Back to Journals » Journal of Inflammation Research » Volume 15
Neutrophil to High-Density Lipoprotein Ratio is Associated with Hemorrhagic Transformation in Patients with Acute Ischemic Stroke
Authors Zhang R, Jin F, Zheng L ![]() , Liao T
, Liao T ![]() , Guan G
, Guan G ![]() , Wang J, Zhao S, Fei S, Chu Z, Xu Y
, Wang J, Zhao S, Fei S, Chu Z, Xu Y
Received 6 July 2022
Accepted for publication 18 October 2022
Published 4 November 2022 Volume 2022:15 Pages 6073—6085
DOI https://doi.org/10.2147/JIR.S381036
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Ruirui Zhang,1 Fanfu Jin,1 Lanlan Zheng,1 Tingwei Liao,1 Guangling Guan,1 Jianfei Wang,1 Shoucai Zhao,1 Shizao Fei,2,* Zhaohu Chu,1,* Yang Xu1,3,*
1Department of Neurology, The First Affiliated Hospital of Wannan Medical College, Wuhu, People’s Republic of China; 2Wuhu Hospital, East China Normal University, Wuhu, People’s Republic of China; 3Key Laboratory of Non-coding RNA Transformation Research of Anhui Higher Education Institutes, Wannan Medical College, Wuhu, Anhui Province, China; Department of Neurology, The First Affiliated Hospital of Wannan Medical College, Wuhu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yang Xu; Zhaohu Chu, Department of Neurology, The First Affiliated Hospital of Wannan Medical College, Wuhu, Anhui, 241000, People’s Republic of China, Tel/Fax +86 0553-5739542, Email [email protected]; [email protected]
Background: Hemorrhagic transformation (HT) is one of the most common and severe complications in patients with acute ischemic stroke (AIS). It indicates a poor prognosis in AIS patients. However, the association of neutrophil to high-density lipoprotein ratio (NHR) with HT remains unclear.
Purpose: This study examined whether the NHR has a predictive effect on HT in AIS patients and explored the predictive cutoff value of the NHR.
Methods: This is a retrospective study and consecutively included AIS patients admitted to the Department of Neurology of the First Affiliated Hospital of Wannan Medical College between December 2019 and January 2022. All subjects had blood samples collected within 24 h of admission, and neutrophil counts and high-density lipoprotein counts were detected. HT was diagnosed with hemorrhage on subsequent magnetic resonance imaging (MRI) or computed tomography (CT) of the brain. Univariate logistic regression analysis was performed to identify confounding factors, and multivariate logistic regression analysis determined the correlation between NHR and HT. Receiver operating characteristic (ROC) curves were used to evaluate the clinical predictive value of NHR.
Results: A total of 725 patients were finally included in this study, of which 87 (12%) developed HT. The median NHR value in the HT group was 4.31, which was significantly higher than that in the non-HT group, and the difference was statistically significant [4.31 (3.54– 6.24) vs 3.63 (2.68– 4.64), p < 0.001]. The binary logistic regression analysis showed that NHR was independently associated with HT in AIS patients (OR: 1.180, 95% CI: 1.036– 1.344, p = 0.013). The area under ROC curve (AUC) of NHR for predicting HT in AIS patients was 0.633 (95% CI: 0.567– 0.699, p < 0.001), and its optimal cutoff were 3.52.
Conclusion: The NHR was a reliable and simple independent predictor of HT in AIS patients.
Keywords: neutrophil to high-density lipoprotein ratio, neutrophil, high-density lipoprotein cholesterol, hemorrhagic transformation, acute ischemic stroke, neuroinflammation
Introduction
HT is one of the most severe and common complications of AIS,1 and its incidence accounts for 10–40% of AIS patients, leading to increased morbidity and mortality.2 HT is associated with poor clinical outcomes in patients with AIS and often results in additional brain injury and severe neurological deficit symptoms.3 Few effective biological predictive markers have been identified to assist neurologists in determining which AIS patients are most likely to develop HT. Therefore, early identification of AIS patients at risk of HT may have important clinical implications and contribute to the scientific basis for the treatment decision-making of AIS.
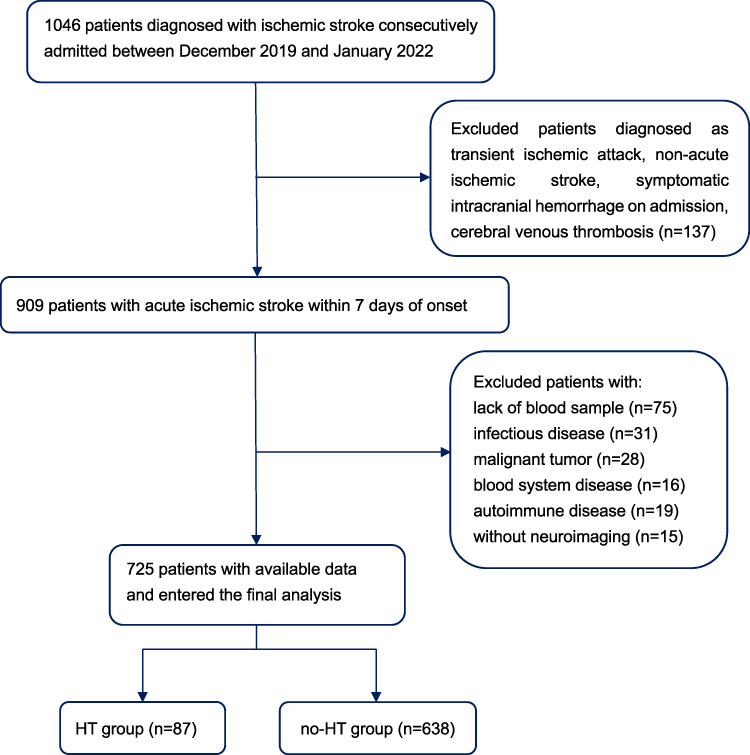 |
Figure 1 Flow chart of the study selection. Abbreviation: HT, hemorrhagic transformation. |
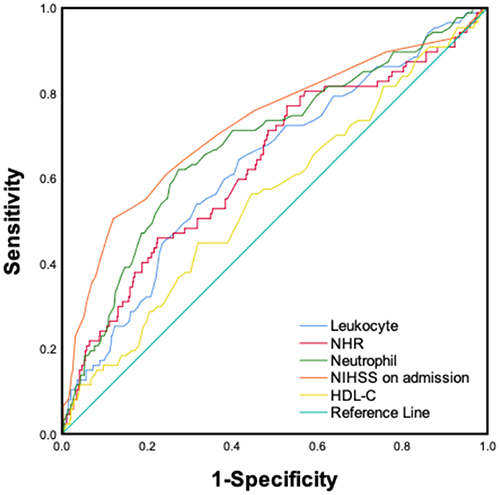 |
Figure 2 ROC curves of NHR, leukocyte, neutrophil, HDL-C and NIHSS on admission predicting HT. Data were analyzed with SPSS statistics software by Ruirui Zhang. Abbreviations: NHR, neutrophil to high-density lipoprotein ratio; ROC, Receiver operating characteristic, NIHSS, National Institutes of Health Stroke Scale, HDL-C, high-density lipoprotein cholesterol. |
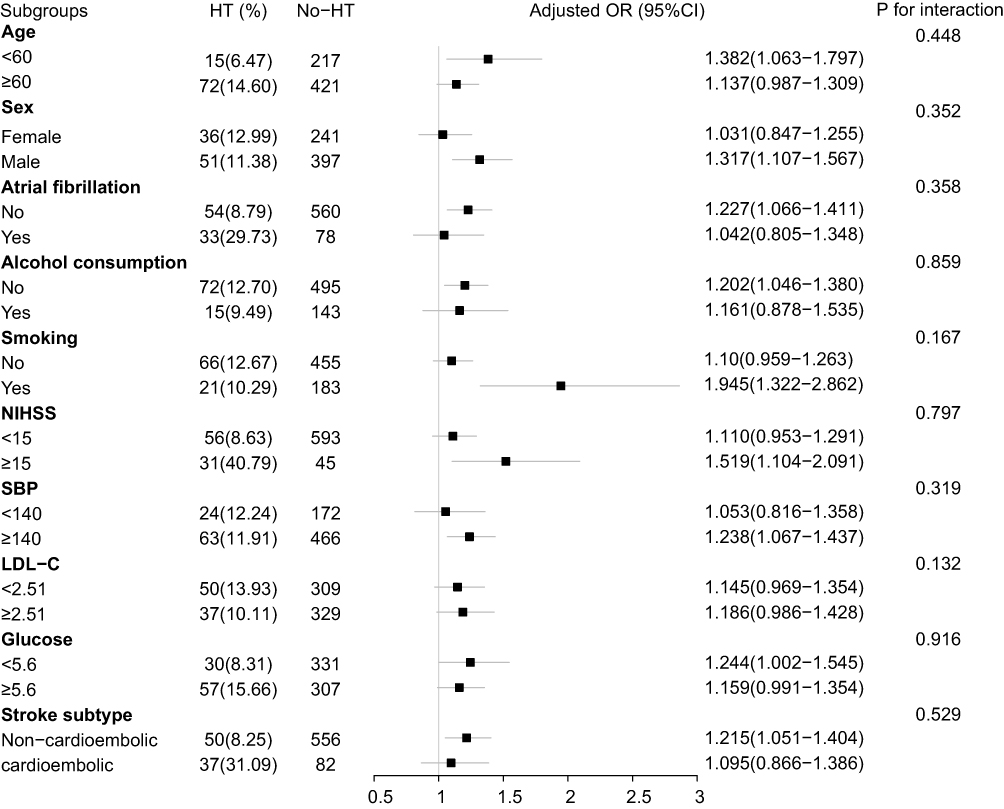 |
Figure 3 Stratified logistic regression analysis model to explore variables affecting the correlation between NHR and HT. Above model adjusted for age, sex, atrial fibrillation, alcohol consumption, smoking, NIHSS, SBP, LDL-C, glucose, and stroke subtype. Abbreviations: NHR, neutrophil to high-density lipoprotein ratio; HT, hemorrhagic transformation; OR, odds ratio; NIHSS, National Institutes of Health Stroke Scale; SBP, systolic blood pressure; LDL-C, low-density lipoprotein cholesterol. Notes: In each subgroup analysis, the model was not adjusted for stratification variables. |
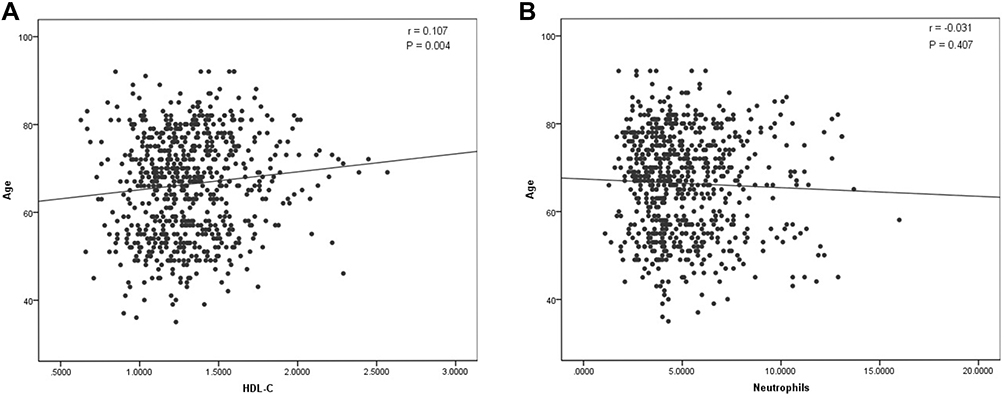 |
Figure 4 Correlation between age and neutrophils and HDL-C in AIS patients (A and B). (A) There was a positive correlation between age and HDL-C: r = 0.107, P = 0.004; (B) There was no correlation between age and neutrophils: r = 0.031, P = 0.407. Abbreviation: HDL-C, high-density lipoprotein cholesterol. |
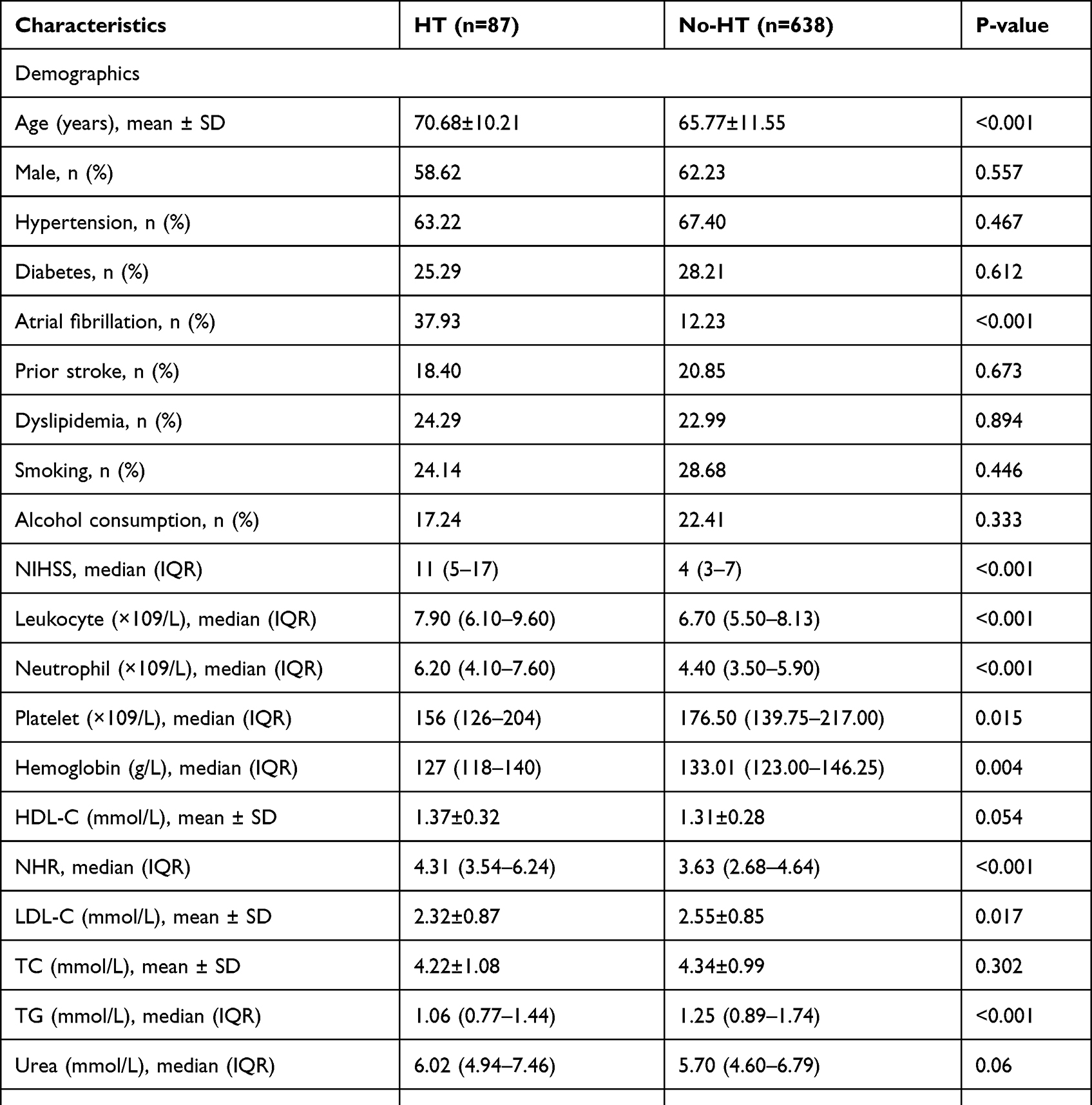 |
Table 1 Baseline Characteristics and Clinical Data of Enrolled Patients |
 |
Table 2 The Predictive Value of NHR for HT in AIS Patients |
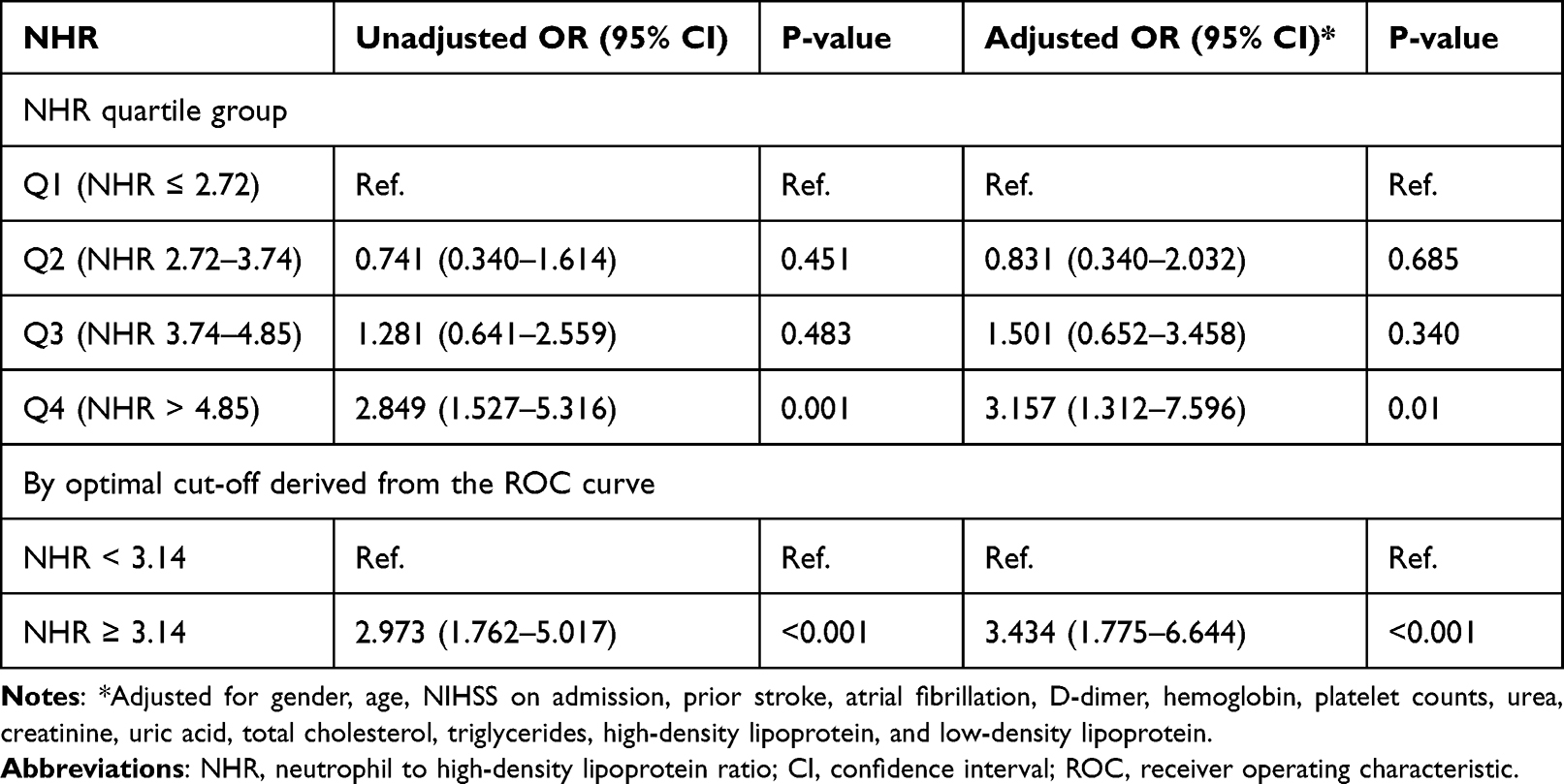 |
Table 3 Multivariate Logistic Analysis to Determine Associations Between NHR Subgroup Levels and HT |
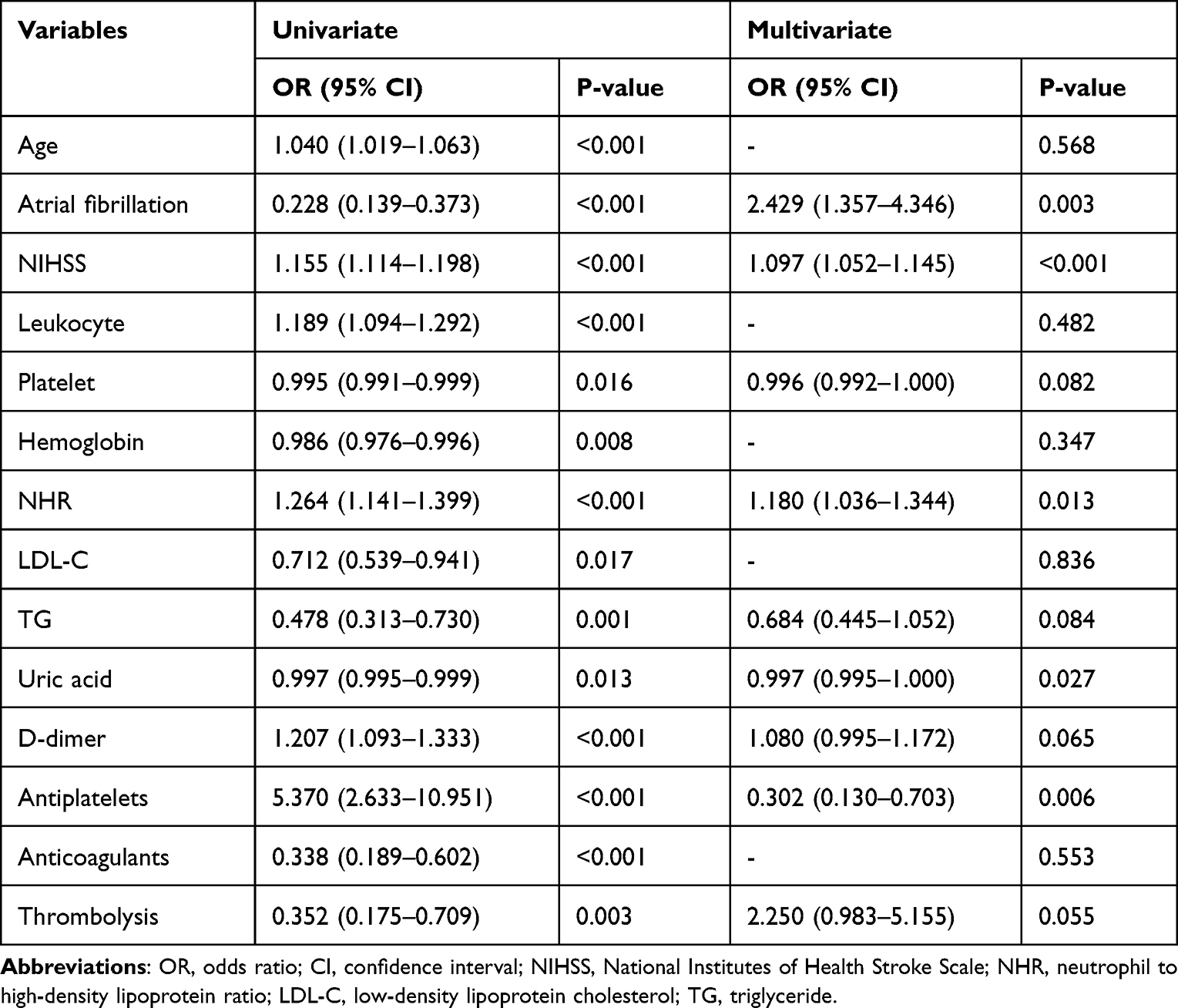 |
Table 4 Univariate and Multivariate Logistic Regression Analysis for the Risk Factors of HT |
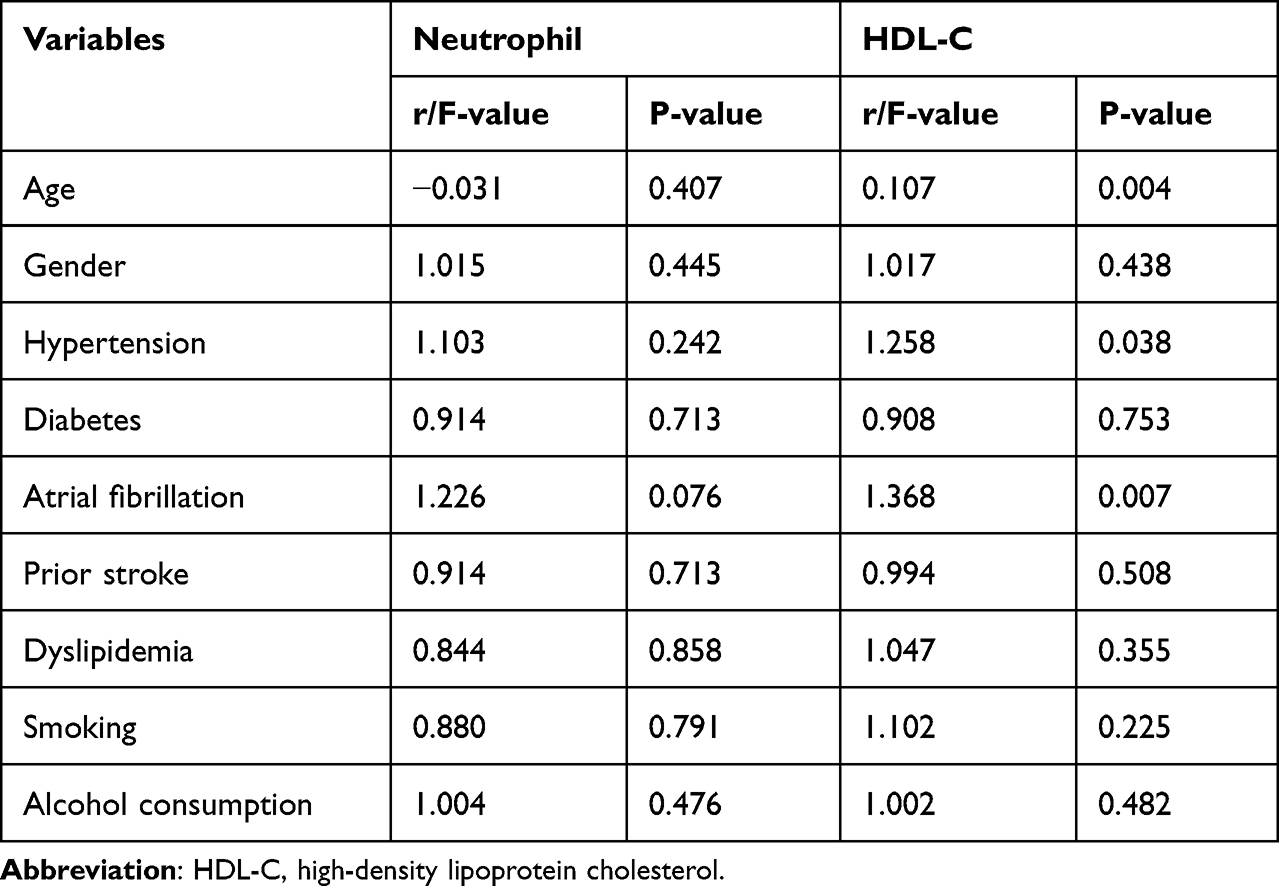 |
Table 5 Correlation Between Neutrophil or HDL-C and Risk Factors of AIS |
HT occurs spontaneously or is induced or exacerbated by multiple factors, including clinical interventions.4 HT was classified as type 1 and 2 hemorrhagic infarction (HI) and type 1 and 2 parenchymal hematomas (PH) in the European Cooperative Acute Stroke Study I (ECASS I).5 The blood-brain barrier (BBB) disruption has been confirmed to be a fundamental mechanism of HT in patients with AIS.6 Both animal and human studies have revealed that proteolysis of the matrix metalloproteinase (MMPs) plays a considerable role in the breakage of BBB.7 Turner et al,8 proved that matrix metalloproteinase 9 (MMP-9), the critical substance of MMPs proteolytic activity, increases the risk of HT by degrading BBB components. Polymorphonuclear neutrophils impair BBB integrity in the first few days after ischemic stroke by producing MMPs, proteases, elastases, and reactive oxygen species (ROS).9 Neutrophils are the primary source of MMP-9, which can promote the destruction of the BBB through direct or indirect mechanisms in the early stage of ischemia, which is the crucial reason for HT.10 High neutrophil counts are independently associated with HT.10,11 However, the changes in peripheral leukocyte count in patients with AIS may be caused by a sterile inflammatory response and the occurrence of early infection. Semerano et al,12 identified a pre-existing infection and early infection after AIS as potential confounders in assessing the association between neutrophil counts and HT, demonstrating that neutrophil count is a potential predictor of HT independent of early post-stroke infection.
The inflammatory response and lipid accumulation play an important role in atherosclerosis formation in stroke development.13 High-density lipoprotein cholesterol (HDL-C), the primary type of human serum lipid profile, has long been recognized as a protective factor that can lower the risk of cardiovascular disease.14–17 Lin et al,18 have validated the correlation between serum lipid profiles and HT. Furthermore, a study that included 22,216 patients who received thrombolytic therapy demonstrated that higher levels of HDL-C are an independent risk factor for increased HT risk.19 However, Rocco et al reported that low HDL-C is independently associated with mortality in AIS patients.20 In addition, studies indicated that HDL-C levels have no association with HT or adverse functional outcomes after thrombolytic therapy for AIS.21 Consequently, the correlation between HDL-C and HT remains controversial.
Existing clinical and basic research has shown that HDL-C can influence the composition and activity of HDL-C by modulating the functional responses of activated neutrophils during inflammation.22,23 NHR, a new biological marker that can reflect inflammation and the lipid profile level, is independently associated with acute myocardial infarction.24 Furthermore, NHR has been demonstrated to be an independent predictor of coronary artery stenosis.25 However, limited studies addressed the association between NHR and HT. Therefore, we aimed to investigate whether NHR’s predictive effect on HT in patients with AIS and clarify its optimal predictive cutoff value.
Materials and Methods
Study Population
This study data were consecutively collected from AIS patients admitted to the Department of Neurology of the First Affiliated Hospital of Wannan Medical College between December 2019 and January 2022. The Medical Research Ethics Committee approved the hospital study (Code: 2020 Lun Shen No. 30). All study subjects or guardians obtained informed consent. The diagnosis of AIS was based on the World Health Organization criteria and confirmed by neuroimaging.26 Inclusion criteria for patients included the following: (1) over 18 years old; (2) ischemic stroke patients within 7 days after symptom onset; (3) The diagnostic criteria of AIS are based on the Guidelines for the Early Management of Adults With Ischemic Stroke developed by the American Heart Association/American Stroke Association (AHA/ASA)27 and confirmed by imaging evidence such as head CT or MRI;28 (4) perform initial brain CT scan within 24 h of admission, and complete MRI or repeat CT within 7 days of admission to prevent sudden neurological deterioration. Exclusion criteria included: (1) bleeding found on CT of the brain at admission; (2) missing repeat head CT or MRI during hospitalization; (3) missing blood sample within 24 h of admission.
Data and Blood Sample Collection
The clinical baseline data were collected, including demographics (sex and age); past medical history (hypertension, diabetes, atrial fibrillation, prior stroke, dyslipidemia, and history of smoking and drinking); laboratory data (leukocyte, neutrophil, platelet, hemoglobin, HDL-C, low-density lipoprotein cholesterol, NHR, total cholesterol, triglycerides, urea, uric acid, creatinine, glucose, d-dimer); systolic blood pressure (SBP) and diastolic blood pressure (DBP) at admission and treatment during the hospitalization. Specially trained neurologists classified stroke etiology using the Trial of ORG 10,172 in Acute Stroke Treatment (TOAST) classification29 and assessed the severity of neurological deficits in stroke at baseline using the NIHSS. In addition, 5 mL of venous blood was collected from all patients within 24 h of admission. The hematological parameters were detected by laser flow cytometry using a Mindray CAL 8000 hematology analyzer (Shenzhen Mindray Biomedical, China). NHR was calculated by dividing neutrophil counts by HDL-C levels.
Definition of HT
All subjects received brain CT on admission and brain MRI or CT within seven days, with repeated CT at any time if clinical function deteriorated. HT includes hemorrhagic infarction (HI) and parenchymal hematoma (PH) based on the European Cooperative Acute Stroke Study I (ECASS I).5 Hemorrhage due to any deterioration in neurological function is considered symptomatic HT. The criteria for deterioration were compared with the neurological status before exacerbation. The total NIHSS score rose by 4 points, or the individual score rose by 2 or more. Our study’s endpoint was HT, defined as hemorrhage in brain tissue within the infarcted area of hemorrhage in the brain parenchyma outside the infarcted area that was undetected on brain CT at admission but was later detected on subsequent CT or MRI. HT was adjudicated by two professional neurologists blinded to this study’s data. Any differences were resolved by consensus or consultation with a third neurologist.
Statistical Analysis
Normally distributed continuous variables were described by mean ± standard deviation and used Student’s t-test and Mann–Whitney U-test for statistical analysis. The median of the interquartile range was used to describe non-normally distributed continuous variables, and statistical analysis was performed by rank-sum test. Percentages were used to describe categorical variables and compared using the chi-square or Fisher’s exact test. We first performed a univariate logistic regression analysis. We included variables with p < 0.05 in multivariate logistic regression for further analysis to explore potential confounding factors affecting the association between NHR levels and HT. Next, subgroup analysis was performed using a stratified logistic regression model to investigate the correlation between NHR and HT. Likelihood ratio tests were used to detect the interactions between NHR and others, each stratification factor on HT (p for interaction). Finally, the ANOVA and Spearman correlation coefficient was computed to calculate the correlation between risk factors for AIS and neutrophil or HDL-C value. All data analyses were performed using SPSS 26.0 (IBM Corp, Armonk, NY, USA) and R 4.1.0 (R Foundation for Statistical Computing, Vienna, Austria). Two-sided tests were used for all statistical tests, and P-values < 0.05 were considered statistically significant.
Results
Clinical Baseline Characteristics
A total of 1046 patients were admitted to our hospital at the beginning of the study, 321 met the exclusion criteria, and 725 were finally included (Figure 1). Clinical baseline demographics and laboratory data were collected from all patients (Table 1). Patients were divided into two groups according to HT occurrence. Among 725 patients in this study, 87 developed HT at a rate of 12%, including 22 (3%) type 1 hemorrhagic infarction (HI-1) and 31 (4.3%) type 2 hemorrhagic infarction (HI-2), 24 (3.3%) cases of parenchymal hematoma type 1 (PH-1) and 10 (1.4%) cases of parenchymal hematoma type 2 (PH-2). Non-significant differences existed in gender, vascular risk factors such as hypertension, diabetes, hyperlipidemia, and personal smoking and drinking history in the two groups’ demographic data (all P > 0.05).
However, the mean age and atrial fibrillation proportion in the HT group were significantly higher than that in the without HT group (70.68 ± 10.21 vs 65.77 ± 11.55 and 37.93 vs 12.23, both p < 0.001). Furthermore, the comparison between the two groups showed that the median NHR in the HT group was 4.31, which was significantly higher than the 3.63 of the non-HT group, and the difference was statistically significant [4.31 (3.54–6.24) vs 3.63 (2.68–4.64), p < 0.001, Table 1]. In addition, the HT group was more likely to have higher baseline NIHSS scores, higher baseline white blood cell, neutrophil count, blood glucose and d-dimer levels, lower baseline platelet, hemoglobin, low-density lipoprotein-cholesterol (LDL-C), triglycerides, and uric acid levels, lower antiplatelet therapy, higher anticoagulation, and reperfusion therapy after admission, and TOAST classification of cardioembolic in the laboratory data of the two groups of patients (all P < 0.05).
ROC Curve Analysis
The receiver operating characteristic (ROC) curve was used to determine each independent risk factor’s predictive power for HT and its predictive value. The best predictive cutoffs for HT by NHR, leukocyte counts, neutrophil counts, and NIHSS scores were 3.52, 7.15, 5.65, and 10.5, respectively, and the differences were all statistically significant (all P < 0.05, Figure 2). Based on the ROC curves (Table 2), the predictive cutoff value of HDL-C for HT was 1.39 (sensitivity 44.8%, specificity 68.0%). ROC curve analysis results also showed that the area under the curve of NHR for predicting HT was 0.633 (95% CI: 0.567–0.699, p < 0.001), with a maximum cutoff value of 3.52 for Youden’s index of 0.242, with a sensitivity of 77% and specificity of 52.8% (Table 2). Consequently, NHR was a significant independent predictor of HT, with a best predictive value of 3.52.
Univariate and Multivariate Logistic Regression Analyses
Univariate and multivariate logistic regression analyses were performed to explore possible risk factors associated with HT. The univariate logistic regression analysis revealed that possible risk factors associated with HT included age, NHR, atrial fibrillation, baseline NIHSS scores, leukocyte counts, platelet counts, hemoglobin, LDL-C and uric acid levels, triglycerides, D-dimer, antiplatelets, anticoagulants, and thrombolysis therapy (all P < 0.05, Table 3). We adjusted for confounding factors which are defined as the non-primary study factors in the regression model in the multivariate logistic regression analysis, and the results revealed that NHR, as a continuous variable, was significantly negatively correlated with HT (OR: 1.180, 95% CI:1.036–1.344, p=0.013). Concurrently, atrial fibrillation (OR: 2.429, 95% CI: 1.357–4.346, p = 0.003), the baseline NIHSS scores (OR: 1.097, 95% CI: 1.052–1.145, p = 0.003), uric acid (OR: 0.997, 95% CI: 0.995–1.000, p = 0.027) and antiplatelets therapy (OR: 0.302, 95% CI: 0.130–0.703, p = 0.006) were also independent predictors of HT. Moreover, we found that the best cutoff value of NHR for predicting HT in AIS patients was 3.52, with a sensitivity of 77%.
To demonstrate the association of NHR with HT, all patients were divided into four groups according to the quartile values of NHR (Q1: NHR ≤ 2.72, Q2: NHR 2.72–3.74, Q3: NHR 3.74–4.85, Q4: NHR > 4.85, Table 4). The OR value of HT in the highest quartile compared with the lowest quartile was 2.849 (95% CI: 1.527–5.316, p = 0.001). After adjusting for gender, age, NIHSS on admission, prior stroke, atrial fibrillation, D-dimer, hemoglobin, platelet counts, urea, creatinine, uric acid, total cholesterol, triglycerides, HDL, and LDL, the risk of HT remained significantly higher in the highest quartile than in the lowest quartile (OR: 3.157, 95% CI: 1.312–7.596, p = 0.01). Finally, all patients were divided into two groups according to the cutoff value derived from the ROC curve of NHR (NHR < 3.52 and NHR ≥ 3.52). The risk of HT in the subgroup with NHR greater than 3.14 was significantly higher than in the group with NHR less than 3.14 (OR: 2.973, 95% CI: 1.762–5.017, p < 0.001). After further adjusting for the above confounding factors, the risk of HT in the NHR ≥ 3.14 group remained significantly higher than that in NHR < 3.14 group and the difference was statistically significant (OR: 3.434, 95% CI: 1.775–6.644, p < 0.001, Table 4).
Subgroup Analyses
Herein, subgroup analysis displayed that the tests for the interaction of age (< 60 vs ≥ 60), sex (female vs male), atrial fibrillation, alcohol consumption, smoking, NIHSS scores (< 15 vs ≥ 15), systolic blood pressure (< 140 vs ≥ 140), HDL-C levels (< 2.51 vs ≥ 2.51), glucose level (< 5.6 vs ≥ 5.6) and stroke subtype on the related effects of NHR and HT were non-significant statistically (all p for interaction > 0.05, Figure 3). The results showed that the various stratification factors in the model unaffected the correlation between NHR and HT.
Correlation Analysis Between Neutrophil or HDL and Risk Factors of AIS
We explored the effect of common risk factors for AIS on neutrophil and HDL-C values. Our analysis showed that Neutrophil has a non-significant association with common risk factors for AIS, including age, gender, hypertension, diabetes, atrial fibrillation, prior stroke, dyslipidemia, smoking, and alcohol consumption (all r/F value for correlation > 0.05, Table 5). A positive correlation existed between age and HDL-C in our population (r = 0.107, p = 0.004, Figure 4). Conversely, there was no correlation between age and neutrophils (r = 0.031, P = 0.407, Figure 4). Herein, we also found a weak but significant positive correlation between atrial fibrillation and HDL-C (F = 1.368, p = 0.007, Table 5).
Discussion
In this retrospective study of 725 patients, HT occurred in 87 individuals, and the rate was 12%, consistent with the incidence rates reported in previous studies. Herein, we first examined whether NHR is linked to HT in AIS patients. We found that higher NHR values on admission were independently associated with an increased risk of HT in patients with AIS and the best-predicted value was 3.14. The findings of our study suggested that after adjustment for confounding factors, AIS patients with high NHR levels (≥ 3.14) had an approximately 3.4-fold higher risk of developing HT than patients with low NLR levels (< 3.14). Consequently, NHR can be used as a simple and efficient independent predictor of HT.
Li and Nakamura et al,30,31 have recently focused on the relationship between inflammatory and lipid-related biomarkers and cerebrovascular diseases. Inflammatory responses and abnormal lipid-related metabolism play critical roles in the pathophysiology of atherosclerosis. Previous studies have revealed that inflammatory response plays a vital role in the process of thrombosis in the body, and thrombus can induce thrombotic inflammatory response related to the degree of tissue organ damage and clinical and functional outcome by recruiting leukocytes.32 Neutrophils are the primary source of MMP-9 that leads to the disruption of BBB in the early stage of AIS.2 A study based on an inflammatory model in vitro and in vivo displayed that neutrophils play a pathogenic role in the immune-inflammatory response in atherosclerosis pathogenesis.33 Neutrophils are one of the first cells to react in the blood after an ischemic stroke. They can lead to the breakdown of the BBB and brain damage by mediating various inflammatory factors such as ROS, proteases, and cytokines.34,35 Neutrophil extracellular traps (NETs) are extracellular DNA lattices produced after the overactivation of neutrophils, which can trap other blood cells, leading to pathological thrombosis that exacerbates the neuroinflammatory response.36,37 Puy and Denorme found evidence of neutrophils and NETs in the brain tissue of patients with spontaneous intracerebral hemorrhage and AIS, which were associated with clinical outcomes.38,39 HDL-C’s reverse cholesterol transport function transports excess cholesterol from peripheral tissues back to the liver for excretion.40
HDL-C has anti-atherosclerotic and anti-inflammatory effects of reducing the BBB disruption in AIS patients.41 Secretory phospholipase A2 modification of HDL-C produces an anti-inflammatory granule that modulates neutrophil effector responses during inflammation by inhibiting neutrophil activation, adhesion, migration, and extracellular trap formation.22 In turn, neutrophils promote atherosclerosis in stroke patients by interacting with platelets, releasing cytokines, activating macrophages, producing low-density lipoprotein, and degrading fibronectin.35 To summarize, elevated NHR in patients with AIS may be associated with abnormal lipid metabolism and inflammatory activity due to reduced HDL-C levels and increased neutrophil counts. Consequently, we hypothesized that NHR is a novel composite biomarker that can more comprehensively reflect the state of inflammation and lipid metabolism than a single biomarker.
Furthermore, NHR was an independent predictor of acute myocardial infarction and coronary stenosis and closely related to the prognosis and severity of cardiovascular disease.24,25 In addition, Chen et al,42 demonstrated that higher levels of NHR at admission are associated with poorer outcomes three months after intravenous thrombolysis in patients with AIS. Nevertheless, whether NHR is independently associated with HT in AIS patients remains unclear. Therefore, this study aims to explore whether NLR can be used as a biological indicator that has predictive value for HT in AIS patients.
Our study excluded 184 patients with incomplete clinical data, infection at admission, blood disease, and an autoimmune disease that may affect inflammation and lipid indicators to explore the relationship between NHR and HT Relationship. In addition, due to the significant collinearity between neutrophil count and other independent variables, this study excluded neutrophil count as an independent variable in the regression equation to eliminate the collinearity between white blood cell indicators.
Our results disclosed that the neutrophil count on admission was significantly higher in the HT group than in the non-HT group (p < 0.001), suggesting that neutrophils on admission may serve as an independent risk factor for HT. However, HDL-C levels on admission were non-significantly different between the two groups. This is contrary to the protective role of HDL-C in atherosclerosis and inflammation, which may be related to the study’s small sample size. Further studies with large samples are needed to explore the role of HDL-C in HT. Univariate and multivariate logistic regression analyses incorporating a variety of HT-related factors revealed that NHR was statistically associated with HT, and NHR was an independent predictor of HT after controlling for relevant confounders (OR: 1.180, 95% CI: 1.036–1.344, p = 0.013). Herein, we found that the best cutoff value of NHR for predicting HT in AIS patients was 3.52, with a sensitivity of 77% (AUC: 0.633, 95% CI: 0.567–0.699, p < 0.001).
Above all, NHR, a novel serum biomarker, has the advantages of simplicity, speediness, and efficiency, which can be used as a potential biological therapeutic target for judging the prognosis of AIS patients. NHR has a particular promotion value in clinical work, and it can assist clinicians in identifying high-risk AIS patients with HT early, allowing them to develop individualized diagnoses and treatment plans for patients more safely and effectively. Nonetheless, the specific mechanism of action of neutrophils and HDL-C in HT remains unclear, and further studies are required to explore the underlying mechanisms in animals and humans.
Although this is the first study to explain NHR-HT correlation, we must acknowledge that it has some limitations. First, we used a retrospective study protocol with a relatively small sample size based on a single-center database. The findings may be unable to be generalized to all Chinese and other ethnic groups. Therefore, a large sample multicenter prospective study is needed to verify the accuracy and reliability of the results. This study is a retrospective and non-prespecified analysis, which may have some selection bias, so prospective intervention cohort studies are needed to confirm our findings. Second, Second, our study dynamically undetected the effect of NHR changes on HT in AIS patients because it is uncertain whether temporal changes in NHR are related to HT. Finally, the specific mechanism of the association between NHR and HT is still unclear. Therefore, further clinical and experimental studies are needed to clarify its pathogenesis and validate our results.
Conclusion
A higher NHR value at admission was an independent predictor of HT in AIS, with a best predictive value of 3.52. We believe that NHR may serve as a potential biomarker to identify AIS patients at higher risk for HT, allowing clinicians to personalize care and avoid possible bleeding complications.
Data Sharing Statement
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of the First Affiliated Hospital of Wannan Medical College (Code: 2020-30). The study was conducted according to the ethical standard criteria set by the Declaration of Helsinki.
Acknowledgments
This research was supported by the National Natural Science Foundation of China (82170368, 81701161); the Open Project of Key Laboratory of Non-coding RNA Transformation Research of Anhui Higher Education Institution (Wannan Medical College) (RNA202201); Education Department of Anhui Province, China (KJ2021ZD0096); Wannan Medical College, Anhui, China (WK2022F07, YR201802, KGF2019G02, WK2022ZF16, WK2022ZF23 and WK2022F23). We thank X-way group assistance for design this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Castro P, Azevedo E, Serrador J, Rocha I, Sorond F. Hemorrhagic transformation and cerebral edema in acute ischemic stroke: link to cerebral autoregulation. J Neurol Sci. 2017;372:256–261. doi:10.1016/j.jns.2016.11.065
2. Jickling GC, Liu D, Stamova B, et al. Hemorrhagic transformation after ischemic stroke in animals and humans. J Cereb Blood Flow Metab. 2014;34(2):185–199. doi:10.1038/jcbfm.2013.203
3. Rao NM, Levine SR, Gornbein JA, Saver JL. Defining clinically relevant cerebral hemorrhage after thrombolytic therapy for stroke: analysis of the National Institute of Neurological Disorders and Stroke tissue-type plasminogen activator trials. Stroke. 2014;45(9):2728–2733. doi:10.1161/STROKEAHA.114.005135
4. Nagaraja N, Tasneem N, Shaban A, et al. Cerebral microbleeds are an independent predictor of hemorrhagic transformation following intravenous alteplase administration in acute ischemic stroke. J Stroke Cerebrovasc Dis. 2018;27(5):1403–1411. doi:10.1016/j.jstrokecerebrovasdis.2017.12.044
5. Fiorelli M, Bastianello S, von Kummer R, et al. Hemorrhagic transformation within 36 hours of a cerebral infarct: relationships with early clinical deterioration and 3-month outcome in the European Cooperative Acute Stroke Study I (ECASS I) cohort. Stroke. 1999;30(11):2280–2284. doi:10.1161/01.STR.30.11.2280
6. Ng FC, Churilov L, Yassi N, et al. Microvascular dysfunction in blood-brain barrier disruption and hypoperfusion within the infarct posttreatment are associated with cerebral edema. Stroke. 2021;53(5):1597–1605.
7. Rosell A, Foerch C, Murata Y, Lo EH. Mechanisms and markers for hemorrhagic transformation after stroke. Acta Neurochir Suppl. 2008;105:173–178.
8. Turner RJ, Sharp FR. Implications of MMP9 for blood brain barrier disruption and hemorrhagic transformation following ischemic stroke. Front Cell Neurosci. 2016;10:56. doi:10.3389/fncel.2016.00056
9. Sarvari S, Moakedi F, Hone E, Simpkins JW, Ren X. Mechanisms in blood-brain barrier opening and metabolism-challenged cerebrovascular ischemia with emphasis on ischemic stroke. Metab Brain Dis. 2020;35(6):851–868. doi:10.1007/s11011-020-00573-8
10. Guo Z, Yu S, Xiao L, et al. Dynamic change of neutrophil to lymphocyte ratio and hemorrhagic transformation after thrombolysis in stroke. J Neuroinflammation. 2016;13(1):199. doi:10.1186/s12974-016-0680-x
11. Song Q, Li Y, Wang Y, Wei C, Liu J, Liu M. Increased neutrophil-to-lymphocyte ratios are associated with greater risk of hemorrhagic transformation in patients with acute ischemic stroke. Curr Neurovasc Res. 2018;15(4):326–335. doi:10.2174/1567202616666181204122457
12. Semerano A, Strambo D, Martino G, et al. Leukocyte counts and ratios are predictive of stroke outcome and hemorrhagic complications independently of infections. Front Neurol. 2020;11:201. doi:10.3389/fneur.2020.00201
13. Malekmohammad K, Bezsonov EE, Rafieian-Kopaei M. Role of lipid accumulation and inflammation in atherosclerosis: focus on molecular and cellular mechanisms. Front Cardiovasc Med. 2021;8:707529. doi:10.3389/fcvm.2021.707529
14. Wang HH, Garruti G, Liu M, Portincasa P, Wang DQ. Cholesterol and lipoprotein metabolism and atherosclerosis: recent advances in reverse cholesterol transport. Ann Hepatol. 2017;16(Suppl 1):S27–S42. doi:10.5604/01.3001.0010.5495
15. Yu C, Wan Y, Xu W, et al. Increased circulating cathepsin L in patients with coronary artery disease. Int Heart J. 2021;62(1):9–15. doi:10.1536/ihj.20-182
16. Zhang Y, Li J, Liu C, et al. High-density lipoprotein cholesterol and the risk of first ischemic stroke in a Chinese hypertensive population. Clin Interv Aging. 2021;16:801–810. doi:10.2147/CIA.S295252
17. Yuan S, Tang B, Zheng J, Larsson SC. Circulating lipoprotein lipids, apolipoproteins and ischemic stroke. Ann Neurol. 2020;88(6):1229–1236. doi:10.1002/ana.25916
18. Lin SF, Chao AC, Hu HH, et al. Low cholesterol levels increase symptomatic intracranial hemorrhage rates after intravenous thrombolysis: a multicenter cohort validation study. J Atheroscler Thromb. 2019;26(6):513–527. doi:10.5551/jat.46151
19. Messe SR, Pervez MA, Smith EE, et al. Lipid profile, lipid-lowering medications, and intracerebral hemorrhage after tPA in get with the guidelines-stroke. Stroke. 2013;44(5):1354–1359. doi:10.1161/STROKEAHA.111.671966
20. Rocco A, Sykora M, Ringleb P, Diedler J. Impact of statin use and lipid profile on symptomatic intracerebral haemorrhage, outcome and mortality after intravenous thrombolysis in acute stroke. Cerebrovasc Dis. 2012;33(4):362–368. doi:10.1159/000335840
21. Lin TC, Lin YK, Chen CI, et al. Serum lipid level is not associated with symptomatic intracerebral hemorrhage after intravenous thrombolysis for acute ischemic stroke. PeerJ. 2018;6:e6021. doi:10.7717/peerj.6021
22. Curcic S, Holzer M, Frei R, et al. Neutrophil effector responses are suppressed by secretory phospholipase A2 modified HDL. Biochim Biophys Acta. 2015;1851(2):184–193. doi:10.1016/j.bbalip.2014.11.010
23. Cogny A, Atger V, Paul JL, Soni T, Moatti N. High-density lipoprotein 3 physicochemical modifications induced by interaction with human polymorphonuclear leucocytes affect their ability to remove cholesterol from cells. Biochem J. 1996;314(Pt 1)):285–292. doi:10.1042/bj3140285
24. Huang JB, Chen YS, Ji HY, et al. Neutrophil to high-density lipoprotein ratio has a superior prognostic value in elderly patients with acute myocardial infarction: a comparison study. Lipids Health Dis. 2020;19(1):59. doi:10.1186/s12944-020-01238-2
25. Kou T, Luo H, Yin L. Relationship between neutrophils to HDL-C ratio and severity of coronary stenosis. BMC Cardiovasc Disord. 2021;21(1):127. doi:10.1186/s12872-020-01771-z
26. Aho K, Harmsen P, Hatano S, Marquardsen J, Smirnov VE, Strasser T. Cerebrovascular disease in the community: results of a WHO collaborative study. Bull World Health Organ. 1980;58(1):113–130.
27. Adams HP, Del Zoppo G, Alberts MJ, et al. Guidelines for the early management of adults with ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: the American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Stroke. 2007;38(5):1655–1711. doi:10.1161/STROKEAHA.107.181486
28. Sacco RL, Kasner SE, Broderick JP, et al. An updated definition of stroke for the 21st century: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2013;44(7):2064–2089. doi:10.1161/STR.0b013e318296aeca
29. Adams HP, Bendixen BH, Kappelle LJ, et al. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke. 1993;24(1):35–41. doi:10.1161/01.STR.24.1.35
30. Li JJ, Gu HQ, Peng YJ, et al. The association of lipid profile and bleeding in patients with minor stroke or transient ischemic attack on antiplatelet therapy: subgroup analysis of CHANCE. Zhonghua Nei Ke Za Zhi. 2018;57(10):723–730. Chinese. doi:10.3760/cma.j.issn.0578-1426.2018.10.006
31. Nakamura A, Otani K, Shichita T. Lipid mediators and sterile inflammation in ischemic stroke. Int Immunol. 2020;32(11):719–725. doi:10.1093/intimm/dxaa027
32. Wang MQ, Sun YY, Wang Y, et al. Platelet-to-neutrophil ratio after intravenous thrombolysis predicts unfavorable outcomes in acute ischemic stroke. Curr Neurovasc Res. 2020;17(4):411–419. doi:10.2174/1567202617666200517111802
33. Jiang M, Sun J, Zou H, et al. Prognostic role of neutrophil to high-density lipoprotein cholesterol ratio for all-cause and cardiovascular mortality in the general population. Front Cardiovasc Med. 2022;9:807339. doi:10.3389/fcvm.2022.807339
34. Segel GB, Halterman MW, Lichtman MA. The paradox of the neutrophil’s role in tissue injury. J Leukoc Biol. 2011;89(3):359–372. doi:10.1189/jlb.0910538
35. Jickling GC, Liu D, Ander BP, Stamova B, Zhan X, Sharp FR. Targeting neutrophils in ischemic stroke: translational insights from experimental studies. J Cereb Blood Flow Metab. 2015;35(6):888–901. doi:10.1038/jcbfm.2015.45
36. Sorvillo N, Cherpokova D, Martinod K, Wagner DD. Extracellular DNA NET-works with dire consequences for health. Circ Res. 2019;125(4):470–488. doi:10.1161/CIRCRESAHA.119.314581
37. Brill A, Fuchs TA, Savchenko AS, et al. Neutrophil extracellular traps promote deep vein thrombosis in mice. J Thromb Haemost. 2012;10(1):136–144. doi:10.1111/j.1538-7836.2011.04544.x
38. Puy L, Corseaux D, Perbet R, Deramecourt V, Cordonnier C, Berezowski V. Neutrophil extracellular traps (NETs) infiltrate haematoma and surrounding brain tissue after intracerebral haemorrhage: a post-mortem study. Neuropathol Appl Neurobiol. 2021;47(6):867–877. doi:10.1111/nan.12733
39. Denorme F, Portier I, Rustad JL, et al. Neutrophil extracellular traps regulate ischemic stroke brain injury. J Clin Invest. 2022;132(10). doi:10.1172/JCI154225
40. Rohatgi A. High-density lipoprotein function measurement in human studies: focus on cholesterol efflux capacity. Prog Cardiovasc Dis. 2015;58(1):32–40. doi:10.1016/j.pcad.2015.05.004
41. Wang Y, Cheng Y, Song Q, et al. The association between monocyte to high-density lipoprotein ratio and hemorrhagic transformation in patients with acute ischemic stroke. Aging. 2020;12(3):2498–2506. doi:10.18632/aging.102757
42. Chen G, Yang N, Ren J, et al. Neutrophil counts to high-density lipoprotein cholesterol ratio: a potential predictor of prognosis in acute ischemic stroke patients after intravenous thrombolysis. Neurotox Res. 2020;38(4):1001–1009. doi:10.1007/s12640-020-00274-1
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Post-Thrombolytic D-Dimer Elevation Predicts Symptomatic Intracranial Hemorrhage and Poor Functional Outcome After Intravenous Thrombolysis in Acute Ischemic Stroke Patients
Jin T, Chen D, Chen Z, Feng D, Zheng M, Wang P, Xu C
Neuropsychiatric Disease and Treatment 2022, 18:2737-2745
Published Date: 22 November 2022
Role of Peripheral Blood Regulatory T Cells and IL-2 in the Collateral Circulation of Acute Ischemic Stroke

Zhang S, Rao C, Wen M, Zhang X, Zha Z, Gu T, Zhu L, Yu C
International Journal of General Medicine 2025, 18:1075-1088
Published Date: 25 February 2025