Back to Journals » Cancer Management and Research » Volume 18

Neoadjuvant Chemoimmunotherapy for the Treatment of Locally Advanced Nasopharyngeal Carcinoma in Non-Endemic Regions: A Single-Arm Phase 2 Clinical Trial
Authors Zhou L, Tao Z, Zhou Y, Yang L, Zhang Y, He J, Sun B, Wang R, Yang J, Gao J
Received 7 August 2025
Accepted for publication 23 December 2025
Published 15 January 2026 Volume 2026:18 559229
DOI https://doi.org/10.2147/CMAR.S559229
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Sanjeev K. Srivastava
Lingran Zhou, Zhenchao Tao, Yan Zhou, Liping Yang, Yangyang Zhang, Jian He, Bin Sun, Ru Wang, Jing Yang, Jin Gao
Department of Radiation Oncology, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, Anhui, People’s Republic of China
Correspondence: Jin Gao, Department of Radiation Oncology, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, Anhui, People’s Republic of China, Email [email protected]
Background and Purpose: Nasopharyngeal carcinoma (NPC) is a malignancy with distinct geographical distribution and is rare in non-endemic regions. Despite significant improvements in NPC survival through chemoradiotherapy, recurrence and metastasis remain major clinical challenges, particularly in non-endemic areas where data on neoadjuvant immunochemotherapy are scarce. This study aimed to address this gap by evaluating the antitumor activity and safety of neoadjuvant gemcitabine–cisplatin plus camrelizumab in patients with locally advanced NPC in non-endemic regions.
Materials and Methods: In this single-center, single-arm, phase 2 trial, patients with stage III–IVA NPC received chemotherapy (gemcitabine 1000 mg/m2 on days 1 and 8, plus cisplatin 80 mg/m2 on day 1) and camrelizumab 200 mg on day 1 for three cycles, followed by radiotherapy. Primary endpoints were objective response rate (ORR). Secondary endpoints included disease-free survival (DFS), overall survival (OS), and biomarker correlations in addition to the primary ORR.
Results: Thirty-eight patients were enrolled and thirty-three completed three cycles of the neoadjuvant therapy, resulting in an ORR of 89.4% (34/38). The median follow-up duration was 18.5 months, and the 12-month disease-free survival rate was 94.7% (34/36). Six patients encountered grade 3 adverse effects: Two with nausea/vomiting, two with thrombocytopenia, one with leukopenia, and one with immune-related hepatitis. No grade 4 treatment-related events or deaths occurred.
Conclusion: Neoadjuvant camrelizumab combined with chemotherapy demonstrated promising antitumor activity and acceptable safety in locally advanced NPC patients from non-endemic regions. However, further randomized studies are needed to confirm these findings and assess long-term survival benefits.
Keywords: neoadjuvant chemoimmunotherapy, PD-1 inhibitor, camrelizumab, nasopharyngeal carcinoma, radiotherapy
Introduction
Concurrent chemoradiotherapy, supplemented by either adjuvant or induction chemotherapy, serves as the cornerstone treatment paradigm for locally advanced nasopharyngeal carcinoma (NPC).1 This regimen has enabled substantial improvements in patient survival. However, despite improved survival, 20%–30% of patients still experience recurrence or distant metastasis, and many suffer from significant treatment-related toxicities such as mucositis, hearing loss, and hematologic toxicity.2 Therefore, it is imperative to investigate more efficacious therapeutic approaches to improve patient prognosis.
NPC is primarily characterized by non-keratinizing carcinoma, closely associated with Epstein-Barr Virus (EBV), which plays a crucial role in its pathogenesis by promoting oncogenic transformation and immune evasion.3,4 This association leads to an upregulation of PD-L1 expression, with a positivity rate frequently exceeding 70%.5 This overexpression enables tumor cells to evade immune surveillance by inhibiting cytotoxic T-cell function through binding to the PD-1 receptor on T cells, making PD-1/PD-L1 blockade a rational immunotherapeutic strategy. According to global cancer statistics from 2022, over 75% of NPC cases are diagnosed in Southeast Asia and Southern China.6 As an intensely immunoinflammatory neoplasm, nasopharyngeal carcinoma’s tumor microenvironment is densely infiltrated by immune cells,7,8 providing a robust theoretical foundation for the use of immunotherapeutic strategies.
Recent years have seen substantial advancements in immunotherapy for nasopharyngeal carcinoma. Currently, a therapeutic regimen combining PD-1 inhibitors with gemcitabine and cisplatin chemotherapy has been approved for the first-line treatment of recurrent or metastatic nasopharyngeal carcinoma.9,10 This approval has increased interest in their use in neoadjuvant therapy, prompting numerous prospective clinical trials. Current research on immunotherapy for NPC predominantly involves patients from high-incidence regions, such as South China. There is still a lack of sufficient data on the efficacy and safety of immunotherapy combined with chemotherapy as neoadjuvant treatment for NPC in regions with low incidence of the disease. Emerging evidence indicates that NPC from non-endemic regions shows a more heterogeneous etiologic and immune profile, with a substantially higher proportion of keratinizing/EBV-negative tumors than endemic populations, where EBV-driven non-keratinizing disease predominates.11 Because EBV-associated NPC typically displays a highly immune-inflamed microenvironment with frequent PD-L1 expression and dense lymphocytic infiltration, regional differences in EBV linkage and tumor immune contexture may alter responsiveness to PD-1 blockade and limit extrapolation from endemic trials.12 Consequently, the compelling efficacy data generated from high-incidence regions cannot be directly extrapolated.
Here, we present the findings from a phase 2 clinical study evaluating the efficacy of camrelizumab combined with chemotherapy for the treatment of patients with locally advanced NPC in non-endemic regions. The aim of this study was to evaluate the efficacy and safety of neoadjuvant camrelizumab combined with gemcitabine and cisplatin in patients with locally advanced nasopharyngeal carcinoma from non-endemic regions.
Materials and Methods
Study Design and Participants
This trial was an open-label, single-arm, Phase II clinical study conducted at Anhui Provincial Cancer Hospital, Hefei, China from January 2022 to January 2024. The trial was registered under the identifier ChiCTR2200057745 on ClinicalTrials.gov.
This single-center study was conducted in a non-endemic region for nasopharyngeal carcinoma. All enrolled patients reported Anhui Province as their hometown. Patients with histologically confirmed NPC, staged as T4, N2 or N3 by the AJCC 8th edition were eligible. Patients with distant metastasis (stage IVB, M1) were excluded. Inclusion criteria included: Eastern Cooperative Oncology Group (ECOG) performance status of 0 to 1, measurable lesions according to RECIST 1.1, and normal organ function. Exclusion criteria included patients with active autoimmune diseases, immunodeficiency, or uncontrolled comorbidities such as active infections, chronic hepatitis, or pregnancy. Informed consent was obtained by the principal investigator. All participants were provided with a written consent form and had the opportunity to ask questions and withdraw from the study at any point.The consent process adhered to the ethical standards set by the Ethics Committee of Anhui Provincial Cancer Hospital (Approval No.2021–98; Date: December 30, 2021).
Procedures
Each patient underwent a comprehensive pre-treatment assessment including physical examination, contrast-enhanced magnetic resonance imaging (MRI) of the head and neck, medical, biochemical, and hematological profiling, nasopharyngoscopy, bone scan, computed tomography (CT) imaging of the chest, sonography or CT imaging of the abdomen, and baseline plasma EBV-DNA load determination.
Biomarker Testing
Plasma EBV-DNA levels were quantified using a real-time quantitative PCR assay targeting the BamHI-W fragment of the EBV genome (Sansure EBV DNA Kit, Sansure Biotech, China). The assay has a lower limit of detection of 500 IU/mL. All samples were processed in a centralized laboratory following internal quality-control procedures. Each sample was run in duplicate, and discordant results were repeated according to laboratory policy.
Immunohistochemical staining of PD-L1 was performed using the PD-L1 IHC 22C3 pharmDx assay (DAKO, Denmark), with appropriate positive and negative controls employed. The combined positive score (CPS) was calculated as the number of PD-L1–positive cells divided by the total number of viable tumor cells, multiplied by 100.
Treatment
Following the initial assessment, participants received three cycles of neoadjuvant chemotherapy with gemcitabine 1000 mg/m2 on days 1 and 8, cisplatin 80 mg/m2 on day 1, plus camrelizumab 200 mg on day 1.
Subsequently, all patients underwent intensity-modulated radiotherapy (IMRT) after a 3-week interval. Target delineation followed consensus guidelines, with a recommended dose of 70 Gy at 2.12 Gy per fraction (once daily, 5 fractions per week).
MRI imaging assessments were conducted at three time points: after neoadjuvant therapy, after 20 sessions of radiotherapy, and one month after the completion of radiotherapy. Tumor response was evaluated by investigators using RECIST version 1.1 criteria.
Sample Size Rationale
The sample size for this single-arm, phase II trial was not determined by a formal power calculation. Instead, an enrollment target of approximately 40 patients was set based on clinical feasibility and patient accrual capacity at our center over the defined study period. This sample size is consistent with those of other published single-arm phase II trials in oncology and was deemed sufficient to provide preliminary evidence of the activity and safety of the regimen in this understudied, non-endemic population.
Statistical Analysis
A total of 38 patients were enrolled. Side effects and adverse events were meticulously monitored and recorded throughout the observation period for descriptive statistical analysis. Statistical methods included non-parametric tests. In univariate analyses across different populations, data meeting assumptions of normality and variance homogeneity were assessed using independent sample t-tests; otherwise, non-parametric tests were employed. All p-values were two-sided, with a significance level set at 0.05. Statistical analyses were performed using SPSS and R software packages.
Data Handling and Management
All clinical and laboratory data were prospectively recorded using an electronic data capture system. Missing data were handled using complete-case analysis, and no outcome variables required imputation. Data were independently reviewed by two investigators to ensure accuracy before statistical analysis.
Follow-Up
Patients were followed every 3 months for the first 2 years and every 6 months thereafter. Follow-up assessments included nasopharyngoscopy, MRI of the nasopharynx and neck, chest CT, abdominal ultrasound, and plasma EBV DNA testing. Progression-free survival (PFS) and overall survival (OS) were calculated from the date of enrollment to the date of progression, death, or last follow-up.
Outcomes
The primary outcome was the objective response rate (ORR), with secondary endpoints including adverse events (AEs) occurring during the trial and disease-free survival (DFS). ORR was defined as the proportion of patients showing complete or partial response after three cycles of neoadjuvant therapy. DFS was defined as the time from the start of neoadjuvant therapy to the first occurrence of recurrence or metastasis. DFS was evaluated by serial imaging (CT and MRI) every 3 months following treatment completion, in accordance with RECIST version 1.1. Adverse events (AEs) and serious adverse events (SAEs) were monitored using the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE) version 5.0. All AEs were reported by grade and type.
Results
Patients
Thirty-eight patients were enrolled between January 2022 and January 2024 from the oncology outpatient clinic of Anhui Provincial Cancer Hospital (Figure 1). Detailed demographics and clinical characteristics are summarized in Table 1. No stage IVB (M1) cases were included. The median age was 51.9 years (range 26–69), and 76.3% were male. Most had non-keratinising undifferentiated histology. At baseline, 27 patients (71.1%) were EBV-DNA positive, and 78.9% (30/38) had PD-L1 CPS ≥20. The most common comorbidities were hypertension (26%) and chronic hepatitis B infection (10.5%).
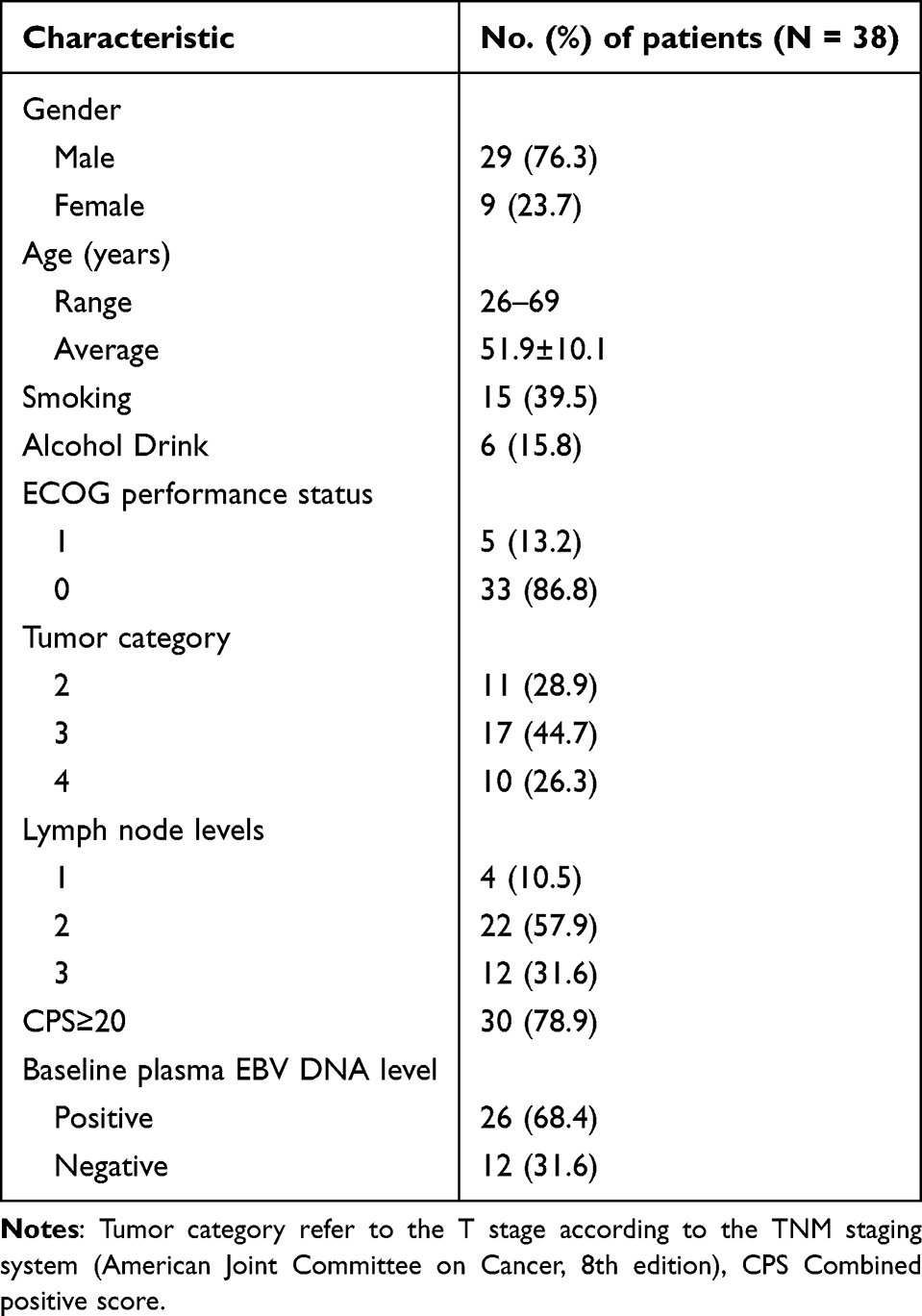 |
Table 1 Patient Characteristics |
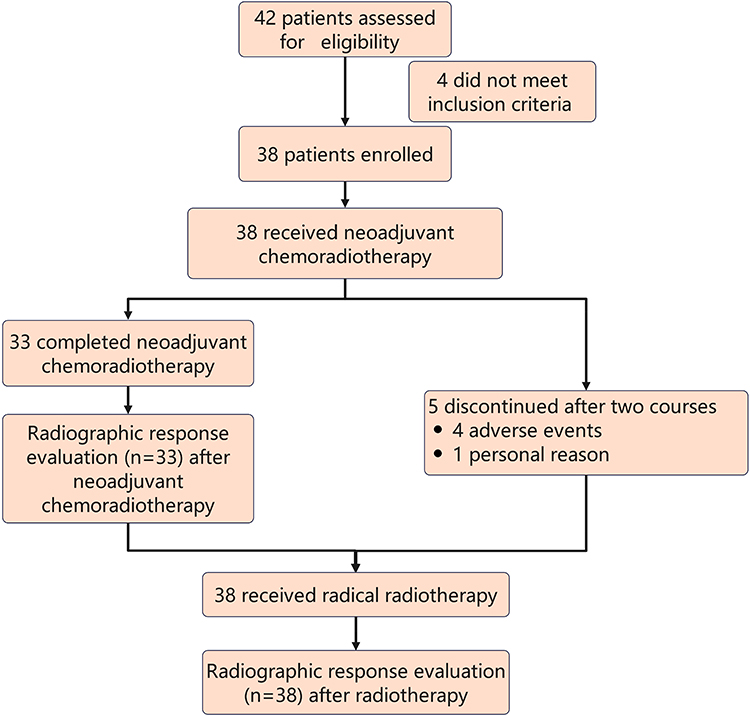 |
Figure 1 Clinical trial flow diagram. |
Safety and Feasibility
Of the 38 patients, 33 (86.8%) completed three cycles of neoadjuvant treatment and proceeded to definitive radiotherapy within the following three weeks. The remaining five patients (13.2%) did not complete the full course of treatment as planned. Four patients discontinued after two cycles of neoadjuvant treatment due to toxicities, and one withdrew for personal reasons. Nonetheless, all 38 patients eventually received radical radiotherapy and completed the entire radiotherapy course.
Treatment-related adverse events (TRAEs) were assessed throughout all three cycles of neoadjuvant therapy and documented per NCI-CTCAE v5.0 criteria. The summary of TRAEs can be found in Table 2. The most common TRAEs were decreased appetite (37; 97.4%), nausea/vomiting (36; 94.7%), and anemia (17; 44.7%). The incidence rates of TRAEs from grades 1 to 4 were 67.8%, 27.3%, 4.9%, and 0%, respectively. Six patients experienced grade 3 adverse reactions: 2 had nausea/vomiting, 2 had thrombocytopenia, 1 had leukopenia, and 1 had immune-related hepatitis. No patients experienced grade 4 adverse reactions or death. AE monitoring was performed at each infusion visit and included blood counts, hepatic and renal panels, and symptom questionnaires. The 3-week interval between the final cycle and radiotherapy allowed for hematologic recovery and radiotherapy planning. Compliance was high: 86.8% completed all cycles on schedule. Among the four patients who withdrew from the study, two discontinued treatments due to grade 3 hematologic toxicity during the second course of neoadjuvant therapy. One patient developed grade 3 immune-related hepatitis, and another developed symptoms consistent with immune-mediated myocarditis (grade 2). After consulting with internists, it was determined that these patients were not suitable for further immunotherapy, leading to their withdrawal from the study. No late severe toxicities were observed within the available follow-up period; ongoing monitoring is planned through 36 months.
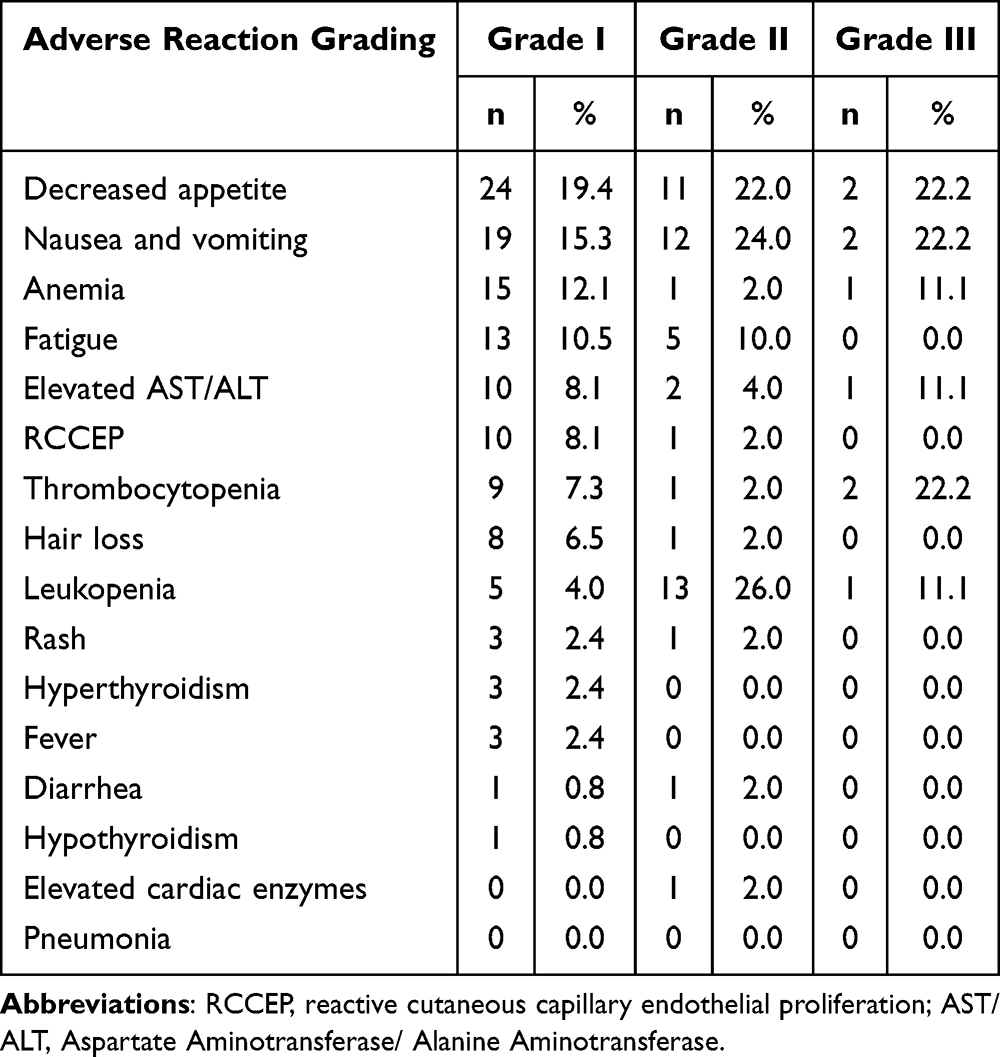 |
Table 2 Treatment‑related Adverse Events (TRAEs) Identified by Investigators |
Efficacy Outcomes
The majority of patients (33 out of 38, 86.8%) completed three cycles of neoadjuvant therapy. Radiological assessments were performed according to RECIST 1.1 criteria. Results are shown in Figure 2. Among these 38 patients, 7 (18.4%, 95% CI, 7.9%-31.6%) achieved a complete response (CR), 27 (71%,95% CI 55.3%-86.8%) achieved a partial response (PR), and 4 (10.6%,95% CI 2.6%–21.1%) had stable disease (SD). The overall response rate (ORR) was 89.4% (95% CI 78.9%-97.4%). No disease progression was observed during neoadjuvant therapy. All patients underwent mid-treatment radiological assessments after 20 sessions of radiotherapy. Among these 38 patients, 19 patient (50%,95% CI 34.2%-65.8%) achieved CR, 19 patients (50%,95% CI 34.2%-65.8%) achieved PR with an ORR of 100.0%. All patients underwent imaging evaluations to assess one month after completing radiotherapy. Among the 38 patients, 32 patient (84.2%,95% CI 71.1%-94.7%) achieved CR, 6 patients (15.8%,95% CI 5.3%-28.9%) achieved PR. The 12-month DFS rate was 94.7% (34/36); two patients were censored due to early recurrence or death.
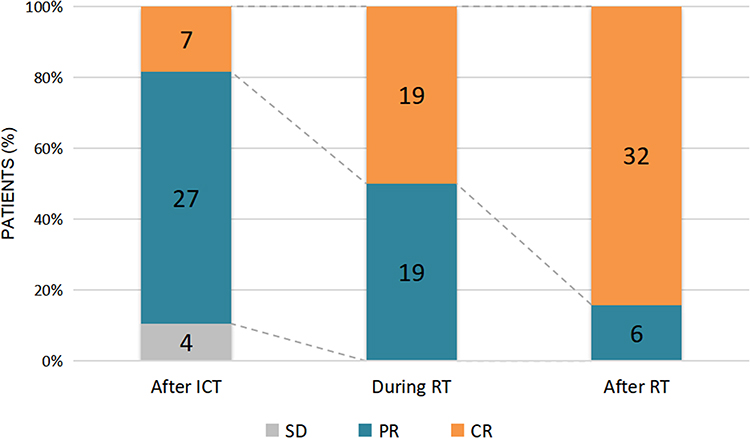 |
Figure 2 Best overall response assessed by RECIST 1.1 at three timepoints. Abbreviations: CR, complete response; PR, partial response; SD, stable disease. |
Biomarker Analysis
To explore potential biomarkers that can predict the efficacy of neoadjuvant chemoimmunotherapy, PD-L1 expression in nasopharyngeal tumor tissues of 35 patients was analyzed. PD-L1 CPS ranged from 0 to 100. CPS ≥20 was observed in 78.9% of patients. No statistically significant correlation was found between CPS and response rate (p = 0.19).
All patients had their peripheral blood plasma EBV-DNA copy numbers measured before treatment, with 27 (71.05%) testing positive for EBV-DNA at baseline. The EBV-DNA values were retested before subsequent treatment cycles. In patients with positive plasma EBV DNA at baseline, 16 patients EBV DNA became negative after the first course of neoadjuvant therapy, 6 patients after the second course, and 4 patients after the third course. Additionally, one patient consistently had positive EBV-DNA levels. Results are shown in Figure 3. Rapid EBV-DNA clearance (within one cycle) was significantly associated with CR at post-radiotherapy evaluation (p = 0.017).
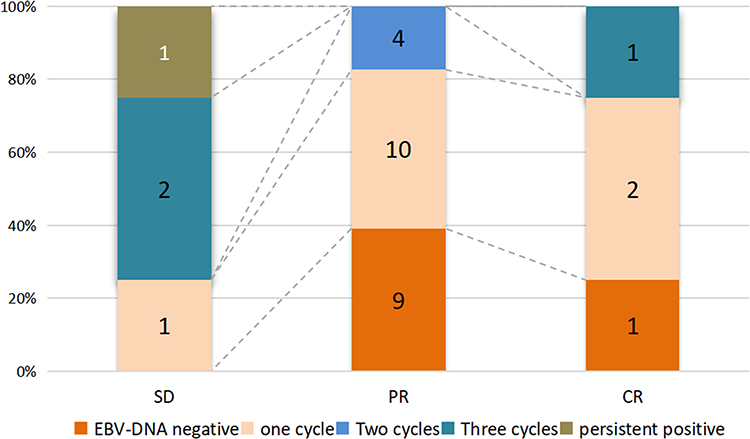 |
Figure 3 EBV-DNA Clearance in Patients with Different Treatment Response. |
Follow Up
As of March 2025, one patient developed liver metastasis 5 months post-radiotherapy, one patient developed lung metastasis 9 months post-radiotherapy, while another experienced recurrence of the primary lesion 6 months post-radiotherapy and subsequently died from complications of malnutrition and infection during chemotherapy. The remaining 35 patients showed no significant disease progression, with a median follow-up time of 25 months (range, 13–37 months) since the start of treatment (Figure 4). The 3-year overall survival (OS) rates will require further follow-up for comprehensive assessment.
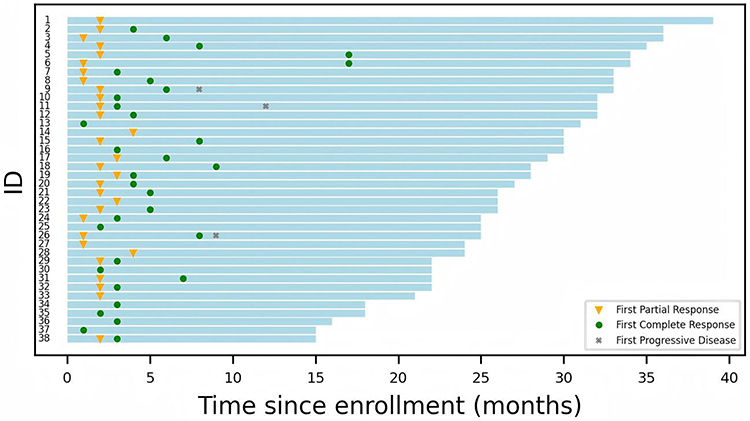 |
Figure 4 Swimlane plot of disease-free survival for individual patients (n=38). |
Discussion
This study demonstrates the feasibility, safety, and promising antitumor activity of neoadjuvant chemoimmunotherapy using camrelizumab combined with gemcitabine and cisplatin in patients with locally advanced NPC (AJCC 8th stage III–IVA, M0) from non-endemic regions.
Treatment feasibility was confirmed by high adherence to the protocol: 86.8% of patients completed all three cycles of neoadjuvant therapy and transitioned to definitive radiotherapy within the scheduled 3-week window. This interval ensured hematologic recovery and allowed time for individualized radiotherapy planning. Only a small fraction required dose delays or modifications, suggesting that the regimen is manageable in real-world clinical practice. In this context, feasibility reflects the combination of protocol compliance, low toxicity-induced dropout, and preservation of downstream radiotherapy timelines.
The ORR of 89.4% after neoadjuvant therapy and 100% mid-radiotherapy ORR compares favorably with previous data from endemic regions. For example, the CAPTAIN-1st trial reported an ORR of 88% in recurrent/metastatic NPC patients treated with camrelizumab plus GP chemotherapy in China.9 Our study extends these findings to the neoadjuvant setting and to non-endemic populations, suggesting that this regimen maintains its efficacy regardless of geographical EBV prevalence. However, the absence of a control arm in our trial limits direct comparison with GP chemotherapy alone or other immunotherapy regimens.
The treatment was well tolerated overall. The most common AEs were gastrointestinal and hematologic, consistent with expected toxicities of GP chemotherapy. Grade 3 AEs occurred in 15.8% of patients, and no grade 4 AEs or treatment-related deaths were observed. A notable camrelizumab-specific toxicity is reactive cutaneous capillary endothelial proliferation (RCCEP), which was observed in 29% of patients, all grade 1, and managed conservatively. This is lower than historical rates of 60–70% reported in hepatocellular and lung cancers treated with camrelizumab,9,13,14 possibly due to the anti-angiogenic properties of gemcitabine. The anti-angiogenic effect of gemcitabine can be achieved through multiple signaling pathways, including the VEGF/VEGFR, PI3K/Akt, MAPK/ERK, and HIF-1α signaling pathways, suggesting that the reduced incidence of RCCEP might be due to the inhibition of these signaling pathways.15
Our study highlights the prognostic utility of plasma EBV DNA kinetics. Among patients with baseline EBV-DNA positivity, early clearance (after the first or second cycle) was significantly associated with improved response (p = 0.017). This finding is consistent with prior studies such as the CAPTAIN-1st trial9 and the POLARIS-02 study,16 both of which demonstrated that early EBV-DNA clearance predicted better objective response and progression-free survival.In contrast, PD-L1 expression measured by CPS was not significantly associated with treatment response (p = 0.19), although 78.9% of tumors expressed CPS ≥20. This may reflect limitations of PD-L1 as a standalone biomarker, as previously suggested by Qian et al in their meta-analysis of immunotherapy predictors in NPC.17 Tumor heterogeneity, assay variability, and the complex immune microenvironment of NPC may all contribute to the inconsistent predictive value of PD-L1. Nonetheless, the high prevalence of PD-L1 positivity in our cohort supports the biological rationale for immune checkpoint blockade in this population. A key insight from our study is the potential for combining EBV-DNA kinetics and PD-L1 expression to improve patient stratification. Patients with early EBV-DNA clearance and high PD-L1 expression may represent an “immune-reactive” subgroup most likely to benefit from neoadjuvant immunotherapy. Conversely, the lack of response in a minority of patients despite high CPS suggests the need for additional biomarkers such as tumor mutational burden, IFN-γ gene signatures, or T-cell receptor clonality.18,19
Our findings, while derived from a single-arm phase II study in a non-endemic setting, align with a growing body of evidence supporting the role of sustained immune modulation in nasopharyngeal carcinoma. Notably, the Phase III CONTINUUM trial in locoregionally advanced NPC demonstrated that the addition of sintilimab to induction chemotherapy and concurrent chemoradiotherapy significantly improved event-free survival (HR ≈ 0.59; 3-year EFS, 86.1% vs 76.0%; P = 0.019), with manageable toxicities.20 These results highlight the therapeutic benefit of continuous PD-1 blockade across multiple treatment phases, extending beyond induction to concurrent and adjuvant settings. Although our trial did not incorporate an adjuvant immunotherapy phase, the promising outcomes observed after neoadjuvant camrelizumab suggest that extending immunotherapy beyond induction may further enhance long-term control. Moreover, comprehensive immune profiling from the CONTINUUM biomarker analysis revealed that baseline and dynamic changes in proliferating Ki67+ regulatory T cells (Tregs) were predictive of relapse and overall response.21 These findings support the rationale for integrating immune-based biomarkers into treatment stratification and for exploring prolonged checkpoint inhibition strategies in future studies.
This trial has several limitations. The single-arm design precludes definitive efficacy comparisons. The modest sample size and relatively short follow-up period limit conclusions regarding long-term outcomes such as overall survival and late toxicities. Additionally, our biomarker analyses were exploratory and limited by sample availability and statistical power. Future randomized controlled trials are necessary to confirm these findings and to explore biomarker-driven strategies. Longitudinal immune profiling, including T-cell activity and cytokine responses, may provide further insight into mechanisms of resistance and response.
Conclusion
Neoadjuvant camrelizumab combined with gemcitabine and cisplatin demonstrated promising efficacy and manageable toxicity in patients with locally advanced NPC from non-endemic regions. Early EBV-DNA clearance may serve as a useful biomarker for treatment response. These findings warrant validation in larger, randomized studies.
Data Sharing Statement
The authors confirm that individual deidentified participant data (including demographic information, baseline characteristics, and clinical outcome variables) will be made available upon reasonable request. The study documents available for sharing include the study protocol, statistical analysis plan, and informed consent form.Data will be accessible by contacting the corresponding author at [email protected]. Data will be available beginning 6 months after publication and will remain available for a period of 5 years. Access will be granted for research purposes following review and approval of a reasonable data request.
Ethical Approval
This study was conducted in accordance with the principles of the Declaration of Helsinki.This study was approved by the Ethics Committee of the West District of The First Affiliated Hospital of USTC, Anhui Provincial Cancer Hospital. All participants provided informed consent.
Acknowledgments
This paper was presented at the SSRN Journal as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in SSRN Journal: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=4930711
Funding
This work was supported by Hefei Municipal Natural Science Foundation Project (Grant No. 202333), the 2023 Provincial Key Medical and Health Specialty Construction Project (Grant No. 2023sjlczdzk01), and the Hefei Clinical Research Center of Proton Radiotherapy, Hefei Comprehensive National Science Center.
Disclosure
The authors declare no conflicts of interest related to this work.
References
1. Caudell JJ, Gillison ML, Maghami E, et al. NCCN guidelines(R) insights: head and neck cancers, version 1.2022. J Natl Compr Canc Netw. 2022;20(3):224–10. doi:10.6004/jnccn.2022.0016
2. Chen L, Zhang Y, Lai SZ, et al. 10-year results of therapeutic ratio by intensity-modulated radiotherapy versus two-dimensional radiotherapy in patients with nasopharyngeal carcinoma. Oncologist. 2019;24(1):e38–e45. doi:10.1634/theoncologist.2017-0577
3. Chen YP, Chan ATC, Le QT, et al. Nasopharyngeal carcinoma. Lancet. 2019;394(10192):64–80. doi:10.1016/S0140-6736(19)30956-0
4. Li X, Peng X, Zhao S, et al. Combined association of tumoral PD-L1 expression and pretreatment presence of epstein-barr virus DNA with risk stratification and prognosis of patients with nasopharyngeal carcinoma. Front Oncol. 2021;11:791411. doi:10.3389/fonc.2021.791411
5. Larbcharoensub N, Mahaprom K, Jiarpinitnun C, et al. Characterization of PD-L1 and PD-1 expression and CD8+ tumor-infiltrating lymphocyte in epstein-barr virus-associated nasopharyngeal carcinoma. Am J Clin Oncol. 2018;41(12):1204–1210. doi:10.1097/COC.0000000000000449
6. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
7. Gong L, Kwong DL, Dai W, et al. Comprehensive single-cell sequencing reveals the stromal dynamics and tumor-specific characteristics in the microenvironment of nasopharyngeal carcinoma. Nat Commun. 2021;12(1):1540. doi:10.1038/s41467-021-21795-z
8. Lee AZE, Tan LSY, Lim CM. Cellular-based immunotherapy in epstein-barr virus induced nasopharyngeal cancer. Oral Oncol. 2018;84:61–70. doi:10.1016/j.oraloncology.2018.07.011
9. Yang Y, Qu S, Li J, et al. Camrelizumab versus placebo in combination with gemcitabine and cisplatin as first-line treatment for recurrent or metastatic nasopharyngeal carcinoma (CAPTAIN-1st): a multicentre, randomised, double-blind, Phase 3 trial. Lancet Oncol. 2021;22(8):1162–1174. doi:10.1016/S1470-2045(21)00302-8
10. Mai H-Q, Chen Q-Y, Chen D, et al. Toripalimab or placebo plus chemotherapy as first-line treatment in advanced nasopharyngeal carcinoma: a multicenter randomized phase 3 trial. Nat Med. 2021;27(9):1536–1543. doi:10.1038/s41591-021-01444-0
11. Dias JM, Santana IVV, da Silva VD, et al. Analysis of epstein-barr virus (EBV) and PD-L1 expression in nasopharyngeal carcinoma patients in a non-endemic region. Int J Mol Sci. 2022;23(19). doi:10.3390/ijms231911720
12. Forder A, Stewart GL, Telkar N, et al. New insights into the tumour immune microenvironment of nasopharyngeal carcinoma. Curr Res Immunol. 2022;3:222–227. doi:10.1016/j.crimmu.2022.08.009
13. Zhou C, Chen G, Huang Y, et al. Camrelizumab plus carboplatin and pemetrexed versus chemotherapy alone in chemotherapy-naive patients with advanced non-squamous non-small-cell lung cancer (CameL): a randomised, open-label, multicentre, phase 3 trial. Lancet Respir Med. 2021;9(3):305–314. doi:10.1016/S2213-2600(20)30365-9
14. Qin S, Ren Z, Meng Z, et al. Camrelizumab in patients with previously treated advanced hepatocellular carcinoma: a multicentre, open-label, parallel-group, randomised, phase 2 trial. Lancet Oncol. 2020;21(4):571–580. doi:10.1016/S1470-2045(20)30011-5
15. Kuwahara K, Sasaki T, Kobayashi K, et al. Gemcitabine suppresses malignant ascites of human pancreatic cancer: correlation with VEGF expression in ascites. Oncol Rep. 2004;11(1):73–80.
16. Wang FH, Wei XL, Feng J, et al. Efficacy, safety, and correlative biomarkers of toripalimab in previously treated recurrent or metastatic nasopharyngeal carcinoma: a phase II clinical trial (POLARIS-02). J Clin Oncol. 2021;39(7):704–712. doi:10.1200/JCO.20.02712
17. Qian X, Chen H, Tao Y. Biomarkers predicting clinical outcomes in nasopharyngeal cancer patients receiving immune checkpoint inhibitors: a systematic review and meta-analysis. Front Immunol. 2023;14:1146898. doi:10.3389/fimmu.2023.1146898
18. Li H, van der Merwe PA, Sivakumar S. Biomarkers of response to PD-1 pathway blockade. Br J Cancer. 2022;126(12):1663–1675. doi:10.1038/s41416-022-01743-4
19. Li Y, Ji L, Zhang Y, et al. The combination of tumor mutational burden and T-cell receptor repertoire predicts the response to immunotherapy in patients with advanced non-small cell lung cancer. MedComm. 2024;5(6):e604. doi:10.1002/mco2.604
20. Liu X, Zhang Y, Yang KY, et al. Induction-concurrent chemoradiotherapy with or without sintilimab in patients with locoregionally advanced nasopharyngeal carcinoma in China (CONTINUUM): a multicentre, open-label, parallel-group, randomised, controlled, phase 3 trial. Lancet. 2024;403(10445):2720–2731. doi:10.1016/S0140-6736(24)00594-4
21. Huang SW, Jiang W, Xu S, et al. Systemic longitudinal immune profiling identifies proliferating Treg cells as predictors of immunotherapy benefit: biomarker analysis from the phase 3 CONTINUUM and DIPPER trials. Signal Transduct Target Ther. 2024;9(1):285. doi:10.1038/s41392-024-01988-w
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effectiveness and Safety of the PD-1 Inhibitor Lenvatinib Plus Radiotherapy in Patients with HCC with Main PVTT: Real-World Data from a Tertiary Centre
Li G, Zhao Y, Li K, Yang S, Xiang C, Song J, Yang Y, Li G, Dong J
Journal of Hepatocellular Carcinoma 2023, 10:2037-2048
Published Date: 9 November 2023
Experience of Symptoms Related to Dysarthria in Patients with NPC During Radiotherapy: A Descriptive Qualitative Study
Li F, Xiong L, Lei C, Zhou S, Leng H, Tang L, Wang C, Ding Z, Ge M, Shi Q
Risk Management and Healthcare Policy 2025, 18:3167-3180
Published Date: 20 September 2025
Thymosin α1 Elevates Lymphocyte Counts and Improves Immunoradiotherapy Outcomes in Patients with Advanced Cancer
Xu M, Chen R, Kong Y, Zhang J, Xing P, Zhao X, Zhang L
Cancer Management and Research 2025, 17:2851-2862
Published Date: 19 November 2025