Back to Journals » Drug Design, Development and Therapy » Volume 20
Obesity Reduces the Median Effective Dose of Remimazolam in Aged 6–18 Pediatric Patients for Procedural Sedation
Authors Liu TT, Chen J, Jin X, Yang ZS, Yu XQ, Xiao F ![]() , Huang XD
, Huang XD
Received 20 March 2026
Accepted for publication 2 June 2026
Published 8 June 2026 Volume 2026:20 610851
DOI https://doi.org/10.2147/DDDT.S610851
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Solomon Tadesse Zeleke
Tian-Tian Liu,1 Junyan Chen,1 Xiao Jin,1 Zhong-Sai Yang,1 Xu-Qi Yu,1 Fei Xiao,1 Xiao-Dong Huang2
1Department of Anesthesiology, the Affiliated Women and Children’s Hospital of Ningbo University, Ningbo City, Zhejiang Province, People’s Republic of China; 2Department of Anesthesiology, Hangzhou Women’s Hospital (Hangzhou Maternity and Child Health Care Hospital), Hangzhou City, Zhejiang Province, People’s Republic of China
Correspondence: Fei Xiao, Department of Anesthesiology, the Affiliated Women and Children’s Hospital of Ningbo University, Ningbo City, Zhejiang Province, People’s Republic of China, Tel +86 574 83887041, Email [email protected] Xiao-Dong Huang, Department of Anesthesiology, Hangzhou Women’s Hospital (Hangzhou Maternity and Child Health Care Hospital), Hangzhou City, Zhejiang Province, People’s Republic of China, Tel +86 571 56005077, Email [email protected]
Background: Remimazolam, a relatively newly developed ultrashort-acting benzodiazepine agent, is utilized for procedural sedation and general anesthesia, and was recently widely used in school-aged pediatric patients. However, few data could be available in obese pediatric patients. We compared the median effective dose (ED50) of remimazolam for procedural sedation in pediatric obese and normal weight patients based on the hypothesis that obese pediatric patients require a lower dose per body weight.
Methods: Sixty pediatric patients were enrolled and allocated into the normal weight group (Group N) and the obese group (Group O). For the first pediatric patient, remimazolam was administered at an initial dose of 0.2 mg/kg. Subsequent doses were adjusted in increments of ± 0.02 mg/kg, with an increase if the preceding dose was ineffective or a decrease if it achieved the desired effect, following a sequential up-and-down design. ED50 was estimated and compared using this approach.
Results: The ED50 of remimazolam was significantly lower in Group O 0.17 mg/kg (95% CI: 0.14– 0.19 mg/kg) than in Group N 0.23 mg/kg (95% CI: 0.19– 0.24 mg/kg) (P < 0.001). The estimated relative median potency was 0.74 (95% CI: 0.41– 0.91) via probit analysis.
Conclusion: In summary, when administered in combination with remifentanil at a dosage of 2 μg/kg, the ED50 value for inducing sedation with remimazolam is reduced by approximately 26% in obese paediatric patients compared to normal-weight children.
Keywords: obesity, pediatric, remimazolam, sedation, ED50
Introduction
Remimazolam, a newly developed ultrashort-acting benzodiazepine agent, is utilized for procedural sedation and general anesthesia. It is characterized by a rapid onset and quick recovery, is metabolized independently of hepatic and renal function, shows no cumulative effects, causes minimal interference with the respiratory and cardiovascular systems, and can be effectively reversed by flumazenil, thereby providing excellent controllability.1,2 The rapid onset of effects, coupled with a relatively fast recovery, may offer advantages when applied for procedural sedation in pediatric patients. The safety, effectiveness, and pharmacokinetic profile of remimazolam used for intravenous sedation in school-aged pediatric patients have been well established and assessed.3–6 However, few data could be available in obese pediatric patients.
Obesity has emerged as a global issue, carrying significant social, economic, and public health consequences.7 Obese children demonstrate a higher proportion of body fat and a lower proportion of lean mass compared to their normal-weight peers. The manner in which a drug distributes between adipose and lean tissues can significantly affect its pharmacokinetic behavior in obese individuals, making appropriate dosage adjustment in this population a crucial clinical consideration. Research indicates a significant disparity in the correlation between drug dosage and therapeutic efficacy when comparing obese individuals with those of normal body weight.8
Based on the aforementioned considerations, it is necessary to clarify the dose–response relationship of remimazolam in obese children to provide a foundation for the safe clinical application of the drug. Thus, this study explores the impact of obesity on the effective dosage of remimazolam when it is used in combination with remifentanil for procedural sedation in children undergoing circumcision. We compared the median effective dose (ED50) of remimazolam for procedural sedation in pediatric obese and non-obese patients based on the hypothesis that obese pediatric patients require a lower dose per body weight.
Materials and Methods
Ethics
We obtained ethical approval from the Ethics Committee of the Affiliated Women’s and Children’s Hospital of Ningbo University (Approval No. NBFE-2025-KY-155) and registered this clinical trial in the Chinese Clinical Trial Registry https://www.chictr.org.cn (ChiCTR2500110458) on October 14, 2025. This study was initiated on October 31, 2025, and completed on January 31, 2026. All patients’ parents signed the written informed consent before enrollment. This study was carried out following the principles of the Declaration of Helsinki.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: (1) American Society of Anesthesiologists (ASA) physical status classification of Class I - II; (2) Patients aged 6 to 18 years; (3) Body Mass Index (BMI) less than or equal to 35 kg/m2; (4) Scheduled for pediatric circumcision receive penile dorsal nerve block under sedation. The exclusion criteria were as follows: (1) Contraindications for penile dorsal nerve block puncture; (2) Complicated by severe congenital medical diseases, including tetralogy of fallot, Down Syndrome et al; (3) History of epilepsy or other psychiatric disorders; (4) Preoperative administration of sedatives; (5) Allergy to remimazolam or other benzodiazepines; (6) Patients declined to participate in the study.
Grouping and Blinding
The pediatric patients were stratified into two groups according to their BMI: the normal weight group (Group N) and the obese group (Group O). The criteria of obese for pediatric patients was according to the “Screening for Overweight and Obesity among School-age Children and Adolescents in China” (WS/T 586–2018, see Supplementary Table 1 and https://www.nhc.gov.cn/fzs/c100048/201803/a41a66b9022b46cfb1662ee949224307/files/1733125465236_97973.pdf). The study medications were prepared by a single investigator (F.X)., who rigorously adhered to the study protocol under sterile conditions. At the commencement of each procedure, F.X. independently ascertained and administered the initial remimazolam dosage, and remained the only individual aware of the allocated treatment level. Two other investigators (T.L. and J.C.) administered anesthesia, collected data. The researchers evaluated the therapeutic efficacy of the administered dose, determining it to be either effective or ineffective, and communicated this assessment to F.X., who subsequently selected the dosage for the next case. Throughout the entire study, investigators T.L. and J.C. were kept unaware of the participants’ dose allocations.
Anesthesia Procedure
All pediatric patients did not receive premedication and were routinely required to fast for 8 hours for solid food and 2 hours for clear liquids before surgery. Peripheral venous access was created via 22-guage cannula under topical anesthesia using lidocaine cream. Routine monitoring, upon entry into the operating room, included non-invasive blood pressure, heart rate, electrocardiogram (ECG), and pulse oximetry. Prior to the induction of general anesthesia, the patient was administered oxygen via a mask at a flow rate of 8 L/min. Three minutes later, remifentanil was slowly administered to the patient at a dose of 2µg/kg. One minute after the administration of remifentanil, the pre-prepared study drug remimazolam was slowly administered to the patient. Subsequently, the Modified Observer’s Assessment of Alertness and Sedation (MOAA/S) score was utilized to assess sedation levels as follows: 5 = The patient is fully alert and responds immediately when called by name; 4 = The patient responds slowly or with a delay upon hearing their name; 3 = The patient responds only after multiple, forceful verbal calls of their name; 2 = The patient responds only to mild physical stimuli, such as gentle shaking or light pushing; 1 = The patient responds exclusively to painful stimulation (eg., trapezius muscle squeeze); 0 = No observable response, even to painful stimulation (eg., trapezius muscle squeeze). Once the patient’s MOAA/S score was ≤1, the penile dorsal nerve block was initiated.
Up-and-Down Allocation
Based on the reports of prior studies9–11 and the preliminary trial results of this study, the initial dose of remimazolam for the first pediatric patient was set at 0.2 mg/kg, with adjacent dose increments or decrements of 0.02 mg/kg. The dosage for the next patient was determined based on the previous patient’s response (effective or ineffective) through the application of the up-and-down allocation technique.12,13 For instance, if the dose was effective, the dose for the next patient was decreased by 0.02 mg/kg; conversely, if the dose was ineffective, the dose for the next patient was increased by 0.02 mg/kg. An effective dose was defined as an MOAA/S score of less than 2 points 1 minutes following the administration of sedation medications. Additionally, during nerve block, there should be no body movement or only slight movement that does not interfere with the anesthesiologist’s operation. Otherwise, it was regarded as an ineffective dose.
Remedial Measure
If the dose is deemed to be an ineffective dose, the patients will receive an additional dose of 0.1 mg/kg remimazolam as a remedial measure. If, one minute after the additional dose, the MOAA/S ≥2 or body movement during the anesthesiologist’s operation, an additional dose of 1 mg/kg propofol may be appropriately administered (repeated if necessarily) immediately to complete the dorsal penile nerve block procedure.
Complications Management
We commenced hypoxic intervention when the oxygen saturation showed a gradual decrease. If a oxygen saturation (SpO2) level of 92% or lower is observed during the procedure, the oxygen flow rate should be immediately increased. Additionally, at the anesthesiologist’s discretion, the airway should be opened by lifting the mandible, or pressure respiration should be administered via a face mask. Hypotension was defined as a reduction of 20% or more in systolic blood pressure (SBP) from the baseline value, and it was managed with intravenous norepinephrine at a dosage ranging from 0.02 to 0.1 µg/kg. Hypertension was defined as an elevation of 20% or more in SBP relative to the baseline value, and it was treated with intravenous Urapidil at a dosage ranging from 0.2 to 0.5 mg/kg. Bradycardia was defined as heart rate (HR) decreased to less than 60 bpm, and it was treated by atropine 0.01 mg/kg.
Data Collection and Outcome Assessment
The primary outcome of this study was the effective or ineffective dose of remimazolam. Secondary outcomes were recorded as follows: the onset time of procedural sedation (the period from the administration of sedative drugs to the initiation of dorsal penile nerve block), the awakening time (from the completion of the last dose administration to the time when the patient responded to a verbal command to open the eyes), the amount of rescued propofol, and adverse reactions during the study period, including injection pain, hypoxemia, hypotension, hiccups, nausea, and vomiting. The mean artery pressure (MAP), SpO2, and HR were recorded at the following time points: T0, representing baseline values; T1, one minute after the intravenous administration of remifentanil; T2, one minute after the intravenous administration of remimazolam; T3, after dorsal penile nerve block; T4, at the commencement of the surgical procedure.
Sample Size
The sample size was determined to be 30 participants per group, in accordance with methodological guidelines which suggest that a range of 20 to 40 participants per group guarantees a reliable and robust estimation of the ED50 when the Dixon up-down procedure is applied.12,14 Moreover, our initial pilot study results suggested that enrolling at least 23 participants per group would provide a statistical power of 90% or higher to identify a 20% disparity in the ED50 of remimazolam across groups, assuming a significance threshold (α) of 0.05. To account for possible participant attrition (anticipated at 20%) and to improve the precision of estimates, which is reflected in narrower confidence intervals, the study recruited a total of 60 participants, with an equal allocation (n = 30 per group).
Statistical Analysis
We used visual examination and Kolmogorov–Smirnov test to assess the normality of continuous variables. For continuous variables, normally distributed data are reported as mean ± standard deviation (SD), and analyzed with Students’ t-test between the two groups; whereas non-normally distributed data are expressed as median [interquartile range, IQR] and analyzed with Mann–Whitney U-test. For categorical variables, data are expressed as the number (percentage), and analyzed using the Chi-square test or Fisher’s exact test appropriate.
The ED50 values for remimazolam were estimated by employing a modified up-and- down sequential allocation design. Specifically, the ED50 was calculated as the average of the midpoints between consecutive doses at which pediatric sedation transitioned from ineffective to effective or from effective to ineffective, that is, at each crossover point. The 95% confidence intervals (CIs) and standard errors associated with the ED50 values were calculated following Choi’s methodology.13 To ascertain whether the ED50 values exhibited a significant difference between the two groups, we utilized the 83% confidence interval (CI) overlap criterion. Non-overlapping intervals were regarded as evidence of a statistically significant difference (P < 0.05). As an additional measure for ensuring robustness, we carried out probit regression and estimated the relative median potency ratio through Fieller’s method. Statistical analyses were performed using GraphPad Prism 8.0 (GraphPad Software, San Diego, CA, USA), IBM SPSS Statistics for Windows (v22.0; IBM Corp., Armonk, NY, USA), and the R programming language (R Core Team, 2023) with the ED50 simulation package (v0.1.1). Statistical significance was defined as P < 0.05.
Results
Sixty-five patients were enrolled and assessed for eligibility. One patient was excluded for not meeting the inclusion criteria, and four patients refused to participate. The analysis incorporated the remaining 60 participants, who were stratified into two cohorts—Group N and Group O—with each cohort consisting of 30 individuals, based on their BMI. The Consolidated Standards of Reporting Trials (CONSORT) diagram, as shown in Figure 1, demonstrates the study flow. No statistically significant differences were detected between Group N and Group O in terms of age, height, American Society of Anesthesiologists (ASA) physical status classification, or baseline vital signs (Table 1). There were significant differences in the BMI and weight between the two groups (both P values <0.0001), Table 1.
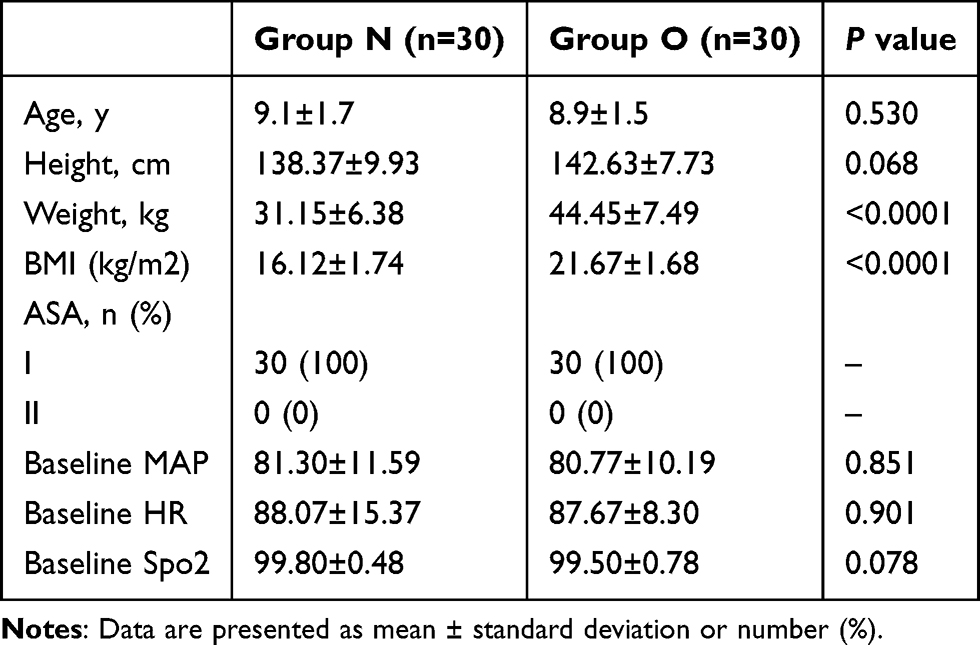 |
Table 1 Patient Characteristics |
 |
Figure 1 CONSORT diagram of patient recruitment. CONSORT indicates Consolidated Standards of Reporting Trials. |
The sequential outcomes observed in relation to the sedative dosage of remimazolam are depicted in the up-down titration patterns shown in Figure 2. The ED50 of remimazolam was significantly lower in Group O (0.17 mg/kg; 95% CI: [0.14–0.19] mg/kg) than in Group N (0.23 mg/kg; 95% CI: [0.19–0.24] mg/kg) (P < 0.001). There was no overlap between 83% CI between the two groups (0.16–0.17 vs. 0.21–0.22), showed no significant difference. Using probit regression, the ED50 of remimazolam required for procedural sedation were 0.16 mg/kg (95% CI, 0.15–0.17 mg/kg) for Group O and 0.22 mg/kg (95% CI, 0.21–0.24 mg/kg) for Group N, respectively. The relative median potency of remimazolam in Group O, compared to Group N, was estimated at 0.74 (95% CI: 0.41–0.91), indicating a statistically significant difference. The ED95 were 0.20 mg/kg (95% CI, 0.18–0.23 mg/kg) for Group O and 0.26 mg/kg (95% CI, 0.25–0.32 mg/kg) for Group N, respectively. The dose-response relationships derived from probit regression modeling are presented in Figure 3.
 |
Figure 2 Individual responses to remimazolam at corresponding dose in Group N and Group O. The ED50 of remimazolam was 0.17 mg/kg (95% CI: 0.14–0.19) mg/kg in Group O and 0.23 mg/kg (95% CI: 0.19–0.24) mg/kg in Group N, respectively. ED50, effective dose in 50% of patients. The solid circles represent effective doses and open circles represent ineffective doses. |
 |
Figure 3 The dose-response relationships derived from probit regression modeling. |
Side effects, incidence of rescued propofol, and onset time of sedation, and awakening time are summarized in Table 2. No significant difference was observed between the two groups. The MAP, SpO2, and HR at different time points are depicted in Figure 4. There was a significant difference between the groups in terms of HR and SpO2 at the 1-minute time point after remimazolam administration.
 |
Table 2 Incidence of Adverse Effects and Patients Required Rescued Propofol, and Time Duration |
 |
Figure 4 The MAP, SpO2, and HR at different time points. T0, representing baseline values; T1, one minute after the intravenous administration of remifentanil; T2, one minute after the intravenous administration of remimazolam; T3, after dorsal penile nerve block; T4, at the commencement of the surgical procedure. |
Discussion
The main finding of this study is that the ED50 values of remimazolam for procedural sedation during dorsal penile nerve block are 0.17 mg/kg and 0.23 mg/kg for obese and normal-weight pediatric patients, respectively. Our data suggests that, when compared with normal-weight pediatric patients, the dose of remimazolam for procedure sedation in obese pediatric patients would be reduced by approximately 26% according to per body weight.
Obesity has an impact on both pharmacokinetics and pharmacodynamics. Dong et al15 reported a 37.9%–38.6% decrease in the 50% of median effective concentration in morbidly obese patients and suggested an increased sensitivity to propofol in morbidly patients. Our data also demonstrated a 26% reduction in the remimazolam dose for obese pediatric patients when compared with normal-weight ones, which is consistent with the study by Dong et al The associations of adipose tissue, lean body weight (LBW), extracellular fluid, and cardiac output with obese patients could serve as reasonable explanations for the pharmacokinetic changes in these studies.16 For instance, obesity results in an increased central volume of distribution and altered drug clearance, both of which have an impact on remimazolam plasma levels. Furthermore, it might change pharmacodynamic parameters, such as the concentration that produces 50% of the maximal effect (EC50) and the rate constant that governs the equilibration between plasma and the effect site.16
Drawing comprehensive conclusions about pharmacokinetic variations between obese and non-obese pediatric populations remains a challenging task, mainly because of the limited number of clinical studies enrolling children with obesity. In pediatric patients with obesity, the volume of distribution, normalized to total body weight (TBW) per kilogram, tends to be higher for lipophilic agents and lower for hydrophilic compounds compared to their counterparts with normal weight. Administering highly hydrophilic drugs—or agents with exceptionally short elimination half-lives, such as remimazolam and remifentanil—based on total body weight often results in higher plasma drug levels in children with obesity compared to their peers of healthy weight. Due to competitive binding of free fatty acids in plasma, these agents quickly accumulate to high concentrations within their active compartments, thereby increasing the risk of adverse effects—such as profound analgesia, pronounced sedation, and suppression of respiratory and cardiovascular functions. For this purpose, LBW was commonly employed to adjust the actual body weight in order to prevent the overdose of anesthetic calculated based on TBW and, consequently, to avoid the side-effects associated with the dose. For example, Chen et al17 used remimazolam in combination with sufentanil (0.5 µg/kg) for general anesthesia induction in obese patients. They determined that the ED50 and ED95 values of remimazolam (using LBW) were 0.115 mg/kg and 0.179 mg/kg in adults, respectively. However, calculating the LBW is not an especially easy task and may lead to errors in calculation, which can subsequently result in dosing errors. Therefore, directly determining the appropriate dose based on weight for obese pediatric patients is convenient for clinical practice.
Although limited data may be available regarding the ideal dose of remimazolam for obese pediatric patients during procedural sedation, it should be noted that the ED95 of remimazolam, determined to be 0.20 mg/kg in this study, is derived from probit analysis. There is a lack of direct observation at this dose in this context. And further studies are warranted in this area.
Obesity—especially among children and adolescents—has emerged as a major public health challenge. Data from the 2011–2012 U.S. National Health and Nutrition Examination Survey (NHANES) indicate that approximately 16.9% of individuals aged 2 to 19 years met the clinical criteria for obesity.18 As studies have recommended that the definitions or classifications of overweight and obesity for children should be in line with the actual conditions of the local population,7 we defined obesity in accordance with the recommendations of the “Guidelines for the Assessment, Treatment and Prevention of Childhood Obesity in China” in this study. Although this study is limited by region and ethnicity, any advancement in obesity-related anesthesia contributes to clinical practice to a certain extent.
Regarding safety, the findings from a study of adverse event reports in the FAERS database suggest that remimazolam shows a significant signal for hypoventilation. In the cardiovascular system, it was linked to severe adverse events, such as cardiac and cardiorespiratory arrest, especially among high-risk patients. Furthermore, severe allergic reactions, such as anaphylactic shock and laryngeal oedema, have been documented.19 Our study indicates that patients experienced transient decreases in mean arterial pressure, heart rate, and SpO2 following remimazolam administration. The incidence of adverse effects, including vomiting, hypotension, injection pain and hiccups, was rare, and the majority of the reported symptoms were mild in severity and of short duration. Twelve patients experienced hypoxemia (SpO2 ≤ 92%), and eight of these patients belonged to the obese cohort. This finding suggests that obese pediatric patients face a higher risk of respiratory obstruction, despite the lack of a significant difference between the two groups. It is difficult to explain the reason for the 1-minute decrease in heart rate after the administration of remimazolam. Perhaps, the transient lack of oxygen offers a plausible explanation for the reduction in heart rate.
We acknowledge some limitations in this study. First, the modified sequential method serves as a convenient approach for calculating the 50% effective drug doses (ED), but the current findings offer an inadequate estimation for ED95. Second, when remifentanil is combined with remimazolam, 2 μg/kg of remifentanil was used in this study; however, the optimal combination ratio remains undetermined. Different institutions may use different dosages of remifentanil, which will result in different appropriate doses of remimazolam. Therefore, the universality of this study will be somewhat affected.
In summary, when administered in combination with remifentanil at a dosage of 2 μg/kg, the ED50 value for inducing sedation with remimazolam is reduced by approximately 26% in obese paediatric patients compared to normal-weight children. Further research should focus on the correlation between adjusted weight-based administration methods and the lean body weight-based approaches.
Abbreviations
ED50, Median effective dose; ASA, American Society of Anesthesiologists; BMI, Body Mass Index.
Data Sharing Statement
Data related to this study can be obtained by contacting the corresponding author (Fei Xiao) if reasonable.
Ethics Approval and Consent to Participate
The Ethics Committee of the Affiliated Women’s and Children’s Hospital of Ningbo University (Approval No. NBFE-2025-KY-155) approved this study. All patients involved in this study were informed and all of them signed a written informed consent.
Funding
This work was supported by the Project of NINGBO Leading Medical & Health Discipline, Project Number: 2026-A35.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Worthington MT, Antonik LJ, Goldwater DR, et al. A phase Ib, dose-finding study of multiple doses of remimazolam (CNS 7056) in volunteers undergoing colonoscopy. Anesthesia Analgesia. 2013;117(5):1093–9. doi:10.1213/ANE.0b013e3182a705ae
2. Wiltshire HR, Kilpatrick GJ, Tilbrook GS, Borkett KM. A placebo- and midazolam-controlled phase i single ascending-dose study evaluating the safety, pharmacokinetics, and pharmacodynamics of remimazolam (CNS 7056): part II. population pharmacokinetic and pharmacodynamic modeling and simulation. Anesthesia Analgesia. 2012;115(2):284–296. doi:10.1213/ANE.0b013e318241f68a
3. Kamata K, Asagi S, Shimoda Y, et al. Successful recording of direct cortical motor-evoked potential from a pediatric patient under remimazolam anesthesia: a case report. JA Clin Rep. 2022;8(1):66. doi:10.1186/s40981-022-00555-y
4. Scheckenbach V, Fideler F. Optimizing Pediatric Sedation: evaluating Remimazolam and Dexmedetomidine for Safety and Efficacy in Clinical Practice. Pediatr Drugs. 2025;27(2):181–189. doi:10.1007/s40272-024-00659-1
5. Pieri M, D’Andria Ursoleo J, Di Prima AL, et al. Remimazolam for anesthesia and sedation in pediatric patients: a scoping review. J Anesth. 2024;38(5):692–710. doi:10.1007/s00540-024-03358-w
6. Kendrick JG, Carr RR, Ensom MHH. Pharmacokinetics and drug dosing in obese children. J Pediatric Pharmacol Therap. 2010;15(2):94–109. doi:10.5863/1551-6776-15.2.94
7. Phelps NH, Singleton RK, Zhou B, et al. Worldwide trends in underweight and obesity from 1990 to 2022: a pooled analysis of 3663 population-representative studies with 222 million children, adolescents, and adults. The Lancet. 2024;403(10431):1027–1050. doi:10.1016/S0140-6736(23)02750-2
8. Van Rongen A, Vaughns JD, Moorthy GS, Barrett JS, Knibbe CAJ, Van Den Anker JN. Population pharmacokinetics of midazolam and its metabolites in overweight and obese adolescents. Brit J Clinical Pharma. 2015;80(5):1185–1196. doi:10.1111/bcp.12693
9. Shi X, Yi F, Xiao H, et al. Low-dose alfentanil effectively reduces the ED50 of remimazolam for loss of consciousness in pediatric patients undergoing general anesthesia: a study using up-and-down sequential allocation method. DDDT. 2025;19:7459–7466. doi:10.2147/DDDT.S532565
10. Jin M, Lin H, Qiu L, Xu H, Zhang H, Hou S. Remimazolam for successful sedation in children with left-to-right shunt congenital heart disease: an up-and-down sequential allocation trial. Eur J Anaesthesiol. 2025;42(8):697–703. doi:10.1097/EJA.0000000000002183
11. Chae D, Kim HC, Song Y, Choi YS, Han DW. Pharmacodynamic analysis of intravenous bolus remimazolam for loss of consciousness in patients undergoing general anaesthesia: a randomised, prospective, double-blind study. Br J Anaesthesia. 2022;129(1):49–57. doi:10.1016/j.bja.2022.02.040
12. Pace NL, Stylianou MP, Warltier DC. Advances in and limitations of up-and-down methodology: a Précis of clinical use, study design, and dose estimation in anesthesia research. Anesthesiology. 2007;107(1):144–152. doi:10.1097/01.anes.0000267514.42592.2a
13. Choi SC. Interval estimation of the LD50 based on an up-and-down experiment. Biometrics. 1990;46(2):485–492. doi:10.2307/2531453
14. Stylianou MP. Sequential Analysis of Durham and Flournoy’s Biased Coin Design for Phase I Clinical Trials. American University; 2000.
15. Dong D, Peng X, Liu J, Qian H, Li J, Wu B. Morbid obesity alters both pharmacokinetics and pharmacodynamics of propofol: dosing recommendation for anesthesia induction. Drug Metabolism Disposition. 2016;44(10):1579–1583. doi:10.1124/dmd.116.071605
16. Kim TK. Obesity and anesthetic pharmacology: simulation of target-controlled infusion models of propofol and remifentanil. Korean J Anesthesiol. 2021;74(6):478–487. doi:10.4097/kja.21345
17. Chen M, Wang H, Sun J, et al. The dose of remimazolam combined with sufentanil for the induction of general anesthesia in obese patients undergoing bariatric surgery: an up-and-down sequential allocation trial. Front Pharmacol. 2024;15:1411856. doi:10.3389/fphar.2024.1411856
18. Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of Childhood and Adult Obesity in the United States, 2011-2012. JAMA. 2014;311(8):806. doi:10.1001/jama.2014.732
19. Ye G, Ding L, Zhou Q. Remimazolam’s clinical application and safety: a signal detection analysis based on FAERS data and literature support. PLoS One. 2025;20(8):e0330769. doi:10.1371/journal.pone.0330769
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Safety of Different Doses of Remimazolam Tosilate Applied in Upper Gastrointestinal Endoscopy: A Prospective Randomized Controlled Double-Blind Trial

Cui X, Cheng Z, Li H, Zhang X, Luan H, Zhao Z, Zhu P
Drug Design, Development and Therapy 2023, 17:2889-2896
Published Date: 20 September 2023
Comparing Remimazolam and Propofol for Postoperative Anesthesia Satisfaction in Outpatient Gynecological Surgery: A Randomized Clinical Trial
Wang XL, Dai LL, Li YN, Zhang JW, Qu MC, Zhou YY, Xing N
Drug Design, Development and Therapy 2024, 18:4615-4627
Published Date: 18 October 2024
Effect-Site Concentration of Remimazolam by Age Groups During Target-Controlled Infusion for Total Intravenous Anesthesia: A Retrospective Comparative Study
Park J, Seo KH, Kwak J, Baek H
Drug Design, Development and Therapy 2024, 18:5149-5159
Published Date: 12 November 2024
Effect of Remimazolam vs Midazolam on Early Postoperative Cognitive Recovery in Elderly Patients Undergoing Dental Extraction: A Prospective Randomized Controlled Study
Liu B, Wang P, Liang L, Zhu W, Zhang H
Drug Design, Development and Therapy 2024, 18:5895-5904
Published Date: 9 December 2024
Alfentanil Enhanced the Sedation of Remimazolam During Anaesthesia Induction in Patients Undergoing Urological Day Surgery: A Randomised Controlled Trial
Lin Y, Chen Q, Liao Y, Xu B, Zhang C, Luo J, Liu S, Wu X, Guan X
Drug Design, Development and Therapy 2025, 19:5653-5662
Published Date: 3 July 2025