Back to Journals » Neuropsychiatric Disease and Treatment » Volume 22
Network Analysis of Post-Traumatic Stress Disorder Symptoms Among Trauma-Exposed Older Adults in Rural Communes in Hanoi and Quang Binh, Vietnam
Authors Bich PTN, Hung LX ![]() , Thanh HTK
, Thanh HTK
Received 17 April 2026
Accepted for publication 26 June 2026
Published 15 July 2026 Volume 2026:22 617817
DOI https://doi.org/10.2147/NDT.S617817
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Taro Kishi
Pham Thi Ngoc Bich,1 Le Xuan Hung,2 Ho Thi Kim Thanh1
1Department of Family Medicine, Hanoi Medical University, Hanoi, Vietnam; 2School of Preventive Medicine and Public Health, Hanoi Medical University, Hanoi, Vietnam
Correspondence: Le Xuan Hung, Email [email protected]
Background: Post-traumatic stress disorder (PTSD) is common among trauma-exposed older adults but often under-recognized. Network analysis conceptualizes PTSD as a system of interacting symptoms and identifies the symptoms most central within the network. Evidence from older adults in Vietnam is scarce.
Objective: To estimate the PTSD symptom network and identify the most central symptoms in trauma-exposed older Vietnamese adults.
Methods: Cross-sectional data came from the second wave (2021– 2022) of the Vietnam Health and Aging Study. From 301 community-dwelling adults aged ≥ 60 years, the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) PTSD symptom network was estimated in the 90 participants with complete symptom data. PTSD symptoms were assessed with the Vietnamese-validated PTSD Checklist for DSM-5 (PCL-5). A regularized partial-correlation network (EBICglasso) was estimated from polychoric correlations. Node centrality was quantified using Expected Influence (EI), and stability was assessed using a case-dropping bootstrap.
Results: The network comprised 19 of 20 PCL-5 nodes (D7 unavailable). Persistent negative emotional states (D4; EI = 1.306) and avoidance of trauma-related thoughts or feelings (C1; EI = 1.196) were the most central nodes, followed by psychological cue reactivity (B4; EI = 1.154). Sleep disturbance (E6; EI = 0.664) and physiological cue reactivity (B5; EI = 0.722) were comparatively peripheral. The ranking of the most central nodes was reproducible under the case-dropping bootstrap.
Conclusion: In older Vietnamese adults with lifetime war trauma, cognitive avoidance and persistent negative affect were the most central PTSD symptoms. Because the design was cross-sectional and the rural sample may not be representative, these findings are associational and cannot establish symptom causation or treatment priority. Trauma-focused approaches, including Prolonged Exposure and Cognitive Behavioral Therapy, warrant further evaluation.
Keywords: post-traumatic stress disorder, network analysis, older adults, Vietnam, symptom centrality, cognitive avoidance, negative affect, aging, community-based
Introduction
Post-traumatic stress disorder (PTSD) is a debilitating psychiatric condition that may develop following exposure to traumatic events such as war, natural disasters, or serious injury, with an estimated lifetime prevalence of approximately 3.9% in cross-national general-population surveys.1 According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), PTSD is characterized by four symptom clusters: intrusion, avoidance, negative alterations in cognitions and mood, and alterations in arousal and reactivity.2 PTSD is associated with substantial impairments in psychological well-being, quality of life, and an elevated risk of comorbid psychiatric and physical conditions.3
Older adults worldwide represent a particularly vulnerable population for PTSD, having accumulated multiple traumatic exposures across the lifespan-including war, forced migration, poverty, and major life stressors.4,5 Age-related biological vulnerability, chronic comorbidities, cognitive decline, and social isolation may increase susceptibility to PTSD and contribute to poorer health outcomes; nonetheless, past-year PTSD prevalence is generally lower among older than among younger adults, reflecting cohort, survival, and symptom-presentation differences.6 Despite this burden, PTSD in older adults remains under-recognized owing to atypical symptom presentations (often prominent somatic complaints, sleep disturbance, and irritability, with comparatively less reported re-experiencing, so that distress is frequently misattributed to physical illness or normal aging), to stigma surrounding mental illness (which in many Asian settings frames psychological distress as personal weakness and favors somatic over psychological expression of symptoms), and to limited screening in community settings.6,7
Conventional epidemiological approaches to PTSD treat all symptoms as interchangeable indicators of a single underlying disease entity-the “latent variable” framework.8 The network approach offers a complementary perspective: rather than treating PTSD as a unitary construct, it models the disorder as a system of interacting symptoms.8 Within this framework, some symptoms function as highly central “hub” nodes that are more strongly interconnected with other symptoms, while others remain comparatively peripheral. In cross-sectional data, centrality reflects the degree of statistical interconnection among symptoms rather than demonstrated causal influence.8,9 Identifying central symptoms is clinically relevant for prioritizing assessment and generating hypotheses about candidate intervention targets; network theory posits that changes in a central symptom may be associated with broader changes across the network, although this remains a hypothesis requiring longitudinal confirmation.8–10 The network approach also has limitations: estimated networks can be sensitive to sample size and estimation choices, may show limited replicability, and can be difficult to distinguish statistically from latent-variable models, so the present results are interpreted as descriptive rather than confirmatory.
Empirical PTSD network studies have proliferated in recent years, predominantly in Western populations.10 In US military veterans and European trauma survivors, intrusive memories and physiological hyperarousal have often emerged as central nodes. However, findings are heterogeneous, with negative affect and detachment symptoms also reported as central in some samples.11 Network studies in non-Western populations remain comparatively rare, and whether the structural patterns observed in Western cohorts generalize to East and Southeast Asian aging populations is largely untested. Vietnam is a particularly apt but understudied setting: most community-dwelling older adults in northern and central Vietnam experienced intensive war-related trauma during the American War, and the lasting mental health consequences of that exposure have been documented in the Vietnam Health and Aging Study (VHAS) cohort.4,5
To our knowledge, no network analysis of PTSD symptoms has been conducted in community-dwelling older Vietnamese adults, a population with high cumulative war-trauma exposure, yet with limited mental-health research. In a companion study of the same Vietnam Health and Aging Study cohort, we compared PTSD symptom cluster profiles across trauma-exposure modalities (direct versus indirect exposure) using group-level cluster-score comparisons;12 the present study is methodologically distinct in applying a network-analytic framework that models the conditional associations among individual DSM-5 symptoms and identifies the most central symptoms by Expected Influence, rather than contrasting aggregate symptom-cluster scores between exposure subgroups. Characterizing which symptoms are most central in this population can inform culturally appropriate screening priorities and generate hypotheses about candidate intervention targets. This study aimed to estimate the regularized partial correlation network of DSM-5 PTSD symptoms, identify the most central symptoms by Expected Influence (EI), assess network stability through case-dropping bootstrap, and interpret the findings within the cultural context of older Vietnamese war survivors. Given the exploratory nature of network analysis in this population, we did not test directional causal hypotheses; rather, we anticipated (i) that the symptom network would contain identifiable central nodes estimable with adequate stability, and (ii) that, given cross-cultural differences in symptom expression, the most central symptoms might differ from the intrusion- and arousal-centered patterns frequently reported in Western samples. Because the design is cross-sectional, these expectations concern patterns of association rather than causal structure.
Methods
Study Design and Data Source
This cross-sectional network analysis used data from the second wave (2021–2022) of the Vietnam Health and Aging Study (VHAS), a population-based longitudinal cohort investigating health, social conditions, and aging in northern and central Vietnam. The VHAS was designed specifically to examine the long-term health consequences of wartime trauma exposure in an aging population.4 Data were collected in rural communes across Hanoi and Quang Binh provinces-areas selected for their spectrum of documented war-related trauma intensity, including exposure to heavy bombing, ground combat, and forced displacement. Full details of the VHAS study design and sampling procedures are described by Korinek et al4 The present analysis was conducted under the VHAS data-use protocol with the permission of the VHAS study investigators; the authors were authorized to access the de-identified second-wave dataset, and the governing institutional approvals are detailed in Ethical Considerations.
Participants and Eligibility
Eligible participants were community-dwelling adults aged ≥60 years who participated in the first wave of the VHAS (Wave 1, conducted in 2018) and were successfully followed up in the second wave (2021–2022). Participants were excluded if they were unavailable at the time of the survey, declined participation, or had severe cognitive impairment or psychiatric conditions that precluded reliable completion of the PTSD assessment instruments; severe cognitive impairment was identified by the trained interviewing clinicians as impairment sufficient to prevent valid self-report and structured interview, rather than by a fixed cut-off on a standardized cognitive screen.
A total of 301 older adults completed the second wave and constitute the full study sample. Five participants who met or potentially met Criterion A had missing PTSD diagnostic determinations (DSM-5 criteria A–G) and were excluded from diagnostic analyses, yielding a diagnostic sample of N = 296. The PTSD symptom network was estimated on the subset of participants with complete PCL-5 symptom data (N = 90 complete cases); these 90 participants constituted the analytic sample for all network analyses, which were conducted on complete-case data without imputation.
Sampling
Participants were selected using stratified random sampling from the VHAS sampling frame in selected communes. Eight communes were randomly selected across the two provinces; within each commune, individuals were sampled using stratification based on their prior PCL-5 score profiles from the 2018 Wave 1 assessment, ensuring representation of a range of symptom burden. Because stratification was based on Wave 1 PCL-5 profiles, the analytic sample may over-represent participants with prior symptom burden relative to a simple random community sample; this potential selection effect is revisited in the Limitations, and prevalence and network estimates should be interpreted accordingly. A formal sensitivity analysis comparing alternative sampling schemes or weights was not conducted. Although a priori power simulation for regularized network models is not yet standardized, the network-analysis sample (N = 90 complete cases) is modest relative to the observations-per-parameter heuristics commonly cited for regularized network estimation; the adequacy and stability of the achieved network were therefore evaluated through the case-dropping bootstrap analysis described in Network Stability Assessment, and the results are interpreted with corresponding caution.
Measures
PTSD Symptoms
PTSD symptom severity was assessed using the Vietnamese version of the PTSD Checklist for DSM-5 (PCL-5), a 20-item self-report instrument assessing DSM-5 PTSD criteria (The VHAS questionnaire and study documentation are publicly available at https://vhas.utah.edu/documentation.php). Items are rated on a five-point Likert scale (0 = “not at all” to 4 = “extremely”). The Vietnamese PCL-5 was developed through standard forward-backward translation procedures and culturally adapted for community-dwelling older adults in Vietnam. Psychometric validation conducted within this VHAS older-adult cohort confirmed excellent internal consistency (Cronbach’s α = 0.92), a four-factor structure consistent with DSM-5 theoretical domains (Intrusion [B1–B5], Avoidance [C1–C2], Negative Alterations in Cognitions and Mood [D1–D7], and Alterations in Arousal and Reactivity [E1–E6]), and high diagnostic accuracy compared with CAPS-5 (AUC = 0.967; 95% CI: 0.921–1.000; optimal screening cutoff ≥11; sensitivity 92.86%, specificity 95.12%). The optimal screening cutoff of ≥11 was derived empirically from this receiver-operating-characteristic analysis; comparatively low PCL-5 cutoffs are frequently reported in culturally adapted and older-adult samples, and this threshold was chosen to maximize screening sensitivity for community case-finding, with the resulting trade-offs for specificity and clinical interpretation considered in the Discussion. Network estimation was performed on 19 of the 20 items; Item D7 (“inability to experience positive emotions”) was excluded because ordinal-scale data for this item were unavailable in the network analysis dataset. The remaining 19 items continued to represent the four DSM-5 symptom domains conceptually.
Diagnostic Reference Standard
Concurrent CAPS-5 (Clinician-Administered PTSD Scale for DSM-5) interviews were conducted and served as the diagnostic reference standard. The current PTSD diagnosis was established when CAPS-5 criteria were met for all required DSM-5 symptom clusters, duration, and functional impairment. Interviews were conducted by trained physicians and reviewed by senior clinicians experienced in mental health assessment. Formal inter-rater reliability statistics for CAPS-5 administration were not computed in the present analysis; diagnostic consistency was supported by senior-clinician review of all interviews, and the absence of a quantified inter-rater estimate is acknowledged as a limitation.
Trauma Exposure
Trauma exposure characteristics were assessed according to DSM-5 Criterion A categories, including type of exposure (direct experience, witnessing, learning about the event) and nature of the event (life-threatening situations, serious physical injury, sexual violence).
Sociodemographic Variables
Age, sex, marital status, education level, and chronic disease history were extracted from the VHAS dataset.
Network Estimation
A regularized partial-correlation network was estimated from item-level PTSD symptom data using the graphical LASSO with extended Bayesian information criterion (EBIC) model selection (EBICglasso), computed from a polychoric correlation matrix of the ordinal symptom items and tuned with an EBIC hyperparameter of gamma (γ) = 0.50, in which negligible partial correlations are shrunk toward zero, yielding a sparse network that retains the more robust conditional associations among symptoms (full network estimation framework in Supplementary Material S2). Each retained edge represents the association between two symptoms after adjustment for all other nodes. Sensitivity analyses across alternative regularization settings were not performed and are recommended for future replication. A post-hoc redundancy assessment was conducted using edge-profile similarity analysis; no symptom pair demonstrated substantial redundancy (the highest observed profile correlation was 0.591), supporting the retention of all 19 nodes (see Supplementary Material S5; Table S3). Analyses were conducted on complete-case data (N = 90); no imputation was applied (see Supplementary Material S1 for derivation of the analytic samples).
GLASSO regularization shrinks small partial correlations to zero, producing a sparse network in which each edge represents the conditional association between two symptoms after controlling for all remaining nodes.9 The resulting network was laid out using the Fruchterman–Reingold algorithm. Nodes were color-coded by DSM-5 cluster: Intrusion (B) = salmon/red; Avoidance (C) = orange; Negative Cognitions/Mood (D) = blue; Arousal/Reactivity (E) = green. Edge width and opacity are proportional to the absolute partial-correlation weights; all retained edges in the present network represent positive associations.
Centrality Analysis
Node centrality was quantified using Expected Influence (EI), computed from the estimated network. EI is the sum of all signed edge weights connected to a node and is recommended over traditional node strength (which uses absolute values) because it preserves edge sign, thereby better reflecting a node’s net association with the rest of the network. EI values greater than zero indicate that a node is, on balance, positively associated with co-occurring symptoms, and higher EI values indicate greater centrality (ie, more hub-like) within the estimated network. Because the analysis is cross-sectional, EI reflects statistical interconnection rather than causal influence.
Network Stability Assessment
Network stability was evaluated using a case-dropping subset bootstrap (1000 iterations), following established methodology.13 This procedure repeatedly re-estimates the network from random subsamples of the data at decreasing sample fractions. It compares the centrality ordering obtained in each subsample with that obtained in the full sample. Greater reproducibility of the centrality ordering across subsamples indicates more stable centrality estimates.
Statistical Analysis
Descriptive statistics were computed using R. Continuous variables are reported as mean (SD); categorical variables as frequency (%). All network estimation and visualization procedures were implemented in R. Network analysis does not rely on null-hypothesis significance testing; rather, the validity of network structure is established through regularized estimation and bootstrap stability evaluation.
Ethical Considerations
The study protocol was approved by the Institutional Review Board of Hanoi Medical University (Approval No. 01.18/HMU IRB, issued January 25, 2018) and by the National Bioethics Committee of the Ministry of Health, Vietnam (Approval No. 29/CN-HĐĐ, issued April 27, 2018). All procedures conformed to the ethical standards of the Declaration of Helsinki. Written informed consent was obtained from all participants before data collection. All data were de-identified before analysis-ethical approvals covered all analyses conducted under this research protocol.
Results
Sample Characteristics
Sociodemographic and trauma-exposure characteristics of the full study sample (N = 301) are presented in Table 1. The PTSD symptom network described below was estimated on the subset of participants with complete PTSD symptom data (N = 90 complete cases; see Figure 1). The cohort had a mean age of 73.6 years (SD = 8.0), with a near-equal sex distribution (50.5% male, 49.5% female). The majority were married or cohabiting (70.8%), and 71.4% had completed at least lower secondary education. Approximately 75.4% reported at least one chronic disease. Direct trauma exposure was reported by 43.2% of participants; the most frequently endorsed trauma nature was life-threatening events to self or others (combined). The prevalence of current PTSD based on CAPS-5 diagnosis was 4.1% (12/296) among participants with a completed diagnostic assessment.
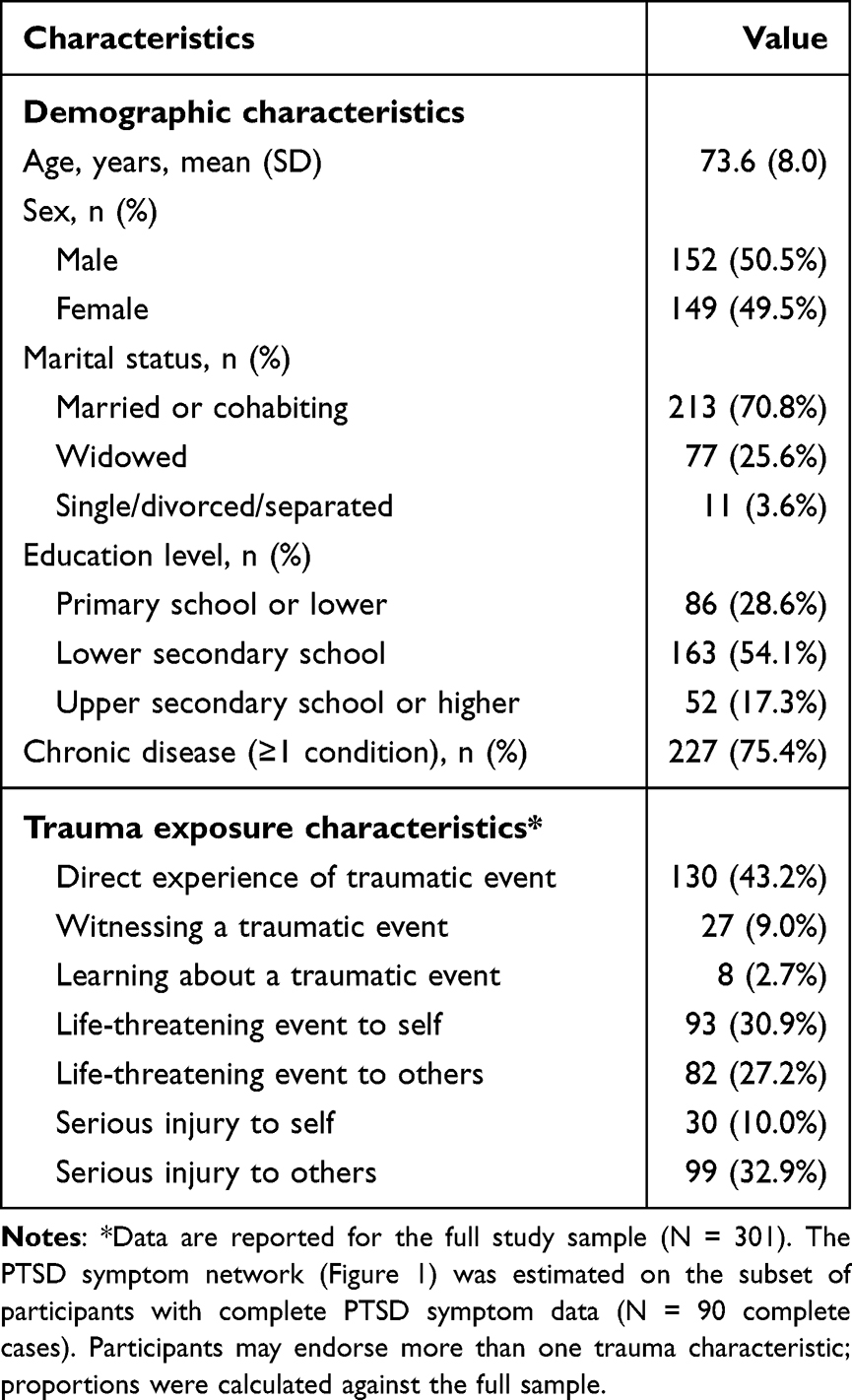 |
Table 1 Demographic and Trauma-Related Characteristics of Participants (N = 301) |
 |
Figure 1 Regularized partial correlation network of 19 DSM-5 PTSD symptoms estimated using a regularized partial-correlation model (graphical LASSO with EBIC model selection, EBICglasso; γ = 0.50) computed from a polychoric correlation matrix (N = 90 complete cases). The network comprised 40 non-zero edges among 19 nodes (density = 0.234). Node colors indicate DSM-5 cluster: salmon/red = Intrusion (B); Orange = Avoidance (C); blue = Negative Cognitions/Mood (D); green = Arousal/Reactivity (E). Edge width is proportional to partial correlation weight; all edges are positive. Node codes follow the DSM-5 PCL-5 items: B1 = intrusive memories; B2 = nightmares; B3 = dissociative reactions (flashbacks); B4 = psychological cue reactivity; B5 = physiological cue reactivity; C1 = avoidance of trauma-related thoughts or feelings; C2 = avoidance of external reminders; D1 = inability to recall key features of the trauma; D2 = persistent negative beliefs about oneself or the world; D3 = distorted cognitions about the cause or consequences of the trauma; D4 = persistent negative emotional state; D5 = markedly diminished interest or participation in activities; D6 = feelings of detachment or estrangement; E1 = irritable behavior or angry outbursts; E2 = reckless or self-destructive behavior; E3 = hypervigilance; E4 = exaggerated startle response; E5 = problems with concentration; E6 = sleep disturbance. Item D7 (inability to experience positive emotions) was excluded from network estimation. |
Item-Level Descriptive Statistics
Item-level descriptive statistics for the 19 PCL-5 symptom nodes are presented in Table 2. Overall, symptom severity scores were relatively low, consistent with a non-clinical community sample. Sleep disturbance (E6; M = 0.93, SD = 1.38) and physiological cue reactivity (B5; M = 0.96, SD = 1.27) had the highest mean severity within their respective clusters in this sample. Notably, persistent negative emotional states (D4; M = 0.44) showed only moderate mean severity yet emerged as the most central node in the network (see Node Centrality), illustrating that symptom severity and network centrality need not track together.
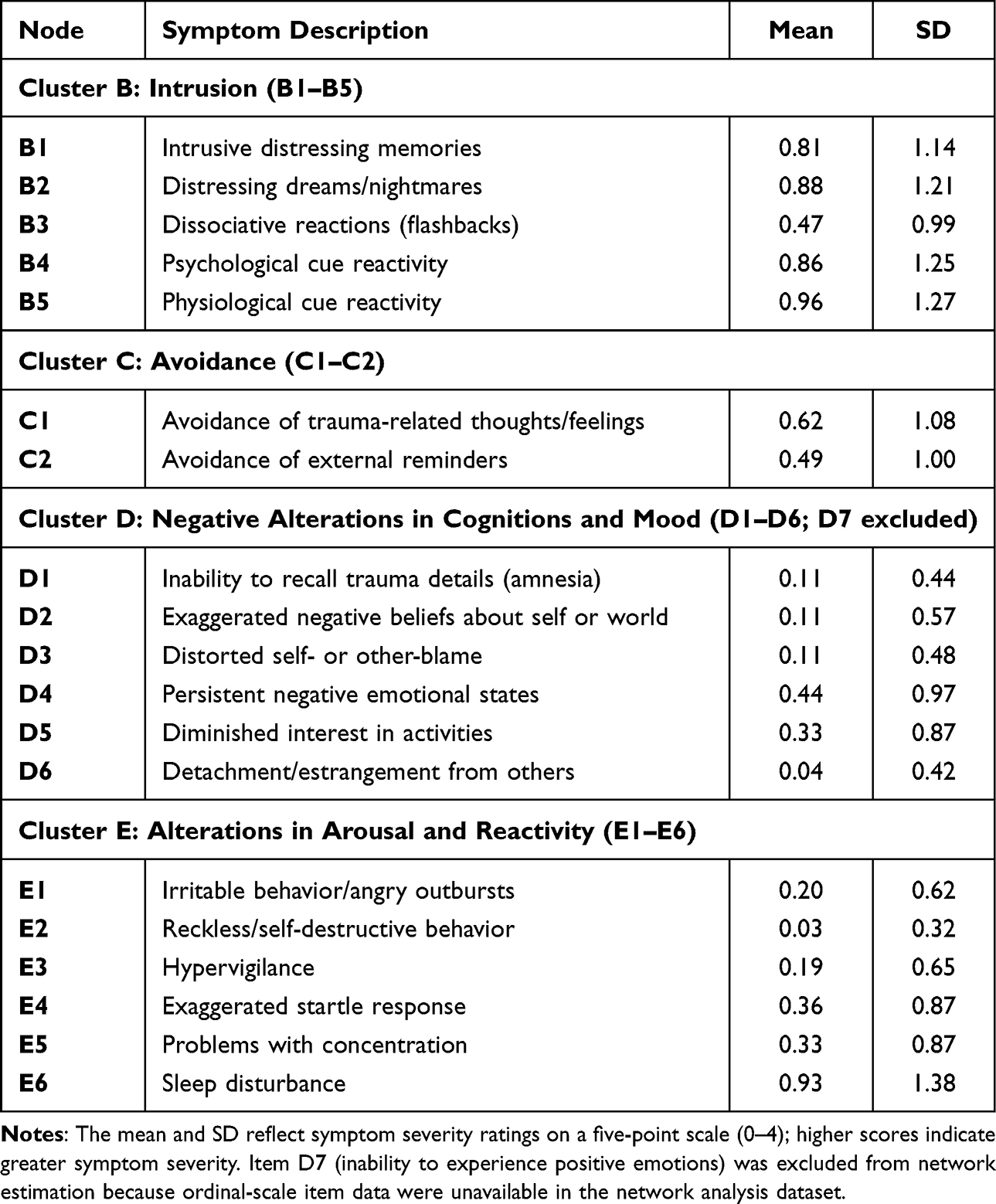 |
Table 2 Item-Level Descriptive Statistics for 19 PCL-5 PTSD Symptom Nodes (N = 90) |
Network Structure
Figure 1 displays the estimated regularized partial correlation network. After regularization, the network retained 19 symptom nodes connected by 40 non-zero edges (all positive), indicating that higher severity on one symptom was associated with higher severity on co-occurring symptoms, controlling for all other nodes. The network had a density of 0.234, calculated as 40 non-zero edges out of 171 possible edges. The strongest partial-correlation edges are summarized in Supplementary Material S3 (Table S1). The Arousal and Reactivity cluster (E) formed the most densely interconnected subgraph in this sample. The Avoidance nodes (C1, C2) occupied a visually prominent bridging position between the Intrusion and Negative Cognitions/Mood clusters.
Node Centrality
Centrality indices are presented in Table 3 and rank-ordered by Expected Influence (full Expected Influence rankings in Supplementary Material S4, Table S2). “Persistent negative emotional states” (D4; EI = 1.306) was the most central symptom, followed by “avoidance of trauma-related thoughts and feelings” (C1; EI = 1.196) and “psychological cue reactivity” (B4; EI = 1.154). This ranking held despite the relatively low mean severity of D4 compared with symptoms such as sleep disturbance (E6) and physiological cue reactivity (B5), which showed relatively high mean severity yet occupied peripheral network positions (EI 0.664 and 0.722, respectively). The least central nodes were “inability to recall trauma details” (D1; EI = 0.189) and “detachment from others” (D6; EI = 0.292)-findings consistent with the systematic review of PTSD networks in which amnesia is consistently the least central symptom.10
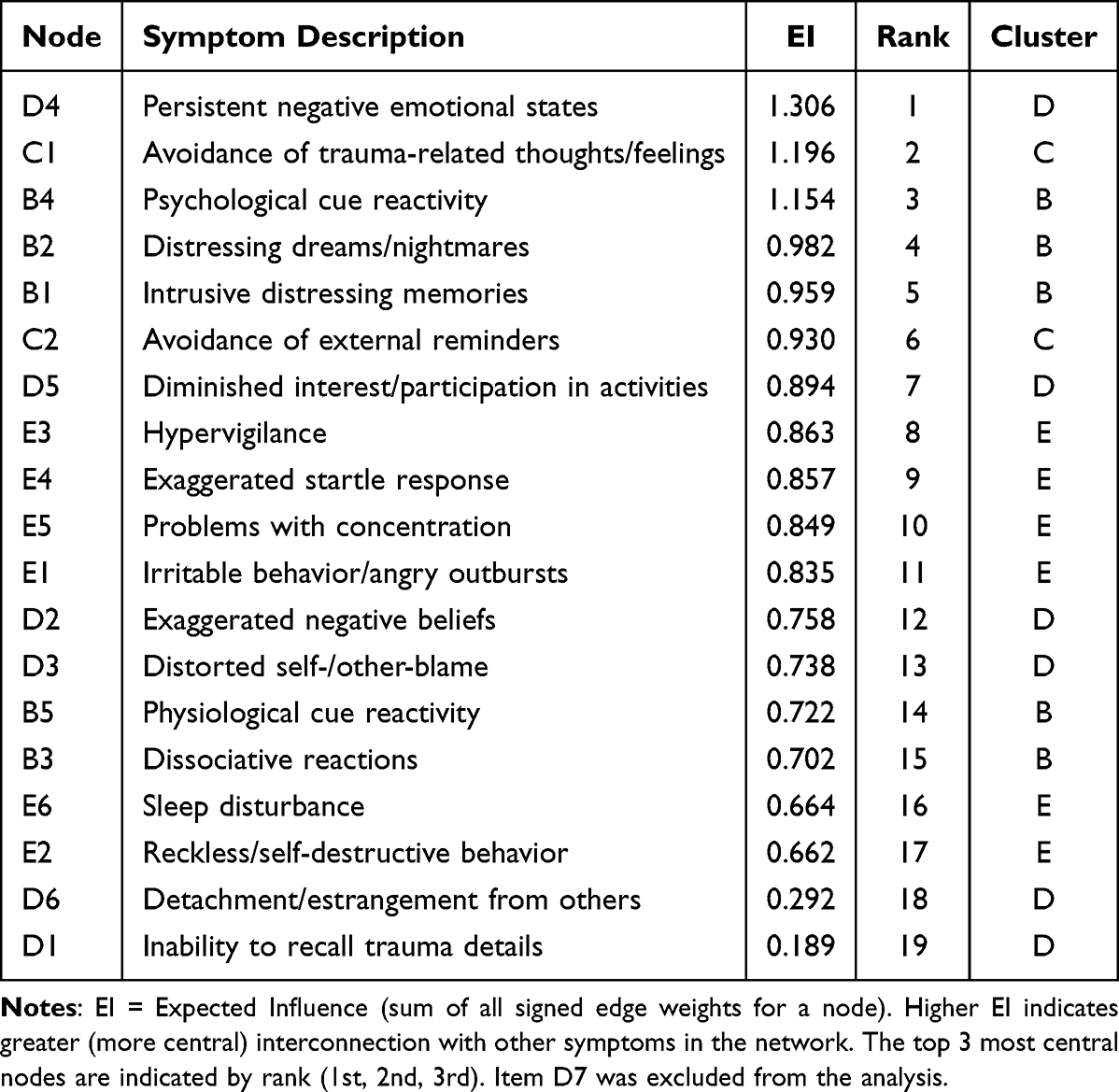 |
Table 3 Centrality Indices of the PTSD Symptom Network Ranked by Expected Influence (EI; N = 90) |
Network Stability
A case-dropping bootstrap (1000 iterations) was used to evaluate the stability of centrality estimates (Figure 2). The three most central nodes were persistent negative emotional states (D4), cognitive avoidance (C1), and psychological cue reactivity (B4). Stability was assessed following established case-dropping methodology,13 and the central-node ranking was reproducible across subsamples rather than driven by a few influential observations. The correlation stability (CS) coefficient for Expected Influence was 0.50 (CS-coefficient = 0.50), indicating that the centrality ordering remained stable when up to 50% of cases were dropped; this and other quantitative stability indices should be interpreted in light of the modest network sample (N = 90); full case-dropping bootstrap reproducibility metrics are reported in Supplementary Material S6 (Tables S4 and S5).
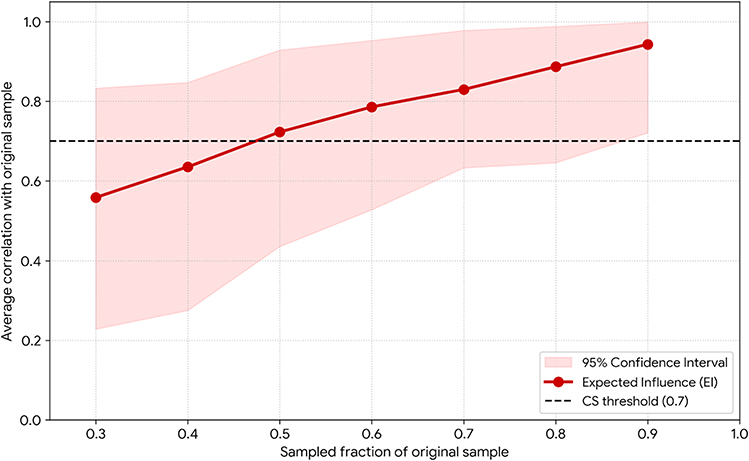 |
Figure 2 Network stability assessed via case-dropping bootstrap (1000 iterations; N = 90 complete cases). The y-axis shows the mean Spearman correlation between centrality indices (Expected Influence) of bootstrapped sub-networks and the full-sample network; the x-axis represents the proportion of the sample retained. The shaded area represents the 95% confidence interval. Dashed horizontal line = the 0.70 reference threshold for the mean rank correlation. |
Discussion
Summary of Principal Findings
This study provides the first network analysis of PTSD symptom interactions in community-dwelling older adults in Vietnam-a population characterized by substantial wartime trauma exposure but largely absent from the global psychotraumatology literature. Persistent negative emotional states (D4) and cognitive avoidance (C1) emerged as the most central nodes. Symptoms with relatively high mean severity (sleep disturbance [E6] and physiological cue reactivity [B5]) were comparatively peripheral within the network. The ordering of the most central nodes was reproducible under the case-dropping bootstrap.
A Culturally Specific Network Topology
The centrality of cognitive avoidance (C1) and persistent negative affect (D4) differs from the patterns most often reported in Western cohorts. The systematic review of Birkeland et al documented that intrusive memories (B1) and physiological hyperarousal are frequently, though not invariably, among the most central nodes in Western samples.10 In US military veterans, negative emotions can be central, but usually together with physiological cue reactivity and flashbacks rather than with cognitive avoidance.11 The greater prominence of C1 and D4 in the present sample is broadly consistent with cross-cultural perspectives on PTSD.14 One possible interpretation is that East Asian cultural norms emphasizing interpersonal harmony and restraint in expressing negative affect may favor emotional suppression and cognitive avoidance as coping strategies; however, because no cultural variables were measured in this study, this explanation remains speculative. Within this interpretation, avoidance (C1) and persistent negative affect (D4) would be expected to be closely associated; however, the cross-sectional design cannot establish whether one precedes, follows, or reciprocally relates to the other, or how either relates to the rest of the network. Direct measurement of cultural coping orientations was not available in this dataset, and this interpretation should be tested in future studies. Cultural norms are unlikely to be the sole explanation: differences in trauma type, socioeconomic conditions, limited access to mental-health services, cohort effects, and the measurement properties of the PCL-5 in this population could each contribute to the observed network structure, and methodological differences between studies, including sample composition and estimation choices, further complicate direct cross-cultural comparison.
Intrusion symptoms (Cluster B) and physiological reactivity were comparatively peripheral in the network despite being commonly reported, illustrating that how often a symptom occurs and how central it is in the network need not coincide. This dissociation between how common a symptom is and how central it is has been described in other network studies; network theory has tentatively interpreted frequently reported symptoms as possible downstream features rather than drivers, although such directional interpretations cannot be tested with cross-sectional data.8 In this sample, sleep disturbance and physiological reactivity were associated with, but less central than, C1 and D4; whether they represent downstream features cannot be determined from cross-sectional data.
Contextual Interpretation of Network Findings
The network findings can be contextualized against known epidemiological patterns in this population. Within this sample, life-threatening events were the most frequently reported trauma exposures. Injury-related trauma may be associated with the C1 and D4 symptoms; however, the present data cannot establish any such pathway, and this remains a hypothesis for prospective research. These associations are descriptive only; the cross-sectional design does not support inferences about how symptom profiles develop or change over time.8
Using the validated PCL-5 screening cutoff of ≥11 (see Measures), 13.2% of trauma-exposed participants in this sample were identified with clinically relevant symptoms. Within this group, the avoidance and negative-affect symptoms may be a useful focus for further clinical investigation. The relatively high sensitivity of the PCL-5 at this cutoff may assist community-level identification of individuals who could be referred for further clinical assessment.
Clinical Implications
These findings have practical relevance for the clinical care of Vietnam’s aging population. Although the cross-sectional design cannot establish that D4 and C1 are causal drivers, their central position may make them useful candidate foci for clinical attention, a possibility that requires prospective testing. Evidence-based trauma-focused interventions, Prolonged Exposure (PE) therapy and Cognitive Behavioral Therapy (CBT), have shown efficacy in older trauma survivors15 and are relevant to these symptoms: PE targets avoidance (C1) by facilitating trauma-memory processing, while CBT addresses maladaptive cognitions and emotion regulation may be relevant to persistent negative affect (D4). Prior research has confirmed the suitability of these treatments for older trauma-exposed populations.15
These mechanistic links are hypotheses generated by the network structure rather than evidence of comparative treatment efficacy; a cross-sectional network cannot establish that any intervention, or any ordering of interventions, is superior to another. Randomized trials would be required to determine whether targeting avoidance and negative affect improves outcomes, and the present results should not be read as establishing the priority of psychotherapy over pharmacotherapy. These results help generate hypotheses for culturally appropriate, integrated mental-health care for older adults in Vietnam.
Strengths and Limitations
Several features strengthen this analysis. It is, to our knowledge, the first network study of PTSD in Vietnamese older adults. The use of a regularized partial-correlation (graphical LASSO) network model and a 1000-iteration case-dropping bootstrap follows current methodological practice.9,13 The ordering of the most central nodes was reproducible across bootstrap subsamples.
Several limitations should be considered when interpreting these findings. First, the cross-sectional design precludes causal inference; the observed centrality reflects statistical interconnection rather than causal influence, and the temporal or directional relationship between symptoms such as cognitive avoidance (C1) and persistent negative emotional states (D4) cannot be established and would require longitudinal or ecological momentary assessment designs. Second, the network was estimated on the 90 participants with complete PTSD symptom data-a modest sample for regularized network estimation-drawn from a larger study sample (N = 301); this complete-case restriction, together with stratified sampling based on Wave 1 symptom profiles, may have introduced selection effects, widened the confidence intervals around some edge weights, and limited statistical power for stable subgroup estimation, so edge and centrality estimates should be interpreted with caution pending replication in larger, more representative samples. Third, generalizability is constrained: participants were recruited from specific rural communes in two provinces, and the findings may not extend to urban, clinical, or other Southeast Asian populations. Fourth, the low observed PTSD prevalence (4.1% by CAPS-5) and the generally low symptom endorsement produced sparse responses at the upper end of the scale, which can reduce the precision of the network estimates and further limit generalization to clinical samples. Fifth, the high proportion of participants with chronic physical illness (75.4%) was not modeled, raising the possibility of residual confounding in associations among somatic symptoms such as sleep disturbance and arousal. Finally, the analysis relied on self-report, which may be subject to culturally patterned social-desirability bias-particularly in the disclosure of emotional avoidance-and one symptom item (D7) was unavailable for inclusion, yielding a 19- rather than 20-node model; cultural influences on symptom expression were not directly measured.
Conclusion
Among community-dwelling older Vietnamese adults with lifetime war trauma exposure, the most central symptoms in the PTSD network were persistent negative emotional states (D4) and cognitive avoidance (C1). This pattern departs from the intrusion-centered networks typically reported in Western populations. This pattern may relate to cultural differences in symptom expression. However, cultural factors were not directly measured.4 Because the design is cross-sectional, these findings cannot establish symptom causation or treatment priority; they tentatively suggest that avoidance and negative affect may be useful foci for further clinical research, including evaluation of trauma-focused psychological interventions. Prospective and longitudinal designs in larger samples, comparison of symptom networks across cultural settings, and randomized trials of treatment would help establish whether these central symptoms are clinically important over time and whether network-informed strategies can improve outcomes for aging populations in Vietnam and comparable low- and middle-income settings.
Declaration on AI-Assisted Tools
The authors used AI-assisted tools solely for language editing and clarity improvement. The authors performed all aspects of the study design, data analysis, interpretation, and conclusions. The authors take full responsibility for the content of this manuscript.
Abbreviations
PTSD, Post-traumatic stress disorder; DSM-5, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; PCL-5, PTSD Checklist for DSM-5; CAPS-5, Clinician-Administered PTSD Scale for DSM-5; AUC, area under the curve; EI, Expected Influence; VHAS, Vietnam Health and Aging Study.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethical Approval and Consent
Approved by Hanoi Medical University IRB (No. 01.18/HMU IRB, January 25, 2018) and National Bioethics Committee of the Ministry of Health, Vietnam (No. 29/CN-HĐĐ, April 27, 2018). Written informed consent was obtained from all participants.
Acknowledgments
The authors sincerely thank the participants of the Vietnam Health and Aging Study (VHAS) for their valuable contribution. We also acknowledge the support of local health staff and field investigators involved in data collection and project coordination.
Author Contributions
Pham Thi Ngoc Bich: Conceptualization, Methodology, Investigation, Data curation, Formal analysis, Writing – original draft. Le Xuan Hung: Conceptualization, Methodology, Formal analysis, Supervision, Writing – review & editing. Ho Thi Kim Thanh: Supervision, Writing – review & editing. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no conflict of interest.
References
1. Koenen KC, Ratanatharathorn A, Ng L, et al. Posttraumatic stress disorder in the world mental health surveys. Psychol Med. 2017;47:2261–12. doi:10.1017/S0033291717000708
2. Bovin MJ, Marx BP, Weathers FW, et al. Psychometric properties of the PTSD checklist for diagnostic and statistical manual of mental disorders-fifth edition (PCL-5) in veterans. Psychol Assess. 2016;28:1379–1391. doi:10.1037/pas0000254
3. Goldstein RB, Smith SM, Chou SP, et al. The epidemiology of DSM-5 posttraumatic stress disorder in the United States: results from the national epidemiologic survey on alcohol and related conditions-III. Soc Psychiatry Psychiatr Epidemiol. 2016;51:1137–1148. doi:10.1007/s00127-016-1208-5
4. Korinek K, Teerawichitchainan B, Zimmer Z, et al. Design and measurement in a study of war exposure, health, and aging: protocol for the Vietnam health and aging study. BMC Public Health. 2019;19:1351. doi:10.1186/s12889-019-7680-6
5. Kovnick MO, Young Y, Tran N, et al. The impact of early life war exposure on mental health among older adults in northern and central Vietnam. J Health Soc Behav. 2021;62:526–544. doi:10.1177/00221465211039239
6. Reynolds K, Pietrzak RH, Mackenzie CS, et al. Post-traumatic stress disorder across the adult lifespan: findings from a nationally representative survey. Am J Geriatr Psychiatry. 2016;24:81–93. doi:10.1016/j.jagp.2015.11.001
7. Sobczak S, Orgeta V, Beenakker M, et al. Post-traumatic stress disorder in older adults: a global collaboration on setting the future research agenda. Lancet Healthy Longev. 2025;6:100720. doi:10.1016/j.lanhl.2025.100720
8. Borsboom D. A network theory of mental disorders. World Psychiatry. 2017;16:5–13. doi:10.1002/wps.20375
9. Jones PJ, Heeren A, McNally RJ, et al. Commentary: a network theory of mental disorders. Front Psychol. 2017;8:1305. doi:10.3389/fpsyg.2017.01305
10. Birkeland MS, Greene T, Spiller TR, et al. The network approach to posttraumatic stress disorder: a systematic review. Eur J Psychotraumatology. 2020;11:1700614. doi:10.1080/20008198.2019.1700614
11. Armour C, Fried EI, Deserno MK, et al. A network analysis of DSM-5 posttraumatic stress disorder symptoms and correlates in U.S. military veterans. J Anxiety Disord. 2017;45:49–59. doi:10.1016/j.janxdis.2016.11.008
12. Thi Ngoc Bich P, Xuan Hung L, Thi Kim Thanh H, et al. Differential PTSD symptom cluster profiles by trauma exposure modality in community-dwelling vietnamese older adults. F1000Research. 2026;15:715–724. doi:10.12688/f1000research.180499.1
13. Epskamp S, Borsboom D, Fried EI, et al. Estimating psychological networks and their accuracy: a tutorial paper. Behav Res Methods. 2018;50:195–212. doi:10.3758/s13428-017-0862-1
14. Hinton DE, Lewis-Fernández R. The cross-cultural validity of posttraumatic stress disorder: implications for DSM-5. Depress Anxiety. 2011;28:783–801. doi:10.1002/da.20753
15. Thorp SR, Glassman LH, Wells SY, et al. A randomized controlled trial of prolonged exposure therapy versus relaxation training for older veterans with military-related PTSD. J Anxiety Disord. 2019;64:45–54. doi:10.1016/j.janxdis.2019.02.003
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Spotlight on the Challenges of Depression following Retirement and Opportunities for Interventions
Dang L, Ananthasubramaniam A, Mezuk B
Clinical Interventions in Aging 2022, 17:1037-1056
Published Date: 7 July 2022
All Types Obesity and Physical Inactivity Associated with the Risk of Activity of Daily Living Limitations Among People with Asthma
Alhammad SA, Alwadeai KS
Journal of Multidisciplinary Healthcare 2022, 15:1573-1583
Published Date: 22 July 2022
Development and Evaluation of Content Validity and Acceptance of a Multidomain Intervention Module for Reversal of Cognitive Frailty Among Older Adults
Mustafa Khalid N, Ponvel P, Ibrahim AM, Mohd Safien A, Md Fadzil NH, Singh DKA, Mat Ludin AF, Ibrahim N, Subramaniam P, Haron H, Rajikan R, Vanoh D, Shahar S
Clinical Interventions in Aging 2024, 19:1189-1202
Published Date: 1 July 2024
A Systematic Review of Continuity of Care Strategies for Enhancing Diabetes Self-Management in Older Adults in Asian Countries
Sari CWM, Haroen H, Juniarti N, Amalia L, Pardosi JF
Journal of Multidisciplinary Healthcare 2025, 18:5441-5459
Published Date: 2 September 2025