both peers and tutors. Communication was perceived as less natural and spontaneous than in in presence seminars. Tutors found it difficult to perceive and react to students’ non-verbal cues. Technical problems such as connection disturbances were reported by both tutors and students, while students mentioned the difficulty to remain concentrating during online seminars in a sometimes noisy home environment (Table 3). Suggestions included limiting the group size (6–7), use of rules for speaking, compulsory activation of the camera option on the internet platform in order to stimulate interactivity with all students, and prior planning of group subdivision in breakout rooms. Both tutors and students supported further tutors’ training in facilitation of online experiential sessions.
Discussion
The results of the survey show several interesting findings: online synchronous clinical communication training allows active involvement if tutors and students respect a set of specific rules. The practice of communication skills is feasible and acceptable online.
Synchronous communication through videoconferencing has been shown to positively influence group discussion and participation for supervision at a distance.15 Since the pandemic outbreak, several organisations have made accessible several practical guides on how to address the challenges and potential adaptations for online communication skills teaching.16,17 This may further enrich teachers’ repertoires on how to stimulate interactivity at a distance. Use of online role plays offers an interesting way to expose students to telemedicine and tele-supervision which are rarely addressed during undergraduate training.18
Tutors quickly adapted to such changes, although they reported facing more technical difficulties than students in using new IT tools. This may be related to tutors having to perform substantially more handling of technical aspects (sharing a video, use of whiteboard, etc.) than students. Negative attitude in engaging with new technologies and tools has often been reported as a barrier to the development and implementation of online learning.19 As experienced and described by several authors, the COVID-19 pandemic seems to have acted as a catalyzer to develop innovative online teaching activities and enhance teachers’ digital literacy.20,21
Maintaining learning activities during the COVID-19 pandemic contributed to an increased sense of belonging to a community of learners/teachers. Integration into a learning and teaching community of practice is important for both the learning process and the development of medical students’ professional identity.22 Role modeling is important to instill professional values, attitudes, and behaviors. Tutors’ quick adaptation to IT tools and keeping in touch with students may have exemplified the challenges faced, the skills needed, and the attitude expected from clinical teachers to ensure learner centeredness in changing conditions.
There are several limitations. First, the fact that the survey took place in one university and included only 3rd year medical students limits the generalizability of our results. We collected only perceptions and did not assess the effectiveness of the online training on higher levels of educational impact according to the Kirkpatrick Model of Training Evaluation.23 The context of the pandemic might have positively influenced the students’ perceptions, since most other courses were cancelled due to lack of tutors’ availability.
Conclusion
Based on these results, we conclude that clinical communication can be taught and practiced online and that tutors can quickly adapt to such changes. Although this format may model synchronous telemedicine skills, it does not replace in-person learning. It requires specific rules and conditions to stimulate interactivity.
Acknowledgments
We thank the Faculty of Geneva IT team who provided written and audio-visual support to transform in-person to remote teaching activities. We also thank all students and tutors who answered the survey.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kurtz S, Silverman J, Draper J. Teaching and Learning Communication Skills in Medicine.
2. Rosenbaum ME. Dis-integration of communication in healthcare education: workplace learning challenges and opportunities. Patient Educ Couns. 2017;100(11):2054–2061. doi:10.1016/j.pec.2017.05.035
3. George PP, Papachristou N, Belisario JM, et al. Online eLearning for undergraduates in health professions: A systematic review of the impact on knowledge, skills, attitudes and satisfaction. J Glob Health. 2014;4(1):010406. doi:10.7189/jogh.04.010406
4. Moule P, Ward R, Lockyer L. Nursing and healthcare students’ experiences and use of e-learning in higher education. J Adv Nurs. 2010;66(12):2785–2795. doi:10.1111/j.1365-2648.2010.05453.x
5. Cook D. Faculty Development Online. In: Steinert Y, editor. Faculty Development in the Health Professions: A Focus on Research and Practice, Innovation and Change in Professional Education. Dordrecht: Springer Science +Business Media; 2014:217–241.
6. Pei L, Wu H. Does online learning work better than offline learning in undergraduate medical education? A systematic review and meta-analysis. Med Educ Online. 2019;24(1):1666538. doi:10.1080/10872981.2019.1666538
7. Kyaw BM, Posadzki P, Paddock S, Car J, Campbell J, Tudor Car L. Effectiveness of digital education on communication skills among medical students: systematic review and meta-analysis by the digital health education collaboration. J Med Internet Res. 2019;21(8):e12967. doi:10.2196/12967
8. Cappi V, Artioli G, Ninfa E, et al. The use of blended learning to improve health professionals’ communication skills: a literature review. Acta Bio-Medica. 2019;90(4–S):17–24.
9. Salgado H, Castro-Vale I. Clinical communication skills training in dental medical education: the covid-19 pandemic challenge. Healthcare. 2020;8:4. doi:10.3390/healthcare8040429
10. Newcomb AB, Duval M, Bachman SL, Mohess D, Dort J, Kapadia MR. Building rapport and earning the surgical patient’s trust in the era of social distancing: teaching patient-centered communication during video conference encounters to medical students. J Surg Educ. 2020. doi:10.1016/j.jsurg.2020.06.018
11. University of Geneva. Available from: https://www.unige.ch/enseignement-a-distance/maitriser-outils/zoom/).
12. Qualtrics. Available from: https://www.qualtrics.com/about/).
13. Health TFOoP. Human research act. Available from: https://www.bag.admin.ch/bag/en/home/medizin-und-forschung/forschung-am-menschen/evaluation-humanforschungsgesetz.html.
14. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
15. Könings KD, Popa D, Gerken M, et al. Improving supervision for students at a distance: videoconferencing for group meetings. Innovations Education Teaching International. 2015;53(4):388–399. doi:10.1080/14703297.2015.1004098
16. International Association for Medical Education (AMEE). Available from: https://amee.org/covid-19.
17. International Association for Communication in Healthcare (EACH). Available from: https://www.each.eu/resources/covid-19.
18. Cantone RE, Palmer R, Dodson LG, Biagioli FE. Insomnia Telemedicine OSCE (TeleOSCE): A simulated standardized patient video-visit case for clerkship students. MedEdPORTAL. 2019;15:10867. doi:10.15766/mep_2374-8265.10867
19. O’Doherty D, Dromey M, Lougheed J, Hannigan A, Last J, McGrath D. Barriers and solutions to online learning in medical education - an integrative review. BMC Med Educ. 2018;18(1):130. doi:10.1186/s12909-018-1240-0
20. An international association for medical education. Covid-19; 2020. Available from: https://amee.org/covid-10#publications.
21. Roskvist R, Eggleton K, Goodyear-Smith F. Provision of e-learning programmes to replace undergraduate medical students’ clinical general practice attachments during COVID-19 stand-down. Education Primary Care. 2020;1–8.
22. Wenger E. Communities of Practice: Learning, Meaning and Identity. Cambridge University Press: Cambridge, UK; 1998.
23. Kirkpatrick D. Great ideas revisited: techniques for evaluating training programs. Train Dev. 1996;50:54–59.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.