Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
An Evidence-Based Medical Review on Preoperative Exercise Prehabilitation in Lung Cancer Patients
Authors Zhang R ![]() , Wu M, Cheng Y, Xu Y, Xia L
, Wu M, Cheng Y, Xu Y, Xia L
Received 26 March 2025
Accepted for publication 23 July 2025
Published 7 August 2025 Volume 2025:18 Pages 4849—4858
DOI https://doi.org/10.2147/JMDH.S528534
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Charles V Pollack
Rui Zhang,1– 3,* Mei Wu,4,* Yun Cheng,2 Yamin Xu,5 Lu Xia4
1Faculty of Military Health Services, Naval Medical University, Shanghai, 200438, People’s Republic of China; 2Department of Nursing, Huadong Hospital Affiliated to Fudan University, Shanghai, 200040, People’s Republic of China; 3School of Nursing, Fudan University, Shanghai, 200030, People’s Republic of China; 4Day Surgery Unit, Huadong Hospital Affiliated to Fudan University, Shanghai, 200040, People’s Republic of China; 5Day Chemotherapy Ward, Huadong Hospital Affiliated to Fudan University, Shanghai, 200040, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yamin Xu, Day Chemotherapy Ward, Huadong Hospital Affiliated to Fudan University, No. 221 of Yanan West Road, Jingan District, Shanghai, 200040, People’s Republic of China, Tel +86 21-62483180-530402, Email [email protected] Lu Xia, Day Surgery Unit, Huadong Hospital Affiliated to Fudan University, No. 221 of Yanan West Road, Jingan District, Shanghai, 200040, People’s Republic of China, Tel +86 21-62483180-530401, Email [email protected]
Objective: Preoperative exercise prehabilitation in lung cancer patients can improve preoperative functional reserve, reduce postoperative complications, accelerate postoperative recovery compared with postoperative rehabilitation. To integrate and evaluate the evidence related to preoperative exercise prehabilitation in patients with lung cancer.
Methods: Conducted utilizing the “ 6S” model of evidence resources, according to the search strategy searching for relevant guidelines, evidence summaries, best practices, systematic reviews, and expert consensuses on preoperative exercise prehabilitation for lung cancer patients. Based on the evidence inclusion and exclusion criteria, filter out relevant literature published between the beginning of each database and December 2024. Evaluated the quality of the selected literature, and then synthesis the evidence from the literature and made the recommendation level formulation.
Results: There were 16 pieces of literature in total, including two guidelines, three evidence summaries, one expert consensus, and ten systematic reviews. Twenty-two pieces of evidence were summarized from seven aspects: patient selection and assessment, exercise implementation and supervision, type of the exercise program, exercise prescription, safety of the exercise program, adherence to exercise program and exercise outcome evaluation.
Conclusion: The evidence presented in this study is scientific, comprehensive and of good clinical applicability, which can provide an evidence-based basis for medical staff to carry out preoperative exercise prehabilitation of lung cancer patients.
Keywords: lung neoplasms, prehabilitation, preoperative exercise, evidence summary, evidence-based nursing
Introduction
Lung cancer is an intricate illness with a variety of clinicopathological characteristics,1–3 which is high on the list in overall morbidity and mortality among all malignant tumors.4 Surgical resection is the only effective treatment for most patients with early lung cancer.5 Current research on exercise interventions for perioperative lung cancer patients focuses mostly on the postoperative rehabilitation phase of the perioperative period, and studies have shown that short-term postoperative rehabilitation in an inpatient setting is not clinically beneficial, so it is particularly important to be able to fully utilize the time prior to surgery, especially prior to admission, for purposeful exercise.6–8 The guidelines for enhanced recovery after surgery emphasize that improving preoperative functional reserve and surgical tolerance by prehabilitation prior to surgery can assist lower perioperative morbidity and postoperative problems.9,10 Therefore, preoperative exercise is an important basis for prehabilitation.
Preoperative exercise prehabilitation continues to be more and more researched, and pertinent clinical trial results have demonstrated its safety and efficacy.11 Previous research has demonstrated the benefits of preoperative exercise, but it has not provided a clear description of the precise nature of the exercise.12,13 It is still unclear to clinical medical personnel how to create the best preoperative exercise prehabilitation program. The content of preoperative exercise prehabilitation for lung cancer patients includes a series of measures recommended to implement and improve the perioperative functional status, but there is still a lack of unified mode. How to select acceptable and suitable interventions among a complex series of recommendations is a challenge for the further implementation and promotion of preoperative exercise prehabilitation for lung cancer patients. In order for clinical medical staff to fully comprehend the specifics and encourage the integration of pertinent evidence into clinical practice, it is necessary to summarize the evidence regarding preoperative exercise prehabilitation for lung cancer patients based on the evidence that is currently available. The present research used an evidence-based methodology to methodically acquire, analyze, and integrate evidence in order to create a reference for preoperative exercise prehabilitation for lung cancer patients.
Materials and Methods
Question Identification
Using the Evidence-based Nursing Center of Fudan University’s Problem Development Tool, we identified questions according to the clinical question “How to do preoperative exercise prehabilitation in lung cancer patients”, adhering to the PIPOST principle.14 The following was the detailed content of the question identification. Population (P): the patients to be operated on for lung cancer. Intervention (I): the measures related to exercise prehabilitation related to the ERAS concept. Professional (P): the medical professionals and lung cancer patients could benefit from the evidence. Outcome (O): the indicators of improvement in the perioperative condition of patients with lung cancer. Setting (S): the evidence could be used in hospitals, homes, and communities. Type of evidence (T): the forms of evidence included guidelines, expert consensuses, systematic reviews, evidence summaries, and clinical practice.
Retrieval Strategy
A top-down searching using the “6S” model of evidence resources was carried out.15 The search included relevant databases as well as guidelines net. The databases included Cochrane Library, PubMed, CNKI, Wanfang database, China Biomedical Literature Database (CBM), Web of Science, Embase, CINAHL. Guidelines net including UpToDate, National Institute for Health and Care (NICE), Registered Nurses’ Association of Ontario (RNAO), Scottish Intercollegiate Guidelines Network (SIGN), National Guideline Clearinghouse (NGC), Guidelines International Network (GIN), BMJ Best Practice, DynaMed, Joanna Briggs Institute Evidence-Based Health Care Center Library (JBI), National Comprehensive Cancer Network (NCCN), British Thoracic Society (BTS), European Society of Thoracic Surgeons (ESTS), Scottish Intercollegiate Guidelines Network (SIGN), New Zealand Guidelines Group (NZGG).
The search strategy was “lung cancer/lung neoplasms[mesh]/lung tumor/pulmonary*” AND “preoperative exercise[mesh]/exercise/prehabilitation/rehabilitation” AND “guideline/consensus/statement/evidence summary/systematic review/meta/practice”. The search encompassed all available literature from the inception of each database to December 2024.
Literature Inclusion and Exclusion Criteria
Inclusion criteria: (1) the study population of the literature is lung cancer patients treated with surgery, (2) the intervention of the literature is preoperative exercise measures related to prehabilitation under the concept of ERAS, (3) the population to which the evidence of the literature can be applied is clinical professionals and lung cancer patients, (4) the outcome indicator of the literature is the improvement of patients’ perioperative conditions, (5) the place to which the evidence of the literature can be applied is hospitals, homes and community or rehabilitation centers, (6) the type of the literature is guidelines, clinical practice, expert consensus, systematic evaluation, evidence summary, printed in Chinese or English language, published from the inception of each database to December 2024. Exclusion criteria: (1) full text was not available, (2) plans in the research stage or systematic evaluations or evidence summaries included in the guidelines, (3) literature for which updated versions were available.
Literature Quality Evaluation Instrument
(1) Clinical guideline quality evaluation tool: the AGREE-II evaluation tool was used to evaluate the quality of the included guidelines.16 (2) Expert consensus quality evaluation tool: the JBI authenticity evaluation tool was used to evaluate expert consensus articles.17 (3) Clinical decision-making and evidence summarization quality evaluation tool: tracing the source of evidence and selecting the appropriate evaluation tool according to the type of literature. (4) Quality evaluation tool for systematic evaluation: evaluated according to the quality evaluation tool of JBI systematic evaluation.18 Three researchers evaluated the quality of the literature separately, and if the evaluators’ opinions were not unanimous, a fourth senior researcher was invited to confer and finally reach a unified opinion.
Evidence Synthesis and Recommendation Level Formulation
Two researchers extracted the resulting evidence, and a third was invited to discuss and come to a consensus if there was a disagreement. If there was a conflict in the extracted evidence, the principle of prioritizing evidence based on evidence, high-quality evidence, recently published evidence, and evidence from national guidelines was followed for integration. The level of evidence for inclusion was categorized as 1~5 according to the JBI evidence pre-grading, where the highest level was 1 and the lowest level was 5.19 All authors of this article have clinical experience and have received systematic training in evidence-based curricula.
Result
General Characteristics of the Included Literature
This study initially searched for 2156 relevant papers. After excluded duplicates, translated versions, paraphrased versions, papers that did not fit the topic, were of lower quality, and did not fit the type of paper or the time of publication, sixteen relevant articles were finally included. Which includes two guidelines, one expert consensus, three evidence summaries, and ten systematic evaluations. The flowchart of literature screening is shown in Figure 1. Basic characteristics of the included literature are shown in Table 1.
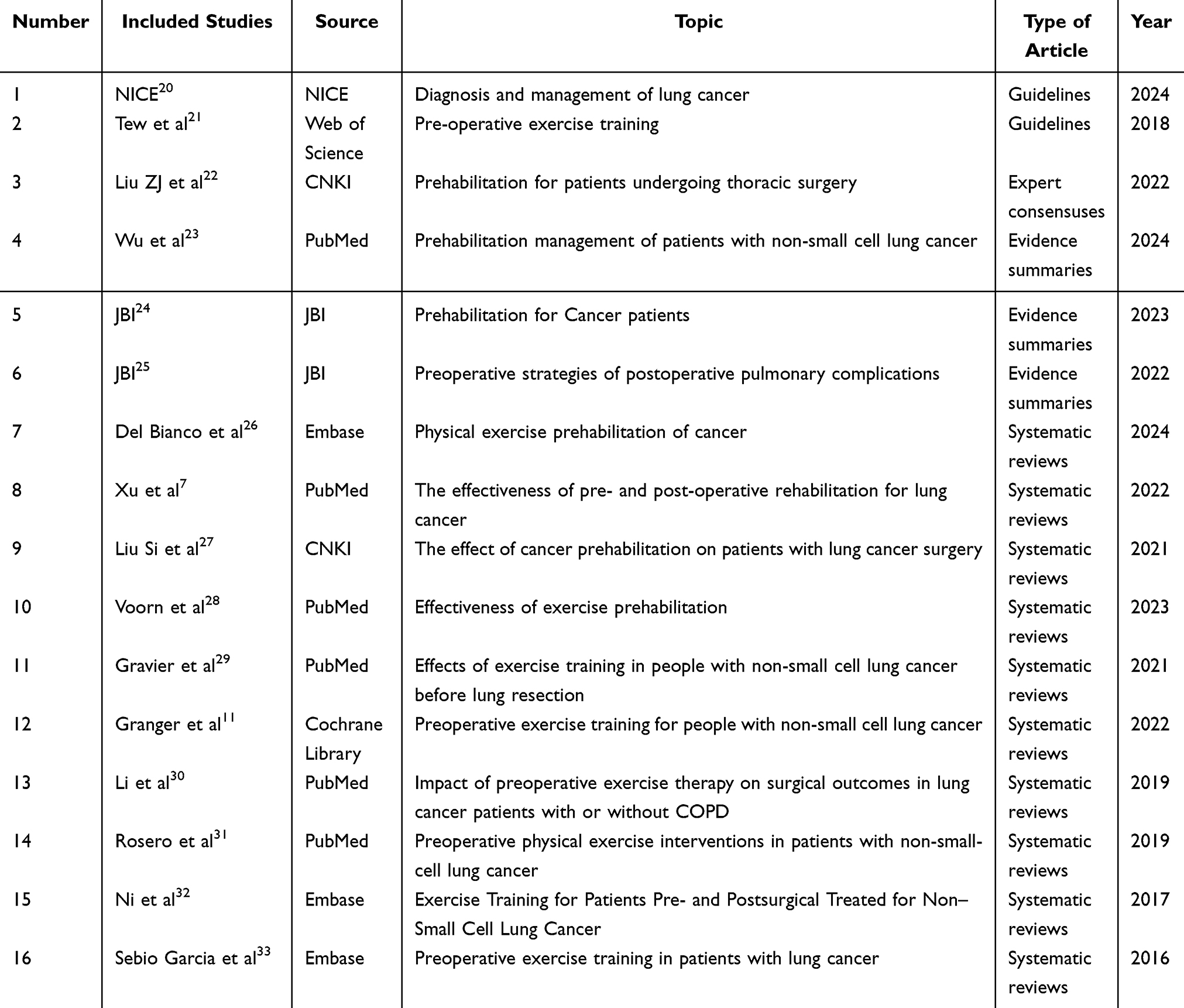 |
Table 1 The Characteristics of the Included Studies (n=16) |
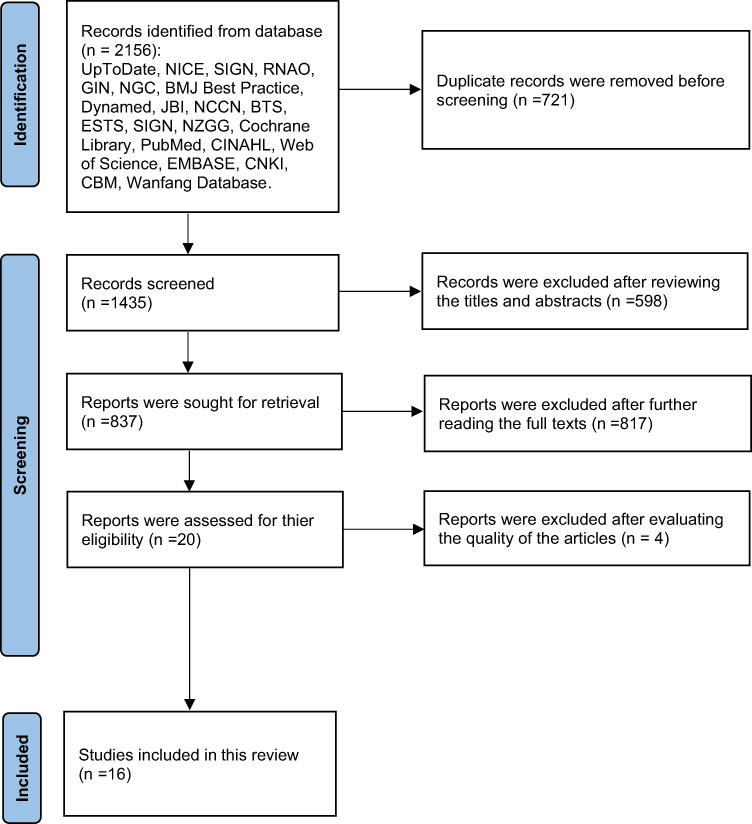 |
Figure 1 Flow chart of literature screening. |
Quality Evaluation Results of Literature
Results of the Quality Evaluation of Guidelines
The two guidelines that were included were assessed with grade A and grade B, then they were approved for inclusion. Table 2 displays the quality assessment’s specifics.
 |
Table 2 Quality Evaluation results of Included Guidelines (n=2) |
Results of the Quality Evaluation of Expert Consensus
One expert consensus was included with “yes” for all entries except entry 1, which was “no”. The expert consensus was of high quality and was allowed to be included. Table 3 summarizes the findings.
 |
Table 3 Quality Evaluation Results of Included Expert Consensus (n=1) |
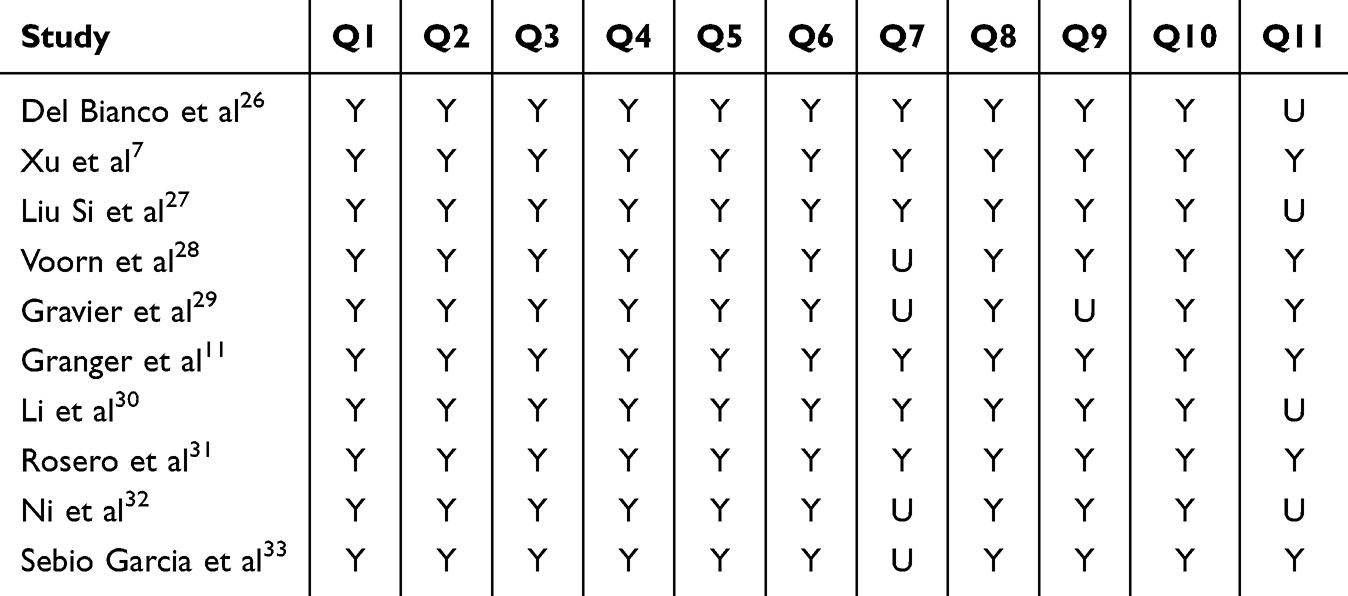 |
Table 4 Quality Evaluation Results of Included Systematic Reviews (n=10) |
Results of the Quality Evaluation of Systematic Reviews
Eight systematic evaluations were included, which were of high overall quality and were also granted inclusion. The results are summarized in Table 4.
Results of the Quality Evaluation of Evidence Summaries
There were two JBI evidence summaries that traced the evidence back to the original literature, and all four were systematic reviews. The systematic reviews’ quality was evaluated, and they all met standard. As a result, two evidence summaries were permitted to be included. The results are summarized in Table 5.
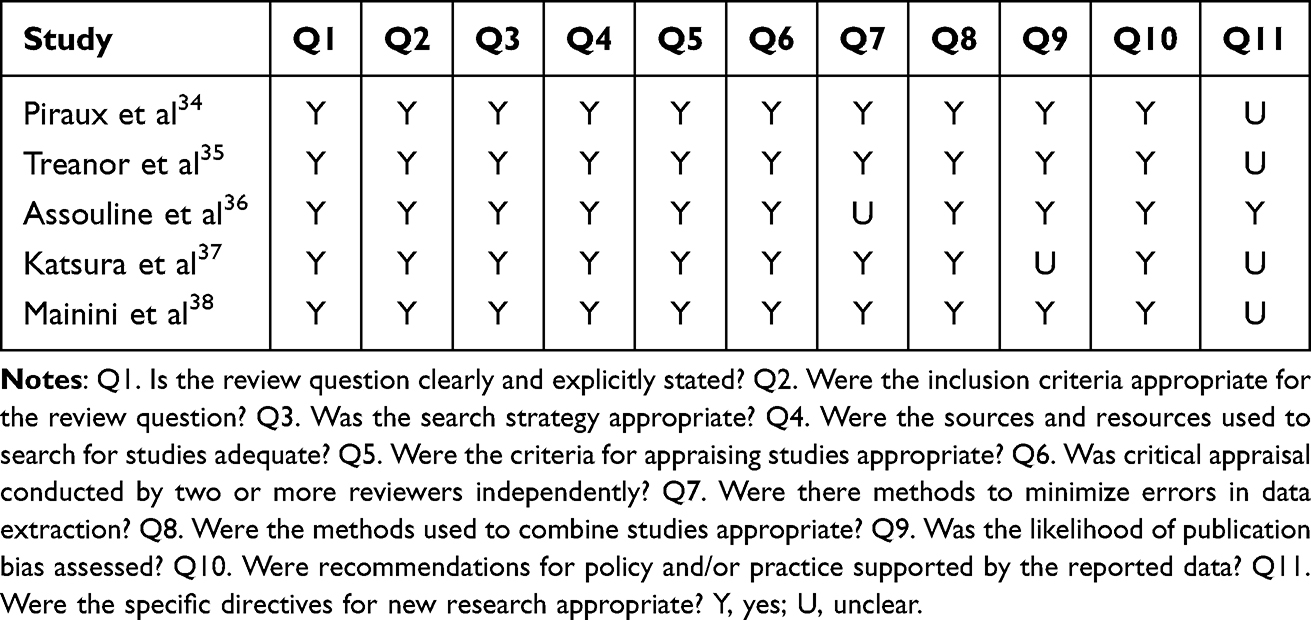 |
Table 5 Quality Evaluation Results of Systematic Reviews From Included Evidence Summaries (n=5) |
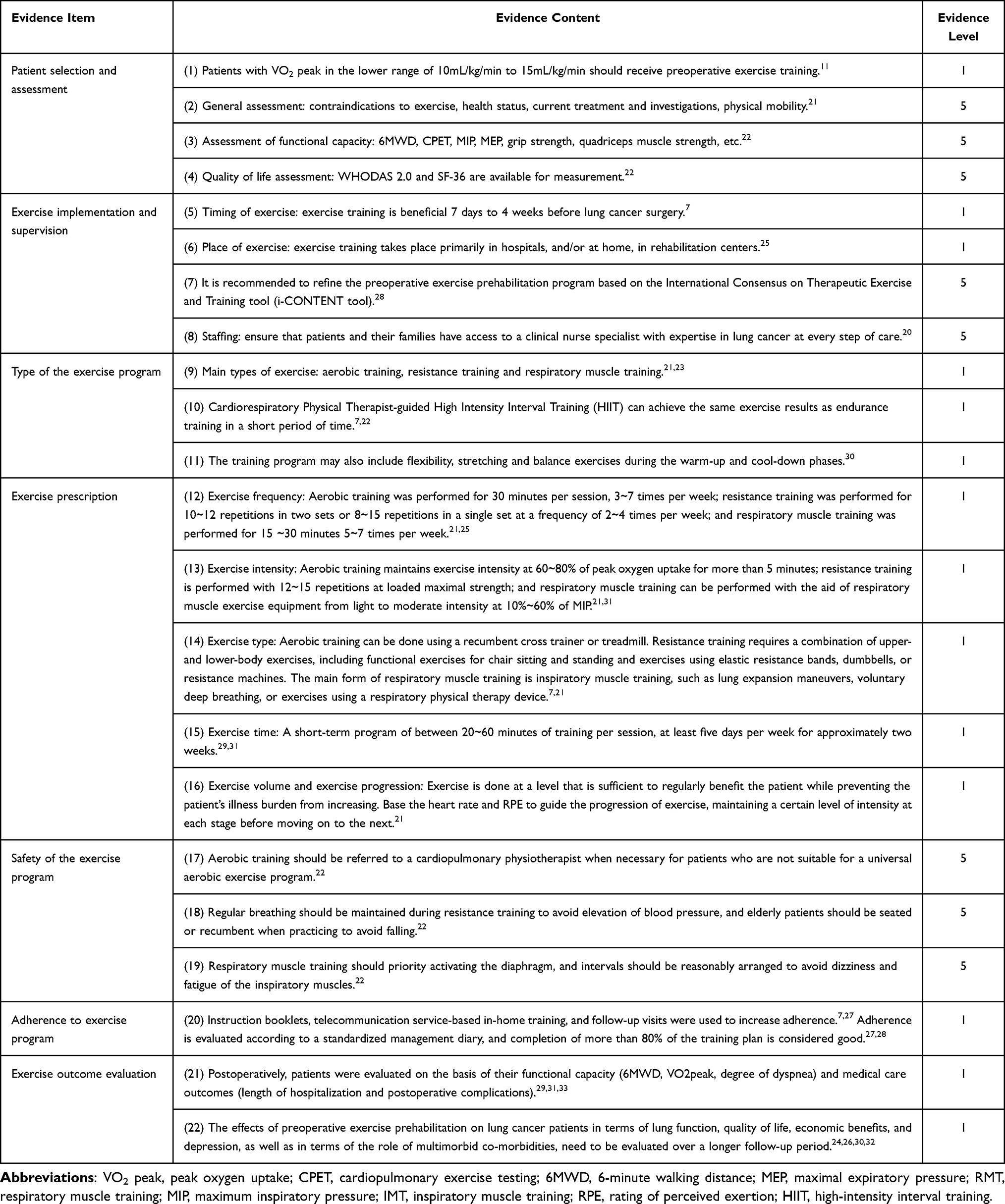 |
Table 6 Summary of the Best Evidence of Preoperative Exercise Prehabilitation in Lung Cancer Patients |
Evidence Summary and Description
After the evidence was summarized by three researchers in a focused discussion and verified by one researcher, a total of 20 pieces of evidence in seven areas were finally arrived at, and the evidence was classified from 1 to 5 according to the JBI evidence pre-grading system, as Table 6.
Discussion
Based on the framework of i-CONTENT tool,39 this study developed a localized summary of the evidence for preoperative exercise prehabilitation based on the seven dimensions of patient selection and assessment, exercise implementation and supervision, type of the exercise program, exercise prescription, safety of the exercise program, adherence to exercise program and exercise outcome evaluation, which is aimed at providing a reference for high-quality, evidence-based exercise therapy programs. This study summarizes the evidence and concludes that patients who are appropriate for preoperative exercise prehabilitation are those with peak oxygen uptake (VO2 peak) in the lower range.11 Ideally, it would be desirable for all patients undergoing elective surgery to undergo preoperative exercise prehabilitation to improve physiological and functional reserve.40 However, patients with lower cardiorespiratory fitness and a higher risk of perioperative complications should be given greater priority for preoperative exercise prehabilitation.41 The main types of exercises are aerobic training, resistance training and respiratory muscle training. High-intensity interval training (HIIT) is also a good option in the preoperative phase when lung cancer patients have limited preparation time. However, it needs to be done under the guidance of a physical therapist, and the patient’s exercise heart rate, blood pressure, and oxygen saturation need to be closely monitored to ensure the patient’s safety, and cannot be done at home.7,22 Furthermore, NICE guidelines recommend that patients and their caregivers receive enhanced assistance by guaranteeing that a clinical nurse specialist with expertise in lung cancer is accessible throughout the entire care process.20 Patient education, adherence assessment, and follow-up necessitate the use of specialist professionals in the form of online supportive training, management diary guidance, and phone communication.42 For it turns out, institutions and departments may want to consider increasing manpower to ensure that preoperative exercise prehabilitation programs are implemented effectively.
With the advancement of the concept of enhanced recovery after surgery, prehabilitation was described as “a range of treatments provided between the diagnosis and surgical treatment of cancer”, has been gradually recognized.43 Current guidelines on rapid rehabilitation for lung cancer patients strongly recommend multimodal prehabilitation in the preoperative phase, including improving exercise capacity.10 Preoperative exercise is the foundation of prehabilitation for lung cancer patients and can reduce healthcare costs by qualifying patients with borderline physical function for surgical treatment and improving perioperative outcomes.13 JBI best practice recommendations entail determining the best program for exercise prehabilitation, including exercise patterns, exercise duration, and exercise intensity.24 Most of the current descriptions of preoperative exercise intervention programs are vague, and the certainty of evidence for all outcomes is suboptimal.28 In this study, we followed the FITT-VP principle and summarized the exercise prescriptions of aerobic training,44 resistance training, and respiratory muscle training, which are easier to be implemented preoperatively in lung cancer patients, based on six factors: exercise frequency, exercise intensity, exercise time, exercise type, exercise volume, and exercise progress. Flexibility exercises, stretching, or balance exercises during the warm-up and cool-down phases can also be used to increase comfort and reduce the risk of exercise injury. We hope that the evidence will further standardize exercise prescription, improve the quality of interventions, and improve patient outcomes after surgery through more precise preoperative exercise prehabilitation.
The process of evidence-based practice is the process of creating and implementing strategies for change in a given clinical situation based on the best available evidence and clinical professional judgment, encouraging evidence translation and scientific decision-making.45 In the process of clinical translation of the evidence related to preoperative exercise prehabilitation, a sound implementation intervention strategy needs to be developed after adequate assessment of potential adopters and practice settings. A plan of action must be constructed for hospital, patient, and specific clinical scenarios during implementation in order to facilitate evidence translation.46 In this study, most of the literature comes from studies in other countries and regions, and in the process of localized clinical practice, it is necessary to fully consider the awareness, attitude, skills, concerns, and practice status of clinical health care workers, and to make adjustments at any time during the application process. In addition, the best evidence needs to be constantly updated and improved as new evidence emerges.47
Conclusion
This study summarized the 22 best evidence which related to preoperative exercise prehabilitation for lung cancer patients, including patient selection and assessment, exercise implementation and supervision, type of the exercise program, exercise prescription, safety of the exercise program, adherence to exercise program and exercise outcome evaluation. To provide an evidence-based basis for preoperative exercise prehabilitation for healthcare professionals, lung cancer patients and family members, and other stakeholder groups. Applicators should apply the evidence according to the feasibility and applicability of the evidence, so as to better provide preoperative exercise prehabilitation programs for lung cancer patients to achieve the best therapeutic outcomes. Currently, the number of relevant high-quality literature is still insufficient. In the future, additional large-sample RCTs and high-quality systematic reviews are needed to provide further evidence for clinical selection. In addition, evidence users need to use the evidence selectively according to the feasibility and suitability of the evidence, so as to formulate appropriate preoperative exercise prehabilitation programs for lung cancer patients.
Funding
This study was funded by Fudan University-Fosun Nursing Research Fund (FNF202436), Nursing Talent Training Program of Huadong Hospital (HLJY2202 and HLXX2202), Shanghai Hospital Development Center Foundation (SHDC12021637).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Thai AA, Solomon BJ, Sequist LV, Gainor JF, Heist RS. Lung cancer. Lancet. 2021;398(10299):535–554. doi:10.1016/s0140-6736(21)00312-3
2. Meyer ML, Peters S, Mok TS, et al. Lung cancer research and treatment: global perspectives and strategic calls to action. Ann Oncol. 2024;35(12):1088–1104. doi:10.1016/j.annonc.2024.10.006
3. Hendriks LEL, Remon J, Faivre-Finn C, et al. Non-small-cell lung cancer. Nat Rev Dis Primers. 2024;10(1):71. doi:10.1038/s41572-024-00551-9
4. National Cancer Center, Lung Cancer Expert Committee of National Cancer Quality Control Center. Quality control index for standardized diagnosis and treatment of lung cancer in China (2022 edition). Chin J Oncol. 2022;44(7):594–599. doi:10.3760/cma.j.cn112152-20220418-00266.
5. Sihoe ADL. Video-assisted thoracoscopic surgery as the gold standard for lung cancer surgery. Respirology. 2020;25(Suppl 2):49–60. doi:10.1111/resp.13920
6. Yang J, Feng J, Ju XX, Cheng Y, Gu Y, Liu X. Construction and preliminary application of exercise rehabilitation program based on patient health engagement model for lung cancer surgery patients. J Nurs Sci. 2022;37(7):1–5. doi:10.3870/j.issn.1001-4152.2022.07.001
7. Xu X, Cheung DST, Smith R, Lai AYK, Lin CC. The effectiveness of pre- and post-operative rehabilitation for lung cancer: a systematic review and meta-analysis on postoperative pulmonary complications and length of hospital stay. Clin Rehabil. 2022;36(2):172–189. doi:10.1177/02692155211043267
8. Zhou N, Ripley-Gonzalez JW, Zhang W, et al. Preoperative exercise training decreases complications of minimally invasive lung cancer surgery: a randomized controlled trial. J Thorac Cardiovasc Surg. 2025;169(2):516–528.e10. doi:10.1016/j.jtcvs.2024.04.009
9. Chinese Society of Surgery, Chinese Society of Anesthesiology. Clinical practice guidelines for enhanced recovery after surgery in China (2021 edition). Chin J Prac Surg. 2021;41(9):961–992. doi:10.19538/j.cjps.issn1005-2208.2021.09.01.
10. Batchelor TJP, Rasburn NJ, Abdelnour-Berchtold E, et al. Guidelines for enhanced recovery after lung surgery: recommendations of the enhanced recovery after surgery (ERAS®) society and the European Society of Thoracic Surgeons (ESTS). Eur J Cardiothorac Surg. 2019;55(1):91–115. doi:10.1093/ejcts/ezy301
11. Granger C, Cavalheri V. Preoperative exercise training for people with non-small cell lung cancer. Cochrane Database Syst Rev. 2022;9(9):Cd012020. doi:10.1002/14651858.CD012020.pub3
12. Sanchez-Lorente D, Navarro-Ripoll R, Guzman R, et al. Prehabilitation in thoracic surgery. J Thorac Dis. 2018;10(Suppl 22):S2593–s2600. doi:10.21037/jtd.2018.08.18
13. Avancini A, Cavallo A, Trestini I, et al. Exercise prehabilitation in lung cancer: Getting stronger to recover faster. Eur J Surg Oncol. 2021;47(8):1847–1855. doi:10.1016/j.ejso.2021.03.231
14. Zhu Z, Hu Y, Xing WJ, Zhou YF, Gu Y. The composition of different types of evidence-based questions. J Nurs Train. 2017;32(21):1991–1994. doi:10.16821/j.cnki.hsjx.2017.21.025
15. Dicenso A, Bayley L, Haynes RB. Accessing pre-appraised evidence: fine-tuning the 5S model into a 6S model. Evid based nurs. 2009;12(4):99–101. doi:10.1136/ebn.12.4.99-b
16. Brouwers MC, Kho ME, Browman GP, et al. AGREE II: advancing guideline development, reporting and evaluation in health care. J Clin Epidemiol. 2010;63(12):1308–1311. doi:10.1016/j.jclinepi.2010.07.001
17. The Joanna Briggs Institute (JBI). JBI Critical Appraisal Checklist for Text and Opinion Papers. 2020. Available from: https://jbi.global/sites/default/files/2020-08/Checklist_for_Text_and_Opinion.pdf.
18. The Joanna Briggs Institute (JBI). Checklist for systematic reviews and research syntheses. 2017. Available from: https://view.officeapps.live.com/op/view.aspx?src=https%3A%2F%2Fjbi.global%2Fsites%2Fdefault%2Ffiles%2F2021-10%2FChecklist_for_Systematic_Reviews_and_Research_Syntheses.docx&wdOrigin=BROWSELINK.
19. Wang CQHY. JBI pre-classification of evidence and levels of recommendations (2014 version). J Nurs Train. 2014;30(11):964–967. doi:10.16821/j.cnki.hsjx.2015.11.002
20. National Institute for Health and Care Excellence. Lung cancer: diagnosis and management. 2024. Available from: www.nice.org.uk/guidance/ng122.
21. Tew GA, Ayyash R, Durrand J, Danjoux GR. Clinical guideline and recommendations on pre-operative exercise training in patients awaiting major non-cardiac surgery. Anaesthesia. 2018;73(6):750–768. doi:10.1111/anae.14177
22. Liu ZJ, Zhang L, Liu HS, et al. Expert consensus on prehabilitation management for enhanced recovery in patients undergoing thoracic surgery (2022). Med J Peking Union Medical College Hospital. 2022;13(3):387–401. doi:10.12290/xhyxzz.2022-0178
23. Wu W, Li H, Fan R. Summary of the best evidence for prehabilitation management of patients with non-small cell lung cancer. Asia Pac J Oncol Nurs. 2024;11(7):100516. doi:10.1016/j.apjon.2024.100516
24. Leaderlou S, Magtoto. Cancer Patients: prehabilitation. 2023. Available from: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=jbi&NEWS=N&AN=JBI21144.
25. Overall B. Postoperative Pulmonary Complications: preoperative Strategies. 2022. Available from: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=jbi&NEWS=N&AN=JBI15884.
26. Del Bianco N, Borsati A, Toniolo L, et al. What is the role of physical exercise in the era of cancer prehabilitation? A systematic review. Crit Rev Oncol Hematol. 2024;198:104350. doi:10.1016/j.critrevonc.2024.104350
27. Liu S, Lu CJ, Wang Y, X XP. The effect of cancer prehabilitation management model on patients with lung cancer surgery: a systematically review. Chin J Rehabil Med. 2021;36(7):838–842. doi:10.3969/j.issn.1001-1242.2021.07.013
28. Voorn MJJ, Franssen RFW, Hoogeboom TJ, et al. Evidence base for exercise prehabilitation suggests favourable outcomes for patients undergoing surgery for non-small cell lung cancer despite being of low therapeutic quality: a systematic review and meta-analysis. Eur J Surg Oncol. 2023;7983(23):90–92. doi:10.1016/j.ejso.2023.01.024
29. Gravier FE, Smondack P, Prieur G, et al. Effects of exercise training in people with non-small cell lung cancer before lung resection: a systematic review and meta-analysis. Thorax. 2022;77(5):486–496. doi:10.1136/thoraxjnl-2021-217242
30. Li X, Yan S, Li S, et al. Impact of preoperative exercise therapy on surgical outcomes in lung cancer patients with or without COPD: a systematic review and meta-analysis. Cancer Manag Res. 2019;11(1):1765–1777. doi:10.2147/cmar.S186432
31. Rosero ID, Ramírez-Vélez R, Lucia A, et al. Systematic review and meta-analysis of randomized, controlled trials on preoperative physical exercise interventions in patients with non-small-cell lung cancer. Cancers. 2019;11(7):944–963. doi:10.3390/cancers11070944
32. Ni HJ, Pudasaini B, Yuan XT, Li HF, Shi L, Yuan P. Exercise training for patients pre- and postsurgically treated for non-small cell lung cancer: a systematic review and meta-analysis. Integr Cancer Ther. 2017;16(1):63–73. doi:10.1177/1534735416645180
33. Sebio Garcia R, Yáñez Brage MI, Giménez moolhuyzen E, Granger CL, Denehy L. Functional and postoperative outcomes after preoperative exercise training in patients with lung cancer: a systematic review and meta-analysis. Interact Cardiovasc Thorac Surg. 2016;23(3):486–497. doi:10.1093/icvts/ivw152
34. Piraux E, Caty G, Reychler G. Effects of preoperative combined aerobic and resistance exercise training in cancer patients undergoing tumour resection surgery: a systematic review of randomised trials. Surg Oncol. 2018;27(3):584–594. doi:10.1016/j.suronc.2018.07.007
35. Treanor C, Kyaw T, Donnelly M. An international review and meta-analysis of prehabilitation compared to usual care for cancer patients. J Cancer Surviv. 2018;12(1):64–73. doi:10.1007/s11764-017-0645-9
36. Assouline B, Cools E, Schorer R, Kayser B, Elia N, Licker M. Preoperative exercise training to prevent postoperative pulmonary complications in adults undergoing major surgery. A systematic review and meta-analysis with trial sequential analysis. Ann Am Thorac Soc. 2021;18(4):678–688. doi:10.1513/AnnalsATS.202002-183OC
37. Katsura M, Kuriyama A, Takeshima T, Fukuhara S, Furukawa TA. Preoperative inspiratory muscle training for postoperative pulmonary complications in adults undergoing cardiac and major abdominal surgery. Cochrane Database Syst Rev. 2015;2015(10):Cd010356. doi:10.1002/14651858.CD010356.pub2
38. Mainini C, Rebelo PF, Bardelli R, et al. Perioperative physical exercise interventions for patients undergoing lung cancer surgery: What is the evidence? SAGE Open Med. 2016;4:2050312116673855. doi:10.1177/2050312116673855
39. Hoogeboom TJ, Kousemaker MC, van Meeteren NL, et al. i-CONTENT tool for assessing therapeutic quality of exercise programs employed in randomised clinical trials. Br J Sports Med. 2021;55(20):1153–1160. doi:10.1136/bjsports-2019-101630
40. Cho AR, Najafi T, Ramanakumar AV, et al. The effect of multimodal prehabilitation on postoperative outcomes in lung cancer surgery. J Thorac Cardiovasc Surg. 2025;169:1631–1644.e2. doi:10.1016/j.jtcvs.2025.02.013
41. Zhao JY, Presley C, Madariaga ML, Ferguson M, Merritt RE, Kneuertz PJ. Prehabilitation for older adults undergoing lung cancer surgery: A literature review and needs assessment. Clin Lung Cancer. 2024;25(7):595–600. doi:10.1016/j.cllc.2024.07.004
42. Lv C, Lu F, Zhou X, et al. Efficacy of a smartphone application assisting home-based rehabilitation and symptom management for patients with lung cancer undergoing video-assisted thoracoscopic lobectomy: a prospective, single-blinded, randomised control trial (POPPER study). Int J Surg. 2025;111(1):597–608. doi:10.1097/js9.0000000000001845
43. Carli F, Silver JK, Feldman LS, et al. Surgical prehabilitation in patients with cancer: state-of-the-science and recommendations for future research from a panel of subject matter experts. Phys Med Rehabil Clin N Am. 2017;28(1):49–64. doi:10.1016/j.pmr.2016.09.002
44. American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription.
45. Zhou YF, Hu Y, Xing WJ, Zhu Z, Chen Y. Promoting evidence-based clinical audit for continuous improvement of clinical quality. Chin J Evidence-Based Med. 2020;20(6):621–627. doi:10.7507/1672-2531.202001003
46. Batchelor J, Hemmert C, Meulenbroeks I, et al. Factors influencing the translation of evidence into clinical practice for hospital allied health professionals in terms of the domains of behaviour change theory: a systematic review. Eval Health Prof. 2024:1632787241285993. doi:10.1177/01632787241285993.
47. Grillo-Ardila CF, Ramírez-Mosquera JJ. Evidence-based medicine and precision medicine: finding the balance between both. Rev Colomb Obstet Ginecol. 2024;75(3). doi:10.18597/rcog.4333
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
An Evidence-Based Medical Review on Promoting Gastrointestinal Function Recovery After Colorectal Cancer Surgery
Zhao CY, Shi WH, Wen ZQ, Jin YM, Shang YB, Zheng L, Li J, Chen XM
Journal of Multidisciplinary Healthcare 2024, 17:1343-1362
Published Date: 23 March 2024
Evidence Summary of Personalized Management of Peritoneal Dialysis Volume in Adults
Yu C, Sha P, Jiang Z, Wei Y, Gong B, Jiang S, Wang R
Journal of Multidisciplinary Healthcare 2025, 18:2707-2719
Published Date: 15 May 2025
Summary of Best Evidence for Psychosocial Interventions in Adults with Alcohol Use Disorder: An Evidence-Based Review
Yan L, Ji CF, Xia LP, Sun W, Shi JQ, Wu XD
Journal of Multidisciplinary Healthcare 2025, 18:6315-6327
Published Date: 2 October 2025
Evidence Summary of Management Strategies for Cognitive Impairment in Patients with Heart Failure
Ni F, Mi W, Wei Y, Li Z, Fan Y, Xi Z
Journal of Multidisciplinary Healthcare 2025, 18:6911-6921
Published Date: 24 October 2025
Best Evidence for Preventing Urinary Tract Infections and Optimizing Care in Adults with Indwelling Urinary Catheters
Tang J, Fan Y, Lu J, Zhang Y
Risk Management and Healthcare Policy 2025, 18:3593-3608
Published Date: 11 November 2025