Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 17
Nomogram for Predicting Hypoglycemia in Type 2 Diabetes Mellitus Patients Treated with Insulin Pump During Enteral Nutrition
Authors Wu J, Wu J, Zhou Y, Lu X, Zhao W, Xu F
Received 21 August 2023
Accepted for publication 3 May 2024
Published 27 May 2024 Volume 2024:17 Pages 2147—2154
DOI https://doi.org/10.2147/DMSO.S436390
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Video abstract presented by Wu.
Views: 92
Jufei Wu,1,* Jishi Wu,2,* Yan Zhou,3 Xiaohua Lu,4 Wane Zhao,4 Fengmei Xu1
1Department of Neurosurgery, The First Affiliated Hospital of Jinan University, Guangzhou, People’s Republic of China; 2Department of General Medicine, The First Affiliated Hospital of Jinan University, Guangzhou, People’s Republic of China; 3Department of Interventional Radiology & Vascular Surgery, The First Affiliated Hospital of Jinan University, Guangzhou, People’s Republic of China; 4Department of Endocrinology, The First Affiliated Hospital of Jinan University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yan Zhou, Department of Interventional Radiology & Vascular Surgery, The First Affiliated Hospital of Jinan University, Guangzhou, People’s Republic of China, Email [email protected] Xiaohua Lu, Department of Endocrinology, The First Affiliated Hospital of Jinan University, Guangzhou, People’s Republic of China, Email [email protected]
Purpose: To develop a prediction model for hypoglycemia in type 2 diabetes mellitus (T2DM) patients treated with an insulin pump during enteral nutrition.
Methods: This retrospective study included T2DM patients treated with an insulin pump during enteral nutrition at the First Affiliated Hospital of Jinan University, Guangzhou Red Cross Hospital, Foshan First People’s Hospital, and Guangdong Provincial Hospital of Traditional Chinese Medicine between January 2016 and December 2023. The patients were randomized 3:1 to the training and validation sets. The risk factors for hypoglycemia were analyzed. A prediction model was developed.
Results: This study included 122 patients, and 57 patients had at least one hypoglycemic event during their hospitalization (46.72%). The multivariable logistic regression analysis showed that the time to reach the glycemic targets (odds ratio (OR)=1.408, 95% confidence interval (CI)=1.084– 1.825, P=0.006), average glycemia (OR=0.387, 95% CI=0.233– 0.643, P=0.010), coronary heart disease (OR=0.089, 95% CI=0.016– 0.497, P< 0.001), and the administration of hormone therapy (OR=6.807, 95% CI=1.128– 41.081, P=0.037) were independently associated with hypoglycemia. A nomogram was built. The receiver operating characteristics analysis showed that the area under the curve of the model was 0.872 (95% CI=0.0.803– 0.940) for the training set and 0.839 (95% CI=0.688– 0.991) in the validation set.
Conclusion: A nomogram was successfully built to predict hypoglycemia in T2DM patients treated with an insulin pump during enteral nutrition, based on the time to reach the glycemic targets, average glycemia, coronary heart disease, and the administration of hormone therapy.
Keywords: T2DM, hypoglycemia, enteral nutrition, insulin pump therapy, nomograms
Introduction
Diabetes mellitus is a prevalent chronic condition that results in significant disruptions in nutrient metabolism, giving rise to various severe complications.1 For patients who are unable to consume nutrients orally but have a functioning gastrointestinal tract, enteral nutrition is the recommended method for providing nutritional support.2 Enteral feeds are commonly prescribed for critically ill patients to provide nutritional support, and this approach is associated with improved mortality and morbidity outcomes.3 However, it is important to note that the provision of carbohydrates in enteral feeds can lead to increased blood glucose excursion and variability.3 Hyperglycemia is a common complication observed in hospitalized patients receiving enteral nutrition, and it affects approximately 21–30% of critically ill patients receiving this form of nutritional support.4–6 The development of hyperglycemia during enteral nutrition is associated with elevated risks of death and infectious complications.4 Among patients with diabetes, the presence of hyperglycemia may have negative effects on wound healing, prolong hospitalization, and increase the risk of complications (eg, diabetic ketoacidosis).7 Therefore, it is important to achieve satisfactory glycemic control during enteral nutrition in patients with diabetes.
Insulin therapy is the preferred regimen for glycemic control in all hospitalized hyperglycemic patients.8 Insulin pump therapy provides flexible diabetic management and has gained popularity among patients with type 1 or 2 diabetes.9 It allows for the customization of basal insulin delivery to meet the individual’s daily insulin requirements and to accommodate variations in insulin needs throughout the day, including circadian patterns.9 Insulin pump therapy is linked to enhanced glycemic control compared with conventional therapy involving multiple daily injections.10 Therefore, it is mainly used in hospitalized patients requiring short-term intensive insulin therapy.11 Hypoglycemia is the most common side effect of insulin therapy and the risk of severe hypoglycemia increases in diabetic patients with tight glucose control.12 It may lead to seizures, unconsciousness, or even death.13 Hypoglycemia is also a crucial indicator used to assess glycemic control. Therefore, it is essential to prevent hypoglycemia in diabetic patients concurrently undergoing enteral nutrition and insulin pump therapy.
Previous studies have identified several risk factors for inpatient hypoglycemia during insulin pump therapy, including female sex, advanced age, impaired renal function, elevated glycosylated hemoglobin (HbA1c) level, higher daily insulin dose, specific insulin regimen, and longer length of stay in the intensive care unit.14–16 Furthermore, few prediction models for hypoglycemia have been developed among outpatient and inpatient individuals.17,18 Although diabetic patients receiving insulin pump therapy are more prone to hypoglycemia during treatment, there is currently a lack of research on prediction models for hypoglycemia during enteral nutrition in this population. Developing such a model could greatly improve the identification and prevention of hypoglycemia in this vulnerable group.
This study aimed to develop a prediction model for hypoglycemia in T2DM patients treated with an insulin pump during enteral nutrition. The prediction model could be advantageous for alleviating hypoglycemia in such patients.
Methods
Study Design and Patients
This retrospective study included T2DM patients who received enteral nutrition between January 2016 and December 2023 at the First Affiliated Hospital of Jinan University (Guangzhou, China), Guangzhou Red Cross Hospital, Foshan First People’s Hospital, and Guangdong Provincial Hospital of Traditional Chinese Medicine. The inclusion criteria were 1) patients who underwent insulin pump therapy during hospitalization,19 2) patients in relatively stable conditions and without systemic edema, and 3) patients who met the relevant criteria of the Chinese Guidelines for the Prevention and Treatment of Type 2 Diabetes Mellitus (2020 Edition).20 The exclusion criteria were 1) patients who underwent gastrointestinal surgery, 2) patients with other gastrointestinal disorders causing dyspepsia, 3) critically ill patients with hemodynamic instability, 4) patients requiring mechanical ventilation, or 5) patients who experienced hypoglycemia before insulin administration. The Ethics Committee of the First Affiliated Hospital of Jilin University approved this study. Patient consent to review their medical charts was not required by the ethics committee because of the retrospective nature of the study. The study was conducted following the tenets of the Declaration of Helsinki (and its amendments) and the Good Clinical Practices. All means were taken to ensure data confidentiality and security.
Data Collection and Definition
The clinical data of the eligible patients were retrieved from the electronic medical record system and retrospectively analyzed.
The following demographic and medical data were collected: general information, blood routine examination, blood biochemistry, complications of T2DM (presence of diabetic nephropathy, hypertension, coronary artery disease, pulmonary infection, cerebral disease, anemia, hypoproteinemia, urinary system infection, gastrointestinal hemorrhage, hepatic insufficiency, and infectious shock), number of days on insulin pump therapy, nasal feeding-related factors (speed of nasal feeding, type of enteral nutrition solution, total amount of nasal feeding, route of infusion, etc.), treatment-related factors (presence of fever, use of antibiotics, hormone therapy, gastrointestinal excitomotor drugs, surgical history, and parenteral nutrition usage were recorded), fingertip blood glucose monitoring data (blood glucose level, number of episodes of hypoglycemia, and the time at which these episodes occurred), and enteral nutrition support. The patients were assessed for nutritional risk using the 2002 Nutritional Risk Screening Scale, and a total score ≥3 points indicated that the patient was at risk of malnutrition or already malnourished.8,21
Hypoglycemia was defined as a blood glucose level ≤3.9 mmol/L or patients with symptoms of hypoglycemia, such as cold sweat, fluster, and dizziness.22 Nocturnal hypoglycemia was defined as hypoglycemia occurring between 0:00 am and 6:00 am. The grading of hypoglycemia was as follows.23 Grade 1 hypoglycemia: blood glucose level <3.9 and ≥3.0 mmol/L, with or without hypoglycemic symptoms. Grade 2 hypoglycemia: blood glucose level <3.0 mmol/L with or without symptoms of hypoglycemia. Grade 3 hypoglycemia: consciousness and/or somatic changes that require medication assistance. There is no specific blood glucose level threshold for grade 3 hypoglycemia, while blood glucose level should be <3.9 mmol/L.
Statistical Analysis
Statistical analysis was conducted using SPSS 25.0 and R language 4.0.2. All continuous variables were tested for normality using the Kolmogorov–Smirnov (KS) test, and all continuous data were non-normally distributed. The continuous variables were presented as means (standard deviations). The categorical variables were presented as n (%). The Wilcoxon rank-sum test was used for the continuous data, while the chi-squared test was used for the categorical data. In order to screen for risk factors for hypoglycemia in nasogastric feeding patients undergoing continuous insulin pump therapy, variables with P-values ≤0.2 in the univariable analyses were included in the multivariable logistic regression analysis. The original dataset was divided into a training set and a validation set in a 3:1 ratio. The model was built using the training set, while the model was validated using the validation set. A column chart was plotted to visualize the factors that are influencing the risk of hypoglycemia in nasal-feeding patients receiving continuous insulin pump treatment. The model was also identified and corrected through receiver operating characteristic (ROC) curves and calibration curves. Ac decision curve analysis (DCA) was used to evaluate the clinical value of predictive models. A decision curve analysis was performed to determine the clinical usefulness of the column chart by quantitatively verifying the net benefits of different threshold probabilities in the dataset. A P-value of <0.05 was considered to indicate a statistically significant difference.
Results
A total of 122 diabetic patients receiving enteral nutrition and insulin pump therapy were included in this study. Among them, 57 (46.72%) patients experienced hypoglycemia. There were statistically significant differences between the non-hypoglycemic group (n=57) and the hypoglycemic group (n=65) in terms of duration of insulin pump usage (P=0.007), the time to reach the glycemic targets (P=0.004), average glycemia (P<0.001), energy (P=0.044), coronary heart disease (P=0.023), and use of hormones (P=0.006), while the other variables were not (Table 1).
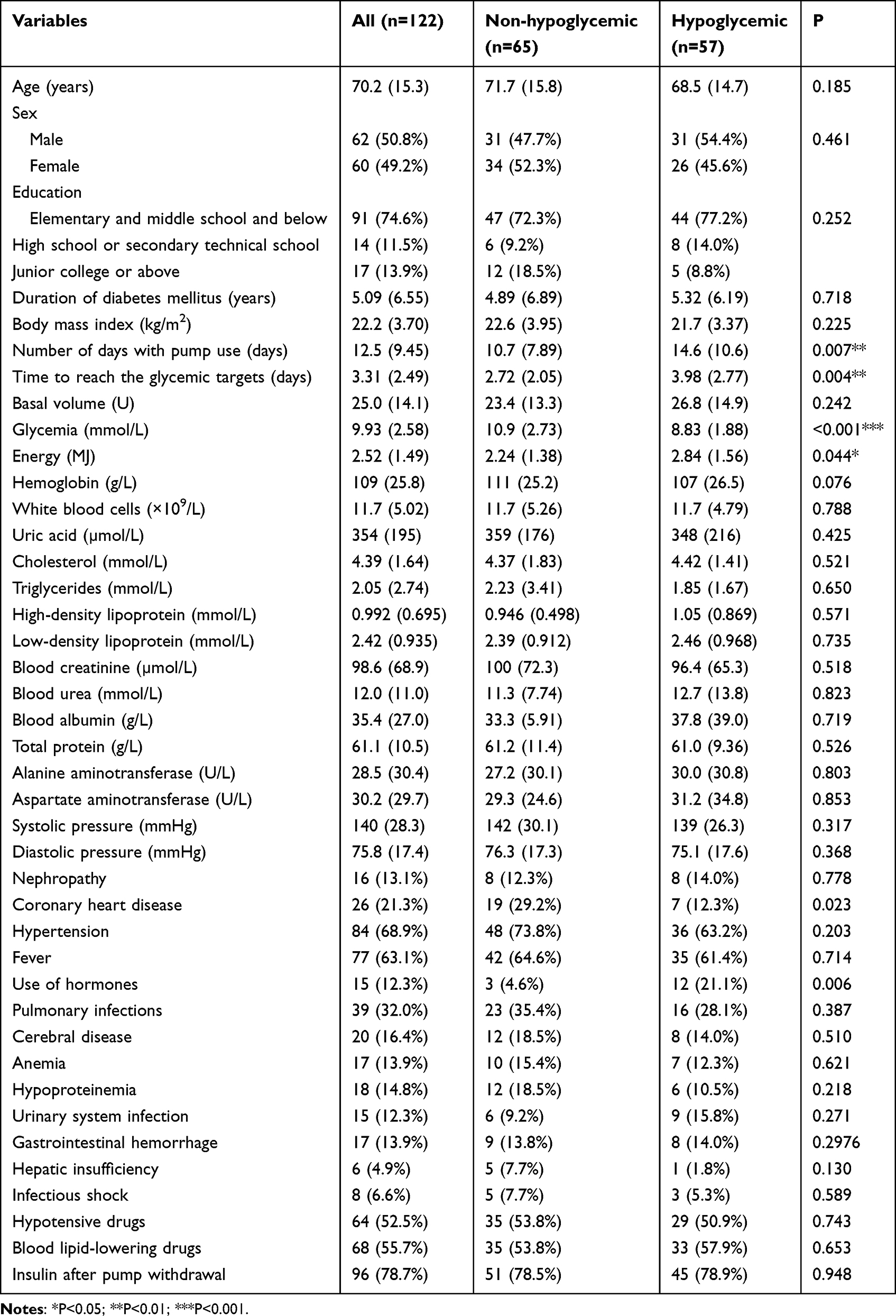 |
Table 1 Demographic and Clinical Characteristics |
The multivariable logistic regression analysis showed that the time to reach the glycemic targets (odds ratio (OR)=1.408, 95% confidence interval (CI)=1.084–1.825, P=0.006), average glycemia (OR=0.387, 95% CI=0.233–0.643, P=0.010), coronary heart disease (OR=0.089, 95% CI=0.016–0.497, P<0.001), and the administration of hormone therapy (OR=6.807, 95% CI=1.128–41.081, P=0.037) were independently associated with hypoglycemia (Table 2).
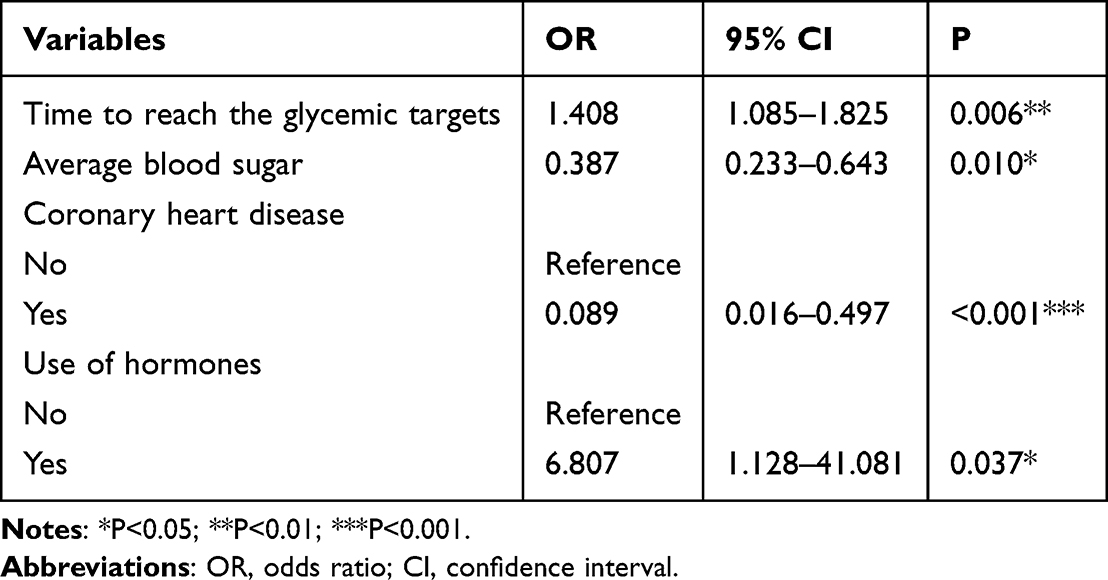 |
Table 2 Multivariable Logistic Regression Analysis |
The results of the multivariable analysis were used to build a nomogram (Figure 1). The ROC analysis showed that the area under the curve (AUC) of the model was 0.872 (95% CI=0.0.803–0.940) for the training set and 0.839 (95% CI=0.688–0.991) in the validation set (Figure 2). The calibration curve showed that the predicted and actual curves were basically superposed in the two sets (Figure 3). The decision curve analysis showed that the net benefit decreased with the increasing high-risk threshold (Figure 4).
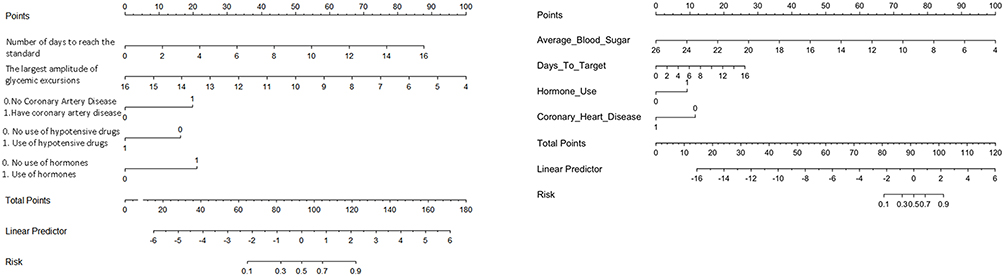 |
Figure 1 Nomogram of the diagnostic model. |
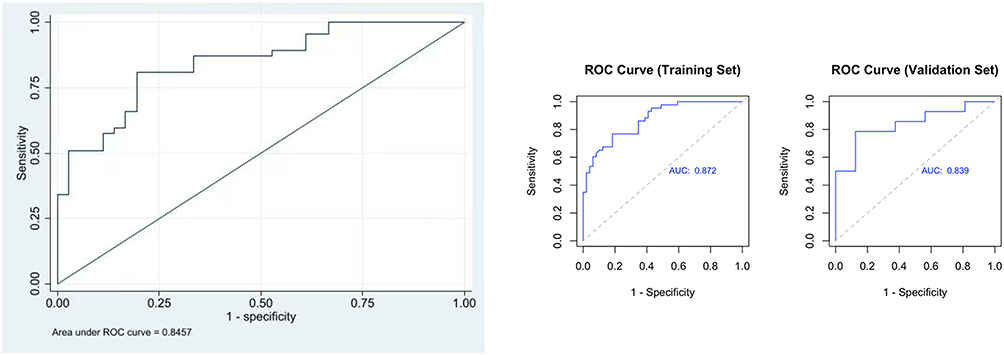 |
Figure 2 Receiver operating curve of the training set (0.872 (95% CI: 0.803–0.940)) and validation set (0.839 (95% CI: 0.688–0.991)). |
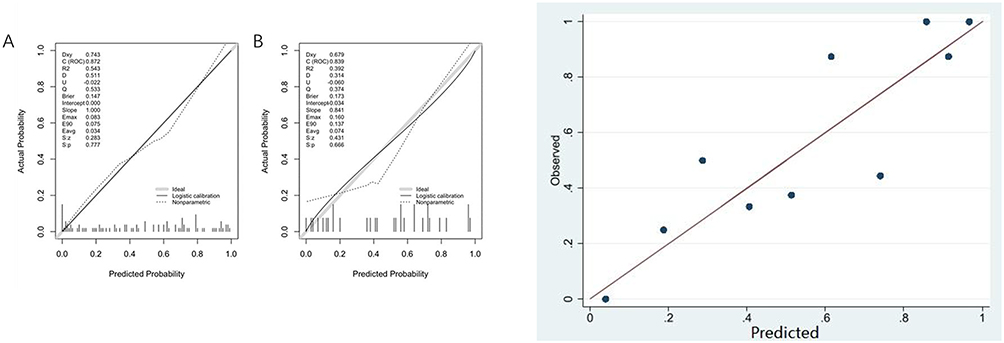 |
Figure 3 Calibration curve of the diagnostic model, (A) Training set; (B) Validation set. |
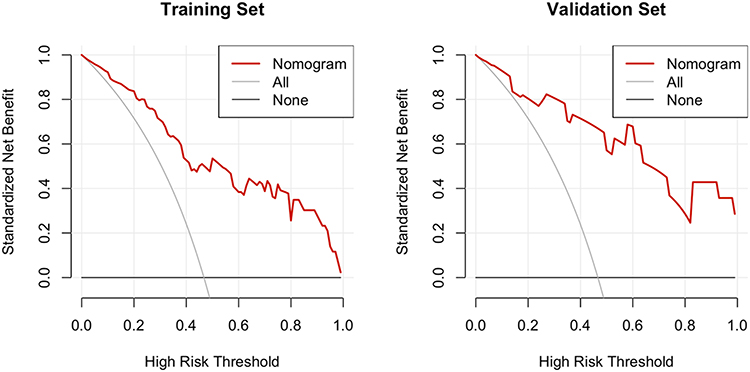 |
Figure 4 Decision curve analysis. |
Discussion
This study suggests a nomogram to predict hypoglycemia in T2DM patients treated with an insulin pump during enteral nutrition, based on the time to reach the glycemic targets, average glycemia, coronary heart disease, and the administration of hormone therapy.
Previous studies have reported that the prevalence of hypoglycemia in patients treated with insulin pump therapy was 5%-31%.14,16 In the present study, the incidence rate was observed to be higher due to several factors affecting the glycemic management of patients receiving enteral nutrition. These factors included administration of hormone therapy, glycogen replenishment, and interruption of enteral nutrition. They contributed to more significant fluctuations in blood glucose levels.24 Therefore, these patients are more prone to hypoglycemia during their hospitalization. Nonetheless, mild cases underwent blood glucose monitoring every 2–3 h to enable early detection and prevent the occurrence of severe hypoglycemic events.
The risk of acute coronary syndrome increases after a hypoglycemia event.25 In addition, patients with coronary heart disease are at increased risk of acute coronary syndrome.26 Patients with coronary artery disease can suffer from arrhythmias and myocardial ischemia during a hypoglycemia event.27 Nevertheless, glycemic control is necessary to avoid the micro- and macrovascular complications of T2DM.28,29 Therefore, in the ICU, particular care is taken by the healthcare providers to avoid any hypoglycemic event in patients with coronary heart disease through more frequent or even continuous blood glucose monitoring to be able to react promptly in the presence of any decrease in blood glucose levels, or even by temporarily setting the blood glucose targets at higher levels. It could explain the negative association observed between coronary heart disease and hypoglycemia in the present study.
One of the risk factors for hypoglycemia was the administration of hormone therapy. Hormone therapy is associated with a significant increase in insulin sensitivity, which may lead to hypoglycemia during intensive insulin therapy.30 In postmenopausal women with T2DM, HbA1c level significantly decreased after 3 months of oral estradiol therapy.30 However, the precise mechanisms underlying the effects of hormone therapy on insulin action in humans have not yet been fully explored. The levels of blood glucose and other biomarkers (eg, HbA1c) should be closely monitored in diabetic patients receiving hormone therapy while concurrently undergoing insulin pump therapy and enteral nutrition. The basal rate of the insulin pump should be appropriately adjusted or temporarily discontinued as needed to prevent hypoglycemia.
The time to reach glycemic targets was significantly associated with the risk of hypoglycemia. Achieving glycemic targets may pose challenges for patients requiring prolonged treatment. Physicians should be cautious in avoiding hypoglycemia and should not aggressively pursue HbA1C reduction.31 Severe hypoglycemia occurred more frequently in patients who underwent intensive glycemic control.31 Regular monitoring of blood glucose levels and making appropriate adjustments to treatment plans, including the consideration of higher glycemic goals, are necessary for patients who require a longer period of time to achieve their glycemic targets.
Notably, the present study revealed an inverse association between average glycemic and the risk of hypoglycemia, indicating that high glucose levels are protective against hypoglycemic events. Previous studies showed that high HbA1c levels were also associated with a lower risk of hypoglycemia.32
This study has several limitations. Firstly, the sample size was relatively small (n=122). Secondly, subjects included in this study were patients with T2DM who were treated with enteral nutrition and insulin pump therapy. Thus, the findings might not be applicable to all diabetic patients. Thirdly, patients with unstable medical conditions who might require treatment for hypoglycemia were excluded. Thus, further large-scale multicenter study is required to eliminate the above-mentioned limitations and to verify the findings of this study.
Conclusions
In conclusion, this study suggests a nomogram to predict hypoglycemia in T2DM patients treated with an insulin pump during enteral nutrition, based on the time to reach the glycemic targets, average glycemia, coronary heart disease, and the administration of hormone therapy. Using this prediction model, clinicians could proactively identify high-risk patients and provide them with the necessary medical attention and intensified blood glucose monitoring.
Funding
The cultivation project of Nursing School from Jinan University (JHA20230604) ; This study was funded by the Nurse Association of Guangdong Province (gdshsxh2023ms15).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Charney P, Hertzler SR. Management of blood glucose and diabetes in the critically ill patient receiving enteral feeding. Nutr Clin Pract. 2004;19(2):129–136. doi:10.1177/0115426504019002129
2. Park R, Hansell D, Davidson L, et al. Management of diabetic patients requiring nutritional support. Nutrition. 1992;8(5):316–320.
3. Eckert I, Kumbier MCC, Silva FM, Franzosi OS, de Almeida JC. Association of specialized enteral nutrition with glycemic control and clinical outcomes in critically ill patients: a meta-analysis of randomized controlled trials. Clin Nutr. 2021;40(6):3940–3949. doi:10.1016/j.clnu.2021.04.030
4. Gosmanov AR, Umpierrez GE. Management of hyperglycemia during enteral and parenteral nutrition therapy. Curr Diab Rep. 2013;13(1):155–162. doi:10.1007/s11892-012-0335-y
5. Li Y, Ren S, Wang Y, Niu Z, Zhao H. Clinical study of enhancing the delivery of enteral nutrition in critically ill patients. Chin J Crit Care Med. 2018;38(2):145–148.
6. Zhang S, Pang X, Wan X, Lin H, Wang F. Investigation and analysis of factors related to hyperglycemia in ICU patients undergoing enteral nutrition. Chin J Nurs. 2019;54(9):1349–1353.
7. Ojo O, Brooke J. Evaluation of the role of enteral nutrition in managing patients with diabetes: a systematic review. Nutrients. 2014;6(11):5142–5152. doi:10.3390/nu6115142
8. Li Y, Teng D, Shi X, et al. Prevalence of diabetes recorded in mainland China using 2018 diagnostic criteria from the American diabetes association: national cross sectional study. BMJ. 2020;369(m997). doi:10.1136/bmj.m997
9. Nimri R, Nir J, Phillip M. Insulin pump therapy. Am J Ther. 2020;27(1):e30–e41. doi:10.1097/MJT.0000000000001097
10. Weissberg-Benchell J, Antisdel-Lomaglio J, Seshadri R. Insulin pump therapy: a meta-analysis. Diabetes Care. 2003;26(4):1079–1087. doi:10.2337/diacare.26.4.1079
11. Zhou Y, Zhou P, Lu X. Multidisciplinary collaboration for in-hospital glucose management in patients with diabetes mellitus and multiple acute and critical illnesses. J Nurs Train. 2020;35(10):924–928.
12. McCall AL. Insulin therapy and hypoglycemia. Endocrinol Metab Clin North Am. 2012;41(1):57–87. doi:10.1016/j.ecl.2012.03.001
13. Steineck I, Ranjan A, Nørgaard K, Schmidt S. Sensor-augmented insulin pumps and hypoglycemia prevention in type 1 diabetes. J Diabetes Sci Technol. 2017;11(1):50–58. doi:10.1177/1932296816672689
14. Farrokhi F, Klindukhova O, Chandra P, et al. Risk Factors for Inpatient Hypoglycemia During Subcutaneous Insulin Therapy in Non-Critically Ill Patients with Type 2 Diabetes. SAGE Publications; 2012.
15. Mahmoodpoor A, Hamishehkar H, Beigmohammadi M, et al. Predisposing factors for hypoglycemia and its relation with mortality in critically ill patients undergoing insulin therapy in an intensive care unit. Anesth Pain Med. 2016;6(1). doi:10.5812/aapm.33849
16. Arabi YM, Tamim HM, Rishu AH. Hypoglycemia with intensive insulin therapy in critically ill patients: predisposing factors and association with mortality. Crit Care Med. 2009;37(9):2536–2544. doi:10.1097/CCM.0b013e3181a381ad
17. Nestoras Nicolas M, Estelle E, Shuvodra R, et al. Development and validation of a prediction model for insulin-associated hypoglycemia in non-critically ill hospitalized adults. BMJ Open Diabetes Res Care. 2018;6(1):e000499. doi:10.1136/bmjdrc-2017-000499
18. Li X, Yu S, Zhang Z, et al. Predictive modeling of hypoglycemia for clinical decision support in evaluating outpatients with diabetes mellitus. Curr Med Res Opin. 2019;35(11):1885–1891. doi:10.1080/03007995.2019.1636016
19. Chinese Medical Association Division of Diabetes Mellitus. Guidelines for clinical application of glucose monitoring in China (2015 edition). Diabetic Ground. 2016;10(5):205–218.
20. Chinese Medical Association Diabetes Society. Guidelines for the prevention and treatment of type 2 diabetes mellitus in China (2020 Edition). Int J Endocrinol Metab. 2021;41(5):482–548.
21. Yu D. Analysis of Nutritional Support Status of Critically Ill Patients in Shengjing Hospital, Affiliated to China Medical University. China Medical University; 2022.
22. Morales J, Schneider D. Hypoglycemia. Am j Med. 2014;127(10):S17–S24. doi:10.1016/j.amjmed.2014.07.004
23. American Diabetes Association. Improving care and promoting health in populations: standards of medical care in diabetes — 2020. Diabetes Care. 2020;43(Supplement_1):S7–S13. doi:10.2337/dc20-S001
24. Sarfo-Adu BN, Hendley JL, Pick B, Oyibo SO. Glycemic control during enteral tube feeding in patients with diabetes mellitus. Cureus. 2019;11(1):e3929. doi:10.7759/cureus.3929
25. Nishioka Y, Okada S, Noda T, et al. Absolute risk of acute coronary syndrome after severe hypoglycemia: a population-based 2-year cohort study using the national database in Japan. J Diabetes Investig. 2020;11(2):426–434. doi:10.1111/jdi.13153
26. Sanchis-Gomar F, Perez-Quilis C, Leischik R, Lucia A. Epidemiology of coronary heart disease and acute coronary syndrome. Ann Transl Med. 2016;4(13):256. doi:10.21037/atm.2016.06.33
27. Snell-Bergeon JK, Wadwa RP. Hypoglycemia, diabetes, and cardiovascular disease. Diabetes Technol Ther. 2012;14(Suppl 1):S51–58. doi:10.1089/dia.2012.0031
28. Goldfine AB, Phua EJ, Abrahamson MJ. Glycemic management in patients with coronary artery disease and prediabetes or type 2 diabetes mellitus. Circulation. 2014;129(24):2567–2573. doi:10.1161/CIRCULATIONAHA.113.006634
29. Chen J, Yin D, Dou K. Intensified glycemic control by HbA1c for patients with coronary heart disease and Type 2 diabetes: a review of findings and conclusions. Cardiovasc Diabetol. 2023;22(1):146. doi:10.1186/s12933-023-01875-8
30. Bitoska I, Krstevska B, Milenkovic T, et al. Effects of hormone replacement therapy on insulin resistance in postmenopausal diabetic women. Open Access Maced J Med Sci. 2016;4(1):83–88. doi:10.3889/oamjms.2016.024
31. American Diabetes Association Professional Practice Committee. Glycemic targets: standards of medical care in diabetes—2022. Diabetes Care. 2021;45(Supplement_1):S83–S96. doi:10.2337/dc22-S006
32. Karges B, Rosenbauer J, Kapellen T, et al. Hemoglobin A1c Levels and risk of severe hypoglycemia in children and young adults with type 1 diabetes from Germany and Austria: a trend analysis in a cohort of 37,539 patients between 1995 and 2012. PLoS Med. 2014;11(10):e1001742. doi:10.1371/journal.pmed.1001742
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.