Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Nurse–Physician Inter-Professional Collaboration and Associated Factors at Public Hospitals in Dessie City, Amhara, Northeastern Ethiopia, 2021
Authors Endris Y, W/Selassie M ![]() , Edmealem A
, Edmealem A ![]() , Ademe S
, Ademe S ![]() , Yimam W
, Yimam W ![]() , Zenebe Y
, Zenebe Y ![]()
Received 20 May 2022
Accepted for publication 26 July 2022
Published 9 August 2022 Volume 2022:15 Pages 1697—1708
DOI https://doi.org/10.2147/JMDH.S373599
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yimer Endris,1 Mulugeta W/Selassie,2 Afework Edmealem,3 Sewunet Ademe,3 Wondwossen Yimam,3 Yosef Zenebe4
1Department of Adult Health Nursing, Tropical College of Medicine, Dessie, Ethiopia; 2Department of Pediatrics and Child Health Nursing, Wollo University, College of Medicine and Health Sciences, Dessie, Ethiopia; 3Department of Comprehensive Nursing, Wollo University, College of Medicine and Health Sciences, Dessie, Ethiopia; 4Department of Psychiatry, Wollo University, College of Medicine and Health Sciences, Dessie, Ethiopia
Correspondence: Mulugeta W/Selassie, Email [email protected]
Introduction: Nurse–physician collaboration is an integral part of quality improvement in health care. Collaboration enables individuals to work together to achieve defined and common health purposes. There is limited evidence related to nurse–physician inter-professional collaboration and its associated factors in Ethiopia, particularly in Dessie city public hospitals.
Objective: To assess nurse–physician inter-professional collaboration and associated factors at public hospitals in Dessie city, Ethiopia, 2021.
Methods: An institutional-based cross-sectional study was conducted among nurses and physicians at public hospitals in Dessie city. A self-administered questionnaire was used for data collection. Stratified simple random sampling techniques were used to select study participants proportional to the sample size allocation. The final sample size was 260 and allocated proportionally to Dessie Comprehensive Specialized Hospital and Boru Meda General Hospital. The data were entered and analyzed using EPI-data version 4.6 and SPSS version 26 software respectively. During analysis, p-values less than 0.25 in binary logistic regression were entered into multivariable logistic regression. Finally, p-values less than 0.05 in multi-variable logistic regression were considered statically significant.
Results: The mean score for inter-professional collaboration was 97.40 ± 19.6SD. In this study, inter-professional collaboration among nurses and physicians was 44.2%. This study showed that favorable attitude [AOR=3.205; CI: 1.781– 5.766], respondents working in the gynecological department [AOR=0.210; CI: 0.052– 0.849], satisfied organizational support [AOR=2.062; CI: 1.140– 3.729] and urban residents [AOR=3.996; CI: 1.069– 14.931] were factors associated with nurse–physician inter-professional collaboration.
Conclusion: In this study, nurse–physician inter-professional collaboration was low. Training on the importance of health teamwork, timely monitoring and evaluation of organizational support, and professional empowerment towards a favorable attitude of nurse–physician inter-professional collaboration shall be provided at hospital levels. Routine assessment and timely intervention of the gynecological department for nurse–physician inter-professional collaboration shall be done at hospital levels. Moreover, both quantitative and qualitative research shall be performed for future research.
Keywords: inter-professional, collaboration, nurse, physician, associated factors
Introduction
Inter-professional collaboration occurs when two or more professions work together to achieve common goals and it is often used as a means to solve a variety of problems and complex issues.1,2 Inter-professional collaboration is a process that involves communication and decision-making, enabling an influence by the synergy of grouped knowledge and skills.3
Inter-professional collaboration between nursing and physicians is described as working together, sharing decision-making around health and social issues, formulating and carrying out plans for patient care, and solving patients’ problems. This determines the overall health care and services.1,4 Health care system complexity demands policy changes in the health system. Health care professionals must deal with multi-disciplinary work to accomplish different programs.5
The rapidly growing health care system and in complexity requires the integration of various systems.1 This broader sector needs collaboration between each department and individual to reduce the complexity of care by providing clear communication between workers.6 Inter-professional collaboration among health professionals generally occurs when multiple health workers from different professional backgrounds work together with patients, families, caregivers, and communities to deliver the highest quality of care.6 In health care, collaboration increases teamwork between health care professionals to deliver better care.2,6
The World Health Organization (WHO) defines inter-professional collaboration practice (IPCP) as a collaborative practice in health care that occurs when multiple health workers from different professional backgrounds provide comprehensive care.7 Collaboration between physicians and nurses is vital for patient care and for building a good working environment.6,8,9 Collaboration between physicians and nurses’ has many advantages in improving clinical outcomes and patient satisfaction. It also decreases the institutional cost, and quality of drugs, and improves behavioral interactions.6
Collaboration between physicians and nurses also provides satisfaction within the profession and increases their knowledge and skills. Collaboration between nurses and physicians helps health professionals resolve their problems.3 Generally, positive nurse–physician inter-professional collaboration is very important in creating safe, effective care, and a satisfying practice environment to provide quality patient care and decrease morbidity and mortality.10
Health professional collaboration is considered one of the healthcare goals because healthcare organizations need many interactions and collaborations between different healthcare professionals with varying levels of education and professional qualifications to provide effective care. It is necessary to ensure that health care teams are efficient and able to provide collaboration and joint decision-making between clients.8,10
Materials and Methods
Study Area and Period
This study was conducted in Dessie town, northeastern Ethiopia. Dessie is a town with a distance of 400 km from Addis Ababa, Ethiopia, and 471 km from Bahir Dar, which is the capital city of the Amhara regional state. In Dessie town, there are governmental and private health institutions. In Dessie town, there were two public hospitals. In Dessie Comprehensive Specialized Hospital, there were 622 health care workers. Among these, 318 were nurses and 201 were GP (40 specialists).22 Another public hospital was Boru Meda General Hospital which had 103 nurses and 37 GPs.23 The study period was from April 15 to June 15, 2021.
Study Design
An institution-based cross-sectional study was conducted among nurses and physicians working in public hospitals of Dessie city administration.
Population
Source population
The source populations were nurses and physicians working in public hospitals of Dessie city administration.
Study Population
The study populations were nurses and physicians working in public hospitals of Dessie city administration during the study period.
Inclusion and Exclusion Criteria
Inclusion Criteria
The study included all nurses and physicians who have been working in public hospitals in Dessie city administration in the clinical area for at least six months.
Exclusion Criteria
- The study excluded nurses and physicians who had been working in public hospitals of Dessie city administration but were currently on annual break, sick, and maternal leave during the study period.
Sample Size and Sampling Techniques
The sample size of the study was determined using a single population proportion formula to estimate the sample size for determining the level of nurse–physician inter-professional collaboration and associated factors at public hospitals in Dessie city administration. In this study, the following assumptions were made: 95% confidence level (Zα/2 = 1.96) and absolute precision or margin of error to be 5% (d = 0.05). The study population proportion on assessments of inter-professional collaboration between nurses and physicians taken from a previous study done in Mekelle was 0.54.10
The total population was calculated as -
- Where n = sample size
- P= proportion of the level of inter-professional collaboration between nurses and physicians taken from a study done in Mekelle which is 0.54,10
- CI: standard normal distribution curve value for the 95% confidence interval (1.96)
- d = the margin of error or accepted error.
As the total study population was less than 10,000, the sample size correction formula was used to obtain the actual sample size . Where, N = population size, no = first calculated sample size then Nf was
. Where, N = population size, no = first calculated sample size then Nf was  . Adding 10%15 for the non-respondent rate was considered. So, the final sample size was 236+24=260.
. Adding 10%15 for the non-respondent rate was considered. So, the final sample size was 236+24=260.
The sample size for nurses and physicians was calculated using the proportion formula: 
- Where ni: Sample size of n categories (Nurse and Physician final sample size)
- Ni: the total population of ni categories (final sample size which was 260)
- n: total population ni categories (Number of nurses and physicians in both hospitals which were 42L and 201 respectively)
- N: total population (total number of nurses and physicians in public hospitals of Dessie city administration which was 622)
The final sample size for each category of nurses and physicians was calculated. The number of nurses was  =176 and the number of physicians was
=176 and the number of physicians was  =84.
=84.
The number of nurses and physicians was 176 and 84 respectively.
In the study, the study populations were stratified into nurses and physicians (including all categories of general practitioners and specialists) and the sample was taken from each stratum proportionally. The final study population was selected by simple random sampling with the lottery method using a computer-generated random list. The sample frame consisted of all lists of nurses and physicians working in each ward of public hospitals. In Dessie, there are two public hospitals, with a proportional number of respondents taken from both hospitals, from which 201 (133 nurses and 68 physicians) from Dessie Comprehensive Specialized Hospital and 59 (43 nurses and 16 physicians) from Boru Meda General Hospital.
Variable
Dependent Variable
- Nurse–physician inter-professional collaboration.
Independent Variables
- Sociodemographic factors include age, sex, education, work experience, marital status, occupation status, religion, income, residence, and family size.
- Attitude toward inter-professional collaboration b/n nurse and physician (Shared education and teamwork, caring versus curing, nurse’s autonomy and physician’s dominance).
- Factors affecting collaboration between nurse and physician include the attitude of nurse and physician toward collaboration, work in area communication (angry, frustrated, feeling equal understood, feeling respected, satisfaction after the interaction, joyful talking, receiving correct information), and organizational related factor (organizational support for collaborations, professional growth of education and training, conflict resolution, monthly salary, and team conferences).
Data Collection Tools and Procedures
The data collection instrument was a self-administered questionnaire. The tool was adopted following the framework suggested by different evidence. A self-administered questionnaire was distributed to a representative sample of the study.
The tool consists of the different parts which developed from retrieving literature. The first part consists of socio-demographic factors such as age, sex, education, title of work, area of work, years of service, religion, and residence after searching relevant literature related to nurse–physician collaboration.10,18 Age of respondent and years of service was collected in continuous data and it was categorized based on reference from literature. The other sociodemographic factor variables were collected as categorical data. The nurse–physician collaboration level was assessed using the nurse–physician collaborative scale (NPCS) which was developed in Japan. Nurse–physician collaborative scale (NPCS) scale contains 27 items divided into three subscales: sharing patient information contains 9 items, 21 decision-making process contains 12 items and the relationship between nurse and physician contains 6 items.15,24 The nurse–physician collaboration (NPCS) item score from five Likert scales (1=Never, 2= rarely, 3= Sometimes, 4=usually, and 5=Always). NPCS overall score was calculated by adding each individual’s scores out of the total. The NPC’s overall score was calculated by summing all 27 items out of 135. The higher mean score indicates a higher level of nurse–physician collaboration. The nurse–physician collaboration (NPCS) means the score was 97.40. NPCS overall score above 97.40 was considered as frequent inter-professional collaboration and a score equal to and below 97.40 was considered as infrequent inter-professional collaboration. The outcome variable was inter-professional collaboration categorized as frequent inter-professional collaboration and infrequent inter-professional collaboration.10,18
The attitude of the respondent was measured using the Jefferson scale of attitudes towards nurse–physician collaboration (JSAPNC). This tool was originally developed and modified by Hojat and Herman at Jefferson medical college in Pennsylvania.25,26 JSAPNC tool includes 15 items which are grouped in four subscales. The first subscales contain seven items that focus on Shared education and teamwork. The second subscales contain three items about caring as opposed to curing. The third group has three items about nurses’ autonomy. The final group has two items about Physician’s dominance. The Jefferson scale item score from four Likert scales (1=strongly disagree, 2= Disagree, 4=agree and 5=strongly agree). A higher score indicates a higher level of nurse–physician collaboration. The overall score will be calculated by adding each individual’s score out of 60. The mean attitude score was calculated for each respondent after summarized of the overall score. JCAHO’s mean score above 49.02 was considered as having a favorable/good attitude and a mean score equal to and below 49.02 was considered an unfavorable/poor attitude. The Cronbach alpha test for JCAHO ranges from 0.70 to 0.93.10,18
The other tool used was to assess nurse–physician work area communication (good communication or poor communication) including factors like anger in the workplace, feeling respected, satisfaction after the interaction, joyful talking, receiving correct information scaled as always, some time, and none, and organizational related factor such as organizational support, professional growth of education and training, conflict resolution, monthly salary scaled in satisfied, unsatisfied, neutral taken from literature in Ethiopia.10,18
Operational Definitions
Frequent inter-professional collaboration: - above higher mean score (>97.40) of overall nurse–physician collaboration result of nurse–physician collaborative scale (NPCS).
Infrequent inter-professional collaboration: -lower mean score (≤97.40) of overall nurse–physician collaboration result of nurse–physician collaborative scale (NPCS).19
Favorable attitude toward nurse–physician collaboration: -above the higher mean score of (>49.02) attitudes toward nurse–physician inter-professional collaboration.
Unfavorable attitude toward nurse–physician collaboration: -lower mean score (≤49.02) of attitudes toward nurse–physician inter-professional collaboration.10
Adequate nurse–physician communication: -above the higher mean score of nurse–physician communication (≤13.29).
Inadequate nurse–physician communication: -below the higher mean score of nurse–physician communication (>13.29).
Satisfied organizational factor: -above the higher mean score of the overall organizational-related questioner (>7.92).
Un-satisfied organizational factor: -below the higher mean score of the overall organizational-related questionnaire (≤7.92).
Data Analysis Procedure
The data were first checked for completeness and consistency. The collected data was cleaned and questionnaires with missing variables were managed. The questionnaires were entered using Epi Data version 4.6. The questionnaires were exported and analyzed using the statistical package for social sciences (SPSS) statistical software package version 26. Analysis of data started with a description of data using mean, standard deviation, and frequencies for the variables. Study results have been presented using tables and charts.
Binary logistic regression analysis was performed to identify independent variables that are predictors of inter-professional collaboration between nurses and physicians. In bi-variable logistic regression analysis, all candidate variables p values less than 0.25 were entered into multivariable logistic regression analysis.
In multivariable logistic regression, all candidate variable p-value less than 0.25 were entered and p-values less than 0.05 were reported as an associated factor for inter-professional collaboration between nurses and physicians. Associated factor interpreted in Odds ratio in 95% confidence interval. Model fitness was checked by the Hosmer-Lemeshow test of goodness of fit and the model was fitted when the p-value >0.05. Multicollinearity was checked by variance inflation factor at a cut point of 10. Variance inflation factor less than 10 was considered as an absence of multicollinearity and the variable was included in the analysis.
Data Quality Control
Data quality control and cleaning commenced in the field by the researcher ensuring that all the information on the questionnaires was properly collected, recorded, and checked for completeness of data. Four health professionals wad selected for data collectors and they were trained for two days, which focused on data collection techniques, ethical issues, rights of the participants, reading through all the questions, and understanding them. The training also includes ways of decreasing under-reporting and maintaining confidentiality. The final version of the questionnaire was translated into the local language of the respondents (Amharic language) and was used for the data collection. Two weeks before the actual data collection, the questionnaire was pre-tested at South Wollo zone (Haike Hospital) selected woreda which is adjacent to the study area, on 5% of the total sample size facilities. It assesses whether the questionnaire and its items are easily understood by study participants, and to make any necessary changes before the main study began.
Result
Socio-Demographic Characteristics of the Study Participants
The response rate of the study was 100% and 260 health professionals among them 176 (67.7%) nurses and 84 (34.3%) physicians participated in the study. Of the total respondents, 163 (62.7%) were male. Of the total respondents, 244 (93.8%) and 118 (45.4%) were urban respondents and had less than five years of experience respectively. Out of the respondents, 140 (53.8%) and 77 (91.7%) had a first-degree educational level for nurses and physicians (general practitioners) respectively (Table 1).
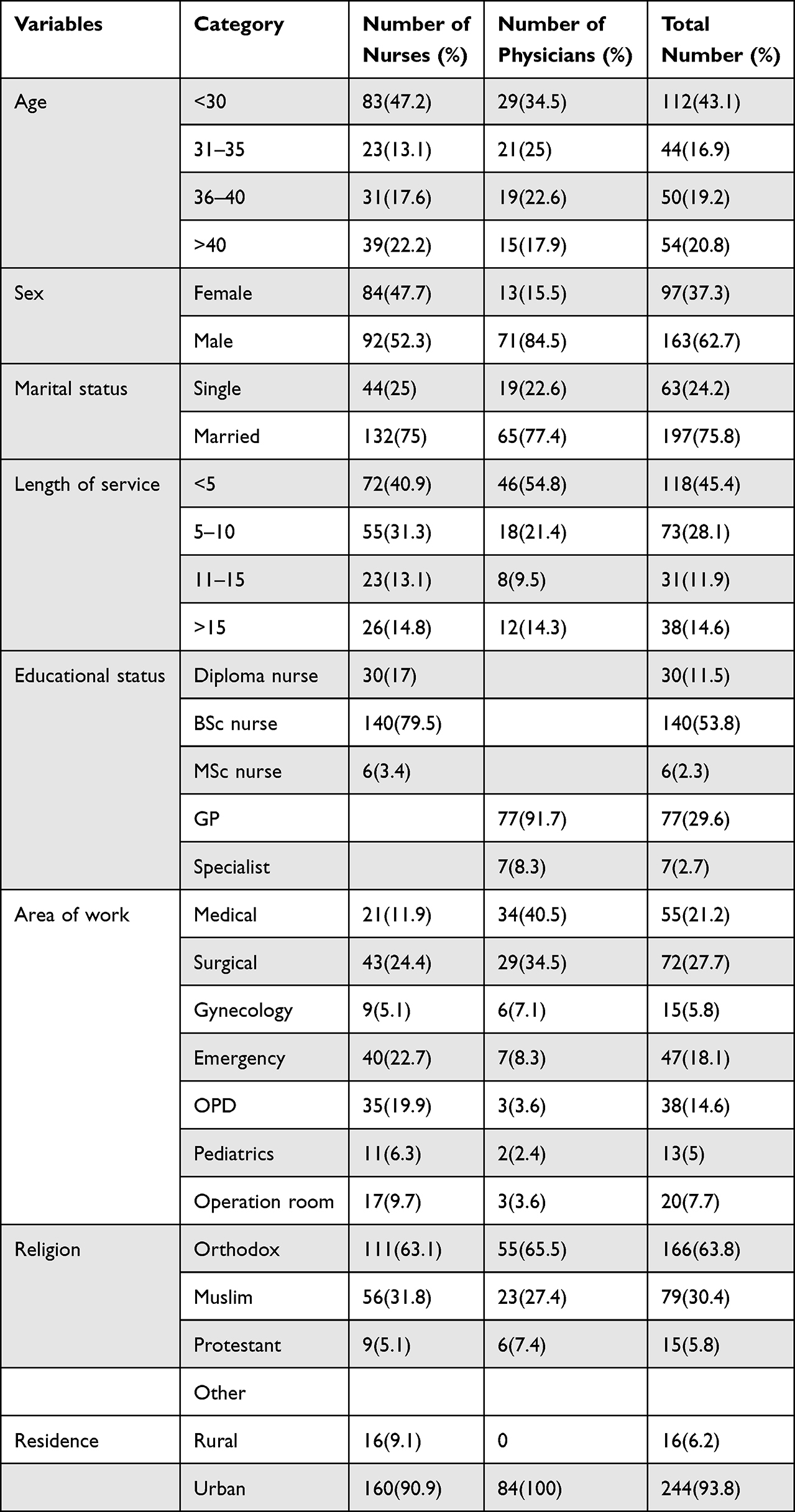 |
Table 1 Sociodemographic Characteristics of Respondents at Public Hospitals in Dessie City, Ethiopia, 2021 (N=260) |
Attitude Towards Nurse–Physician Inter-Professional Collaboration
The mean score of attitude towards nurse–physician inter-professional collaboration was 49.02 ± 5.87SD. The mean score for the subscale was higher for shared education and teamwork (23.23 ± 3.18SD). The mean score for other subscales like caring vs curing, nurse autonomy, and physician dominance were 10.22 ± 1.59SD, 10.22 ± 1.59SD, and 5.33 ± 1.85SD respectively.
Of the total respondents, 136 (52.3%) had a favorable attitude toward nurse–physician inter-professional collaboration. The nurses’ attitude toward nurse–physician inter-professional collaboration was 93 (52.8%) when compared to physicians 43 (51.2%). Regarding shared education and teamwork, fifty-one physicians (60.7%) have favorable shared education and teamwork (Table 2.)
 |
Table 2 Attitude Toward Nurse–Physician Inter-Professional Collaboration at Public Hospitals in Dessie City, Ethiopia, 2021(N=260) |
Communication and Organization-Related Factors Among the Study Participants
The nurse–physician communication showed that 133 (51.2%) of the respondents had good communication between nurse and physician. Regarding organization support, 133 (51.2%) of the respondents had satisfied with organizational support for nurse–physician inter-professional collaboration (Table 3).
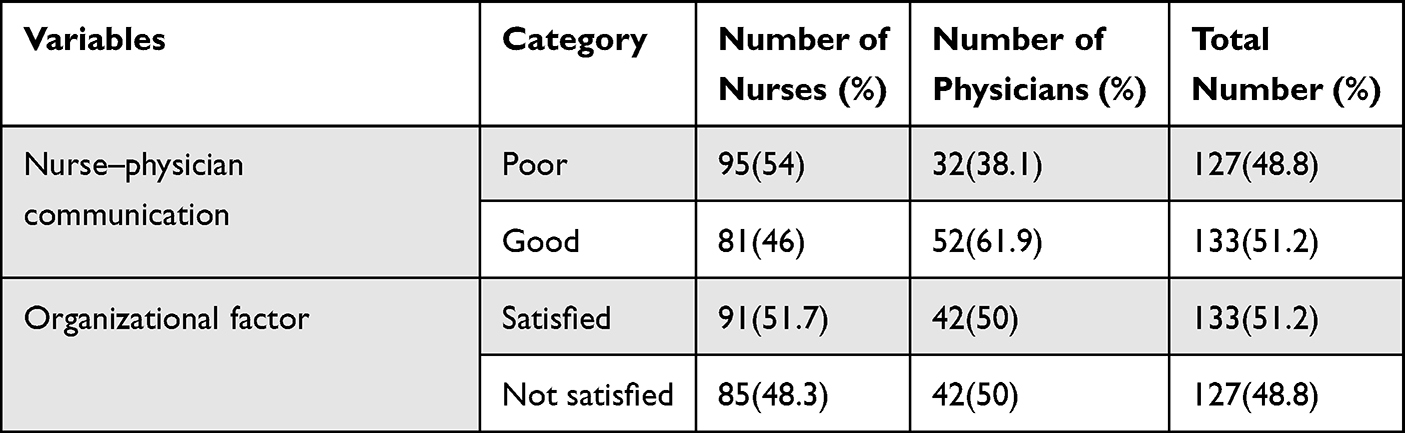 |
Table 3 Communication and Organization-Related Factors Among Nurses and Physicians at Public Hospitals in Dessie City, Ethiopia, 2021(N=260) |
Nurse–Physician Inter-Professional Collaboration
The mean score for inter-professional collaboration was 97.40 ± 19.6SD. Out of the total respondents, 114.9 (44.2%) of them had frequent inter-professional collaboration. This study showed that nurses had more frequent nurse–physician inter-professional collaboration (46.6%) when compared to physicians (39.9%) (Figure 1).
 |
Figure 1 A graph showing nurse–physician inter-professional collaboration at public hospitals in Dessie city, Ethiopia, 2021 (N=260). |
Factors Affecting Nurse–Physician Inter-Professional Collaboration
In bi-variable logistic regression, age of respondent, length of service, area of work, religion, residence, attitude toward inter-professional collaboration, and organization factor were factors with a p-value less than 0.25. These variable that satisfied bi-variable logistic regression was selected for multivariable logistic regression analysis.
In multivariable logistic regression, respondent who work in gynecological department [AOR=0.210; CI: 0.052–0.849], favorable attitude toward nurse–physician inter-professional collaboration [AOR=3.205; CI: 1.781–5.766], satisfied organization support [AOR=2.062; CI: 1.140–3.729] and urban residents [AOR=3.996; CI: 1.069–14.931] were factors associated with nurse–physician inter-professional collaboration (Table 4).
 |
Table 4 Bi-Variable and Multi-Variable Logistic Regression to Identify Factors Associated with Nurse–Physician Inter-Professional Collaboration at Public Hospitals in Dessie City, Ethiopia, 2021(N=260) |
Discussion
Nurse–physician inter-professional collaboration is important to improve the quality of health care. Nurse–physician inter-professional collaboration is affected by different determinants. So, this study explored nurse–physician inter-professional collaboration and associated factors at public hospitals in Dessie city administration, Ethiopia.
In this study, nurse and physician inter-professional collaborations were 44.2%. This study was supported by a study done in Addis Ababa.19 But this finding is lower than the study done in Mekele10 and Jimma.18 The possible reason for this difference might be health professional training related to collaboration, manager conflict management skills and health professional communication skills, and teamwork.27 There was a discrepancy with a study done in the United States, which reported that 72% of nurses were collaborating between nurses and physicians.16 The discrepancy may be a result of the difference in the study setting and sociodemographic factors.
The study also showed that nurses had more frequent collaboration compared to physicians. The possible reason might be the difference between the two professionals in terms of their academic ability, ability to make a decision, interpersonal skills, and being team players.28
Attitude toward nurse–physician inter-professional collaboration is higher among nurses. This is supported by a study done in another study which concluded that nurses had positive attitude toward nurse–physician inter-professional collaboration when compared to physicians.5,18,20,34 Additionally, a study was done in Palestine and Nigeria that stated nurses expressed a more positive attitude toward collaboration by the mentioned nurse were more involved and partners in inpatient care.11,21 This might be the integration of health training programs related to collaboration in the nurse curriculum.28 Another study, done in a different country showed that physicians had a more positive attitude toward collaboration than nurses.3,12 The discrepancy might be a difference in the study area and study design.
Attitude was a significant factor affecting inter-professional collaboration among nurses and physicians. Those respondents who had a favorable attitude toward collaboration had 3 times more frequent nurse–physician inter-professional collaboration. This study was supported by a study done in Mekelle,10 Jimma,18 and Turkey.34 The pleasurable reason might be due to hierarchical differences, professional dominant authority, and low participation in the decision-making of nurses and physicians.21,29,30
Organization support was statistically significantly associated with satisfied inter-professional collaboration. Satisfied organization support had 2 times more frequent nurse–physician inter-professional collaboration when compared to unsatisfied organization support. This is in line with studies done in Mekele10 and Kenya.13 This might be due to a supportive working environment, salary, continuous professional development, and the existence of a conflict management system that is required to ensure professionals’ adequate collaboration.28,31
Nurse–physician inter-professional collaboration factors were significantly influenced by residency and respondents who reside in urban had 4 times more likely to have frequent nurse–physician inter-professional collaboration. This could be related to urban residents having more opportunities to adapt collaboration behavior and teamwork than physicians.32
The working department was found to be another factor associated with nurse–physician inter-professional collaboration. Those respondents who work in the gynecological department had less frequent inter-professional collaboration when compared to other departments. This is supported by a study done in India.17 The possible reason for the difference might be a variation in the professional title, and individual competencies.28,33 Additionally, the workplace was one of the influential factors in nurse–physician inter-professional collaboration.17 But the working department is not mentioned as a significant factor for nurse–physician inter-professional collaboration in a study done in Jimma and Addis Ababa.19
Conclusion
In this study, nurse–physician inter-professional collaboration was low. Of the total respondents, nurses had more frequent inter-professional collaboration when compared to physicians. In addition, attitudes toward nurse–physician inter-professional collaboration were higher among nurses when compared to physicians.
Unsatisfied satisfied organization support, favorable attitude toward inter-professional collaboration, rural residents, and working in the gynecology department were associated factors for nurse–physician inter-professional collaboration.
Training on the importance of health teamwork, timely monitoring and evaluation of organizational support, and professional empowerment towards the attitude of nurse–physician inter-professional collaboration shall be provided at hospital levels. Routine assessment and timely intervention of different departments for nurse–physician inter-professional collaboration shall be done at hospital levels. Moreover, both quantitative and qualitative research shall be performed for future research.
Abbreviations
AOR, adjusted odd ratio; CI, confidence interval; COR, crude odd ratio; GPs, general practitioners; IPCP, inter-professional collaboration practice; JSAPNC, Jefferson scale of attitudes towards nurse–physician collaboration; IRB, Institution Review Board; NPCS, nurse–physician collaborative; SPSS 26, Statistical Package for Social Science 26; WHO, World Health Organization.
Data Sharing Statement
The data used to support the findings of this study is available upon request from the corresponding author.
Ethical Approval and Consent to Participate
Ethical approval was obtained from the Ethical Review Committee of Tropical College of Medicine with approval number NURS3420/13. Permission letter was received from Dessie Comprehensive Specialized Hospital and Boru Meda General Hospital. The purpose and importance of the study were explained to each study participant. The confidentiality and privacy of participants were secured by avoiding any personal identifier. Written consent was obtained from each participant before study commencement, and this study was conducted as per the Declaration of Helsinki. Participants were informed of their full right to withdraw from the study at any time they wish. The study did not have any physical harm, social discrimination, psychological trauma, and economic loss to the study participants.
Acknowledgment
We would like to acknowledge the Tropical College of Medicine, data collectors, and study participants. Moreover, we would like to thank Dessie Comprehensive Specialized Hospital and the staff of Boru Meda General Hospital for their valuable responses to conducting this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
All authors declare that they have no conflicts of interest in this work.
References
1. Bridges D, Davidson RA, Soule Odegard P, Maki IV, Tomkowiak J. Inter-professional collaboration: three best practice models of inter-professional education. Med Educ Online. 2011;16(1):6035. doi:10.3402/meo.v16i0.6035
2. Leathard A. Inter-Professional Collaboration: From Policy to Practice in Health and Social Care. Psychology Press; 2003.
3. El Sayed K, Sleem WF. Nurse–physician collaboration: a comparative study of the attitudes of nurses and physicians at Mansoura University Hospital. Life Sci J. 2011;8(2):140–146.
4. Pakpour V, Ghafourifard M, Salimi S. Iranian nurses’ attitudes toward nurse-physician collaboration and its relationship with job satisfaction. J Caring Sci. 2019;8(2):111. doi:10.15171/jcs.2019.016
5. Jasemi M, Hassankhani H, Zamanzadeh V. Effective factors on the inter-professional relationship between nurses and physicians. Medbiotech J. 2017;1(03):130–134.
6. Green BN, Johnson CD. Inter-professional collaboration in research, education, and clinical practice: working together for a better future. J Chiropr Educ. 2015;29(1):1–10. doi:10.7899/JCE-14-36
7. World Health Organization. Inter-professional collaboration practice (IPCP); 2010.
8. Herath C, Zhou Y, Gan Y, Nakandawire N, Gong Y, Lu Z. A comparative study of inter-professional education in global health care: a systematic review. Medicine. 2017;96(38):38. doi:10.1097/MD.0000000000007336
9. Smit LC, Dikken J, Moolenaar NM, Schuurmans MJ, de Wit NJ, Bleijenberg N. Implementation of an inter-professional collaboration in practice program: a feasibility study using social network analysis. Pilot Feasibility Stud. 2021;7(1):1–12. doi:10.1186/s40814-020-00746-3
10. Eukubay T, Abate A. Inter-professional collaboration and associated factors among nurses and physicians working at public Hospitals in Mekelle city Tigray region, north Ethiopia, 2017. Nurse Care Open Acces J. 2019;6(6):185–192.
11. Falana TD, Afolabi OT, Adebayo AM, Ilesanmi OS. Collaboration between doctors and nurses in a tertiary health facility in southwest Nigeria: implication for effective healthcare delivery. Int J Caring Sci. 2016;9(1):165.
12. Collette AE, Wann K, Nevin ML, et al. An exploration of nurse-physician perceptions of collaborative behavior. J Interprof Care. 2017;31(4):470–478.
13. Koech RC. Factors influencing Inter-professional collaboration among healthcare workers in primary healthcare facilities. A case of Nakuru county Kenya: KeMU; 2020.
14. Bell ML. Nurses’ attitudes towards nurse-physician collaboration, their collaborative behaviors and associated demographic, organizational and relational factors in nurses working in the acute care context in Ireland and the United States of America. University College Cork; 2018.
15. Han PK, Babrow A, Hillen MA, Gulbrandsen P, Smets EM, Ofstad EH. Uncertainty in health care: towards a more systematic program of research. Patient Educ Couns. 2019;102(10):1756–1766. doi:10.1016/j.pec.2019.06.012
16. House S, Havens D. Nurses’ and physicians’ perceptions of nurse-physician collaboration: a systematic review. JONA. 2017;47(3):165–171. doi:10.1097/NNA.0000000000000460
17. Aghamohammadi D, Dadkhah B, Aghamohammadi M. Nurse–physician collaboration and the professional autonomy of intensive care units nurses. Indian J Crit Care Med. 2019;23(4):178. doi:10.5005/jp-journals-10071-23149
18. Melkamu E, Woldemariam S, Haftu A. Inter-professional collaboration of nurses and midwives with physicians and associated factors in Jimma University specialized teaching hospital, Jimma, Southwest Ethiopia, 2019: a cross-sectional study. BMC Nurs. 2020;19(1):1–9. doi:10.1186/s12912-020-00426-w
19. Tsegay L. Assessment of Inter-professional collaboration between nurses and physicians working at Tikur Anbessa Specialized Hospital Addis Ababa, Ethiopia; 2015.
20. Hossny EK, Sabra HE. The attitudes of healthcare professionals towards nurse-physician collaboration. Nurs Open. 2020;8(3):1406–1416.
21. Elsous A, Radwan M, Mohsen S. Nurses and physicians attitudes toward nurse-physician collaboration: a survey from Gaza Strip, Palestine. Nurs Res Pract. 2017;2017:1.
22. Hospital Dcs. Human resource management in disk Hi, editor. Dessie; 2021.
23. Hospital BMR. Information disk in management Hr, editor. Dessie; 2021.
24. Ushiro R. Nurse–Physician Collaboration Scale: development and psychometric testing. J Adv Nurs. 2009;65(7):1497–1508. doi:10.1111/j.1365-2648.2009.05011.x
25. Hojat M, Fields SK, Veloski JJ, Griffiths M, Cohen MJ, Plumb JD. Psychometric properties of an attitude scale measuring physician-nurse collaboration. Eval Health Prof. 1999;22(2):208–220. doi:10.1177/01632789922034275
26. Malliarou M, Domeyer P, Bamidis P, Sarafis P. Translation and validation of the Greek version of the Jefferson Scale of Attitudes toward Physician and Nurse Collaboration (JSAPNC). J Interprof Care. 2020;35:1–8.
27. Tang CJ, Zhou WT, Chan SWC, Liaw SY. Inter-professional collaboration between junior doctors and nurses in the general ward setting: a qualitative exploratory study. J Nurs Manag. 2018;26(1):11–18. doi:10.1111/jonm.12503
28. Karam M, Brault I, Van Durme T, Macq J. Comparing inter-professional and inter-organizational collaboration in healthcare: a systematic review of the qualitative research. Int J Nurs Stud. 2018;79:70–83. doi:10.1016/j.ijnurstu.2017.11.002
29. Hossny EK, Sabra HE. The attitudes of healthcare professionals towards nurse-physician collaboration. Nurs Open. 2021;8(3):1406–1416. doi:10.1002/nop2.756
30. Molina-Mula J, Gallo-Estrada J, Perelló-Campaner C. Impact of inter-professional relationships from nurses’ perspective on the decision-making capacity of patients in a clinical setting. Int J Environ Res Public Health. 2018;15(1):49. doi:10.3390/ijerph15010049
31. Lai GC, Taylor EV, Haigh MM, Thompson SC. Factors affecting the retention of indigenous Australians in the health workforce: a systematic review. Int J Environ Res Public Health. 2018;15(5):914. doi:10.3390/ijerph15050914
32. Ohta R, Ryu Y, Otani J. Rural physicians’ perceptions about the challenges of participating in inter-professional collaboration: insights from a focus group study. J Interprof Educ Pract. 2020;20:100345.
33. Matthys E, Remmen R, Van Bogaert P. An overview of systematic reviews on the collaboration between physicians and nurses and the impact on patient outcomes: what can we learn in primary care? BMC Fam Pract. 2017;18(1):1–22. doi:10.1186/s12875-017-0698-x
34. Filizli G, Önler E. Nurse-physician collaboration in surgical units: a questionnaire study. J Interprof Educ Pract. 2020;21:100386.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Collaboration Between Physicians from Different Medical Specialties in Hospital Settings: A Systematic Review
Braam A, Buljac-Samardzic M, Hilders CGJM, van Wijngaarden JDH
Journal of Multidisciplinary Healthcare 2022, 15:2277-2300
Published Date: 7 October 2022
A Scoping Review of Interprofessional Education in Saudi Arabia: Outcomes, Barriers, and Implementation Challenges
Almater L, Almalag HM, Aljuffali L, Saja MF, Alzamil H, Alzamel F
Advances in Medical Education and Practice 2025, 16:1683-1694
Published Date: 15 September 2025