Back to Journals » Clinical Ophthalmology » Volume 17
Ahmed Glaucoma Valve Implantation to Reduce Intraocular Pressure: Updated Perspectives
Received 12 September 2022
Accepted for publication 24 May 2023
Published 29 June 2023 Volume 2023:17 Pages 1833—1845
DOI https://doi.org/10.2147/OPTH.S342721
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Gul Arikan, Uzeyir Gunenc
Dokuz Eylul University School of Medicine, Department of Ophthalmology, Izmir, Turkey
Correspondence: Gul Arikan, Dokuz Eylül University, School of Medicine, Department of Ophthalmology, Izmir, 35340, Turkey, Tel +90 531 7919687, Email [email protected]
Abstract: Trabeculectomy and glaucoma drainage device implantation are the most commonly performed glaucoma surgeries worldwide. Although trabeculectomy is the gold standard, at the present time there is an increase in the use of glaucoma drainage devices. The Ahmed glaucoma valve is one of the most widely used glaucoma drainage devices worldwide. Corneal endothelial cell loss and eventually corneal decompensation is one of the serious complication of glaucoma drainage device implantation. To avoid this, drainage tube can be inserted into the ciliary sulcus instead of the anterior chamber, especially in eyes with high risk for corneal decompensation. Tube/plate exposure, hypertensive phase, endophthalmitis, cataract formation, diplopia and ocular hypotony are the other potential complications that can develop after Ahmed glaucoma valve implantation.
Keywords: Ahmed glaucoma valve, glaucoma, glaucoma drainage device, tube shunt surgery
Introduction
Glaucoma is the leading cause of irreversible blindness worldwide and the main treatment modality for glaucoma is the reduction of intraocular pressure (IOP).1,2 If IOP remains medically uncontrolled, glaucoma filtration surgeries are indicated. Currently, trabeculectomy and glaucoma drainage device (GDD) implantation remain the mainstay of glaucoma surgical procedures. Although trabeculectomy remains the “gold standard” for glaucoma surgery, it has high rates of potential serious complications in the early postoperative period such as hypotony, choroidal effusion, shallow anterior chamber and hyphema, and long-term complications usually associated with bleb, such as bleb leakage, blebitis and endophthalmitis. Since the introduction of the Molteno implant in 1969, GDDs have been used widely in the management of complicated and refractory glaucomas.3,4 GDDs consist of a long silicone tube which provides a channel for outflow of aqueous from the anterior chamber to an endplate which was placed in the sub-Tenon's space in the equatorial area. A number of GDDs are commercially available. They differ in size, shape and material composition of the endplate. Valved implants have a flow restrictor to limit flow through the device. GDDs are usually preferred as a second line of management after a failed trabeculectomy or as a primary procedure in clinical situations considered high risk for trabeculectomy failure such as previous vitreoretinal surgery, previous penetrating keratoplasty, uveitic glaucoma or neovascular glaucoma, etc.
As stated before, trabeculectomy and tube shunt surgery are the most effective and mostly used glaucoma procedures worldwide. Studies analysing glaucoma surgeries demonstrated that, in recent years, there is a significant increase in GDD implantation and a decrease in trabeculectomy surgery.5–8 GDDs have been used increasingly in the management of glaucoma as a primary surgical option, even in eyes at low risk for failure with trabeculectomy.4–8 The Tube Versus Trabeculectomy (TVT) study is a multicenter randomized clinical trial comparing the efficacy and safety of GDD (350-mm2 Baerveldt implant) and trabeculectomy with mitomycin C in eyes with prior ocular surgery (cataract extraction with intraocular lens implantation and/or failed filtering surgery). In this study, during the five years of follow-up it was found that success was higher in tube shunt surgery compared to trabeculectomy. At five years, the cumulative probability of failure was found to be 29.8% in the tube shunt group and 46.9% in the trabeculectomy group.9 The Primary Tube Versus Trabeculectomy (PTVT) study is another multicenter randomized clinical trial comparing the efficacy and safety of GDD (350-mm2 Baerveldt glaucoma implant) and trabeculectomy with mitomycin C (0.4 mg/mL for 2 minutes) in eyes without prior ocular surgery. Study results were reported after 1, 3, and 5 years of follow-up.10–12 In this study, the failure rate was found to be higher with the tube shunt surgery, however the difference was statistically significant only at one year, but not at 3 and 5 years of follow-up. Early postoperative complications occurred more commonly after trabeculectomy surgery. Frequency of serious complications producing vision loss or requiring reoperation was lower after tube shunt surgery relative to trabeculectomy at one year of follow-up.
There is a growing tendency in GDD implantation among glaucoma surgeons and in this review we discuss the surgical success rate and complications and recent surgical modifications of the Ahmed glaucoma valve implant which is one of the most commonly used GDDs worldwide.
Method of Literature Search
We searched the PubMed database using the keywords “Ahmed glaucoma valve”, “glaucoma drainage device”, “glaucoma drainage implant”, “aqueous shunt”, “Baerveldt glaucoma implant”, “Molteno implant”.
Criteria and Fundamentals of Ahmed Glaucoma Valve Implantation
Ahmed glaucoma valve (AGV, New World Medical, Rancho Cucamonga, California) is a glaucoma drainage device that has a 184 mm2 silicone plate and, as the name implicates, is equipped with a valve mechanism which reduce the incidence of early hypotony and hypotony related complications after surgery. The aqueous humor flows through the tube to a valve comprised of two silicone elastomer membranes measuring 8 mm in length and 7 mm in width which create a venturi-shaped chamber. The venturi-shaped chamber uses Bernoulli’s principle. As the inlet cross section of the chamber is wider than the outlet, a pressure ensues across the chamber. The valve is designed to open when the IOP is 8 mmHg.13 AGV received approval by the US Food and Drug Administration in glaucoma surgery in 1993.14 Since then it has been used for many glaucoma cases worldwide and became one of the most preferred GDDs at the present time. AGV and the other GDDs are usually preferred in eyes with refractory glaucoma when trabeculectomy has failed or is unlikely to succeed. Baerveldt glaucoma implant (BGI) is another GDD commercially available. AGV and BGI are the two commonly used GDDs worldwide but differ in design.
Comparison of Ahmed Glaucoma Valve and Baerveldt Glaucoma Implant
The major difference between AGV and BGI is that, BGI, unlike AGV, is a nonvalved implant. For this reason, to prevent early hypotony in eyes implanted with BGI, an internal stent (prolene suture) or external tube ligation is required to temporarily obstruct the flow in the tube lumen. BGI has a surface area that is larger (350 mm2) than AGV (184 mm2). The large surface area of BGI requires the wings of the endplate to be implanted under adjacent rectus muscles. There are randomized controlled trials comparing the efficacy and safety of AGV and BGI. The Ahmed Baerveldt Comparison (ABC) study is the first, multicenter prospective, randomized clinical trial comparing the Ahmed valve (model FP7) and Baerveldt implant (model 101–350).15–17 In the ABC study there was no obvious superiority of one implant over the other. Surgical success was similar during the 5 years of follow-up (The cumulative probability of failure was 44.7% in the AGV group and 39.4% in the BGI group, p = 0.65). Failure was usually due to high IOP end points in the AGV group, but due to safety end points in the BGI group. Among patients with 5-year follow-up, mean IOP values of Ahmed and Baerveldt groups were reduced from 29.6±10.1 mmHg and 28.3±9.3 mmHg at baseline to 14.7±4.4 mmHg and 12.7±4.5 mmHg at five years, respectively. The decrease in IOP was statistically significant in both groups (p < 0.001). The Ahmed Versus Baerveldt (AVB) study is another multicenter prospective randomized clinical trial comparing the efficacy and safety of the AGV and BGI.18–20 Mean baseline IOP values in AGV and BGI groups were reduced from 31.1±10.5 mmHg and 31.7 ±11.1 mmHg to 16.6±5.9 mmHg and 13.6±5.0 mmHg, respectively. Decrease in IOP was statistically significant in both groups (p < 0.001). At 5 years postoperatively the AGV group had a higher failure rate (53%) compared to the BGI group (40%). The main reason for failure was found to be a high IOP in both groups. Hypotony resulted in failure in 4% of patients in the BGI group, but none in the AGV group. Authors stated that both AGV and BGI were effective in lowering IOP, but in patients that need a lower target IOP level, BGI might be a good choice. Christakis et al21 determined the efficacy of AGV and BGI by utilizing pooled data from the ABC and AVB studies. They found that both devices were effective in lowering IOP, however, BGI had a lower failure rate, had a lower rate of further glaucoma surgery and had a lower IOP on fewer medications at 5 years, but had a higher risk for hypotony.
Success Rate of AGV Implantation and Risk Factors for Failure
Reported success rate of AGV implantation in studies varies widely between 9% to 98.3%.13–45 This high variation may be due to the differences in the lengths of follow-up period, glaucoma diagnosis, definition of success criteria and surgical technique between the studies. The reported success rate of AGV implantation in different studies are shown in Table 1. Coleman et al13 reported the success rate as 78% at 1 year. Topouzis et al14 reported cumulative probabilities of success at 1, 2, 3 and 4 years as 76%, 68%, 54% and 45%, respectively. When corneal complications were excluded from the definition of failure, cumulative probabilities of success at 1, 2, 3 and 4 years were reported as 87%, 82%, 76% and 76%, respectively. Yalvac et al39 evaluated results of AGV implantation in neovascular glaucoma and they reported success rates as 63.2% at 1 year, 56.1% at 2 years, 43.2% at 3 years, 37.8% at 4 years and 25.2% at 5 years. In the AVB study the cumulative probability of failure was reported as 43% at 1 year, 51% at 3 years and 53% at 5 years.18–20 In the ABC study the cumulative probability of failure was reported as 16.4% at 1 year, 31.3% at 3 years and 44.7% at 5 years.15–17 AGV underwent a modification of plate material from polypropylene in the original form to a silicone version. The silicone model is more flexible and has a lower profile than the polypropylene model and studies showed that success rate had been higher in the silicone AGV implanted eyes compared to the polypropylene AGV implanted eyes.24,25 In Ishida et al’s study24 a total of 132 eyes of 132 patients were included in the study. Sixty-six eyes were implanted with the silicone model and 66 eyes were implanted with the polypropylene model. Success rates for the silicone and polypropylene models were 94.2% and 83.2% at 12 months and 82.4% and 56.7% at 24 months, respectively when the success criteria was defined as IOP ≥6 mmHg and ≤21 mmHg. In another study, Hinkle et al25 compared the outcomes of eyes implanted with silicone versus polypropylene model AGV, retrospectively. In their study, 25 eyes received the silicone and 26 eyes received the polypropylene model AGV. At 12 months the success rate was higher in the silicone group compared to the polypropylene group (96% and 81%, respectively). However the result was not statistically significant.
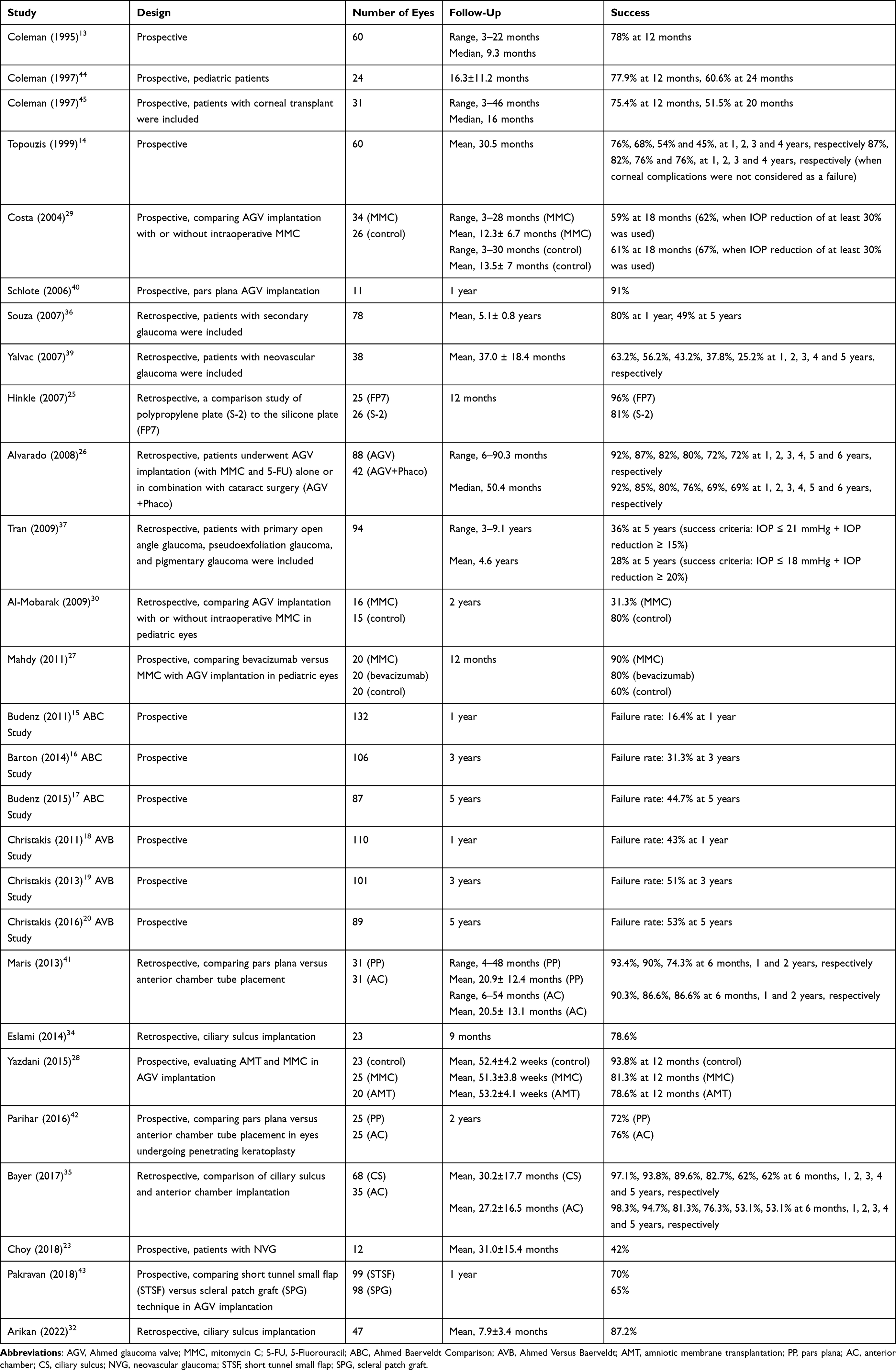 |
Table 1 The Rates of Success in Selected Studies Evaluating Ahmed Glaucoma Valve Implantation |
Bowden et al46 evaluated the risk factors associated with failure of tube shunt surgery by utilizing pooled data from ABC, AVB, and TVT studies. They found that lower preoperative IOP, neovascular glaucoma, AGV implantation, and a younger age were predictors of tube shunt failure. Tran et al37 compared the long-term surgical success of AGV implantation with trabeculectomy with mitomycin C in patients with open angle glaucoma. They found that, at 5 years, eyes with AGV have a similar success rate compared with eyes which had a trabeculectomy, when success was defined as an IOP ≤21 mmHg plus an IOP reduction of ≥15% from the baseline (36% and 48%, respectively, p = 0.094). However, when success was defined as IOP ≤18 mmHg plus an IOP reduction of ≥20% from the baseline, eyes with AGV had a statistically significantly lower success rate compared to eyes that had a trabeculectomy (28% and 44%, respectively, p = 0.024). Souza et al36 evaluated the long term outcomes of AGV implantation in 78 eyes. Success was found to be 80% after one year and 49% after 5 years in their study. They stated that prior glaucoma surgery was a significant risk factor for failure. A fibrous capsule develops around the endplate after implantation and this provides resistance to aqueous flow in the postoperative period. Failure of the tube shunts is mostly due to the excessive fibrosis around the plate. Use of antimetabolites (mitomycin C or 5-fluorouracil) may improve the outcomes of AGV implantation.26,27 Some studies showed no benefit.28–30 When there is AGV failure due to bleb encapsulation, needle revision with 5-fluorouracil can be considered.47 Surgical excision of the encapsulated bleb is also an effective procedure.48 Additional GDD insertion is another treatment option. However, the risk of corneal edema or corneal decompensation increases after sequential GDD implantation. Besides, diplopia is another concern when the two GDDs are implanted in the same eye.49,50
Complications
Hypertensive Phase
Hypertensive phase (HP) is described as an increase in IOP in the early postoperative period following GDD implantation. It is due to gradual congestion and edema of the fibrous capsule around the endplate and usually develops at 3–6 weeks after surgery and this leads to a transient increase in IOP. The hypertensive phase is usually over within 6 months and occurs more commonly in valved GDDs like AGV.31,51,52 Ozalp et al31 evaluated the risk factors for HP development retrospectively. In their study HP was observed in 31 of 60 eyes (51.7%). The resolution of HP was observed in 27 eyes (87.1%) at 3 months after the surgery. Younger age and higher mean preoperative IOP were found to be risk factors for HP development. At the last follow-up visit, eyes with HP had higher mean IOP and required more antiglaucomatous medication compared to eyes without HP. In another retrospective study, Pitukcheewanont et al51 evaluated the factors associated with HP development after GDD surgery. Seventy-two eyes of 72 patients were included in the study. Eighteen eyes had valve GDD (AGV) and 54 eyes had non-valve GDD (Molteno double-plate or BGI). Hypertensive phase developed in 38 eyes (52.8%) and occurred in about half of all types of GDD implantation. Authors found no significant difference in terms of reduction in IOP and number of medications from baseline at the 12-month follow-up visit when compared to the eyes which developed HP and eyes which did not develop HP. A risk factor of HP was pre-operative visual acuity equal or better than 20/70. Interestingly it was found that the presence of underlying heart disease was found as a protective factor for HP. Patients with heart disease were using anti-platelets and it was speculated that the anti-inflammatory effect of the antiplatelets, particularly aspirin, might be responsible for controlling inflammation and retarding fibrosis formation around the drainage device. Ocular digital massage may be useful in the management of HP after GDD implantation. Smith et al53 conducted a prospective study to evaluate the role of ocular massage during the HP after AGV implantation. In the study, 18 patients with high IOP (at 1 to 8 weeks after surgery) underwent digital ocular massage. Fifty percent of the patients achieved a 20% drop in IOP with massage and the 20% drop in IOP was maintained at the 2-week, 6-week, and 6-month review, although by 6 months, 50% of the patients required glaucoma eye drops to achieve their target IOP. In a retrospective study, Mcllraith et al54 evaluated the efficacy and safety of ocular massage in patients who developed HP after AGV implantation. Massage resulted in an immediate reduction of IOP, and, despite initial higher postoperative IOP in the massage group, there were no differences between the patients who developed HP and the patients who did not develop HP at 1 year after surgery with regard to IOP reduction or requirements for hypotensive medications. No complication observed after ocular massage. According to these studies, it seems that ocular massage is useful.
Hypotony
Although AGV is a valved device, ocular hypotony (transient or persistent) can be seen in the early postoperative period. In the literature, the rate of hypotony after AGV implantation was reported in a wide range, from 1% to 37%.13,20,22,23,28,32,36,37,39 Hypotony may be due to over-priming of the tube and valve failure, outflow of aqueous humor around the silicone tube or decrease in aqueous production due to ciliary body function failure. In hypotonic eyes hypotony maculopathy, choroidal detachment and shallow or flat anterior chamber may develop. Thus, intraoperatively, partial ligation of the silicone tube with vicryl suture can be applied to prevent early ocular hypotony.55 Hypotony risk seems to be higher in eyes implanted with BGI. In the AVB study hypotony resulted in failure in 5 patients (4%) in the Baerveldt group compared with none in the Ahmed group.20
Encapsulated Cyst Formation
Encapsulated cyst formation is a late complication of AGV implantation. It is the most important reason for GDD failure. In this situation fibrous tissue forms around the plate, restricts aqueous humor diffusion around the plate. Frequency of encapsulated cyst formation varies from 5% to 30% in different studies. Antimetabolite application can be useful to prevent this complication.56
Corneal Edema/Decompensation
Corneal endothelial cell loss and eventual corneal edema and decompensation is a well known complication of tube shunt surgery. The rate of corneal complications after tube shunt surgeries are reported to be as high as 16% to 27% in previous reports and eyes with corneal graft have higher risk.14,17,57–61 Postoperative hypotony, flat anterior chamber, tube-cornea touch and chronic inflammation are the proposed mechanisms for corneal endothelial cell loss after tube shunt surgery.14,20,57,58,62 In the AVB study, 11% of the patients in the AGV group and 12% of the patients in the BGI group developed a corneal edema as a long term complication and 7% of the patients in the AGV group and 4% of the patients in the BGI group required a corneal transplant.19 To avoid corneal complications, pars plana placement of the drainage tube has been also described.40,41,63 In this situation, complete pars plana vitrectomy is required before inserting the drainage tube. Studies reported no differences between pars plana and anterior chamber placement in terms of success rate.41,64 However, after pars plana implantation of the GDD tube, posterior segment complications including vitreous incarceration of the tube, vitreous hemorrhage and retinal detachment may develop.65 As pars plana implantation of the tube is a more complex procedure and has potential serious posterior segment complications, it should be considered in conditions where anterior chamber implantation is not feasible or is likely to create corneal decompensation. However, it should be kept in mind that after pars plana implantation the risk of corneal decompensation does not disappear completely. Interestingly different results were reported by studies comparing pars plana and anterior chamber tube shunt implantation in terms of corneal complications. In some studies corneal complications were found to be similar in both groups and in some studies it was reported that corneal complications were lower in pars plana implanted group.41,42,59,64
Another potential space for the tube shunt placement is the ciliary sulcus. To minimize corneal endothelial cell loss, especially in eyes with shallow anterior chamber depth or compromised corneal endothelium, ciliary sulcus can be considered for the tube shunt implantation. Its effectiveness and safety has been demonstrated in some previous reports.32–35,66 Ciliary sulcus tube shunt placement was first described by Rumelt and Rehany in 1998.66 They performed this surgical approach in 3 patients with corneal grafts. They used AGV in 2 eyes and a Molteno implant in one eye. Ciliary sulcus insertion of the tube was performed by the authors owing to the combination of pseudophakia or aphakia, corneal graft and moderate shallowing of the anterior chamber. Intraocular pressure levels were within normal limits (range, 8–14 mmHg) without any antiglaucomatous medication during the mean follow-up period of 18 months and corneal grafts remained unchanged. They suggested this surgical approach in pseudophakic or aphakic eyes in the presence of compromised corneal endothelium, corneal graft, shallow anterior chamber depth or extensive synechial angle closure. To date, the results of ciliary sulcus tube shunt placement was evaluated in various studies and success rates were reported as high as 78.6% to 98.3%.32–35 Eslami et al34 evaluated retrospectively the results of 23 eyes of 23 patients that underwent AGV tube implantation into the ciliary sulcus. In the study the mean follow-up period was 9 months (range 3–24 months) and IOP reduced from 37.9 ± 12.4 mmHg to 16.2 ± 3.6 mmHg at last follow-up visit and the success rate was found as 78.6%. Serious complications were endophthalmitis in one eye, tube exposure in one eye and vitreous tube occlusion in one eye. Corneal edema or decompensation was not reported. Bayer et al35 compared the efficacy and safety of anterior chamber (68 eyes) vs ciliary sulcus (35 eyes) AGV tube placement. Success rates were found to be similar between the ciliary sulcus and anterior chamber implanted groups and was found to be 85.3% (mean follow-up period was 30.2 ± 17.7 months) and 83.8% (mean follow-up period was 27.2 ± 16.5 months), respectively. During the follow-up period corneal failure was developed in one patient in the anterior chamber AGV implanted group, but in none of the patients in the ciliary sulcus implanted group. Arikan et al32 evaluated the results of patients who underwent AGV implantation with the tube placement in the ciliary sulcus retrospectively. A total of 47 eyes of 43 patients were included in the study and success was achieved in 41 eyes (87.2%) at their last follow-up visit (mean follow-up period was 7.9 ± 3.4 months). In the follow-up period corneal or corneal graft edema/decompensation did not develop in any eye. Recently, Zhang et al67 evaluated the corneal endothelial cell loss after anterior chamber vs ciliary sulcus AGV tube placement. A total of 106 eyes with anterior chamber tube inserted (mean follow-up time was 37.6 ± 20.1 months) and 105 eyes with ciliary sulcus tube inserted (mean follow-up time was 20.1 ± 17.2 months) were included in the study. Mean monthly loss in central corneal endothelial density was significantly lower in the ciliary sulcus implanted group compared to the anterior chamber implanted group (15.3 ± 20.7 cells/mm2 and 29.3 ± 29.7 cells/mm2, respectively). One year after AGV implantation mean IOP values were found to be similar in both groups. Kim et al68 evaluated the corneal endothelial cell loss in the ciliary sulcus AGV implanted and anterior chamber AGV implanted eyes and they found that the anterior chamber AGV implanted eyes had higher monthly endothelial cell density loss compared to the ciliary sulcus AGV implanted eyes (17.47 ± 11.50 cells/mm2 and 6.40 ± 7.69 cells/mm2, respectively). Success rates were found to be 83.3% and 78.9% at 12 months, and 83.3% and 76.3% at 24 months in the ciliary sulcus and anterior chamber groups, respectively. There was no statistically significant difference between the groups in terms of success rate. These studies support the efficacy and safety of the ciliary sulcus tube shunt placement and it seems that IOP reduction is similar between ciliary sulcus and anterior chamber tube shunt placement. However corneal endothelial cell loss is lower in ciliary sulcus implanted eyes. So ciliary sulcus implantation can be considered especially in eyes with a high risk of corneal decompensation. Samuel et al69 evaluated the outcomes of anterior chamber, ciliary sulcus, and pars plana glaucoma drainage device (AGV or BGI) placement retrospectively. A total of 120 eyes of 120 glaucoma patients were included in the study. The mean follow-up period was 16.4±10.1 months. The success rate for all three tube locations were similar and there was no significant difference in complication rates between the groups after 3 months. To the best of our knowledge, this is the only study in the literature evaluating the anterior chamber, ciliary sulcus and pars plana tube placement in GDD surgery. To determine the best tube position in terms of IOP decrease and corneal endothelial cell loss randomized controlled trials are required.
Tube/Plate Exposure
Conjunctival erosion over the tube/plate is a potentially serious complication after the GDD implantation. The incidence of this complication was reported between 0% and 8.3% in previous studies.14,28,70–72 Exposed implant serves as a nidus for infection and poses a risk for endophthalmitis. Younger age, inflammation (eyes with uveitic glaucoma or neovascular glaucoma), inferior device placement, performing concomitant surgery (mostly cataract surgery or pars plana vitrectomy) are the reported risk factors for erosion.70,73 To reduce the likelihood of tube exposure, the tube should be implanted under the partial-thickness scleral flap or covered with a patch graft. Tube implantation under a scleral tunnel or scleral pocket without using a patch graft were also described.43,74–77 Pericardium, duramater, sclera, cornea or fascia lata can be used as a patch graft. Patch grafts may thin or disappear after implantation. So, despite the use of a patch graft, tube exposure can still emerge. In a study, double-thickness pericardium patch grafts were found to be less likely to be associated with tube exposure than single-thickness pericardium patch grafts.78 Various methods have been described for the treatment of exposed tubes. Placement of a patch graft material (sclera, pericardium, dura, fascia lata or duramater), repositioning of the tube to the pars plana, using full-thickness corneal buttons, conjunctival-tenons pedicle flap from the fornix or oral buccal mucous membrane graft from the lower lip are the reported surgical approaches in the literature.70 Using a Tenon cyst patch graft is another option for the surgical repairing of the tube exposure.79 In this approach Tenon tissue harvested around the plate is used for the tube coverage.
Endophthalmitis
Endophthalmitis is a rare complication after AGV implantation. Al-Torbak et al80 investigated the rate and risk factors of endophthalmitis following AGV implantation. A total of 542 eyes of 505 patients were included in the study and endophthalmitis developed in 9 eyes (1.7%). The rate was 5 times higher in children and conjunctival erosion over the AGV tube was present in 6 of 9 eyes. The authors stated that young age and conjunctival erosion over the tube were significant risk factors associated with endophthalmitis. In a retrospective study Zheng et al81 also investigated the rate of infectious endophthalmitis after GDD implantation and they found that 14 of 1891 eyes (0.7%) developed endophthalmitis and most of them (9/14) had GDD erosion. Thus conjunctival erosion over the implant can be considered as a risk factor for endophthalmitis and should be repaired promptly.
Tube Migration
Tube anterior migration or retraction can be observed as an early or late complication. To avoid this complication the plate should be fixated to the sclera in a tight manner.38 Tube retraction may develop in children due to increasing globe size. Various methods have been used for the managing of tube retraction. Repositioning the whole tube/plate complex anteriorly, extension of the tube using a 22-gauge intravenous angiocatheter, silastic sleeve or commercially available AGV tube extender. “Tube-in-tube” technique and implanting a new AGV implant are the other methods described in the literature for managing tube retraction.82–84
Cataract Formation/Progression
Like trabeculectomy, tube shunt surgery can also cause cataract development and progression. In the AVB study, in 5 years, 26% of the AGV implanted eyes had visually significant cataracts and required cataract surgery.20 In patients with GDD, phacoemulsification surgery can disrupt the IOP control.85,86 Optimum timing of cataract surgery after GDD implantation is not known. Further studies are needed to identify risk factors for GDD failure after cataract surgery.
Strabismus and Diplopia
Diplopia is one of the more debilitating complications after GDD surgery. It is likely due to restrictive strabismus.20,87,88 The rates of persistent diplopia in AGV implanted eyes were reported as 5% in the AVB study and 12.7% in the ABC study.20,87 Robbins et al88 evaluated 732 patients who underwent AGV implantation retrospectively and they found that 29 patients (4%) developed new-onset strabismus postoperatively and 21 of 29 patients (72%) had diplopia. Exotropia was the most common type of strabismus in both the superotemporal and superonasal AGV implanted groups. Kilgore et al89 examined the prevalence of diplopia and strabismus in patients implanted with BGI-250, BGI-350 and AGV-FP7. Diplopia was developed in 22.9% of the AGV implanted eyes and 6.3% and 21% of the BGI-250 and BGI-350 implanted eyes, respectively. Authors concluded that patients with the larger (BGI-350) or higher profile plate (AGV-FP7) were more likely to experience diplopia than controls and diplopia was attributable to GDD in ~6% of patients with either a AGV-FP7 or a BGI-350. As diplopia can affect the quality of life, the risk of diplopia should be discussed with the patient preoperatively. In GDD implantation superotemporal quadrant is the first preferred location for the implant placement as there is more space for GDD, surgical access is easy and diplopia risk is relatively low due to the absence of the oblique muscles. If the superotemporal quadrant is not convenient for tube shunt implantation the superonasal quadrant can be considered. However, placement of the GDD in the superonasal quadrant may cause acquired Brown syndrome due to the restriction of the superior oblique muscle.90 In eyes with superior conjunctival scarring or the presence of intraocular silicone oil, AGV should be implanted in the inferior quadrants. If the implant is placed in the inferotemporal quadrant a large filtering bleb may distort the eyelid. Moreover, diplopia may develop as the inferior oblique muscle complex lies in the inferotemporal quadrant. Thus, when superior quadrants are not appropriate for GDI placement the inferonasal quadrant can be chosen.91,92
Conclusions
Glaucoma drainage devices are typically indicated in eyes with previous failure of glaucoma surgery or eyes with a high risk of failure after standard filtering surgery. In recent years there is an increasing demand for GDD usage and an Ahmed glaucoma valve implant is one of the most widely used GDDs worldwide. Due to the valve mechanism AGV seems to be safer than the other non-valved implants. However, ocular hypotony and related complications can also develop after AGV implantation. Tube/plate exposure, hypertensive phase, endophthalmitis, cataract formation and diplopia are the other complications that can be encountered after AGV implantation. Corneal decompensation is another well-known potential serious complication. To avoid this, ciliary sulcus implantation of the AGV tube can be considered in eyes with a high risk of corneal decompensation.
Abbreviations
IOP, intraocular pressure; GDD, glaucoma drainage device; AGV, Ahmed glaucoma valve; BGI, Baerveldt glaucoma implant; TVT, tube versus trabeculectomy; ABC, Ahmed Baerveldt comparison; AVB, Ahmed versus Baerveldt; HP, hypertensive phase; MMC, mitomycin-C; 5-FU, 5-Fluorouracil; AMT, amniotic membrane transplantation; PP, pars plana; AC, anterior chamber; CS, ciliary sulcus; NVG, neovascular glaucoma; STSF, short tunnel small flap; SPG, scleral patch graft.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tham Y-C, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090. doi:10.1016/j.ophtha.2014.05.013
2. Leske MC, Heijl A, Hussein M, Bengtsson B, Hyman L, Komaroff E. Factors for glaucoma progression and the effect of treatment: the early manifest glaucoma trial. Arch Ophthalmol. 2003;121(1):48–56. doi:10.1001/archopht.121.1.48
3. Molteno AC. New implant for drainage in glaucoma. Clinical trial. Br J Ophthalmol. 1969;53(9):606–615. doi:10.1136/bjo.53.9.606
4. Patel S, Pasquale LR. Glaucoma drainage devices: a review of the past, present, and future. Semin Ophthalmol. 2010;25(5–6):265–270. doi:10.3109/08820538.2010.518840
5. Vinod K, Gedde SJ, Feuer WJ, et al. Practice preferences for glaucoma surgery: a survey of the American Glaucoma Society. J Glaucoma. 2017;26(8):687–693. doi:10.1097/IJG.0000000000000720
6. Murphy C, Ogston S, Cobb C, MacEwen C. Recent trends in glaucoma surgery in Scotland, England and Wales. Br J Ophthalmol. 2015;99(3):308–312. doi:10.1136/bjophthalmol-2013-304465
7. Bron AM, Mariet AS, Benzenine E, et al. Trends in operating room-based glaucoma procedures in France from 2005 to 2014: a nationwide study. Br J Ophthalmol. 2017;101(11):1500–1504. doi:10.1136/bjophthalmol-2016-309946
8. Arora KS, Robin AL, Corcoran KJ, Corcoran SL, Ramulu PY. Use of various glaucoma surgeries and procedures in medicare beneficiaries from 1994 to 2012. Ophthalmology. 2015;122(8):1615–1624. doi:10.1016/j.ophtha.2015.04.015
9. Gedde SJ, Schiffman JC, Feuer WJ, et al. Treatment outcomes in the Tube Versus Trabeculectomy (TVT) study after five years of follow-up. Am J Ophthalmol. 2012;153:789–803. doi:10.1016/j.ajo.2011.10.026
10. Gedde SJ, Feuer WJ, Shi W, et al. Treatment outcomes in the Primary Tube Versus Trabeculectomy Study after 1 year of follow-up. Ophthalmology. 2018;125:650–663. doi:10.1016/j.ophtha.2018.02.003
11. Gedde SJ, Feuer WJ, Lim KS, et al. Treatment outcomes in the Primary Tube Versus Trabeculectomy Study after 3 years of follow-up. Ophthalmology. 2020;127:333–345. doi:10.1016/j.ophtha.2019.10.002
12. Gedde SJ, Feuer WJ, Lim KS, et al. Treatment outcomes in the Primary Tube Versus Trabeculectomy Study after 5 years of follow-up. Ophthalmology. 2022;129:1344–1356. doi:10.1016/j.ophtha.2022.07.003
13. Coleman AL, Hill R, Wilson MR, et al. Initial clinical experience with the Ahmed glaucoma valve implant. Am J Ophthalmol. 1995;120:23–31. doi:10.1016/S0002-9394(14)73755-9
14. Topouzis F, Coleman AL, Choplin N, et al. Follow-up of the original cohort with the Ahmed glaucoma valve implant. Am J Ophthalmol. 1999;128(2):198–204. doi:10.1016/S0002-9394(99)00080-X
15. Budenz DL, Barton K, Feuer WJ, et al. Treatment outcomes in the Ahmed Baerveldt Comparison Study after 1 year of follow-up. Ophthalmology. 2011;118:443–452. doi:10.1016/j.ophtha.2010.07.016
16. Barton K, Feuer WJ, Budenz DL, et al. Three-year treatment outcomes in the Ahmed Baerveldt Comparison study. Ophthalmology. 2014;121:1547–1557. doi:10.1016/j.ophtha.2014.01.036
17. Budenz DL, Barton K, Gedde SJ, et al. Five-year treatment outcomes in the Ahmed Baerveldt comparison study. Ophthalmology. 2015;122(2):308–316. doi:10.1016/j.ophtha.2014.08.043
18. Christakis PG, Kalenak JW, Zurakowski D, et al. The Ahmed versus Baerveldt study. One-year treatment outcomes. Ophthalmology. 2011;118:2180–2189. doi:10.1016/j.ophtha.2011.05.004
19. Christakis PG, Tsai JC, Kalenak JW, et al. The Ahmed versus Baerveldt study. Three-year treatment outcomes. Ophthalmology. 2013;120:2232–2240. doi:10.1016/j.ophtha.2013.04.018
20. Christakis PG, Kalenak JW, Tsai JC, et al. The Ahmed versus Baerveldt study: five-year treatment outcomes. Ophthalmology. 2016;123(10):2093–2102. doi:10.1016/j.ophtha.2016.06.035
21. Christakis PG, Zhang D, Budenz DL, et al. Five-year pooled data analysis of the Ahmed Baerveldt comparison study and the Ahmed versus Baerveldt study. Am J Ophthalmol. 2017;176:118–126. doi:10.1016/j.ajo.2017.01.003
22. Yildirim N, Yalvac IS, Sahin A, Ozer A, Bozca T. A comparative study between diode laser cyclophotocoagulation and the Ahmed glaucoma valve implant in neovascular glaucoma: a long-term follow-up. J Glaucoma. 2009;18(3):192–196. doi:10.1097/IJG.0b013e31817d235c
23. Choy BNK, Lai JSM, Yeung JCC, Chan JCH. Randomized comparative trial of diode laser cyclophotocoagulation versus Ahmed glaucoma valve for neovascular glaucoma in Chinese - a pilot study. Clin Ophthalmol. 2018;12:2542–2552. doi:10.2147/OPTH.S188999
24. Ishida K, Netland PA, Costa VP, Shiroma L, Khan B, Ahmed II. Comparison of polypropylene and silicone Ahmed Glaucoma Valves. Ophthalmology. 2006;113(8):1320–1326. doi:10.1016/j.ophtha.2006.04.020
25. Hinkle DM, Zurakowski D, Ayyala RS. A comparison of the polypropylene plate Ahmed glaucoma valve to the silicone plate Ahmed glaucoma flexible valve. Eur J Ophthalmol. 2007;17(5):696–701. doi:10.1177/112067210701700502
26. Alvarado JA, Hollander DA, Juster RP, Lee LC. Ahmed valve implantation with adjunctive mitomycin C and 5-fluorouracil: long-term outcomes. Am J Ophthalmol. 2008;146(2):276–284. doi:10.1016/j.ajo.2008.04.008
27. Mahdy RAR. Adjunctive use of bevacizumab versus mitomycin C with Ahmed valve implantation in treatment of pediatric glaucoma. J Glaucoma. 2011;20(7):458–463. doi:10.1097/IJG.0b013e3181efbea5
28. Yazdani S, Mahboobipour H, Pakravan M, Doozandeh A, Ghahari E. Adjunctive Mitomycin C or amniotic membrane transplantation for Ahmed glaucoma valve implantation: a randomized clinical trial. J Glaucoma. 2016;25(5):415–421. doi:10.1097/IJG.0000000000000256
29. Costa VP, Azuara-Blanco A, Netland PA, Lesk MR, Arcieri ES. Efficacy and safety of adjunctive mitomycin C during Ahmed glaucoma valve implantation: a prospective randomized clinical trial. Ophthalmology. 2004;111(6):1071–1076. doi:10.1016/j.ophtha.2003.09.037
30. Al-Mobarak F, Khan AO. Two-year survival of Ahmed valve implantation in the first 2 years of life with and without intraoperative mitomycin-C. Ophthalmology. 2009;116(10):1862–1865. doi:10.1016/j.ophtha.2009.03.030
31. Ozalp O, Ilguy S, Atalay E, Simsek T, Yildirim N. Risk factors for hypertensive phase after Ahmed glaucoma valve implantation. Int Ophthalmol. 2022;42(1):147–156. doi:10.1007/s10792-021-02009-3
32. Arikan G, Akbulut B, Utine CA, et al. Ahmed glaucoma valve implantation with the tube placement in the ciliary sulcus: short term results. Int Ophthalmol. 2022;42(3):969–980. doi:10.1007/s10792-021-02080-w
33. Kim NE, Kim SS, Lee JS, et al. Effect of intraoperative mitomycin C on the surgical outcomes of Ahmed glaucoma valve implantation with ciliary sulcus tube placement. Korean J Ophthalmol. 2023;37(3):216–223. doi:10.3341/kjo.2022.0146
34. Eslami Y, Mohammadi M, Fakhraie G, Zarei R, Moghimi S. Ahmed glaucoma valve implantation with tube insertion through the ciliary sulcus in pseudophakic/aphakic eyes. J Glaucoma. 2014;23(2):115–118. doi:10.1097/IJG.0b013e318265bc0b
35. Bayer A, Onol M. Clinical outcomes of Ahmed glaucoma valve in anterior chamber versus ciliary sulcus. Eye. 2017;31(4):608–614. doi:10.1038/eye.2016.273
36. Souza C, Tran DH, Loman J, Law SK, Coleman AL, Caprioli J. Long-term outcomes of Ahmed glaucoma valve implantation in refractory glaucomas. Am J Ophthalmol. 2007;144(6):893–900. doi:10.1016/j.ajo.2007.07.035
37. Tran DH, Souza C, Ang MJ, et al. Comparison of long-term surgical success of Ahmed valve implant versus trabeculectomy in open-angle glaucoma. Br J Ophthalmol. 2009;93(11):1504–1509. doi:10.1136/bjo.2008.150870
38. Kapelushnik N, Singer R, Barkana Y, et al. Surgical outcomes of Ahmed glaucoma valve implantation without plate sutures: a 10-year retrospective study. J Glaucoma. 2021;30(6):502–507. doi:10.1097/IJG.0000000000001813
39. Yalvac IS, Eksioglu U, Satana B, Duman S. Long-term results of Ahmed glaucoma valve and Molteno implant in neovascular glaucoma. Eye. 2007;21(1):65–70. doi:10.1038/sj.eye.6702125
40. Schlote T, Ziemssen F, Bartz-Schmidt KU. Pars plana-modified Ahmed glaucoma valve for treatment of refractory glaucoma: a pilot study. Graefes Arch Clin Exp Ophthalmol. 2006;244(3):336–341. doi:10.1007/s00417-005-0008-5
41. Maris PJ, Tsai JC, Khatib N, Bansal R, Al-Aswad LA. Clinical outcomes of Ahmed glaucoma valve in posterior segment versus anterior chamber. J Glaucoma. 2013;22(3):183–189. doi:10.1097/IJG.0b013e318237c115
42. Parihar JKS, Jain VK, Kaushik J, Mishra A. Pars plana-modified versus conventional Ahmed glaucoma valve in patients undergoing penetrating keratoplasty: a prospective comparative randomized study. Curr Eye Res. 2017;42(3):436–442. doi:10.1080/02713683.2016.1185130
43. Pakravan M, Hatami M, Esfandiari H, et al. Ahmed glaucoma valve implantation: graft-free short tunnel small flap versus scleral patch graft after 1-year follow-up: a randomized clinical trial. Ophthalmol Glaucoma. 2018;1(3):206–212. doi:10.1016/j.ogla.2018.10.008
44. Coleman AL, Smyth RJ, Wilson MR, Tam M. Initial clinical experience with the Ahmed Glaucoma Valve implant in pediatric patients. Arch Ophthalmol. 1997;115:186–191. doi:10.1001/archopht.1997.01100150188007
45. Coleman AL, Mondino BJ, Wilson MR, Casey R. Clinical experience with the Ahmed glaucoma valve implant in eyes with prior or concurrent penetrating keratoplasties. Am J Ophthalmol. 1997;123:54–61. doi:10.1016/S0002-9394(14)70992-4
46. Bowden EC, Choudhury A, Gedde SJ, et al. Risk factors for failure of tube shunt surgery: a pooled data analysis. Am J Ophthalmol. 2022;240:217–224. doi:10.1016/j.ajo.2022.02.027
47. Quaranta L, Floriani I, Hollander L, Poli D, Katsanos A, Konstas AGP. Needle revision with 5-fluorouracil for the treatment of Ahmed glaucoma valve filtering blebs: 5-fluorouracil needling revision can be a useful and safe tool in the management of failing Ahmed glaucoma valve filtering blebs. J Glaucoma. 2016;25(4):e367–371. doi:10.1097/IJG.0000000000000366
48. Eibschitz-Tsimhoni M, Schertzer RM, Musch DC, Moroi SE. Incidence and management of encapsulated cysts following Ahmed glaucoma valve insertion. J Glaucoma. 2005;14(4):276–279. doi:10.1097/01.ijg.0000169391.94555.c1
49. Smith M, Buys YM, Trope GE. Second Ahmed valve insertion in the same eye. J Glaucoma. 2009;18(4):336–340. doi:10.1097/IJG.0b013e318182edfb
50. Lee NY, Hwang HB, Oh SH, Park CK. Efficacy of additional glaucoma drainage device insertion in refractory glaucoma: case series with a systematic literature review and meta-analysis. Semin Ophthalmol. 2015;30(5–6):345–351. doi:10.3109/08820538.2013.874487
51. Pitukcheewanont O, Tantisevi V, Chansangpetch S, Rojanapongpun P. Factors related to hypertensive phase after glaucoma drainage device implantation. Clin Ophthalmol. 2018;12:1479–1486. doi:10.2147/OPTH.S166244
52. Hong C, Arosemena A, Zurakowski D, Ayyala RS. Glaucoma drainage devices: a systematic literature review and current controversies. Surv Ophthalmol. 2005;50(1):48–60. doi:10.1016/j.survophthal.2004.10.006
53. Smith M, Geffen N, Alasbali T, Buys YM, Trope GE. Digital ocular massage for hypertensive phase after Ahmed valve surgery. J Glaucoma. 2010;19:11–14. doi:10.1097/IJG.0b013e31819c485b
54. Mcllraith I, Buys Y, Campbell RJ, Trope GE. Ocular massage for intraocular pressure control after Ahmed valve insertion. Can J Ophthalmol. 2008;43:48–52. doi:10.3129/i07-188
55. Kee C. Prevention of early postoperative hypotony by partial ligation of silicone tube in Ahmed glaucoma valve implantation. J Glaucoma. 2001;10(6):466–469. doi:10.1097/00061198-200112000-00005
56. Bikbov MM, Khusnitdinov II. The results of the use of Ahmed valve in refractory glaucoma surgery. J Curr Glaucoma Pract. 2015;9(3):86–91. doi:10.5005/jp-journals-10008-1191
57. Koo EB, Hou J, Keenan JD, Stamper RL, Jeng BH, Han Y. Effects of glaucoma tube surgery on corneal endothelial cells: a review. Eye Contact Lens. 2016;42(4):221–224. doi:10.1097/ICL.0000000000000171
58. Lee EK, Yun YJ, Lee JE, et al. Changes in corneal endothelial cells after Ahmed glaucoma valve implantation: 2-year follow-up. Am J Ophthalmol. 2009;148:361–367. doi:10.1016/j.ajo.2009.04.016
59. Arroyave CP, Scott IU, Fantes FE, Feuer WJ, Murray TG. Corneal graft survival and intraocular pressure control after penetrating keratoplasty and glaucoma drainage device implantation. Ophthalmology. 2001;108(11):1978–1985. doi:10.1016/S0161-6420(01)00803-X
60. Gedde SJ, Herndon LW, Brandt JD, et al. Postoperative complications in the tube versus trabeculectomy (TVT) study during five years of follow-up. Am J Ophthalmol. 2012;153(5):804–814. doi:10.1016/j.ajo.2011.10.024
61. Mills RP, Reynolds A, Emond MJ, Barlow WE, Leen MM. Long-term survival of Molteno glaucoma drainage devices. Ophthalmology. 1996;103(2):299–305. doi:10.1016/S0161-6420(96)30700-8
62. Chen J, Gedde SJ. New developments in tube shunt surgery. Curr Opin Ophthalmol. 2019;30(2):125–131. doi:10.1097/ICU.0000000000000549
63. Kaynak S, Tekin NF, Durak I, Berk AT, Saatci AO, Soylev MF. Pars plana vitrectomy with pars plana tube implantation in eyes with intractable glaucoma. Br J Ophthalmol. 1998;82(12):1377–1382. doi:10.1136/bjo.82.12.1377
64. Wang B, Li W. Comparison of pars plana with anterior chamber glaucoma drainage device implantation for glaucoma: a meta-analysis. BMC Ophthalmol. 2018;18(1):212. doi:10.1186/s12886-018-0896-x
65. Kumar H, Thulasidas M. Pars plana implantation of glaucoma drainage devices- the way to succeed in refractory glaucoma. Indian J Ophthalmol. 2021;69(7):1650–1651. doi:10.4103/ijo.IJO_688_21
66. Rumelt S, Rehany U. Implantation of glaucoma drainage implant tube into the ciliary sulcus in patients with corneal transplants. Arch Ophthalmol. 1998;116(5):685–687. doi:10.1001/archopht.116.5.685
67. Zhang Q, Liu Y, Thanapaisal S, et al. The effect of tube location on corneal endothelial cells in patients with Ahmed glaucoma valve. Ophthalmology. 2021;128(2):218–226. doi:10.1016/j.ophtha.2020.06.050
68. Kim JY, Lee JS, Lee T, et al. Corneal endothelial cell changes and surgical results after Ahmed glaucoma valve implantation: ciliary sulcus versus anterior chamber tube placement. Sci Rep. 2021;11(1):12986. doi:10.1038/s41598-021-92420-8
69. Samuel S, Chang EK, Gupta S, et al. Outcomes of anterior chamber, sulcus, and pars plana glaucoma drainage device placement in glaucoma patients. J Ophthalmol. 2022;2022:5947992. doi:10.1155/2022/5947992
70. Bains U, Hoguet A. Aqueous drainage device erosion: a review of rates, risks, prevention, and repair. Semin Ophthalmol. 2018;33(1):1–10. doi:10.1080/08820538.2017.1353805
71. Stewart WC, Kristoffersen CJ, Demos CM, Fsadni MG, Stewart JA. Incidence of conjunctival exposure following drainage device implantation in patients with glaucoma. Eur J Ophthalmol. 2010;20(1):124–130. doi:10.1177/112067211002000117
72. Trubnik V, Zangalli C, Moster MR, et al. Evaluation of risk factors for glaucoma drainage device-related erosions: a retrospective case-control study. J Glaucoma. 2015;24:498–502. doi:10.1097/IJG.0000000000000034
73. Chaku M, Netland PA, Ishida K, Rhee DJ. Risk factors for tube exposure as a late complication of glaucoma drainage implant surgery. Clin Ophthalmol. 2016;10:547–553. doi:10.2147/OPTH.S104029
74. Ozdamar A, Aras C, Ustundag C, Tamcelik N, Ozkan S. Scleral tunnel for the implantation of glaucoma Seton devices. Ophthalmic Surg Lasers. 2001;32(5):432–435. doi:10.3928/1542-8877-20010901-14
75. Ollila M, Falck A, Airaksinen J. Placing the Molteno implant in a long scleral tunnel to prevent postoperative tube exposure. Acta Ophthalmol Scand. 2005;83:302–305. doi:10.1111/j.1600-0420.2005.00450.x
76. Mesa-Gutiérrez JC, Lillo-Sopena J, Monés-Llivina A, Sanz-Moreno S, Arruga-Ginebreda J. Graft-free Ahmed tube insertion: a modified method at 5 mm from limbus. Clin Ophthalmol. 2010;4:359–363. doi:10.2147/OPTH.S9461
77. Maki H, Mori S, Imai H, et al. Autologous scleral pocket technique for Ahmed glaucoma valve implantation with pars plana tube insertion for neovascular glaucoma. J Clin Med. 2021;10(8):1606. doi:10.3390/jcm10081606
78. Lankaranian D, Reis R, Henderer JD, Choe S, Moster MR. Comparison of single thickness and double thickness processed pericardium patch graft in glaucoma drainage device surgery: a single surgeon comparison of outcome. J Glaucoma. 2008;17(1):48–51. doi:10.1097/IJG.0b013e318133fc49
79. Alvarez-Ascencio D, Lazcano-Gomez G, Flores-Reyes E, Duenas-Angeles K, Jimenez-Roman J, Kahook MY. Tenon cyst patch graft for Ahmed glaucoma valve tube exposure: case series report. J Glaucoma. 2021;30(8):e367–e371. doi:10.1097/IJG.0000000000001776
80. Al-Torbak AA, Al-Shahwan S, Al-Jadaan I, Al-Hommadi A, Edward DP. Endophthalmitis associated with the Ahmed glaucoma valve implant. Br J Ophthalmol. 2005;89(4):454–458. doi:10.1136/bjo.2004.049015
81. Zheng CX, Moster MR, Khan MA, et al. Infectious endophthalmitis after glaucoma drainage implant surgery. Clinical features, microbial spectrum, and outcomes. Retina. 2017;37(6):1160–1167. doi:10.1097/IAE.0000000000001329
82. Chiang MY, Camuglia JE, Khaw PT. A novel method of extending glaucoma drainage tube: ‘Tube-in-Tube’ technique. J Glaucoma. 2017;26(2):93–95. doi:10.1097/IJG.0000000000000567
83. Kooner KS. Repair of Molteno implant during surgery. Am J Ophthalmol. 1994;117(5):673. doi:10.1016/S0002-9394(14)70080-7
84. Sarkisian SR, Netland PA. Tube extender for revision of glaucoma drainage implants. J Glaucoma. 2007;16(7):637–639. doi:10.1097/IJG.0b013e3180640f6c
85. Sa HS, Kee C. Effect of temporal clear corneal phacoemulsification on intraocular pressure in eyes with prior Ahmed glaucoma valve insertion. J Cataract Ref Surg. 2006;32(6):1011–1014. doi:10.1016/j.jcrs.2006.02.031
86. Gujral S, Nouri-Mahdavi K, Caprioli J. Outcomes of small-incision cataract surgery in eyes with preexisting Ahmed glaucoma valves. Am J Ophthalmol. 2005;140(5):911–913. doi:10.1016/j.ajo.2005.04.049
87. Budenz DL, Feuer WJ, Barton K, et al. Postoperative complications in the Ahmed Baerveldt comparison study during five years of follow-up. Am J Ophthalmol. 2016;163:75–82. doi:10.1016/j.ajo.2015.11.023
88. Robbins L, Goseki T, Law SK, et al. Strabismus after Ahmed glaucoma valve implantation. Am J Ophthalmol. 2021;222:1–5. doi:10.1016/j.ajo.2020.08.019
89. Kilgore KP, Wang F, Stern NC, et al. Rates of diplopia in Ahmed FP7, Baerveldt 250, and 350. Glaucoma patients compared with medical controls. J Glaucoma. 2021;30:579–584. doi:10.1097/IJG.0000000000001886
90. Ventura MP, Vianna RNG, Filho JPS, Solari HP, Curi RLN. Acquired Brown’s syndrome secondary to Ahmed valve implant for neovascular glaucoma. Eye. 2005;19(2):230–232. doi:10.1038/sj.eye.6701439
91. Harbick KH, Sidoti PA, Budenz DL, et al. Outcomes of inferonasal Baerveldt glaucoma drainage implant surgery. J Glaucoma. 2006;15(1):7–12. doi:10.1097/01.ijg.0000195597.30600.27
92. Aref AA, Gedde SJ, Budenz DL. Glaucoma drainage implant surgery. Dev Ophthalmol. 2012;50:37–47. doi: 10.1159/000334777
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of Short and Long-Tunnel Needle Track for Ahmed Glaucoma Valve Implantation in a Private Eye Center in the Philippines: A Retrospective Study
San Pedro MJB, Gomez JPS, Leuenberger EU
Clinical Ophthalmology 2023, 17:1691-1699
Published Date: 21 June 2023
Functionality and Priming Stream Patterns of the Ahmed Glaucoma Valve in a Laboratory Setting
Amiri IM, Gebreyesus HW, Patnaik JL, Kahook MY, Seibold LK
Clinical Ophthalmology 2025, 19:1411-1416
Published Date: 28 April 2025
Novel Non-Valved Glaucoma Drainage Device with Reduced Inner Lumen Diameter: 6-Month Safety and Efficacy Outcomes
Shi KSY, Vasu P, Oyama K, Thé RY, Wang M, Banoub RG, Ang BCH, Dorairaj SK
Clinical Ophthalmology 2026, 20:615265
Published Date: 23 June 2026
A Comparison of the Efficacy and Safety of Modified Baerveldt Drainage Implants versus Ahmed Glaucoma Valves After 1 Year of Follow-Up
Davis KL, Christensen QH, VandeLune JA, Pellack DR, Donegan PJ, Meyer MD, Singh RS, Al-Kaylani HM, Boese EA, Pouw AE
Clinical Ophthalmology 2026, 20:588163
Published Date: 8 July 2026