")
Back to Journals » Nature and Science of Sleep » Volume 12
Number of Chronic Nighttime Insomnia Symptoms and Risk of Chronic Widespread Pain and Pain-Related Disability: The HUNT Study
Authors Skarpsno ES , Mork PJ , Hagen K, Nilsen TIL, Marcuzzi A
Received 2 October 2020
Accepted for publication 25 November 2020
Published 29 December 2020 Volume 2020:12 Pages 1227—1236
DOI https://doi.org/10.2147/NSS.S284498
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Steven A Shea
Eivind Schjelderup Skarpsno,1,2 Paul Jarle Mork,1 Knut Hagen,3,4 Tom Ivar Lund Nilsen,1,5 Anna Marcuzzi1
1Department of Public Health and Nursing, Norwegian University of Science and Technology (NTNU), Trondheim, Norway; 2Department of Neurology and Clinical Neurophysiology, St. Olavs Hospital, Trondheim, Norway; 3Department of Neuromedicine and Movement Science, Norwegian University of Science and Technology (NTNU), Trondheim, Norway; 4Clinical Research Unit Central Norway, St. Olavs Hospital, Trondheim, Norway; 5Clinic of Anaesthesia and Intensive Care, St. Olavs Hospital, Trondheim University Hospital, Trondheim, Norway
Correspondence: Eivind Schjelderup Skarpsno
Department of Public Health and Nursing, Norwegian University of Science and Technology (NTNU), Håkon Jarls Gate 11, Samfunnsmedisinbygget, Trondheim 7030, Norway
Tel +47 97521297
Email [email protected]
Study Objectives: To examine the association between the number of chronic nighttime insomnia symptoms and the risk of chronic widespread pain (CWP) and pain-related disability.
Methods: A prospective study of 10,847 participants in the Norwegian HUNT Study without chronic musculoskeletal pain at baseline in 2006– 2008. We used a modified Poisson regression model to estimate adjusted risk ratios (RRs) with a 95% confidence interval (CI) for CWP and pain-related disability at follow-up in 2017– 2019 associated with insomnia and number of nighttime insomnia symptoms at baseline. Chronic insomnia was defined according to the current classification system and grouped into three categories based on the number of reported nighttime symptoms (ie, difficulty initiating sleep, trouble maintaining sleep and early morning awakenings).
Results: Compared to the reference group of people without insomnia, people with insomnia had RRs for CWP and pain-related disability of 1.64 (1.26– 2.14) and 1.63 (1.37– 1.94), respectively. When people with insomnia were categorized based on the number of nighttime symptoms, people who reported one, two, or three nighttime symptoms had RRs of CWP of 1.19 (95% CI 0.80– 1.78), 1.78 (95 CI 1.13– 2.80) and 3.08 (95% CI 1.93– 4.92), respectively, compared to people without insomnia. The corresponding RRs for pain-related disability were 1.49 (95% CI 1.17– 1.89), 1.46 (95% CI 2.04– 2.05), and 2.46 (95% CI 1.76– 3.42).
Conclusion: These findings indicate that people with insomnia characterized by symptoms in all phases of the sleep period have a substantially increased risk of CWP and pain-related disability.
Keywords: sleeplessness, insomnia disorder, chronic insomnia, musculoskeletal, pain, chronic, widespread chronic pain, relative risk, epidemiology
Plain Language Summary
Research shows that insomnia is associated with increased risk of chronic musculoskeletal pain. However, previous studies have not considered the complexity of the insomnia disorder in terms of the possible inter-individual differences in the number of nighttime symptoms. The aim of this prospective study was therefore to examine the influence of the number of chronic nighttime insomnia symptoms on the risk of chronic widespread pain and pain-related disability. Our results show that people with insomnia symptoms in all phases of the sleep period (difficulty initiating sleep, trouble maintaining sleep, and early morning awakenings) are particularly vulnerable to develop chronic widespread pain and pain-related disability. These findings are important because they indicate that insomnia is a heterogenous condition and that the number of nighttime symptoms is an important factor that influences the association between insomnia and the risk of chronic pain. To fully understand the role of insomnia in the development of chronic musculoskeletal pain, there is a need for studies exploring if combinations of specific nighttime symptoms are particularly related to chronic pain.
Introduction
Insomnia is the most common sleep disorder in the general population.1,2 To be diagnosed with insomnia according to the current classification system,3 the individual has to report at least one nighttime symptom (eg, difficulty initiating sleep, trouble maintaining sleep, or early morning awakenings), accompanied by daytime impairment in social, occupational and/or educational areas. The symptoms must also occur at least three times a week for at least three months, despite adequate opportunity and circumstances for sleep. Although these diagnostic criteria are recommended for use in clinical practice,3 it has been shown that the type and the number of insomnia symptoms can vary across individuals diagnosed with insomnia,4–6 and that non-restorative sleep may occur independently of other insomnia symptoms.7 This heterogeneity has led to the view that insomnia is a complex disorder and that several insomnia phenotypes with different disease burden may co-exist.8,9
Despite the growing body of evidence showing a strong relation between insomnia and the risk of chronic musculoskeletal pain,10–13 most studies have not considered the complexity of the insomnia disorder in terms of the possible inter-individual differences in the number of nighttime symptoms.10–12 Some observational studies indicate that insomnia severity, defined by the frequency of sleeplessness or number of insomnia symptoms, is associated with an increased risk of chronic widespread pain (CWP), although questions fulfilling the diagnostic criteria of insomnia were unavailable.13,14 The link between specific sleep-related characteristics and pain is further underscored by experimental studies showing that disruption of restorative sleep without reduced sleep efficiency is associated with decreased pain threshold15 and that disruption of sleep continuity is more strongly associated with spontaneous pain reports, compared with restricted but continuous sleep.16 However, the long-term effect of different sleep characteristics on the development of chronic musculoskeletal pain is unknown. Exploring the influence of the number of nighttime insomnia symptoms in people with insomnia can help identifying individuals at high risk for developing CWP and pain-related disability and provide further insight into the processes that link these conditions.
The aim of this population-based study was to examine the influence of the number of chronic nighttime insomnia symptoms on the risk of CWP and pain-related disability. To explore the hypothesis that the number of nighttime insomnia symptoms is dose-dependently associated with the risk of chronic musculoskeletal pain, we grouped people with chronic insomnia into three categories based on the number of reported nighttime symptoms (ie, difficulty initiating sleep, trouble maintaining sleep and early morning awakenings).
Materials and Methods
Study Population
This prospective study utilized data from the third (2006–2008) and fourth (2017–2019) surveys of the Norwegian HUNT Study. All inhabitants aged 20 years or older residing in the Nord-Trøndelag County (now Trøndelag County) in Norway have been invited to participate in the HUNT Study. Information on lifestyle and health-related factors was collected by questionnaires and clinical examination in both surveys. The HUNT surveys were completed with ~11-year intervals. More detailed information about the HUNT Study can be found at http://www.ntnu.edu/hunt.
In the third survey, 50,839 (54%) people accepted the invitation. In the fourth survey, 56,078 (55%) people accepted the invitation. For the purpose of the current study, we included 33,900 who participated in both 2006–2008 and 2017–2019. Of these, 13,326 persons reported no chronic musculoskeletal pain at baseline in 2006–2008. Furthermore, we excluded 156 persons who had incomplete information about insomnia symptoms. Of the remaining 13,170 participants, 10,847 answered relevant pain questions at follow-up in 2017–2019 and were included in the analysis.
Insomnia Symptoms
Insomnia symptoms at baseline in 2006–08 were assessed by the following four questions: 1) “How often during the last three months have you had difficulty falling asleep at night?”, 2) “How often during the last three months have you woken up repeatedly during the night?”, 3) “How often during the last three months have you woken too early and couldn’t get back to sleep?”, and 4) “How often during the last three months have you felt sleepy during the day?”, with three response options for each question: “Never/seldom”, “Sometimes” and “Several times a week”. The information retrieved from these four questions was used to approximate the information necessary to diagnose insomnia according to current diagnostic classification systems.3 Participants were therefore classified with chronic insomnia if they answered, “Several times a week” on at least one of the questions 1–3, and “Several times a week” on question 4. To examine the influence of number of nighttime insomnia symptoms, people classified with chronic insomnia were further categorized into three subgroups: 1) “Insomnia with one nighttime symptom”, 2) “Insomnia with two nighttime symptoms“, and 3) “Insomnia with three nighttime symptoms”. The reliability (test-retest) of the summed scores of these three items has previously found to be good (kappa value 0.51; 95% CI 0.40–0.63).17 It should be noted that although insomnia symptoms were obtained also at the follow-up survey, this information was not included in the analysis as it would have induced bias due to reverse causation between incident chronic pain and insomnia symptoms.
Chronic Musculoskeletal Pain and Pain-Related Disability
Questions on musculoskeletal pain were adopted from the Standard Nordic Questionnaire.18 At baseline, participants were defined to have any chronic musculoskeletal pain if they answered “yes” to the following question: “During the last year, have you had pain and/or stiffness in your muscles and joints that lasted for at least three consecutive months?”. Participants reporting any chronic musculoskeletal pain at baseline were excluded from the study.
At follow-up, participants were defined to have any chronic musculoskeletal pain if they answered “yes” to the following question: “During the last year, have you had pain in your muscles and joints that lasted for at least three consecutive months?” Participants defined to have any chronic musculoskeletal pain were asked to indicate the affected body area(s), ie, neck, shoulders, upper back, elbows, low back, hips, wrists/fingers, knees, calf, and ankles/feet. Participants were also asked the following question: “Have you been suffering from pain in both left and right sides of the body?”. Participants were defined to have CWP if they reported chronic pain in the axial skeleton, above and below the waist, and in both left and right sides of the body. The reliability of any chronic musculoskeletal pain and CWP has been evaluated previously, reporting kappa values of 0.63 (95% CI 0.53–0.73) and 0.48 (95% CI 0.38–0.64), respectively.19
Pain-related disability was assessed separately for work ability and leisure time activity. Participants were asked the following two questions 1) “Have the pain in muscles or joints reduced your ability to work?”, and 2) “Have the pain in muscles or joints reduced your leisure activity?”, with the response options “no” and “yes”. Participants were classified with pain-related disability if they answered, “yes” to at least one of these questions. The questions on pain-related disability have not been validated.
Assessment of Covariates
Possible confounders were assessed at baseline in 2006–08. Body mass index (BMI) was calculated as weight divided by the square of height (kg/m2) using standardized measurements of height (to the nearest centimeter) and weight (to the nearest half kilogram) from the clinical examination. Smoking status was assessed by questions about past or present use of cigarettes and were divided in three categories: “never smoked”, “former smoker” and “current smoker”. Leisure time physical activity was assessed by two questions on the number of hours per week of light (no sweating or heavy breathing) and/or hard (sweating and heavy breathing) physical activity. The response options for both questions were “none”, “less than 1 hour”, “1–2 hours”, and “3 or more hours”. We constructed a variable with three categories combining information on light and hard activities: “inactive”, “low”, and “moderate-to-high”. The questions on light and hard physical activity have been validated in a relatively selected sample of young/middle-aged men20 showing that light leisure time physical activity was not clearly related to objectively measured oxygen uptake, whereas hard physical activity was moderately correlated with this objective measure. Shift work was assessed by the question “Do you work shifts, at night, or on call?”, with response options “no” and “yes”. Alcohol consumption was assessed by the CAGE (Cut down, Annoyed, Guilty, Eye-opener) questionnaire using a cutoff score ≥2 to indicate possible alcohol abuse.21 Symptoms of anxiety and depression were assessed by the validated questionnaire (Hospital Anxiety and Depression Scale, HADS) including seven questions on anxiety and seven questions on depression. As recommended, the cut-off score was set to ≥8 on both anxiety and depression and was dichotomized as the presence or no presence of anxiety and/or depression.22 To assess comorbid conditions, participants were asked about current and previous disease (heart disease, lung diseases, diabetes, cancer, fibromyalgia, rheumatic diseases or degenerative joint disease). Other possible sleep complaints such as sleep apnea and restless legs syndrome were assessed by the question: “How often during the last three months have you stopped breathing while sleeping and/or had tingling in legs during the context of sleep?”, with the response options “never/seldom”, “sometimes” and “several times a week”. People answering “several times a week” to this question were classified as having other sleep complaints.
Statistical Analyses
A modified Poisson regression model was used to estimate risk ratios (RR) for the association between the number of chronic nighttime insomnia symptoms at baseline in 2006–08 (i.e., exposure variable) and the binary outcome variables chronic musculoskeletal pain (yes, no), CWP (yes, no), and pain-related disability (yes, no) at follow-up in 2017–19. The precision of the RRs was assessed by 95% confidence interval (CI) using robust variance estimation to obtain valid standard error, and thus CIs. Participants with chronic insomnia were compared with the reference group without insomnia. Participants reporting chronic insomnia with one, two, or three nighttime symptoms were compared with the reference group without insomnia. The selection of confounders was based on a priori knowledge about factors that potentially could be related to both the exposure and outcomes under study. After careful considerations, all associations were adjusted for age (continuous), gender (women, men), BMI (continuous), leisure time physical activity (inactive, low, moderate-to-high), shift work (no, yes), alcohol consumption (no alcohol abuse, possible alcohol abuse) and smoking (never, former, current smoker). Since physical activity (1%), smoking (2%), body mass index (0.1%), shift work (22%), and alcohol consumption (12%) had missing data, we imputed missing data (20 imputations). The predictors in the imputation model for missing data were all the variables used in the main analysis, along with other comorbid conditions and other sleep disorders.
We conducted two supplementary analyses to assess the robustness of the results. First, since there is a considerable overlap between insomnia, mental health disorders and medical conditions,23–25 we repeated the main analysis adjusting for depression and/or anxiety and other comorbid conditions (diabetes, heart disease, lung disease, and rheumatic diseases). Second, since obstructive sleep apnea syndrome and restless leg syndrome represent distinct sleep disorders that are associated with chronic pain,26,27 we repeated the main analysis excluding people who self-reported frequent breathing pauses during the night and/or symptoms of discomfort, tingling or prickling in the legs.
All statistical analyses were performed using Stata for Windows, version 16.0 (StataCorp LP, College Station, Texas).
Results
The baseline characteristics of the 10,847 participants stratified by insomnia and number of insomnia symptoms are reported in Table 1. The proportion of participants categorized with insomnia according to the ICSD-3 criteria was 3.6%. Overall, 4063 (37.5%) participants reported any chronic musculoskeletal pain, 571 (5.3%) reported CWP, and 1640 (15.1%) reported pain-related disability at follow-up.
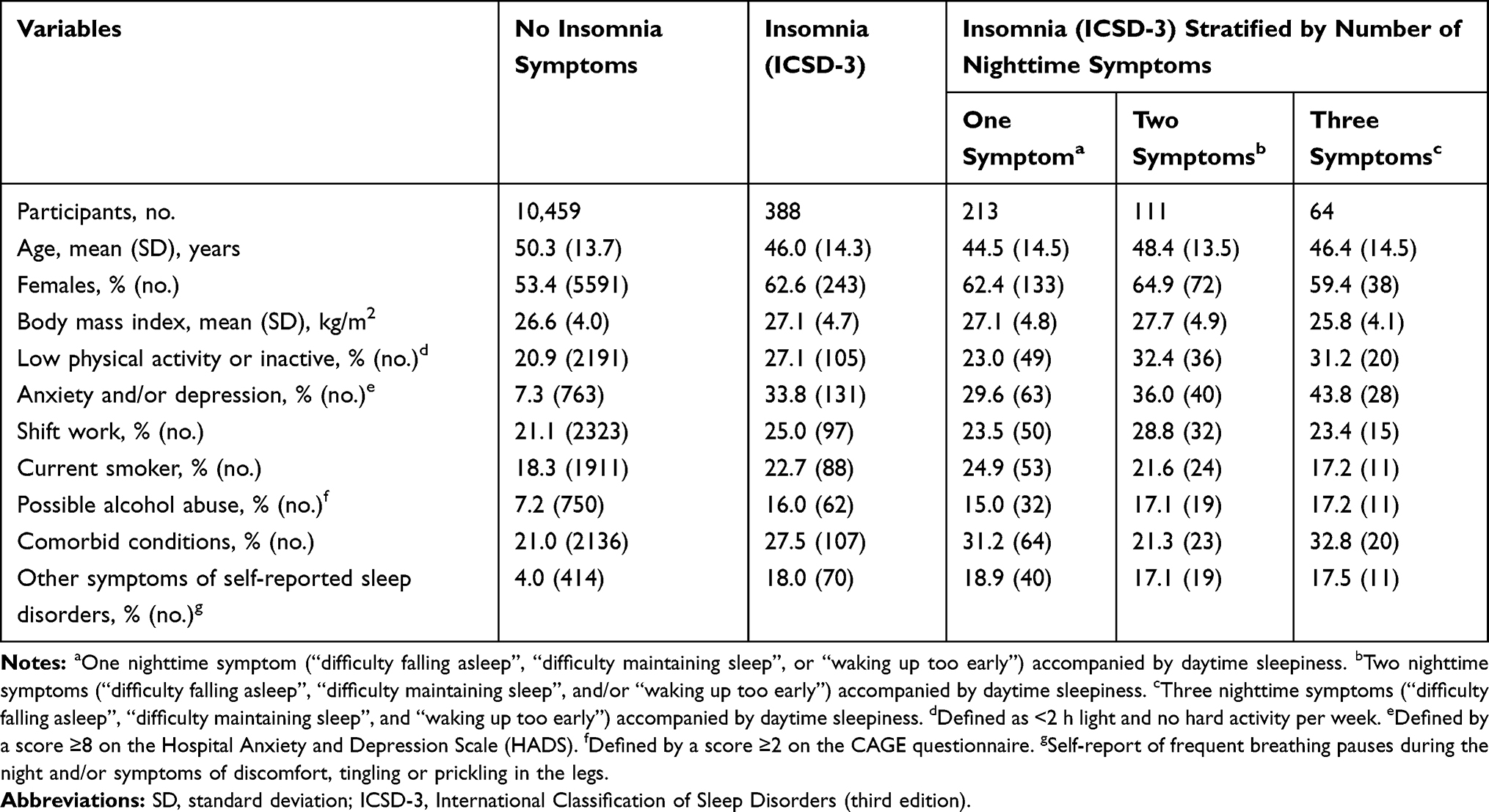 |
Table 1 Characteristics of the Study Population at Baseline in 2006–2008 Stratified by Insomnia Symptom Status |
Table 2 shows the association between insomnia and the number of insomnia symptoms at baseline and the risk of any chronic musculoskeletal pain at follow-up. Compared with the reference group of people without insomnia, people with insomnia had a RR for any chronic musculoskeletal pain of 1.39 (95% CI 1.25–1.53). When people with insomnia were categorized based on the number of nighttime symptoms, those who reported one, two or three nighttime symptoms had RRs of 1.37 (95% CI 1.20–1.57), 1.29 (95% CI 1.07–1.57) and 1.60 (95% CI 1.30–1.85), respectively.
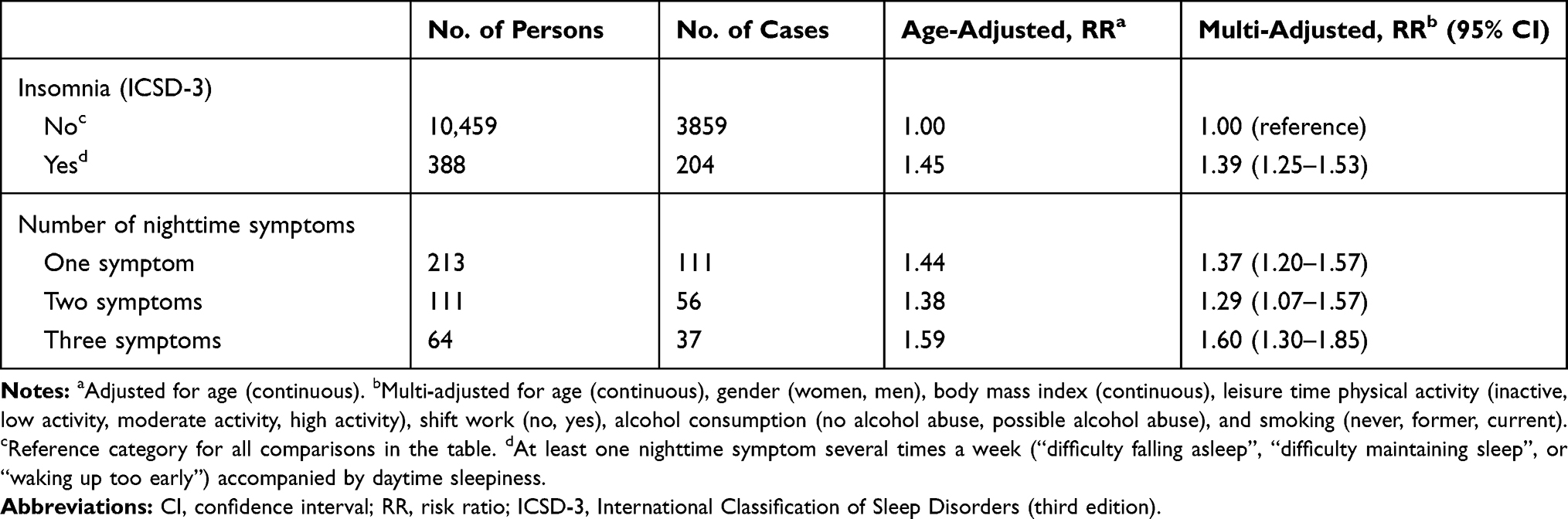 |
Table 2 Risk of Any Chronic Musculoskeletal Pain at Follow-Up in 2017–2019 Associated with Insomnia at Baseline in 2006–2008 |
Table 3 shows the association between insomnia and the number of insomnia symptoms at baseline and the risk of CWP. Compared to those without insomnia, people with insomnia had a RR for CWP of 1.64 (95% CI 1.26–2.14). The number of nighttime symptoms was strongly associated with the risk of CWP, ie, people who reported one nighttime symptom had a RR for CWP of 1.19 (95% CI 0.80–1.78), increasing to 3.08 (95% CI 1.93–4.92) in those who reported three nighttime symptoms.
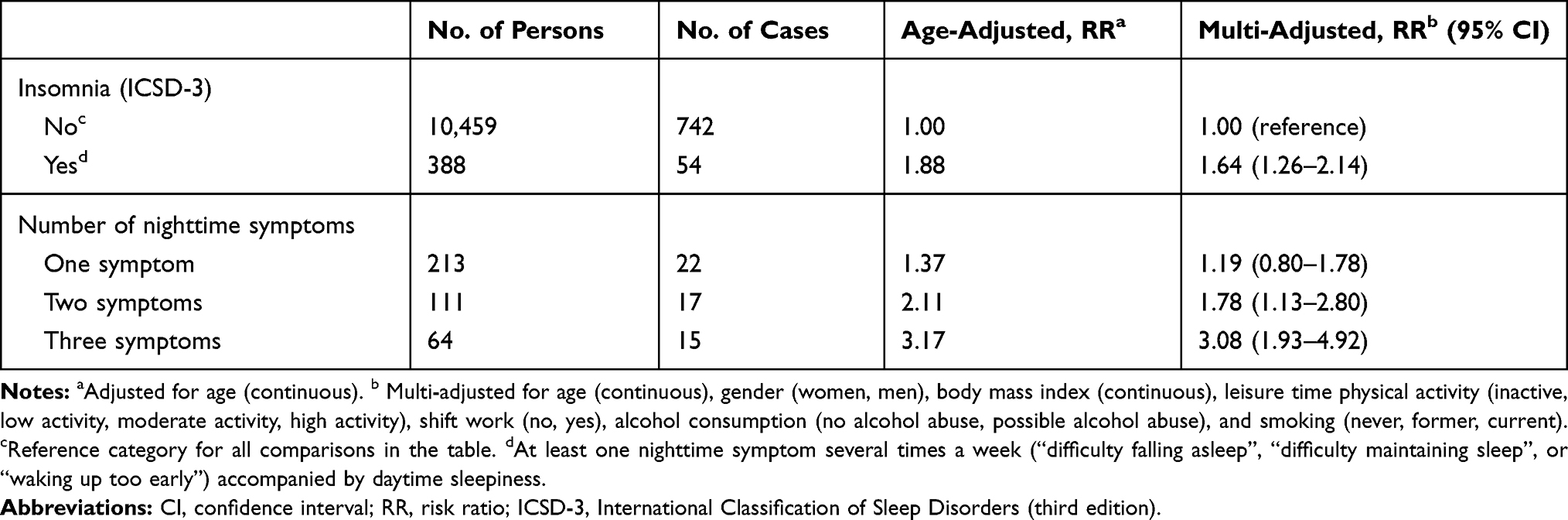 |
Table 3 Risk of Chronic Widespread Pain at Follow-Up in 2017–2019 Associated with Insomnia at Baseline in 2006–2008 |
The RRs for pain-related disability were 1.63 (95% CI 1.37–1.94) for those with insomnia, compared to those without insomnia (Table 4). Among those with insomnia, those who reported one nighttime symptom had a RR of 1.49 (95% CI 1.17–1.89) for pain-related disability, increasing to 2.46 (95% CI 1.76–3.42) in those who reported all three nighttime symptoms.
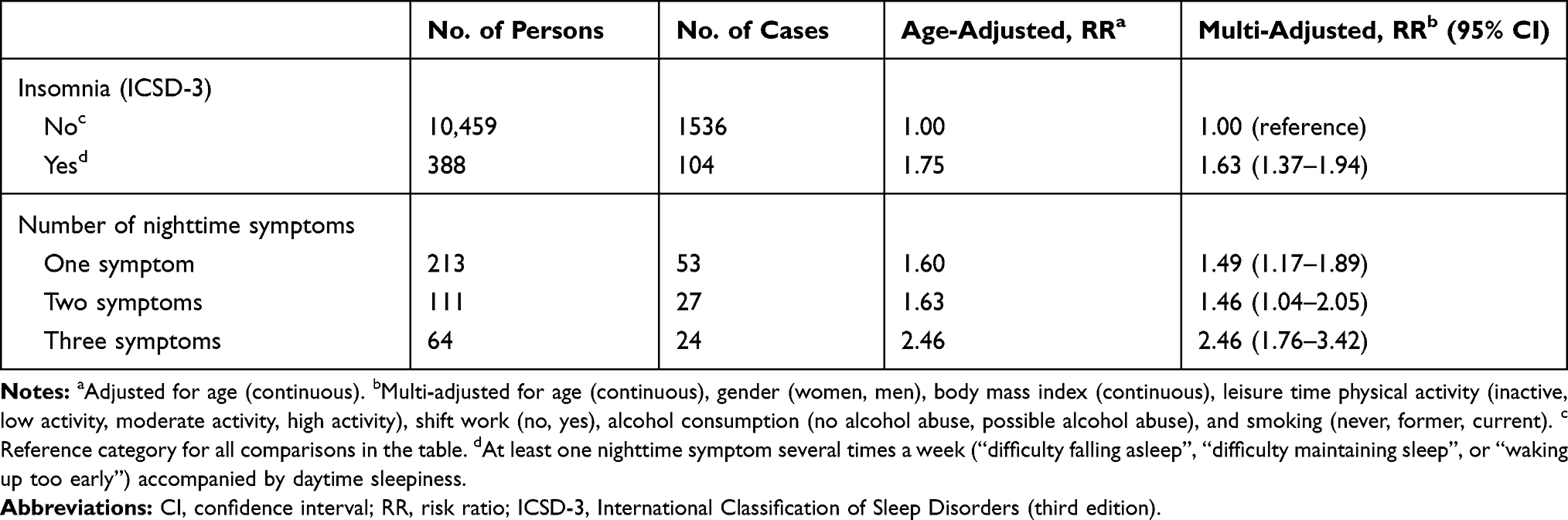 |
Table 4 Risk of Pain-Related Disability at Follow-Up in 2017–2019 Associated with Insomnia at Baseline in 2006–2008 |
Figure 1 shows the association between the number of insomnia symptoms at baseline and the risk of CWP and pain-related disability among people with insomnia. Taking people with one nighttime insomnia symptoms as the reference group, people with three nighttime symptoms had RRs of 2.29 (95% CI 1.24–4.23) and 1.55 (95% CI 1.04–2.32) for CWP and pain-related disability, respectively.
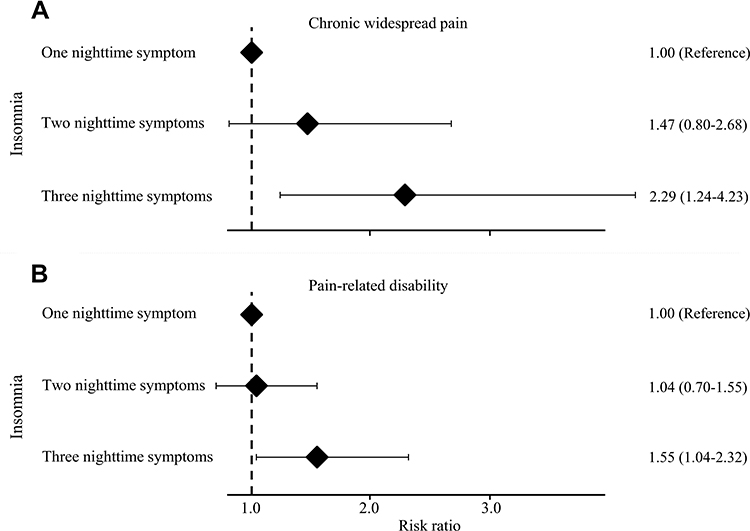 |
Figure 1 Risk of chronic widespread pain (A) and pain-related disability (B) associated with number of nighttime insomnia symptoms. People classified with chronic insomnia according to the current classification system were grouped into three categories based on the number of reported nighttime symptoms (ie, difficulty initiating sleep, trouble maintaining sleep and early morning awakenings). People with one nighttime symptom serve as the reference category. |
Supplementary Analyses
Two supplementary analyses were conducted to assess the robustness of the results. First additional adjustments for depression and/or anxiety and other comorbid conditions (diabetes, heart disease, lung disease, and rheumatic diseases) had negligible influence on the estimates showing ~5–15% reduction in risk compared to the main analysis. For instance, additional adjustments for poor mental health and medical conditions gave RRs for CWP of 0.99 (95% CI 0.60–1.64) for those who reported one nighttime symptoms, increasing to 2.62 (95% CI 1.46–4.70) in those who reported three nighttime symptoms. Second, the estimates in the main analysis remained unchanged after excluding people who reported frequent breathing pauses during the night and/or symptoms of discomfort, tingling or prickling in the legs.
Discussion
Our study shows that the risk of chronic musculoskeletal pain increases with the number of nighttime insomnia symptoms. People with insomnia characterized by symptoms in all phases of the sleep period, ie, difficulty initiating sleep, trouble maintaining sleep, and early morning awakenings, have a substantially greater risk of any chronic musculoskeletal pain, CWP and pain-related disability, compared to people without insomnia or people with insomnia but fewer nighttime symptoms. These findings suggest that insomnia is a heterogeneous condition and that the number of nighttime insomnia symptoms is an important factor influencing the association between insomnia and the risk of chronic musculoskeletal pain.
No previous study has explored whether the number of nighttime symptoms in people with insomnia is differentially associated with the risk of chronic musculoskeletal pain. It has been shown that insomnia, the number of insomnia symptoms and the frequency of sleep problems are associated with an increased risk for any chronic musculoskeletal pain,10,14 localized pain10,28 and widespread pain,10,13,14,29 although the criteria used to categorize people with insomnia were highly variable and not based on the current classification system.3 A large prospective study based on a previous survey of the HUNT Study found that the number of insomnia symptoms was strongly associated with the risk of fibromyalgia in women.13 However, since questions fulfilling the insomnia diagnosis were unavailable, participants were not classified with insomnia according to the current classification system. The current study adds to the literature by showing a cumulative effect of nighttime insomnia symptoms on the risk of CWP in people with a self-reported insomnia diagnosis. Although the precision of the estimates should be considered when interpreting our findings, it should be noted that people with one nighttime symptom did not have an increased risk of CWP compared to people without insomnia, whereas the risk was more than threefold among those who experienced three nighttime symptoms. This is in line with the view that symptoms in all phases of the sleep period (i.e., difficulty initiating sleep, trouble maintaining sleep, and early morning awakenings) are the most severe insomnia subtype,30 influencing daily functioning such as energy and mood.9,30 Our finding has important clinical implications, suggesting that reducing the severity of insomnia symptoms in people with chronic insomnia could be an important strategy towards the prevention of chronic pain and pain-related disability. However, further investigations are needed to establish whether it is the number of nighttime symptoms per se that impose an increased risk or if these associations are modified by certain combinations of nighttime symptoms.
There is a lack of studies investigating the association between the number of nighttime insomnia symptoms and the risk of pain-related disability. It has been shown that disturbed sleep may predict pain-related disability in patients with chronic pain, but the cross-sectional design precludes any conclusion about temporality.31,32 Our findings are consistent with prospective studies that have revealed a pathway between insomnia symptoms and reduced functional ability33 or work disability due to a chronic pain diagnosis.34,35 However, a direct comparison with our study is difficult since previous studies used different methods to assess pain-related disability, included participants with pain at baseline, and did not classify insomnia according to diagnostic criteria. Notably, our finding that those who reported three nighttime symptoms had more than 50% increased risk of developing disabling pain compared to those with one nighttime symptom is important because it indicates that the number of nighttime symptoms is a strong contributor to the development of chronic pain that impairs work ability and functioning in daily life.
The explanation for the strong association between the number of nighttime symptoms and risk of CWP and pain-related disability is unclear, but it is conceivable that people with sleeplessness in all phases of sleep have the greatest amount of total sleep loss or that specific nighttime symptoms are more strongly related to the development of chronic pain. Although speculative, it is possible that poor sleep maintenance is the most troublesome symptom when it comes to pain,15,16,36 and that problems with initiating sleep and/or early awakening are related to other characteristics such as age, gender and comorbid conditions (eg, mental health, use of hypnotics).9 However, further investigations are required to disentangle whether the development of chronic and disabling pain depends on the specific type and duration of the nighttime symptoms. So far, the processes linking insomnia and chronic musculoskeletal pain may be conceptualized through a framework of interconnected processes including immune responses, neurobiological changes, and altered cognitive and emotional pain processing.37–41 Prolonged sleep loss can induce an increased pro-inflammatory response by interfering with the hypothalamic-pituitary-adrenal axis and sympathetic nervous system.38 Prolonged dysregulation of pro-inflammatory markers can induce changes in peripheral and central pain processing,42 which have been implicated in the development of chronic pain states.43 Sleep loss may also exaggerate the sensation of pain by moderating the protective effect of positive affect on pain,40 weaken the ability to disengage from painful stimuli,41 or causing significant mood disruption (eg, anxiety and/or depression).39
The strengths of the current study include the large population with detailed information about insomnia symptoms, enabling long-term prospective analyses of the association between insomnia classified according to the third version of the ICSD and risk of chronic musculoskeletal pain. Other strengths include the detailed information on several possible confounders and that we were able to classify pain-free people based on the number of nighttime symptoms. However, due to the limited number of cases of CWP and pain-related disability at follow-up we could not classify participants into insomnia subtypes based on specific combinations of nighttime insomnia symptoms as suggested in a recent study.9 Unfortunately, we had no information on objectively measured sleep duration or sleep quality, nor did we have any information about pain intensity. Moreover, we could not stratify our analyses by gender, age, or other potential effect modifiers. Other limitations include the lack of information about the progression of insomnia symptoms and pain during the follow‐up or if new risk factors appeared. However, such risk factors need to be differential between the insomnia categories to influence our results. Moreover, pain-related disability was assessed by two questions related to work-disability and leisure activity rather than a validated scale. Changes in insomnia, chronic pain and other important confounders occurring between these two measurement points, or before our baseline could not be considered, and we cannot exclude the possibility of reverse causation. Poor sleep may be an early symptom of an undiagnosed or subclinical disease, and it should be noted that the analytical sample comprised individuals who were available for follow-up approximately a decade after initial recruitment. Thus, we might have had a healthy cohort that underestimates the association between insomnia and chronic pain. Finally, residual confounding by unmeasured or poorly measured factors cannot be ruled out.
Conclusions
In conclusion, this prospective study shows that people with chronic insomnia characterized by difficulty initiating sleep, trouble maintaining sleep and early morning awakenings have a substantially greater risk of any chronic musculoskeletal pain, CWP and pain-related disability, compared to people without insomnia or people with insomnia but fewer nighttime symptoms. These findings suggest that insomnia is a heterogenous condition and that the number of nighttime symptoms is an important factor that influences the association between insomnia and the risk of chronic musculoskeletal pain.
Data Sharing Statement
This study used data from the HUNT Study (https://www.ntnu.edu/hunt). Any research group with a Principal Investigator affiliated with a Norwegian research institute can apply for access to use data from the HUNT Study. This means that researchers from non-Norwegian countries must have a collaboration partner in Norway to be able to use data from the HUNT Study. Each project needs to be approved by the HUNT Data Access Committee, Regional Medical Ethical Committee, in some cases also the Data Inspectorate. Due to participant confidentiality, participant data are not publicly available.
Ethical Approval
The study was approved by the Regional Committee for Ethics in Medical Research (project no. 2014/612 REK Mid-Norway). The study was carried out according to the Declaration of Helsinki.
Acknowledgment
The Trøndelag Health Study (The HUNT Study) is a collaboration between the HUNT Research Centre (Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology), the Trøndelag County Council, the Central Norway Regional Health Authority, and the Norwegian Institute of Public Health. This work was supported by a grant to Eivind Schjelderup Skarpsno from the Liaison Committee between the Central Norway Regional Health Authority (RHA) and the Norwegian University of Science and Technology (NTNU).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Roth T, Coulouvrat C, Hajak G, et al. Prevalence and perceived health associated with insomnia based on DSM-IV-TR; International statistical classification of diseases and related health problems, tenth revision; and research diagnostic criteria/international classification of sleep disorders, second edition criteria: results from the America Insomnia Survey. Biol Psychiatry. 2011;69(6):592–600.
2. Winkelman JW, Solomon CG. Clinical practice. Insomnia disorder. N Engl J Med. 2015;373(15):1437–1444. doi:10.1056/NEJMcp1412740
3. Riemann D, Baglioni C, Bassetti C, et al. European guideline for the diagnosis and treatment of insomnia. J Sleep Res. 2017;26(6):675–700.
4. Hohagen F, Käppler C, Schramm E, Riemann D, Weyerer S, Berger M. Sleep onset insomnia, sleep maintaining insomnia and insomnia with early morning awakening–temporal stability of subtypes in a longitudinal study on general practice attenders. Sleep. 1994;17(6):551–554.
5. Pillai V, Roth T, Drake CL. The nature of stable insomnia phenotypes. Sleep. 2015;38(1):127–138. doi:10.5665/sleep.4338
6. Yokoyama E, Kaneita Y, Saito Y, et al. Association between depression and insomnia subtypes: a longitudinal study on the elderly in Japan. Sleep. 2010;33(12):1693–1702. doi:10.1093/sleep/33.12.1693
7. Roth T, Zammit G, Lankford A, et al. Nonrestorative sleep as a distinct component of insomnia. Sleep. 2010;33(4):449–458. doi:10.1093/sleep/33.4.449
8. Blanken TF, Benjamins JS, Borsboom D, et al. Insomnia disorder subtypes derived from life history and traits of affect and personality. Lancet Psychiatry. 2019;6(2):151–163. doi:10.1016/S2215-0366(18)30464-4
9. Bjorøy I, Jørgensen VA, Pallesen S, Bjorvatn B. The prevalence of insomnia subtypes in relation to demographic characteristics, anxiety, depression, alcohol consumption and use of hypnotics. Front Psychol. 2020;11:527. doi:10.3389/fpsyg.2020.00527
10. Uhlig BL, Sand T, Nilsen TI, Mork PJ, Hagen K. Insomnia and risk of chronic musculoskeletal complaints: longitudinal data from the HUNT study, Norway. BMC Musculoskelet Disord. 2018;19(1):128. doi:10.1186/s12891-018-2035-5
11. Agmon M, Armon G, Landau R. Increased insomnia symptoms predict the onset of back pain among employed adults. PLoS One. 2014;9(8):e103591. doi:10.1371/journal.pone.0103591
12. Morphy H, Dunn KM, Lewis M, Boardman HF, Croft PR. Epidemiology of insomnia: a longitudinal study in a UK population. Sleep. 2007;30(3):274–280.
13. Skarpsno ES, Nilsen TIL, Sand T, Hagen K, Mork PJ. The joint effect of insomnia symptoms and lifestyle factors on risk of self-reported fibromyalgia in women: longitudinal data from the HUNT Study. BMJ Open. 2019;9(8):e028684. doi:10.1136/bmjopen-2018-028684
14. Skarpsno ES, Mork PJ, Nilsen TIL, Steingrimsdottir OA, Zwart JA, Nilsen KB. The interplay between sleeplessness and high-sensitivity C-reactive protein on risk of chronic musculoskeletal pain. Longitudinal data from the Tromso Study. Sleep. 2019;42(9). doi:10.1093/sleep/zsz127
15. Lentz MJ, Landis CA, Rothermel J, Shaver JL. Effects of selective slow wave sleep disruption on musculoskeletal pain and fatigue in middle aged women. J Rheumatol. 1999;26(7):1586–1592.
16. Smith MT, Edwards RR, McCann UD, Haythornthwaite JA. The effects of sleep deprivation on pain inhibition and spontaneous pain in women. Sleep. 2007;30(4):494–505. doi:10.1093/sleep/30.4.494
17. Engstrøm M, Ødegård S, Sand T, Stovner L, Zwart J, Hagen K. The reliability of a new sleep screening questionnaire for large population-based studies: the third Nord-Trøndelag Health Study. Open Sleep J. 2011;4:14–19. doi:10.2174/1874620901104010014
18. Kuorinka I, Jonsson B, Kilbom Å, Vinterberg H, Biering-Sørensen F, Andersson G. Standardised nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon. 1987;18(3):233–237. doi:10.1016/0003-6870(87)90010-X
19. Hagen K, Linde M, Heuch I, Stovner LJ, Zwart JA. Increasing prevalence of chronic musculoskeletal complaints. A large 11-year follow-up in the general population (HUNT 2 and 3). Pain Med. 2011;12(11):1657–1666. doi:10.1111/j.1526-4637.2011.01240.x
20. Kurtze N, Rangul V, Hustvedt BE, Flanders WD. Reliability and validity of self-reported physical activity in the Nord-Trondelag Health Study (HUNT 2). Eur J Epidemiol. 2007;22(6):379–387. doi:10.1007/s10654-007-9110-9
21. Ewing JA. Detecting alcoholism. The CAGE questionnaire. JAMA. 1984;252(14):1905–1907. doi:10.1001/jama.1984.03350140051025
22. Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the hospital anxiety and depression scale. An updated literature review. J Psychosom Res. 2002;52(2):69–77. doi:10.1016/S0022-3999(01)00296-3
23. Taylor DJ, Mallory LJ, Lichstein KL, Durrence HH, Riedel BW, Bush AJ. Comorbidity of chronic insomnia with medical problems. Sleep. 2007;30(2):213–218. doi:10.1093/sleep/30.2.213
24. Katz DA, McHorney CA. Clinical correlates of insomnia in patients with chronic illness. Arch Intern Med. 1998;158(10):1099–1107. doi:10.1001/archinte.158.10.1099
25. Alvaro PK, Roberts RM, Harris JK. A systematic review assessing bidirectionality between sleep disturbances, anxiety, and depression. Sleep. 2013;36(7):1059–1068. doi:10.5665/sleep.2810
26. Tentindo GS, Fishman SM, Li CS, Wang Q, Brass SD. The prevalence and awareness of sleep apnea in patients suffering chronic pain: an assessment using the STOP-bang sleep apnea questionnaire. Nat Sci Sleep. 2018;10:217–224. doi:10.2147/NSS.S167658
27. Hoogwout SJ, Paananen MV, Smith AJ, et al. Musculoskeletal pain is associated with restless legs syndrome in young adults. BMC Musculoskelet Disord. 2015;16:294. doi:10.1186/s12891-015-0765-1
28. Mork PJ, Vik KL, Moe B, Lier R, Bardal EM, Nilsen TIL. Sleep problems, exercise and obesity and risk of chronic musculoskeletal pain: the Norwegian HUNT study. Eur J Public Health. 2014;24(6):924–929. doi:10.1093/eurpub/ckt198
29. Gupta A, Silman AJ, Ray D, et al. The role of psychosocial factors in predicting the onset of chronic widespread pain: results from a prospective population-based study. Rheumatology (Oxford). 2007;46(4):666–671. doi:10.1093/rheumatology/kel363
30. Espie CA, Kyle SD, Hames P, Cyhlarova E, Benzeval M. The daytime impact of DSM-5 insomnia disorder. J Clin Psychiatry. 2012;73(12):e1478–e1484. doi:10.4088/JCP.12m07954
31. McCracken LM, Iverson GL. Disrupted sleep patterns and daily functioning in patients with chronic pain. Pain Res Manag. 2002;7(2):75–79. doi:10.1155/2002/579425
32. Naughton F, Ashworth P, Skevington SM. Does sleep quality predict pain-related disability in chronic pain patients? The mediating roles of depression and pain severity. Pain. 2007;127(3):243–252. doi:10.1016/j.pain.2006.08.019
33. Baker S, McBeth J, Chew-Graham CA, Wilkie R. Musculoskeletal pain and co-morbid insomnia in adults; a population study of the prevalence and impact on restricted social participation. BMC Fam Pract. 2017;18(1):17. doi:10.1186/s12875-017-0593-5
34. Ropponen A, Silventoinen K, Hublin C, Svedberg P, Koskenvuo M, Kaprio J. Sleep patterns as predictors for disability pension due to low back diagnoses: a 23-year longitudinal study of finnish twins. Sleep. 2013;36(6):891–897. doi:10.5665/sleep.2718
35. Salo P, Oksanen T, Sivertsen B, et al. Sleep disturbances as a predictor of cause-specific work disability and delayed return to work. Sleep. 2010;33(10):1323–1331.
36. Moldofsky H, Scarisbrick P. Induction of neurasthenic musculoskeletal pain syndrome by selective sleep stage deprivation. Psychosom Med. 1976;38(1):35–44. doi:10.1097/00006842-197601000-00006
37. Haack M, Simpson N, Sethna N, Kaur S, Mullington J. Sleep deficiency and chronic pain: potential underlying mechanisms and clinical implications. Neuropsychopharmacology. 2020;45(1):205–216. doi:10.1038/s41386-019-0439-z
38. Irwin MR, Olmstead R, Carroll JE. Sleep disturbance, sleep duration, and inflammation: a systematic review and meta-analysis of cohort studies and experimental sleep deprivation. Biol Psychiatry. 2016;80(1):40–52. doi:10.1016/j.biopsych.2015.05.014
39. Whibley D, AlKandari N, Kristensen K, et al. Sleep and pain: a systematic review of studies of mediation. Clin J Pain. 2019;35(6):544–558. doi:10.1097/AJP.0000000000000697
40. Finan PH, Quartana PJ, Remeniuk B, et al. Partial sleep deprivation attenuates the positive affective system: effects across multiple measurement modalities. Sleep. 2017;40:1. doi:10.1093/sleep/zsw017
41. Tiede W, Magerl W, Baumgartner U, Durrer B, Ehlert U, Treede RD. Sleep restriction attenuates amplitudes and attentional modulation of pain-related evoked potentials, but augments pain ratings in healthy volunteers. Pain. 2010;148(1):36–42. doi:10.1016/j.pain.2009.08.029
42. Wieseler-Frank J, Maier SF, Watkins LR. Central proinflammatory cytokines and pain enhancement. Neurosignals. 2005;14(4):166–174. doi:10.1159/000087655
43. Zhang JM, An J. Cytokines, inflammation, and pain. Int Anesthesiol Clin. 2007;45(2):27–37. doi:10.1097/AIA.0b013e318034194e
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.