Back to Journals » Clinical Epidemiology » Volume 14
Nitrate in Drinking Water and Time to Pregnancy or Medically Assisted Reproduction in Women and Men: A Nationwide Cohort Study in the Danish National Birth Cohort
Authors Ebdrup NH ![]() , Knudsen UB, Schullehner J, Arendt LH, Liew Z, Lyngsø J, Bay B, Clemmensen PJ
, Knudsen UB, Schullehner J, Arendt LH, Liew Z, Lyngsø J, Bay B, Clemmensen PJ ![]() , Sigsgaard T
, Sigsgaard T ![]() , Hansen B, Ramlau-Hansen CH
, Hansen B, Ramlau-Hansen CH ![]()
Received 27 December 2021
Accepted for publication 24 March 2022
Published 13 April 2022 Volume 2022:14 Pages 475—487
DOI https://doi.org/10.2147/CLEP.S354926
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Vera Ehrenstein
Ninna Hinchely Ebdrup,1– 3 Ulla Breth Knudsen,1,3 Jörg Schullehner,2,4 Linn Håkonsen Arendt,2,5 Zeyan Liew,6,7 Julie Lyngsø,2,5 Bjørn Bay,1,8 Pernille Jul Clemmensen,2 Torben Sigsgaard,2,9,10 Birgitte Hansen,4 Cecilia Høst Ramlau-Hansen2
1Department of Obstetrics and Gynecology, Horsens Regional Hospital, Horsens, Denmark; 2Department of Public Health, Aarhus University, Aarhus, Denmark; 3Department of Clinical Medicine, Aarhus University, Aarhus, Denmark; 4Geological Survey of Denmark and Greenland, Aarhus, Denmark; 5Department of Obstetrics and Gynecology, Aarhus University Hospital, Aarhus, Denmark; 6Department of Environmental Health Sciences, Yale School of Public Health, New Haven, CT, USA; 7Yale Center for Perinatal, Pediatric, and Environmental Epidemiology, Yale School of Public Health, New Haven, CT, USA; 8Maigaard Fertility Clinic, Aarhus, Denmark; 9Centre for Integrated Register-based Research at Aarhus University, Aarhus, Denmark; 10Danish Big Data Centre for Environment and Health (BERTHA), Aarhus University, Aarhus, Denmark
Correspondence: Ninna Hinchely Ebdrup, Department of Obstetrics and Gynecology, Horsens Regional Hospital, Regionshospitalet Horsens, Sundvej 30, Horsens, 8700, Denmark, Tel +4528472111, Email [email protected]
Purpose: No studies have investigated if drinking water nitrate affects human fecundity. Experimental studies point at detrimental effects on fetal development and on female and male reproduction. This cohort study aimed to explore if female and male preconception and long-term exposure to nitrate in drinking water was associated with fecundability measured as time to pregnancy (TTP) or use of medically assisted reproduction (MAR) treatment.
Methods: The study population consisted of pregnant women recruited in their first trimester in 1996– 2002 to the Danish National Birth Cohort. Preconception drinking-water nitrate exposure was estimated for the pregnant women (89,109 pregnancies), and long-term drinking water nitrate exposure was estimated from adolescence to conception for the pregnant women (77,474 pregnancies) and their male partners (62,000 pregnancies) by linkage to the national drinking water quality-monitoring database Jupiter. Difference in risk of TTP > 12 months or use of MAR treatment between five exposure categories and log-transformed continuous models of preconception and long-term nitrate in drinking water were estimated. Binominal regression models for risk ratios (RR) were adjusted for age, occupation, education, population density, and lifestyle factors.
Results: Nitrate in drinking water (median preconception exposure: 1.9 mg/L; median long-term exposure: 3.3 mg/L) was not associated with TTP > 12 months or use of MAR treatment, neither in the categorical nor in the continuous models.
Conclusion: We found no association between preconception or long-term exposure to drinking water nitrate and fecundability.
Keywords: environmental pollutant, subfecundity, time to pregnancy, public health, groundwater
Introduction
Infertility, ie, the inability to conceive after 12 months of regular intercourse, affects one in six couples worldwide. Exposure to environmental pollutants may be a contributing factor apart from age, reproductive diseases in men and women and lifestyle factors.1–3 A couple’s fecundability is the biological ability to conceive and is often measured as the waiting time to pregnancy (TTP), eg, the number of menstrual cycles it takes to conceive.4
Nitrate is a widespread drinking water pollutant.5,6 Although evidence from animal studies suggests an impairment of reproduction and fetal development following nitrate exposure,7–13 limited human research has been undertaken regarding the potential impact on reproductive health. The evidence from experimental studies calls for more research in humans of low dose every day exposure to nitrate, as studies have mainly been conducted in rodents and at exposure levels far above the drinking water standard set by the World Health Organization.14 Nitrate partly converts to nitrite, which can be endogenously transformed to N-nitroso compounds (NOCs) with DNA damaging potential. The formation of DNA damaging substances may have teratogenic and hormone disruptive effects in humans. Adverse birth outcomes were found at nitrate exposures below the drinking water standard, and thyroid and steroid imbalance have been speculated to potentially harm human reproductive function.14–21 Further nitrate after reduction to nitrite can bind to hemoglobin and form methaemoglobin.22 Methaemoglobin interferes with the oxygen-carrying capacity of the blood and might cause hypoxia in fetuses.23 NOC formation and methaemoglobinemia are the suspected biological mechanisms potentially affecting reproduction in humans.15,24–31 Humans are exposed to nitrate and NOCs throughout life and during susceptible reproductive windows. The current drinking water standard of nitrate is set at 50 mg/L,16 a level above which there is a risk of acute infant methemoglobinemia. However, lower doses may also cause long-term health effects and the question remains whether the drinking water standard safeguards our reproductive health.32,33
To the best of our knowledge, no human studies exist on the potential effects of nitrate in drinking water on measures of fecundity.17 We studied the association between exposure to preconception and long-term nitrate in drinking water and fecundability measured as waiting time to pregnancy (TTP) and use of medically assisted reproductive (MAR) treatment. We hypothesized that couples with higher nitrate exposure from drinking water had a higher risk of TTP >12 months and MAR treatment to conceive.
Materials and Methods
Study Population
This cohort study is based on all pregnant women participating in the Danish National Birth Cohort (DNBC) in 1996–2002 (n=91,380). We included 89,109 pregnancies and excluded pregnancies with missing exposure or covariate information according to the flow diagram (Figure 1). The DNBC had an estimated participation rate of 60% and included 30% of all pregnant women in Denmark during the study period.34 Women were enrolled around gestational week 11 (SD 3.4) and provided information on lifestyle factors, health status, TTP, and potential use of MAR treatment. Computer-assisted telephone interviews were conducted in the first trimester, irrespective of whether the pregnancy ended in the birth of a child or pregnancy loss.35 We linked information on age, residence, and vital status across national registries36 using the unique personal identification number registered in the Danish Civil Registration System (CRS) and assigned to all Danish residents at birth or immigration.37 The CRS contains current and historical information on sex, birthdate, vital status, spouse, and residence, including date of moving, immigration, and emigration. To study the potential effects of exposure to nitrate in drinking water in men, we linked the male partner to the female partner included in the DNBC by the unique identifier using registered information for married couples and cohabiting couples with mutual children. We also included the male partner in cohabiting couples with less than 15 years of age difference without mutual children in the CRS and not in close family relationship with each other. Using this algorithm, we were able to link 62,000 (70%) of the pregnancies included in the DNBC to a male partner. The CRS is recognized for its practically complete registration due to the general acceptance of registration requested by law, and data recorded in the CRS are considered to have high validity.37
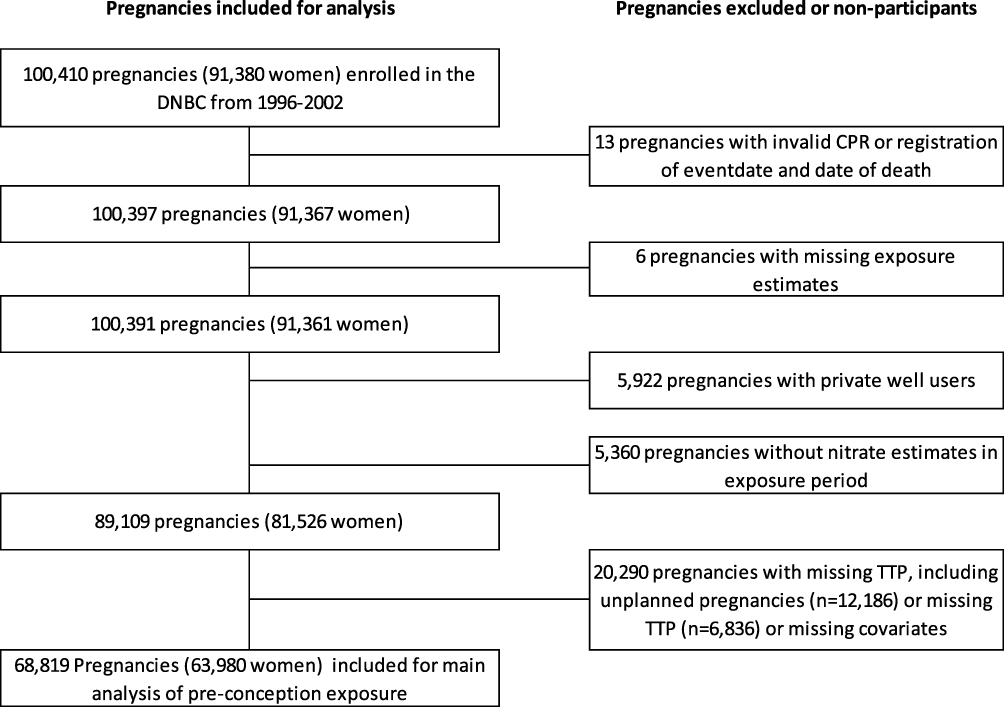 |
Figure 1 Flow chart of the study population from the Danish National Birth Cohort (1996–2002). Abbreviations: DNBC, Danish National Birth Cohort; CPR, personal identification number; TTP, time to pregnancy. |
Exposure
In Denmark, drinking water originates from groundwater, where nitrate concentrations vary mainly due to differences in agricultural nitrogen fertilization and management as well as the geology and geochemistry characteristics of the subsurface.38,39 Household-level data have been used to estimate individual-level nitrate exposure from drinking water across several studies of nitrate associated with adverse health outcomes.15,33,40 In brief, to determine nitrate concentrations in drinking water at each household, we linked the national drinking water quality monitoring database41 to the geocoded residential history for every person registered in the CRS from 1978 onwards37 by using digitized water supply areas.
We excluded non-detects exceeding the upper level of detection (1 mg/L) and calculated annual nitrate levels for each household. For years without nitrate measurements, we imputed concentrations by interpolation if there was a measurement available within 3 years.42 We excluded private well users because they are monitored far less than public waterworks in Denmark.43 We calculated time-weighted average exposures while taking into account both temporal changes of nitrate levels at the households and changes of residency. For a more detailed description of the approach, see Schullehner et al.38,42,43 We calculated each woman’s average nitrate exposure from 2 years prior to conception (hereinafter “preconception exposure”). For 83% of the DNBC couples, the couples shared the preconception exposure estimates because the exposure levels were estimated based on the residential history of the woman. To study separately the potential effects in women and men and to cover the period from adolescence until conception and gain larger exposure contrast, we calculated long-term individual nitrate estimates for both sexes (n=74,774 women, n=62,000 men). The long-term exposure window was defined from January 1, 1978 (or from the date of birth if the women or men were born after January 1, 1978) until date of conception (hereinafter “female and male long-term exposure”).
For the preconception exposure assessment, we included exclusively participants with complete exposure data. For the long-term exposure assessments, we allowed participants to have missing exposure information for a maximum of 50% of the exposure window.33
Outcome
In the first DNBC interview, which was conducted around gestational week 15, women reported their TTP into five predefined categories (less than 1 month, after 1–2 months, after 3–5 months, after 6–12 months, more than 12 months). MAR treatment was included in the questionnaire if the women reported a TTP of 6 months or longer. In the present study, we defined the outcome as TTP >12 months or use of MAR treatment (reference TTP ≤12 months). Women also reported if their pregnancy was planned. In the main analysis, we excluded unplanned pregnancies (14%) as they were considered to include pregnancies of highly fecund or subfecund couples.44
Covariates
We made an a priori decision on which covariates to include by reviewing the literature and using directed acyclic graphs (Supplemental Figure 1).45 We included age, body mass index (BMI), smoking, alcohol consumption, occupation, education, and population density (as a proxy for area and environment)46 as listed in Table 1. We modeled age and population density as restricted cubic splines. Level of education and occupation at conception were derived from Statistics Denmark.47,48 Age and lifestyle variables were available from the DNBC interviews. Lifestyle was included to improve the precision as we expected BMI, smoking, and alcohol to be strongly associated with the outcome.
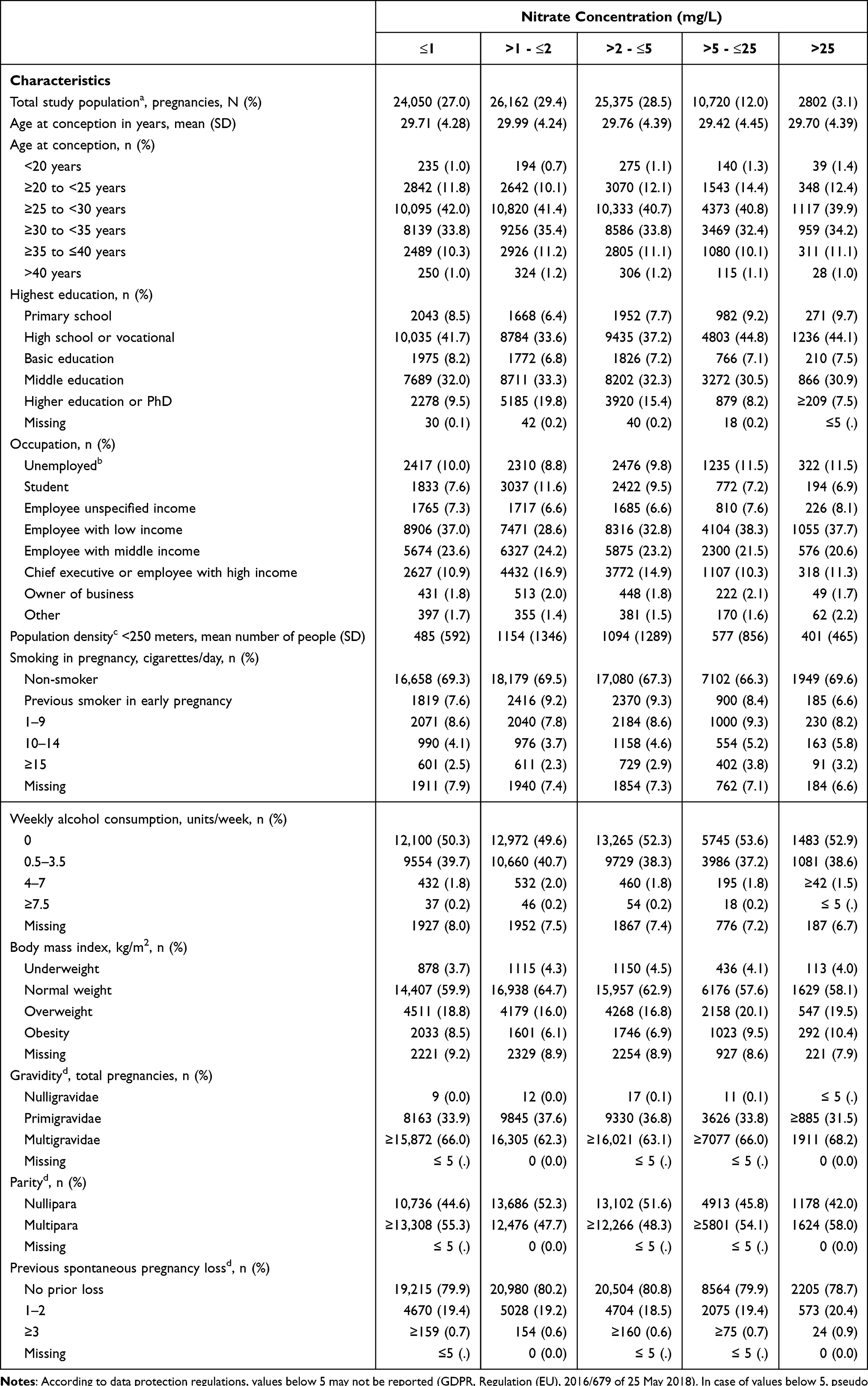 |
Table 1 Characteristics of the Female Study Population from the Danish National Birth Cohort (1996–2002) According to Preconception Drinking Water Nitrate |
Statistical Analyses
To address our aim, we used two different analytical models. In the first analytical model for the analyses of preconception and long-term nitrate exposures, we applied binominal regression models and estimated adjusted risk ratios (RR) with 95% confidence intervals (CIs) comparing the risk of TTP >12 months or MAR treatment between five categories of drinking water nitrate exposure (mg/L NO3−). We categorized drinking water nitrate into five a priori defined groups (≤ 1 mg/L (reference), >1 - ≤2 mg/L, >2 - ≤5 mg/L, >5 - ≤25 mg/L, and >25 mg/L).15 The continuous variable was log-transformed and modeled using restricted cubic splines with four knots.49
We conducted several sensitivity analyses. In the first sensitivity analysis, we studied MAR treatment as the outcome (reference: no MAR treatment). In the second and third sensitivity analyses, we introduced unplanned pregnancies to the group with the longest TTP (TTP >12 months or MAR treatment) and the group with the shortest TTP (the reference), respectively. The couple’s lifestyle may be reflected in the individual’s lifestyle. However, as female lifestyle is only a proxy of male lifestyle, we omitted female lifestyle in a fourth sensitivity analysis of male long-term nitrate exposure. To reduce the risk of exposure misclassification in the long-term exposure analyses, the study population was restricted in the fifth and sixth sensitivity analyses to those who had lived 75% of the exposure window at residences with a nitrate estimate.
In the second analytical model, we estimated the mean differences in TTP (days) between the five categories of nitrate exposure compared to the reference concentration below 1 mg/L using linear regression with robust variance to account for departures from normality. We used simple imputation relying on clinical knowledge50,51 to impute TTP based on the categories given from the DNBC interview (TTP <1 month = TTP 0 month, TTP 1–2 months = TTP 1.5 months, TTP 3–5 months = TTP 4 months, TTP 6–12 months = TTP 9 months, TTP above 12 months = TTP 13 months, MAR treatment = TTP 18 months).
In quantitative bias analyses, we addressed the risk of bias due to selection on fetal survival in the inclusion to the DNBC.
All models were fitted using robust variance estimation to account for dependencies between pregnancies by the same individual. There was no statistically significant interaction between any of the exposures and adjusting variables. Continuous variables (age and population density) were included as restricted cubic splines with four knots.
We conducted the statistical analyses and modeling of the exposure by use of R (version 3.6; R Development Core Team) and Stata, version 15.0 (StataCorpLP, College Station, TX, USA).
Ethical Considerations
The participating women in the DNBC gave written consent. The data were pseudo-anonymized, and Aarhus University approved the study as Data Controller (No. 2015-57-002, project No. 1643). No ethical approval from the Danish Ethics Committee was required for this study in accordance with Danish legislation.
Results
Of the 100,410 pregnancies in the DNBC, we identified 89,109 as the female study population with the characteristics presented in Table 1. We included 68,819 (69%) pregnancies with sufficient exposure data and TTP data for the main analysis of preconception exposure (Figure 1). Among these, 11,626 (17%) women had a TTP >12 months or needed MAR treatment to conceive. The median preconception nitrate exposure was 1.9 mg/L (95% prediction interval (PI): 0.2–16.1 mg/L).
In the analyses of long-term nitrate exposure, the right skewed exposure distribution was 3.3 mg/L (95% PI: 0.5–23.8) (median among women) and 3.3 mg/L (95% PI: 0.4–24.5) (median among men). The mean time of long-term exposure was 22 years (16–25 years) for women and 21 years (18–25 years) for men, corresponding to follow-up from age 8 in women and age 11 in men. The characteristics of the male study population are presented in Supplemental Table 1.
Table 2 shows adjusted RRs for TTP >12 months or MAR treatment according to preconception exposure and female and male long-term exposures. Overall, we found no higher risk of TTP >12 months or MAR treatment with increasing levels of nitrate. In the analysis of preconception exposure, drinking water nitrate was associated with a slightly lower risk of TTP >12 months or MAR treatment at nitrate levels 1–5 mg/L compared to the reference category (below highest level of detection, 1 mg/L). Nitrate in drinking water was not associated with TTP >12 months or MAR treatment in the long-term analyses.
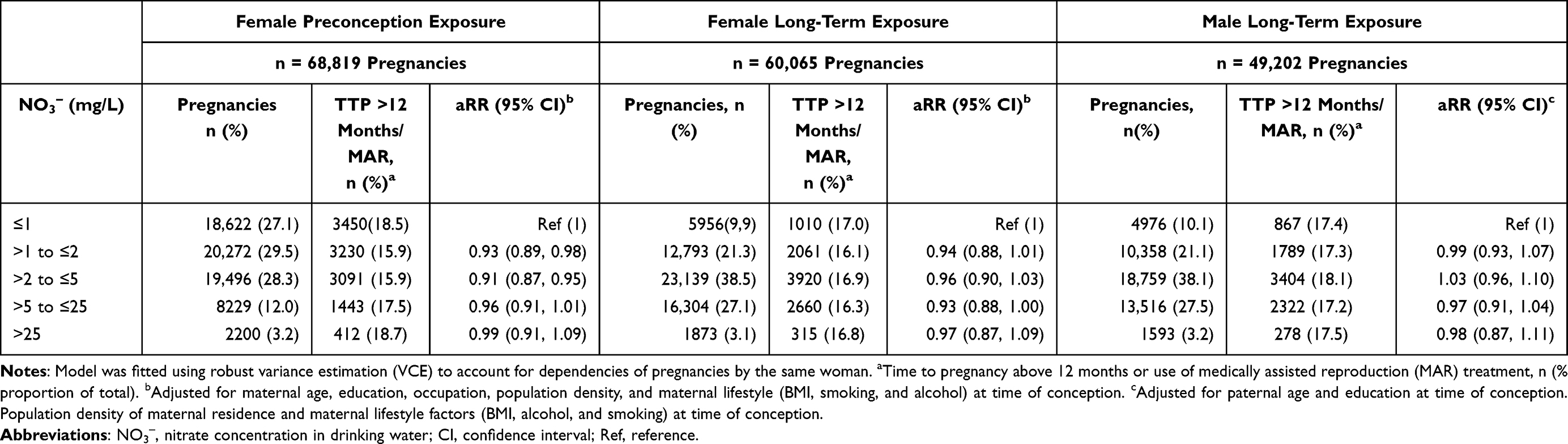 |
Table 2 Adjusted Risk Ratios for the Association Between Nitrate in Drinking Water and Time to Pregnancy Above 12 Months or Use of Medically Assisted Reproduction (MAR) Treatment, The Danish National Birth Cohort (1996–2002) |
When using cubic splines to assess the association (Figure 2), we found no differences in the adjusted RRs according to levels of drinking water nitrate, neither in the preconception nor in the long-term exposure models.
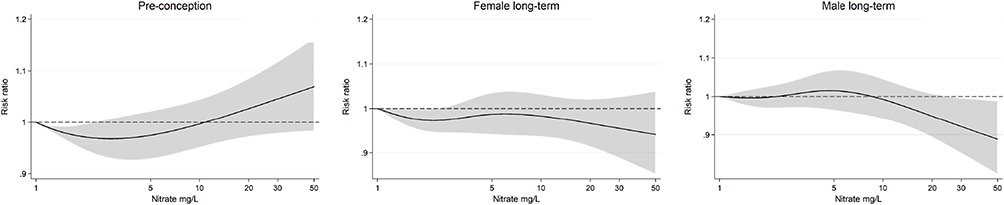 |
Figure 2 Adjusted risk ratios of time to pregnancy above 12 months or use of MAR treatment by drinking water nitrate exposure (log scale) with 1 mg/L as reference. Exposure below the highest detection limit 1 mg/L and above 50 mg/L is not shown but is included in the model. The gray scale area represents the confidence interval (CI). Female splines were adjusted for female age, education, occupation, population density, body mass index, smoking, and alcohol. Male splines were adjusted for male age and education and female population density, body mass index, smoking, and alcohol. Robust variance estimation (VCE) accounted for dependencies of pregnancies. |
The estimated mean differences in TTP ranged from −15 days (96% CI: −18, −12) to −2 days (95% CI: −9, 6) when we compared the four preconception exposure categories above 1 mg/L NO3− to the TTP of the reference group (mean TTP 164 days (95% CI: 162, 167)) (Supplemental Table 2).
The sensitivity analyses of both preconception exposure and long-term exposure supported the findings of the main analyses (Supplemental Tables 3–8). Bias analyses were reported in Supplemental Tables 9–13.
Discussion
Key Findings
The findings did not support our hypothesis of higher risk of TTP >12 months or MAR treatment with increasing levels of drinking water nitrate, neither for the preconception exposure nor for the long-term exposure in women or men. When we modelled the exposure as a continuous variable, no difference in risk was found. In the categorical analyses, we found slightly lower risk estimates in the lowest categories of exposure in the analysis of preconception nitrate in drinking water and no difference in risk in the long-term models. In absolute measures, the mean difference in TTP in days was found to be clinically negligible.
Current Evidence
To our knowledge, no published studies exist on the association between drinking water nitrate and female or male infertility or fertility treatment, and the biological mechanism by which nitrate exposure may impair reproductive function remains unclear.17 Nitrate may, after reduction to nitrite, form water-soluble teratogenic and endocrine disruptive compounds that may expose reproductive organs and developing fetuses.52–54 In humans, nitrate exposures below 50 mg/L have previously been associated with thyroid dysfunction, neonatal death, fetal growth restriction, prematurity, and congenital malformations.15,24–31 However, this suggestion of reproductive toxicity was not reflected in a case–control study from 1989 of fetal death of 286 women who had a pregnancy loss and 1391 controls with live births admitted to the same hospital. The exposure was estimated based on public water supply samples taken after the time of pregnancy loss and were below the drinking water standard. In a Danish cohort study of 652,810 women with the first recorded singleton pregnancy, the risk of stillbirth was not associated with nitrate below the drinking water standard.24,40 The hypothesis of adverse methaemoglobin reproductive effects was suggested after evaluation of 25 women with pregnancy loss in the first trimester and higher levels of methaemoglobin.23 Methaemoglobin associated pregnancy loss was not found in women with pregnancy loss compared to women with term delivery, by long-term measurements of serum methemeglobin levels in pregnancy.55
In animals, nitrite has been associated with impaired reproduction in mice, rats, guinea pigs, and cattle, with longer days to litter and perinatal death.7,11,52,56 In utero exposure to nitrite has also shown trans-placental effects of mutagenic cell damage in hamster embryos.53 Likewise, impaired male reproductive function has been reported at exposures to 31.5–122 mg/L NO3− in rats and to 214–427 mg/L NO3− in rabbits.12,57 Nitrate has also been suspected of steroid hormone disruptive effects at nitrate exposures of 30.5 mg/L NO3−, although with inconsistent findings in experimental studies.18,20,58 In addition other experimental studies in rodents found no reproductive harmful effects at toxic doses to nitrite and nitrate.17
Strengths and Limitations
A major strength of our study was the inclusion of a large study population with individual-level exposure assessments of both women and men. In a life course perspective, the peri-conceptual period, adolescence, and young adulthood are all critical biological periods. Exposure in these susceptible windows may have a lifelong and irreversible effect and may influence future reproductive health.59 The female ovaries are fully developed in perinatal life and are thus exposed lifelong. In men, the testes remain dormant after organogenesis until puberty, in which spermatogenesis kick-starts the recurrent gamete production.60
The analyses of long-term nitrate exposure (ie, 21 years of exposure) covering from pre-puberty until conception (age 8–29 in women, age 11–32 in men) allowed us to investigate low-dose effects on later reproductive health, not previously tested in human or animal models. We relied on a unique resource of longitudinally collected drinking water samples from certified laboratories.38,39,41 Nitrate levels in drinking water in Denmark are without seasonal variation, and the bioavailability is considered steady, with continuous drinking water intake.38,61 As a result, exposure changes are more likely due to change of address, which we accounted for by day-specific residential data. Further, we included confounding variables from interviews and national registries of high validity and completeness.34,38,62 Thus, this nationwide study is a significant contribution to an overlooked field, despite the global exposure to nitrate and the potential influence on public health as a modifiable risk factor.
The study included only women who obtained a pregnancy lasting at least to the end of first trimester. Around 30% of all pregnancies are lost in the first months of pregnancy, with the highest percentage in the earliest weeks of fetal life.63,64 The DNBC included women when they consulted their general practitioner, with a mean gestational age at enrollment of 11 completed weeks. Even though we also included women experiencing pregnancy loss after inclusion, we could not include the earliest of pregnancy losses. Moreover, the inclusion of pregnancies conceived after MAR treatment was not representative, as 30% of couples receiving MAR treatment do not get a child.65 In this regard, the DNBC comprises a cohort of couples with proven fertility and fetal survivors. This may have led to biased results, as collider stratification bias may have been present if both high nitrate exposure and inability to conceive are associated with selection into the study. Collider stratification bias due to selection has long been an issue of concern in studies of environmental exposures, and even inverse associations have been speculated to be due to selection of survivors.66,67 To quantify the magnitude of potential selection bias towards the null we conducted bias analyses for the preconception exposure as presented in the Supplemental Material Tables 12 and 13. We found that in scenarios with selection >30% and high degree of effect modification by individual factors related to endogenous nitrosation capacity, biased results might have masked reproductive harmful effects.
We relied on exposure assessments at residential level and estimated nitrate in drinking water as a proxy for endogenous nitrate exposure, as biological samples were unavailable. We expect only moderate degrees of non-differential misclassification of exposure, which is likely to have produced bias towards the null. In a Swedish study, 70% of cold tap water was consumed at home,68 and the Danish population consumes the least bottled water in Europe.69,70 In addition, we expect that most people have jobs and homes in geographical proximity, and their drinking water source will thereby originate from the same area.
Fecundability is a couple concept, and the preconception exposure assessment based on female residence may be identical to the male preconception exposure. The two-year exposure window was set after discussions in the author group of a clinically relevant preconception exposure window, while considering the rather constant nitrate level over the years. In our study, the couple’s preconception exposures were highly correlated, as 83% of the couples shared residence at the time of conception. Further, one would expect the couples to share lifestyle and other potential confounding factors.71,72 The risk of misclassification cannot be ruled out, and it is however reassuring that the sensitivity analysis solely including male covariates in the model (Supplemental Table 6) did not change the estimates significantly.
We relied on retrospectively reported TTP, although with short recall time as it was reported in early pregnancy. In Denmark, couples are offered MAR treatment free of charge for up to three in vitro attempts or a child. In a validation study, the self-reported MAR treatment in the DNBC was compared to that in the Danish national registries, and a positive predictive value of 88% was reported.73 Thus, we expect the risk of misclassification to be of little importance.74 Further, we do not anticipate a potential misclassification to be differential because participants are expected to be unaware of their nitrate exposure. We had no information on other aspects of family planning, such as timing and frequency of intercourse or contraceptive planning, but we do not expect these to be associated with nitrate levels.
The women with unplanned pregnancies could not report their TTP and were excluded from the main analyses. They may represent either the most fecund or the least fecund women. However, in the sensitivity analyses, in which we included women with unplanned pregnancies in first the TTP >12 months category and second the reference category, we found no changes from the main analysis.
Even though we were able to adjust for important potential confounders and precision variables, including socioeconomic position, lifestyle factors, and environmental factors, we cannot rule out residual confounding, eg, by nitrate in diet or other agricultural pollutants in drinking water. To address potential co-contamination of nitrate and other anthropogenic pollutants, ie, pesticides, we adjusted for population density as proxy for other environmental pollutants. Still, residual confounding of other pollutants cannot be ruled out.75 Nitrate is also found in green vegetables and cured meat, and diet may contain inhibitory antioxidants and vitamins that may protect against nitrate-associated adverse health effects.76
The generalizability of these results is subject to certain limitations, as we relied on a selected cohort of women and their male partners, who all obtained a pregnancy. Sterile and subfecund couples are underrepresented, as we condition on pregnancy, and the findings cannot be generalized to sterile people or exposure above the drinking water standard. We need novel strategies for recruiting couples to measure TTP in the general population when studying potential adverse effects of environmental exposures. Longitudinal measurements of TTP in populations of pregnancy planners and enrollment of pregnancies by the same mother will enable us to better understand potential sensitive windows and effects in susceptible populations.
Conclusion
Preconception and long-term drinking water nitrate exposure at comparatively low exposure levels were not associated with higher risk of TTP >12 months or MAR treatment in couples who obtained a pregnancy. Selection and exposure misclassification may have biased our results towards the null, and our findings need replication in the general population.
Acknowledgments
We thank all the women in the DNBC. The DNBC was established with a significant grant from the Danish National Research Foundation. Additional support was obtained from the Danish Regional Committees, the Pharmacy Foundation, the Egmont Foundation, the March of Dimes Birth Defects Foundation, the Health Foundation and other minor grants. The DNBC Biobank has been supported by the Novo Nordisk Foundation and the Lundbeck Foundation. Follow-up of mothers and children has been supported by the Danish Medical Research Council (SSVF 0646, 271-08-0839/06-066023, O602-01042B, 0602-02738B), the Lundbeck Foundation (195/04, R100-A9193), The Innovation Fund Denmark 0603-00294B (09-067124), the Nordea Foundation (02-2013-2014), Aarhus Ideas (AU R9-A959-13-S804), University of Copenhagen Strategic Grant (IFSV 2012), and the Danish Council for Independent Research (DFF – 4183-00594 and DFF – 4183-00152).
Funding
This work was supported by Horsens Regional Hospital, the Health Research Foundation of the Central Denmark Region, Aarhus University, Aase and Ejnar Danielsen’s Foundation, and Merck Denmark and Ferring Denmark funded the study.
Disclosure
Mr Bjørn Bay reports personal fees from MSD, outside the submitted work. The authors report no conflicts of interest in this work.
References
1. European Society of Human Reproduction and Embryology. ART fact sheet. 2020 data 2016–2020. Available from: file:///C:/Users/au631982/Downloads/ESHRE_ARTFactSheet_2022.pdf.
2. Segal TR, Giudice LC. Before the beginning: environmental exposures and reproductive and obstetrical outcomes. Fertil Steril. 2019;112(4):613–621. doi:10.1016/j.fertnstert.2019.08.001
3. Zegers-Hochschild F, Adamson GD, Dyer S, et al. The international glossary on infertility and fertility care, 2017. Hum Reprod. 2017;32:1786–1801. doi:10.1093/humrep/dex234
4. Vander Borght M, Wyns C. Fertility and infertility: definition and epidemiology. Clin Biochem. 2018;62:2–10. doi:10.1016/j.clinbiochem.2018.03.012
5. Hansen B, Thorling L, Kim H, Blicher-Mathiesen G. Long-term nitrate response in shallow groundwater to agricultural N regulations in Denmark. J Environ Manage. 2019;240:66–74.
6. van Grinsven HJ, Rabl A, de Kok TM. Estimation of incidence and social cost of colon cancer due to nitrate in drinking water in the EU: a tentative cost-benefit assessment. Environ Health. 2010;9:58. doi:10.1186/1476-069X-9-58
7. Anderson LM, Giner-Sorolla A, Ebeling D. Effects of imipramine, nitrite, and dimethylnitrosamine on reproduction in mice. Res Commun Chem Pathol Pharmacol. 1978;19:311–327.
8. Anderson LM, Giner-Sorolla A, Haller IM, Budinger JM. Effects of cimetidine, nitrite, cimetidine plus nitrite, and nitrosocimetidine on tumors in mice following transplacental plus chronic lifetime exposure. Cancer Res. 1985;45:3561–3566.
9. Greenlee AR, Ellis TM, Berg RL. Low-dose agrochemicals and lawn-care pesticides induce developmental toxicity in murine preimplantation embryos. Environ Health Perspect. 2004;112:703–709. doi:10.1289/ehp.6774
10. National Toxicology Program. Toxicology and carcinogenesis studies of sodium nitrite (CAS NO. 7632-00-0) in F344/N rats and B6C3F1 mice (drinking water studies). Natl Toxicol Program Tech Rep Ser. 2001;495:7–273.
11. Sund JM, Wright MJ, Simon J. Weeds containing nitrates cause abortion in cattle. Agron J. 1957;49:278–279. doi:10.2134/agronj1957.00021962004900050019x
12. Aly HA, Mansour AM, Abo-Salem OM, Abd-Ellah HF, Abdel-Naim AB. Potential testicular toxicity of sodium nitrate in adult rats. Food Chem Toxicol. 2010;48:572–578. doi:10.1016/j.fct.2009.11.034
13. Pant N, Srivastava SP. Testicular and spermatotoxic effect of nitrate in mice. Hum Exp Toxicol. 2002;21:37–41. doi:10.1191/0960327102ht206oa
14. Ward MH, Jones RR, Brender JD, et al. Drinking water nitrate and human health: an updated review. Int J Environ Res Public Health. 2018;15:1557. doi:10.3390/ijerph15071557
15. Coffman VR, Jensen AS, Trabjerg BB, et al. Prenatal exposure to nitrate from drinking water and markers of fetal growth restriction: a population-based study of nearly one million Danish-born children. Environ Health Perspect. 2021;129:27002. doi:10.1289/EHP7331
16. Water and health in Europe. A joint report from the European Environment Agency and the WHO Regional Office for Europe. WHO Reg Publ Eur Ser. 2002;III-XXIII:1–222.
17. Clausen HS, Ebdrup NH, Barsoe IM, et al. Association between drinking water nitrate and adverse reproductive outcomes: a systematic PRISMA review. Water. 2020;12:2287. doi:10.3390/w12082287
18. Panesar NS, Chan KW. Decreased steroid hormone synthesis from inorganic nitrite and nitrate: studies in vitro and in vivo. Toxicol Appl Pharmacol. 2000;169:222–230. doi:10.1006/taap.2000.9079
19. De Groef B, Decallonne BR, Van der Geyten S, Darras VM, Bouillon R. Perchlorate versus other environmental sodium/iodide symporter inhibitors: potential thyroid-related health effects. Eur J Endocrinol. 2006;155:17–25. doi:10.1530/eje.1.02190
20. Edwards TM, Hamlin HJ. Reproductive endocrinology of environmental nitrate. Gen Comp Endocrinol. 2018;265:31–40. doi:10.1016/j.ygcen.2018.03.021
21. Blaisdell J, Turyk ME, Almberg KS, Jones RM, Stayner LT. Prenatal exposure to nitrate in drinking water and the risk of congenital anomalies. Environ Res. 2019;176:108553. doi:10.1016/j.envres.2019.108553
22. Greer FR, Shannon M;, Committee on Environmental Health. Infant methemoglobinemia: the role of dietary nitrate in food and water. Pediatrics. 2005;116:784–786. doi:10.1542/peds.2005-1497
23. Schmitz JT. Methemoglobinemia–a cause of abortions? Preliminary report. Obstet Gynecol. 1961;17:413–415.
24. Aschengrau A, Zierler S, Cohen A. Quality of community drinking water and the occurrence of spontaneous abortion. Arch Environ Health. 1989;44:283–290. doi:10.1080/00039896.1989.9935895
25. Migeot V, Albouy-Llaty M, Carles C, et al. Drinking-water exposure to a mixture of nitrate and low-dose atrazine metabolites and small-for-gestational age (SGA) babies: a historic cohort study. Environ Res. 2013;122:58–64. doi:10.1016/j.envres.2012.12.007
26. Sherris AR, Baiocchi M, Fendorf S, Luby SP, Yang W, Shaw GM. Nitrate in drinking water during pregnancy and spontaneous preterm birth: a retrospective within-mother analysis in California. Environ Health Perspect. 2021;129:57001. doi:10.1289/EHP8205
27. Bukowski J, Somers G, Bryanton J. Agricultural contamination of groundwater as a possible risk factor for growth restriction or prematurity. J Occup Environ Med. 2001;43:377–383. doi:10.1097/00043764-200104000-00016
28. Stayner LT, Almberg K, Jones R, Graber J, Pedersen M, Turyk M. Atrazine and nitrate in drinking water and the risk of preterm delivery and low birth weight in four Midwestern states. Environ Res. 2017;152:294–303. doi:10.1016/j.envres.2016.10.022
29. Croen LA, Todoroff K, Shaw GM. Maternal exposure to nitrate from drinking water and diet and risk for neural tube defects. Am J Epidemiol. 2001;153:325–331. doi:10.1093/aje/153.4.325
30. Dorsch MM, Scragg RK, McMichael AJ, Baghurst PA, Dyer KF. Congenital malformations and maternal drinking water supply in rural South Australia: a case-control study. Am J Epidemiol. 1984;119:473–486. doi:10.1093/oxfordjournals.aje.a113764
31. Radikova Z, Tajtakova M, Kocan A, et al. Possible effects of environmental nitrates and toxic organochlorines on human thyroid in highly polluted areas in Slovakia. Thyroid. 2008;18:353–362. doi:10.1089/thy.2007.0182
32. van Grinsven HJ, Ward MH, Benjamin N, de Kok TM. Does the evidence about health risks associated with nitrate ingestion warrant an increase of the nitrate standard for drinking water? Environ Health. 2006;5:26. doi:10.1186/1476-069X-5-26
33. Schullehner J, Hansen B, Thygesen M, Pedersen CB, Sigsgaard T. Nitrate in drinking water and colorectal cancer risk: a nationwide population-based cohort study. Int J Cancer. 2018;143:73–79. doi:10.1002/ijc.31306
34. Olsen J, Melbye M, Olsen SF, et al. The Danish national birth cohort–its background, structure and aim. Scand J Public Health. 2001;29:300–307. doi:10.1177/14034948010290040201
35. Danish National Birth Cohort (DNBC). Interview 1-4. Available from: https://www.dnbc.dk/data-available/interviews-1—4.
36. Schmidt M, Pedersen L, Sørensen HT. The Danish civil registration system as a tool in epidemiology. Eur J Epidemiol. 2014;29(8):541–549. doi:10.1007/s10654-014-9930-3
37. Pedersen CB. The Danish civil registration system. Scand J Public Health. 2011;39:22–25. doi:10.1177/1403494810387965
38. Schullehner J, Stayner L, Hansen B. Nitrate, nitrite, and ammonium variability in drinking water distribution systems. Int J Environ Res Public Health. 2017;14:276. doi:10.3390/ijerph14030276
39. Hansen B, Dalgaard T, Thorling L, Sorensen B, Erlandsen M. Regional analysis of groundwater nitrate concentrations and trends in Denmark in regard to agricultural influence. Biogeosciences. 2012;9:3277–3286. doi:10.5194/bg-9-3277-2012
40. Thomsen AML, Ramlau-Hansen CH, Schullehner J, et al. Prenatal nitrosatable prescription drug intake, drinking water nitrate, and the risk of stillbirth: a register- and population-based cohort of Danish pregnancies, 1997–2017. Environ Health. 2021;20:118. doi:10.1186/s12940-021-00805-z
41. Hansen M, Pjetursson B. Free, online Danish shallow geological data. Geol Surv Den Greenl Bull. 2011;23:53–56. doi:10.34194/geusb.v23.4842
42. Schullehner J, Hansen B. Nitrate exposure from drinking water in Denmark over the last 35 years. Environ Res Lett. 2014;9(9):095001. doi:10.1088/1748-9326/9/9/095001
43. Schullehner J, Jensen NL, Thygesen M, Hansen B, Sigsgaard T. Drinking water nitrate estimation at household-level in Danish population-based long-term epidemiologic studies. J Geochem Explor. 2017;183:178–186. doi:10.1016/j.gexplo.2017.03.006
44. Bonde JP, Joffe M, Sallmen M, et al. Validity issues relating to time-to-pregnancy studies of fertility. Epidemiology. 2006;17:347–349. doi:10.1097/01.ede.0000210239.80406.46
45. Greenland S, Pearl J, Robins JM. Causal diagrams for epidemiologic research. Epidemiology. 1999;10:37–48. doi:10.1097/00001648-199901000-00008
46. Samuelsson K, Chen T-HK, Antonsen S, Brandt SA, Sabel C, Barthel S. Residential environments across Denmark have become both denser and greener over 20 years. Environ Res Lett. 2020;16:014022. doi:10.1088/1748-9326/abcf7a
47. Elias P. Occupational Classification (ISCO-88): Concepts, Methods, Reliability, Validity and Cross-National Comparability. OECD Labour Market and Social Policy Occasional Papers; 1997:20.
48. Jensen VM, Rasmussen AW. Danish education registers. Scand J Public Health. 2011;39:91–94. doi:10.1177/1403494810394715
49. Harrell FE. Regression Modeling Strategies.
50. Bonde JP, Hjollund NH, Jensen TK, et al. A follow-up study of environmental and biologic determinants of fertility among 430 Danish first-pregnancy planners: design and methods. Reprod Toxicol. 1998;12:19–27. doi:10.1016/S0890-6238(97)00096-8
51. Gnoth C, Godehardt D, Godehardt E, Frank-Herrmann P, Freundl G. Time to pregnancy: results of the German prospective study and impact on the management of infertility. Hum Reprod. 2003;18:1959–1966. doi:10.1093/humrep/deg366
52. Gruener N, Shuval HI, Behroozi K, Cohen S, Shechter H. Methemoglobinemia induced by transplacental passage of nitrites in rats. Bull Environ Contam Toxicol. 1973;9:44–48. doi:10.1007/BF01856770
53. Inui N, Nishi Y, Taketomi M, et al. Transplacental mutagenesis of products formed in the stomach of golden hamsters given sodium nitrite and morpholine. Int J Cancer. 1979;24:365–372. doi:10.1002/ijc.2910240316
54. Poulsen R, Cedergreen N, Hayes T, Hansen M. Nitrate: an environmental endocrine disruptor? A review of evidence and research needs. Environ Sci Technol. 2018;52:3869–3887. doi:10.1021/acs.est.7b06419
55. Skrivan J. Methemoglobinemia in pregnancy (clinical and experimental study). Acta Univ Carol Med. 1971;17:123–161.
56. Sleight SD, Atallah OA. Reproduction in the Guinea pig as affected by chronic administration of potassium nitrate and potassium nitrite. Toxicol Appl Pharmacol. 1968;12:179–185. doi:10.1016/0041-008X(68)90029-X
57. Attia YA, Abd El Hamid EA, Ismaiel AM, El-Nagar A. The detoxication of nitrate by two antioxidants or a probiotic, and the effects on blood and seminal plasma profiles and reproductive function of New Zealand white rabbit bucks. Animal. 2013;7:591–601. doi:10.1017/S1751731112002054
58. Hansen PR, Taxvig C, Christiansen S, et al. Evaluation of endocrine disrupting effects of nitrate after in utero exposure in rats and of nitrate and nitrite in the H295R and T-screen assay. Toxicol Sci. 2009;108:437–444. doi:10.1093/toxsci/kfp023
59. Kuh D, Ben-Shlomo Y, Lynch J, Hallqvist J, Power C. Life course epidemiology. J Epidemiol Community Health. 2003;57:778–783. doi:10.1136/jech.57.10.778
60. Lanciotti L, Cofini M, Leonardi A, Penta L, Esposito S. Up-to-date review about minipuberty and overview on hypothalamic-pituitary-gonadal axis activation in fetal and neonatal life. Front Endocrinol. 2018;9. doi:10.3389/fendo.2018.00410
61. Hord NG, Tang Y, Bryan NS. Food sources of nitrates and nitrites: the physiologic context for potential health benefits. Am J Clin Nutr. 2009;90:1–10. doi:10.3945/ajcn.2008.27131
62. Erlangsen A, Fedyszyn I. Danish nationwide registers for public health and health-related research. Scand J Public Health. 2015;43:333–339. doi:10.1177/1403494815575193
63. Wilcox AJ, Weinberg CR, O’Connor JF, et al. Incidence of early loss of pregnancy. N Engl J Med. 1988;319:189–194. doi:10.1056/NEJM198807283190401
64. Wilcox AJ, Harmon Q, Doody K, Wolf DP, Adashi EY. Preimplantation loss of fertilized human ova: estimating the unobservable. Hum Reprod. 2020;35:743–750.
65. Danish Fertility Association. Annual report 2019. Danish. Available from: https://fertilitetsselskab.dk/wp-content/uploads/2020/10/dfs2019-til-hjemmesiden.pdf.
66. Leung M, Kioumourtzoglou MA, Raz R, Weisskopf MG. Bias due to selection on live births in studies of environmental exposures during pregnancy: a simulation study. Environ Health Perspect. 2021;129:47001. doi:10.1289/EHP7961
67. Liew Z, Olsen J, Cui X, Ritz B, Arah OA. Bias from conditioning on live birth in pregnancy cohorts: an illustration based on neurodevelopment in children after prenatal exposure to organic pollutants. Int J Epidemiol. 2015;44:345–354. doi:10.1093/ije/dyu249
68. Save-Soderbergh M, Toljander J, Mattisson I, Akesson A, Simonsson M. Drinking water consumption patterns among adults-SMS as a novel tool for collection of repeated self-reported water consumption. J Expo Sci Environ Epidemiol. 2018;28:131–139. doi:10.1038/jes.2017.8
69. Rygaard M, Arvin E, Binning PJ. The valuation of water quality: effects of mixing different drinking water qualities. Water Res. 2009;43:1207–1218. doi:10.1016/j.watres.2008.12.014
70. Union of European Soft Drinks Associations. Industry volume data: Denmark. Vol 2021. Available from: https://www.unesda.eu/consumption/.
71. Falba TA, Sindelar JL. Spousal concordance in health behavior change. Health Serv Res. 2008;43:96–116. doi:10.1111/j.1475-6773.2007.00754.x
72. Meyler D, Stimpson JP, Peek MK. Health concordance within couples: a systematic review. Soc Sci Med. 2007;64:2297–2310. doi:10.1016/j.socscimed.2007.02.007
73. Hvidtjorn D, Grove J, Schendel D, et al. Validation of self-reported data on assisted conception in the Danish national birth cohort. Hum Reprod. 2009;24:2332–2340. doi:10.1093/humrep/dep179
74. Cooney MA, Buck Louis GM, Sundaram R, McGuiness BM, Lynch CD. Validity of self-reported time to pregnancy. Epidemiology. 2009;20:56–59. doi:10.1097/EDE.0b013e31818ef47e
75. Hansen B, Sonnenborg TO, Moller I, et al. Nitrate vulnerability assessment of aquifers. Environ Earth Sci. 2016;75:999. doi:10.1007/s12665-016-5767-2
76. Moller H, Landt J, Pedersen E, Jensen P, Autrup H, Jensen OM. Endogenous nitrosation in relation to nitrate exposure from drinking water and diet in a Danish rural population. Cancer Res. 1989;49:3117–3121.
77. Chen SX, Rasmussen KM, Finkelstein J, Stovring H, Nohr EA, Kirkegaard H. Maternal reproductive history and premenopausal risk of hypertension and cardiovascular disease: a Danish cohort study. BMJ Open. 2019;9:e030702. doi:10.1136/bmjopen-2019-030702
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.