Back to Journals » Clinical Ophthalmology » Volume 20
Novel Non-Valved Glaucoma Drainage Device with Reduced Inner Lumen Diameter: 6-Month Safety and Efficacy Outcomes
Authors Shi KSY ![]() , Vasu P, Oyama K
, Vasu P, Oyama K ![]() , Thé RY
, Thé RY ![]() , Wang M
, Wang M ![]() , Banoub RG, Ang BCH, Dorairaj SK
, Banoub RG, Ang BCH, Dorairaj SK
Received 15 April 2026
Accepted for publication 18 June 2026
Published 23 June 2026 Volume 2026:20 615265
DOI https://doi.org/10.2147/OPTH.S615265
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sotiria Palioura
Kelvin SY Shi,1 Pranav Vasu,2 Kody Oyama,3 Ryan Y Thé,4 Melanie Wang,5 Raphael G Banoub,1 Bryan CH Ang,6 Syril K Dorairaj1
1Department of Ophthalmology, Mayo Clinic, Jacksonville, FL, USA; 2Department of Medicine, Creighton University School of Medicine, Phoenix, AZ, USA; 3Department of Medicine, Albert Einstein College of Medicine, New York, NY, USA; 4Department of Medicine, Wayne State University School of Medicine, Detroit, MI, USA; 5Department of Medicine, Carle Illinois College of Medicine, Urbana, IL, USA; 6Department of Ophthalmology, Tan Tock Seng Hospital, Singapore, Singapore
Correspondence: Syril K Dorairaj, Mayo Clinic Florida, 4500 San Pablo Road S, Jacksonville, FL, 32224, USA, Tel +1 904 953-7110, Email [email protected]
Purpose: To evaluate the safety and clinical efficacy of the Ahmed ClearPath® Small Tube (ACP-ST), a novel non-valved glaucoma drainage device with a reduced inner lumen diameter, in the management of glaucoma.
Methods: This retrospective chart review included 17 eyes that underwent ACP-ST implantation between February 25, 2025, and November 24, 2025. Surgical success was defined as a ≥ 20% reduction in IOP from baseline with a postoperative IOP > 5 mmHg and no need for additional surgical intervention. Changes in IOP, glaucoma medication burden, and best-corrected visual acuity (BCVA) were evaluated through 6 months. Intraoperative and postoperative complications were recorded.
Results: Fourteen eyes had available 6-month follow-up data. Mean IOP decreased from 27.19 ± 6.29 mmHg at baseline to 12.21 ± 5.45 mmHg at 6 months, representing a 55.1% reduction (P < 0.0001). Mean glaucoma medication use decreased from 3.35 ± 1.14 to 1.07 ± 0.99 medications, corresponding to a 68.1% reduction (P < 0.0001). Surgical success was achieved in all 14 eyes (100%) with available 6-month follow-up. No intraoperative complications occurred, and no cases of postoperative hypotony or IOP spikes were observed.
Conclusion: These preliminary findings suggest that ACP-ST may achieve clinically meaningful reductions in IOP and glaucoma medication burden while maintaining a favorable short-term safety profile, as no cases of postoperative hypotony or IOP spikes were observed. However, given the retrospective design, small sample size, and limited duration of follow-up, further longitudinal studies with larger cohorts will be necessary to better evaluate the durability and long-term safety of ACP-ST.
Keywords: glaucoma drainage device, Glaucoma, Ahmed ClearPath Small-Tube, Ahmed implants
Introduction
Glaucoma is a progressive optic neuropathy characterized by the acquired loss of retinal ganglion cells and their axons, leading to characteristic optic nerve head changes and corresponding visual field loss.1,2 Among the various risk factors, intraocular pressure (IOP) remains the only proven modifiable factor for slowing disease progression.1,2 Reduction of IOP can be achieved with pharmacotherapy, laser interventions, or surgical procedures such as trabeculectomy. However, for eyes with refractory glaucoma that cannot be controlled with these measures, the Tube versus Trabeculectomy (TVT) study showed that glaucoma drainage devices (GDDs) have become the preferred surgical option and provide a viable alternative to repeat trabeculectomy.3,4 Since the first GDD was developed by Molteno in 1969, advances in device design, including modifications in size, shape, and biomaterials, have improved surgical efficacy and reduced complication rates.5
Among these devices, the Ahmed ClearPath® (ACP, New World Medical Inc., Rancho Cucamonga, CA, USA) is a valveless GDD approved by the United States Food and Drug Administration (FDA) in 2019. It has since gained global attention for its efficacy, with 88.9% of eyes maintaining a ≥20% IOP reduction in a 12-eye cohort at 36 months.3 In the study by Grover et al, however, hypotony remained one of the most frequent postoperative complications, ranking third overall and accounting for 6.7% of all adverse events.4
The ACP Small Tube (ST) represents a newer generation of valveless GDDs. Compared to ACP, which has an inner lumen diameter of 305 μm, the ACP-ST features a reduced inner diameter of 127 μm (manufacturer-reported specification from a trade publication; official peer-reviewed documentation is not yet available).6 This smaller lumen is intended to maintain the principle of non-restrictive outflow while allowing for the utilization of a rip-cord to regulate aqueous humor drainage, thereby potentially reducing early postoperative complications such as hypotony. Launched in 2025, the ACP-ST is available in two plate sizes, 250 mm2 and 350 mm2, offering a compact design aimed at improving IOP control while enhancing safety.
Given the recent introduction of the ACP-ST across global markets since 2025, available literature evaluating its clinical performance remains limited. To address this gap, the present study retrospectively evaluates the safety and efficacy of the ACP-ST when implanted as a standalone procedure in eyes with uncontrolled glaucoma, analyzing early clinical outcomes from a cohort of 17 eyes.
Methods
A retrospective, single surgeon, noncomparative study was conducted at the Mayo Clinic. The study protocol was reviewed and approved with a waiver of informed consent by the Mayo Clinic Institutional Review Board (IRB Number: 26–004408) due to the retrospective nature of the study. All patient identifying information was removed prior to analysis, and patient confidentiality was maintained throughout the study. This study was conducted in accordance with the tenets of the Declaration of Helsinki of 1964 and its later amendments. The medical records of consecutive patients who underwent ACP-ST implantation between February 25th, 2025 and November 24th, 2025, were reviewed and deidentified data were collected. Patients 18 years or older with a diagnosis of uncontrolled glaucoma with medical therapy with or without prior laser/surgical procedures were included in the study.
Surgical Technique
A single surgeon performed all procedures. For each eye, the ACP-ST device was implanted in the superotemporal quadrant. After a 100-degree peritomy and posterior dissection of Tenon’s capsule, the lateral rectus and superior rectus muscle insertions were identified, and the underbelly of each was cleaned with a muscle hook. The ACP-ST plate was then positioned posterior to the rectus muscle insertions and secured approximately 8 mm posterior to the limbus with two 8–0 nylon sutures. No ligation of the tube was performed in any case. The tube was trimmed to the appropriate length with the bevel facing up, and 2 mm of the tube was inserted into the anterior chamber through a beveled 25-gauge scleral incision, leaving 4 mm external to the entry site, where it was secured with 8–0 nylon. The built-in 6–0 polypropylene ripcord had its distal end tucked into the inferior fornix. A Tutoplast patch graft, pre-soaked in antibiotic solution, was then placed over the tube and secured with 8–0 nylon and Tisseel glue. The conjunctiva and Tenon’s capsule were advanced to the limbus and reapproximated with 10–0 nylon and Tisseel glue. At the conclusion of surgery, topical antibiotic-steroid ointment and atropine drops were administered, and the eye was patched and shielded. The ripcord suture was subsequently removed at the postoperative day 1 visit.
Data Collection
Demographic and clinical data, including age, sex, race, lens status, glaucoma type and severity, and history of prior glaucoma surgery, were obtained from the electronic medical record. Patients were evaluated preoperatively, intraoperatively, and postoperatively at day 1, week 1, and months 1, 3, and 6. Preoperative and postoperative assessments included IOP, number of glaucoma medications, and BCVA. Glaucoma medications included alpha agonists, beta blockers, carbonic anhydrase inhibitors, prostaglandin analogs, pilocarpine, and combination formulations. IOP was measured using Goldmann applanation tonometry, and BCVA was assessed using a Snellen chart at a testing distance of 20 feet. Baseline measurements were obtained one day prior to surgery. Slit lamp microscopy and dilated fundus examination were performed to evaluate the anterior and posterior segments. Glaucoma severity was classified according to the International Classification of Diseases, Tenth Revision.7
Statistical Methods
All data were de-identified and independently analyzed by two investigators using GraphPad Prism Version 10.2.2 (GraphPad Software, Boston, MA, USA) and RStudio (Posit PBC, Boston, MA, USA). Descriptive statistics were used to summarize baseline characteristics and demographics, with continuous variables presented as means with standard deviations and categorical variables reported as frequencies and percentages.
Quantitative outcomes assessed included changes from baseline in IOP, number of glaucoma medications, and BCVA at each postoperative visit, as well as intraoperative and postoperative complications and the proportion of eyes achieving surgical success at each follow-up time point. Surgical success was defined as a ≥20% reduction in IOP from baseline with an IOP >5 mmHg and without the need for additional surgical intervention. BCVA measurements obtained using Snellen visual acuity charts were converted to logarithm of the minimum angle of resolution (logMAR) values using the formula: logMAR = log10(Snellen denominator/Snellen numerator).
Normality of continuous data was first assessed. For comparisons involving paired observations with normally distributed data, two tailed paired t tests were used, while Wilcoxon signed rank tests were applied for paired data that were not normally distributed. For comparisons involving unpaired observations with unequal sample sizes and non-normal distributions, unpaired t tests were used. Statistical significance was defined as P < 0.05.
Results
Demographic and Preoperative Glaucoma Status
Demographic information of patients and baseline characteristics are detailed in Table 1. In total, 17 eyes from 16 patients were collected, with an average follow up of 156.06 ± 53.77 days. The mean (SD) age of the cohort was 68.8 (15.0) and the majority of patients were Caucasian (n = 11, 68.75%) and female (n = 10, 62.5%). Various glaucoma etiologies were represented, including primary open-angle glaucoma (POAG; 82.35%), secondary open-angle glaucoma (SOAG; 11.76%), and secondary angle-closure glaucoma (SACG; 5.88%). Of the total sample, 2 eyes had moderate glaucoma (11.76%) and 15 eyes had severe glaucoma (88.24%). 3 eyes were phakic (17.65%) and 14 eyes were pseudophakic (82.35%) at the time of surgery. Twelve eyes (70.59%) had undergone at least one prior glaucoma surgery, while one eye (5.9%) had no prior surgical intervention. Nine eyes were right eyes (52.9%) and eight were left eyes (47.1%) (Table 1).
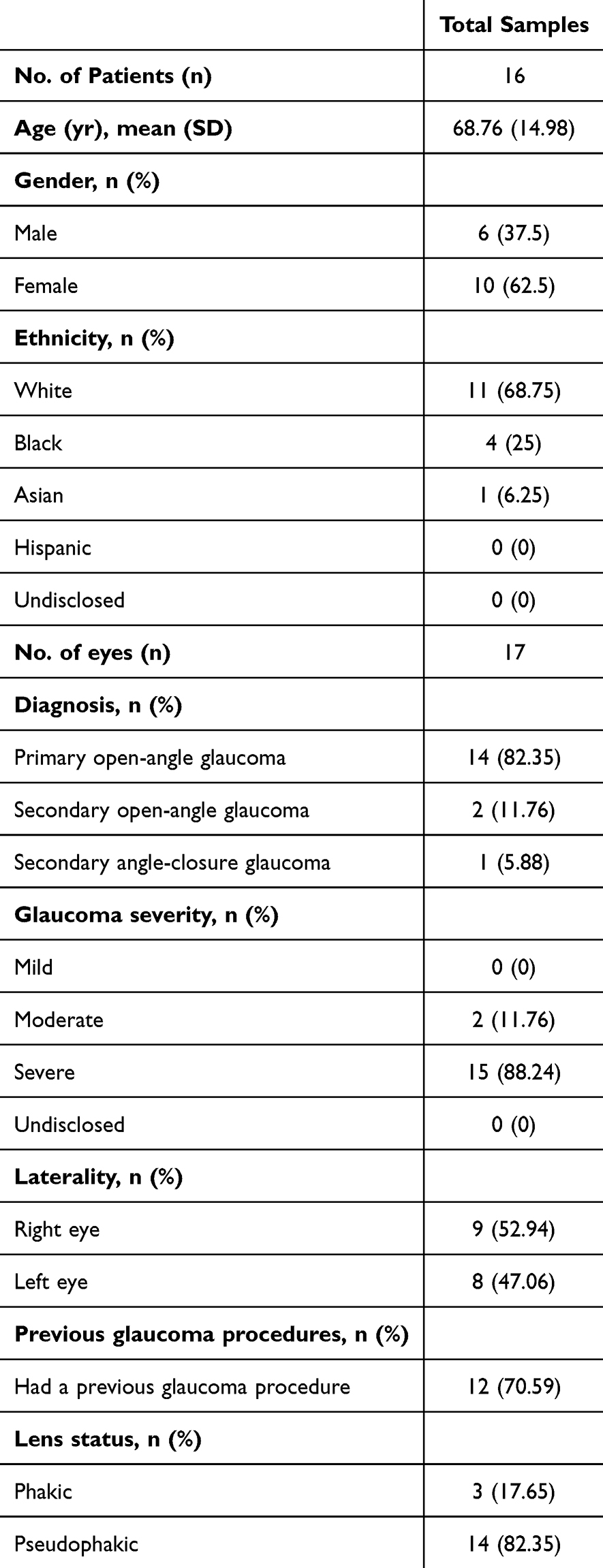 |
Table 1 Demographic and Preoperative Glaucoma Status of Study Patients |
Mean IOP from Baseline Through Follow-Up
Mean IOP at baseline and each postoperative visit demonstrated a significant reduction from baseline at all time points (Figure 1). The mean (SD) baseline IOP was 27.19 (6.29) mmHg. On postoperative day 1, mean IOP significantly decreased to 11.12 (8.48) mmHg, representing a 59.1% reduction from baseline (p < 0.0001). At postoperative week 1, mean IOP was 11.76 (6.68) mmHg, corresponding to a 56.7% reduction (p < 0.0001). At postoperative month 1, mean IOP was 13.59 (7.62) mmHg, representing a 50.0% reduction from baseline (p < 0.0001). At postoperative month 3, mean IOP decreased to 10.82 (7.48) mmHg, corresponding to a 60.2% reduction (p < 0.0001). At postoperative month 6, among the remaining 14 eyes, mean IOP was 12.21 (5.45) mmHg, representing a 55.1% reduction from baseline (p < 0.0001).
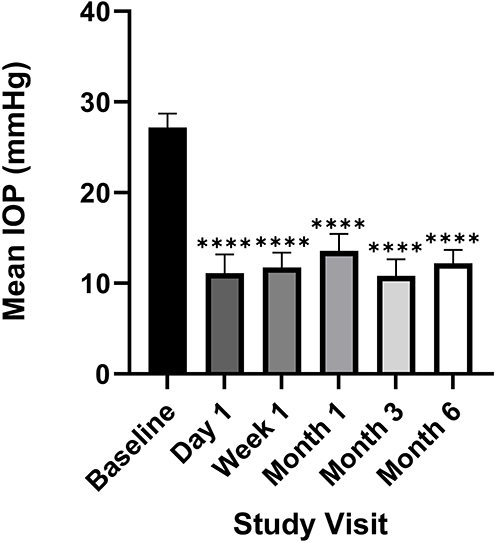 |
Figure 1 Mean intraocular pressure (IOP) over time. Error bar represents standard error of the mean. Statistical comparisons were performed relative to baseline (****p < 0.0001). |
Glaucoma Medication Usage from Baseline Through Follow-Up
Mean glaucoma medication use at baseline and each postoperative visit demonstrated a significant reduction from baseline at all time points (Figure 2). The mean (SD) number of medications at baseline was 3.35 (1.41). On postoperative day 1, mean medication use significantly decreased to 1.88 (1.27), representing a 43.9% reduction from baseline (p = 0.0005). At postoperative week 1, mean medication use was 1.06 (1.14), corresponding to a 68.4% reduction (p < 0.0001). At postoperative month 1, mean medication use was 1.18 (1.29), representing a 64.8% reduction from baseline (p < 0.0001). At postoperative month 3, mean medication use decreased to 1.00 (1.06), corresponding to a 70.1% reduction (p < 0.0001). At postoperative month 6, among the remaining 14 eyes, mean medication use was 1.07 (0.99), representing a 68.1% reduction from baseline (p < 0.0001).
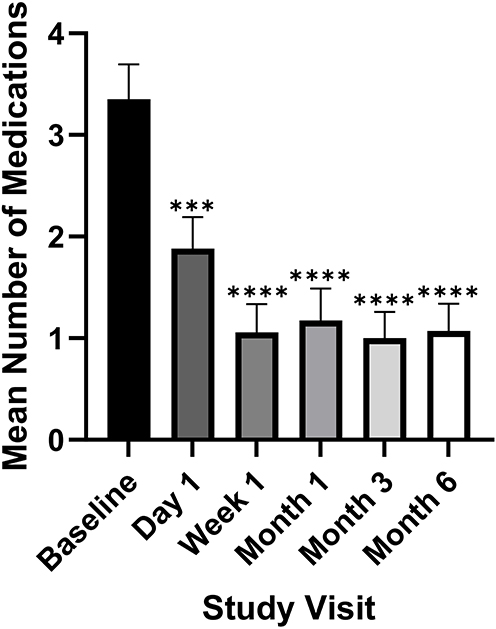 |
Figure 2 Mean glaucoma medication use over time. Error bar represents standard error of the mean. Statistical comparisons were performed relative to baseline (***p < 0.001; ****p < 0.0001). |
The proportion of eyes requiring no glaucoma medications was also recorded at each postoperative visit. At postoperative day 1, 3 of 17 eyes (17.6%) were medication-free. This proportion increased to 8 of 17 eyes (47.1%) at postoperative week 1 and remained unchanged at postoperative month 1 and postoperative month 3, with 8 of 17 eyes (47.1%) requiring no glaucoma medications at either time points. At postoperative month 6, among the remaining 14 eyes, 6 eyes (42.9%) remained medication-free.
BCVA from Baseline Through Follow-Up
BCVA was collected at all time points and converted to logMAR for analysis. The mean (SD) baseline logMAR BCVA was 0.57 (0.68). On postoperative day 1, mean logMAR BCVA was 0.84 (0.59) (p = 0.0085). At postoperative week 1, mean logMAR BCVA was 0.81 (0.72) (p = 0.12). At postoperative month 1, mean logMAR BCVA was 0.67 (0.76) (p = 0.48). At postoperative month 3, mean logMAR BCVA was 0.74 (0.72) (p = 0.2930). At postoperative month 6, mean logMAR BCVA was 0.39 (0.58) (p = 0.3060). Statistical significance relative to baseline was observed only at postoperative day 1.
Complications
The procedure was performed without intraoperative complications in all eyes. Mild hyphema (noted in 3 eyes), defined as circulating red blood cells without a layered blood level or a blood layer measuring less than 1 mm in the anterior chamber, was not classified as a major complication given its self-limiting nature. No cases of postoperative hypotony or IOP spikes were observed at any follow-up time point. No vision-threatening complications were noted throughout the follow-up period.
Although no complications were directly attributable to ACP-ST, two notable postoperative events were observed. In one case, a patient developed a suprachoroidal hemorrhage during the postoperative period. The patient had been taken off anticoagulation for surgery and initially demonstrated a favorable course, with well-controlled IOP and no need for medications at postoperative day 1 and week 1. However, following early resumption of antithrombotic therapy, the patient subsequently presented with a sudden IOP spike and was found to have hemorrhagic choroidal effusions. Given the timing and the presence of significant underlying coagulopathic risk factors, this event was considered more likely related to systemic anticoagulation rather than ACP-ST implantation. In a second case, ACP-ST explantation was required due to patient-related factors rather than device performance. The patient, with dementia and a recent diagnosis of Alzheimer’s disease, repeatedly manipulated the operative eye, including rubbing the implantation site and attempting to irrigate it with an alkaline solution, ultimately necessitating device removal.
Surgical Success
On postoperative day 1 and week 1, 13 of 17 eyes (76.5%) achieved surgical success, defined as an IOP reduction of ≥20% from baseline with a postoperative IOP >5 mmHg. At postoperative month 1, 14 of 17 eyes (82.4%) achieved surgical success, while at postoperative month 3, 13 of 17 eyes (76.5%) met the success criterion. At month 6, all 14 eyes with available follow-up (100%) met this criterion successfully. A scatter plot illustrating surgical success among eyes with available 6-month follow-up is presented in Figure 3.
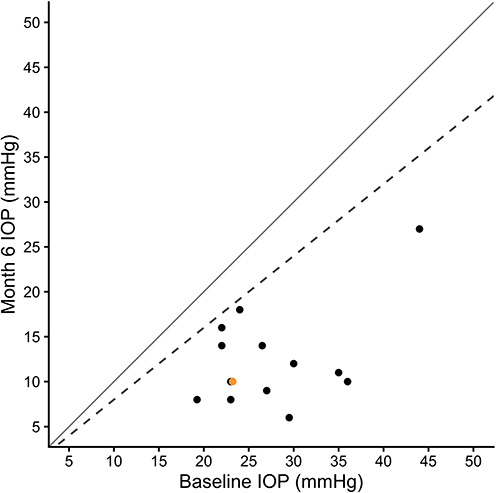 |
Figure 3 Scatter Plot of Preoperative Intraocular Pressure (IOP) Versus Postoperative IOP at 6 Months. The plot demonstrates the relationship between preoperative IOP (x-axis) and postoperative IOP at the 6-month visit (y-axis). Each point represents one eye with available 6-month follow-up; eyes without available data were omitted. A total of 14 eyes were included. Two eyes exhibited identical values and are displayed as separate adjacent Orange and black markers to facilitate visualization of both data points. The solid line represents equality between baseline and 6-month IOP. The dashed line indicates a 20% reduction from baseline. Eyes below the dashed line achieved at least a 20% reduction in IOP at 6 months. |
Discussion
GDDs are broadly classified as valved or non-valved based on the presence of a flow-restricting mechanism.8 In the five-year Ahmed–Baerveldt Comparison (ABC) study, valveless GDDs were compared with valved GDDs and were shown to be associated with a significantly lower risk of failure due to inadequate IOP control or need for reoperation (p = 0.003), but at the cost of increased safety-related failures, including persistent hypotony.9 These findings underscore the fundamental trade-off in valveless GDD design between improved efficacy and higher hypotony risk, which led to the development of the ACP-ST to potentially preserve IOP-lowering efficacy while mitigating early postoperative hypotony through increased intrinsic outflow resistance.
In this retrospective study, we report early clinical and safety efficacy data from a cohort of patients who were followed 6 months after undergoing standalone ACP-ST implantation. All procedures were performed at the same center by a single surgeon, ensuring consistency and validity of the surgical technique and results. To the best of our knowledge, this analysis represents the first data regarding ACP-ST outcomes to date.
Efficacy Profile
The Paul Glaucoma Implant (PGI; Advanced Ophthalmic Innovations, Singapore, Republic of Singapore) represents the most comparable valveless GDD with a similarly reduced inner lumen diameter of 127 μm. In José et al’s study evaluating the initial clinical safety and efficacy of PGI, 10 eyes had undergone prior glaucoma procedures, including trabeculotomy (2 eyes), GDD implantation (3 eyes), trabeculectomy (4 eyes), and microshunt implantation (1 eye).10 Similarly, in our cohort, 12 eyes had a history of prior glaucoma surgical management, including gel stent implantation (6 eyes), GDD implantation (1 eye), and trabeculectomy (3 eyes), reflecting a comparably complex and surgically experienced population.
In José et.al’s PGI evaluation, mean IOP decreased from 31.4 ± 10.0 mmHg at baseline to 13.8 ± 5.3 mmHg at 6 months, representing a 56.1% reduction (p < 0.001).10 At similar 6-month time point, our ACP-ST cohort demonstrated a reduction in mean IOP from 27.19 ± 6.29 mmHg at baseline to 12.21 ± 5.45 mmHg, representing a 55.1% reduction (p < 0.0001), indicating a comparable magnitude of IOP lowering to PGI. These findings support the ability of ACP-ST to achieve effective IOP control comparable to the current small lumen valveless GDD.
Meanwhile, the ACP-ST cohort also demonstrated a comparable reduction in medication burden to PGI. In José et.al’s study, mean medication use decreased from 2.7 ± 1.5 at baseline to 0.8 ± 1.1 at 6 months, representing a 70.4% (p < 0.05).10 Similarly, in our cohort, the mean (SD) number of medications decreased from 3.35 ± 1.41 at baseline to 1.07 ± 0.99 at postoperative month 6 among the remaining 14 eyes, representing a 68.1% reduction (p < 0.0001). These findings further support the comparable efficacy of ACP-ST in reducing both IOP and medication burden at a similar follow up time point.
Safety Profile
No intraoperative complications were observed, and postoperative events were transient, self-limited, and consistent with those expected following GDD implantation. Importantly, no complications were directly attributable to the ACP-ST device. Although two notable postoperative events occurred during the study period, both were considered more likely to be related to patient-specific factors than device performance. In the case of the suprachoroidal hemorrhage, the patient demonstrated an initially favorable postoperative course with well-controlled IOP and no complications at postoperative day 1 and week 1; the hemorrhagic event developed only after resumption of systemic antithrombotic therapy in the setting of significant underlying medical comorbidities and coagulopathic risk factors. Similarly, the patient who ultimately required ACP-ST explantation had an otherwise standard postoperative recovery during the early follow-up period, with device removal becoming necessary only after repeated postoperative manipulation of the operative eye three months after implantation.
Beyond these individual cases, a major safety concern following GDD implantation is postoperative hypotony, especially in valveless GDDs.9,11 The ACP-ST was specifically engineered to mitigate this risk through a reduced inner lumen diameter, thereby providing intrinsic resistance to aqueous outflow, especially in the early postoperative period prior to fibrous encapsulation. Unlike traditional valved GDDs, which rely on a mechanical valve to restrict flow, the ACP-ST achieves flow modulation through its small-lumen design while maintaining the efficacy advantages associated with non-valved devices. Compared to the standard ACP device, which has an inner lumen diameter of 305 μm and an outer diameter of 635 μm, the ACP-ST features a reduced inner lumen diameter of 127 μm and an outer diameter of 457 μm.6 Although this represents an approximately 60% reduction in lumen diameter, resistance to flow increases exponentially. This substantial increase in resistance, alongside proper suture size and placement, enables controlled aqueous drainage without the need for adjunctive flow-restricting techniques such as tube ligation. Consistent with this intended mechanism, no cases of hypotony were observed in our cohort, suggesting that the ACP-ST effectively achieves its design goal while maintaining stable postoperative intraocular pressure control.
While reducing the risk of hypotony is a key advantage of small-lumen designs in valveless GDDs, this approach introduces a distinct set of considerations, particularly the potential for early postoperative occlusion and subsequent transient IOP elevations. Devices with similarly small lumen diameters, such as the XEN 45 Gel Stent (XEN 45; Allergan PLC, Irvine, CA, United States), which has an inner lumen diameter of 45 μm, have been associated with early postoperative occlusion rates ranging from 3.9% to 8.0%, which can lead to transient IOP spikes.12–14 The substantially smaller lumen diameter of the XEN 45 compared with the ACP-ST (45 μm vs 127 μm) may contribute to these differing postoperative flow dynamics and occlusion profiles. For a more directly comparable lumen diameter, José et al reported postoperative iris synechiae around the tube in 3 of 24 PGI-implanted eyes (13%), a complication that may further contribute to impaired aqueous outflow and subsequent IOP elevation.10 In contrast, no cases of early postoperative IOP spikes or tube-related occlusion were observed in the ACP-ST cohort, suggesting that ACP-ST may provide stable early postoperative flow dynamics without the occlusion-related complications reported with other small-lumen devices; however, longer-term follow-up is required, as current observations are limited to 6 months.
Beyond device-specific considerations, a well-recognized concern associated with all GDDs, particularly with anterior chamber tube placement, is progressive corneal endothelial cell loss (CECL). Prior studies have demonstrated ECL of approximately 6–15% at 12 months and 11–18% at 24 months following GDD implantation.15 In our cohort, at the current 6-month follow-up, no significant corneal complications have been observed, and any corneal edema noted has been transient and consistent with expected postoperative findings. However, this time point remains insufficient to fully assess the impact on endothelial cell density, and longer-term follow-up is required, as the risk of progressive CECL cannot be excluded.
Limitations
This study has several limitations. First, it is a retrospective analysis and is therefore subject to inherent biases, including selection bias and incomplete data capture. As this study was designed as a retrospective case series, no a priori sample size calculation or formal power analysis was performed, and the findings should be interpreted as exploratory rather than confirmatory. Additionally, the study was conducted at a single center, and all procedures were performed by a single surgeon, which may limit the generalizability of the findings to broader patient populations and surgical settings. It should also be recognized that, as a manufacturer-funded retrospective device study, there remains potential for bias despite adherence to standardized data collection and outcome assessment methods.
Another important limitation is the relatively small cohort size and incomplete availability of 6-month follow-up data. Of the original 17 eyes included in the study, only 14 had evaluable 6-month follow-up. Two eyes had not yet reached the 6-month postoperative time point at the time of analysis, and one eye underwent ACP-ST explantation prior to 6 months. Consequently, the reported 6-month outcomes and surgical success rates were calculated based on the 14 eyes with available follow-up data and should be interpreted within this context.
Finally, the duration of follow-up remains relatively short, with primary outcomes assessed at 6 months. Although the early results are encouraging, longer-term follow-up is necessary to more fully evaluate the safety, efficacy, and durability of ACP-ST. In particular, complications such as progressive corneal endothelial cell loss and late tube-related occlusion may not be fully captured within the current follow-up period. Patients are currently undergoing continued follow-up, and additional data collection will be important for assessing long-term IOP control, medication burden, and overall surgical success.
Conclusion
In this retrospective cohort, ACP-ST demonstrated favorable early safety and efficacy outcomes, with significant reductions in IOP and medication burden through 6 months of follow-up, alongside a high rate of surgical success. No device-related complications, including hypotony or postoperative IOP spikes, were observed, suggesting that ACP-ST may provide early postoperative flow dynamics while achieving its intended design goal of mitigating hypotony risk. Taken together, these findings support the potential of ACP-ST as an effective small-lumen valveless glaucoma drainage device in the initial postoperative setting.
However, longer-term follow-up and prospective comparative studies are necessary to more fully define the safety and efficacy profile of ACP-ST. Future investigation should include continued follow-up of the current cohort through at least 12 and 24 months to assess the durability of IOP reduction, medication burden, surgical success, bleb function, and the potential development of CECL. In addition, prospective, multicenter comparative studies evaluating ACP-ST against established non-valved GDDs, such as ACP and the Baerveldt implant, are warranted. Such studies should incorporate standardized success criteria and longitudinal endothelial cell density monitoring to better characterize the relative efficacy and safety profile of ACP-ST and to guide device selection across different clinical scenarios.
Consent for Publication
No personal identifying information is contained within this review article. All images have been de-identified.
Acknowledgment
This study received an unrestricted grant from New World Medical. The sponsor had no role in the study design, data collection, analysis, interpretation, or manuscript preparation. The authors declare no conflict of interest.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dietze J, Blair K, Zeppieri M, Havens SJ. Glaucoma. In: StatPearls. StatPearls Publishing; 2024.
2. Asrani SG, McGlumphy EJ, Al-Aswad LA, et al. The relationship between intraocular pressure and glaucoma: an evolving concept. Prog Retin Eye Res. 2024;103:101303. doi:10.1016/j.preteyeres.2024.101303
3. Boopathiraj N, Wagner IV, Lentz PC, et al. 36-Month outcomes of Ahmed ClearPath(®) glaucoma drainage device in severe primary open angle glaucoma. Clin Ophthalmol. 2024;18:1735–10. doi:10.2147/opth.S467894
4. Grover DS, Kahook MY, Seibold LK, et al. Clinical outcomes of Ahmed clearpath implantation in glaucomatous eyes: a novel valveless glaucoma drainage device. J Glaucoma. 2022;31(5):335–339. doi:10.1097/ijg.0000000000002013
5. Molteno AC. New implant for drainage in glaucoma. Clinical trial. Br J Ophthalmol. 1969;53(9):606–615. doi:10.1136/bjo.53.9.606
6. Harp MD. New world medical launches non-valved glaucoma drainage device, Ahmed ClearPath ST. Ophthalmology Times. 2025. Available from: https://www.ophthalmologytimes.com/view/new-world-medical-launches-non-valved-glaucoma-drainage-device-ahmed-clearpath-st.
7. ICD-10-CM quick reference guide for glaucoma. American Academy of Ophthalmology. 2015.
8. Agrawal P, Bhardwaj P. Glaucoma drainage implants. Int J Ophthalmol. 2020;13(8):1318–1328. doi:10.18240/ijo.2020.08.20
9. Budenz DL, Barton K, Gedde SJ, et al. Five-year treatment outcomes in the Ahmed Baerveldt comparison study. Ophthalmology. 2015;122(2):308–316. doi:10.1016/j.ophtha.2014.08.043
10. José P, Barão RC, Teixeira FJ, et al. One-Year efficacy and safety of the PAUL glaucoma implant using a standardized surgical protocol. J Glaucoma. 2022;31(3):201–205. doi:10.1097/ijg.0000000000001969
11. Gupta S, Jeria S. A review on glaucoma drainage devices and its complications. Cureus. 2022;14(9):e29072. doi:10.7759/cureus.29072
12. Gan L, Wang L, Chen J, Tang L. Complications of XEN gel stent implantation for the treatment of glaucoma: a systematic review. Review. Front Med. 2024;11.doi:10.3389/fmed.2024.1360051.
13. Busch T, Skiljic D, Rudolph T, Bergström A, Zetterberg M. Four-Year outcome of XEN 45 gel stent implantation in a swedish population. Clin Ophthalmol. 2023;17:1897–1910. doi:10.2147/opth.S412400
14. Pinto Ferreira N, Abegão Pinto L, Marques-Neves C. XEN gel stent internal ostium occlusion: ab-Interno revision. J Glaucoma. 2017;26(4):e150–e152. doi:10.1097/ijg.0000000000000625
15. Oatts JT, Han Y. Glaucoma drainage device implantation, outcomes, and complications. Int Ophthalmol Clin. 2023;63(4):93–101. doi:10.1097/iio.0000000000000499
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Patient Tolerability of Omidenepag Isopropyl in the Treatment of Glaucoma and Ocular Hypertension
Matsuo M, Matsuoka Y, Tanito M
Clinical Ophthalmology 2022, 16:1261-1279
Published Date: 26 April 2022
Retrospective Analysis of Switching Bimatoprost 0.01% to Bimatoprost 0.03% in Patients with Various Types of Glaucoma and Ocular Hypertension
Xu KM, Cho R, Chan TYB
Clinical Ophthalmology 2022, 16:2385-2390
Published Date: 29 July 2022
Multicenter Effectiveness and Disease Stability Through 3 Years After iStentTrabecular Micro-Bypass with Phacoemulsification in Glaucoma and Ocular Hypertension
Clement C, Howes F, Ioannidis A, Shiu M, Manning D, Lusthaus JA, Skalicky SE, Goodwin TW
Clinical Ophthalmology 2022, 16:2955-2968
Published Date: 1 September 2022
Triple Fixed-Combination Bimatoprost/Brimonidine/Timolol in Glaucoma and Ocular Hypertension in India: A Multicenter, Open-Label, Phase 3 Study
Menon MG, Goodkin ML
Clinical Ophthalmology 2022, 16:3559-3569
Published Date: 20 October 2022
Ahmed Glaucoma Valve Implantation to Reduce Intraocular Pressure: Updated Perspectives
Arikan G, Gunenc U
Clinical Ophthalmology 2023, 17:1833-1845
Published Date: 29 June 2023