Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Nutritional Support Strategies for Refeeding Syndrome in ICU Patients: A Review of Current Evidence
Authors Tang H, Chen Y, Li B ![]() , Yuan L, Sun R
, Yuan L, Sun R
Received 29 January 2026
Accepted for publication 22 May 2026
Published 24 June 2026 Volume 2026:19 599708
DOI https://doi.org/10.2147/JMDH.S599708
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ferry Efendi
Huixian Tang,1,* Yongjun Chen,1,* Bo Li,1 Liping Yuan,2 Ruixiang Sun2
1Graduate School of Wannan Medical College, Wuhu, Anhui, 241002, People’s Republic of China; 2Department of Critical Care Medicine, Yijishan Hospital of Wannan Medical College, Wuhu, Anhui, 241001, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ruixiang Sun, The Affiliated Yijishan Hospital of Wannan Medical College, Wuhu, Anhui, 241000, People’s Republic of China, +86 19955353952, Email [email protected] Liping Yuan, The Affiliated Yijishan Hospital of Wannan Medical College, Wuhu, Anhui, 241000, People’s Republic of China, Tel +86-13855377237, Email [email protected]
Objective: This study employed an evidence-based approach to synthesize and integrate relevant evidence regarding early nutritional support for patients with ICU refeeding syndrome, identifying clinically applicable nutritional support strategies to provide a reference for early nutritional management in such patients.
Methods: Based on the “ 6S” pyramid evidence hierarchy model, systematic searches were conducted in core domestic and international databases for guidelines, expert consensus documents, high-quality randomized controlled trials (RCTs), systematic reviews, and evidence summaries related to early nutritional support for ICU refeeding syndrome patients, with the search period spanning from database establishment to December 25,2025.
Results: A total of 16 publications were included, comprising 3 guidelines, 2 clinical decision-making documents, 4 systematic reviews, 2 cohort studies, 1 RCT, and 4 expert consensus documents. The evidence was systematically organized into 24 key evidence-based recommendations covering five aspects: multidisciplinary team collaboration, timing of nutritional assessment, indications for initiating and terminating nutritional support, specific nutritional interventions, and health education.
Conclusion: The evidence framework developed in this study provides a standardized reference for early nutritional management of ICU refeeding syndrome patients, addressing the lack of unified clinical guidelines and holding significant implications for reducing complication risks and improving patient outcomes.
Keywords: intensive care unit, ICU, refeeding syndrome, nutritional support, evidence review, evidence-based nursing
Introduction
Nutritional support, as one of the critical interventions in the management of critically ill patients, effectively provides the body with essential energy and nutrients, maintains organ function, and promotes immune repair, serving as a pivotal approach to improving nutritional status and clinical outcomes in ICU patients.1 However, due to factors such as disease spectrum and clinical treatment requirements, some critically ill patients may develop refeeding syndrome (RFS) during treatment—a metabolic disorder occurring when enteral or parenteral nutrition is reintroduced after prolonged starvation or malnutrition.2 Clinical manifestations include electrolyte disturbances, abnormal glucose and lipid metabolism, deficiencies in thiamine and other trace elements, and other systemic symptoms;3 severe cases may lead to multiple organ dysfunction syndrome and mortality. Current studies indicate4 that the incidence of RFS among ICU patients during nutritional support ranges from 30% to 59%, with a mortality rate as high as 33.9% within six months, posing a significant threat to patient survival. Existing research confirms that RFS is closely associated with energy metabolism imbalance and malnutrition resulting from impaired absorption function, making targeted nutritional interventions a key therapeutic measure.5 Therefore, developing a safe and effective nutritional support protocol, along with interventions such as electrolyte correction and supplementation of essential nutrients, constitutes the core strategy for managing RFS and holds substantial practical significance for enhancing the quality of critical care nutrition.6 Current research on ICU refeeding syndrome (RFS) both domestically and internationally primarily focuses on its epidemiological incidence, risk factors, and early identification.7,8 However, most studies are limited to current status analyses and risk screening, with insufficient emphasis on early clinical intervention strategies. Moreover, a unified nutritional support protocol and comprehensive management system have yet to be established. Therefore, a scientific, systematic, standardized, and effective nutritional support strategy is of critical importance for patients developing RFS. This study aims to systematically synthesize evidence-based findings on ICU RFS, summarize effective early nutritional support strategies, and establish a standardized clinical management framework to provide evidence-based guidance for critical care clinical nutrition practice.
Materials and Methods
Defining the Evidence-Based Question
The study was designed based on the PICOS principles to establish well-defined evidence-based questions. The study population (P) consisted of adult patients in the ICU who developed refeeding syndrome; the intervention (I) involved nutritional support measures for refeeding syndrome in the ICU; the control (C) comprised conventional measures or a blank control; the outcomes (O) included key indicators such as the incidence of refeeding syndrome, nutritional status, and the prevalence of metabolic disturbances; and the study types (S) encompassed guidelines, randomized controlled trials (RCTs), clinical decision-making, expert consensus, systematic reviews, meta-analyses, and evidence summaries. The study has been registered with the Fudan University Evidence-Based Nursing Center under project registration number ES20259574.
Retrieval Strategy
This study adopts the “6S” pyramid model of evidence resources and follows a top-down order in evidence retrieval. It systematically searches core domestic and international databases, professional organization websites, and Chinese and English guideline websites, such as the U.S. National Guideline Clearinghouse (NGC), the UK National Institute for Health and Care Excellence (NICE) guideline database, databases including PubMed, Web of Science, MedSci, UpToDate, BMJ Best Practice, YimaiTong guideline website, CNKI, and Wanfang, among others. A combination of subject terms and free terms is used.The Chinese search terms are “Intensive Care Unit/ICU/critically ill patients/severely ill patients”,
Refeeding syndrome/hypophosphatemia/nutrition support/nutrition intervention/enteral and parenteral nutrition/feeding intolerance/electrolyte disorders/metabolic disorders
“guidelines/expert consensus/evidence summary/systematic review/randomized controlled trial/best practice”.The English Search term is”Intensive Care Unit/ICU/critical care unit/critically ill”refeeding syndrome/hypophosphatemia/nutritional support/nutrition intervention/enteral and parenteral nutrition/feeding intolerance/electrolyte imbalance/metabolic disorders
“systematic review/meta-analysis/guideline/evidence summary/consensus/best practice/randomized controlled trial”Taking PubMed as an example, the search query is ((“Intensive Care Unit”[MeSH Terms] OR ICU[All Fields] OR “critical care unit”[All Fields] OR “critically ill”[All Fields]) AND (“refeeding syndrome”[MeSH Terms] OR hypophosphatemia[All Fields] OR “nutritional support”[All Fields] OR “nutrition intervention”[All Fields] OR “enteral and parenteral nutrition”[All Fields] OR “feeding intolerance”[All Fields] OR “electrolyte imbalance”[All Fields] OR “metabolic disorders”[All Fields])) AND (“systematic review”[All Fields] OR meta-analysis[All Fields] OR guideline[All Fields] OR “evidence summar*”[All Fields] OR consensus[All Fields] OR “best practice”[All Fields] OR randomiz*[All Fields]) Taking the Chinese database CNKI as an example, the search query is (subject: intensive care unit ICU critically ill patients critically ill patients) AND (subject: refeeding syndrome hypophosphatemia nutritional support nutritional intervention enteral and parenteral nutrition feeding intolerance electrolyte disorders metabolic disorders) AND (subject: guidelines expert consensus evidence summary systematic review randomized controlled trials best practice). The search period is from the database inception to December 25, 2025.
Inclusion and Exclusion Criteria for Literature
Inclusion criteria: ① Study subjects were ICU patients meeting diagnostic criteria; ② The research focuses on nutritional support strategies, risk assessment, or interventions for refeeding syndrome in ICU patients; ③ Study types included guidelines, clinical decision-making, systematic reviews, RCTs, expert consensus, etc; ④ The languages of included literature were Chinese or English.
Exclusion criteria: ① Guidelines, systematic reviews, or expert consensus/opinions that have been updated; ②The quality assessment is rated C by AGREE II; ③ Literature that cannot be accessed in full; ④ Duplicate literature; ⑤ Translated or interpreted versions of foreign literature.
Literature Screening
The literature screening was conducted using a dual-independent screening method. Initially, two researchers—both certified critical care nurses with over five years of clinical nursing experience, who had completed systematic training at the JBI Evidence-Based Nursing Center and held evidence-based practice qualifications, and were proficient in literature retrieval, screening, and quality assessment methods—performed preliminary screening by reviewing titles and abstracts to exclude studies that clearly did not meet the inclusion criteria. Subsequently, full-text reviews were conducted on the remaining studies to rigorously verify compliance with inclusion and exclusion criteria, ultimately determining each study’s inclusion status with detailed documentation of exclusion reasons. In case of discrepancies during screening, consensus was reached through group discussions or arbitration by a third-party evidence-based expert. Each exclusion rationale was meticulously recorded, culminating in a PRISMA flowchart. Literature quality assessment was performed independently by two researchers using the appropriate JBI Critical Evaluation Tool tailored to each study type. Disagreements were resolved through discussion or third-party arbitration to ensure objective and reliable evaluation results.
Criteria for Evaluating Literature Quality
The quality assessment tools employed in this study adhered to unified and standardized principles, with corresponding criteria applied based on the different types of included literature: (1) For guideline quality assessment, the Appraisal of Guidelines for Research and Evaluation (AGREE II)9 was utilized. This tool comprises 23 items divided into six core domains: ① Scope and purpose, ② Stakeholder involvement, ③ Rigor of formulation, ④ Clarity of expression, ⑤ Applicability, and ⑥ Editorial independence. Prior to assessment, two researchers trained in evidence-based nursing independently completed training and calibration of the AGREE II tool to ensure consistent understanding of the scoring criteria for each item; (2) Systematic reviews, meta-analyses, expert consensus reports, and cohort studies were evaluated using the respective literature quality assessment tools from the Australian JBI Centre for Evidence-Based Healthcare (2016 edition);10,11 (3) Clinical decisions retrieved from Uptodate were automatically classified as high-quality evidence and not assessed separately; clinical decisions from other databases were traced back to their original source literature and evaluated using the corresponding JBI literature quality assessment tool (2016 edition).
Literature Quality Control Process
The literature quality assessment was independently conducted by researchers trained by the Fudan University Evidence-Based Nursing Center. Each literature was evaluated independently by two researchers with professional qualifications in evidence-based nursing; the researchers reviewed each article and extracted evidence. In case of discrepancies during the assessment process, these were resolved through consultation or arbitration by a third party. The final literature quality grade was determined by synthesizing the evaluation results of all entries.
Evidence Description and Summary
The evidence synthesis adhered to the principles of “priority by hierarchy, categorized integration, and clinical relevance,” prioritizing studies with higher methodological quality. Evidence on the same topic was classified and summarized by study type; in cases of conflicting conclusions, higher-grade evidence was adopted, with final conclusions derived from heterogeneity analysis. Two intensive care nurses with systematic evidence-based nursing training and professional qualifications extracted and synthesized evidence from the 16 selected literature articles. Standardized data extraction forms were used to independently obtain basic literature information, study participant characteristics, intervention measures, and outcome indicators. Evidence on the same topic was further categorized by study type, and the JBI Evidence-Based Healthcare Center (2014 edition) pre-classification system was employed to assess evidence strength. Consistency of evidence was evaluated by comparing the direction of study conclusions; conflicting conclusions were resolved by prioritizing higher-grade evidence, ultimately forming a rigorous evidence framework.
Evidence Classification and Recommendation Levels
This study employed the 2014 edition of the Australian JBI Evidence-Based Healthcare Centre Evidence Classification and Recommendation Levels System12 to classify the included evidence, categorizing evidence levels into grades 1–5 (with grade 1a being the highest and grade 5c the lowest). Two researchers independently evaluated and graded the included evidence; in cases of disagreement, hospital-based evidence experts were consulted to resolve the discrepancy. When conflicting evidence was encountered, the evidence with the higher classification level was prioritized.
Results
General Characteristics of the Included Literature
A preliminary literature search yielded 4,031 articles. After removing duplicates using literature management software, 3,133 articles remained. Following review of titles and abstracts, 154 articles were selected. Upon full-text review, 138 articles that did not meet inclusion criteria or were of low quality were excluded, leaving 16 final included articles. These comprised 3 guidelines,13–15 2 clinical decision-making studies,16,17 4 systematic reviews,18–21 2 cohort studies,22,23 1 randomized controlled trial (RCT),24 and 4 expert consensus reports.5,25–27 The literature screening process is illustrated in Figure 1, and the basic characteristics of the included articles are presented in Table 1.
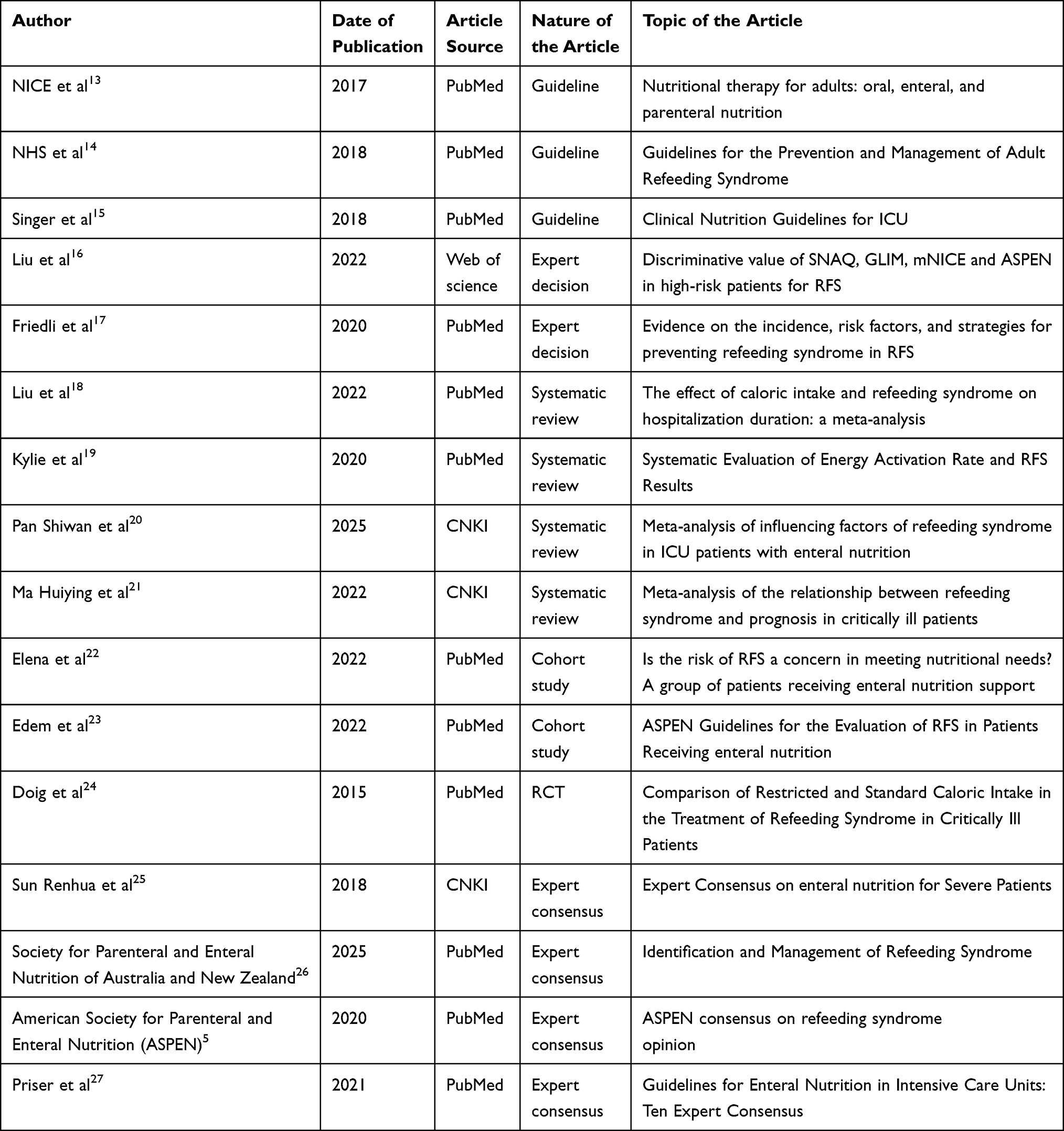 |
Table 1 Basic Characteristics of Included Literature (n=16) |
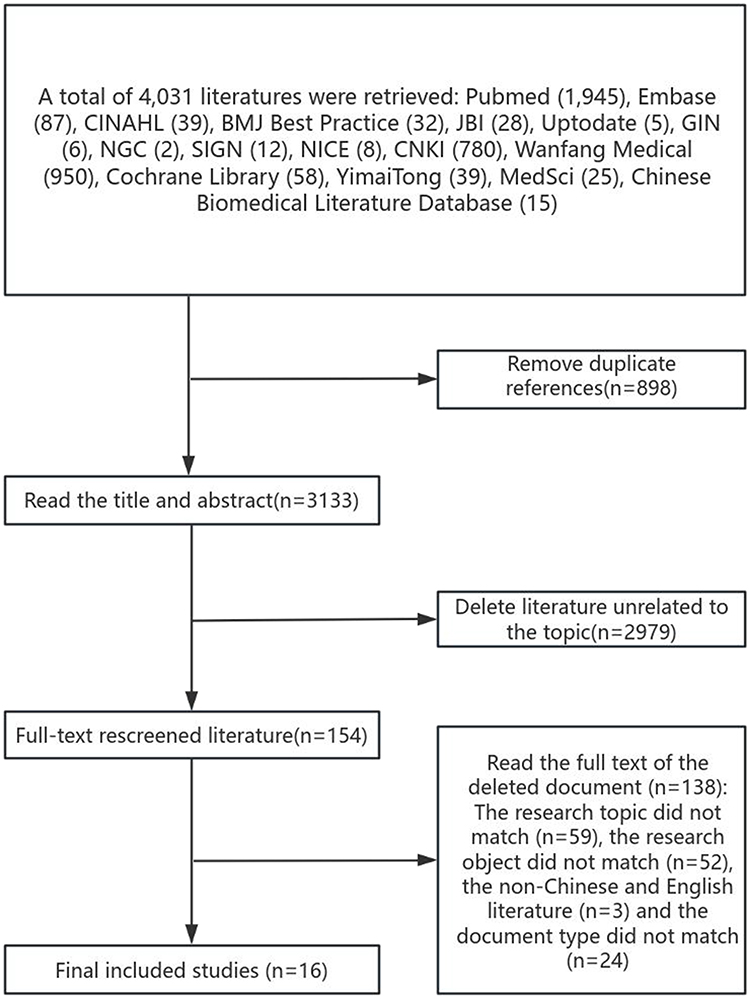 |
Figure 1 Literature Screening Process. |
Incorporation of Literature Quality Evaluation Results
Results of Guideline Quality Evaluation
This study evaluated the quality of the three included guidelines according to the AGREE II guideline assessment criteria, covering six aspects such as scope and purpose, and participants. The scores and recommended levels for each domain are detailed in Table 2.
 |
Table 2 Quality Evaluation Results of the Guidelines (n=3) |
Systematic Review Analysis of Quality Evaluation Results
This study conducted a methodological quality assessment of the four included systematic reviews using the quality evaluation criteria of the Australian Centre for Evidence-Based Healthcare (JBI), evaluating item compliance across 11 dimensions such as research questions, literature inclusion, and search strategies. The results indicate that the majority of literature items demonstrated satisfactory compliance, with overall research methods being relatively standardized. Detailed evaluation findings for each systematic review are presented in Table 3.
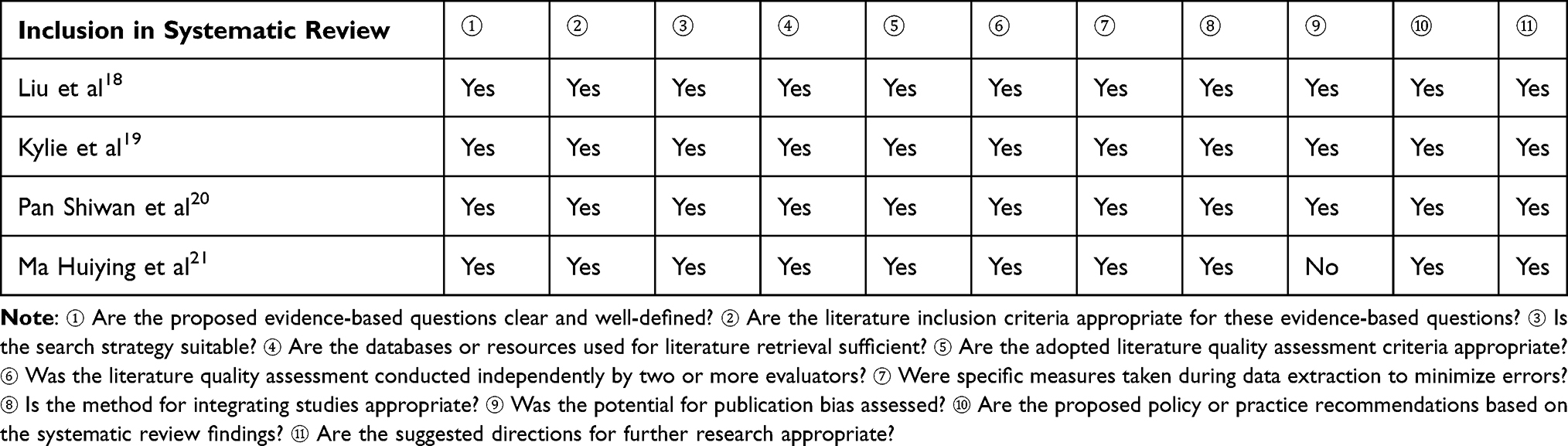 |
Table 3 Systematic Review Quality Results (n=4) |
Results of Quality Evaluation for Cohort Studies
Using the Australian Journal of Biomedical Research (JBI) cohort study quality assessment tool, a methodological quality evaluation was conducted on the two included studies. The standardization of research methods was assessed item-by-item based on 11 core criteria. The evaluation results indicated that the overall quality of the included cohort studies was acceptable, with only one study demonstrating deficiencies in confounding factor management. The specific criterion compliance is detailed in Table 4.
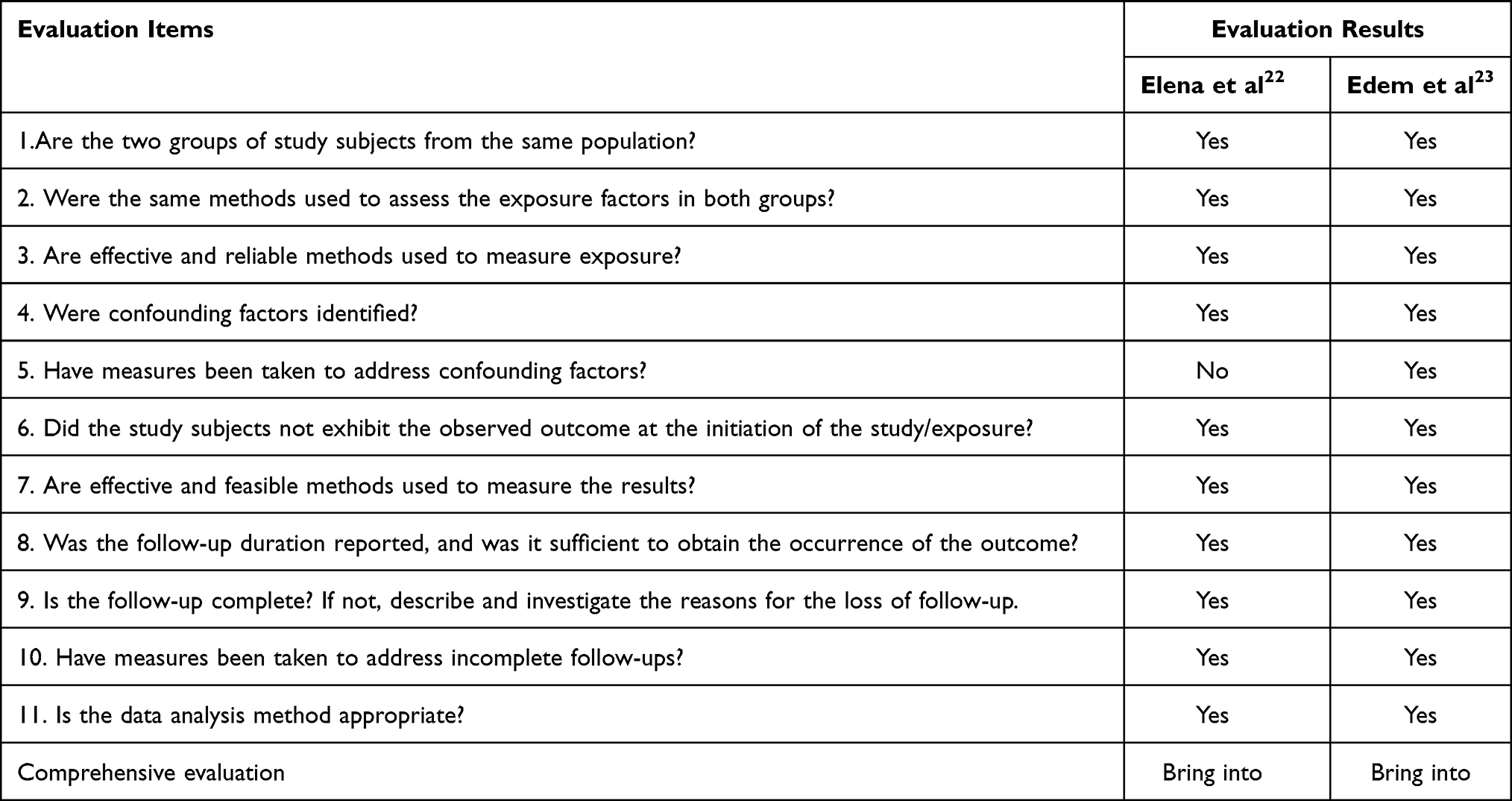 |
Table 4 Quality Assessment Results of the Cohort Study (n=2) |
Quality Evaluation Results of Randomized Controlled Trials
The study included one randomized controlled trial (RCT).24 The literature review indicated that only the evaluation criteria regarding blinding of participants and blinding of interveners received a “no” rating, while all other criteria were rated “yes.” This study was deemed of high quality and was therefore included.
Results of Expert Consensus Quality Evaluation
Among the four expert consensus articles included in the study,5,25–27 all literature evaluation entries were rated as “yes,” indicating high overall quality; thus, they were included.
Clinical Decision Evaluation Results
Among the two clinical decision-making studies16,17 included in the review, all literature evaluation entries yielded a “yes” response, indicating high overall literature quality, and both were thus included. This evaluation did not trace back to the original studies cited in the literature; instead, it conducted a quality assessment solely on the included studies themselves, which consisted of a prospective observational study and a review article.
Summary of Optimal Evidence
The relevant content from the included literature was extracted and summarized. The 2014 edition of the JBI Evidence-Based Healthcare Center Evidence Pre-classification and Evidence Recommendation Levels System was employed to evaluate and grade the included evidence. The evidence levels were categorized as levels 1–5: Level 1 represented systematic reviews and high-quality randomized controlled trials; Level 2 represented cohort studies; Level 3 represented case-control studies; Level 4 represented cross-sectional studies and quasi-experimental studies; Level 5 represented expert opinions, case reports, and experience summaries. Based on the evidence’s feasibility, relevance, clinical significance, and validity, the recommendations were classified as Level A (strong recommendation) or Level B (weak recommendation). A total of 24 relevant pieces of evidence were identified, detailed in Table 5.
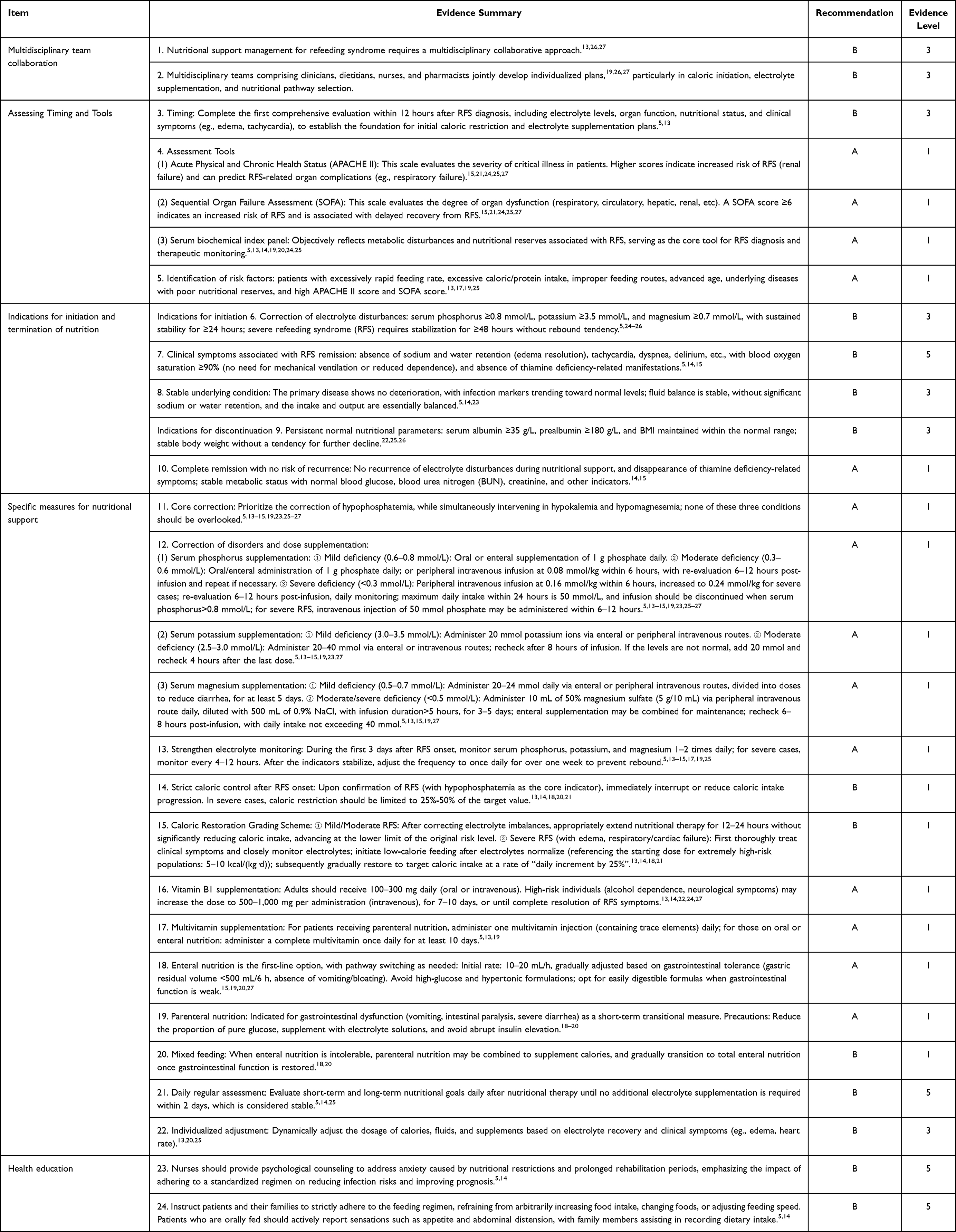 |
Table 5 Summary of Evidence on Nutritional Support for ICU Refeeding Syndrome |
Discussion
Establishing a Multidisciplinary Team is the Direction for Providing Nutritional Support to Patients
Both the Australian Nutrition Society26 and ASPEN5 have explicitly identified multidisciplinary collaboration as the core strategy for RFS nutritional support, advocating for the involvement of a professional team comprising physicians, nurses, clinical dietitians, and pharmacists throughout the entire intervention process. The multicenter randomized controlled trial (RCT) conducted by Doig et al24 has demonstrated that this physician-nurse-dietitian collaborative nutritional support approach not only significantly reduces the incidence of major infections and 60-day mortality rates in RFS patients but also improves adherence to the nutritional regimen. Compared to traditional single-disciplinary, decentralized models, multidisciplinary teamwork enhances the comprehensiveness of interventions, reduces adverse events, optimizes work efficiency and outcome quality, and better addresses complex clinical challenges through the integration of multidisciplinary expertise and collaborative decision-making.28 The conclusions of this study are highly consistent with this high-quality evidence, further validating the efficacy of multidisciplinary collaboration in improving RFS patient outcomes. Currently, standardized protocols for multidisciplinary management of RFS remain inadequate in China, with varying levels of collaboration depth and implementation consistency across healthcare institutions.29 Future efforts should focus on developing standardized multidisciplinary collaboration frameworks tailored to regional healthcare resource characteristics.
The Timing and Tools for Evaluation are Essential
Appropriate assessment tools and appropriate timing are key evidence-based safeguards for the safe implementation of nutritional support for patients with refeeding syndrome. The comprehensive evidence of this study found24 that RFS-related assessment must be carried out throughout the entire process of nutritional support, rather than a single screening: the first nutritional risk and RFS high-risk screening must be completed within 24 hours of admission, electrolyte levels monitored every 12 hours for 72 hours after nutritional support is initiated, and a comprehensive assessment completed within 12 hours after the occurrence of RFS. Compared with the previous practice of only a single risk screening before the initiation of nutritional support, standardized assessment throughout the whole process can significantly improve the sensitivity of early identification and reduce the risk of missed diagnosis and complications of RFS. In terms of the selection of assessment tools, some studies have pointed out that the30 NRS 2002 scale can effectively identify the nutritional risk of ICU patients, and the score of ≥3 is an independent influencing factor for the occurrence of RFS. SOFA score can accurately judge the degree of organ function damage and provide a basis for the formulation of the starting dose of the nutrition regimen. APACHE II. score and SOFA score combined with dynamic monitoring data of blood phosphorus, potassium and magnesium can comprehensively evaluate the patient’s organ function status and nutritional support tolerance, and avoid intervention delay or improper feeding caused by insufficient assessment. This comprehensive assessment model can more comprehensively cover the key links of RFS than single-tool screening, and provide an evidence-based path for clinical development of individualized nutritional support plans.
Nutritional Support for RFS Patients Still Faces Significant Challenges
Refeeding syndrome (RFS) is a metabolic disorder syndrome triggered by the resumption of nutritional intake after prolonged malnutrition, characterized primarily by electrolyte imbalance and organ dysfunction.31 The initiation and termination criteria for RFS interdependently provide clear clinical guidance for avoiding complications and ensuring the safety of nutritional interventions. The initiation and cessation of nutritional support in RFS patients must simultaneously meet three core criteria: stabilization of electrolyte levels, alleviation of clinical symptoms, and controllable underlying disease status. These criteria are derived from multicenter studies,24 meta-analyses,18–21 and consensus guidelines from international authoritative societies.5,25,26 Their integrated application enables precise timing of nutritional interventions, preventing exacerbation of metabolic disturbances due to premature refeeding and avoiding nutritional deficiencies caused by delayed feeding, thereby supporting standardized management of RFS patients. Traditional RFS intervention criteria primarily focus on energy requirements, organ function, or disease stage, lacking targeted metabolic safety considerations for high-risk individuals, which may lead to metabolic disturbances or nutritional deficiencies.32 In contrast, the multidimensional indicator system integrated in this study addresses both the patient’s overall condition and the specific metabolic risks associated with RFS, effectively compensating for the limitations of conventional criteria and providing more evidence-based guidance for individualized nutritional support strategies. However, this system is applicable only to specific RFS populations, and some criteria lack quantitative definitions, necessitating further prospective studies to validate its clinical relevance and feasibility.
Implementing Specific Nutritional Support Measures is Crucial
Caloric adjustment and control constitute the cornerstone of nutritional support following refeeding syndrome (RFS),33 directly influencing the efficacy of metabolic disorder correction and patient clinical outcomes. Evidence from this study5,13–15,19,23,25–27 demonstrates that supplementation with phosphorus or thiamine during nutritional therapy effectively prevents refeeding syndrome and hypophosphatemia, while reducing mortality and adverse prognosis risks in high-risk patients. Supplementation of essential nutrients forms the foundation of post-RFS nutritional support,19 with the selection of appropriate feeding routes based on individual needs ensuring both safety and efficacy of nutrient delivery. This approach must be precisely tailored to the patient’s gastrointestinal function, disease severity, and nutritional tolerance. Enteral nutrition remains the most commonly used and recommended pathway,5 offering superior physiological compatibility and fewer complications, making it suitable for patients with tolerable gastrointestinal function. Further research5,13 underscores that individualized assessment and adjustment are critical components of post-RFS nutritional support, serving as the cornerstone for achieving a balance between nutrient delivery and physiological tolerance while minimizing treatment deviations. This requires dynamic, comprehensive adaptation tailored to the patient’s specific condition.34
Implementing Standardized Health Education is a Key Pathway to Improving Nutritional Support Compliance in Refeeding Syndrome
Implementing standardized health education is an indispensable key component of the comprehensive RFS nutritional support management and a core measure for improving patient outcomes.35 Nurses should provide psychological counseling addressing anxiety stemming from nutritional restrictions and prolonged rehabilitation periods, emphasizing the impact of adherence to standardized protocols on reducing infection risks and enhancing prognosis. Evidence synthesis from this study18 demonstrates that systematic health education significantly improves patient and family compliance with nutritional support regimens, reduces RFS recurrence due to unauthorized protocol modifications, and enhances adherence to critical measures such as electrolyte monitoring and medication adherence. Consequently, this approach shortens hospital stays, lowers the incidence of complications like infections, and ensures evidence-based, standardized management of RFS nutritional support.36
Conclusion
This study summarizes the evidence-based evidence regarding nutritional support for ICU refeeding syndrome, covering five aspects: multidisciplinary team collaboration, timing and tools for assessment, indications for initiating and terminating nutritional support, specific measures of nutritional support, and health education. A total of 24 evidence-based recommendations were identified. The studies included in this review exhibited certain heterogeneity in terms of study design, sample size, nutritional support protocols, and outcome measures, with some conclusions being inconsistent. Therefore, when formulating recommendations, we prioritized high-quality evidence with consistent results, providing only qualitative descriptions of controversial conclusions, and advised cautious application based on individual patient circumstances. Currently, the application of multidisciplinary team collaboration, assessment timing and tools, indications for initiating and terminating nutritional support, specific nutritional support measures, and health education in refeeding syndrome still requires further validation and exploration through large-scale, multicenter, high-quality randomized controlled trials. Since most existing studies are based on international guideline consensus and clinical data, there are relatively few specialized domestic studies focusing on ICU patients, elderly patients, or patients with underlying comorbidities, which may differ from China’s actual clinical practices, patient comorbidity profiles, and the availability of nutritional support resources. When applying relevant evidence in clinical practice, it is recommended to comprehensively consider factors such as the severity of the patient’s condition, nutritional risk level, gastrointestinal function status, the patient’s and family’s treatment willingness, and financial capacity to develop safe and appropriate individualized nutritional support management plans. This approach aims to minimize the risk of refeeding syndrome-related complications and improve clinical outcomes. Subsequent research should focus on China’s local ICU population and high-risk patients to explore suitable quantitative indicators and management pathways for RFS nutritional support, thereby facilitating the development of localized clinical guidelines.
Data Sharing Statement
The datasets generated and analysed during the current study are not publicly available but are available from the corresponding author (Liping Yuan) on reasonable request.
Funding
Special Project of the China Society of Gerontology and Geriatrics “China Aging Work Development Research Report” (CAGG2025ZX043); Humanities and Social Sciences Research Project of the Anhui Provincial Department of Education (2023AH051723); Key Project of Wannan Medical College for 2023 (Project No.: WK2023SZD06).
Disclosure
None of the authors have any conflicts of interest in this work.
References
1. A RB, Starkopf J, Alhazzani W, et al. Early enteral nutrition in critically ill patients:ESICM clinical practice guidelines. Intensive Care Med. 2017;43(3):380–14. doi:10.1007/S00134-016-4665-0
2. Lew CCH, Yandell R, Fraser RJL, Chua AP, Chong MFF, Miller M. Association between malnutrition and clinical outcomes in the intensive care unit: a systematic review [Formula: see text]. JPEN J Parenter Enteral Nutr. 2017;41(5):744–758. doi:10.1177/0148607115625638
3. Kondrup J. Nutritional-risk scoring systems in the intensive care unit. Curr Opin Clin Nutr Metab Care. 2014;17(2):177–182. doi:10.1097/MCO.0000000000000041
4. Crook MA. Cardiac abnormalities in the refeeding syndrome. Nutrition. 2017;35:146–147. doi:10.1016/j.nut.2017.01.004
5. da Silva JSV, Seres DS, Sabino K, et al. ASPEN consensus recommendations for refeeding syndrome. Nutr Clin Pract. 2020;35(2):178–195. doi:10.1002/ncp.10474
6. Jeon TJ, Lee KJ, Woo HS, et al. Refeeding syndrome as a possible cause of very early mortality in acute pancreatitis. Gut Liver. 2019;13(5):576–581. doi:10.5009/gnl18458
7. Chen LJ, Chen HL, Bair MJ, et al. Refeeding syndrome in Southeastern Taiwan: our experience with 11 cases. World J Gastroenterol. 2014;20(30):10525–10530. doi:10.3748/wjg.v20.i30.10525
8. Brown CA, Sabel AL, Gaudiani JL, Mehler PS. Predictors of hypophosphatemia during refeeding of patients with severe anorexia nervosa. Int J Eat Disord. 2015;48(7):898–904. doi:10.1002/eat.22406
9. Brouwers MC, Kho ME, Browman GP, et al. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010;182(18):E839–E842. doi:10.1503/cmaj.090449
10. McArthur A, Klugárová J, Yan H, Florescu S. Innovations in the systematic review of text and opinion. Int J Evid Based Healthc. 2015;13(3):188–195. doi:10.1097/XEB.0000000000000060
11. Ying G, Huiwen Z. Zhou yingfeng, et al.jbi evidence-based healthcare center’s quality assessment tool for different types of research: methodological quality evaluation of systematic reviews. J Nurs Contin Educ. 2018;33(08):701–703.
12. Chunqing W. hu yan.jbi evidence pre-classification and evidence recommendation level system (2014 Edition). J Nurs Educ. 2015;30(11):964–967.
13. Nutrition Support for Adults: Oral Nutrition Support, Enteral Tube Feeding and Parenteral Nutrition. London: National Institute for Health and Care Excellence (NICE); August 2017
14. Hamilton AAK, Allsopp K. CNSG east cheshire NHS trust guidelines for prevention and management of refeeding syndrome in adults. East Cheshire NHS Trust. [2018-12-01].
15. Singer P, Blaser AR, Berger MM, et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clin Nutr. 2019;38(1):48–79. doi:10.1016/j.clnu.2018.08.037
16. Liu N, Zhao XL, Xiong RQ, et al. The Performances of SNAQ,GLIM, mNICE, and ASPEN for identification of neurocritically ill patients at high risk of developing refeeding syndrome. Nutrients. 2022;14(19):4032. doi:10.3390/nu14194032
17. Friedli N, Odermatt J, Reber E, Schuetz P, Stanga Z. Refeeding syndrome: update and clinical advice for prevention, diagnosis and treatment. Curr Opin Gastroenterol. 2020;36(2):136–140. doi:10.1097/MOG.0000000000000605
18. Liu P, Chen L, Zhong T, Zhang M, Ma T, Tian H. Impact of calorie intake and refeeding syndrome on the length of hospital stay of patients with malnutrition: a systematic review and meta-analysis. Clin Nutr. 2022;41(9):2003–2012. doi:10.1016/j.clnu.2022.07.023
19. Matthews-Rensch K, Capra S, Palmer M. Systematic review of energy initiation rates and refeeding syndrome outcomes. Nutr Clin Pract. 2021;36(1):153–168. doi:10.1002/ncp.10549
20. Pan SW, Hong YH, Li JJ, et al. Meta-analysis of influencing factors on refeeding syndrome in ICU patients receiving enteral nutrition. Evidence Based Nurs. 2025;11(04):610–616.
21. Huiying M, Sheng Y, Xinyu Z, et al. Meta-analysis of the relationship between refeeding syndrome and prognosis in critically ill patients. Nurs res. 2022;36(17):3023–3031.
22. Sandoval-Cartagena EM, Guevara-Cruz M, Rivera-Duarte A, et al. Is the risk of refeeding syndrome a problem in reaching nutritional requirements? A cohort of patients on enteral nutrition support. Nutr Hosp. 2022;39(1):12–19. doi:10.20960/nh.03767
23. Adika E, Jia R, Li J, Seres D, Freedberg DE. Evaluation of the ASPEN guidelines for refeeding syndrome among hospitalized patients receiving enteral nutrition: a retrospective cohort study. JPEN J Parenter Enteral Nutr. 2022;46(8):1859–1866. doi:10.1002/jpen.2368
24. Doig GS, Simpson F, Heighes PT, et al. Restricted versus continued standard caloric intake during the management of refeeding syndrome in critically ill adults: a randomised, parallel-group, multicentre, single-blind controlled trial. Lancet Respir Med. 2015;3(12):943–952. doi:10.1016/S2213-2600(15)00418-X
25. Renhua S, Ronglin J, Man H, et al. Expert consensus on clinical practice of early enteral nutrition in critically ill patients. Chin J. Crit. Care Med. 2018;30(8):715–721.
26. Matthews-Rensch K, Blackwood K, Lawlis D, et al. The australasian society of parenteral and enteral nutrition: consensus statements on refeeding syndrome. Nutr Diet. 2025;82(2):128–142. doi:10.1111/1747-0080.70003
27. Preiser JC, Arabi YM, Berger MM, et al. A guide to enteral nutrition in intensive care units: 10 expert tips for the daily practice. Crit Care. 2021;25(1):424. doi:10.1186/s13054-021-03847-4
28. Rinninella E, Marco D, Angelo RB, Galasso T, Cintoni M. Incidence and impact of refeeding syndrome in an internal medicine and gastroenterology ward of an italian tertiary referral center: a prospective cohort study. Nutirents. 2022;14(7):1343. doi:10.3390/nu14071343
29. Yu Q, Jin D, Wang YF, et al. Multidisciplinary team collaboration in the diagnosis and treatment of Crohn’s disease complicated by refeeding syndrome and lymph node tuberculosis: a case report. Chin. J. Inflamm. Bowel Dis. 2023;07(1):86–89.
30. Maciel LRMA, Franzosi OS, Nunes DSL, et al. Nutritional risk screening 2002 cut-off to identify high-risk is a good predictor of icu mortality in critically ill patients. Nutr Clin Pract. 2019;34(1):137–141. doi:10.1002/ncp.10185
31. Manish S, Alexandra P, Eric L. Refeeding syndrome as an unusual cause of anion gap metabolic acidosis. Mil Med. 2012;177(11):1393–1395. doi:10.7205/MILMED-D-11-00432
32. Wei M, Wu YF. Advances in refeeding syndrome. Parenteral Enteral Nutr. 2020;27(4):243–247.
33. Kawamura H, Tanaka S, Uenami Y, et al. Hypophosphatemia occurs with insulin administration during refeeding by total parenteral nutrition in rats. J Med Invest. 2018;65(1.2):50–55. doi:10.2152/jmi.65.50
34. M MH, Moledina J, Travis J. Refeeding syndrome: what it is, and how to prevent and treat it. BMJ. 2008;336(7659):1495–1498. doi:10.1136/bmj.a301
35. Pohlenz-Saw JAE, Merriweather JL, Wandrag L. (Mal)nutrition in critical illness and beyond: a narrative review. Anaesthesia. 2023;78(6):770–778. doi:10.1111/anae.15951
36. Yoshida M, Izawa J, Wakatake H, et al. Mortality associated with new risk classification of developing refeeding syndrome in critically ill patients: a cohort study. Clin Nutr. 2021;40(3):1207–1213. doi:10.1016/j.clnu.2020.07.034
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
An Evidence-Based Medical Review on Promoting Gastrointestinal Function Recovery After Colorectal Cancer Surgery
Zhao CY, Shi WH, Wen ZQ, Jin YM, Shang YB, Zheng L, Li J, Chen XM
Journal of Multidisciplinary Healthcare 2024, 17:1343-1362
Published Date: 23 March 2024
Evidence Summary of Personalized Management of Peritoneal Dialysis Volume in Adults
Yu C, Sha P, Jiang Z, Wei Y, Gong B, Jiang S, Wang R
Journal of Multidisciplinary Healthcare 2025, 18:2707-2719
Published Date: 15 May 2025
An Evidence-Based Medical Review on Preoperative Exercise Prehabilitation in Lung Cancer Patients
Zhang R, Wu M, Cheng Y, Xu Y, Xia L
Journal of Multidisciplinary Healthcare 2025, 18:4849-4858
Published Date: 7 August 2025
Summary of Best Evidence for Psychosocial Interventions in Adults with Alcohol Use Disorder: An Evidence-Based Review
Yan L, Ji CF, Xia LP, Sun W, Shi JQ, Wu XD
Journal of Multidisciplinary Healthcare 2025, 18:6315-6327
Published Date: 2 October 2025
Best Evidence for Preventing Urinary Tract Infections and Optimizing Care in Adults with Indwelling Urinary Catheters
Tang J, Fan Y, Lu J, Zhang Y
Risk Management and Healthcare Policy 2025, 18:3593-3608
Published Date: 11 November 2025