Back to Journals » Journal of Inflammation Research » Volume 18
Novel Inflammatory Markers and Their Association with the Severity of Hypertriglyceridemia-Associated Acute Pancreatitis
Authors Zhong L ![]() , Ding J, Chen M, Cai X, Chen L, Du X, Rao Y, Zhang D
, Ding J, Chen M, Cai X, Chen L, Du X, Rao Y, Zhang D ![]()
Received 25 June 2025
Accepted for publication 14 October 2025
Published 24 October 2025 Volume 2025:18 Pages 14771—14790
DOI https://doi.org/10.2147/JIR.S549115
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Adam Bachstetter
Lin Zhong,1,2 Jiezhu Ding,3 Manqin Chen,2 Xiaoyu Cai,2 Ling Chen,2 Xianrong Du,2 Yinhua Rao,2 Dingguo Zhang4
1Department of Gastroenterology, Shantou University Medical College, Shantou, Guangdong, People’s Republic of China; 2Department of Gastroenterology, Shenzhen People’s Hospital (The First Affiliated Hospital, Southern University of Science and Technology; The Second Clinical Medical College, Jinan University), Shenzhen, Guangdong, People’s Republic of China; 3Department of Pulmonary and Critical Care Medicine, Shenzhen Hospital, Peking University, Shenzhen, Guangdong, People’s Republic of China; 4Department of Surgical Endoscopy Center, Shenzhen People’s Hospital (The First Affiliated Hospital, Southern University of Science and Technology; The Second Clinical Medical College, Jinan University), Shenzhen, Guangdong, People’s Republic of China
Correspondence: Dingguo Zhang, Email [email protected]
Objective: To investigate associations between novel inflammatory biomarkers and disease severity in Hypertriglyceridemia-associated acute pancreatitis (HTG-AP) and to evaluate their prognostic utility for risk stratification.
Methods: This retrospective cohort study included 340 HTG-AP patients. Neutrophil-to-high-density lipoprotein Cholesterol Ratio (NHR), Monocyte-to-High-Density Lipoprotein Cholesterol Ratio (MHR), Lymphocyte-to-HDL cholesterol ratio (LHR), Platelet-to-high-density lipoprotein cholesterol ratio (PHR), Systemic Immune-Inflammation Index (SII), Systemic Inflammatory Response Index (SIRI), and aggregate index of systemic inflammation (AISI) indices were calculated. Multivariable logistic regression (unadjusted/age-sex-adjusted/fully-adjusted models) was conducted, and ROC analysis was performed to determine the predictive performance for MSAP+SAP/SAP.
Results: Among 340 HTG-AP patients (156 MAP, 130 MSAP, 54 SAP), novel inflammatory markers NHR, SII, SIRI, MHR, PHR, and AISI significantly increased with severity (P < 0.01). Restricted cubic splines revealed nonlinear associations of NHR, SII, AISI, MHR, and SIRI with MSAP+SAP risk (Overall P < 0.05; Nonlinear P < 0.05). In fully adjusted models: For each 1-unit increase in NHR, the OR was 1.06 (95% CI: 1.03– 1.09; P < 0.001). Comparing the highest tertile (Q3) to the lowest (Q1), the OR was 6.03 (95% CI: 2.98– 12.19; P < 0.001). MHR Q3 vs Q1: OR=4.52 (2.26– 9.03; P < 0.001). SIRI Q3 vs Q1: OR = 3.12 (1.61– 6.06; P < 0.001). SII Q3 vs Q1: OR 3.12–(1.61– 6.04; P < 0.001). AISI Q3 vs Q1: OR = 2.74 (95% CI: 1.42– 5.28; P = 0.003). LHR and PHR showed no statistically significant associations (P > 0.05). ROC analysis demonstrated that NHR was the best predictor of MSAP+SAP (AUC = 0.701; optimal cutoff = 14.484), outperforming other indices (SII: AUC = 0.666; LHR: AUC = 0.505).
Conclusion: NHR is a novel independent predictor of moderate-severe or severe HTG-AP, with the highest tertile conferring a 6.03-fold increased risk (95% CI: 2.98– 12.19; P < 0.001) and an AUC of 0.701 for MSAP+SAP prediction. SII, MHR, SIRI, and AISI provide complementary prognostic value, supporting early risk stratification using NHR (cutoff = 14.484).
Keywords: hypertriglyceridemia-associated acute pancreatitis, novel inflammatory markers, NHR, disease severity, severity prediction
Introduction
Acute pancreatitis (AP), a common acute condition in the digestive system, has an annual global incidence rate of approximately 34 per 100,000 people.1 With the increasing prevalence of metabolic diseases, hypertriglyceridemia (HTG) has surpassed alcohol to become the second leading cause of acute pancreatitis (AP) in China, accounting for 21% of the total incidence of AP.2,3 Multiple studies that have been conducted indicate that patients with Hypertriglyceridemia-associated acute pancreatitis (HTG-AP) have a higher risk of developing complications and organ failure compared to those with non-triglyceride-related acute pancreatitis (NTG-AP), are more likely to progress to acute severe pancreatitis (SAP), have more extended hospital stays, and have a higher mortality rate.4–6 Early, accurate assessment of the condition is vital for formulating a reasonable treatment plan and improving the prognosis of patients.
Since there is currently no specific scoring system for evaluating HTG-AP, the commonly used tools for predicting the severity of acute pancreatitis include Ranson criteria, Acute Physiology and Chronic Health Evaluation System (APACHE-II), Bedside Acute Pancreatitis Severity Index (BISAP), modified Marshall score (mMarshall), and modified CT severity index (mCTSI), etc. Multiple studies have questioned the clinical value of traditional scoring systems in predicting severe pancreatitis early, indicating that none apply to all forms of pancreatitis. The clinical value of the four commonly used scoring systems (BISAP, APACHE-II, Ranson, and SIRS) in predicting severe acute pancreatitis (SAP) has been established. It is pointed out that although traditional scoring systems such as BISAP, APACHE-II, and Ranson are widely used, their predictive efficacy is limited, with positive predictive values (PPV) ranging from 40% to 50% and negative predictive values (NPV) being relatively high (88% to 95%).7 It indicates that the traditional scoring system performs well in excluding severe pancreatitis (with a high negative predictive value, NPV) but has a mediocre performance in predicting severe pancreatitis (with a low positive predictive value, PPV). Additionally, scoring systems typically require the dynamic collection of numerous complex laboratory data and clinical parameters, which is not convenient for implementation in primary hospitals. However, single laboratory parameters (such as neutrophils (NEU), lymphocytes (LYM), and monocytes (MON), among others) are prone to being affected by dehydration or fluid resuscitation, blood specimen dilution, and blood specimen processing, and thus exhibit poor stability.8 Therefore, finding more efficient and convenient new biological markers for predicting the condition and risk stratification is a clinical need.
In recent years, numerous studies have explored the significance of novel inflammatory composite indicators (such as the neutrophil-to-high-density lipoprotein cholesterol ratio (NHR), monocyte-to-high-density lipoprotein cholesterol ratio (MHR), platelet-to-high-density lipoprotein ratio (PHR), systemic immune inflammation index (SII), and systemic inflammatory response index (AISI)) in predicting the risk and prognosis of metabolic diseases, cardiovascular diseases, neurological disorders, and infectious diseases. They have demonstrated their considerable value in this regard.9–13 These inflammatory complexes reflect inflammatory responses and metabolic manifestations, performing exceptionally well in complex disease mechanisms. Moreover, compared with scoring systems with numerous complex parameters, they are more convenient and have higher clinical practicability.
Based on these advantages, we conducted this study to explore the relationship between novel composite inflammatory markers and the severity of the disease in patients with HTG-AP. Our study is the first systematic study in this clinical context to evaluate the feasibility of multiple inflammatory complexes as potential prognostic indicators.
Materials and Methods
Study Design
This study was a single-center retrospective cohort study. Data from patients diagnosed with Hypertriglyceridemia-associated acute pancreatitis (HTG-AP) at Shenzhen People’s Hospital from January 2015 to April 2025. The data mainly came from the hospital’s electronic medical record system. This study was approved by the Medical Ethics Committee of Shenzhen People’s Hospital (Ethical Approval Number: LL-KY-202411901).The study was conducted in accordance with the Declaration of Helsinki.
Clinical Definitions
AP Diagnostic Criteria
The diagnosis of AP required the presence of at least two of the following three features, as per the Revised Atlanta Classification: (1) characteristic abdominal pain (acute onset of persistent, severe epigastric pain often radiating to the back); (2) serum amylase and/or lipase activity ≥3 times the upper limit of normal; (3) characteristic imaging findings of AP on contrast-enhanced computed tomography (CECT), magnetic resonance imaging (MRI), or transabdominal ultrasonography.14
HTG-AP Diagnostic Criteria
Given the absence of a universally defined minimum triglyceride threshold for hypertriglyceridemia (HTG)- associated acute pancreatitis (AP), this study adopts diagnostic criteria aligned with current guidelines and prior research. Specifically, HTG-AP is defined as meeting the diagnostic requirements for acute pancreatitis, plus either of the following: a triglyceride (TG) level ≥1,000 mg/dL (11.30 mmol/L) or a TG level of 500–1,000 mg/dL (5.65–11.30 mmol/L) with milky serum (chylomicronemia).15–17
Severity Grading
According to the revised Atlanta classification (RAC),14 the severity of AP is categorized into Mild AP (No organ failure and no local complications), Moderately severe AP (Transient organ failure (≤ 48 hours) or local complications), and severe AP: Persistent organ failure (> 48 hours).
Systemic Inflammatory Response Syndrome (SIRS)
SIRS is a systemic inflammatory reaction triggered by infectious or non-infectious insults. The diagnostic criteria require the presence of at least two of the following clinical manifestations: (1) Body temperature >38°C or <36°C; (2) Heart rate >90 beats per minute; (3) Respiratory rate >20 breaths per minute or PaCO2 <32 mmHg; (4) White blood cell count >12×109/L or <4×109/L, or immature neutrophils >10%.18
Acute Peripancreatic Fluid Collection (APFC)
Acute Peripancreatic Fluid Collection (APFC) is defined as peripancreatic fluid accumulation occurring within 4 weeks of onset in patients with interstitial edematous pancreatitis, lacking features of a pseudocyst (eg, well-defined wall or internal septations).14
Study Population
During the study period from January 2015 to April 2025, a total of 1996 patients with acute pancreatitis were admitted. To ensure a homogeneous study population and to specifically investigate the role of inflammatory markers in HTG-AP—a distinct entity with a unique pathophysiology—we exclusively enrolled patients meeting the HTG-AP criteria detailed above, thereby excluding those with other etiologies such as biliary, alcoholic, or idiopathic AP. All HTG-AP patients hospitalized during the study were assessed for eligibility. After applying the inclusion and exclusion criteria, a total of 340 patients were enrolled and classified according to the RAC criteria into mild acute pancreatitis (MAP), moderate-to-severe acute pancreatitis (MSAP), and severe acute pancreatitis (SAP).
Inclusion Criteria
(1) Diagnosed according to HTG-AP criteria (serum triglycerides ≥ 11.3 mmol/L or with chylous blood and excluding other causes); (2) Time from onset to admission ≤ 48 hours; (3) Age ≥ 18 years.
Exclusion Criteria
(1) History of chronic pancreatitis; (2) Age < 18 years; (3) Time from symptom onset to admission > 48 hours; (4) Pregnant or lactating women; (5) Complicated with chronic liver disease (Child-Pugh B/C grade) or chronic kidney disease (eGFR < 60 mL/min/1.73m²); (6) Autoimmune diseases (such as systemic lupus erythematosus), malignant tumors or hematological diseases; (7) Missing clinical data > 20%. Figure 1 describes the case screening process.
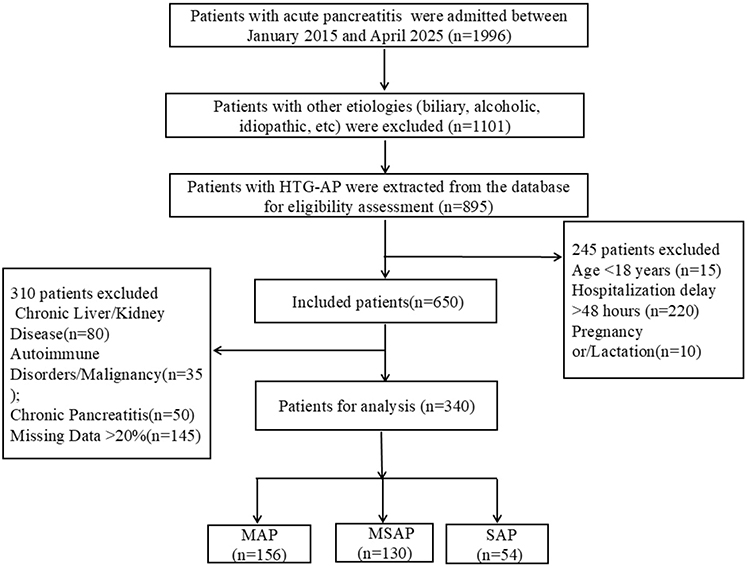 |
Figure 1 Flowchart of patient screening and enrollment. Abbreviations: MAP, mild acute pancreatitis; MSAP, moderate-to-severe acute pancreatitis; SAP, severe acute pancreatitis. |
Data Collection
Comprehensive clinical data were systematically collected from all enrolled patients. Demographic and clinical characteristics included age, sex, smoking history, alcohol consumption history, and preexisting comorbidities (hypertension, diabetes mellitus, fatty liver disease). Laboratory parameters assessed within 48 hours of symptom onset comprised neutrophil count (Neu), absolute monocyte count (Mon), absolute lymphocyte count (Lym), absolute platelet count (PLT), serum triglyceride (TG), serum albumin (ALB), and serum calcium ion (Ca2+), high-density lipoprotein cholesterol (HDL-C), blood urea nitrogen (BUN), serum creatinine (CR). Clinical complications, including acute peripancreatic fluid collection (APFC) and systemic inflammatory response syndrome (SIRS), were documented. Interventions administered within 48 hours, including plasma exchange and insulin therapy (administered intravenously and subcutaneously), were recorded. Laboratory parameters were measured in SI units: triglycerides (TG) and HDL cholesterol in mmol/L; blood cell counts (neutrophils, monocytes, lymphocytes, platelets) in ×109/L; hematocrit in %; blood urea nitrogen (BUN) in mmol/L; serum creatinine (Cr) in μmol/L; albumin (ALB) in g/L; and serum calcium (Ca2+) in mmol/L. Novel inflammatory indices were calculated as follows: Neutrophil-to-HDL cholesterol ratio (NHR = Neu/HDL-C); Monocyte-to-HDL cholesterol ratio (MHR = Mon/HDL-C); Lymphocyte-to-HDL cholesterol ratio (LHR = Lym/HDL-C); Platelet-to-HDL cholesterol ratio (PHR = PLT/HDL-C); Systemic inflammatory response index (SII = (PLT × Neu)/Lym); Systemic inflammation response index (SIRI = (Neu × Mon)/Lym); Aggregate index of systemic inflammation (AISI = (Neu × PLT × Mon)/Lym). Parameter definitions were based on previous predictive studies of pancreatitis.19–24
Statistical Analysis
For continuous quantitative data, such as those following a normal distribution, the mean ± standard deviation is used for description, and a t-test is employed to compare two groups. In contrast, one-way ANOVA is used for comparisons among multiple groups. If the data do not follow a normal distribution, the median [P25, P75] is used for statistical description, and the rank sum test is used for group comparisons. For count data, the number of cases (%) is used for description, and the chi-square test or Fisher’s exact probability method is used for group comparisons. Multiple imputation is used to fill in missing values.
Given the relatively small sample size in the SAP group (n=54) and to enhance the statistical power for identifying predictors of non-mild disease, the primary composite outcome was defined as MSAP+SAP. Additional analyses comparing MAP vs MSAP and MSAP vs SAP are provided in the Supplementary Materials for reference. To explore the association between the numerical values of the new inflammatory markers as independent variables and MSAP + SAP/SAP, restricted cubic spline plots were drawn using the rms package in R language. The median was used as the reference point, and the model was corrected for relevant covariates (age, gender, drinking, smoking, hypertension, diabetes, TG, HCT, BUN, Ca2+, and serum albumin (ALB)). The overall association P value and nonlinearity P value were calculated through the Wald test.
According to the Strengthening Statement of Observational Research Report,25 single-variable and multivariate logistic regressions were further used to explore the association between different levels of independent variables (excluding those included in the model as continuous variables and grouped according to numerical levels using tertiles) and MSAP + SAP/SAP, and multiple models were constructed. In model 1, confounding factors were not controlled; in model 2, age and gender were controlled for; in model 3, age, gender, drinking, smoking, hypertension, diabetes, TG, HCT, BUN, Ca2+, ALB, and medication were controlled for. Trend tests were conducted based on the medians of different tertiles. Finally, receiver operating characteristic (ROC) curve analysis was used to evaluate the predictive performance for MSAP+SAP/SAP, reporting the area under the curve (AUC) with 95% confidence intervals, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV).
All statistical analyses and related chart drawings were conducted in R language (version 4.4.1), and a two-sided P value < 0.05 was considered statistically significant.
Results
Basic Characteristics
A total of 340 patients were included in the study. The severity of AP was grouped according to RAC, and the groups were divided into three categories: mild (MAP, n = 156), moderate-severe (MSAP, n = 130), and severe (SAP, n = 54). Among them, 273 were male (80.3%), and 67 were female (19.7%). Their median age was 36 years (interquartile range [IQR]: 32–42 years).
Table 1 presents the baseline demographic and clinical characteristics of the three groups. Patients with more severe disease had higher SIRS incidence (p < 0.001). In terms of laboratory indicators, the higher the levels of neutrophil count (Neu), triglycerides (TG), and hematocrit (HCT), the more severe the condition, and the difference was statistically significant (P < 0.05). However, as the condition worsened, the values of HDL, Lym, ALB, and Ca2+ became lower, and the differences were statistically significant (P < 0.001). The differences in complications (SIRS, APFC) and treatment measures (insulin therapy and plasma exchange) within 48 hours among the three groups were statistically significant (P < 0.01).
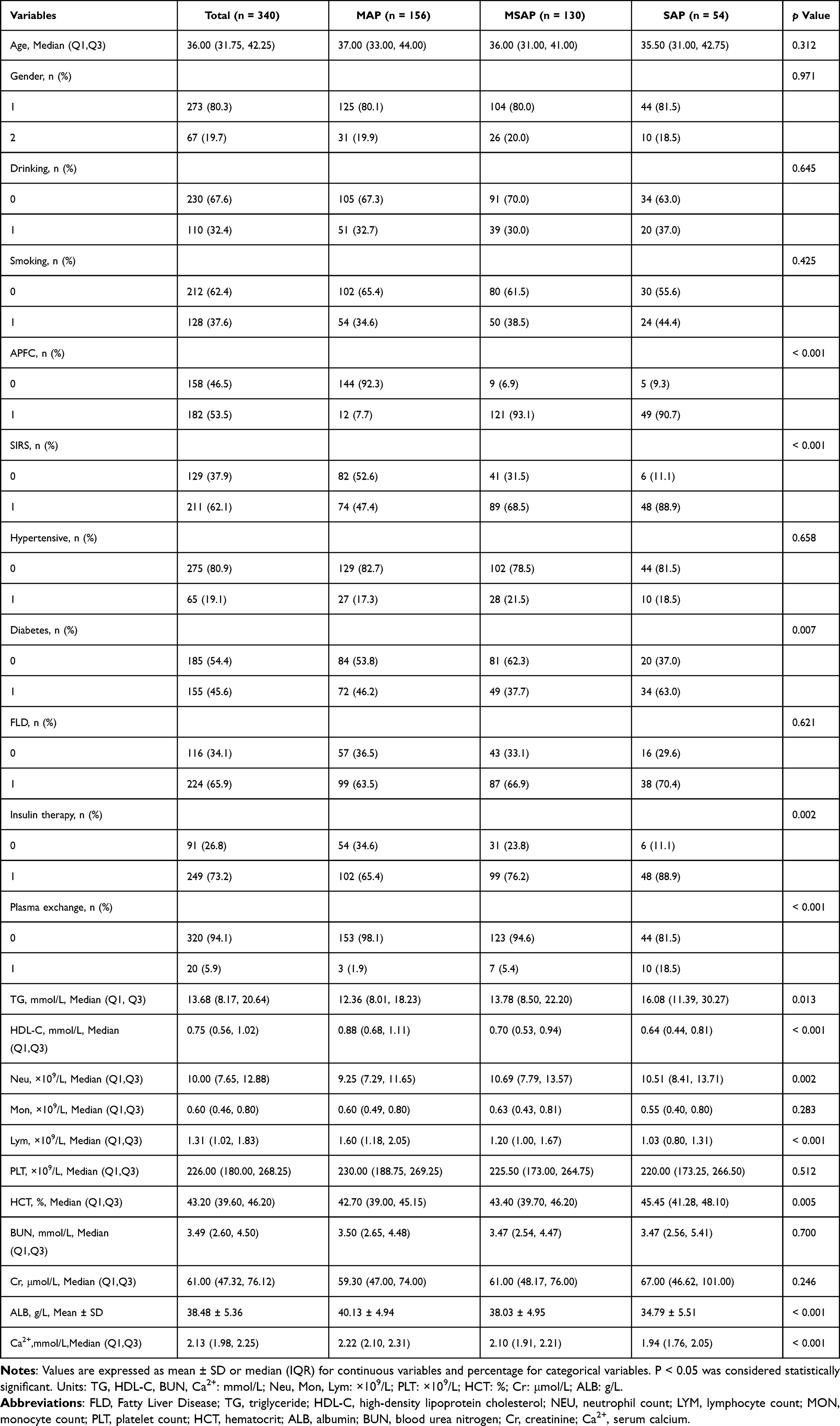 |
Table 1 Baseline Demographic and Clinical Characteristics of Patients with Hypertriglyceridemia-Associated Acute Pancreatitis, Stratified by Disease Severity |
Table 2 presents the baseline characteristics of the three groups of new inflammatory markers. It was observed that NHR, MHR, PHR, SII, SIRI, and AISI all were significantly higher in patients with MSAP or SAP compared to the mild cases (MAP) (P < 0.01). Among them, NHR, SII, and SIRI showed a strictly increasing trend with the severity of the disease. In contrast, MHR, PHR, and AISI rose overall in the severe group but did not form a statistically significant gradient between the MSAP and SAP groups. Figure 2 presents the pairwise comparisons of inflammatory indicators among the three patient groups to explore the differences between these two groups further. NHR demonstrated statistically significant differences across all comparisons: MAP vs MSAP (P<0.001), MAP vs SAP (P<0.001), and MSAP vs SAP (P<0.05). MHR, SII, SIRI, PHR, and AISI showed significant differences between the MAP and MSAP groups, as well as between the MAP and SAP groups (all P<0.05), but did not show statistically significant differences between the MSAP and SAP groups (P>0.05). LHR was not statistically significant in any group comparison (all P>0.05). It should be noted that the sample size of the SAP group was relatively small, which may have limited the statistical power to detect differences in the MSAP vs SAP comparisons.
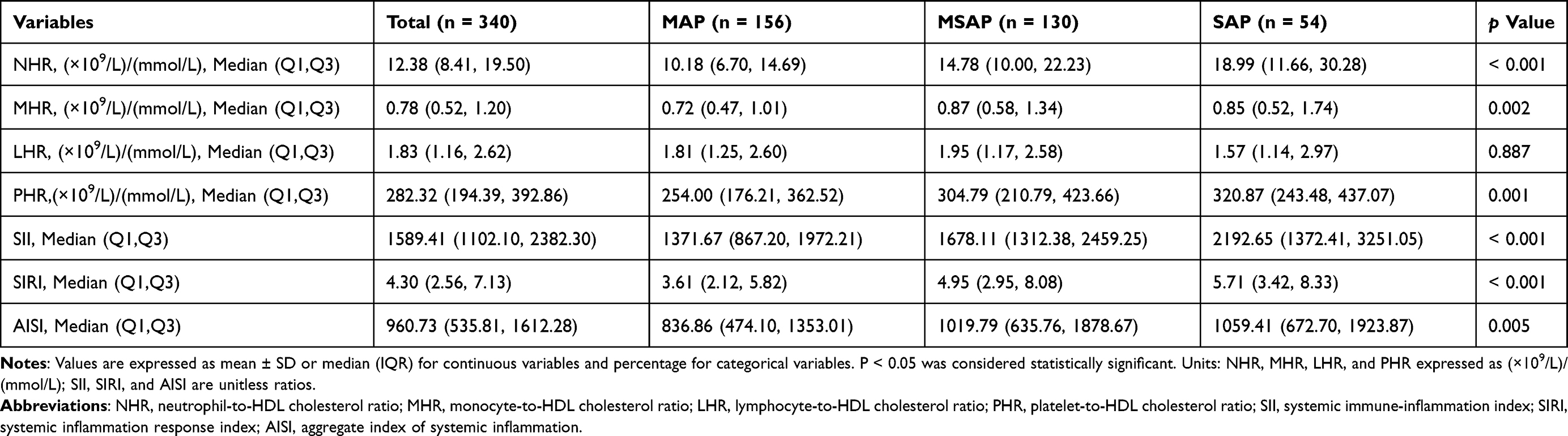 |
Table 2 Baseline Levels of Novel Inflammatory Markers in Patients with Hypertriglyceridemia-Associated Acute Pancreatitis, Stratified by Disease Severity |
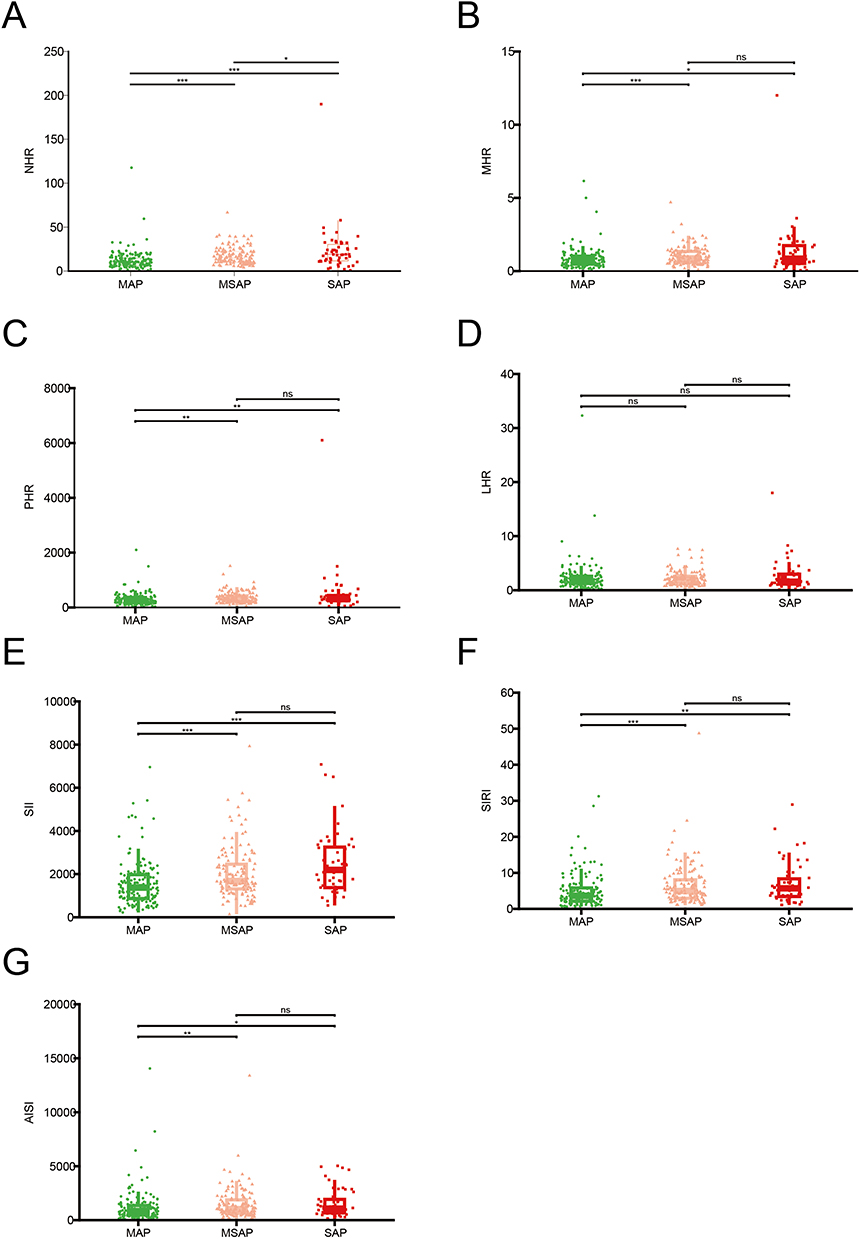 |
Figure 2 Distribution of novel inflammatory markers across disease severity groups. (A) The box plots among the three groups of NHR. (B) The box plots among the three groups of MHR. (C) The box plots among the three groups of PHR. (D) The box plots among the three groups of LHR. (E) The box plots among the three groups of SII. (F) The box plots among the three groups of SIRI. (G) The box plots for the three AISI groups. The asterisks indicate the P-values after the Benjamini-Hochberg correction (*P < 0.05; **P < 0.01; *** P < 0.001). Abbreviation: ns, not significant. |
Nonlinear Relation of Novel Inflammatory Markers with Severity of HTG-AP
To explore the potential nonlinear relationship between various inflammatory indicators and the severity of HTG-AP, we used restricted cubic spline (RCS) models. MSAP+SAP, representing the non-mild disease population, was used as the primary composite outcome. As shown in Figure 3, when MSAP+SAP was used as the outcome variable, significant nonlinear associations were observed for NHR (Overall association P < 0.001, Nonlinear P = 0.002), SII (Overall association P < 0.001, Nonlinear P = 0.006), AISI (Overall association P = 0.003, Nonlinear P = 0.002), MHR (Overall association P = 0.003, Nonlinear P = 0.026), and SIRI (Overall association P = 0.001, Nonlinear P = 0.011). These markers exhibited a threshold effect, with the risk of severe disease significantly increasing beyond specific values, suggesting their potential value as prognostic indicators for HTG-AP severity. In contrast, LHR (Overall association P = 0.267, Nonlinear P = 0.122) and PHR (Overall association P = 0.061, Nonlinear P = 0.066) did not show significant associations. When SAP alone was used as the outcome variable (Figure 4), only SII showed a statistically significant overall association (P = 0.014), while none of the other inflammatory indicators reached significance. The small sample size of the SAP group may have limited the ability to detect significant nonlinear relationships in these analyses.
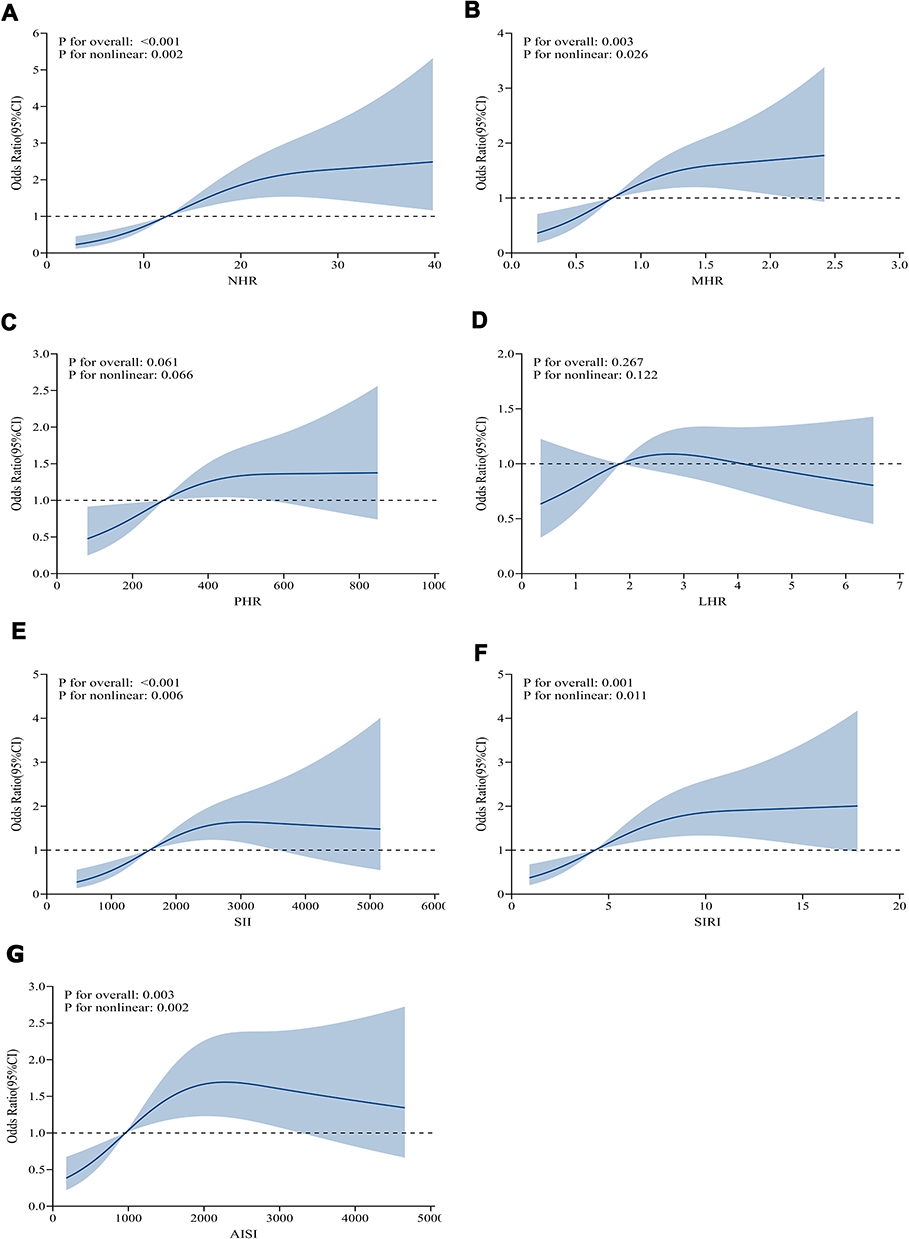 |
Figure 3 Restricted cubic spline analyses depicting the nonlinear associations between novel inflammatory markers and the risk of developing moderate-severe or severe acute pancreatitis (MSAP+SAP). (A) RCS analysis of the correlation between NHR and the outcomes of MSAP + SAP. (B) RCS analysis of the correlation between MHR and the outcomes of MSAP + SAP. (C) RCS analysis of the correlation between PHR and the outcomes of MSAP + SAP. (D) RCS analysis of the correlation between LHR and the outcomes of MSAP + SAP. (E) RCS analysis of the correlation between SII and the outcomes of MSAP + SAP. (F) RCS analysis of the correlation between SIRI and the outcomes of MSAP + SAP. (G) RCS analysis of the correlation between AISI and the outcomes of MSAP + SAP. |
 |
Figure 4 Restricted cubic spline analyses depicting the nonlinear associations between novel inflammatory markers and the risk of developing severe acute pancreatitis (SAP). (A) RCS analysis of the correlation between NHR and the outcomes of SAP. (B) RCS analysis of the correlation between MHR and the outcomes of SAP. (C) RCS analysis of the correlation between PHR and the outcomes of SAP. (D) RCS analysis of the correlation between LHR and the outcomes of SAP. (E) RCS analysis of the correlation between SII and the outcomes of SAP. (F) RCS analysis of the correlation between SIRI and the outcomes of SAP. (G) RCS analysis of the correlation between AISI and the outcomes of SAP. |
Independent Associations with Full Adjustment for Confounders
Multivariable logistic regression analysis was performed to evaluate the independent associations between inflammatory markers and disease severity, with full adjustment for clinical confounders including age, gender, drinking, smoking, hypertension, diabetes, TG, HCT, BUN, Ca2+, albumin, and medication use. Several markers showed significant associations for the primary outcome of MSAP+SAP (representing the non-mild disease population, Figure 5). When analyzed as continuous variables, NHR (OR = 1.06, 95% CI: 1.03–1.10, P < 0.001), MHR (OR = 1.73, 95% CI: 1.14–2.62, P = 0.010), SII (OR = 1.00, 95% CI: 1.00–1.00, P = 0.005), and SIRI (OR = 1.09, 95% CI: 1.02–1.15, P = 0.006) demonstrated significant positive associations. Categorical analysis by tertiles revealed significant dose-response relationships for NHR, MHR, SII, SIRI, and AISI, with the highest tertile (Q3) showing elevated risks compared to the reference (Q1) (all P for trend < 0.05). The fully adjusted OR for the highest tertile of NHR was 6.03 (95% CI: 2.98–12.19, P < 0.001). LHR was not significantly associated with MSAP+SAP risk in any of the models. For the outcome of SAP alone (Figure 6), NHR and SII maintained significant trends when analyzed by tertiles (P for trend = 0.012 and 0.008, respectively). In contrast, most markers, when analyzed as continuous variables, did not retain statistical significance after full adjustment. It should be noted that the relatively small sample size in the SAP group may have limited the statistical power to detect significant associations. Additional analyses comparing MSAP with MAP and SAP with MSAP are provided in Figures S1 and S2. The MSAP vs MAP comparisons showed association patterns generally consistent with the primary outcome, whereas fewer significant associations were observed in the SAP vs MSAP comparisons.
 |
Figure 5 Forest plot showing the association between novel inflammatory markers and the risk of moderate-severe or severe acute pancreatitis (MSAP+SAP) in multivariate logistic regression models. The blocks in the figure represent continuous variables (for each 1-unit increase) or the odds ratio (OR) values of the interquartile range (Q3 - Q1) in the multivariate logistic regression model. The horizontal lines represent the 95% confidence interval (CI). Here: Model 1 (unadjusted), Model 2 (adjusted for age and gender), Model 3 (adjusted for age, gender, alcohol consumption, smoking, hypertension, diabetes, triglycerides (TG), hematocrit (HCT), blood urea nitrogen (BUN), blood calcium (Ca2+), serum albumin (ALB), and medication status). |
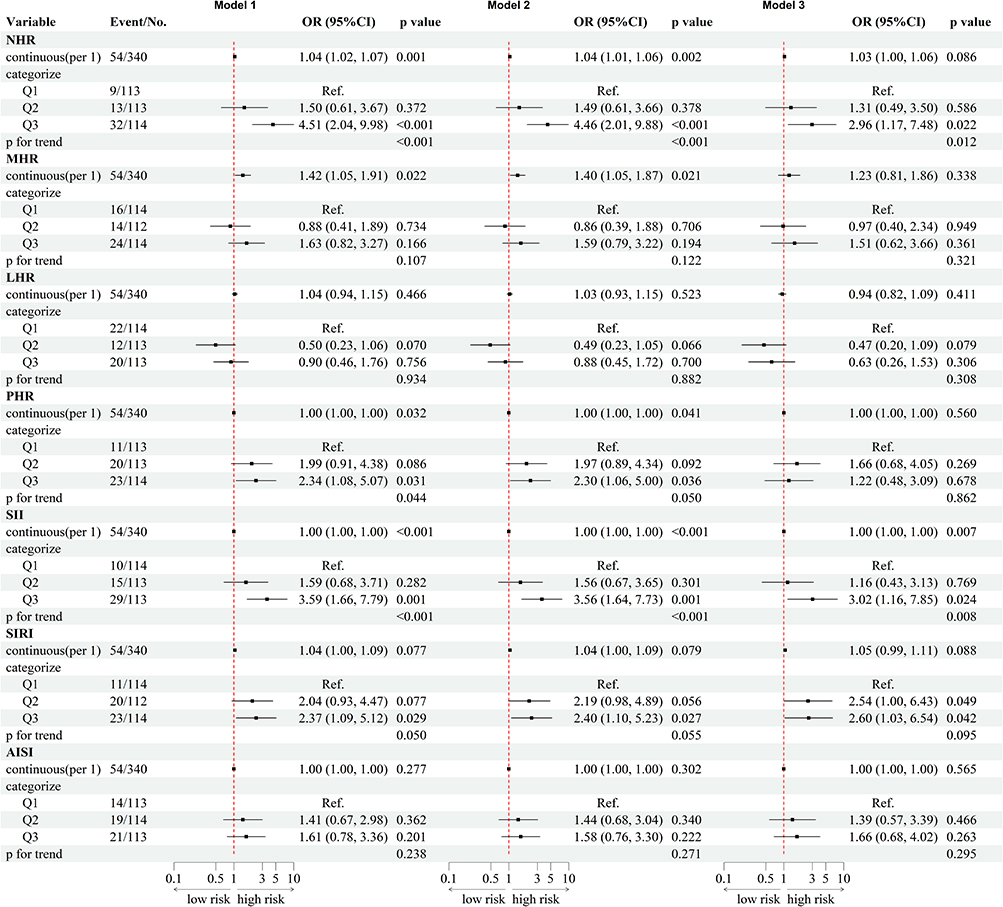 |
Figure 6 Forest plot showing the association between novel inflammatory markers and severe acute pancreatitis (SAP) risk in multivariate logistic regression models. The blocks in the figure represent continuous variables (for each 1-unit increase) or the odds ratio (OR) values of the interquartile range (Q3 - Q1) in the multivariate logistic regression model. The horizontal lines represent the 95% confidence interval (CI). Here: Model 1 (unadjusted), Model 2 (adjusted for age and gender), Model 3 (adjusted for age, gender, alcohol consumption, smoking, hypertension, diabetes, triglycerides (TG), hematocrit (HCT), blood urea nitrogen (BUN), blood calcium (Ca2+), serum albumin (ALB), and medication status). |
Predictive Performance of Inflammatory Markers for Disease Severity
Receiver operating characteristic (ROC) analysis was conducted to assess the predictive accuracy of inflammatory markers for disease severity. For the primary composite outcome of MSAP+SAP (indicating non-mild disease, Figure 7 and Table 3), the AUC values were as follows: NHR showed the highest predictive ability (AUC = 0.701, 95% CI: 0.646–0.756), followed by SII (AUC = 0.666, 95% CI: 0.608–0.723), SIRI (AUC = 0.622, 95% CI: 0.562–0.681), MHR (AUC = 0.612, 95% CI: 0.553–0.672), PHR (AUC = 0.611, 95% CI: 0.551–0.671), and AISI (AUC = 0.601, 95% CI: 0.541–0.661). All these markers demonstrated statistically significant predictive value (P < 0.05). Notably, SII had the highest sensitivity (0.826) for detecting non-mild cases but showed moderate specificity (0.429), whereas NHR offered a more balanced profile, with a sensitivity of 0.565 and a specificity of 0.744. Conversely, LHR did not show significant predictive value (AUC = 0.505, 95% CI: 0.444–0.567, P = 0.569). For the outcome of SAP alone (Figure 8 and Table 4), the predictive performance of most markers was generally reduced. NHR (AUC = 0.674, 95% CI: 0.587–0.762) and SII (AUC = 0.661, 95% CI: 0.582–0.739) maintained the highest predictive ability among all markers, with NHR again showing a balanced performance (sensitivity = 0.574, specificity = 0.745) and SII demonstrating improved specificity (0.773) compared to its performance in the composite outcome. Other markers, such as MHR and AISI, exhibited limited discriminative ability (AUC < 0.600, P > 0.05). PHR and SIRI, though statistically significant (P < 0.05), showed only modest AUC values (0.594 for both), with high sensitivity but low specificity, indicating a tendency for false positives in predicting SAP. Additional ROC analyses are provided in SAP vs MSAP (Figure S3) and MSAP vs MAP (Figure S4). The observed patterns for MSAP vs MAP were generally consistent with those for MSAP+SAP, while the SAP vs MSAP comparisons showed reduced discrimination across all markers. Detailed AUC values, optimal cutoff points, sensitivity, specificity, and other performance metrics—including accuracy, positive predictive value, negative predictive value, and Youden’s index—for all markers across these comparisons are summarized in Table S1 (SAP vs MSAP) and Table S2 (MSAP vs MAP). For example, in the MSAP vs MAP comparison, NHR (cutoff = 12.146) achieved an AUC of 0.686, while SII (cutoff = 1381.787) had an AUC of 0.643. Conversely, in the SAP vs MSAP comparison, all markers showed lower discriminatory power, with the highest AUC being 0.597 for NHR.
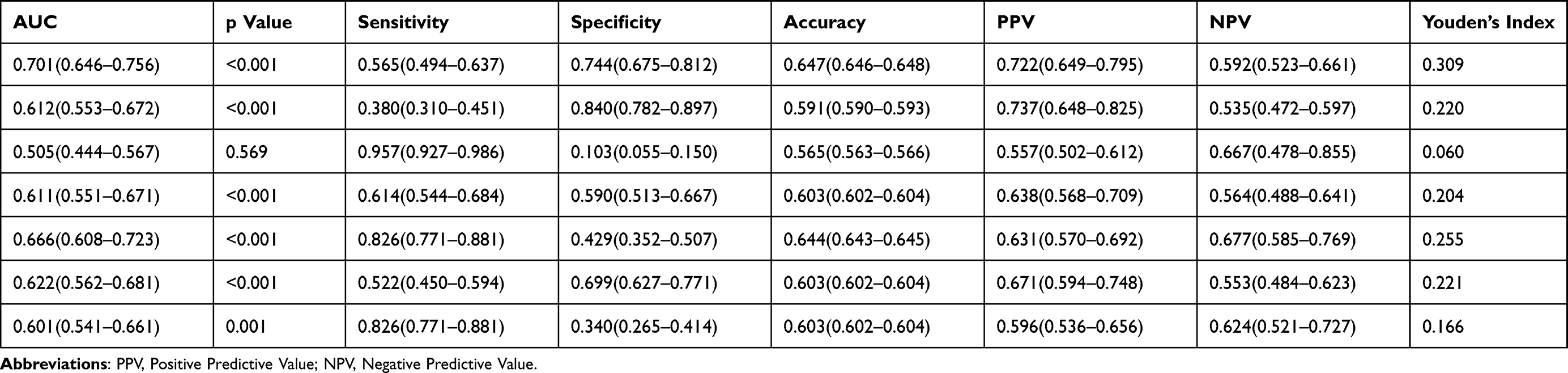 |
Table 3 Predictive Performance of Novel Inflammatory Markers for Moderate-Severe and Severe Acute Pancreatitis (MSAP+SAP) |
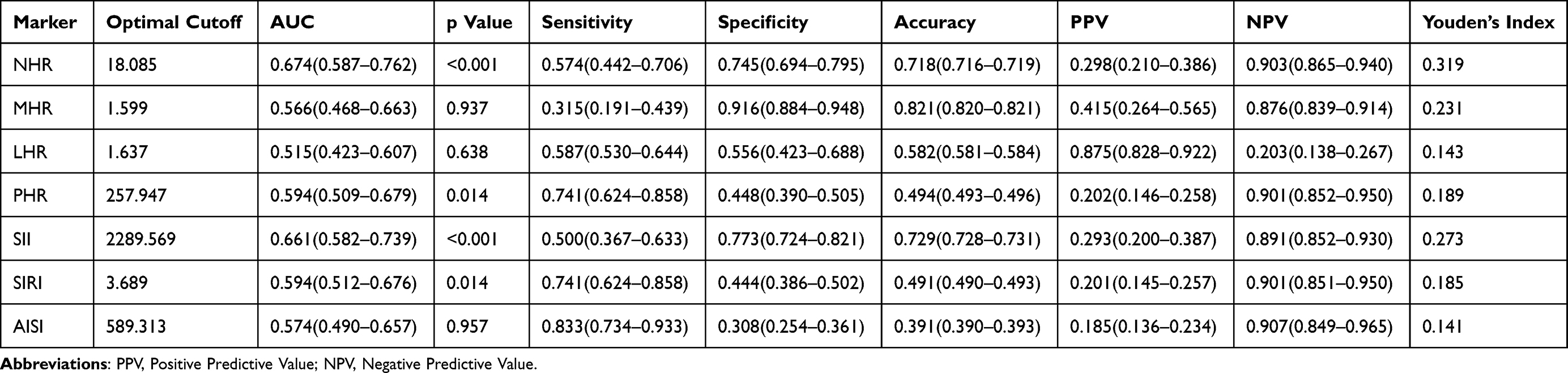 |
Table 4 Predictive Performance of Novel Inflammatory Markers for Severe Acute Pancreatitis (SAP) |
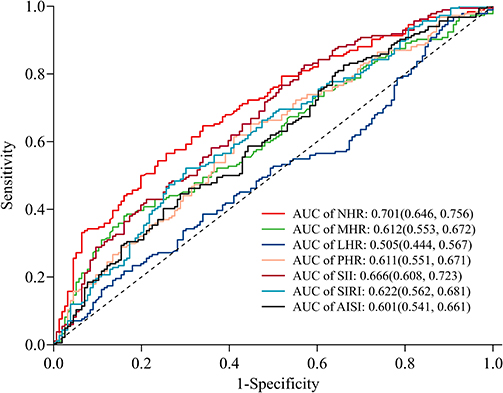 |
Figure 7 Receiver operating characteristic (ROC) curves assessing the predictive performance of novel inflammatory markers for moderate-severe or severe acute pancreatitis (MSAP+SAP). Abbreviations: NHR, neutrophil-to-HDL cholesterol ratio; MHR, monocyte-to-HDL cholesterol ratio; LHR, lymphocyte-to-HDL cholesterol ratio; PHR, platelet-to-HDL cholesterol ratio. SIRI, systemic inflammation response index; SII, systemic inflammatory response Index; AISI, aggregate index of systemic inflammation. |
 |
Figure 8 Receiver operating characteristic (ROC) curves assessing the predictive performance of novel inflammatory markers for severe acute pancreatitis (SAP). Abbreviations: NHR, neutrophil-to-HDL cholesterol ratio; MHR, monocyte-to-HDL cholesterol ratio; LHR, lymphocyte-to-HDL cholesterol ratio; PHR, platelet-to-HDL cholesterol ratio. SIRI, systemic inflammation response index; SII, systemic inflammatory response Index; AISI, aggregate index of systemic inflammation. |
Discussion
This study offers the first comprehensive assessment of a panel of novel inflammatory ratios for early risk stratification in Hypertriglyceridemia-associated Acute Pancreatitis (HTG-AP). Our results align with our internal findings and are strongly supported by existing scientific literature. They directly address the study’s objective and highlight their importance in the broader context of inflammatory and metabolic disease research.
The central finding of our study is the superior predictive performance of the neutrophil-to-high-density lipoprotein cholesterol ratio (NHR). We demonstrated that NHR was significantly elevated with increasing disease severity (Figure 2A and Table 2) and emerged as the most powerful independent predictor of progression to MSAP + SAP (fully-adjusted OR for Q3: 6.03; AUC: 0.701; Figures 5 and 7). The mechanistic plausibility of this finding is supported by the well-established pathobiology of both AP and metabolic syndrome. Neutrophils are primary effector cells in AP; their activation leads to protease release and neutrophil extracellular trap (NET) formation, directly causing acinar cell injury and amplifying systemic inflammation.26,27 Conversely, high-density lipoprotein cholesterol (HDL-C) is not merely a lipid marker but a potent anti-inflammatory and antioxidant agent that can mitigate endothelial damage and neutralize inflammatory mediators.28 The NHR elegantly captures this critical balance between a key driver of injury (neutrophils) and a crucial defender (HDL-C). Our results are further bolstered by Mendelian randomization studies confirming that genetically lower HDL-C levels are a causal risk factor for AP,29 and by clinical studies outside gastroenterology where NHR has proven to be a valuable prognostic marker in cardiovascular and neurological diseases.12,30
Similarly, the significant associations we observed for the systemic immune-inflammation index (SII) and systemic inflammation response index (SIRI) reinforce their role as integrative indicators of a dysregulated immune response. The predictive value of SII (AUC = 0.666) is consistent with its proven utility in forecasting outcomes in various cancers and inflammatory conditions.31,32 It integrates the proliferative capacity of platelets, the inflammatory drive of neutrophils, and the immune regulatory state of lymphocytes. Likewise, the prognostic value of the monocyte-to-HDL ratio (MHR) is supported by growing evidence of its role in metabolic syndrome and its components,33 and specifically in HTG-AP, where monocytes are known to be significantly elevated and dynamically changed in severe cases.34 This convergence of our results with external evidence across different disciplines underscores the fundamental role of systemic inflammation in disease progression.
In contrast to the significant associations observed for NHR and other markers, the lymphocyte-to-HDL ratio (LHR) demonstrated no substantial prognostic value in our cohort. This finding appears to contradict several studies in general acute pancreatitis, which have identified lymphopenia as a reliable marker of disease severity and a predictor of complications like infected pancreatic necrosis.35,36 This discrepancy, however, may be attributed to the unique pathophysiology of HTG-AP. The early hyperinflammatory phase of HTG-AP, captured within our 48-hour admission window, may be so overwhelmingly dominated by neutrophilic and monocytic activation26,34 that the role of lymphocyte depletion is masked or becomes secondary in the initial risk stratification. Furthermore, the function of specific lymphocyte subsets (eg, T cells, B cells) may be more relevant than the total lymphocyte count, as suggested by ongoing research into lymphocyte dynamics in AP.37 Therefore, while lymphopenia remains a valuable prognostic marker in broader AP contexts, its derivative ratio (LHR) may not be optimal for early risk assessment, specifically in HTG-AP.
An intriguing and nuanced finding was the limited discriminatory power of most markers between MSAP and SAP, as opposed to their strong performance in identifying non-mild (MSAP+SAP) disease. While the limited sample size in our SAP group (n = 54) may contribute to this, it also offers a plausible pathophysiological insight. These early (<48h) hematological markers are exquisitely sensitive to the initial systemic inflammatory “storm” that defines the transition from local to systemic illness (ie, from MAP to MSAP). However, the subsequent progression from transient to persistent organ failure (ie, MSAP to SAP) is likely governed by a “second hit”, such as the development of infected pancreatic necrosis or gut-derived sepsis, events that may not be fully predicted by admission blood counts alone. This concept is supported by studies showing that different clinical or biochemical markers often predict later complications in AP.38,39
We acknowledge the limitations of our study, primarily the single-center retrospective design and the modest sample size of the SAP subgroup, which constrained our power to analyze this most severe category in isolation. Future prospective multicenter studies with larger cohorts are warranted to validate our proposed NHR cutoff and explore the dynamic changes in these ratios throughout the disease course. Furthermore, integrating these promising inflammatory markers with clinical scoring systems or imaging findings could yield a more powerful composite model for early prediction.
In conclusion, our findings are relevant and directly correlate with the study’s results and objectives. We have identified NHR as a novel, robust, and clinically accessible biomarker for the early risk stratification of HTG-AP. The strength and consistency of our results, underpinned by solid pathophysiological mechanisms and supported by a body of external literature, affirm that these inflammatory ratios are not merely statistical associations but reflect core biological processes driving HTG-AP severity. Integrating NHR (cutoff = 14.484) into initial clinical assessment provides a rapid and straightforward tool to facilitate earlier targeted interventions for high-risk patients, aiming to improve outcomes in this challenging disease.
Conclusion
Our findings show that the neutrophil-to-HDL-C ratio (NHR) is an independent predictor of non-mild HTG-AP (MSAP+SAP), with the highest tertile associated with a 6.03-fold increased odds (95% CI: 2.98–12.19; P < 0.001) and an AUC of 0.701. While NHR and SII also have predictive value for SAP alone, their performance is stronger for the combined outcome of MSAP+SAP, emphasizing their potential in early detection of patients at risk of progressing beyond mild disease. Further validation is needed to confirm their ability to differentiate between MSAP and SAP. Incorporating NHR (using the optimal cutoff of 14.484 [(×109/L)/(mmol/L)]) into current clinical practices may support early risk stratification and prognosis. Additional research should explore the mechanistic links between inflammatory dysregulation—such as NHR-related neutrophil activation and HDL-C dysfunction—and the severity of HTG-AP to inform targeted treatments.
Data Sharing Statement
The data sets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This article is an analysis and study of the medical records and biological samples obtained from previous clinical treatments, and it meets all of the following conditions: 1) The risks to the research subjects do not exceed the minimum risk; 2) The exemption of the informed consent procedure will not have any adverse impact on the rights and health of the research subjects; 3) The privacy and personal identity information of the research subjects have been protected. Therefore, we applied for the exemption of informed consent. Subsequently, the Research Ethics Committee of Shenzhen People’s Hospital approved our application for the exemption of informed consent.
This retrospective study was approved by the Research Ethics Committee of Shenzhen People’s Hospital (LL-KY-202411901) and conducted in accordance with the Declaration of Helsinki.
Acknowledgments
We thank Dr. Yu Chuanchuan from the Medical Statistics Department at the School of Public Health, Sun Yat-sen University, in Guangdong Province, for his statistical support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Iannuzzi JP, King JA, Leong JH, et al. Global incidence of acute pancreatitis is increasing over time: a systematic review and meta-analysis. Gastroenterology. 2022;162(1):122–134. doi:10.1053/j.gastro.2021.09.043
2. Zhu Y, Pan X, Zeng H, et al. A study on the etiology, severity, and mortality of 3260 patients with acute pancreatitis according to the revised atlanta classification in jiangxi, china over an 8-year period. Pancreas. 2017;(4):504–509.
3. Deng H, Peng K, Zhang L, et al. Clinical outcomes in a multicenter cohort involving 919 patients with hypertriglyceridemia-associated acute pancreatitis. Am J Gastroenterol. 2025. doi:10.14309/ajg.0000000000003319
4. Lu Z, Zhang G, Guo F, et al. Elevated triglycerides on admission positively correlate with the severity of hypertriglyceridaemic pancreatitis. Int J Clin Pract. 2020;74(3):e13458. doi:10.1111/ijcp.13458
5. Song K, Wu Z, Meng J, et al. Hypertriglyceridemia as a risk factor for complications of acute pancreatitis and the development of a severity prediction model. HPB. 2023;25(9):1065–1073. doi:10.1016/j.hpb.2023.05.006
6. Bálint ER, Fűr G, Kiss L, et al. Assessment of the course of acute pancreatitis in the light of aetiology: a systematic review and meta-analysis. Sci Rep. 2020;10(1):17936. doi:10.1038/s41598-020-74943-8
7. Capurso G, Pisani RPDL, Lauri G, et al. Clinical usefulness of scoring systems to predict severe acute pancreatitis: a systematic review and meta-analysis with pre and post-test probability assessment. United Eur Gastroenterol J. 2023;11(9):825–836. doi:10.1002/ueg2.12464
8. Qin B, Ma N, Tang Q, et al. Neutrophil to lymphocyte ratio (NLR) and platelet to lymphocyte ratio (PLR) were useful markers in assessment of inflammatory response and disease activity in SLE patients. Mod Rheumatol. 2016;26(3):372–376. doi:10.3109/14397595.2015.1091136
9. Santoro L, Ferraro PM, Nesci A, et al. Neutrophil-to-lymphocyte ratio but not monocyte-to-HDL cholesterol ratio nor platelet-to-lymphocyte ratio correlates with early stages of lower extremity arterial disease: an ultrasonographic study. Eur Rev Med Pharmacol Sci. 2021;25(9):3453–3459. doi:10.26355/eurrev_202105_25826
10. Yu S, Guo X, Li G, Yang H, Zheng L, Sun Y. Lymphocyte to high-density lipoprotein ratio but not platelet to lymphocyte ratio effectively predicts metabolic syndrome among subjects from rural China. Front Cardiovasc Med. 2021;8:583320. doi:10.3389/fcvm.2021.583320
11. Wang W, Chen ZY, Guo XL, Tu M. Monocyte to high-density lipoprotein and apolipoprotein a1 ratios: novel indicators for metabolic syndrome in chinese newly diagnosed type 2 diabetes. Front Endocrinol. 2022;13:935776. doi:10.3389/fendo.2022.935776
12. Liu Z, Fan Q, Wu S, Wan Y, Lei Y. Compared with the monocyte to high-density lipoprotein ratio (MHR) and the neutrophil to lymphocyte ratio (NLR), the neutrophil to high-density lipoprotein ratio (NHR) is more valuable for assessing the inflammatory process in Parkinson’s disease. Lipids Health Dis. 2021;20(1):35. doi:10.1186/s12944-021-01462-4
13. Jialal I, Jialal G, Adams‐Huet B. The platelet to high density lipoprotein ‐cholesterol ratio is a valid biomarker of nascent metabolic syndrome. Diab Metabol Res. 2021;37(6):e3403. doi:10.1002/dmrr.3403
14. Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62(1):102–111. doi:10.1136/gutjnl-2012-302779
15. Zhang R, Deng L, Jin T, et al. Hypertriglyceridaemia-associated acute pancreatitis: diagnosis and impact on severity. HPB. 2019;21(9):1240–1249. doi:10.1016/j.hpb.2019.01.015
16. Yang AL, McNabb-Baltar J. Hypertriglyceridemia and acute pancreatitis. Pancreatology. 2020;20(5):795–800. doi:10.1016/j.pan.2020.06.005
17. Jaber S, Garnier M, Asehnoune K, et al. Guidelines for the management of patients with severe acute pancreatitis, 2021. Anaesth Crit Care Pain Med. 2022;41(3). doi:10.1016/j.accpm.2022.101060
18. Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992;101(6):1644–1655. doi:10.1378/chest.101.6.1644
19. Lin XY, Zeng Y, Zhang ZC, Lin ZH, Chen LC, Ye ZS. Incidence and clinical characteristics of hypertriglyceridemic acute pancreatitis: a retrospective single-center study. World J Gastroenterol. 2022;28(29):3946–3959. doi:10.3748/wjg.v28.i29.3946
20. Yasak IH, Yilmaz M. The relationship between systemic immune-inflammation index and length of hospitalization in acute pancreatitis. Ann Clin Analytical Med. 2023;14(4):340–344. doi:10.4328/ACAM.21511
21. Song X, Shi D, Cui Q, et al. Intensive insulin therapy versus plasmapheresis in the management of hypertriglyceridemia-induced acute pancreatitis (Bi-TPAI trial): study protocol for a randomized controlled trial. Trials. 2019;20(1). doi:10.1186/s13063-019-3498-x
22. Yang L, He C, Wang W. Association between neutrophil to high-density lipoprotein cholesterol ratio and disease severity in patients with acute biliary pancreatitis. Ann Med. 2024;56(1). doi:10.1080/07853890.2024.2315225
23. Liu X, Guan G, Cui X, Liu Y, Liu Y, Luo F. Systemic immune-inflammation index (SII) can be an early indicator for predicting the severity of acute pancreatitis: a retrospective study. Int J Gen Med. 2021;14:9483–9489. doi:10.2147/IJGM.S343110
24. Afari ME, Shafqat H, Shafi M, Marmoush FY, Roberts MB, Minami T. Hypertriglyceridemia-induced pancreatitis: a decade of experience in a community-based teaching hospital. R I Med J. 2015;98(12):40–43.
25. Cuschieri S. The STROBE guidelines. Saudi J Anaesth. 2019;13(Suppl 1):S31–S34. doi:10.4103/sja.SJA_543_18
26. Wu X, Yang Z, Wang H, Zhao Y, Gao X, Zang B. High-mobility group box protein-1 induces acute pancreatitis through a activation of neutrophil extracellular trap and subsequent production o f IL-1β. Life Sci. 2021;286:119231. doi:10.1016/j.lfs.2021.119231
27. Wan J, Ren Y, Yang X, Li X, Xia L, Lu N. The role of neutrophils and neutrophil extracellular traps in acute pa ncreatitis. Front Cell Dev Biol. 2021;8. doi:10.3389/fcell.2020.565758
28. Soran H, Hama S, Yadav R, Durrington PN. HDL functionality. Curr Opin Lipidol. 2012;23(4):353–366. doi:10.1097/MOL.0b013e328355ca25
29. Biqi W, Jacqueline SD, Yuxuan W, et al. Lipid levels and risk of acute pancreatitis using bidirectional Mendelian randomization. Sci Rep. 2024. doi:10.1038/s41598-024-56946-x
30. Lamichhane P, Agrawal A, Abouainain Y, Abousahle S, Regmi PR. Utility of neutrophil-to-high-density lipoprotein-cholesterol ratio in patients with coronary artery disease: a narrative review. J Int Med Res. 2023;51(4):3000605231166518. doi:10.1177/03000605231166518
31. Nakamoto S, Ohtani Y, Sakamoto I, Hosoda A, Ihara A, Naitoh T. Systemic immune-inflammation index predicts tumor recurrence after radical resection for colorectal cancer. Tohoku J Exp Med. 2023;261(3):229–238. doi:10.1620/tjem.2023.J074
32. Zhou Q, Su S, You W, Wang T, Ren T, Zhu L. Systemic inflammation response index as a prognostic marker in cancer patients: a systematic review and meta-analysis of 38 cohorts. Dose-Response. 2021;19(4). doi:10.1177/15593258211064744
33. Jun WT, Qi CX, Gong J, Fang XQ, Yan XG, Di XL. Association of monocytes to high-density lipoprotein cholesterol ratio with metabolic syndrome and its components. Am J Hypertens. 2021;34(8):888–889. doi:10.1093/ajh/hpab042
34. Zheng J, Fan J, Huang C, et al. Dynamic detection of monocyte subsets in peripheral blood of patients with acute hypertriglyceridemic pancreatitis. Gastroenterol Res Pract. 2019;2019:5705782. doi:10.1155/2019/5705782
35. Shen X, Sun J, Ke L, et al. Reduced lymphocyte count as an early marker for predicting infected pa ncreatic necrosis. BMC Gastroenterol. 2015;15(1). doi:10.1186/s12876-015-0375-2
36. Malheiro F, Leitão Do Nascimento M, Miguel Borrego L. Circulating blood B and T lymphocytes and severity of acute pancreatitis: a systematic review protocol. Acta Med Port. 2024;37(4):274–279. doi:10.20344/amp.20087
37. Ding L, Yang Y, Li H, Wang H, Gao P. Circulating lymphocyte subsets induce secondary infection in acute pan creatitis. Front Cell Infect Microbiol. 2020;10. doi:10.3389/fcimb.2020.00128
38. Tarján D, Szalai E, Lipp M, et al. Persistently high procalcitonin and C-reactive protein are good predictors of infection in acute necrotizing pancreatitis: a systematic review and meta-analysis. IJMS. 2024;25(2):1273. doi:10.3390/ijms25021273
39. Tran A, Fernando SM, Rochwerg B, et al. Prognostic factors associated with development of infected necrosis in patients with acute necrotizing or severe pancreatitis-A systematic review and meta-analysis. J Trauma Acute Care Surg. 2022;92(5):940–948. doi:10.1097/TA.0000000000003502
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Combined Diagnostic Value of Serum Trefoil Factor 2 and microRNA-186-5p for Evaluating Disease Severity in Patients with Acute Pancreatitis
Fang Z, Zhao H, Cheng Y, Yu L
Journal of Inflammation Research 2025, 18:7921-7931
Published Date: 17 June 2025