Back to Journals » Patient Preference and Adherence » Volume 19
Effectiveness of a Short-Term Advance Care Planning Intervention (VOICE) for Dialysis Patients with ESRD: A Randomized Controlled Trial
Authors Xu F, Cheng S ![]() , Shu P
, Shu P ![]() , Liang Y, Chen J, Bai H
, Liang Y, Chen J, Bai H
Received 12 September 2025
Accepted for publication 16 December 2025
Published 22 December 2025 Volume 2025:19 Pages 4191—4206
DOI https://doi.org/10.2147/PPA.S567240
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ramón Morillo-Verdugo
Fang Xu,* Shuang Cheng,* Peng Shu, Yilan Liang, Jie Chen, Haitao Bai
Department of Nephrology, The Central Hospital of Wuhan, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430014, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Haitao Bai, Email [email protected]
Background: Most randomized controlled trials (RCTs) on advance care planning (ACP) focus on advanced cancer, while evidence for dialysis patients with end-stage renal disease (ESRD) remains limited. This study aimed to evaluate the effectiveness of a structured educational intervention in enhancing ACP engagement among dialysis patients.
Methods: The VOICE study, an RCT, was conducted at the Central Hospital of Wuhan. Initially, 117 patients were enrolled; ultimately, data from 50 participants in the intervention group and 52 in the control group were included in the final analysis. Patients in the control group received standard care, while those in the intervention group received a structured ACP intervention specifically tailored to the needs of ESRD patients. The primary outcome assessed in the study was decisional conflict, evaluated through the use of the Decisional Conflict Scale (DCS). Secondary outcomes included ACP engagement (ACPES), attitudes toward death (DAP-R), and quality of life (KDQOL-36™).
Results: After six weeks, the intervention group showed significant but small reductions in the DCS Uncertainty subscale (P = 0.001, Cohen’s d=− 0.17), and improvements in the Informed (P = 0.049, Cohen’s d=− 0.12), Values Clarity (P = 0.003, Cohen’s d=− 0.11), and Effective Decision (P = 0.012, Cohen’s d=− 0.12) subscales. Regarding secondary outcomes, the intervention group demonstrated significantly higher scores across all ACP engagement domains (P < 0.05), reduced fear of death and death avoidance, and greater natural acceptance of death (all P < 0.05). Moreover, the intervention group reported significantly better quality of life, particularly in the Effects of Kidney Disease and Burden of Kidney Disease subscales (P < 0.05).
Conclusion: The VOICE ACP intervention improved short-term ACP engagement and led to modest improvements in several domains of decisional conflict in dialysis patients. Future multicenter, longitudinal trials are warranted to evaluate the sustainability and cost-effectiveness of such interventions.
Trial Registration: Chinese Clinical Trial Registry: ChiCTR2500097890. Registered 27 February 2025.
Keywords: dialysis, advance care planning, decision conflict, engagement, death attitudes, quality of life
Introduction
Chronic kidney disease (CKD) impacts around 8.2% of the population in China, accounting for an estimated 110 million individuals.1 As the condition advances, a significant number of patients advance to end-stage renal disease (ESRD). According to the Chinese National Renal Data System, more than one million people in China currently require dialysis treatment. Patients with ESRD often face considerable physical challenges and elevated mortality risks. They are also frequently confronted with complex medical decisions, such as whether to initiate or continue dialysis therapy.
Advance care planning (ACP) is a structured process through which patients, while mentally competent and informed about their medical condition and prognosis, communicate their treatment preferences based on personal values and life experiences. These discussions typically involve healthcare professionals, family members, or other trusted individuals.2,3 ACP is a fundamental element of palliative care and is broadly documented as a key indicator of high-quality end-of-life care. It prioritizes respect for patient autonomy and facilitates treatment decisions that align with individual preferences. In 2015, the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines suggested that palliative care be integrated into the management of patients with ESRD, regardless of whether dialysis is initiated.4 Central to palliative care, ACP discussions ensure that care plans are consistent with patients’ goals and values. However, both domestic and international studies have shown that awareness of ACP among ESRD patients remains relatively low.5,6 Evidence suggests that implementing ACP interventions can enhance end-of-life quality of life, improve communication of patients with healthcare providers, and shape treatment preferences during the final stages of life.
Although an increasing number of interventions have targeted ACP in non-cancer populations, randomized trials involving CKD or dialysis cohorts remain limited. Most ACP interventions in CKD populations have been feasibility studies, suggesting that nurse-led ACP conversations may enhance patient acceptance and satisfaction but rarely evaluating decisional conflict or ACP engagement.7 Likewise, the multicenter HIGHway project showed that structured ACP tools can improve documentation and patient–provider communication among dialysis patients; however, evidence on decisional conflict or quality-of-life outcomes remains insufficient, and studies conducted in Asian cultural contexts are notably scarce.8 The VOICE intervention was developed to address these gaps. VOICE is a structured, theory-driven program that provides corrective education to improve illness understanding, applies shared-decision principles to translate patients’ values into specific medical choices, and incorporates cultural adaptation with active family participation to enhance fidelity and contextual relevance. VOICE aims to improve ACP engagement and decision quality through two primary mechanisms: (1) offering structured exploration and tailored clarification of illness perceptions to reduce misconceptions about prognosis and treatment trade-offs, thereby decreasing uncertainty and enhancing values clarity; and (2) introducing guided family involvement and shared-decision techniques to redistribute decisional burden, strengthen surrogate preparedness, and support value-concordant medical decisions.
Therefore, the present study seeks to design and implement an ACP-based intervention specifically tailored for ESRD patients in China. The goal is to increase patients’ understanding of ACP, encourage active involvement in medical decision-making, and uphold their right to make autonomous healthcare choices. We hypothesized that the VOICE intervention would reduce decisional conflict and enhance ACP engagement and quality of life compared with standard care.
Methods
Study Design
The Values, Options, Informed Choice, Engagement (VOICE) investigation was a pragmatic randomized controlled trial (RCT), conducted in a single-center, intended to evaluate the impact of an ACP intervention. Ethical approval was attained from the Ethics Committee of the Central Hospital of Wuhan, China (Approval No. WHZXKYL2024-069), and written informed consent was secured from all participants. Moreover, the trial was prospectively registered in the Chinese Clinical Trial Registry (ChiCTR2500097890) and conducted in accordance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines for pragmatic clinical trials.9
Outcomes and Endpoints
The primary endpoint was the change in decisional conflict, measured by the total score of the Decisional Conflict Scale (DCS). Secondary endpoints included: (1) ACP engagement, assessed using the ACP Engagement Survey (ACPES); (2) attitudes toward death, assessed using the Death Attitude Profile–Revised (DAP-R); and (3) health-related quality of life, assessed using the Kidney Disease Quality of Life–36 (KDQOL-36™). All outcomes were measured at baseline and at the 6-week follow-up.
Study Setting and Participants
A convenience sample of ESRD patients undergoing dialysis was recruited from the outpatient department, Central Hospital of Wuhan between February 2025 and August 2025. All participants were receiving routine dialysis treatment at the study site. Additionally, inclusion criteria were: (1) age of 18 or older; (2) identified by their attending physician as meeting the “surprise question” criteria (“Would I be surprised if this patient died within the next year?”, with a response of “No”). To ensure consistent application of this criterion, all attending physicians received brief training on the intent and use of the question prior to the recruitment period; (3) no prior accomplishment of an advance directive (AD); (4) clear consciousness, intact cognitive function, as determined by the attending physician’s clinical judgment and confirmed with a Mini-Mental State Examination (MMSE) score ≥ 24, and the ability to communicate verbally and in writing; and (5) voluntary promise to participate, with signed informed consent. Furthermore, exclusion criteria were as: (1) unwillingness or inability to fully comprehend the study. And, participants were withdrawn from the study if they: (1) voluntarily chose to discontinue or became unable to complete the intervention due to external factors; or (2) experienced a significant clinical deterioration that precluded continued participation.
Randomisation
Patients with ESRD undergoing dialysis were randomly assigned in a 1:1 ratio to either the intervention group (receiving ACP discussions) or the control group (receiving standard care). The randomization sequence was computer-generated by a researcher who was independent of the intervention process. A fixed block size of four was used to ensure balanced allocation, and no stratification factors (eg, dialysis modality) were applied. Group allocation was conducted through a centralized, web-based randomization system by a separate researcher not involved in outcome assessment, thereby ensuring proper allocation concealment.
Blinding
Because of the nature of the ACP intervention, blinding of participants and intervention providers was not feasible. However, outcome assessment and data analysis were blinded. The principal investigators and outcome assessors remained unaware of group assignments throughout the trial, and all statistical analyses were conducted by an independent researcher who was blinded to allocation. The randomization key was held by an independent coordinator and was not released until the database had been locked for final analysis.
Sample Size
Determination of the sample size was guided by the primary outcome variable, the Decisional Conflict Scale (DCS). Using PASS 2023 software (NCSS, LLC, Kaysville, Utah, USA), the calculation assumed a two-sided significance level (α) of 0.05, a statistical power of around 90%, and an effect size estimated from a previous pilot study.10 The results indicated that 49 participants per group were required. To account for a potential 10% attrition rate, the final target sample size was increased to 54 participants per group, yielding a total of 108 patients.
Intervention
Formation of the Intervention Team
To ensure smooth implementation of the study, a dedicated project team was established. The team comprised one head nurse from the Department of Nephrology and one from the Hemodialysis Center, both serving as project supervisors; one attending nephrologist responsible for disease diagnosis and basic treatment; and three nurses tasked with delivering the intervention and managing study data.
Before the start of the study, all research personnel underwent a standardized 12-hour training program to ensure consistency in intervention delivery. The program was led by the principal investigators and included weekly supervision meetings throughout the study period to address challenges and maintain protocol adherence. Training focused on the study protocol, intervention procedures, and administration of the survey instruments. Specific training content included:
(1) core concepts and ethical principles of ACP;
(2) use of semi-structured interviews to facilitate conversations;
(3) understanding of essential medical legal documents (eg, living wills, healthcare proxy forms);
(4) common communication challenges and strategies to address them;
(5) examples of key discussion topics and suggested communication prompts;
(6) procedures for documentation and record-keeping.
Development and Implementation of the Intervention Protocol
The VOICE intervention was established based on two foundational theoretical frameworks: Illness Representations Theory11 and the Shared Decision-Making (SDM) model.12 Illness Representations Theory aids in exploring how patients and their family members perceive the illness and its prognosis, helping to identify misconceptions or cognitive biases that may hinder informed decision-making. The SDM model promotes a collaborative approach by integrating clinical expertise with patients’ personal values and preferences, ensuring that healthcare decisions genuinely reflect the patient’s goals. It emphasizes active participation from healthcare providers and patients and their family members in the decision-making process. Guided by these frameworks, the VOICE intervention protocol included five structured components: (1) assessment of illness understanding, (2) clarification of goals and concerns, (3) introduction of treatment options, (4) summary and clarification of information, and (5) establishment of care goals. To enhance transparency and reproducibility, the intervention description adhered to the TIDieR (Template for Intervention Description and Replication) checklist.13 Before the main trial, the protocol was pilot-tested with three patients to assess feasibility, which informed iterative refinements to the intervention content. The final structure and components of the VOICE intervention are summarized in Table 1.
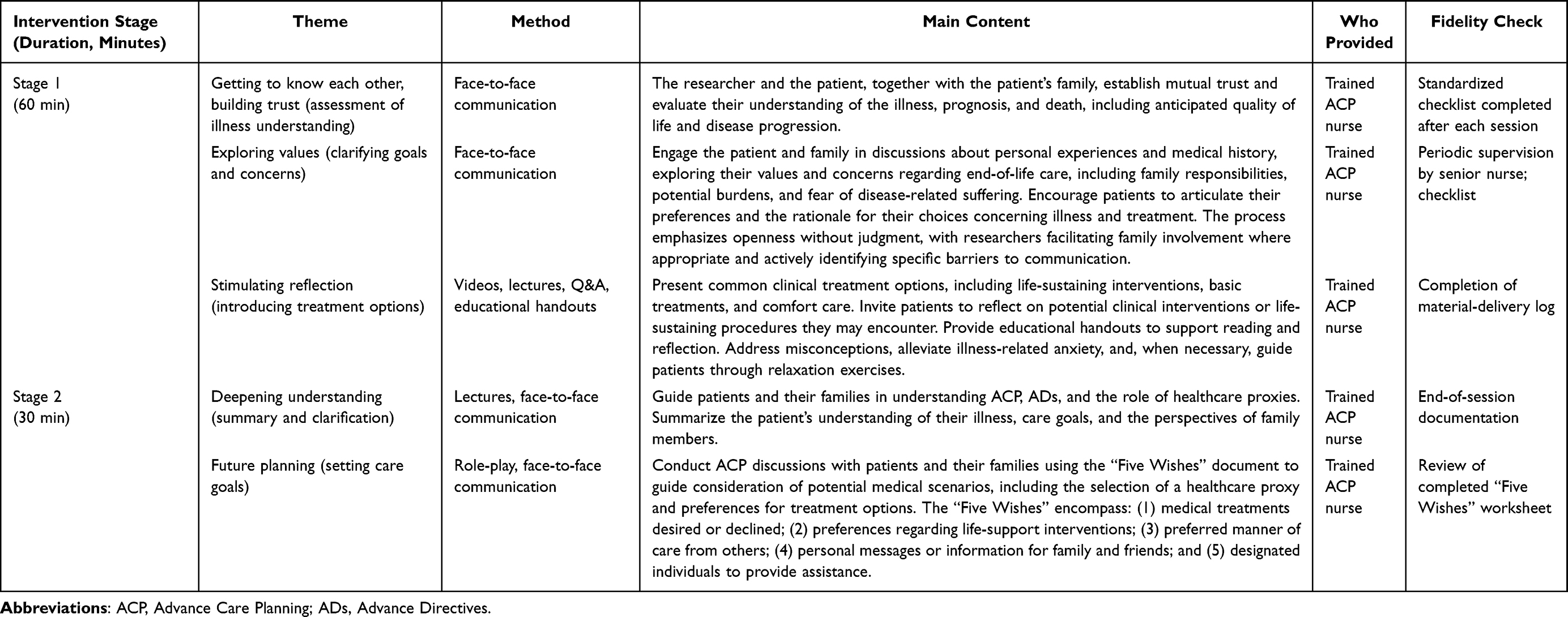 |
Table 1 Summary of the ACP Intervention Protocol for Dialysis Patients with ESRD |
In this study, the intervention comprised two sequentially structured sessions conducted with patients and their family members. The content and duration of each session were flexible within predefined guidelines, allowing for adjustments based on the patient’s emotional state, personal values, and individual needs. Researchers meticulously documented patients’ responses following each session. The second session, scheduled approximately 2~3 weeks after the initial meeting, began with a review of the patient’s reflections and experiences from the first conversation, providing a natural and thoughtful transition. The intervention incorporated multiple materials, including educational videos, printed ACP handouts, and the “Five Wishes” document to guide discussions. All sessions were conducted in quiet, private rooms to ensure comfort and confidentiality. The study was conducted between February and August 2025, and no adaptations related to COVID-19 were required. A schematic timeline summarizing screening, randomization, VOICE sessions, and outcome assessments is provided in Figure 1.
 |
Figure 1 Timeline of Study Procedures. |
Intervention Fidelity and Ethical Safeguards
To ensure intervention fidelity, the nurse completed a self-evaluation checklist after each session. The checklist recorded session duration, verified that all core topics were addressed, and documented any deviations from the protocol. Along with standardized training and a detailed intervention manual, these procedures minimized inter-provider variability and supported consistent delivery. To reduce contamination between groups, all VOICE sessions were conducted as one-to-one interviews in a private consultation room, separate from the dialysis area, and no group-based ACP activities were offered. Participants in the intervention group were also reminded not to share session content with other patients. Because ACP discussions and conversations about death attitudes may evoke emotional distress, specific ethical safeguards were implemented. Before each session, participants were informed that they could decline any question, pause the conversation, or stop the session at any time without affecting their routine care. During the sessions, nurses continuously monitored for verbal and non-verbal indicators of distress (eg, tearfulness, pronounced anxiety, agitation). If significant distress was observed, the discussion was paused or redirected, supportive listening and reassurance were provided, and referral to psychological counselling services or the attending nephrologist was offered when appropriate.
Intervention for the Control Group
The control group received standard ACP care, which was primarily delivered by the patients’ usual clinical team (nephrologists and dialysis nurses) throughout the study period. The research team’s interaction was limited to providing patients and their families with general education on the disease and guidance on maintaining a healthy lifestyle. Participants were also given a written document on ADs, which typically outlines how individuals can communicate their care preferences and appoint a healthcare proxy in the event that they lose decision-making capability. While researchers offered a brief standardized 5-minute explanation of the document’s content, they did not engage in detailed discussions about patients’ personal attitudes, treatment preferences, or decisions regarding proxy designation. Furthermore, to prevent contamination, the research team did not provide any structured psychosocial support related to end-of-life issues.
Measurements
Demographic and Clinical Characteristics
A structured questionnaire was used to collect sociodemographic data, including gender, age, marital status, and educational level. It also captured the number of hospitalizations in the past two years and assessed participants’ prior awareness of ACP and familiarity with ADs.
Decision Conflict
The Decision Conflict Scale (DCS), constructed by Canadian scholar O’Connor in 1995,14 is a validated instrument utilized to assess an uncertainty of an individual in taking healthcare decisions, the adjustable factors that add to the uncertainty, and the decision’s perceived quality. The DCS has been translated and validated in different languages, such as Mandarin,15 and comprises five subscales: Uncertainty, Informed, Values Clarity, Support, and Effective Decision. Each item was measured on a 5-point Likert scale, which ranged from “strongly agree” (scored 0) to “strongly disagree” (scored 4). Total scores are standardized on a 0–100 scale, with 0 suggesting no decisional conflict and 100 representing extremely high conflict. Because no universally accepted minimal clinically important difference (MCID) has been established for the DCS, the clinical relevance of score changes was interpreted using recommended threshold values: a score larger than 25 implies the existence of decisional conflict, whereas values above 37.5 could signal a delay in decision-making or substantial uncertainty during the decision-making process. Higher scores reflect larger decisional conflict and a poorer overall decision-making experience. In this study, the scale demonstrated good internal consistency, with a Cronbach’s α of 0.942. The study protocol also pre-specified analysis of the five DCS subscales as secondary outcomes to enable domain-specific interpretation of the intervention effects.
ACP Engagement
The Chinese version of the ACP Engagement Survey (ACPES), originally constructed by Sudore et al16 in 2013, is designed to assess individuals’ engagement in ACP across four key domains: Surrogate Decision-Makers (SDMs), Quality of Life (conversing personal goals and values with clinicians and the SDM), Decision Flexibility (determining the level of autonomy granted to the SDM), and Clinical Inquiry (asking clinicians questions to support informed decision-making). Liu et al17 subsequently adapted this tool for use among Chinese community-dwelling older adults with chronic illnesses. The adapted version consists of 34 items categorized into four dimensions: Self-efficacy, Knowledge, Readiness, and Contemplation, each rated on a 5-point Likert scale. The instrument demonstrated strong psychometric properties, with an overall Cronbach’s α of 0.817, signifying good internal consistency. Internal reliability in the present sample was high, with a Cronbach’s α of 0.941.
Death Attitude
The Death Attitude Profile–Revised (DAP-R), originally created by Wong et al in 1994,18 is a validated tool designed to measure individuals’ attitudes toward death, encompassing both negative and positive viewpoints. It includes 32 items categorized into five dimensions: Death Avoidance, comprising 5 items; Fear of Death, with 7 items; Escape Acceptance and Neutral Acceptance, each consisting of 5 items; and Approach Acceptance, which includes 10 items. Among these, fear of death and death avoidance indicate negative perceptions, whereas escape acceptance, approach acceptance, and neutral acceptance reflect more positive orientations. Responses are collected using a 5-point Likert scale, from “strongly disagree” (1) to “strongly agree” (5), where elevated scores denote stronger agreement with the stated attitude. The Mandarin adaptation, translated by Tang et al19 showed robust psychometric validity, achieving a Cronbach’s alpha of 0.875 and a split-half reliability of 0.864, confirming solid internal consistency and measurement reliability. The scale demonstrated good internal consistency in this study (Cronbach’s α = 0.863).
Quality of Life
The Kidney Disease Quality of Life-36 (KDQOL-36™) is a condition-specific tool designed to assess health-related quality of life (HRQoL) in CKD patients, especially those receiving dialysis treatment. It comprises five key dimensions: the Physical Component Summary, which includes items 1 to 6; the Mental Component Summary, covering items 7 to 12; Burden of Kidney Disease (BKD), assessed through items 13 to 16; Symptoms and Problems Related to Kidney Disease, reflected in items 17 to 28; and Effects of Kidney Disease (EKD), represented by items 29 to 36. The Cronbach’s α coefficients for these subscales range from 0.69 to 0.78,20 indicating acceptable to good internal consistency. According to the official scoring manual, each item is converted to a 0–100 scale, depending on the number of response categories, with certain items reverse-scored as appropriate. Each dimension’s score is derived by computing the average of its related items, where a higher value specifies a better quality of life. Reliability in our sample was strong, with a Cronbach’s α of 0.936.
Data Collection Procedure
Participants completed all questionnaires at two time points: baseline (before the intervention) and the 6-week follow-up. To ensure consistency and accuracy in responses, all participants were guided by standardized instructions. When participants experienced difficulty understanding or answering items, researchers provided clarifications as needed. For those unable to complete the questionnaires independently, researchers conducted objective, face-to-face interviews, carefully recording participants’ responses. Upon collection, each questionnaire was immediately reviewed for omissions or inaccuracies. Any discrepancies were promptly addressed and corrected on site to ensure the completeness and validity of the data.
Statistical Analysis
Data analysis was carried out by a blinded researcher (PS) who remained unaware of the participants’ group allocation (control vs intervention). Primary analyses were conducted per protocol, including the 102 participants who completed the full study procedures and provided 6-week outcome data. Given the low attrition rate and the absence of outcome data for the few withdrawals, complete-case analyses were performed without imputation. All statistical analyses were conducted utilizing SPSS software, version 26.0. The distribution of continuous variables was examined using the Shapiro–Wilk test and inspection of histograms, while homogeneity of variances between groups was assessed with Levene’s test. Baseline demographic and clinical variables were compared between the two groups utilizing independent t-tests for continuous data, while Chi-squared or Fisher’s exact tests were applied for categorical comparisons. The Mann–Whitney U-test was utilized to examine intergroup differences in ACP engagement, decision conflict, and attitudes toward death. Within-group pre- and post-intervention comparisons were assessed utilizing the Wilcoxon signed-rank test. For the major outcomes, we also reported effect sizes for between-group differences, expressed as Cohen’s d and calculated using group means and pooled standard deviations, with corresponding 95% confidence intervals. In exploratory analyses, ANCOVA models were applied to assess whether intervention effects on DCS total scores and ACP engagement varied by age. Age was dichotomized (<65 vs ≥65 years), and each model included group, age category, the group × age interaction, and the relevant baseline score as a covariate. All tests were two-sided, with statistical significance set at p < 0.05.
Results
A total of 117 patients were enrolled, with 54 participants allocated to each of the intervention and control groups. During the course of the study, 6 participants withdrew, resulting in 102 individuals who completed the full study protocol (intervention group: n = 50; control group: n = 52). The flow of participants through the trial, including numbers screened, randomized, lost to follow-up, and analyzed, along with reasons for attrition, is summarized in the CONSORT diagram (Figure 2). In the intervention group, three participants withdrew voluntarily, and one was lost due to clinical deterioration. In the control group, two participants withdrew voluntarily. Baseline characteristics of the two groups are presented in Table 2. The mean age of participants was 64.76 years (SD = 6.05), and 56.9% were male. The majority of participants (71.6%) were currently married. Only 4.9% had previously heard of ACP, and 13.7% were aware of ADs. Furthermore, 69.6% of participants had experienced at least one hospitalization in the past two years. Statistical analysis revealed no significant variances between the control and intervention groups in terms of sociodemographic or clinical health characteristics.
 |
Table 2 Baseline Characteristics of Patients |
 |
Figure 2 Flow of participants through the trial. |
In the intervention group, 50 of the 54 patients randomized to the VOICE arm (92.6%) attended both planned sessions and completed the assessment. In the control group, 52 of the 54 patients (96.3%) completed the assessment. The average duration of the first intervention session was 96 minutes (range: 62–134 minutes), while the second session lasted an average of 62 minutes (range: 34–93 minutes). Overall, this corresponded to a mean total nurse time of approximately 158 minutes per participant for delivering the two VOICE sessions. Participant satisfaction was not formally measured using a standardized questionnaire; however, informal feedback during and after the sessions suggested that most participants found the VOICE conversations acceptable and helpful. Regarding the primary outcome, no significant variances were noted between the control and intervention groups at baseline across all DCS subdomains (all P > 0.05; Table 3). However, following the intervention, the intervention group showed a significantly lower score on the Uncertainty subscale compared to the control group (95% CI: –5.852 to –1.690, P = 0.001; Table 3). Similar reductions were noted in the Informed subscale (95% CI: –3.078 to –0.005, P = 0.049) and the Values Clarity subscale (95% CI: –3.799 to –0.829, P = 0.003). Furthermore, the Effective Decision subscale score was significantly improved in the intervention group (95% CI: –3.648 to –0.471, P = 0.012). In contrast, no statistically significant difference was noted between groups in the Support subscale (P = 0.626). In the intervention group, the DCS total score decreased from 33.38 ± 13.86 to 30.63 ± 12.78 (absolute change −2.74 points; relative change −8.2%). In the control group, it decreased from 33.00 ± 13.85 to 31.19 ± 13.33 (absolute change −1.82 points; relative change −5.5%; Table 3).
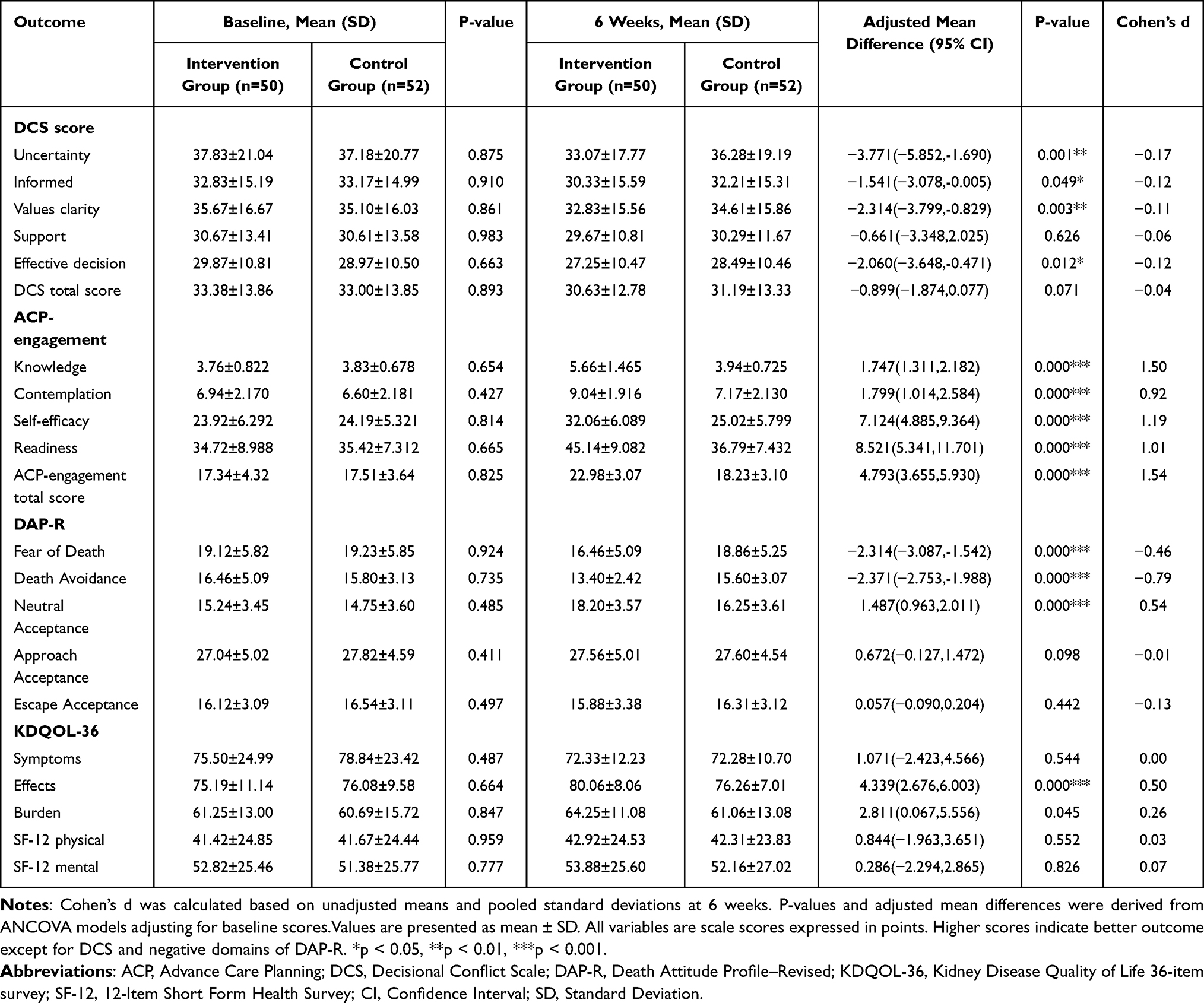 |
Table 3 Outcome Measure Scores at Baseline and 6 Weeks (Mean ± SD) |
Regarding secondary outcomes, the mean score on the four-item ACPES was significantly higher in the intervention group relative to the control group after exposing to the intervention (P < 0.001; see Table 3). In the intervention group, the ACP engagement total score increased from 17.34 ± 4.32 at baseline to 22.98 ± 3.07 at 6 weeks, an absolute improvement of 5.64 points (approximately 32.5%). In contrast, the control group showed only a modest change, with scores increasing from 17.51 ± 3.64 to 18.23 ± 3.10 (absolute change 0.72 points; relative change about 4.1%; Table 3). In terms of attitudes toward death, no statistically significant variances were revealed between the groups in the Approach Acceptance and Escape Acceptance dimensions (P > 0.05). However, participants in the intervention group exhibited significantly lower scores on the Fear of Death and Death Avoidance subscales, along with a significantly higher score in the Neutral Acceptance dimension after the intervention (P < 0.05; Table 3). With respect to quality of life, the intervention group showed significant improvements in the EKD and BKD subscales compared to the control group (P < 0.05; Table 3). In contrast, no significant between-group differences were found in the Symptoms of Kidney Disease subscale (P = 0.544), or in the Physical Component Summary and Mental Component Summary scores (P = 0.552 and P = 0.826, respectively).
In exploratory ANCOVA models adjusting for baseline scores, there was no evidence that the intervention effect varied by age. For DCS total scores, the interaction between group and age category (<65 vs ≥65 years) was not statistically significant (p = 0.517). Similarly, for ACP engagement, the group × age interaction was non-significant (p = 0.665), indicating that intervention effects were comparable across age groups.
Discussion
This randomized controlled trial demonstrated that, compared with standard ACP care, the structured VOICE intervention produced meaningful reductions in several DCS subdomains, and improved ACP-related and psychosocial outcomes among dialysis patients with ESRD. At six weeks, intervention participants showed modest reductions in total DCS scores, particularly in the uncertainty, informed decision-making, and values-clarity subscales. They also reported higher ACP engagement, especially in knowledge, contemplation, self-efficacy, and readiness. Favourable changes were further observed in selected dimensions of death attitudes and disease-related quality of life. However, because these outcomes were measured only six weeks post-intervention, the durability of these effects remains unclear, highlighting the need for longer-term follow-up.
Overall, the results indicate several pathways through which the VOICE intervention may operate. By encouraging patients and family members to examine their understanding of end-stage renal disease and dialysis, and by providing tailored prognostic information, the intervention likely corrects misconceptions and reduces uncertainty, central elements in models of illness representation. Structured conversations with nephrology nurses and family members create a protected setting in which patients can clarify values and preferences and practice shared decision-making. Within this context, patients gain knowledge, confidence, and a greater sense of readiness to participate in ACP. Increased ACP engagement likely mediates the reduction in decisional conflict by improving values clarification, decreasing uncertainty, and enhancing perceived control over care decisions. Improved engagement may also shift death attitudes from fear or avoidance to a more neutral or accepting orientation, as patients feel better prepared for end-of-life decision-making. Although formal mediation analyses were not conducted, these patterns align with the conceptual models of illness representation and shared decision-making that underpin the VOICE intervention.
Although ACP has a long history and well-established initiatives in Western countries,21 its implementation in Asian societies, including mainland China, encounters substantial cultural and systemic barriers. Major obstacles include pervasive death taboos, family-centered decision-making practices that may override patient autonomy, and the absence of supportive legislation. In contrast to mainland China, regions such as Hong Kong and Taiwan have made earlier and more structured progress in implementing ACP. For example, Taiwan legally recognized patients’ right to refuse life-sustaining treatment as early as 2000.22 In Hong Kong, the Law Reform Commission released a report in 2006 titled Substitute Decision-Making and ADs about Medical Treatment, which recommended promoting ADs within the existing common law framework.23 By contrast, mainland China continues to face significant barriers due to the absence of clear legal frameworks, leading to hesitation and uncertainty among healthcare professionals regarding the implementation of ACP. This legal ambiguity also fosters skepticism among patients about the validity and practicality of ACP in clinical settings. A nationwide survey involving 6,628 individuals in mainland China found that only 17.8% had previously heard of ACP. However, once informed, 68.3% expressed a willingness to create an ACP, indicating low public awareness but a generally positive attitude and high potential acceptance of ACP.24 Similarly, although hemodialysis patients demonstrate limited knowledge of ACP and ADs, they often hold positive attitudes and express strong interest in future participation.25 Through targeted ACP interventions, patients and their families can be supported in engaging in meaningful medical decision-making conversations, thereby facilitating alignment between individual values and treatment plans.8
In end-of-life care, the preparedness of both patients and their designated SDMs plays a crucial role in ensuring that medical decisions are of high quality and aligned with patients’ values and goals. The DCS is one of the most widely used tools to evaluate uncertainty in decision-making among patients and surrogates.26 Findings from the present study revealed significant improvements in decisional conflict scores following the intervention, with the exception of the Support subscale, a result consistent with the findings reported by Saeed et al.10 Similarly, in a study by Song et al27 the Sharing Patients’ Illness Representations to Increase Trust intervention significantly reduced decisional conflict in both patients and caregivers, with marked reductions in DCS scores at follow-up. In another study, an interactive, web-based decision aid tailored for CKD older adults effectively decreased decisional conflict, especially in the Informed and Values Clarity subscales, while also promoting preference-concordant care such as increased consideration of conservative management and ACP documentation.28 High levels of decisional conflict have been associated with regret, anxiety, poor treatment adherence, and unfavorable health outcomes. In the context of CKD, which often involves complex medical decisions and significant lifestyle implications, improvements in DCS scores may serve as a key indicator of enhanced decision quality and patient-centered care.
Multimorbidity, polypharmacy, and frailty are common among patients with ESRD and have a profound impact on their functional status, psychological well-being, and social engagement, ultimately diminishing their quality of life. For older adults approaching ESRD, it is imperative to engage in SDM that allows for the careful consideration of treatment options.29 In the study by Saeed,10 palliative care interventions led to improvements only in the BKD subscale of the KDQOL-36 instrument. In contrast, our study demonstrated that the VOICE intervention significantly improved both the EKD and BKD subscales. However, evidence on the effectiveness of ACP in improving quality of life remains mixed, with a large trial in advanced cancer patients reported no significant effect,30 likely because the primary aim of ACP is to improve psychological preparedness and ensure that care aligns with patient values, rather than directly alleviating physical symptoms.31
Regarding ACP engagement, our findings revealed that post-intervention scores for Readiness, Self-efficacy, Contemplation, and Knowledge were significantly higher in the intervention group relative to the control group. As such, these results underscore the effectiveness of a multifaceted intervention strategy, including face-to-face discussions, educational booklets, and health seminars, in cultivating a more positive attitude toward ACP among patients with ESRD, thereby enhancing overall engagement. Supporting this, a RCT conducted across dialysis clinics in five US states also confirmed that ACP interventions can improve end-of-life decision-making during the terminal phase of illness.27 A key component of successful ACP interventions lies in raising awareness and deepening understanding of ACP-related concepts. The lack of knowledge about the definition and objectives of ACP has been widely recognized as a major barrier to initiating such discussions. Educating patients about the principles, importance, and implications of ACP can strengthen both their behavioral intention and willingness to engage in meaningful conversations.24 Enhanced understanding not only leads to more frequent and comprehensive ACP discussions but also increases the completion of ACP documentation and the designation of SDMs.32 In our study, the majority of patients were in the precontemplation stage before the intervention, consistent with the findings of Tan’s meta-analysis.33 Among various ACP-related behaviors, participants demonstrated the greatest readiness to discuss the trade-off between quality and quantity of life with healthcare providers, family members, or loved ones. Although many participants were unfamiliar with the specific term “ACP,” a substantial proportion had already engaged in related behaviors, such as discussing care preferences with physicians or family and reflecting on the meaning of life. In the Chinese context, the observed increase in ACP engagement must be understood within a strongly family-centred and collectivist cultural framework. Decisions regarding life-sustaining treatment are typically negotiated within the family rather than determined solely by the patient, and individuals often consider not only their own preferences but also perceived filial duties and the need to preserve family harmony. By explicitly including family members in the VOICE conversations, the intervention likely served as a form of family mediation, facilitating a relational decision-making process consistent with the concept of Confucian relational autonomy. This gradual alignment of patient preferences with family expectations may account for the enhanced ACP engagement, rendering such discussions more acceptable and feasible in clinical practice. Death attitude refers to an individual’s psychological response, evaluative stance, and internal disposition toward death. In this study, patients in the intervention group reported significantly lower scores in the dimensions of fear of death and death avoidance, while showing significantly higher scores in natural acceptance compared to the control group. However, no statistically significant differences were noted between the two groups in the dimensions of approach acceptance and escape acceptance. Patients with ESRD often undergo long-term dialysis, which is frequently accompanied by physical discomfort and psychological distress, potentially contributing to negative emotional responses toward death. ACP interventions appear to mitigate such responses by reducing fear and avoidance of death, while simultaneously promoting natural acceptance. Supporting this, a study involving 965 older adults in Chinese communities identified a significant negative correlation between death anxiety and ACP engagement, indicating that higher levels of death anxiety are associated with lower readiness to participate in ACP discussions.34 These findings suggest that open dialogue and targeted psychological interventions can play a crucial role in enhancing death acceptance among seriously ill patients. Consequently, healthcare providers must remain attentive to the psychological dimensions of terminal illness and be proactive in offering timely support, such as life review therapy, counseling, or relaxation training, to help patients develop a more balanced and constructive understanding of death.
Patients with ESRD often require long-term dialysis, whether through hemodialysis or peritoneal dialysis, both of which place significant physical, psychological, and social burdens on patients and their families. In this study, patients with longer disease duration and advanced age demonstrated a greater openness toward ACP discussions. This trend suggests that as patients age, there is a discernible shift in priorities, from life extension toward quality of life, resulting in increased receptiveness to ACP. However, the interaction between age and ACP engagement was not statistically significant, suggesting that although older adults may be more receptive to ACP discussions, other factors, such as individual health status and family dynamics, likely exert a stronger influence. Similarly, no significant gender differences in ACP engagement were observed, although studies with larger samples are needed to determine whether more subtle gender-related variations in ACP readiness exist. However, during the intervention phase, we encountered widespread misconceptions among patients and their families. Many mistakenly equated ACP with the promotion of withdrawing life-sustaining treatments, which fostered resistance to ACP conversations and reluctance to engage in SDM planning. These findings underscore the importance of dispelling myths surrounding ACP through culturally sensitive and diversified educational strategies aimed at improving awareness and understanding among both patients and their families. For patients who are emotionally vulnerable, direct references to “death” or other emotionally charged language should be avoided. Instead, ACP conversations should adopt a patient-centered approach, emphasizing individual values, expectations, and preferences for care near the end of life. Additionally, social support, particularly emotional support from family members and close friends, emerged as a key factor in influencing ACP engagement. Such support not only increases patients’ willingness to participate in ACP discussions but also enhances their receptivity to the planning process.35 Involving family members in these discussions promotes shared understanding and empowers patients to make informed, values-congruent medical decisions, thereby safeguarding their autonomy and dignity.
The findings of this trial indicate that the VOICE intervention is both feasible and acceptable for dialysis patients with ESRD and could be incorporated into routine clinical practice. First, ACP discussions can be scheduled alongside regular dialysis sessions, thereby minimizing additional burden for patients and clinicians. Second, telemedicine platforms or mobile health applications could facilitate digital ACP engagement, improving convenience and expanding access, particularly for patients in rural or underserved settings. Finally, although the intervention requires considerable nursing time and resources, its potential to enhance end-of-life decision-making and reduce decisional conflict may yield long-term cost savings through fewer hospitalizations, fewer emergency interventions, and improved quality of end-of-life care.
Limitations
ACP interventions have the potential to enhance engagement among dialysis patients with ESRD, carrying significant implications for improving the quality of end-of-life care. However, this study presents several limitations. Firstly, although ACP is inherently a dynamic and evolving process, the current study employed a short-term follow-up design without longitudinal follow-up, thereby limiting the ability to evaluate long-term outcomes related to end-of-life care. As such, the sustained impact of the intervention on actual end-of-life decisions and care delivery remains uncertain. Secondly, while most patients in the intervention group had family members involved in ACP discussions, the study did not assess outcomes concerning the family members themselves. Future prospective cohort studies are needed to examine the enduring effects of ACP interventions, not only on patients but also on their families, particularly in terms of psychological well-being after the patient’s death, including levels of anxiety, depression, and post-traumatic distress. In addition, although the VOICE sessions were delivered by trained nurses using a standardized protocol and checklists, we did not conduct independent fidelity assessments or evaluate inter-rater reliability, which should be incorporated into future implementation studies. A further limitation is the potential for measurement bias, as all primary outcomes were based on self-reported questionnaires rather than observer-rated or clinician-assessed endpoints. Self-report measures may be influenced by emotional state, social desirability, or misinterpretation of items, potentially affecting the accuracy of the observed changes. Moreover, the single-center design and cultural homogeneity of the sample limit the generalizability of the findings to other healthcare settings or cultural contexts. Finally, the statistical model did not adjust for potential confounders such as education, income, or disease duration, which may shape ACP engagement and decision-making outcomes. Future studies should account for these variables to improve understanding of how ACP interventions function across diverse populations.
Conclusion
This RCT demonstrated that the structured ACP intervention enhanced clarity in medical decision-making and improved ACP engagement among dialysis patients with ESRD, with modest reductions observed in overall decisional conflict and significant improvements in specific decisional conflict domains. The intervention also improved ACP engagement and facilitated more effective communication between patients and healthcare providers. Although these short-term benefits were clear, multicenter studies with longer follow-up periods are needed to evaluate the sustainability and cost-effectiveness of the intervention.
Data Sharing Statement
The data underlying this study can be obtained from the Ethics Committee of the Central Hospital of Wuhan. However, access is restricted and not available to the public. Interested parties may request the data from the corresponding author, subject to approval by the Ethics Committee.
Ethics Statement
This study received ethical clearance from the Ethics Committee of the Central Hospital of Wuhan, China (Approval No. WHZXKYL2024-069). All procedures complied with the Declaration of Helsinki, and written informed consent was secured from each participant before enrollment.
Acknowledgments
We gratefully acknowledge all the participants who took part in this study for their valuable time and contributions. We also extend our sincere thanks to the Central Hospital of Wuhan for its continuous support throughout the project.
Funding
The authors acknowledge the financial support received for the research, authorship, and/or publication of this article. This work was supported by the Central Hospital of Wuhan under (Grant No. 23YJ55).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang L, Xu X, Zhang M, et al. Prevalence of chronic kidney disease in china: results from the sixth china chronic disease and risk factor surveillance. JAMA Intern Med. 2023;183(4):298. doi:10.1001/jamainternmed.2022.6817
2. Mori M, Chan HYL, Lin C-P, et al. Definition and recommendations of advance care planning: a Delphi study in five Asian sectors. Palliat Med. 2025;39(1):99–112. doi:10.1177/02692163241284088
3. Chiu HHL, Murphy-Burke DM, Thomas SA, et al. Advancing palliative care in patients with CKD: from ideas to practice. Am J Kidney Dis. 2021;77(3):420–426. doi:10.1053/j.ajkd.2020.09.012
4. Davison SN, Levin A, Moss AH, et al. Executive summary of the KDIGO controversies conference on supportive care in chronic kidney disease: developing a roadmap to improving quality care. Kidney Int. 2015;88(3):447–459. doi:10.1038/ki.2015.110
5. Ernecoff NC, Kurtz EC, Pearson EM, et al. Advanced care planning in chronic kidney disease: qualitative impact of the MY WAY intervention. J Pain Symptom Manage. 2024;68(3):e167–e173. doi:10.1016/j.jpainsymman.2024.05.030
6. Ladin K, Neckermann I, D’Arcangelo N, et al. Advance care planning in older adults with CKD: patient, care partner, and clinician perspectives. J Am Soc Nephrol JASN. 2021;32(6):1527–1535. doi:10.1681/ASN.2020091298
7. O’Halloran P, Noble H, Norwood K, et al. Nurse-led advance care planning with older people who have end-stage kidney disease: feasibility of a deferred entry randomised controlled trial incorporating an economic evaluation and mixed methods process evaluation (ACReDiT). BMC Nephrol. 2020;21(1):478. doi:10.1186/s12882-020-02129-5
8. de Sosa G R, Nicklas A, Thamer M, et al. Implementing advance care planning for dialysis patients: hIGHway project. BMC Palliat Care. 2022;21(1):129. doi:10.1186/s12904-022-01011-5
9. Zwarenstein M, Treweek S, Gagnier JJ, et al. Improving the reporting of pragmatic trials: an extension of the CONSORT statement. BMJ. 2008:
10. Saeed F, Horowitz RK, Allen RJ, et al. Feasibility and acceptability of a palliative care intervention among older adults with advanced CKD and their caregivers. Kidney360. 2025;6(2):236–246. doi:10.34067/KID.0000000622
11. Leventhal H, Phillips LA, Burns E. The Common-Sense Model of self-regulation (CSM): a dynamic framework for understanding illness self-management. J Behav Med. 2016;39(6):935–946. doi:10.1007/s10865-016-9782-2
12. Elwyn G, Frosch D, Thomson R, et al. Shared decision making: a model for clinical practice. J Gen Intern Med. 2012;27(10):1361–1367. doi:10.1007/s11606-012-2077-6
13. Hoffmann TC, Glasziou PP, Boutron I, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. 2014;348(mar07 3):g1687–g1687. doi:10.1136/bmj.g1687
14. O’Connor AM. Validation of a Decisional Conflict Scale. Med Decis Making. 1995;15(1):25–30. doi:10.1177/0272989X9501500105
15. Lu C, Mu W, Jin Y-H, et al. Cross-cultural adaptation and psychometric assessment of the statement format decisional conflict scale for mandarin version. BMC Health Serv Res. 2019;19(1):873. doi:10.1186/s12913-019-4717-6
16. Sudore RL, Stewart AL, Knight SJ, et al. Development and validation of a questionnaire to detect behavior change in multiple advance care planning behaviors. PLoS One. 2013;8(9):e72465. doi:10.1371/journal.pone.0072465
17. Liu D, Zhang L, Li J, Wang Z, Liu X, Zhang Q. Verification of the mandarin chinese version of advance care planning engagement survey scale in community-dwelling older people. Int J Older People Nurs. 2023;18(1):e12502. doi:10.1111/opn.12502
18. Wong PTP, Reker GT, Profile GGDA. Revised: a multidimensional measure of attitudes toward death. death anxiety handbook: research, instrumentation, and application. In: Series in Death Education, Aging, and Health Care. Philadelphia, PA: Taylor & Francis; 1994:121–148.
19. Tang L, Zhang L, Li YX, et al. Validation and reliability of a Chinese version Death Attitude Profile-Revised (DAP-R) for nurses. J Nurs Sci. 2014;29(14):64–66
20. Tao X, Chow SKY, Wong FKY. Determining the validity and reliability of the Chinese version of the Kidney Disease Quality of Life Questionnaire (KDQOL-36™). BMC Nephrol. 2014;15(1):115. doi:10.1186/1471-2369-15-115
21. Sabatino CP. The evolution of health care advance planning law and policy. Milbank Q. 2010;88(2):211–239. doi:10.1111/j.1468-0009.2010.00596.x
22. Chang HY, Takemura N, Chau PH, Lin CC. Prevalence and predictors of advance directive among terminally ill patients in Taiwan before enactment of patient right to autonomy act: a nationwide population-based study. BMC Palliat Care. 2022;21(1). doi:10.1186/s12904-022-01069-1
23. Chu LW. One step forward for advance directives in Hong Kong. Hong Kong Med J Xianggang Yi Xue Za Zhi. 2012;18(3):176–177.
24. Wang X, Wu Y, Bai X, et al. Acceptance level of advance care planning and its associated factors among the public: a nationwide survey. BMC Palliat Care. 2024;23(1). doi:10.1186/s12904-024-01533-0
25. Tsai SF, Chang CY, Yang JY, et al. Exploring knowledge, attitude, and intention towards advance care planning, advance directive, and the patient self-determination act among hemodialysis patients. BMC Palliat Care. 2023;22(1). doi:10.1186/s12904-023-01321-2
26. Song MK, Higgins MK, Ward SE, Lee H, Noorani N, Happ MB. Measures of patient and surrogate preparedness for end-of-life decision-making. J Pain Symptom Manage. 2024;67(5):429–440.e2. doi:10.1016/j.jpainsymman.2024.02.005
27. Nouri SS, Barnes DE, Shi Y, et al. The PREPARE for Your Care program increases advance care planning engagement among diverse older adults with cancer. Cancer. 2021;127(19):3631–3639. doi:10.1002/cncr.33676
28. Ladin K, Tighiouart H, Bronzi O, et al. Effectiveness of an intervention to improve decision making for older patients with advanced chronic kidney disease: a randomized controlled trial. Ann Intern Med. 2023;176(1):29–38. doi:10.7326/M22-1543
29. Chen HC, Wu CY, Hsieh HY, He JS, Hwang SJ, Hsieh HM. Predictors and assessment of hospice use for end-stage renal disease patients in Taiwan. Int J Environ Res Public Health. 2021;19(1):85. doi:10.3390/ijerph19010085
30. Korfage IJ, Carreras G, Arnfeldt Christensen CM, et al. Advance care planning in patients with advanced cancer: a 6-country, cluster-randomised clinical trial. PLOS Med. 2020;17(11):e1003422. doi:10.1371/journal.pmed.1003422
31. De L, A A, A E, et al. Advance care planning coaching in CKD clinics: a pragmatic randomized clinical trial. Am J Kidney Dis off J Natl Kidney Found. 2022;79(5). doi:10.1053/j.ajkd.2021.08.019
32. Volandes AE, Zupanc SN, Paasche-Orlow MK, et al. Association of an advance care planning video and communication intervention with documentation of advance care planning among older adults: a nonrandomized controlled trial. JAMA Network Open. 2022;5(2):e220354. doi:10.1001/jamanetworkopen.2022.0354
33. Tan M, Ding J, Johnson CE, et al. Stages of readiness for advance care planning: systematic review and meta-analysis of prevalence rates and associated factors. Int J Nurs Stud. 2024;151:104678. doi:10.1016/j.ijnurstu.2023.104678
34. Gao F, Chui PL, Che CC, Wang K. The mediating role of family cohesion in the relationship between death anxiety and readiness toward advance care planning among Chinese community-dwelling older adults: a cross-sectional study. Geriatr Nur. 2025;61:192–199. doi:10.1016/j.gerinurse.2024.10.061
35. Senteio CR, Callahan MB. Supporting quality care for ESRD patients: the social worker can help address barriers to advance care planning. BMC Nephrol. 2020;21(1). doi:10.1186/s12882-020-01720-0
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Nursing Interventions in Palliative Care for Advanced Dementia: A Systematic Review of Symptom, Relief, Comfort, and Caregiver Support
Pujante VGB, Sami W, Al-Kuwari NF, Rizvi MR
Journal of Multidisciplinary Healthcare 2025, 18:6545-6564
Published Date: 9 October 2025