Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 17
Obesity-Related Knowledge and Practice Among the Healthcare Professions Students in Saudi Arabia
Authors Elsafi SH ![]() , Al-Dossari RH, Al-shaqi RA, Fakirah WE, Al-Dossari RF, Al-sharif OJ, Maawadh RM
, Al-Dossari RH, Al-shaqi RA, Fakirah WE, Al-Dossari RF, Al-sharif OJ, Maawadh RM ![]() , Al Musallam LD, Alaohali A, Abu Hassan AM, Alfahad OA, Al Naam YA
, Al Musallam LD, Alaohali A, Abu Hassan AM, Alfahad OA, Al Naam YA ![]() , Al Zahrani EM
, Al Zahrani EM
Received 18 October 2023
Accepted for publication 16 January 2024
Published 26 January 2024 Volume 2024:17 Pages 427—434
DOI https://doi.org/10.2147/DMSO.S445385
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Salah H Elsafi,1 Reem H Al-Dossari,1 Ruaa A Al-shaqi,1 Wateen E Fakirah,1 Rawan F Al-Dossari,1 Omniyyah J Al-sharif,1 Rawan M Maawadh,1 Lenah D Al Musallam,1 Abeer Alaohali,2 Abdulelah M Abu Hassan,3 Othman A Alfahad,4 Yaser A Al Naam,1 Eidan M Al Zahrani5
1Clinical Laboratory Sciences Department, Prince Sultan Military College of Health Sciences, Dhahran, Saudi Arabia; 2Dental and Oral Health Department, Prince Sultan Military College of Health Sciences, Dhahran, Saudi Arabia; 3Faculty of Medicine, University of Almaarefa, Riyadh, Saudi Arabia; 4Department of Biomedical Technology, Prince Sultan Military College of Health Sciences, Dhahran, Saudi Arabia; 5College Deanship, Prince Sultan Military College of Health Sciences, Dhahran, Saudi Arabia
Correspondence: Salah H Elsafi, Department of Clinical Laboratory Sciences, Prince Sultan Military College of Health Sciences, P.O. Box 33048, Dhahran, 31932, Saudi Arabia, Tel +966138405448, Email [email protected]
Objective: The objectives of this study are to identify the prevalence and the factors behind overweight and obesity among the healthcare profession’s students.
Methods: A well-structured and validated questionnaire was distributed to a heterogeneous purposive sample of the healthcare profession’s students in Saudi Arabia.
Results: About 21.0% and 15.5% were overweight and obese, respectively. The average knowledge score was 70.6% and increased with age and among obese participants. The average attitude score was 74.8% with no variation within age, body mass index (BMI), and gender. The average practice score was only 36.7%. There was a significant variation of the practice within the different age groups (P = 0.021). There was a significant association between the participant’s knowledge and attitude, and practice.
Conclusion: The average practice score was poor. Despite their good knowledge and positive attitude, the students are exposed to heavy junk food marketing, which encourages overconsumption by instilling positive emotional associations with the junk food. They are mostly physically inactive, anxious and sleep deprived, which can lead to poor eating habits. For this group, various strategies and motivators will likely be needed.
Keywords: obesity prevention, awareness, practice, healthcare students, Saudi Arabia
Introduction
Obesity is a complicated, multifaceted condition, defined as an excess health risk induced by adiposity that exceeds the normal size observed in the population, ie a body mass index (BMI) of 30 or above for adults.1 Since 1980, the prevalence of overweight and obesity has risen globally, to the point where about a third of the global population is now considered to be either overweight or obese.2 Regardless of geographic location, ethnicity, or socioeconomic status, the prevalence of obesity has increased in people of all ages and genders, however it tends to be higher in older people and women.2 A recent countrywide survey in Saudi Arabia indicated an obesity prevalence of a 24.7%.3 Overweight and obesity among the general population of Saudi Arabia were represented by 32.8% and 23%, respectively.3
The rise in obesity and overweight is being attributed to a number of interconnected factors of metabolic, genetic, environmental, and behavioral factors. However, the substantial increase in obesity rates is directly caused by environmental and behavioral factors.4 Obesity rates are also influenced by dietary habits, sedentary lifestyle.5 Obesity in Saudi Arabia has been mostly attributed to the dietary habit, particularly the shift to a Western diet and the high consumption of sugary drink, as well as the high levels of inactivity.6
The economy of the Kingdom of Saudi Arabia has recently expanded at an unparalleled rate. This has brought about a change in the food habit and diet as becoming more westernized.7
Basic knowledge and skills on obesity related factors can lead to an affective attitudes and stress values, hence promoting optimal practice towards obesity prevention. According to the knowledge, attitude, and practice theory, human health behavioral change is achieved through the acquisition of the right knowledge, generation of positive attitudes, and adoption of practices.8 Regular health screenings are necessary to manage the increased incidence of overweight and obesity and lower the risk of obesity-related comorbidities.9 Literature on the awareness and practice of the healthcare profession’s students towards obesity and overweight n Saudi Arabia is lacking. Medical and health allied science students with their presumably good awareness of obesity complications are often thought of as good potential educators and may provide reliable information on their perception and practice to their prospective clients. Moreover, due to the rapid increase in obesity, there has been a continuous need to assess the current prevalence standing. Therefore, the objective of this study is to identify the prevalence of overweight and obesity among college students in Saudi Arabia, evaluate their knowledge, perception, and practice towards obesity prevention. In addition, the study aimed to investigate the factors and reasons behind the prevalence of obesity among the healthcare profession’s students and suggest the perfect interventions for obesity prevention.
Methods
The Ethics Review Board of Prince Sultan Military College of Health Sciences, Dhahran approved this study (IRB-2023-CLS-028). All participant signed an informed consent form. A well-structured, validated, and pretested bilingual questionnaire (English and Arabic) was prepared in accordance with the study’s objectives for this cross-sectional study. After conducting a thorough review of the literature, the research team created the questionnaire. The questionnaire consisted of four sections of close-end type questions. The first section included the demographic variables such as age, gender, body weight, and height. The second part consisted of seven knowledge questions about the obesity risk factors, consequences, and prevention, with a total score of fourteen. The third part included of six questions for measuring the attitude and perception towards obesity and the participant’s concern about body weight, with a total score of six. The fourth part consisted of eleven questions related to practices for obesity prevention such as the participant’s nutritional habit, physical activity, and their compliance with healthy behaviors, with a total score of thirty. The final version of the questionnaire was tested for reliability by distributing to a sample of 60 students of the targeted population, who were not included in the study. The aggregate Cronbach’s alpha score for the survey items was 0.87.
A heterogeneous purposive sample of the healthcare professions students in Saudi Arabia from January 1 to April 30, 2023 were included in this study. The questionnaire was distributed to participants through a web link via several social media platforms. Data collectors located at various Healthcare Colleges campuses have assisted in the distribution of the questionnaire and ensured the inclusion participants of the targeted participants.
Statistical Analysis
Several close-ended questions were used to assess participants’ knowledge, attitude, and practice. Each accurate response to all questions received a score. The average knowledge, attitude, and practice scores were calculated out of the total marks of 14, 6, and 30, which were assigned based on the number of questions in each domain. The data was processed with SPSS software version 28.0 (SPSS, Chicago, Illinois). Cronbach’s alpha was used to assess the questionnaire’s internal consistency reliability, with coefficients of 0.7 indicating internal consistency reliability. We used one way ANOVA to test the significant differences in the knowledge, attitude, and practice due to various demographic variables. We used correlation Pearson coefficient to measure the association between the knowledge, attitude, and practice. Bivariate correlation between the knowledge, attitude, and practice towards obesity prevention was computed. The statistical significance was set at P < 0.05 for all analyses.
Results
The study included 709 (92.8%) of the 764 respondents who successfully completed the questionnaire. Table 1 displays the demographic information of the participants. Female participants made up 55.7% of the total. The mean age of the total participants was 22.11 ± 1.91 years. Those aged less than 24 years made up 59.0% of the population. The vast majority of responses were Saudi nationals (98.8%). The normal body mass index (18.51–24.99) was detected among 56.1% of the participants. However, 21.0% and 15.5% were overweight (25.00–29.99) and obese (> 30.00), respectively, while 7.3% were underweight (< 18.50).
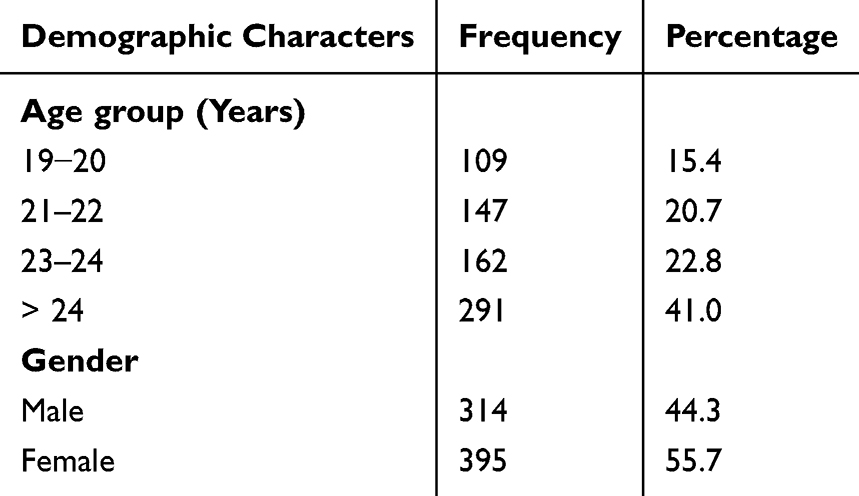 |
Table 1 Demographic Factor of the Total Participants (n = 709) |
Table 2 demonstrates that there was no difference in body mass index across genders, except that more males were underweight than their female peers.
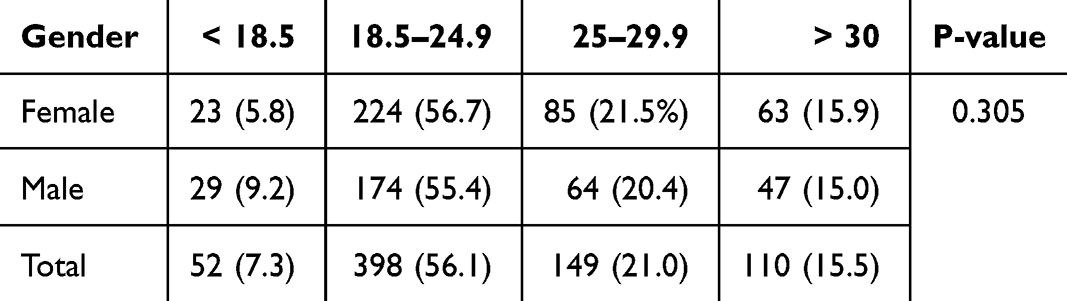 |
Table 2 Body Mass Index Within Gender (n = 709) |
Table 3 shows that the average knowledge score was 9.89 out of 14 (70.6%). The knowledge score varied significantly with age (P=0.048). Older students of more than 24 years were slightly more knowledgeable (10.14 or 72.4%), while the youngest group of less than 18 years were the least knowledgeable (9.39 or 67.1%). The average attitude score was 4.49 out of 6 (74.8%). The attitude score does not vary between all age groups.
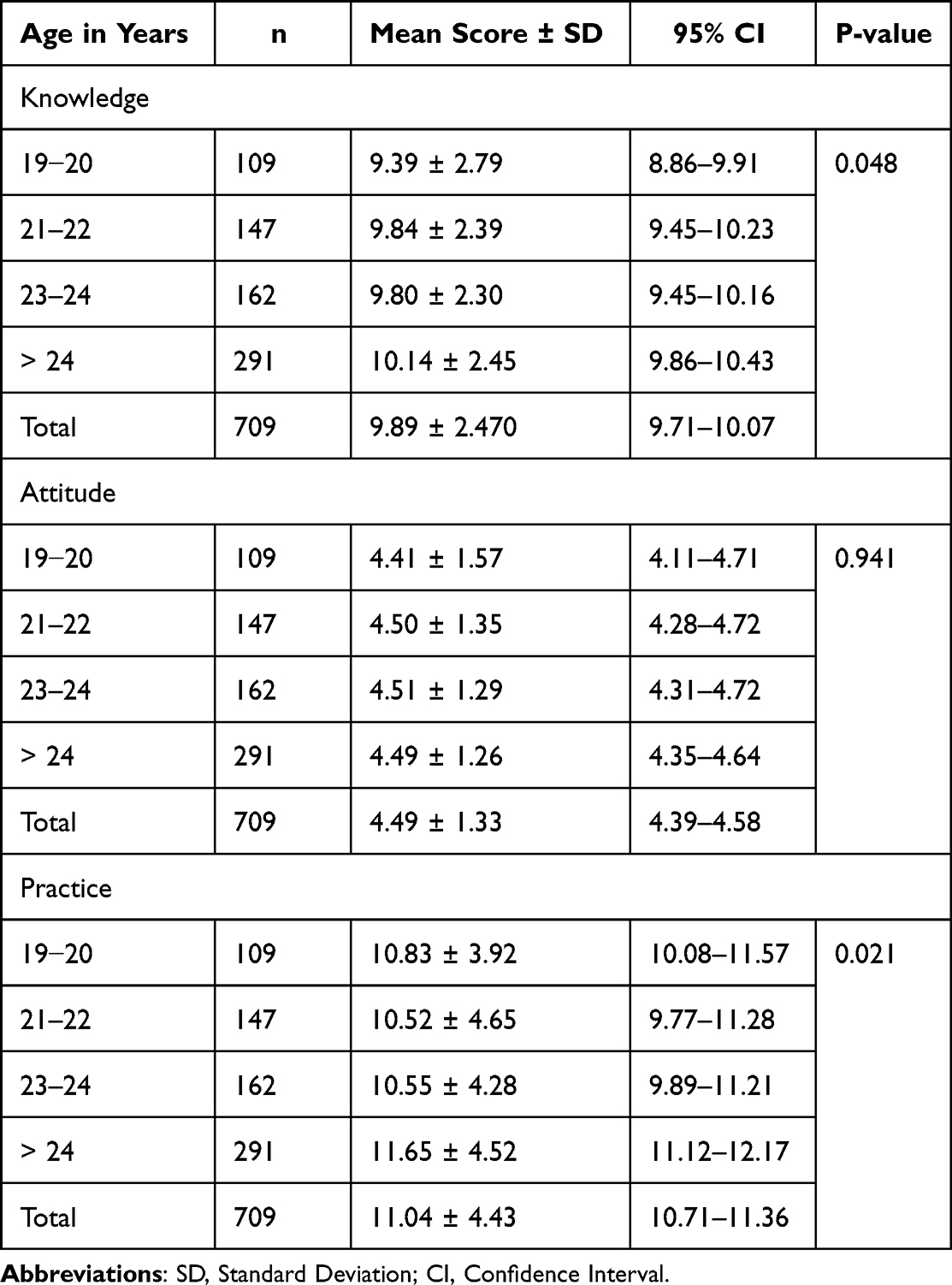 |
Table 3 Mean Scores ± SD of the Knowledge (Out of 14), Attitude (Out of 6), and Practice (Out of 30) of the Participants Towards Obesity by Age-Group and the 95% (CI) (n = 709) |
The average practice score was poor (11.04 out of 30 or 36.7%). There was a significant variation of the practice within the different age groups (P = 0.021). Older students seemed to maintain better practice than younger ones.
Table 4 represents the mean scores of the knowledge, attitude, and practice of the participants towards obesity by body mass index. Although the amount of knowledge increased with increased body mass index, yet the difference was not statistically significant. Individuals with normal or underweight body mass demonstrated the best attitude compared to overweight and obese groups (P<0.001). Table 5 demonstrates the mean scores of the knowledge, attitude, and practice of the participants towards obesity by gender.
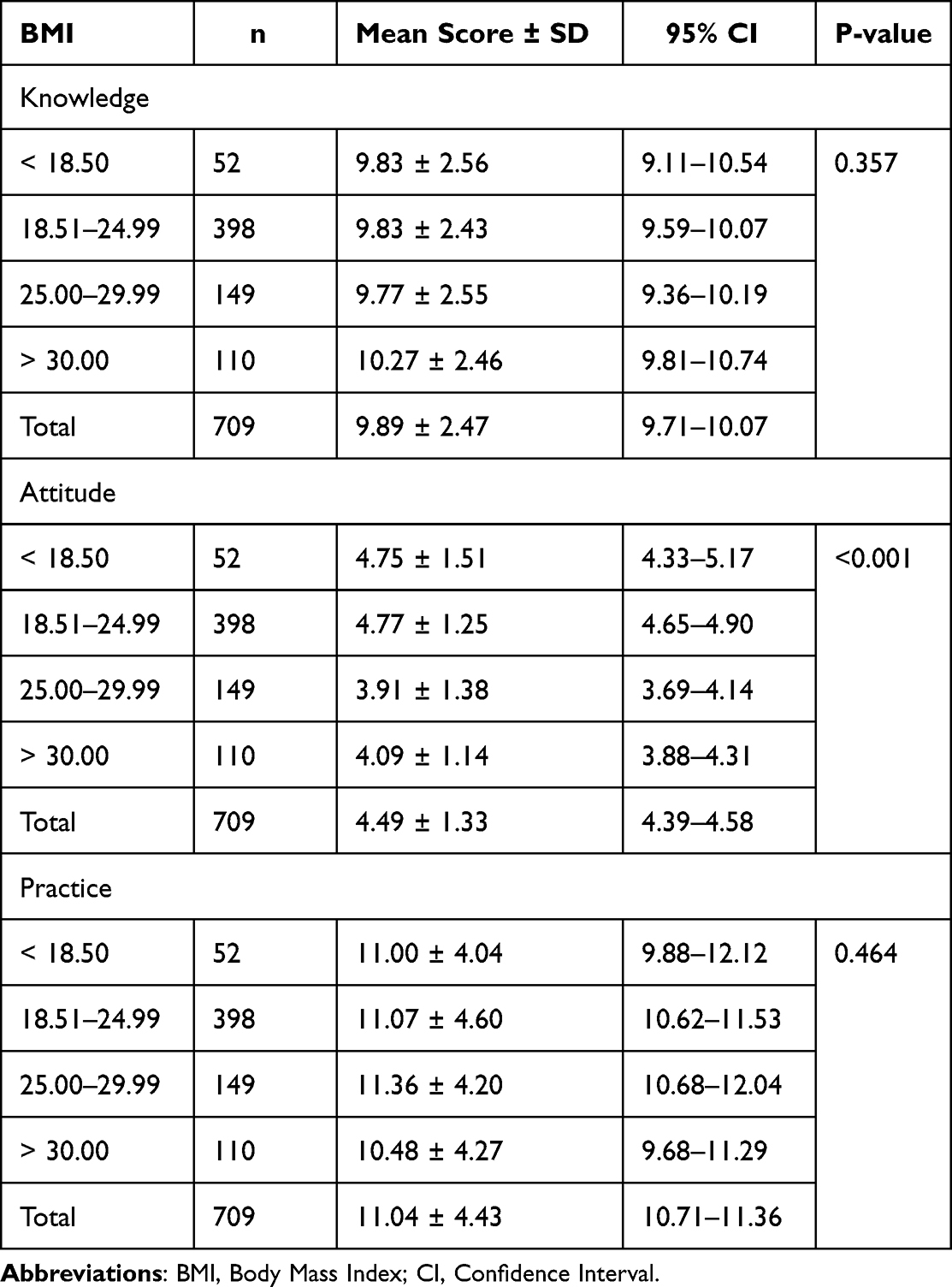 |
Table 4 Mean Scores of the Knowledge, Attitude, and Practice of the Participants Towards Obesity by BMI and the 95% CI (n = 709) |
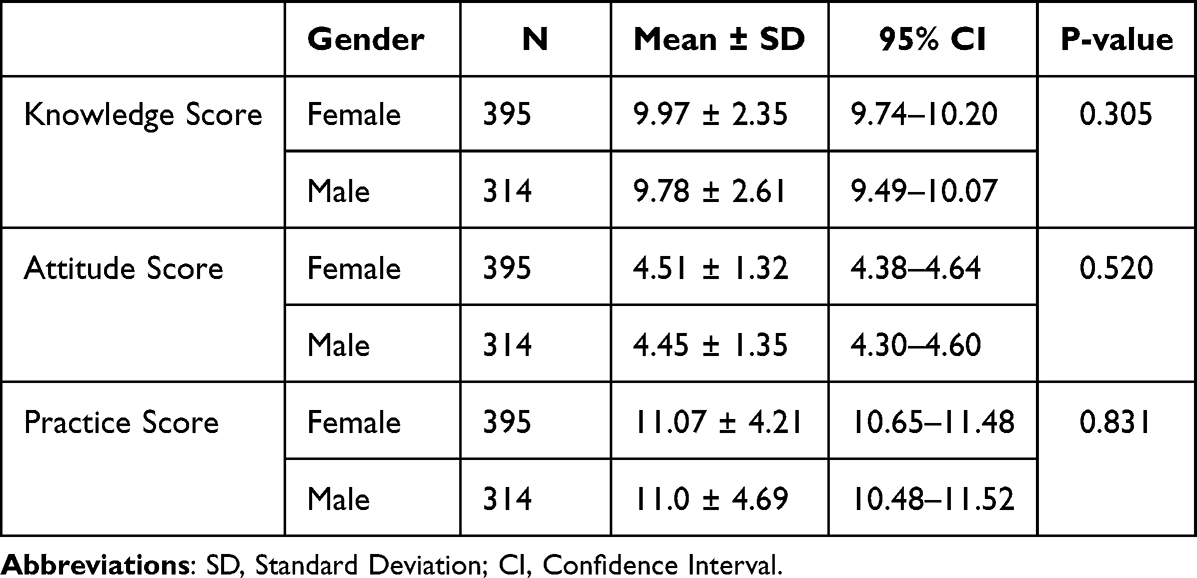 |
Table 5 Mean Scores of the Knowledge, Attitude, and Practice of the Participants Towards Obesity by Gender and the 95% Confidence Interval (CI) (n = 709) |
The Pearson correlation between knowledge, attitude, and practice scores towards obesity is shown in Table 6. This indicates a significant association between the participant’s knowledge and attitude (P <0.001), knowledge and practice (P = 0.029), and attitude and practice (P <0.001).
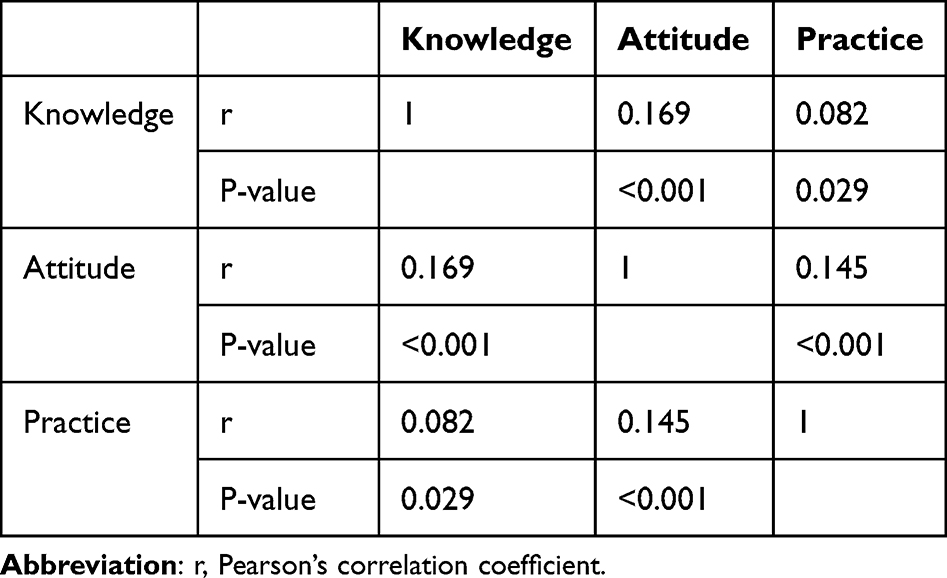 |
Table 6 Pearson Correlation Between Knowledge, Attitude, and Practice Scores Towards Obesity (n=709) |
Discussion
The normal body mass index was noticed among 56.1% of the participants. Overweight and obesity were determined among 21.0% and 15.5%, respectively. 7.3% of people were underweight. A similar recent study in Saudi Arabia resulted in 13.5%, 53.6%, 20.1%, and 12.9% being underweight, normal, overweight, and obese, respectively.10 Although the absolute prevalence rates of overweight and obesity varied greatly across areas and countries, this tendency was consistent with similar studies. Overweight and obesity are most prevalent in American and European countries.2 Obesity prevalence in the United States grew from 30.5% to 42.4% between 1999 and 2018.11 According to the WHO, 60% of European inhabitants are either overweight or obese.12 A study on European population indicated an average of 48.1% of overweight or obesity with a wide variation between countries and males reported greater rates.13 The prevalence of overweight and obesity has increased many folds in most Asian countries during the last few decades, with the amount varying by country.14 Overweight and obesity were recorded in 48.3% of people from various Asian and Midwestern nations, with participants from Bangladesh having the lowest prevalence (19.4%) and those from Egypt having the highest rate (67.5%).15 Obesity was related with higher age and lower level of education and socioeconomic status.13 The prevalence of overweight and obesity in the Eastern Mediterranean region increased to 49.6% and 19.6%, respectively. Adult overweight and obesity have increased dramatically in Sub-Saharan Africa, reaching 41.7% in 2016.16 In contrast to European and American countries, there were large differences in the prevalence of overweight and obesity between the countries of the Eastern Mediterranean and Africa.17 The NCD-RisC estimated that Obesity would affect 18% of men and 21% of women by 2025.18 The incidence of overweight and obesity among men and women varies substantially within and between countries, and overall, more women are obese than men.19 The current study revealed that males and females had comparable obesity rates. Obesity among college students is caused by a variety of circumstances. College students are more likely to consume unhealthy foods such as fast food, processed meals, and sugary beverages. They are mostly physically inactive, anxious and sleep deprived, which can lead to poor eating habits.
We measured the student’s understanding of the obesity causes, diagnosis, complications, and prevention. The average amount of knowledge score was optimal (70.6%) and not surprisingly increased with age. Previous studies also showed similar outcomes.20 Knowledge increased slightly with increased body mass index, yet the difference was not statistically significant. While 91.2% of the participants considered obesity is a risk factor for type 2 diabetes, only 39.0% of them recognized Low-carbohydrate diets as helpful for obesity prevention. 53.1% were aware of BMI as measurement of obesity and 70.3% related obesity to bad Life style factors. A similar study conducted in China revealed that undergraduate students have a poor understanding of the general idea of obesity.21 These findings indicated that obese and normal-weight students had equivalent levels of knowledge, implying that there may be other factors than knowledge that account for obesity and overweight. This findings are in accordance with a recently reported study.22
We assessed the participants’ personal perceptions of obesity, such as dissatisfaction with their present body weight, concern about body form, and willingness to prevent obesity. The average attitude was also optimal (74.8%) within all age groups and BMI classes. The students have a good positive attitude towards preventing obesity in the study. The demonstrated attitude is proportional to their knowledge amount. In this study, 77.9% of our participants recognized obesity as a disease and 79.3% considered it as a serious health problem. Of the total participants, 28.3% considered themselves as obese while the actual prevalence among them was 15.5%. The majority of students stated that they were willing to control their weight in order to stay fit. However, this mentality was not shared by their practice. The average practice score was poor (36.7%) compared to the knowledge and attitude. There was a significant variation of the practice within the different age groups. Older students appeared to sustain more practice than younger ones. Practice questions included healthy eating, physical exercise, and obesity prevention measures. Although 90.0% declared that they care about body shape, only 27.4% mentioned that they care about your calories amount in the meals. Moreover, only 34.5% of the participants admitted that they exercise regularly. Out of the total participant, 24.4% admitted that they eat fast food at least every two days. Of the total participants, 44.6% admitted that electronic games are usually practiced during their free times.
There are currently few obesity teaching materials available to healthcare students in training programs around the world.23 To ensure that obese people receive the best care possible, it has been suggested that undergraduate healthcare education should provide more information about obesity.24 Students may be aware of nutritional requirements and the health repercussions of poor diet, but this is insufficient to develop and sustain healthy practices.25 However, healthy eating habit, aligned with the student’s own values such as self-governance, social justice, and peer group connection may be more efficacious.26
Students are subjected to heavy junk food marketing, which encourages overconsumption by instilling positive emotional associations with the junk food.27
It has been suggested that advocating for healthy eating is a smart method to stand up to the food industry’s deceptive and unethical food marketing practices. As a result, students’ connections with unhealthy food marketing were reduced, and their healthful choices were improved.27
Digital technology have the ability to influence the student’s behavior. Nearly all 16- to 24-year-olds in high-income countries own a smartphone,28 which can be an obvious mechanism of low-cost delivery of population-level dietary interventions for young people.
The effectiveness of digital interventions can lead to improved diet and physical activity patterns among students.29
Furthermore, students may be able to lose extra body weight by adding digital interventions into multicomponent school-based techniques.
Incorporating digital interventions within multicomponent school-based initiatives, along with changes to the school environment and curricula, family involvement, and health information provided by teachers, is suggested.30 However, research on interventions that improve the diet and weight status of young people from low-income families is limited. Individual knowledge and competencies are mediated by organizational structures and the availability of resources that enable people to access, comprehend, assess, and use information and services in ways that promote and sustain good health.31 European studies have uncovered that wellbeing education varies inside and between nations which nearly one in two individuals on normal have restricted wellbeing education.12 Practice is highly influenced by a person’s positive attitude which by itself is influenced by knowledge. In this study, Knowledge, attitude, and practice scores were interrelated. Uncourtly, greater knowledge leads to a better attitude, which leads to better practice.32 Furthermore, persons who have a better attitude and/or practice with a certain subject are more willing to pursue further knowledge.
Given the difficulty in treating obesity among students with typical weight-management programs, different tactics and motivators are likely to be required for this group.33 Students’ poor food habits are not due to a lack of knowledge. Behavioral weight-management programs are the first-line treatment for patients who are overweight or obese, although varied outcomes have been reported.34 This diversity in effectiveness could be attributed to differences in intervention content and format, including how long support is delivered.
The cross-sectional design of the study is the main limitation, despite the large sample size. Other limitations included the potential for participant recall bias and the influence of socially desirable features on their response. Moreover, the study did not include more demographical information such as geographical location and socioeconomic status.
Data Sharing Statement
The raw data used in this study are available from the corresponding author: Salah H. Elsafi. All data will be deidentified prior to sharing.
Ethics Approval and Consent to Participate
According to the principles of the Declaration of Helsinki, the Ethics Review Board of Prince Sultan Military College of Health Sciences approved this study (IRB-2023-CLS-028). Written informed consent was obtained from each participant.
Acknowledgments
The authors are grateful for the data collectors and the study participants.
Funding
This work received no grant.
Disclosure
The authors report no commercial or financial relationship that might be seen as creating a conflict of interest throughout the research’s conduct for this work.
References
1. World Health Organization. Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation. World Health Organization; 2000.
2. Chooi YC, Ding C, Magkos F. The epidemiology of obesity. Metabolism. 2019;92:6–10. doi:10.1016/j.metabol.2018.09.005
3. Althumiri NA, Basyouni MH, AlMousa N, et al. Obesity in Saudi Arabia in 2020: prevalence, distribution, and its current association with various health conditions. In: Healthcare. Vol. 2021. MDPI; 2021:311.
4. Mahmood TA, Arulkumaran S. Obesity: A Ticking Time Bomb for Reproductive Health. Newnes; 2012.
5. Agrawal P, Gupta K, Mishra V, Agrawal S. Effects of sedentary lifestyle and dietary habits on body mass index change among adult women in India: findings from a follow-up study. Ecol Food Nutr. 2013;52(5):387–406. doi:10.1080/03670244.2012.719346
6. Salem V, AlHusseini N, Abdul Razack HI, Naoum A, Sims OT, Alqahtani SA. Prevalence, risk factors, and interventions for obesity in Saudi Arabia: a systematic review. Obesity Rev. 2022;23(7):e13448. doi:10.1111/obr.13448
7. Syed NK, Syed MH, Meraya AM, et al. The association of dietary behaviors and practices with overweight and obesity parameters among Saudi university students. PLoS One. 2020;15(9):e0238458. doi:10.1371/journal.pone.0238458
8. Qiquan Z. The KAP theory. In: The Logic of China’s New School Reforms. Brill; 2021:38–50.
9. Adebayo RA, Balogun MO, Adedoyin RA, Obashoro-John OA, Bisiriyu LA, Abiodun OO. Prevalence and pattern of overweight and obesity in three rural communities in southwest Nigeria. Diabetes Metab Syndr Obes. 2014;153–158. doi:10.2147/DMSO.S55221
10. Alhazmi A, Aziz F, Hawash MM. Association of BMI, physical activity with academic performance among female students of Health Colleges of King Khalid University, Saudi Arabia. Int J Environ Res Public Health. 2021;18(20):10912. doi:10.3390/ijerph182010912
11. Boutari C, Mantzoros CS. A 2022 Update on the Epidemiology of Obesity and a Call to Action: As Its Twin COVID-19 Pandemic Appears to Be Receding, the Obesity and Dysmetabolism Pandemic Continues to Rage on. Vol. 133. Elsevier; 2022:155217.
12. World Health Organization. WHO European Regional Obesity Report 2022. World Health Organization. Regional Office for Europe; 2022.
13. Odoneb CSALA, van den Brandtd PA, Fernandezf E, et al. Prevalence and correlates of overweight and obesity in 12 European countries in; 2022.
14. Florentino RF. The burden of obesity in Asia: challenges in assessment, prevention and management. Asia Pac J Clin Nutr. 2002;11(s8):S676–S680. doi:10.1046/j.1440-6047.11.s8.4.x
15. Alagal RI, AlFaris NA, AlTamimi JZ, et al. Differences in overweight and obesity prevalence among young men from twelve middle eastern and Asian countries living in Saudi Arabia. In: Healthcare: 2022. MDPI; 2022:690.
16. World Health Organization. Obesity and Overweight—Key Facts. Geneva: World Health Organization; 2018.
17. Bovet P, Chiolero A, Gedeon J. Health effects of overweight and obesity in 195 countries. New Engl J Med. 2017;377(15):1495–1496.
18. Collaboration NRF. Trends in adult body-mass index in 200 countries from 1975 to 2014: a pooled analysis of 1698 population-based measurement studies with 19.2 million participants. Lancet. 2016;387(10026):1377–1396.
19. Kanter R, Caballero B. Global gender disparities in obesity: a review. Adv Nutr. 2012;3(4):491–498. doi:10.3945/an.112.002063
20. Sharif Ishak SIZ, Chin YS, Taib M, Nasir M, Chan YM. Effectiveness of a school-based intervention on knowledge, attitude and practice on healthy lifestyle and body composition in Malaysian adolescents. BMC Pediatric. 2020;20(1):1–12. doi:10.1186/s12887-020-02023-x
21. Xue B, Zhang X, Li T, et al. Knowledge, attitude, and practice of obesity among university students. Ann Palliat Med. 2021;10(4):4539–4546. doi:10.21037/apm-21-573
22. O’Brien G, Davies M. Nutrition knowledge and body mass index. Health Educ Res. 2007;22(4):571–575. doi:10.1093/her/cyl119
23. Mastrocola MR, Roque SS, Benning LV, Stanford FC. Obesity education in medical schools, residencies, and fellowships throughout the world: a systematic review. Int J Obesity. 2020;44(2):269–279. doi:10.1038/s41366-019-0453-6
24. Harvey E, Glenny A, Kirk S, Summerbell C. A systematic review of interventions to improve health professionals’ management of obesity. Int J Obesity. 1999;23(12):1213–1222. doi:10.1038/sj.ijo.0800932
25. Strömmer S, Shaw S, Jenner S, et al. How do we harness adolescent values in designing health behaviour change interventions? A qualitative study. Br J Health Psychol. 2021;26(4):1176–1193. doi:10.1111/bjhp.12526
26. Yeager DS, Bryan C. Harnessing adolescent values to motivate healthier eating-Bryan, Yeager et al; 2016.
27. Bryan CJ, Yeager DS, Hinojosa CP. A values-alignment intervention protects adolescents from the effects of food marketing. Nat Human Behav. 2019;3(6):596–603. doi:10.1038/s41562-019-0586-6
28. O’Dea S. UK: Smartphone Ownership by Age from 2012–2021. Statista; 2021.
29. Rose T, Barker M, Jacob CM, et al. A systematic review of digital interventions for improving the diet and physical activity behaviors of adolescents. J Adolesc Health. 2017;61(6):669–677. doi:10.1016/j.jadohealth.2017.05.024
30. Jacob CM, Hardy-Johnson PL, Inskip HM, et al. A systematic review and meta-analysis of school-based interventions with health education to reduce body mass index in adolescents aged 10 to 19 years. Int J Behav Nutr Phys Act. 2021;18:1–22. doi:10.1186/s12966-020-01065-9
31. World Health Organization. Health Promotion Glossary of Terms 2021. World Health Organization; 2021.
32. Launiala A. How much can a KAP survey tell us about people’s knowledge, attitudes and practices? Some observations from medical anthropology research on malaria in pregnancy in Malawi. Anthropol Matters. 2009;11(1):1.
33. Campbell K, Waters E, O’meara S, Kelly S, Summerbell C. Interventions for preventing obesity in children. Cochrane Database Syst Rev. 2002;2:CD001871.
34. Hartmann‐Boyce J, Johns DJ, Jebb S, Summerbell C, Aveyard P; Group BWMR. Behavioural weight management programmes for adults assessed by trials conducted in everyday contexts: systematic review and meta‐analysis. Obesity Rev. 2014;15(11):920–932. doi:10.1111/obr.12220
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Physicians’ Knowledge and Practices Regarding Asthma: A Cross-Sectional Study in Saudi Arabia
Dairi MS
International Journal of General Medicine 2022, 15:6671-6680
Published Date: 19 August 2022
Attitude, Practice, and Knowledge Regarding Fluoridated Toothpaste, Brushing, and Rinse Usage Among Residents of Jeddah City in Saudi Arabia
Al-Zain AO, Fakhry LM, Tallab RA, Natto ZS
Patient Preference and Adherence 2023, 17:23-39
Published Date: 5 January 2023
Dermatologists’ Knowledge, Attitude, and Practice Pattern Toward Low-Dose Oral Minoxidil in Hair Loss in Saudi Arabia
Altalhab S
Clinical, Cosmetic and Investigational Dermatology 2024, 17:653-662
Published Date: 15 March 2024
Knowledge, Attitude and Practice Toward Artificial Intelligence Among Healthcare Workers in Private Polyclinics in Jeddah, Saudi Arabia
Serbaya SH, Khan AA, Surbaya SH, Alzahrani SM
Advances in Medical Education and Practice 2024, 15:269-280
Published Date: 5 April 2024
Knowledge, Attitude and Practice Towards Hepatitis B Infection and HBV Vaccine Among the Healthy Population in Makkah, Saudi Arabia
Almalki F, Alraffah YM, Alasiri RA, Dhafar MW, Albogami FM, Alhazmi MN, Alyazidi AM, Alharbi LA, Alotaibi ME
Infection and Drug Resistance 2025, 18:2153-2164
Published Date: 28 April 2025