Back to Journals » International Journal of General Medicine » Volume 16
Objective Neurological Testing Methods Used to Follow Up Vestibular Neuritis Depending on Different Factors
Authors Li Z ![]() , Miao L
, Miao L ![]() , Zhang T
, Zhang T ![]() , Li X
, Li X
Received 29 August 2023
Accepted for publication 20 October 2023
Published 1 November 2023 Volume 2023:16 Pages 4991—5002
DOI https://doi.org/10.2147/IJGM.S436206
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Zidong Li,1 Lu Miao,1 Tianyi Zhang,2 Xinyi Li1
1Third Hospital of Shanxi Medical University, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Taiyuan, 030032, People’s Republic of China; 2School of Basic Medical Sciences, Shandong University, Jinan, 250000, People’s Republic of China
Correspondence: Xinyi Li, Email [email protected]
Purpose: We analyze the impact of different factors on clinical performance and prognosis in vestibular neuritis (VN) and explore indicators that could accurately reflect changes in patients’ symptoms at different stages.
Methods: We observed patients with VN during the acute and recovery phases. Clinical symptoms, vertigo-related scales, neurological examination, vestibular function tests (caloric test, video head impulse test (vHIT), vestibular evoked myogenic potential (VEMP)), and the history of disease (underlying diseases, glucocorticoid therapy) were recorded at onset and at 4 and 12 weeks after onset in VN patients. Multiple linear regression analysis was used to identify vestibular function tests that had a linear regression relationship with the subjective quantitative results.
Results: At 4 weeks after onset, the group without underlying disease had better improvement in EEV, gain, and UW than the group with underlying disease (P < 0.05). There was a significant difference in the change in DHI, EEV, gain of the affected horizontal semicircular canal in the vHIT and unilateral weakness (UW) between the glucocorticoid treatment group and the no glucocorticoid treatment group (P < 0.05), and glucocorticoid treatment group was better. The change value in the gain of horizontal canals in the vHIT was mainly positively and linearly correlated with the EEV scores (P< 0.001). Possible dynamic correlation between vHIT results and vestibular symptoms.
Conclusion: The absence of underlying disease and the receipt of glucocorticoid therapy significantly contributed to the improvement of objective vestibular function tests in the short term, while the improvement of subjective vertigo may correlate with the different objective measures and questionnaire. We believe that the improvement of the affected horizontal semicircular canal gain value in the vHIT can be used as a reference indicator of the degree of improvement of vestibular symptoms with superior vestibular neuritis.
Keywords: vestibular neuritis, video head impulse test, vertigo symptoms, caloric test, Dizziness Handicap Inventory and European Evaluation of Vertigo Scale
Introduction
Vestibular neuritis (VN) is a representative disease of acute peripheral vertigo syndrome. The latest consensus document of the Bárány Society Committee on Classification of Vestibular Disorders has included acute unilateral vestibular disease (AUVP) as a synonym for VN and recommended its use. The clinical characteristics mainly include acute onset. Some patients may have a history of preinfection 1–2 weeks before the vertigo attack, accompanied by nausea, vomiting, vibratory hallucinations and a sense of tipping to one side, and vertigo symptoms often last from a few hours to a few days. The main clinical sign of VN is a spontaneous peripheral vestibular nystagmus with a relatively constant direction, enhanced by the removal of fixation, whose trajectory corresponds to the semicircular afferents on the involved pathway (usually horizontal with torsion).1
Ongoing dizziness, nystagmus, nausea/vomiting, head motion intolerance or poor balance, collectively termed acute vestibular syndrome (AVS).2 This includes both central nervous and peripheral vestibular disorders, such as posterior circulation strokes and vestibular neuritis. There is a very strong advantage of HINTS (normal/clinical horizontal head impulse, gaze-direction nystagmus or skew deviation) as a means of differentiating between posterior circulation stroke and peripheral vestibular disease, especially in emergency patients who are in the negative imaging window phase and have atypical symptoms.3,4 Recently, with the in-depth study of caloric test, VEMPs, and vHIT in multiple vestibular dysfunction disorders, the treatment of patients with VN has gradually become systematic and comprehensive. vHIT and caloric test are both tests to evaluate the vestibulo-ocular reflex (VOR), but no correlation was found between them. This is because they assess the VOR at different frequencies (vHIT:2–5Hz; caloric test:0.003Hz), and there may be a complementary relationship between them.5 Current studies have shown that vHIT is significantly better than the traditional clinical head impulse test (cHIT) combined with the torsional deflection test, which can effectively reduce the misdiagnosis rate of peripheral vertigo disease and avoid delaying the diagnosis and treatment of diseases such as stroke.6 Several papers have also suggested that caloric test is an effective complementary test to a normal vHIT result when considering someone with VN and other vestibular diseases, also considering their different sensitivity and specificity values.5,7,8 VEMP is also very valuable for VN, especially to distinguish superior vestibular neuritis/inferior vestibular neuritis, or combined damage. Superior vestibular nerve damage is more common, but studies of recovery period is not sufficient.9–11 However, there are few studies on the dynamic changes of the above mentioned tests during the recovery period of VNs. In particular, there is a lack of clear conclusions about the relationship between these vestibular function tests and clinical subjective vertigo symptoms during the course of VN.
In addition to common symptomatic treatments such as rest, antiemesis and fluid rehydration, the most common and effective treatments for VN patients include glucocorticoid therapy and vestibular rehabilitation exercise. Early studies considered that VN patients were infected with some kind of virus caused and linked to secondary immune response, but antiviral treatment did not benefit patients, while short-term glucocorticoid therapy may effectively improve the nerve with swelling, entrapment and other conditions (similar to acute idiopathic peripheral facial palsy) to improve the symptoms of patients.12–14 Since then, there has been much debate about the effectiveness of glucocorticoid therapy, including long-term benefits, short-term recovery in symptoms, and improvement in auxiliary test results.15–17
Therefore, we aimed to determine the dynamic effects of different factors on subjective vertigo symptoms and objective ancillary (vHIT, caloric test, and VEMP) findings in VN patients and to clarify the correlation between the results of quantity measures of symptomatology and indices of vestibular function tests.
Materials and Methods
Patients
The study was approved by the ethics committee of Shanxi Bethune Hospital of Shanxi Medical University. Patients with VN diagnosed and admitted to the Department of Neurology of the Third Affiliated Hospital of Shanxi Medical University from January 2021 to November 2022 were enrolled. Inclusion and exclusion criteria: 1. meeting the diagnostic criteria of vestibular neuritis:18 1) acute or subacute onset of spontaneous vertigo lasting at least 24 hr or with nausea or vomiting; 2) spontaneous nystagmus (SPN), horizontal or horizontal with torsion, toward the healthy side; 3) new onset of gait or postural imbalance; 4) exclusion of hearing impairment (Pure tone audiometric testing); 5) absence of signs and symptoms of neurological deficit; 6) normal (eg, age-related changes) or nonspecific abnormalities on magnetic resonance imaging (MRI) and diffusion-weighted imaging (within 1–10 days of onset); and 7) at least 1 week of follow-up. The final diagnosis was determined by two or more neurologists with 5 years of experience in practice. Treatment must be initiated within 7 days of symptom onset. Voluntarily cooperate with all questionnaires, physical examinations, including HINTS test, vestibular function tests, and MRI examinations. Written informed consent was obtained from the patient or family.
Assessment of Vertigo-Related Scales
The Chinese version of the Dizziness Handicap Inventory (DHI) is a very widely validated and used symptom-based assessment scale.19 It provides a global assessment of the patient’s subjective vertigo symptoms and the decrease in quality of life due to vertigo.20
The European Evaluation of Vertigo scale (EEV), in Chinese, is a physician-administered scale that assesses only the symptoms caused by vestibular dysfunction in five aspects: motor illusion, duration of illusion, motor intolerance, neurovegetative signs, and instability.21
Vestibular Function Tests
Caloric test: Videonystagmography and binaural air caloric tests (cold and hot water vapors) of the Vestibular Examination Unit (VO425, Denmark) were used to measure the maximum slow-phase velocity (SPV) on the horizontal or vertical vectors of the SPN. The recorded nystagmus time was no less than 30s, and the recording frequency was 174 frames. The system was calibrated before each examination. The unilateral weakness (UW) was calculated according to the Jongkees22 formula. Grade: UW 50% was severely abnormal, UW from 25% to 50% was intermediate abnormal, and UW < 25% was normal. SPV normal range:12–140°/s, Cold stimulation:5–30°/s, hot stimulation:20–140°/s. The caloric test can only examine the functioning of the horizontal canals and superior parts of the vestibular nerve. If only inferior neuritis is abnormal, the caloric testing will present normal results.
vHIT: The vestibular examination unit (EyeSeeCam, Denmark) was used for testing. The patient wore the eyepiece and sat with the head tilted forward 30°. The person being examined is required to stare at 1.5 m ahead as a target, and give the passive, fast, low, random direction (cannot be predicted) impulse movement 20 times (dynamic angular acceleration test head 200°/s, by 10~20°) in horizontal semicircular canal and vertical semicircular canal plane. Recording patients’ eye movement curve and head movement curve by frequency 220 frames/points. The system was calibrated before each examination. Gain value=peak velocity of eye movement curve/peak velocity of head movement curve. The mean gain value after 20 effective swings was used as the final result. The gain value of the horizontal semicircular canal was measured in the normal range of 0.8–1.1, and the gain value of the vertical semicircular canal was measured in the normal range of 0.7–1.0. Gain asymmetry ratio = (healthy side gain-damage side gain)/(healthy side gain + damage side gain) x100%. Gain asymmetry ratio of 15% was considered abnormal, suggesting an asymmetry of bilateral vestibular function.
Pure tone audiometric testing: It is performed by presenting a pure tone to the ear through an earphone and measuring the lowest intensity in decibels (dB) at which this tone is perceived 50% of the time. This measurement is called threshold. The testing procedure is repeated at specific frequencies from 250 to 8000 hertz (Hz, or cycles per second) for each ear, and the thresholds are recorded on a graph called an audiogram. Bone conduction testing is done by placing an oscillator on the mastoid process and measuring thresholds at the same frequencies. Masking noise is sometimes used in the nontest ear to prevent its participation in the test.
VEMP: Cervical vestibular evoked myogenic potentials (cVEMP) and ocular vestibular evoked myogenic potentials (oVEMP) were recorded using Eclipse (Interacoustics, Denmark). cVEMP: The examinee was asked to lie on his back on a hard bed surface, lift his head approximately 30° away from the bed surface, and turn his head to the opposite side and lower his head so that the mandibular angle was close to the medial end of the ipsilateral clavicle. The recording electrode was attached to the middle of the sternocleidomastoid muscle near the examinee side, the reference electrode was attached to the upper sternum, and the ground electrode was attached to the middle of the forehead. oVEMP: The patient was asked to lie supine, and the recording electrode was placed 1 cm below the center of the contralateral lower eyelid of the examined ear. The reference electrode was attached 2 cm below the recording electrode, and the ground electrode was attached above the middle of the forehead. During the recording of ocular muscle potential, the patient was instructed to stare upward at the fixed target at approximately 30° with the horizontal plane as a reference (marked at approximately 0.5 m from the eye). The cVEMP anatomic parts, posterior semicircular canal - balloon sac - inferior vestibular nerve - vestibular nucleus - spinal oculomotor nucleus - sternocleidomastoid muscle; oVEMPanatomic parts, anterior semicircular canal and horizontal semicircular canal - oval sac - superior vestibular nerve - vestibular nucleus - medial longitudinal tract - oculomotor nucleus - external inferior oblique muscle.10
Click pure tone of 0.1 ms at a rate of 5.1/s at an intensity of 100 dB nHL were presented to the ipsilateral ear by air conduction insert ear phones, with 200 stimuli at 500 Hz and −20–80ms milliseconds recording time. The rise and fall time was 2ms. The first negative wave appearing in the recorded waveform is N1, and the first positive wave is P1. N1-P1 can represent the amplitude of this side. For convenience of statistical comparison, the asymmetric ratio (AR) of oVEMP and cVEMP amplitudes is used as an observation index. AR=((healthy side amplitude – affected side amplitude)/(healthy side amplitude + affected side amplitude) x100%. If AR≥30%, it is determined that the VEMP on this side is abnormal.23
Patient Follow-Up
The included group of underlying diseases including hypertension, coronary artery disease, diabetes mellitus, renal insufficiency, and other common diseases with multisystem involvement.
Vestibular rehabilitation was started when VN patients could tolerate bed exercise (within 1 week after onset). Patients were instructed to rotate and move their head up and down while keeping their eyes anchored on a static target. After becoming familiar with the exercise, patients were instructed to perform the same head movement while keeping their eyes anchored on the same target moving in the opposite direction. They were also instructed on exercises to improve posture and gait, which were started after the VOR exercises. All exercises were performed three times a day for 5 to 10 min each time.
After the informed consent of the patient himself or his family members, the clinician gave 40–80 mg of methylprednisolone (intravenous drip), stopped after 3–5 days and recorded. This is largely influenced by the clinical experience of the supervising physician and the speed with which the patient recovers from symptoms. Patients using glucocorticoids must also take adjuvant drugs such as proton pump inhibitors and calcium agents to avoid complications. All dosage sizes and cycles used are in accordance with expert consensus.18
Independent standing time was defined as the time period from the patient’s constant bed rest at the onset to the first independent standing, and the standing time was no less than 3 min.
This study is a prospective observational study. The first information collection was performed within 3 days of the onset of vertigo symptoms. Symptomatological changes, physical examination, necessary vestibular function tests and persistence time of vestibular rehabilitation were also recorded at the patients’ follow-up at 4 and 12 weeks after disease onset.
Statistical Analysis
Statistical analysis was performed using SPSS 26.0 (SPSS, Inc., Chicago, IL). All of the data were tested for normality test (Shapiro-wilk test, SW). In addition to SPV, the other data are in normal distribution. SPV is presented as median (25th percentile, 75th percentile). The measurement data were expressed as the mean ± standard deviation (M±SD) and compared by t test, one-way analysis of variance (ANOVA), or Kruskal‒Wallis test. The change values of DHI score (ΔDHI), EEV score (ΔEEV), horizontal SPV of SPN (ΔSPV), gain of affected side horizontal semicircular canal in vHIT (ΔGain), and UW in caloric test (ΔUW) of VN patients at 4 weeks and 12 weeks after onset were each combined into 5 groups of data and corresponded to each of them according to the basic patient information to establish a database. A corrected chi-square test or Fisher test was selected between the group variables, such as the rate of combined underlying disease and preinfection by sex group and the rate of glucocorticoid use by combined underlying disease group. The Spearman test is used for the correlation analyses. Multiple linear regression analysis (stepwise regression analysis) was used to identify the vestibular function tests that had a linear regression relationship with the subjective quantitative results. All tests were two-tailed, and P < 0.05, p<0.01 were considered statistically significant.
Results
General Comparison
The mean age of the 41 patients was 42.39 ± 14.42, ranging from 15 to 79 years old. These included 17 males (41.46%) with a mean age of 40.9 and 24 females (58.54%) with a mean age of 43.5. Thirty patients received glucocorticoids, and 11 had no clear contraindications but refused such treatment. Age, prevalence of hypertension and diabetes, SPN direction, history of preinfection, the rate of glucocorticoid used, and independent standing time were not found to be significantly different between the two groups by sex (P>0.05). At the first visit of VN patients, eight patients had posterior semicircular canal gain reduction, of which 3 (37.5%) had a vertical upward vector in the SPN, and the composition ratio was not statistically significantly different (χ2 = 1.23, P > 0.05) compared with the group of 33 patients without posterior semicircular canal involvement (22 patients (66.7%) with a vertical vector in the SPN). Based on the results of vHIT, caloric test and VEMP, we concluded that all 41 patients had superior vestibular nerve damage (all had horizontal gain of vHIT reduction and UW over 25%). There were no VN patients presenting with SPN downwards vector alone. Three of the eight cases with posterior semicircular canal gain reduction had horizontal and upward vector of SPN. In contrast, only horizontal vector in SPN was present in the other five cases beside eight cases with posterior semicircular canal gain reduction. In two of these five cases, both oVEMP and cVEMP were abnormal. Therefore, we concluded that there were two cases of superior vestibular neuritis combined with inferior vestibular neuritis and no simple inferior vestibular neuritis in 41 patients.
Because SPV data of SPN did not fit the normal distribution, the non-parametric test (Kolmogorov Smirnov test) was chosen, and the SPV of VN patients at onset (12.5(8.7,17.5)), after 4 weeks (2.7(0.5,3.4)), and 12 weeks (0.5(0.1,1.1)) later and gradually decreased. DHI and EEV score, horizontal SPV of SPN, gain of affected side horizontal semicircular canal in vHIT, asymmetric ratio of oVEMP, and UW in caloric test was significantly improved after 4 and 12 weeks (Table 1). In particular, the improvement was higher in the first 4 weeks. As we known, the pathologic rates of oVEMP depend on the nerve involvement in VN and the lower positive rate of VEMPs in our study is different from previous studies.11,24 At the time of onset, only 10 of the 41 patients (24.39%) with VN had abnormal appearance of oVEMP, which was mainly characterized by AR and no significant prolongation of latency, including 2 cases of combined cVEMP examination abnormality, with the vast majority returning to within the normal range at 4 weeks. Dynamic changes of typical caloric test (Figure S1–3), vHIT (Figure S4–7), and oVEMP (Figure S8–11), in patients with VN are shown in the Supplementary.
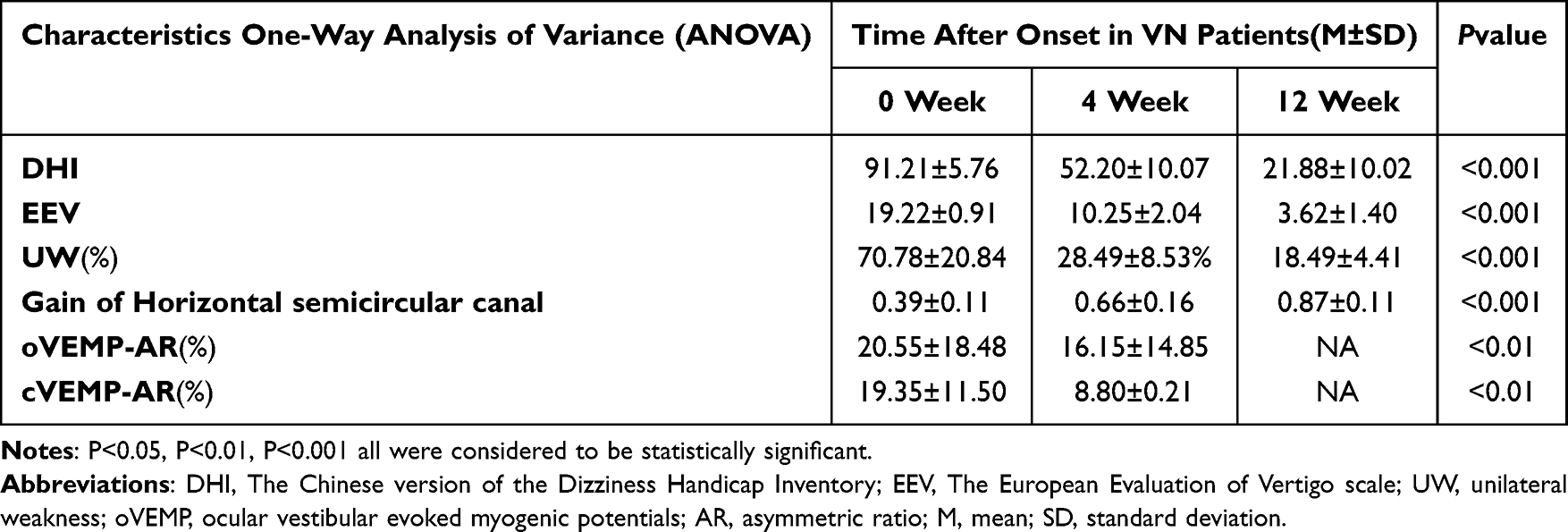 |
Table 1 Dynamic changes in indices of vestibular function in patients with vestibular neuritis at the onset of the disease and at 4 and 12 weeks after its onset |
Prognostic Analysis
Grouping by preinfection, independent standing time longer than 3 days and performing vestibular rehabilitation exercises as seen in Table 2, there was no significant difference in DHI and EEV scale scores, UW and gain values in vHIT between the two groups at each time point (P > 0.05). Statistical analysis of glucocorticoid therapy was performed based on the absolute value of the difference in the above mentioned variables from those at onset. Grouping by underlying diseases or glucocorticoid therapy, a significant difference was observed between the groups after 12 weeks of follow-up in all characteristics (P < 0.05). The absence of underlying disease and receiving glucocorticoid therapy can significantly promote the recovery of vertigo symptoms and objective vestibular function tests for VN patients in 4 weeks (Table 3 and Table 4). At 12 weeks, UW and Gain showed no significant difference between the two groups except on the DHI or EEV scales (P < 0.05). There was a statistically significant difference in age between the no underlying disease group and the underlying disease group (p<0.01), the underlying disease group was older but not in glucocorticoid therapy (χ2 = 1.41, P > 0.05). The composition of patients in the included underlying disease group included three cases of hypertension, four cases of combined diabetes mellitus, and one case of combined renal insufficiency.
 |
Table 2 Influence of vestibular rehabilitation, history of preinfection, and independent standing time on indicators in patients with vestibular neuritis |
 |
Table 3 Influence of comorbid underlying diseases on indicators in patients with vestibular neuritis |
 |
Table 4 The influence of the use of glucocorticoids on the indicators of patients with vestibular neuritis |
Correlation Analysis
Table 5 shows the Spearman correlation coefficients between ΔDHI with ΔEEV, ΔGain, ΔSPV and ΔUW. ΔDHI was most strongly correlated with EEV (r=0.9, p<0.001). Gain was most strongly positive correlated with ΔEEV (R=0.678, p<0.001) and was significantly correlated with ΔDHI (R=0.643, p<0.01).
 |
Table 5 Correlation analysis between the main observables in patients with vestibular neuritis |
Table 6 shows the results of a stepwise regression analysis for investigating Gain. The results revealed that ΔEEV and ΔUW were significant and independent determinants, and the following estimation formula was created: ΔGain=0.023 × ΔEEV + 0.02 × ΔUW − 0.03. The coefficient was R2=0.507 (p<0.01). In addition, the regression coefficients in the results of the regression analysis with EEV as the dependent variable are the same as the regression coefficients in Model 1 in the regression analysis with Gain as the dependent variable (R=0.473, p<0.01).
 |
Table 6 Multiple linear regression regression analysis of the change values of total scores of DHI scale and EEV scale using stepwise regression method |
Discussion
Clinical symptoms such as severe vertigo symptoms and abnormal vestibular function test results always improve gradually over time in most VN patients, but the speed of recovery of signs and vestibular function test abnormalities show significant differences between different signs and vestibular function test abnormalities.25 This corresponds well with the results of our clinical observation group and with the dynamic observations of individual vestibular examination follow-up in our (Supplementary Figure 1–11). Based on our results, poorer recovery of vertigo symptoms and objective vestibular function tests were observed in the combined underlying disease group for VN patients at 4 weeks. However, our study was limited to common underlying diseases such as hypertension, diabetes and renal insufficiency, and was a single-center study, so the conclusions were not very accurate. There was a significant difference in age between the two groups above, combined underlying disease group being older. At 12 weeks post-onset, only the DHI scale, which measures vertigo-related quality of life and residual symptoms, was worse than the group without underlying disease. This is generally compatible with the results of past evidence.26,27 Age-related decline of vestibular function has been shown to correlate with the age-related decrease in the number of vestibular hair cells and neurons. The mechanism of age-related cellular loss in vestibular end organ is unclear, but it is thought that genetic predisposition and cumulative effect of oxidative stress may both play an important role.28 In our study, the combined underlying disease group was also elderly, and the effect of age on the study results was clear. Major contributing factors for vestibular impairment in hypertension and diabetes are microangiopathic effects, such as ischemia of the vestibular microcirculation, alteration of the metabolism of the inner ear fluid, and loss of type-I hair cells in the saccule.29,30 They mainly cause vestibular nerve signal transduction and vestibular organ structure changes. However, the evidence for their involvement in the etiology of vestibular neuritis is not strong. However, in the follow-up of VN patients by Tao Yan et al, the elderly group with more patients combined with underlying diseases recovered worse in DHI and UW. They suspected that the slow recovery of elderly VN patients may be related to secondary psychiatric disorders such as anxiety and depression, as the Hamilton’s Anxiety Scale and the Depression Scale were lowest in the adolescent group and the DHI score was significantly correlated with the Hamilton Anxiety Scale score in the VN acute phase.26 Another study has also observed a significant correlation between DHI and depression and anxiety scores, not only in the acute phase of VN, but among other vestibular disorders.31 More studies are needed to clarify the extent to which residual vestibular impairment and secondary mental psychosocial factors affect these indicators in patients with VN in the acute and recovery phases. At the same time, active interventions for possible anxiety and depression in the acute phase of VN are worth discussing.
After a statistical analysis with or without combined glucocorticoid therapy as a grouping condition, we found that the glucocorticoid-treated group had an advantage over the no glucocorticoid-treated group in terms of improvement of subjective vertigo symptoms and objective vestibular function tests in VN patients during the early recovery period (4 weeks). The improvement in UW abnormalities within 4 weeks was in general agreement with the results of the meta-analysis by Fishman and Molnár.15,32 In another recent meta-analysis comparing VN patients who both received basic treatment (stop dizziness, vomiting and other conventional treatment) at 4 weeks after onset, there was a statistically significant difference in the advantage of early single glucocorticoid therapy than single vestibular rehabilitation in terms of improvement in UW abnormalities, while there was an advantage of vestibular rehabilitation in terms of improvement in subjective vertigo symptoms such as DHI scale assessment, again significantly different.33 However, in our study, patients with VN who adhered to vestibular rehabilitation for more than 4 or 8 weeks did not have a significant advantage in all observed indicators. It has also been noted in the literature that regarding DHI scores, there was no significant difference between glucocorticoid therapy combined with vestibular rehabilitation versus glucocorticoid therapy alone at the 12-month follow-up.16 Therefore, we believe that there is a short-term benefit for VN patients after glucocorticoid therapy in improving objective vestibular function tests such as UW abnormalities and reduced vHIT gain, while the value of glucocorticoid therapy and vestibular rehabilitation for short-term clinical symptom improvement remains controversial, and more evidence is urgently needed.
In analyzing the medium- to long-term (12 weeks) prognosis of patients with VN, our study found a benefit of glucocorticoid therapy only in terms of improving vestibular symptoms (eg, EEV), and the results were not sufficiently significant. As stated in numerous publications, there is still a lack of evidence that the use of glucocorticoids is effective in improving long-term clinical outcomes.15,16,33–36 This is the same in vestibular rehabilitation.33,35,36
Most of the earlier literature confirmed that there is no clear linear relationship between either DHI values or ΔDHI and UW, gain or asymmetry ratio within 1–3 months after onset in VN patients, and they do not seem to reflect patient-specific subjective vertigo symptoms at a given moment in time.37–39 Riska et al40 also did not find a relationship with DHI depending on the type of corrective saccade (dominant or recessive) grouping. Although in some recent vHIT studies,17,41 the authors considered that corrective saccades appear to be involved in visual retention and oculomotor compensation during head rotation, there is no evidence that corrective saccades contribute to the recovery of subjective vertigo symptoms in patients with VN. Furthermore, George et al42 concluded that there was no clear correlation between parameters such as corrective saccades and gain in vHIT and DHI.
In theory, the deficiency of dynamic vision in vestibular dysarthria is due to the illusion of instability caused by the mismatch between the speed of eye movement and the speed of head movement during high-speed activities.43 The gain of vHIT is a new generation measurement method for measuring the relationship between eye movement speed and head movement speed for evaluating VOR function quantitatively, and it is comparable to the gold standard technique (each coil recordings) in identifying peripheral vestibular diseases.44 We considered that there should be some relationship between the gain of vHIT and the vertigo symptoms of patients. In the current literature,45,46 there is indeed a connection between gait abnormalities and vertigo symptoms in some dizziness/vertigo patients. In this study, a significant linear regression was found between the value of the change in the affected horizontal semicircular canal gain in the vHIT and the results of the EEV scale, which represents vestibular symptoms and better reflects the degree of recovery of subjective vestibular symptoms. The DHI scale, which includes the patient’s life disability, psychological characteristics, and overall assessment of vestibular symptoms, was less well correlated. This suggests that when we find a patient recovered on vHIT but still show poor improvement on subjective vertigo and dizziness, this is likely to suggest that the patient has recovered well from impaired peripheral vestibular organ function and that the vertigo symptoms caused by it may no longer play a dominant role. Additional screening should be performed for possible co-occurring psychosomatic factors or psychiatric disorders such as persistent postural dizziness and anxiety states.47
The drawback of our study is the absence of longer-term follow-up data and more cases for analysis. In addition, factors such as corrective saccades included the peak velocity of eye movement and time to peak or abnormal saccade rates are not integrated for correlation analysis. Additionally, more cases are needed due to issues such as the low positive rate and cooperation rate of VEMP. This requires further research in the future.
Conclusion
The absence of underlying disease and the receipt of glucocorticoid therapy significantly contributed to the improvement of objective vestibular function tests in the short term, while the improvement of subjective vertigo may correlate with the different objective measures and questionnaire. We believe that the improvement of the affected horizontal semicircular canal gain value in the vHIT can be used as a reference indicator of the degree of improvement of vestibular symptoms with superior vestibular neuritis.
Data Sharing Statement
The raw data supporting the conclusions of this article will be made available. Further inquiries can be directed to the corresponding author.
Ethics Approval
Approval notice number: YXLL-2023-059. Studies involving human participants were reviewed and approved by Institutional review board of Medical Ethics Committee of Shanxi Bethune Hospital. Our study complies with the Declaration of Helsinki.
Acknowledgments
We thank the participants and their family members for participating in the trial.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Strupp M, Bisdorff A, Furman J, et al. Acute unilateral vestibulopathy/vestibular neuritis: diagnostic criteria. J Ves Res. 2022;32(5):389–406. doi:10.3233/VES-220201
2. Hotson JR, Baloh RW. Acute vestibular syndrome. N Engl J Med. 1998;339(10):680–685. doi:10.1056/NEJM199809033391007
3. Kattah JC. Use of HINTS in the acute vestibular syndrome. An Overview Stroke Vasc Neurol. 2018;3(4):190–196. doi:10.1136/svn-2018-000160
4. Krishnan K, Bassilious K, Eriksen E, et al. Posterior circulation stroke diagnosis using HINTS in patients presenting with acute vestibular syndrome: a systematic review. Eur Stroke J. 2019;4(3):233–239. doi:10.1177/2396987319843701
5. Strupp M, Feil K, Dieterich M, Brandt T. Bilateral vestibulopathy. Handb Clin Neurol. 2016;137:235–240.
6. Thomas JO, Sharobeam A, Venkat A, et al. Video head impulse testing to differentiate vestibular neuritis from posterior circulation stroke in the emergency department: a prospective observational study. BMJ Neurol Open. 2022;4(1):e000284. doi:10.1136/bmjno-2022-000284
7. Redondo-Martínez J, Bécares-Martínez C, Orts-Alborch M, García-Callejo FJ, Pérez-Carbonell T, Marco-Algarra J. Relationship between video head impulse test (vHIT) and caloric test in patients with vestibular neuritis. Acta Otorrinolaringol. 2016;67(3):156–161. doi:10.1016/j.otorri.2015.07.005
8. Molnár A, Maihoub S, Tamás L, Szirmai Á. Comparison between caloric and video-head impulse tests in Ménière’s disease and vestibular neuritis. Int J Audiol. 2023;62(5):393–399. doi:10.1080/14992027.2022.2059711
9. Dlugaiczyk J. Evidence-based diagnostic use of VEMPs: from neurophysiological principles to clinical application. HNO. 2020;68(Suppl 2):69–78. doi:10.1007/s00106-019-00767-2
10. Curthoys IS, Manzari L, Smulders YE, Burgess AM. A review of the scientific basis and practical application of a new test of utricular function--ocular vestibular-evoked myogenic potentials to bone-conducted vibration. Acta Otorhinolaryngol Ital. 2009;29(4):179–186.
11. Chang CM, Lo WC, Young YH, et al. Galvanic vestibular-evoked myogenic potentials in evaluating damaged sites of vestibular neuritis. Laryngoscope Investig Otolaryngol. 2022;7(2):506–514. doi:10.1002/lio2.745
12. Strupp M, Zingler VC, Arbusow V, et al. Methylprednisolone, valacyclovir, or the combination for vestibular neuritis. N Engl J Med. 2004;351(4):354–361. doi:10.1056/NEJMoa033280
13. Karlberg ML, Magnusson M. Treatment of acute vestibular neuronitis with glucocorticoids. Otol Neurotol. 2011;32(7):1140–1143. doi:10.1097/MAO.0b013e3182267e24
14. Zaper D, Adamec I, Gabelić T, et al. Vestibularni neuronitis: patofiziologija, dijagnoza i lijecenje [Vestibular neuronitis: pathophysiology, diagnosis and treatment]. Lijec Vjesn. 2012;134(11–12):340–345.
15. Fishman JM, Burgess C, Waddell A. Corticosteroids for the treatment of idiopathic acute vestibular dysfunction (vestibular neuritis). Coch Data Sys Rev. 2011;5(5):CD008607.
16. Ismail EI, Morgan AE, Abdel Rahman AM. Corticosteroids versus vestibular rehabilitation in long-term outcomes in vestibular neuritis. J Vestib Res. 2018;28(5–6):417–424. doi:10.3233/VES-180645
17. Martin-Sanz E, Rueda A, Esteban-Sanchez J, Yanes J, Rey-Martinez J, Sanz-Fernandez R. Vestibular restoration and adaptation in vestibular neuritis and Ramsay hunt syndrome with vertigo. Otol Neurotol. 2017;38(7):e203–e208. doi:10.1097/MAO.0000000000001468
18. Professional Committee on Vertigo, Division of Neurology, Chinese Medical Doctor Association Stroke and Vertigo Branch, Chinese Stroke Association. Multidisciplinary experts consensus on vestibular neuritis. Chin J Geriat. 2020;39(9):985–994.
19. Zhang Y, Liu B, Wang Y, et al. 眩晕残障量表(DHI)中文版的信度和效度分析 [Analysis of reliability and validity of the Chinese Version of Dizziness Handicap Inventory (DHI)]. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2015;50(9):738–743. Chinese.
20. Jacobson GP, Newman CW. The development of the dizziness handicap inventory. Arch Otolaryngol Head Neck Surg. 1990;116(4):424–427. doi:10.1001/archotol.1990.01870040046011
21. Mègnigbêto CA, Sauvage JP, Launois R. Validation clinique d’une échelle du vertige: EEV (European Evaluation of Vertigo) [The European Evaluation of Vertigo (EEV) scale: a clinical validation study]. Rev Laryngol Otol Rhinol. 2001;122(2):95–102.
22. Jongkees LB, Maas JP, Philipszoon AJ. Clinical nystagmography. A detailed study of electro-nystagmography in 341 patients with vertigo. Pract Otorhinolaryngol. 1962;24:65–93.
23. Fröhlich L, Curthoys IS, Kösling S, Obrist D, Rahne T, Plontke SK. Cervical and ocular vestibular-evoked myogenic potentials in patients with intracochlear schwannomas. Front Neurol. 2020;11:549817. doi:10.3389/fneur.2020.549817
24. Murofushi T, Halmagyi GM, Yavor RA, Colebatch JG. Absent vestibular evoked myogenic potentials in vestibular neurolabyrinthitis. An indicator of inferior vestibular nerve involvement? Arch Otolaryngol Head Neck Surg. 1996;122(8):845–848. doi:10.1001/archotol.1996.01890200035008
25. Choi KD, Oh SY, Kim HJ, Koo JW, Cho MB, Kim JS. Recovery of vestibular imbalances after vestibular neuritis. Laryngoscope. 2010;117(7):1307–1312. doi:10.1097/MLG.0b013e31805c08ac
26. Yan T, Zong F, Han X, et al. Vestibular neuritis in patients among different age groups: clinical features and outcomes. J Am Acad Audiol. 2020;31(9):629–635. doi:10.1055/s-0040-1717067
27. Fujimoto C, Egami N, Kinoshita M, Sugasawa K, Yamasoba T, Iwasaki S. Postural stability in vestibular neuritis: age, disease duration, and residual vestibular function. Laryngoscope. 2014;124(4):974–979. doi:10.1002/lary.24342
28. Iwasaki S, Yamasoba T. Dizziness and imbalance in the elderly: age-related decline in the vestibular system. Aging Dis. 2014;6(1):38–47. doi:10.14336/AD.2014.0128
29. Oron Y, Shemesh S, Shushan S, et al. Cardiovascular risk factors among patients with vestibular neuritis. Ann Otol Rhinol Laryngol. 2017;126(8):597–601. doi:10.1177/0003489417718846
30. Kumar P, Singh NK, Apeksha K, Ghosh V, Kumar RR, Kumar Muthaiah B. Auditory and vestibular functioning in individuals with type-2 diabetes mellitus: a systematic review. Int Arch Otorhinolaryngol. 2021;26(2):e281–e288. doi:10.1055/s-0041-1726041
31. Molnár A, Maihoub S, Mavrogeni P, Tamás L, Szirmai Á. Depression scores and quality of life of vertiginous patients, suffering from different vestibular disorders. Eur Arch Otorhinolaryngol. 2022;279(11):5173–5179. doi:10.1007/s00405-022-07366-y
32. Molnár A, Jassoy BD, Maihoub S, Mavrogeni P, Tamás L, Szirmai Á. Long-term follow-up of patients with vestibular neuritis by caloric testing and directional preponderance calculation. Eur Arch Otorhinolaryngol. 2023;280(4):1695–1701. doi:10.1007/s00405-022-07660-9
33. Hidayati HB, Imania HAN, Octaviana DS, et al. Vestibular rehabilitation therapy and corticosteroids for vestibular neuritis: a systematic review and meta-analysis of randomized controlled trials. Medicina. 2022;58(9):1221. doi:10.3390/medicina58091221
34. Bogdanova A, Dlugaiczyk J, Heckmann JG, Schwab S. Corticosteroids in patients with vestibular neuritis: an updated meta-analysis. Acta Neurol Scand. 2022;146(5):429–439. doi:10.1111/ane.13676
35. Shupak A, Issa A, Golz A, Braverman I, Braverman I. Prednisone treatment for vestibular neuritis. Otol Neurotol. 2008;29(3):368–374. doi:10.1097/MAO.0b013e3181692804
36. Goudakos JK, Markou KD, Psillas G, Vital V, Tsaligopoulos M. Corticosteroids and vestibular exercises in vestibular neuritis. Single-blind randomized clinical trial. JAMA Otolaryngol Head Neck Surg. 2014;140(5):434–440. doi:10.1001/jamaoto.2014.48
37. Zellhuber S, Mahringer A, Rambold HA. Relation of video-head-impulse test and caloric irrigation:A study on the recovery in unilateral vestibular neuritis. Eur Arch Otorhinolaryngol. 2014;271(9):2375–2383. doi:10.1007/s00405-013-2723-6
38. McCaslin DL, Jacobson GP, Bennett ML, Gruenwald JM, Green AP. Predictive properties of the video head impulse test: measures of caloric symmetry and self-report dizziness handicap. Ear Hear. 2014;35(5):e185–91. doi:10.1097/AUD.0000000000000047
39. Manzari L, Graziano D, Tramontano M. The different stages of vestibular neuritis from the point of view of the video head impulse test. Audiol Res. 2020;10(2):31–38. doi:10.4081/audiores.2020.248
40. Riska KM, Bellucci J, Garrison D, Hall C. Relationship between corrective saccades and measures of physical function in unilateral and bilateral vestibular loss. Ear Hear. 2020;41(6):1568–1574. doi:10.1097/AUD.0000000000000885
41. Yang CJ, Cha EH, Park JW, et al. Diagnostic value of gains and corrective saccades in video head impulse test in vestibular neuritis. JAMA Otolaryngol Head Neck Surg. 2018;159(2):347–353. doi:10.1177/0194599818768218
42. Psillas G, Petrou I, Printza A, et al. Video Head Impulse Test (vHIT): value of gain and refixation saccades in unilateral vestibular neuritis. J Clin Med. 2022;11(12):3467. doi:10.3390/jcm11123467
43. Halmagyi GM, Curthoys IS, Cremer PD, Henderson CJ, Todd MJ. The human horizontal vestibulo-ocular reflex in response to high-acceleration stimulation before and after unilateral vestibular neurectomy. Exp Brain Res. 1990;81(3):479–490. doi:10.1007/BF02423496
44. MacDougall HG, Weber KP, McGarvie LA, Halmagyi GM, Curthoys IS. The video head impulse test: diagnostic accuracy in peripheral vestibulopathy. Neurology. 2009;73(14):1134–1141. doi:10.1212/WNL.0b013e3181bacf85
45. Chang TP, Schubert MC. Association of the video head impulse test with improvement of dynamic balance and fall risk in patients with dizziness. JAMA Otolaryngol Head Neck Surg. 2018;144(8):696–703. doi:10.1001/jamaoto.2018.0650
46. Guan R, Zhao Z, Guo X, Sun J. The semicircular canal function tests contribute to identifying unilateral idiopathic sudden sensorineural hearing loss with vertigo. Am J Otolaryngol. 2020;41(3):102461. doi:10.1016/j.amjoto.2020.102461
47. Cousins S, Kaski D, Cutfield N, et al. Predictors of clinical recovery from vestibular neuritis: a prospective study. Ann Clin Trans Neurol. 2017;4(5):340–346. doi:10.1002/acn3.386
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.