Back to Journals » Infection and Drug Resistance » Volume 15
Nomogram Analysis of Clinical Characteristics and Mortality Risk Factor of Non-Fermentative Gram-Negative Bacteria-Induced Post-Neurosurgical Meningitis
Authors Zheng G, Wang S, Lv H, Zhang G
Received 16 August 2022
Accepted for publication 15 October 2022
Published 1 November 2022 Volume 2022:15 Pages 6379—6389
DOI https://doi.org/10.2147/IDR.S385502
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Guanghui Zheng,1– 3 Siqi Wang,4 Hong Lv,1– 3 Guojun Zhang1– 3
1Laboratory of Beijing Tiantan Hospital, Capital Medical University, Beijing, 100076, People’s Republic of China; 2NMPA Key Laboratory for Quality Control of in vitro Diagnostics, Beijing, 100076, People’s Republic of China; 3Beijing Engineering Research Center of Immunological Reagents Clinical Research, Beijing, 100076, People’s Republic of China; 4School of clinical laboratory diagnostics, Capital Medical University, Beijing, 100076, People’s Republic of China
Correspondence: Guojun Zhang, Laboratory of Beijing Tiantan Hospital, Capital Medical University, NO. 119 Nansihuan West Road, Fengtai District, Beijing, People’s Republic of China, Tel +86 15811219411, Email [email protected]
Objective: To explore the clinical characteristics of post-neurosurgical meningitis (PNM) patients infected with nonfermenting Gram-negative bacilli (NFGNB) and to evaluate the related mortality risk factors.
Methods: A cohort analysis of PNM patients infected with NFGNB in Beijing Tiantan Hospital and Capital Medical University from 2012.1 to 2020.12. The microbial distribution, antimicrobial sensitivity and genotypes were tested, and potential mortality risk factors were evaluated using Mann–Whitney U or chi-squared tests. Independent risk factors for mortality were established by constructing a logistic model.
Results: A total of 2940 PNM patients were enrolled in this study, of whom 207 (17.1%) were infected with NFGNB. Among these patients, 29 died of NFGNB meningitis, with an overall mortality rate of 14.0%. The top three NFGNBs were Acinetobacter baumannii (105 cases, 50.7%), Pseudomonas aeruginosa (29 cases, 14.0%) and Acinetobacter lwoffii (20 cases, 9.7%). Nomogram analysis revealed that hypertension (OR 4.551, 95% CI: 1.464– 14.154, P = 0.009), external ventricular drainage (EVD) (OR 3.944, 95% CI: 1.286– 12.095, P = 0.016), and assisted mechanical ventilator (AMV) (OR 6.192, 95% CI: 1.737– 22.081, P = 0.005) were independent risk factors for mortality. In addition, antibiotic prophylaxis was shown to play a vital role in NFGNB-induced PNM therapy.
Conclusion: PNM patients infected with NFGNB have a high mortality rate. Hypertension, EVD and AMV were independent mortality risk factors, and clinical attention should be paid to their prevention and treatment.
Keywords: clinical characteristics, nomogram analysis, meningitis, mortality, nonfermenting Gram-negative bacilli
Introduction
Post-neurosurgical meningitis (PNM) is one of the most common complications in neurosurgical patients, followed by neurosurgery itself, trauma or shunt devices. It is closely related to perioperative morbidity and mortality, with an incidence of 0.7–25%.1–3 Patients undergoing neurosurgery often have immune deficiency due to ecomplex and lengthy neurosurgical procedures, leading to PNM treatment challenges.4 Therefore, reducing the incidence of PNM and patient mortality is one of the vital tasks associated with neurosurgery.
The etiology of PNM has shown that a wide spectrum of pathogens can be responsible, including bacteria, fungi, Cryptococcus, and so on. Of these, during the last decade, nonfermenting Gram-negative bacilli (NFGNB) have exhibited a trend towards antibiotic resistance and pathogenicity. These pathogens cannot utilize glucose through fermentation, and include Acinetobacter, Pseudomonas, Flavobacterium, Burkholderia, etc.5 With higher antibiotic resistance and pathogenicity characteristics, NFGNB are perhaps the main types of pathogens causing nosocomial infections.6,7 In 2017, the World Health Organization (WHO) released a list of bacteria that pose the greatest threat to human health, with carbapenem-resistant Acinetobacter baumannii and carbapenem-resistant Pseudomonas aeruginosa in the top two rankings (critical), seriously affecting the clinical therapy.8
Therefore, we carried out a longitude clinical cohort study in the largest neurosurgery center in China from 2012 to 2020 with the main specific objective of this study is to explore the clinical characteristics of PNM patients infected with NFGNB and to evaluate the related mortality risk factors. Based on the results, neurosurgical surgeons can better accurately prevent or therapeutically target PNM induced by NFGNB. As far as we are aware, this is the first cohort study globally to analyze the clinical characteristics and mortality risk factors for PNM induced by NFGNB.
Methods and Materials
Study Design
This study was conducted in Beijing Tiantan Hospital & Capital Medical University. The clinical characteristics of PNM patients from January 2012 to December 2020 were analyzed to evaluate the mortality risk factors. The microbial distribution, drug resistance spectrum, genotypes were also analyzed for epidemiology. Neurosurgery including craniotomy, transsphenoidal surgery and spinal surgery were also investigated. The study was approved by the Ethical Committees of Beijing Tiantan Hospital & Capital Medical University (Approval number: KY-2021-079-02). Each patient enrolled in the study signed an informed consent form.
Inclusion and Exclusion Criteria
The PNM patients included in this study were followed-up for 90 days, and the inclusion criteria were implement as reported in a previous study,3 briefly: 1) adult patients (>18 years); 2) patients survived for ≥7 days; 3) had a NFGNB infection with at least one cerebrospinal fluid (CSF) culture.
Exclusion criteria9 were patients 1) who had undergone EVD, CSF shunt or stereotaxic surgery; 2) had common clinical contamination bacteria (Coagulase-negative Staphylococcus, Bacillus, Propionibacterium, etc) but without infectious symptoms; 3) who died within 7 days; and 4) without anti-infective treatment in hospital and/or incomplete clinical records.
Diagnosis Criteria
The definition of NFGNB-induced PNM defined by the US Centers for Disease Control and Prevention (CDC) criteria was followed.10 Patients with a diagnosis of NFGNB-induced PNM who were included in the study presented with at least one kind of NFGNB proliferation in the cerebrospinal fluid (CSF) or at least one of the signs of meningeal irritation (headache, neck stiffness, or cranial nerve involvement for no other reason). These patients also displayed at least one of the following features: 1) increased protein and/or decreased glucose levels in the CSF; 2) an increased neutrophil count; 3) a positive CSF Gram stain; and 4) a positive blood culture or positive antigen test in the blood or CSF, or an increased antibody titer against the pathogen.
Microbiology
NFGNBs, isolated from the PNM patients’ CSF, underwent bacteria culture, identification, antimicrobial susceptibility tests (ASTs), and genotyping for resistance screening. All the target patient CSF samples underwent a standard procedure for bacterial culture, with 1–3 mL infused into an aerobic automated culture bottle (bioMerieux, Marcy l’Etoile, France). Then, the bottles containing patients’ CSF were transferred into a BACT/ALERT® 3D automated culture system (bioMerieux, Marcy l’Etoile, France) until the bacteria grew to positive detection levels. Subsequently, 50 μL of broth was sub-cultured into a Columbia sheep blood agar for 24 h until obvious colony growth. Bacteria with NFGNB characteristics were identified using VITEK-2 compact and VITEK MS systems (bioMerieux, Marcy l’Étoile, France). All bacteria identified as NFGNB were chosen for AST, and two methods were selected, namely the disk agar diffusion method (Kirby–Bauer method) and the micro-broth dilution method. The breakpoints of each antibiotic followed the Clinical and Laboratory Standards Institute (CLSI) 2021 guidelines (CLSI, 2021). A total of 17 resistances genes from 5 antibiotics resistance phenotypes were selected for screening. These included meropenem (blaKPC,blaOXA-66,blaOXA-23,blaNDM,blaVIM,blaIMP), ceftriaxone (blaTEM,blaSHV,blaCTX-M-9,blaCMY,blaCTX-M-1), amikacin (aadA1, aaaC1), levofloxacin (qnrA, qnrS) and polymyxin B (mcr-1). The genotypes of target resistance were tested by MNCP-II, a method based by LAMP method which can test 35 different kinds of antibiotic related genes in one panel, and the platform was developed by our research group in 2020.
Risk Factors
In the present study, all of the NFGNB-induced PNM patients’ clinical records were reviewed and the relevant risk factors extracted, including gender, age (years), body temperature (°C), malignant tumor, traumatic brain injury (TBI), diabetes; hypertension, long operation duration (>3 h), reoperation, craniotomy, surgical site (head or spine), type of incision (I or II), ICU admission, CSF leakage, external ventricular drainage (EVD), lumbar drainage (LD), and assisted mechanical ventilation (AMV).
Therapy
In this study, three categories of antibiotics usage composed the whole therapy regimen, including antibiotic prophylaxis (AP), antibiotic empirical therapy (AET) and antibiotic definitive therapy (ADT). The three categories were defined as follows: 1) PNM patients who had AP, received antibiotics 0.5 h ahead of their neurosurgical operation; 2) PNM patients who had AET received antibiotics before the AST result; 3) patients who had ADT received antibiotic therapy by AST guidance. Three other categories of antibiotic choice were defined as follows: 1): mono-antibiotic: only one type of antibiotic was used in the treatment; 2) dual antibiotic: two different types of antibiotics combination in the treatment; 3) triple or more antibiotic: three or more types of antibiotics combination in the treatment. In addition, the usage rate of high-grade antibiotics (third- or fourth-generation cephalosporin or carbapenem) was evaluated.
Statistical Analysis
Categorical data are shown given counts and percentages. Numerical data are presented as the mean ± SD or median with interquartile range (IQR), depending on the degree of skewness in the distributions evaluated using the Kolmogorov–Smirnov (K-S) test. χ² or Fisher’s exact tests and a t-test or Mann–Whitney U-test were used for descriptive statistics to evaluate risk factors, when appropriate. To determine the independent risk factors for mortality caused by NFGNB-induced PNM, any variables with a P-value <0.05 in the univariate analysis were carried forward for inclusion in the logistic regression model. Statistical significance was defined as P < 0.05 and the calibration was analysed with the Hosmer-Lemeshow (H-L) test for goodness-of-fit. Pathogen distribution and AST were performed by WHONET 5.5. Statistical analyses were carried out using SPSS version 22.0 (IBM, New York, USA). Graphs were generated using Prism 7.0 (GraphPad, San Diego, USA).
Results
Patients
Over the 9-year study period, 3344 episodes of patients with CSF culture positive were recorded in Beijing Tiantan Hospital and Capital Medical University. Among them, 188 patients only underwent a CSF shunt, 73 exhibited cultured Corynebacterium or Micrococcus, 37 patients survived for <7 days, 64 had incomplete medical records, and 42 patients had multiple infections. A total of 2940 patients were included in the study, 59.4% (1746/2940) were Gram-positive bacterial PNM, and 40.5% (1194/2949) were Gram-negative PNM. In the Gram-negative group, 207 patients (17.3%) were infected by NFGNB, among all NFGNB-induced PNM patients, 29 died from meningitis and 178 survived, with a mortality rate of 14.0%. The flow chart of the study is shown in Figure 1.
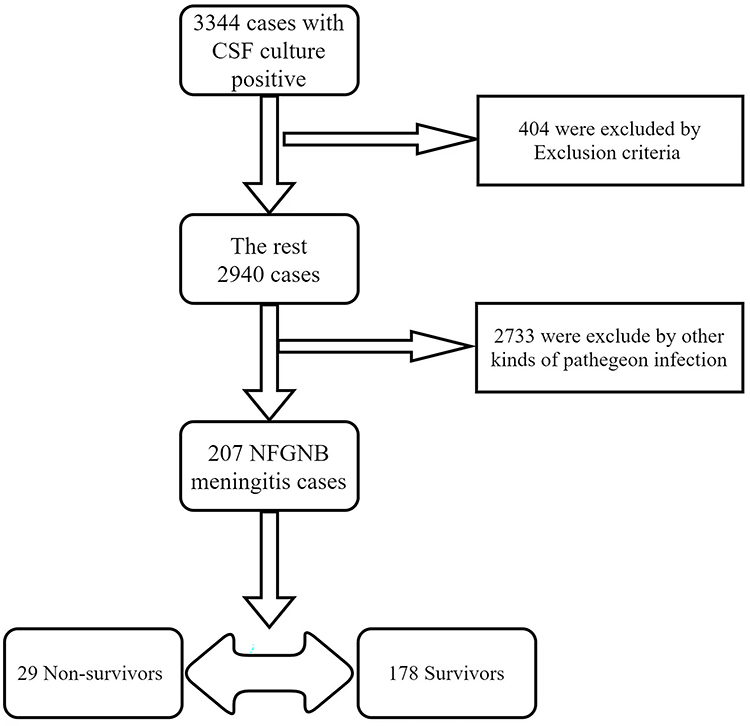 |
Figure 1 Flow chart of the whole study. |
Microbiology Distribution
In 207 NFGNB-induced PNM, A. baumannii (105, 50.7%), P. aeruginosa (29, 14.0%) and Acinetobacter lwoffii (20 cases, 9.7%) occupied the first three classes. The bacterial distribution ratio of patients in the survivors and non-survivor groups was similar; however, the distribution in the non-survivor group was more concentrated, mainly for A. baumannii and P. aeruginosa (Figure 2).
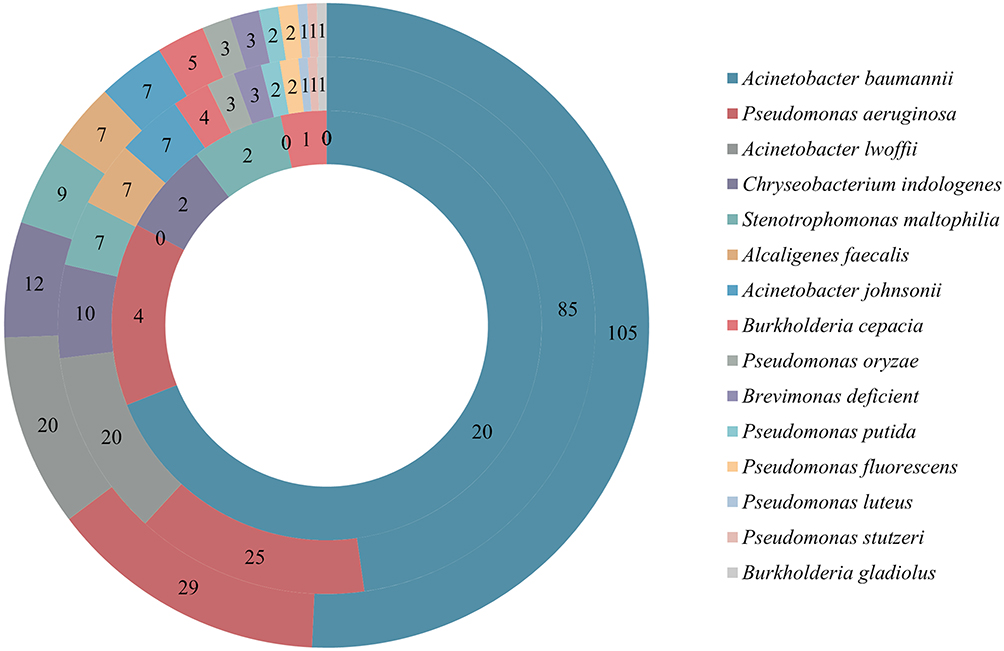 |
Figure 2 Bacterial distribution of NFGNB-induced PNM (Out ring: Distributions of whole NFGNB enrolled in this study; Middle ring: distribution of NFGNB isolated from the survived PNM patients; Inner ring: distribution of NFGNB isolated from the non-survived PNM patients). |
AST
Due to the huge difference in AST of NFGNB, this study conducted statistics on the two types of bacteria (A. baumannii and P. aeruginosa) with the highest ratio. And, 49.5% of A. baumannii were resistance to meropenem, while the resistance rate of P. aeruginosa to imipenem and meropenem was different (31.0% vs 24.1%), respectively. For polymyxin B, resistance of A. baumannii was slightly lower than that of P. aeruginosa, which were 1.0% and 6.9%, respectively. Other AST results are shown in Figure 3.
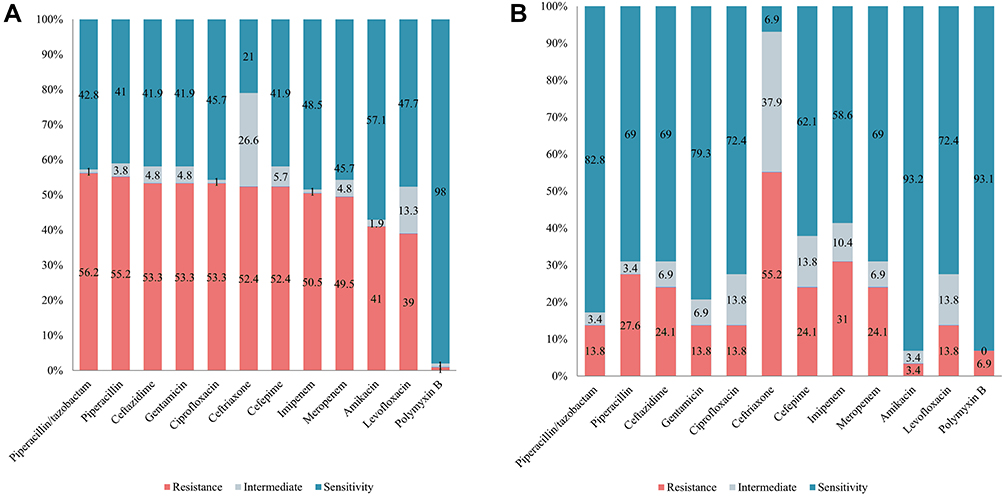 |
Figure 3 AST of A. baumannii (A) and P. aeruginosa (B). |
Genotypes of A. baumannii and P. aeruginosa
The AST genotypes of A. baumannii and P. aeruginosa are shown in Table 1. The carbapenemase genotype blaOXA in A. baumannii had the highest proportion, while ESBL-related enzymes exhibited the highest proportion of blaTEM. For P. aeruginosa, the ratio of blaKPC, ESBL + OMPK was greater, and blaSHV was greater than that of blaTEM. The aminoglycoside resistance gene aada1 accounted for a large proportion. In contrast, the detection rate of aaaC1 and the quinolone genes qnrA and qnrS were low. It is noteworthy that mcr-1 was not detected in A. baumannii and P. aeruginosa at all.
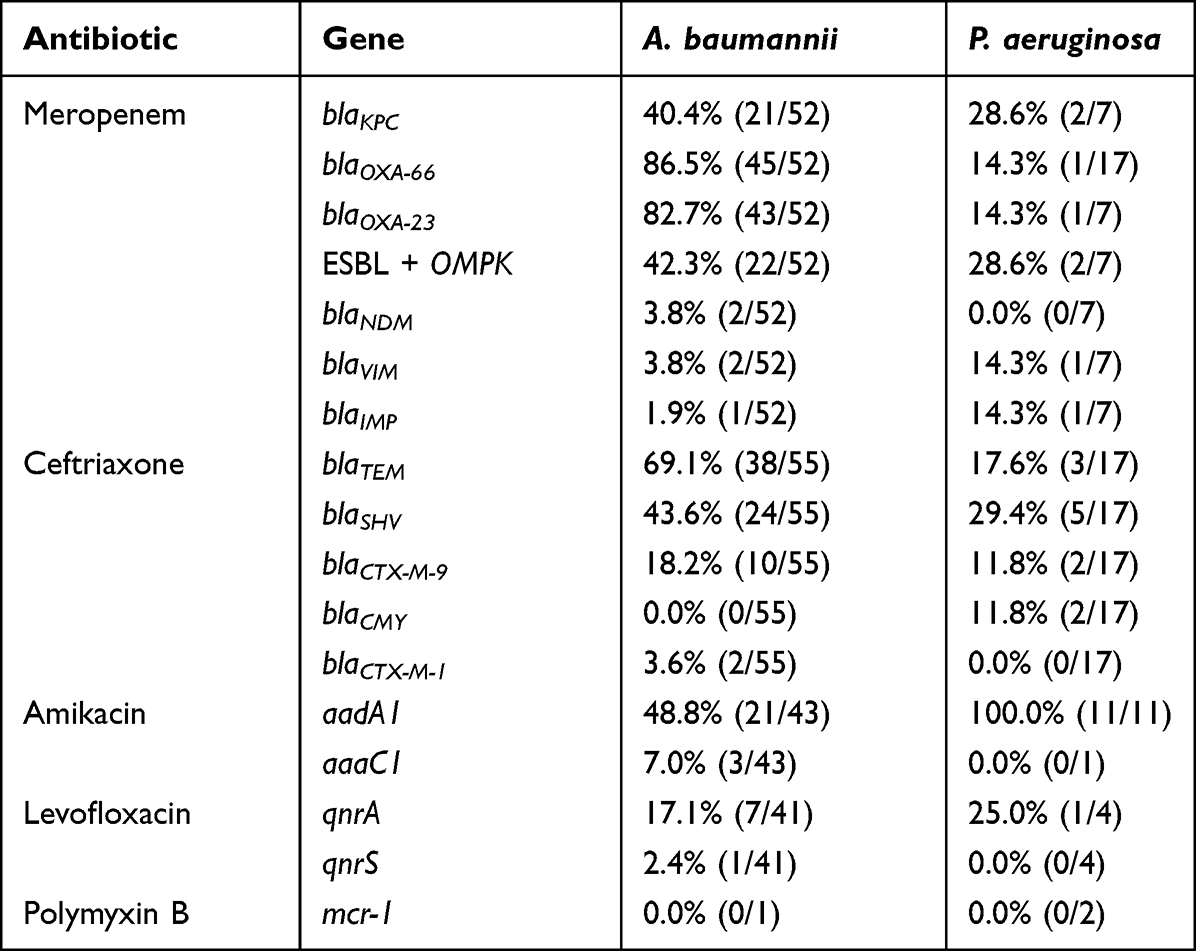 |
Table 1 Distribution of Antibiotic Usage and Gene in A. baumannii and P. aeruginosa |
Univariate Analysis of NFGNB-Induced PNM
Of the 207 patients included in the final analysis (Table 2), their mean age was 36.3 years (SD 14.8). Of the patients, 119 (57.4%) were male and 88 (42.6%) were female, with a primary body temperature of 37.8°C (SD 0.9). Univariate analyses revealed that NFGNB-induced PNM patients with TBI (P = 0.004), hypertension (P = 0.003), ICU admission (P = 0.001), EVD (P < 0.001) and AMV (P < 0.001) were significantly different in the two groups.
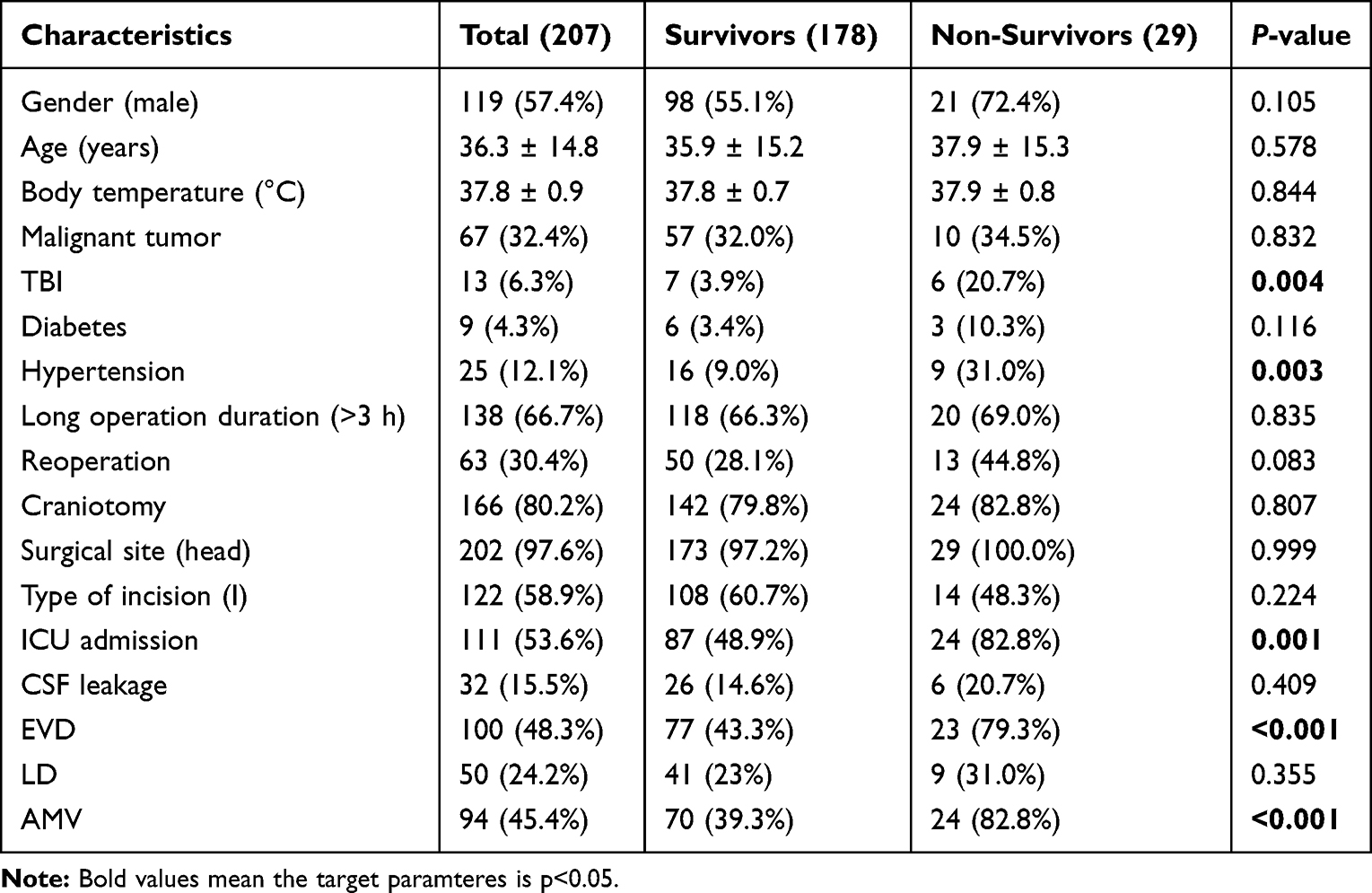 |
Table 2 Univariate Analysis of NFGNB-Induced PNM |
Multivariate Analysis of NFGNB-Induced PNM
A multivariable logistic model was established for the independent risk factors with statistical significance, as shown in Figure 4. The nomogram prediction model is shown in Figure 5 and Supplementary Material (Figures S1 and S2), either. In NFGNB-induced PNM patients, hypertension (HR 4.551, 95% CI: 1.464–14.154, P = 0.009), EVD (HR 3.944, 95% CI: 1.286–12.095, P = 0.016) and AMV (HR 6.192, 95% CI: 1.737–22.081, P = 0.005) were shown to be independent risk factors for mortality. The verification of the model was carried out as ROC and H-L. The AUC of the model was 0.852, and H-L was 0.193 (>0.05) reflecting the fact that the model was of great clinical significance.
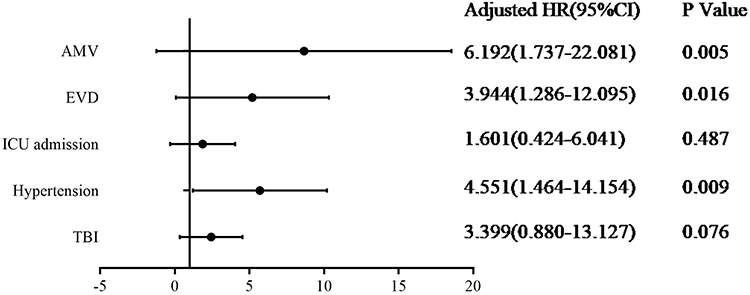 |
Figure 4 Multivariate analysis of NFGNB-induced PNM. |
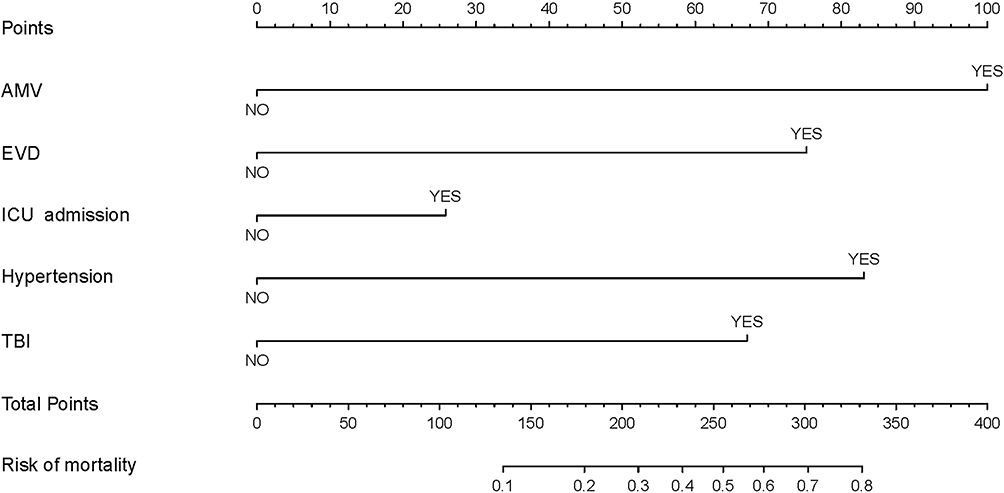 |
Figure 5 Nomogram of the risk of NFGNB-induced PNM mortality. |
Therapy
Of 207 patients, 171(82.6%) received AP, with cefuroxime being the most frequent antibiotic administered. In contrast, 188(90.8%) patients received AET, with high-grade antibiotics usage of 86.7%. A total of 200 patients received ADT, with 90.6% high-grade antibiotics usage. In the present study, between the two groups, a significant difference in the employment of AP was found (P = 0.015), but no difference was detected between AET and ADT. Nevertheless, the use rate of ADT and AET in the triple antibiotics regimens was greater in the non-survivors group (Table 3).
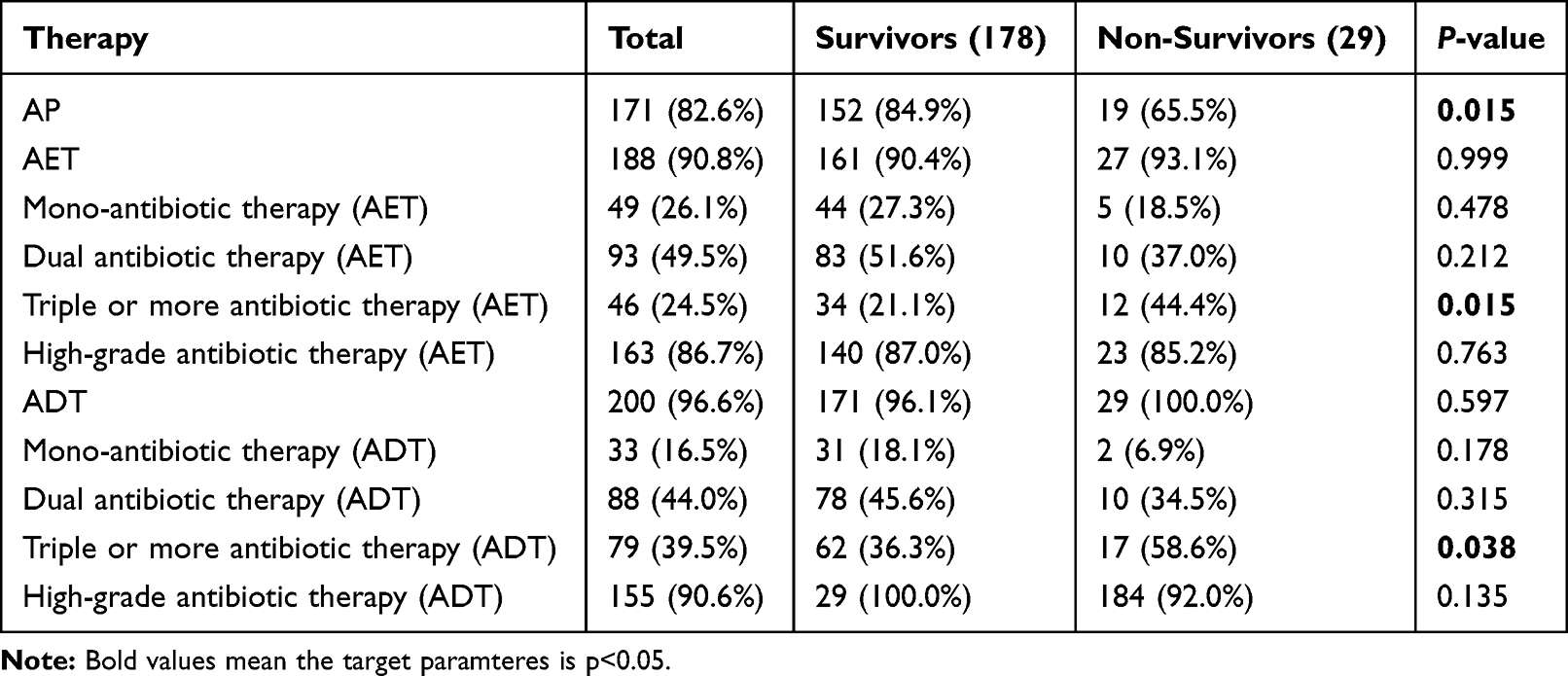 |
Table 3 Therapy of NFGNB-Induced PNM |
Discussion
Our study highlights the fact that NFGNB-induced PNM patients are at risk of treatment failure and poor outcomes. We first investigated the clinical and microbial epidemiology of NFGNB-induced PNM and explored the factors associated with mortality. In the largest neurosurgery center of China, we conducted this cohort study from 2012 to 2020 and found three factors, which were important predictors of NFGNB-induced PNM, namely hypertension, EVD and AMV. The clinical and microbiological epidemiology of PNM caused by NFGNB was analyzed and the risk factors for death evaluated. The findings have great significance for the diagnosis and treatment of PNM and for preventive interventions for the entire meningitis diseases. In addition, the importance of AP is highlighted in NFGNB-induced PNM, and whether patients experience AP or not can lead to completely different clinical outcomes.
NFGNB are one of the most important groups of pathogens that cause clinical infections, due to their similar metabolism (inability to ferment glucose). In previous reports, Staphylococcus aureus, coagulase-negative Staphylococcus, and Enterobacter accounted for a large proportion of pathogens causing PNM.11–13 In the past decade, however, PNM caused by NFGNB, especially A. baumannii and P. aeruginosa has increased year by year with a concomitant increase in drug resistance. According to one report, the carbapenem resistance rate of A. baumannii in intensive care units can be as high as 60–70%,14 and therefore the clinical treatment of patients is extremely difficult. With the widespread use of antibiotics, carbapenem-resistant A. baumannii and carbapenem-resistant P. aeruginosa have become huge clinical threats. In addition, other NFGNB such as Burkholderia cepacia and Stenotrophomonas maltophilia possess extensive natural resistance meaning that fewer antibiotics can be used clinically, which also makes treatment problematic.15,16
From the perspective of the bacterial distribution, the distribution of the entire NFGNB is relatively concentrated, among which A. baumannii and P. aeruginosa account for nearly 65%. In the non-survivor group, the two occupied even more of the spectrum, up to 82.8%. It has been reported that the invasiveness of A. baumannii and P. aeruginosa is higher than that of other NFGNB.17 P. aeruginosa meningitis is much complicated to treat due to the existence of the quorum sensing system and biofilm formation,18 which can induce drug resistance and lead to an increase in mortality. The carbapenem resistance rate of P. aeruginosa can be up to 30%, and the resistance rate of imipenem is even higher than that of meropenem. Resistance to A. baumannii in PNM patients is about 50%, therefore carbapenem cannot be widely used for the treatment of NFGNB-induced PNM. In previous studies, polymyxin B, tigecycline and even fosfomycin emerged as effective antibiotics of choice against NFGNB-induced PNM. Nevertheless, these antibiotics have frequently been shown to produce major adverse reactions, such as liver and kidney toxicity, etc, and it has been reported that the employing of loading doses of polymyxin to treat infections caused by NFGNB does not improve clinical outcomes significantly and increases nephrotoxicity.19,20 Resistance genotypes of NFGNB are different to Enterobacteriaceae, where the carbapenem-resistant genotype proportion of blaOXA-66 and blaOXA-23 exhibits the highest proportion in A. baumannii and P. aeruginosa, and a lower proportion of metalloenzymes (blaVIM,blaIMP,blaNDM). The high proportion of blaTEM in ESBLs was similar to that reported in previously published literature. However, due to the limited genotypes we used, the genotype coverage for aminoglycosides and quinolones was insufficient.
To better dealt with the NFGNB-induced PNM, physicians, pharmacists, and healthcare professionals around the world recognizing the importance of risk factors. As we all know, risk factor assessment is an important measure for predicting the prognosis of a certain type of disease. Physicians and other healthcare professionals can reduce the mortality of meningitis by NFGNB-induced PNM risk factors evaluation, and pharmacists can choose more accurate and effective antibiotics by precious medical procedure, which conducted by risk factor evaluation partly.21 However, in the treatment of PNM, most previous studies have focused on the risk factors for the occurrence of neurosurgical meningitis, such as EVD, LD, diabetes, hydrocephalus, Koos grade IV and long operation duration (>3h). An intraoperative blood loss >400 mL is an independent risk factor for PNM for vestibular schwannoma.22,23 However, few studies have focused on the risk factors for predicting the outcomes of neurosurgical patients, and even fewer have reported mortality risk prediction studies targeting a specific class of pathogens. For example, a study of Enterobacteriaceae meningitis predicted patient survival and suggested that a Glasgow Coma Scale (GCS) <8 was a clinical risk factor for death from infection in these patients.24 To the best of our knowledge, no risk factor evaluation study has been carried out to target NFGNB as a PNM-related pathogen. In the present study, 16 related risk factors for NFGNB-induced PNM were evaluated using multivariate logistic analysis, and it was concluded that hypertension, EVD and AMV were the main risk factors for the poor prognosis of PNM patients. Patients with hypertension usually mean that they have a certain underlying disease and a low immune status, which contributes to poor clinical outcomes.25 Similar to our study, an Indian study conducted in 2019 showed comorbidities (diabetes, p = 0.036; hypertension, p = 0.01) were associated with poor outcome of post-neurosurgical Acinetobacter meningitis.26 For patients with EVD, necessary to maintain adequate intracranial pressure or having a CSF shunt, the external persistence exists, making the meningitis difficult to cure.27 The incidence of EVD infection ranges from 2 to 22%,28 The best way to reduce infection risk is to remove the EVD as soon as it is no longer needed, thereby decreasing the duration of catheterization which is the most significant risk factor for ventriculitis.29 The patient needs assisted breathing in the state of PNM, which means that the health of a patient is more serious, and that is one of the risk factors for death.30 In a Denmark 10 years study target on bacterial meningitis, AMV was calculated as one of the independent mortality risk factors by multivariate analysis.31 Therefore, for hypertensive patients and those with EVD and AMV, special intensive treatment and prophylaxis care is needed to reduce the mortality rate caused by these insidious infecting pathogens.
Another important discovery in our study was that there was a significant mortality difference in the AP of patients with NFGNM-induced PNM, and the present authors’ previous study showed no difference between the two for multidrug-resistant Enterobacteriaceae infections. For the non-survivors, the preventive application of antibiotics has great clinical significance. The probable reason may be that, compared with Enterobacteriaceae, the prophylactic administration of antibiotics can alleviate the pathogenesis of NFGNB. The pathogenicity of NFGNB is also lower than that of Enterobacteriaceae and AP can greatly improve the prognosis of patients. It reports that the combination of antibiotics usage has significant clinical significance in response to NFGNB infections especially in multi-resistance isolates, and when combined with polymyxin and meropenem in treatment of severe carbapenem resistance A. baumannii infections,32 there was a significant decrease in 30-days mortality with no significant difference in nephrotoxicity.33 Therefore, the combination of polymyxin and meropenem therapy is clinically significant for patients with multi-drug resistant NFGNB infections.34
The present study had several limitations. First, it was a retrospective study subject to potential unmeasured confounding factors. Neverthelessto date, it is the largest cohort of patients studied with NFGNB-induced PNM and includes a very extensive list of established prognostic comorbidities, as well as known specific predisposing factors for its development. Second, it was a single-center study, and distributions of antibiotic usage and gene in A. baumannii and P aeruginosa of the other hospital were not evaluated. Third, the study did not include all the risk factors related to mortality, such as tumor grading, multiple catheterizations, etc. In our next study, a multicenter cohort will be constructed for mortality assessment, when even more risk factor will be identified.
Overall, this study is the first to analyze the risk factors for mortality after NFGNB infection. NFGNB-induced PNM is a relatively serious clinical challenge worldwide. Hypertension, EVD and AMV were identified as independent mortality risk factors for NFGNB-induced PNM.
Data Sharing Statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
Ethical Approval and Consent to Participate
The study was approved by the Ethical Committees of Beijing Tiantan Hospital & Capital Medical University (No. KY-2021-079-02) and the study complies with the Declaration of Helsinki. Each patient enrolled in the study signed an informed consent form.
Acknowledgments
The authors want to take this chance to thank Miss Yumeng Cai and for her help in drawing the figures.
Author Contributions
GHZ: design and drafting of the article; data collection and analysis and interpretation. SQW: statistics and genotypes test. HL and GJZ: conduct the whole study.
Funding
Beijing Hospital Authority Clinical Medicine Development of Special Funding [Grant No. ZYLX202108]; Beijing Municipal Administration of Hospitals Incubating Program [Grant No. PX2022021].
Disclosure
All of the authors declared that no conflict exists in this study.
References
1. Chen C, Zhang B, Yu S, et al. The incidence and risk factors of meningitis after major craniotomy in China: a retrospective cohort study. PLoS One. 2014;9(7):e101961. doi:10.1371/journal.pone.0101961
2. Strahm C, Albrich WC, Zdravkovic V, Schöbi B, Hildebrandt G, Schlegel M. Infection rate after cranial neurosurgical procedures: a prospective single-center study. World Neurosurg. 2018;111:e277–e285. doi:10.1016/j.wneu.2017.12.062
3. Zheng G, Cao Y, Liu C, et al. Phenotype, molecular characterisation and risk factors for postoperative meningitis caused by ESBL-producing-Enterobacteriaceae: a six years multi-Centre comparative cohort study. BMC Infect Dis. 2021;21(1):85. doi:10.1186/s12879-021-05784-7
4. Jain A, Arora N, Meher R, Passey JC, Bansal R. Intracranial complications of CSOM in pediatric patients: a persisting problem in developing countries. Int J Pediatr Otorhinolaryngol. 2017;100:128–131. doi:10.1016/j.ijporl.2017.06.038
5. Metan G, Demiraslan H, Kaynar LG, Zararsız G, Alp E, Eser B. Factors influencing the early mortality in haematological malignancy patients with nosocomial Gram negative bacilli bacteraemia: a retrospective analysis of 154 cases. Braz J Infect Dis. 2013;17(2):143–149. doi:10.1016/j.bjid.2012.09.010
6. Jean SS, Liao CH, Sheng WH, Lee WS, Hsueh PR. Comparison of commonly used antimicrobial susceptibility testing methods for evaluating susceptibilities of clinical isolates of Enterobacteriaceae and nonfermentative Gram-negative bacilli to cefoperazone-sulbactam. J Microbiol Immunol Infect. 2017;50(4):454–463. doi:10.1016/j.jmii.2015.08.024
7. Wongsurakiat P, Tulatamakit S. Clinical pulmonary infection score and a spot serum procalcitonin level to guide discontinuation of antibiotics in ventilator-associated pneumonia: a study in a single institution with high prevalence of nonfermentative gram-negative bacilli infection. Ther Adv Respir Dis. 2018;12:1753466618760134. doi:10.1177/1753466618760134
8. Willyard C. The drug-resistant bacteria that pose the greatest health threats. Nature. 2017;543(7643):15. doi:10.1038/nature.2017.21550
9. Shukla B, Aguilera EA, Salazar L, et al. Aseptic meningitis in adults and children: diagnostic and management challenges. J Clin Virol. 2017;94:110–114. doi:10.1016/j.jcv.2017.07.016
10. Horan TC, Gaynes RP, Martone WJ, Jarvis WR, Emori TG. CDC definitions of nosocomial surgical site infections, 1992: a modification of CDC definitions of surgical wound infections. Infect Control Hosp Epidemiol. 1992;13(10):606–608. doi:10.2307/30148464
11. Zheng G, Li S, Zhao M, et al. Time to positive culture can differentiate post-neurosurgical coagulase-negative Staphylococci other than S epidermidis meningitis from contamination: a case-control observational study. J Clin Lab Anal. 2020;34(10):e23447. doi:10.1002/jcla.23447
12. Kizilates F, Keskin AS, Onder KD. Clinical features of post-operative nosocomial meningitis in adults and evaluation of efficiency of intrathecal treatment. Surg Infect. 2021;22(10):1059–1063. doi:10.1089/sur.2021.024
13. Yu XB, Huang YY, Zhang XS, et al. Intraventricular colistin sulphate as a last resort therapy in a patient with multidrug-resistant Acinetobacter baumannii induced post-neurosurgical ventriculitis. Br J Clin Pharmacol. 2022;88(7):3490–3494. doi:10.1111/bcp.15238
14. Zhang H, Jia P, Zhu Y, et al. Susceptibility to imipenem/relebactam of pseudomonas aeruginosa and Acinetobacter baumannii isolates from Chinese intra-abdominal, respiratory and urinary tract infections: SMART 2015 to 2018. Infect Drug Resist. 2021;14:3509–3518. doi:10.2147/IDR.S325520
15. Mir MA, Ashraf MW, Tripathi V, et al. Isolation, characterization and prevention of various microbial strains in NIC unit and PIC unit. Sci Rep. 2021;11(1):647. doi:10.1038/s41598-020-79364-1
16. Xie L, Zhou A, Zhao J, et al. Comparative insights into multiple drug resistance determinants in Stenotrophomonas maltophilia MER1. J Glob Antimicrob Resist. 2021;27:20–25. doi:10.1016/j.jgar.2021.07.017
17. Chang KY, Wu PC, Lee CH, et al. Clinical features and antimicrobial susceptibility of pseudomonas aeruginosa and Acinetobacter baumannii complex isolates in intensive care patients with chronic obstructive pulmonary disease and community-acquired pneumonia in Taiwan. Int J Chron Obstruct Pulmon Dis. 2021;16:1801–1811. doi:10.2147/COPD.S311714
18. Ma Y, Shi Q, He Q, et al. Metabolomic insights into the inhibition mechanism of methyl N-methylanthranilate: a novel quorum sensing inhibitor and antibiofilm agent against Pseudomonas aeruginosa. Int J Food Microbiol. 2021;358:109402. doi:10.1016/j.ijfoodmicro.2021.109402
19. Katip W, Uitrakul S, Oberdorfer P. Clinical efficacy and nephrotoxicity of the loading dose colistin for the treatment of carbapenem-resistant Acinetobacter baumannii in critically ill patients. Pharmaceutics. 2021;14(1):31. doi:10.3390/pharmaceutics14010031
20. Katip W, Uitrakul S, Oberdorfer P. Clinical outcomes and nephrotoxicity of colistin loading dose for treatment of extensively drug-resistant Acinetobacter baumannii in cancer patients. Infect Drug Resist. 2017;10:293–298. doi:10.2147/IDR.S144314
21. Jeffres MN. The whole price of vancomycin: toxicities, troughs, and time. Drugs. 2017;77:1143–1154. doi:10.1007/s40265-017-0764-7
22. Pintado V, Pazos R, Jiménez-Mejías ME, et al. Staphylococcus aureus meningitis in adults: a comparative cohort study of infections caused by methicillin-resistant and methicillin-susceptible strains. J Hosp Infect. 2019;102(1):108–115. doi:10.1016/j.jhin.2018.11.008
23. Ramos M, Paniguel PL, Sadatsune T, Graziano KU, Mondelli AL, Bocchi S. Decontamination of stainless-steel bowls with 80% (w/v) alcohol for 30s and 60s: randomized experimental study. Rev Lat Am Enfermagem. 2021;29:e3475. doi:10.1590/1518-8345.4997.3475
24. Shi YJ, Zheng GH, Qian LY, et al. Longitudinal analysis of risk factors for clinical outcomes of Enterobacteriaceae meningitis/encephalitis in post-neurosurgical patients: a comparative cohort study during 2014–2019. Infect Drug Resist. 2020;13:2161–2170. doi:10.2147/IDR.S252331
25. Lo MW, Woodruff TM. Complement: bridging the innate and adaptive immune systems in sterile inflammation. J Leukoc Biol. 2020;108(1):339–351. doi:10.1002/JLB.3MIR0220-270R
26. Sharma R, Goda R, Borkar SA, et al. Outcome following postneurosurgical Acinetobacter meningitis: an institutional experience of 72 cases. Neurosurg Focus. 2019;47:E8. doi:10.3171/2019.5.FOCUS19278
27. Konovalov A, Shekhtman O, Pilipenko Y, et al. External ventricular drainage in patients with acute aneurysmal subarachnoid hemorrhage after microsurgical clipping: our 2006–2018 experience and a literature review. Cureus. 2021;13(1):e12951. doi:10.7759/cureus.12951
28. Leverstein-van Hall MA, Hopmans TE, van der Sprenkel JW, et al. A bundle approach to reduce the incidence of external ventricular and lumbar drain-related infections. J Neurosurg. 2010;112:345–353. doi:10.3171/2009.6.JNS09223
29. Nilsson A, Uvelius E, Cederberg D, Kronvall E. Silver-coated ventriculostomy catheters do not reduce rates of clinically diagnosed ventriculitis. World Neurosurg. 2018;117:e411–411e416. doi:10.1016/j.wneu.2018.06.045
30. Chen CY, Lin WC, Yang HY. Diagnosis of ventilator-associated pneumonia using electronic nose sensor array signals: solutions to improve the application of machine learning in respiratory research. Respir Res. 2020;21(1):45. doi:10.1186/s12931-020-1285-6
31. Meyer CN, Samuelsson IS, Galle M, Bangsborg JM. Adult bacterial meningitis: aetiology, penicillin susceptibility, risk factors, prognostic factors and guidelines for empirical antibiotic treatment. Clin Microbiol Infect. 2004;10:709–717. doi:10.1111/j.1469-0691.2004.00925.x
32. Katip W, Oberdorfer P. Clinical efficacy and nephrotoxicity of colistin alone versus colistin plus vancomycin in critically ill patients infected with carbapenem-resistant Acinetobacter baumannii: a propensity score-matched analysis. Pharmaceutics. 2021;13(2):162. doi:10.3390/pharmaceutics13020162
33. Katip W, Uitrakul S, Oberdorfer P. A comparison of colistin versus colistin plus meropenem for the treatment of carbapenem-resistant Acinetobacter baumannii in critically ill patients: a propensity score-matched analysis. Antibiotics. 2020;9(10):647. doi:10.3390/antibiotics9100647
34. Katip W, Oberdorfer P, Kasatpibal N. Effectiveness and nephrotoxicity of loading dose colistin-meropenem versus loading dose colistin-imipenem in the treatment of carbapenem-resistant Acinetobacter baumannii infection. Pharmaceutics. 2022;14(6):1266. doi:10.3390/pharmaceutics14061266
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Characteristics of Severe COVID-19 Patients During Omicron Epidemic and a Nomogram Model Integrating Cell-Free DNA for Predicting Mortality: A Retrospective Analysis
Lu Y, Xia W, Miao S, Wang M, Wu L, Xu T, Wang F, Xu J, Mu Y, Zhang B, Pan S
Infection and Drug Resistance 2023, 16:6735-6745
Published Date: 18 October 2023