Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Negotiating Professional Tasks in a Hospital: A Qualitative Study of Rheumatologists and Occupational Therapists in the Management of Hand Osteoarthritis
Authors Magnussen HJ ![]() , Kjeken I
, Kjeken I ![]() , Pinxsterhuis I, Sjøvold TA, Feiring M
, Pinxsterhuis I, Sjøvold TA, Feiring M ![]()
Received 22 June 2023
Accepted for publication 5 October 2023
Published 18 October 2023 Volume 2023:16 Pages 3057—3074
DOI https://doi.org/10.2147/JMDH.S425640
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Hege Johanne Magnussen,1,2 Ingvild Kjeken,1– 3 Irma Pinxsterhuis,1 Trine Amalie Sjøvold,4 Marte Feiring1– 3
1Department of Rehabilitation Science and Health Technology, Faculty of Health Sciences, Oslo Metropolitan University, Oslo, Norway; 2Norwegian National Advisory Unit on Rehabilitation in Rheumatology, Diakonhjemmet Hospital, Oslo, Norway; 3REMEDY - Center for Treatment of Rheumatic and Musculoskeletal Diseases, Diakonhjemmet Hospital, Oslo, Norway; 4REMEDY Patient Council, Diakonhjemmet hospital, Oslo, Norway
Correspondence: Hege Johanne Magnussen, Email [email protected]
Purpose: Societal change and rise in demand for healthcare call for new health professional practices and task redistribution. Through negotiated order theory, this study explores how hospital rheumatologists (RT) and occupational therapists (OT) negotiate professional tasks in the clinical management of hand osteoarthritis.
Methodology: Fourteen qualitative interviews and 16 observations in clinical consultations were conducted in two hospitals specialized in rheumatology in Norway. Participants included eight OTs, six RTs, and patients in consultations. Data were analyzed using reflexive thematic analysis.
Results: Three themes were developed from codes: hierarchical ordering of hospital work impacts interprofessional negotiations; diagnostic organization of tasks preserves RT authority; and evidence-based recommendations in rheumatology enhance OT responsibilities. Overall, RTs and OTs enact tasks in succession where higher-ranking RTs establish a diagnosis and decide the subsequent in-hospital trajectory entrenched in a medical knowledge system. When medicine does not hold evidence-based treatment alternatives for patients, OTs respond by providing therapeutic interventions that are legitimized through international recommendations in rheumatology when they equip patients with tools to cope with chronic illness.
Conclusion: Negotiations over tasks do not take place from equal power positions when status and knowledge hierarchies frame professional practices. The enactment of tasks is concurrently highly influenced by the arena of the workplace, where the two professional groups both cross boundaries and work together in concert despite professional differences in order to meet patient interests and provide relevant healthcare.
Keywords: professional boundaries, negotiated order, disease trajectory, hand osteoarthritis, reflexive thematic analysis
Introduction
Ageing populations with increasingly complex healthcare needs and greater attention to person-centered healthcare transform the organization of healthcare services1,2 and, subsequently, health professional work. To address these changes, policymakers call for a stronger focus on health workforce resources over the traditional division of professional labor, with consequences for health professions and their patients, and the distribution of tasks between them.3 Changing the tasks of one profession will impact those of others, highlighting relational aspects of health professionals and their work.4 Through abstract knowledge and specialized skills, health professionals control their own work.4,5 Simultaneously, the large majority works within the public sector in Norway, thus employment and career opportunities depend considerably on the state in welfare societies.6,7
Professional boundaries can broadly be understood as socially constructed demarcations of what the competencies and activities of a profession are.8 Health professionals work in complex and constantly changing environments that influence the relationship between them.9 In rheumatology, European recommendations emphasize key competencies of rheumatologists (RT) and occupational therapists (OT) in managing hand OA, including appropriate knowledge, skills, clinical reasoning, values, and reflective practice.10,11 RT tasks are to diagnose and explain hand OA and decide on relevant treatment and referrals.12,13 OTs typically offer patient education, propose hand exercises, and recommend assistive devices,14 often upon referral from RTs. However, evolving healthcare needs have prompted investigations into alternative care delivery models. Studies have indicated that when OTs diagnose and manage hand OA, patient pathways and standards of care can be improved.15,16 These changes are shaped in the workplace arena where demarcation lines are constantly negotiated in the process of controlling tasks through jurisdiction.4 As such, professional boundaries can serve differentiation and exclusion purposes in the hospital when health professionals interact17–19 and contribute to protecting autonomy and control.20
Professional boundaries are also valuable sites for communication and inclusion through boundary objects in the relationship between actors.21 Boundary objects are shared objects that are anchored in and have different meaning for different actors, while also having the capacity to stay meaningful and bridge intersecting social worlds. Such shared objects enable collaboration across professional disciplines through agreed methods of standardization,22 making it possible to develop mutual understandings about who will do what in the hospital.23
In Norway, the Health Personnel Act24 regulates health professionals’ work without distinguishing between which professional is responsible for providing specific services and tasks. One exception is “matters concerning medicine” (section 4) where the superior position of medical practitioners in decisions regarding diagnosis and treatment is explicated, harmonious with Freidson’s medical dominance perspective.25,26 Medical education was included in the establishment of the first Norwegian university in 1811.27 State authorization to practice medicine was introduced in 1927,28 and historically the medical profession has had an influential role in defining medical reality, representing a biomedical care model. The rheumatology discipline was approved as a medical specialization by the Norwegian Medical Association in 1949.29 Together with OTs, RTs30 are central in responding to the needs of persons with hand osteoarthritis (OA).31
OT education was first established in Norway in 1952 in response to increased demands for health and rehabilitation services after World War II.32,33 Authorization to practice was obtained in 1975,34 and OT involvement in rheumatology was realized in the 1950s upon their employment at the first Nordic rheumatism hospital.35
Hospital hierarchies and political struggles influence day-to-day professional work.36 The outcome of one interaction will be brought into the next, and power manifests through prestige, priorities, and professional knowledge differences that shape negotiations.37,38 These negotiations are influenced by existing structural arrangements that have come into existence through earlier negotiations within what Strauss et al39,40 coined a “negotiated order”. The negotiated order theory is rooted empirically in fieldwork in two psychiatric hospitals to understand social interaction. The perspective proposes that all social orders have temporal limits when continuously negotiated. Taken-for-granted social structures resulting from patterned negotiations will eventually be evaluated, renewed, and adjusted as events occur over time.41
The negotiated order perspective articulates both the individual agency of and structural influences on those involved in understanding social life in hospitals. We root our study in the principle that hospitals are highly institutionalized, inherently structured, and permeated with societal norms and expectations that influence negotiations in the clinical management of hand OA. Power must therefore be taken into consideration if we are to better comprehend interprofessional interactions in the hospital division of labor. In our study, we understand power in negotiated order as fluid, unfinalized, contextually situated, and inherent in all negotiations. The power of the actors therefore continuously transforms in response to unfolding events over time. Through such a lens we align ourselves with Clarke,42 who emphasizes that power clearly matters in negotiations.
Studies of health professional interactions have used the negotiated order perspective to characterize the range of negotiations that take place, from those agreements easily made to those more forcefully put in place,43–46 demonstrating how negotiations can be seen as processual arrangements between actors that influence structure.42,47 At the same time, calls have been made for more attention to be paid to the order in negotiated order to increase comprehension of what such structures do to healthcare interactions.38,48 Inspired by a constructionist approach,49 we use empirical data from outpatient hospital services to explore how structural arrangements impact the governing rules of negotiation and action when health professionals demarcate their own domain of expertise and control in the distribution and enactment of tasks. In this article, we understand professional tasks as “human problems amenable to expert service” based on three acts: classifying a problem, reasoning about it, and taking action on it.4 In this context, we formulated the following research question: how do RTs and OTs negotiate tasks in outpatient hospital services?
Methodology
Context
The Norwegian welfare state has increased healthcare spending considerably in recent decades, and political concerns over public healthcare funding contributed to implementing reforms inspired by New Public Management to increase efficiency and coordination.50,51 Following a hospital reform in 2002, the state has responsibility for hospital healthcare. Both hospitals in our study are specialized in rheumatology, privately owned through trusts and not for profit. State funding and referral mechanisms are equal to public hospitals.
In rheumatology, the introduction of new medicines into clinical practice over the past two decades has revolutionized the treatment of major chronic inflammatory diseases. Disease remission became an achievable target that improved outcomes.52 Consequently, in-hospital treatment of numerous complex patients was transferred to rheumatology departments focusing largely on outpatient services. This transformation influenced healthcare organization and, subsequently, OTs and RTs work. In Norway, persons with hand OA should mainly be attended to in primary health care.53 However, due to poor access to relevant services, they are often referred to outpatient specialist care where services are mainly provided by RTs and OTs.54,55 The diagnosis is based on the patient’s history and a clinical examination.56 Recommended treatment for all persons with hand OA include patient education and hand exercises, while orthotics, pain medication and surgery are considered individually.57
Research Team
Our study is part of a three-phase project with the following aims: to gain a comprehensive understanding of current hand OA healthcare practices and task distribution along the trajectory (qualitative methods); to evaluate through a randomized controlled trial whether OT-led care is as safe, effective and cost-effective as traditional RT-led care with respect to treatment response and patient satisfaction,58 and to design a novel, safe and feasible care pathway for patients with hand OA and develop strategies for implementing this pathway (Delphi consensus process). The first author, HJM, currently a PhD student, has 20 years of clinical and managerial experiences as a physiotherapist and humanitarian health worker. The co-authors include two professors and an associate professor with occupational therapy backgrounds, one of whom is also a sociologist, and a patient research partner. Additionally, an international advisory board was consulted, consisting of researchers representing diverse professional backgrounds.
Participant Recruitment
Two hospitals providing services to persons with hand OA were included to provide “similar and contrasting” contexts.59 Eight OTs and six RTs were included after being approached by a study coordinator. Upon agreeing to participate, the professionals were contacted by HJM for further information about the study. The participants included two men and 12 women aged between 27 and 67, six of whom worked in hospital A and eight in hospital B (Table 1).
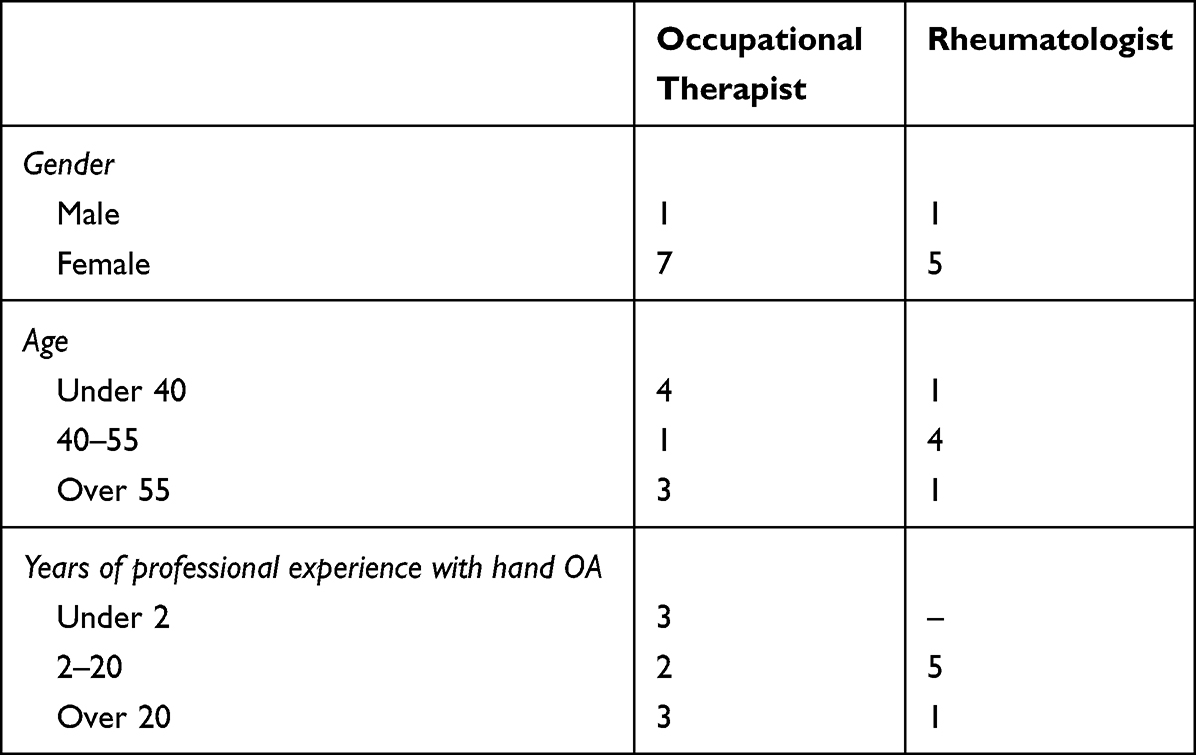 |
Table 1 Participant Demographics |
Relevant consultations for observation were identified by the study coordinators or through RT referrals evaluation. Participants were asked by HJM during interviews if she could participate in consultations subject to the patients’ approval. Four OTs and three RTs agreed. The remaining seven participants had either changed job or said they no longer worked with the patient group. Patients with suspected or confirmed hand OA were contacted for inclusion by study coordinators and gave their approval prior to the consultations. Consequently, a relationship between HJM and the included professionals had already been established through interviews conducted prior to the observations, while encounters between HJM and the patients took place for the first time. To ensure rigor, authors continuously discussed analytical steps, including adequate number of study participants. Malterud’s information power, determined by study objective, participant specificity, theoretical framework, quality of interviewing and analytical approach60 informed our decision to stop at 14 interviews and 16 consultations. Our evaluation was guided by study participants having specific characteristics for the study aim, application of negotiated order theory to the analysis, and HJM’s health professional background and previous qualitative in-depth interviewing experiences facilitating quality dialog.
Data Generation
Our research question about how health professionals negotiate tasks was approached using qualitative interviews with RTs and OTs and the participation of HJM in hand OA clinical consultations (Table 2). Data were generated between December 2020 and February 2023. In-depth interviews were seen as applicable in exploring participants’ perspectives, providing us with detailed accounts of events and situations that would otherwise be inaccessible. We developed and piloted an interview guide (Supplementary Material 1) that focused on tasks and responsibilities, collaborative practices, and competencies. Interviews were 45–75 minutes in length. Eleven interviews took place face to face in rooms in the hospitals that allowed for private conversations, and three interviews were conducted digitally.
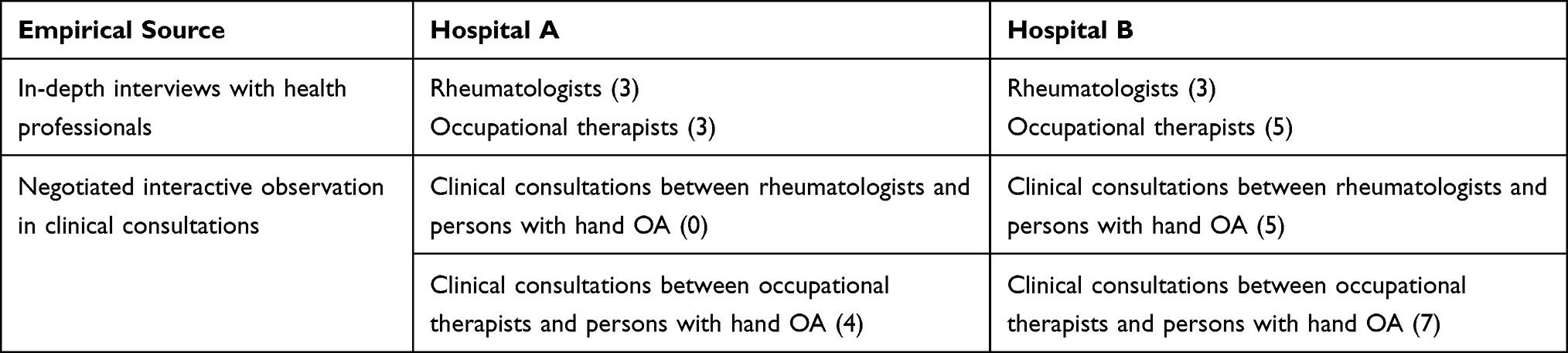 |
Table 2 Overview of Empirical Sources for the Two Hospitals |
We used an interview style whereby participants shared experiences while HJM directed the conversation towards the study goal by asking questions and probing.61 We intentionally used an open posture and listening style, maintained eye contact and repeated what participants said in efforts to enhance and progress the interview encounter. The interviews made professional practices understandable when participants talked about them,62 while we also recognized that complementing participants’ stories with observations in clinical consultations would benefit our understanding of how RTs and OTs negotiate tasks.63 Through observations, we aimed to study first-hand how participants went about their day-to-day work to gain situated understandings of encounters across the two hospitals.64 Thus, HJM participated in 16 clinical consultations, providing an insider perspective through participation while simultaneously placing HJM on the outside as an observer,65 negotiating interactively in the clinical consultations to obtain a credible role during observations.66 Negotiated interactive observations were structured through planned consultation times and locations. This approach was chosen to capture the clinical work that is often a central site of interprofessional collaboration.43,67
From an ethics perspective, observing patients required us to obtain their informed consent in advance. We therefore also made consultations the focus of observations to safeguard the process of obtaining patients’ informed consent. During observations, the negotiated role of HJM altered from that of an observer to that of an assistant, advisor or researcher when health professionals and patients actively engaged. Requests from health professionals to pull curtains aside, check colleagues’ availability or confirm or elaborate on information provided to patients were examples of HJM’s shifting roles. During observations HJM consciously positioned herself in the background as a respectful gesture to participants. We used the Services for sensitive data secure platform to store data, in compliance with the Norwegian privacy regulation. Audio files were immediately encrypted and transferred post-interviews.
Data Analysis
Our analysis arose from an interest in understanding interprofessional tasks division from our own experiences as health professionals and patients, combined with a theoretical curiosity in Abbott’s professional tasks and Strauss’ negotiations. We applied reflexive thematic analysis to report patterns in the data,68 where the subjective and active positions of the researchers in engaging with the data and the larger context were integral to the analytical process.69,70 In practicing reflexive consciousness about our own perspectives and welcoming the perspectives of others throughout the data generation process, we strived to understand perspectives in context and encourage dialogue through interviews and observations, rather than aiming for a singular truth.71 Data structuring was done through NVivo R1, 2020. All interviews were conducted by HJM, who took field notes and transcribed 11 interviews verbatim. A research assistant transcribed three interviews. Debriefs with co-authors and peers took place after each interview to increase awareness about how HJM influenced the research process and data development. Such discussions were valuable to better grasp the strengths and constraints of analyzing from HJM’s perspective as a former clinician and a current researcher. To become familiar with the content breadth and depth, HJM initially read the transcripts in the order in which the interviews had been conducted to gain an overview of the data material while taking reflective notes. The transcripts were thereafter organized by profession and hospital and re-read to provide HJM with a more comprehensive understanding from a contextual and professions perspective.
The analysis of negotiated interactive participation began in the field with note summaries and by identifying salient ideas. Separate fieldnotes from the two hospital sites were merged to examine data from all observations jointly. We approached the data through combining empirical data and theoretical understandings72 in generating codes and themes. Through a combination of inductively reading the data, using scholarly literature focusing on interaction, professional boundaries and negotiations, and her own experiences, HJM developed a series of semantic and latent codes. Semantic codes were developed from the interview data at an early stage. Eleven out of 14 interviews had already been conducted and the coding process was ongoing when we obtained ethical approval for the negotiated interactive observation in consultations. Our early analysis of interviews therefore influenced the subsequent understanding of data from observations. Integration of both data sources into one dataset resulted in the evolving and organic development into more latent codes.
Codes were thereafter sorted into potential themes, discussed by the research team, reviewed, refined, and further discussed to ensure that patterns of shared meaning with relevance to the codes had been captured across the dataset.73 As we moved forward in the analysis, we produced empirical material which over time gave rise to refinements of concepts and to the development of themes from codes (Table 3). Early semantic focus of the data suggested an unequivocal division of labor with few common tasks and sparse negotiations. Through developing a more interpretative, contextualized, and theoretically informed analysis, our analytical focus shifted from that of negotiations to that of the social structures that framed interaction. As such, we used the accounts of participants as an introduction to enhancing our understanding of broader sociocultural aspects of outpatient hospital work, where we viewed language as an active creator of meaning. The iterative process gave us a deeper understanding of the themes and how they were connected, resulting in the development of an overarching interpretive story of interprofessional hospital negotiations.74 Engaging multiple authors in the analysis helped uncover and challenge taken-for-granted assumptions. Only HJM was immersed in the field, and critical discussions with co-authors and peers provided a balance of closeness and analytical distance. Our complementary data generation approach through interviews and observations, prolonged field engagement, deep and insightful interactions with the data set, and a detailed description of the analytical process contributed to enhance the study’s rigor.
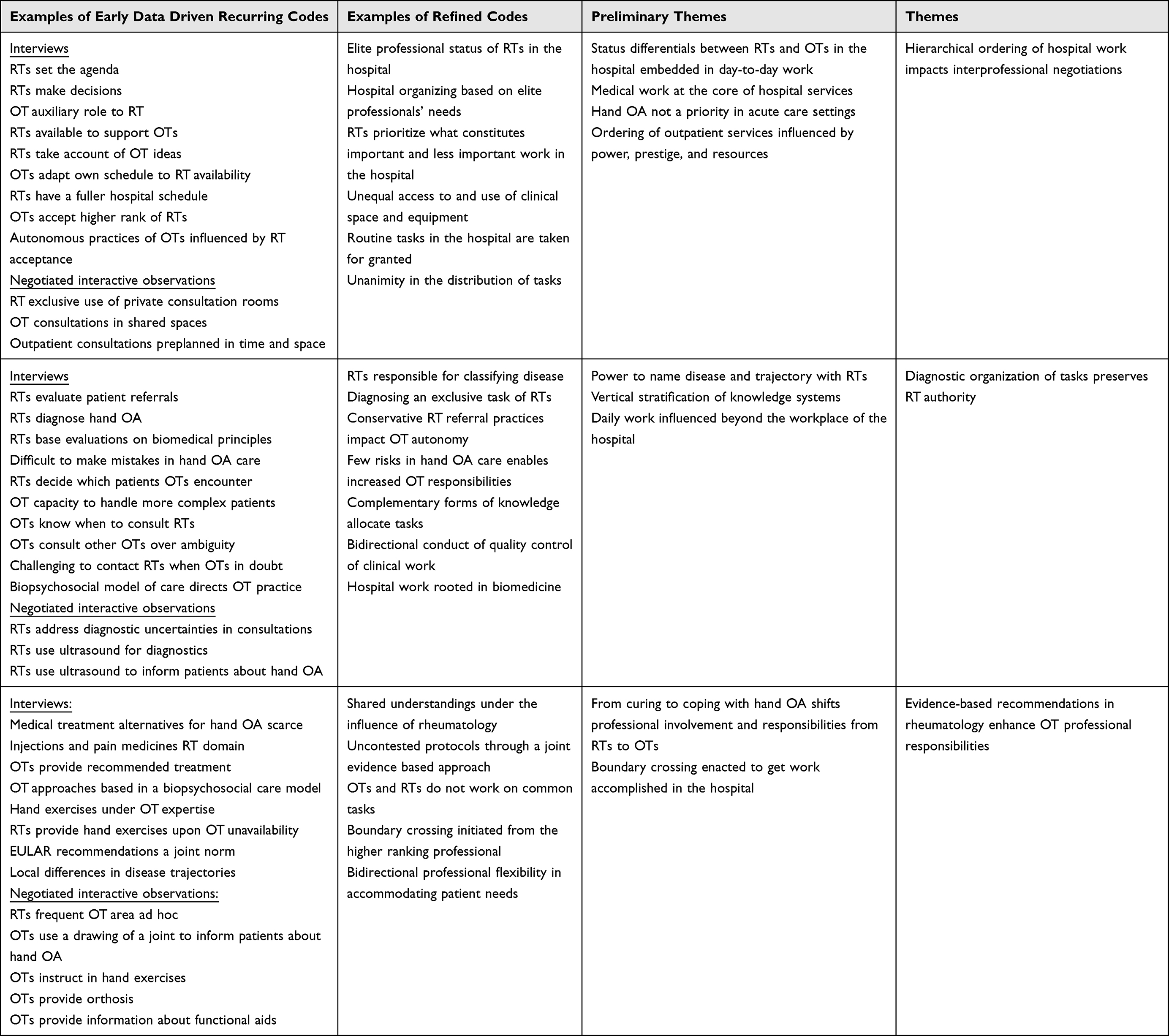 |
Table 3 Codes and Themes Development |
Ethical Considerations
Ethical approval for this project was granted by the Regional Committee for Medical and Health Research Ethics (case number 2017/742, 2020/8450) and the Norwegian Centre for Research Data (reference number 197320). The study was performed according to the Declaration of Helsinki. Written informed consent was obtained from participants, including publication of anonymized responses. Participants were informed that they could withdraw from the study at any time and that data would be handled confidentially. To preserve anonymity and support participation, we have limited participants’ demographic information. Throughout the analytical process and in encounters with participants, HJM emphasized her role as a PhD student with an interest in healthcare encounters and with little clinical experience in hand OA. This was done to inform participants that the research aims did not in any way involve testing their professional competencies or skills and that the research participants were seen to hold expert knowledge about their own professional practices.
Results
In our analysis, we developed three main themes from codes (Table 3) to explore how RTs and OTs negotiate professional tasks in hand OA care. First: hierarchical ordering of hospital work impacts interprofessional negotiations. Second: diagnostic organization of tasks preserves RT authority. Third: evidence-based recommendations in rheumatology enhance OT responsibilities.
Hierarchical Ordering of Hospital Work Impacts Interprofessional Negotiations
Our analysis showed status and legitimacy differentials between the two professional groups, where medical dominance impacted task distribution in the hospitals.75 The hierarchical organization of hospital work is well recognized.76,77 In our study, we could observe the hierarchy in action through the allocation of clinical spaces for therapists and doctors, exemplified in hospital B where 13 RTs and three OTs worked. Each doctor occupied a 20-square-meter room containing an examination bench, an ultrasound apparatus, a trolley, a sink, a double desk with computer and printer, chairs and a bookshelf. A large window with striped curtains in blue, green, and burgundy looked out onto a small forest area. Rooms were assigned to single RTs for a full day, demarcated through a sign on the room doors showing the doctors’ full name. During clinical consultations, RTs made use of digital patient journals, a dictation device and an ultrasound apparatus.
Three OTs shared a room situated in the same outpatient corridor. The room used for patient consultations was a former training kitchen measuring 10 square meters, and contained a one-by-one-meter square table, two chairs and a bookshelf, kitchen cabinets and equipment. The room was frequently used by one of the therapists. A transit area adjoining the room was used for patient consultations. The transit area also served as an orthopedic workshop where OTs fabricated orthotic devices. A window looked out onto the outpatient corridor, where people’s movements and conversations and various alarms impacted consultation privacy. A dark green partition wall partly covered a round table used for consultations to maintain patient confidentiality. A sign above a door in the outpatient corridor read “Occupational therapy services”. During clinical consultations, therapists wrote on printed paper and used an illustration of a joint and a skeleton hand model to provide OA information to patients. These distinctions between access to and use of clinical space and equipment contribute to labeling value, quality, and relevance in the hospital, to vertically stratifying practitioners across groups and sustaining a taken-for-granted hierarchical ordering of outpatient services based on power, prestige, and resources.
Such an ordering was further reflected in the therapists’ perspectives when they talked about doctors as agenda setters and decision makers: “And the doctors set the agenda, they make decisions at the end of the day, no matter what.” (OT5). This influential RT position described by OTs in day-to-day hospital work shaped professional relationships to the extent that “rheumatologists set the agenda in such a way that we [OTs] cannot make progress here if they are not on board” (OT4). This reflects how RTs are perceived by OTs to have the power to impact the professional autonomy of OTs through the hierarchical hospital structure when advances in OT practices depended on RT acceptance. Subsequently, doctors’ professional status within the negotiated hospital order influences how hand OA services are defined and acted upon. Concurrently, subjective reports of the therapists we interviewed contained few expressions of dissatisfaction with RTs in daily work related to status or power. In contrast, therapists commended the collaboration with RTs, describing how RTs took account of their ideas and opinions. In a similar vein, doctors made few claims in interviews to control the therapists’ work: “I have never taken part in their patient consultations. I assume it is well taken care of by the occupational therapist” (RT5). Doctors conveyed that the therapists carried out independent work and that doctors were “available in the background to help the occupational therapist” (RT2) upon request. In our study, OTs did not contest the higher rank of RTs in making decisions and setting the agenda. This notion was further reinforced when therapists described their auxiliary roles in relation to doctors. When discussing the expansion of clinical responsibilities, therapists emphasized the relief they provided to doctors’ work rather than their own independent and meaningful contribution to patient care. This serves to illustrate how, through a hierarchical structuring, the hospital work environment positions doctors at the center of activities.
The key position of doctors was further highlighted during interviews with therapists who often described planning their own clinical tasks in accordance with RT schedules. Therapists would plan for fewer patients and have time slots available ad hoc to cohere with the doctors’ work patterns and routines, contributing to preserve RTs position at the apex of the hospital interprofessional hierarchy. The RTs’ strong influence on the temporal organization of work provided stability through a predictable timetable. In combination with the flexibility of OTs, a structuring of tasks to facilitate the patient pathway could be sustained. By understanding and complying with these rules, OTs contributed to a collaborative environment with RTs and to sustaining the hierarchical order that influences negotiations. Given that medical work is fundamental in the hospitals, the organization of tasks and activities is based on the needs of RTs regarding technological, infrastructural and personnel support. As such, the medical dominance is an organizing principle in the delivery of outpatient services and can be seen as a taken-for-granted structural feature of the labor division in the hospital.
The hierarchical structuring was also visible in disease and patient prioritization, where hand OA was perceived by RTs to be of low priority compared with other rheumatic diseases. The low status of hand OA shows how RTs play a central role in distinguishing between important and less important work within the hospital which have implications for OTs, illustrating how negotiations do not take place from positions of equal power. At the same time, professional boundaries are agreed upon and reinforced by cooperating RTs and OTs. This demonstrates how the hospital hierarchy establishes and maintains a social order and provides a template for how to interact and execute daily tasks. Such social structures contribute to sustaining consensual allocation of tasks and a fixed rather than flexible negotiated order through a taken-for-granted hierarchy.
The Diagnostic Organizing of Tasks Preserves RTs’ Authority
Our analysis shows that the hand OA diagnosis shaped the hospital structure and contributed to social order through the explanation of illness, identification of treatment and resource allocation.78 Hence, the diagnosis was useful in the everyday organization and routines in hospitals.79 In our study, referrals of persons with hand symptoms to the hospitals were evaluated by RTs, who decided on whether RTs or OTs should assume responsibility in the subsequent in-hospital trajectory:
It’s like a sieve when a referral comes to a senior doctor, a rheumatologist. Once you have a good referral, you can see what it concerns. But when in doubt, we see the patients. Not because of questions about hand osteoarthritis, but because we suspect there may be something else, but then we need a good referral, right? It is therefore the senior doctors who evaluate the referrals. This is about how much experience you have in the field and how much you gain by reading the referral. (RT2)
The metaphor of a sieve was used by the RT to highlight the key position of her profession in reducing ambiguity and enabling relevant clinical decisions based on a diagnosis rooted in medical knowledge. This shows how classification through diagnosing is a key organizing principle within the hospitals that is controlled by RTs. The social power of RTs to name hand OA and the subsequent disease trajectory served an important purpose in organizing the tasks of both RTs and OTs under the RTs’ authority:
When we read referrals, we see that ok, this patient can primarily see the occupational therapist, that’s most important. If the referral clearly states osteoarthritis, we don’t automatically channel them to a doctor; then it’s mainly an occupational therapist and hand exercises. (RT4)
As such, doctors control the diagnostic process that structures the healthcare services organization and tasks distribution in the hospital. These practices undertaken by RTs were often perceived as conservative by therapists:
Now, if there are some [patients] who they [rheumatologists] see clearly have osteoarthritis, then they [patients] come to us first. I think they [rheumatologists] are very cautious about who they send to us. I feel they’re very cautious – it has to be crystal clear to them that it’s osteoarthritis – [they] could perhaps take more of a chance on it, that we can fix this. (OT1)
In interviews, OTs expressed opinions about having the capacity to deal with more complex patients than what the conservative RT referral practices allowed for. This shows how RTs influence OT professional boundaries when deciding the degree of patient complexity under therapist expertise and control. Concurrently, by claiming ownership of patients with uncertain diagnostic status, RTs preserve their own professional authority originating in a medical knowledge system. The conservative referral practice may serve the purpose of sustaining RTs’ control of the diagnostic process. OTs had few opportunities to influence the diagnostic process, which illustrates RTs’ decisive position in drawing up the boundaries of medical knowledge in the hospital’s negotiated order.
When doctors saw it as their responsibility to handle diagnostic uncertainty, they also assigned the task of diagnosing exclusively to their own profession: “I feel very strongly that establishing a diagnosis, deciding treatment, that’s the responsibility of the doctor” (RT5). This illustrates how diagnosing patients is a central task and closely linked to their professional identity. It also shows how diagnosing calls for medical decisions and conclusions that are exclusively under RTs’ area of medical expertise when they classify the problem and reason about the subsequent pathway. Therapists shared this view: “It should be clear that it is osteoarthritis when we get them [patients]. We don’t diagnose”, (OT6) “we don’t have the medical competence to establish a diagnosis” (OT8). Even though the task to diagnose was exclusive to RTs in our study, the perceived low risk associated with a hand OA diagnosis impacted the clearly demarcated boundary:
I think it’s important not to sort of dilute what are medical tasks and what are not medical tasks. But at the same time, we’re at this with hand osteoarthritis. Then you must look at these individual cases where you kind of acknowledge that there are no clear pitfalls here. It’s hard to make mistakes here. And if you have other professions that have good experience and are well trained and have a lot of knowledge, they also have that ability to kind of acknowledge when the patient might have to be assessed by a doctor then, right, in the few cases there might be. In the case of hand osteoarthritis. (RT6)
The RT specify minimal risk and few consequences for patients when considering the possibility of OTs to see more complex patients and potentially independently diagnose. RTs accepted increased OT responsibilities by therapist abilities to know when to consult a doctor for support, limiting the scope for OTs in diagnosing. One RT described situations where a more severe diagnosis like rheumatoid arthritis was not detected in the medical screening process:
[…] something is overlooked, presented as an osteoarthritis, and ends up with the occupational therapist after we channel them there for hand exercises and orthosis. My experience then is that the occupational therapists react and send the patient back to us. (RT5)
Both RTs and OTs described how therapists consulted doctors if they detected symptoms beyond hand OA. “I believe we have a duty to report to a rheumatologist if we discover something that deviates from what we know about osteoarthritis” (OT6). New information, increased pain or symptom changes increased OT responsibilities when they had to decide on whether to consult a doctor. Most OTs involved other OT colleagues prior to consulting a RT, either to reduce clinical uncertainties through intra-professional discussions or by receiving confirmation from peers that could justify RT contact. While uncertainties could often be addressed with doctors ad hoc in the joint outpatient corridor in hospital B, therapists in hospital A had less frequent face-to-face interactions with RTs. OTs in hospital A therefore depended largely on the on-call doctor, and RTs were perceived as either collaborative and easy to contact or as lacking any interest in hand OA, which subsequently discouraged OTs from contacting them. The OTs’ practice of questioning the established hand OA diagnosis was not perceived by RTs to challenge their diagnostic jurisdiction. On the contrary, the actions of therapists in disclosing other potential diseases were seen by doctors as acts of quality assurance in favor of good clinical practice.
The exclusive task of RTs to establish a diagnosis also influenced OTs when providing patients with orthoses. Orthotic management was solely under therapist jurisdiction, but refund entitlement from the Norwegian Labour and Welfare Administration depended on diagnostic confirmation and a doctor’s signature. This shows how the diagnostic power of RTs goes beyond the negotiated order of the hospital when day-to-day work in the hospital is intertwined with societal structures that influence understandings of who should do what in the hospital. The superiority of medical knowledge in establishing a diagnosis and organizing work narrows the scope of interprofessional negotiations. Subsequently, the medical knowledge system embedded in the negotiated order of the hospital contributed to preserving RTs’ authority over the distribution of tasks.
Evidence-Based Recommendations in Rheumatology Enhance OTs’ Responsibilities
In our study, hand OA diagnostic confirmation by doctors changed the disease trajectory from that of providing a potential cure to one of offering patients support to cope with the disease based on recommendations rooted in evidence-based medicine and healthcare. This major evidence-based trend has gained substantial momentum in the past decade,80 advocating that effective healthcare interventions are based on scientific knowledge. Accompanying guidelines, checklists, and performance indicators in increasingly bureaucratic healthcare systems contribute to further standardizing the practices of clinicians.81,82 The change in disease trajectory in our study was accompanied by a transfer of responsibilities from doctors to therapists:
When it comes to hand osteoarthritis, we as rheumatologists cannot offer a specific rheumatic treatment. Patients will get the most relevant help from occupational therapists. (RT3)
RTs had few medical alternatives beyond temporary pain medication for patients with hand OA. OTs were consequently given a key role in providing services:
It’s obvious that hand exercises and the right use of assistive devices are central to treatment; it’s the only treatment when it comes to improved function, that’s how I see it. (RT6)
As such, OTs are in the position to take action to address the problem.
Doctors emphasized how they fell short of treating hand OA as long as research evidence and experiences for medical interventions was scarce. Concurrently, RTs highlighted the relevance of clinical interventions by therapists, often aligning with the European Alliance of Associations for Rheumatology’s (EULAR) hand OA management recommendations when they cited information, patient education and hand exercises as central to patient management. OTs expressed similar views: “We have EULAR’s guidelines, we follow the guidelines that are laid down in rheumatology” (OT3), emphasizing their own pertinence in providing relevant interventions: “I think that seeing an occupational therapist is the most important thing for these patients” (OT1); “Patients don’t get it elsewhere, they don’t get it from their GP, they don’t get it from the rheumatologist, they have to get it from us” (OT4). This shows how professional tasks are structured in line with current medical research and disciplinary recommendations. A joint evidence-based approach enabled a disease trajectory without contested boundaries. Influential EULAR recommendations contribute to sustaining order by uniting doctors and therapists in interpreting, understanding, and managing hand OA. The consolidated scientific base allowed for tacit agreements where shared understandings and knowledge existed under the umbrella of rheumatology. Altering such an evidence-based order would require the emergence of new knowledge and the availability of more efficient medicines, illustrating how the division of tasks can be more prone to external developments than to day-to-day negotiations in the workplace arena.
A clear indication of a hand OA diagnosis resulted in different negotiated orders and trajectories in the two hospitals in our study. In hospital B, where a randomized controlled trial had taken place to evaluate whether OT-led care was as safe, effective, and cost-effective as traditional RT-led care, persons with hand OA were assigned to individual outpatient consultations with a therapist. OTs and RTs worked in proximity to each other along the same hospital corridor. This proximity facilitated a culture where day-to-day work frequently included brief encounters to discuss patients, request support and check availability. Observations showed that RTs repeatedly entered the OT’s office to ask for therapist availability in following up individual patients. OTs made efforts to accommodate such requests even though that was not always possible due to heavy workloads. In interviews, both OTs and RTs highlighted flexibility in accommodating patient needs:
I can say that it is successful when I have a patient who mainly has a hand osteoarthritis and I get an appointment for that patient with the occupational therapist on the same day. Then I feel it’s successful. (RT5)
This shows how continuous negotiations over patient management take place in daily encounters to address patient needs.
In hospital A, doctors routinely referred patients with hand OA to a monthly one-day patient education program organized by OTs. Health professionals (nurses, nutritionists, physiotherapists, and OTs) and a patient representative provided information about hand OA, hand exercises, orthosis, assistive devices and medicines, followed by participants’ questions, comments and exercises. Finally, an RT would attend for one hour to answer questions and “tie up loose ends” (RT1). Through the structuring of the patient education program, a social order was negotiated and sustained. OTs were responsible for the organization while RTs assured quality and concluded the day, aligning with their higher rank and superior medical knowledge. Negotiations about the low status hand OA diagnosis during monthly interactions in hospital A take on different forms than daily negotiations over need of individual patients with hand OA in hospital B, thus contributing to different hospital orders.
Even though RTs and OTs did not work together on common tasks, our analysis also indicate boundary crossing in the division of labor. RTs who instructed patients in exercises for the hands made on-The-spot accommodations to overcome boundary rigidities: “And occasionally, if an occupational therapist is not available, I give some instruction in training methods and refer to websites that may be useful” (R6). In situations where patients had travelled long distances or where functional limitations made it challenging to return to the hospital later, RTs performed work outside of their regular scope of practice. These impromptu acts were performed to accommodate individual patient needs in the absence of available OTs rather than to intentionally enter and test the therapists’ jurisdiction. Such a rupture in the hospital order was initiated by the RT, the elite professional. OTs were aware of these practices, though with some reservations: “Rheumatologists present easy solutions; patients don’t get the careful explanations we provide” (OT2). Therapists emphasized how they “do exercises with the patients, make sure they are doing it right, explain why they should do it this way and that way so that they can understand the purpose” (OT8). This illustrates how OTs perceived hand exercises to be within their domain of expertise and control. When highlighting the superficial approaches to hand exercises by RTs, OTs demarcate the professional competence of hand exercise therapy from that of RTs. Concurrently, RTs do not claim the task, possibly because it is too rudimentary, but see it as a way of getting things accomplished in the hospital. Such emphasis on getting things done in the workplace increases the negotiating space in both directions.
Discussion
In our study we engaged the negotiated order perspective to explore the division of tasks between doctors and therapists in hospital outpatient services. By giving prominence to the order in negotiated order, we sought to capture how hospital social structures had ramifications for health professionals in negotiating and enacting tasks. Our analysis showed that the hierarchical localization and organization of work narrowed negotiation spaces and opportunities to shift taken-for-granted tasks when RTs and OTs negotiated jurisdiction from different positions of power. Furthermore, the organization of diagnostic tasks preserved RTs’ authority and favored medical knowledge over therapeutic approach when RTs classified the diagnosis and reasoned about it. Changes in constructs of professional boundaries were realized when international treatment recommendations in rheumatology assigned OTs responsibilities to act and enable patients to cope with the disease. This shows how fuzzy workplace realities can be more prone to change through negotiation than can structures influenced by legal and public arenas where adjustments to task division take longer.4
Interprofessional Interactions in an Uneven Negotiating Order
Medical influence on the division of labor in hospitals frames interactions between health professionals83 and sustains fixed rather than fluid boundaries between the RTs and OTs in our study, where the structural ordering had more impetus on interactions than vice versa. This is in line with previous studies that refer to a “non-negotiated” rather than a negotiated order of a hospital.79,84 Reeves et al84 found that negotiations between different professionals rarely took place in hospital departments where non-medical health professionals were not comfortable engaging in medically oriented dialog, resulting in few opportunities for rich interprofessional negotiation. In our study, interprofessional interaction in the outpatient department was infrequent, which left few arenas for explicit negotiation. Contrary to a study by Allen,45 where the initiation of medical tasks by nurses created challenges in collaborating with doctors, our study identified the existence of social agreements whereby higher-status RTs initiated the workflow of lower-status OTs. This shows how negotiations are few when tacit and explicit agreements about work distribution allocate resources efficiently without the need for substantial interpretive work. Consequently, consolidated understanding prevails.
When doctors maintain their historically developed advantaged position,85 OTs abide by an identity defined in the workplace and rooted in biomedicine.86 Our analysis demonstrates a biomedical scaffolding of tasks where an interprofessional hierarchy and medical knowledge influence health realities and interaction.87 These social structures contribute to shaping the epistemic space for OTs and RTs to enact tasks by framing what is conceivable and achievable. In our study, influential RTs frame both clinical and organizational hospital circumstances, resonating with Nugus et al’s43 study of hospital clinicians’ exercise of power. They found that doctors determine patient care. Consistent with other studies, the OTs in our study have challenges in initiating negotiation from their own biopsychosocial base.88 Moreover, when the OTs describe their role as auxiliary to that of RTs rather than emphasize their own contributions to hand OA care in line with evidence-based interventions, they contribute to sustaining a taken-for-granted medical dominance. OTs who position themselves as gap fillers rather than key professionals providing relevant healthcare have previously been described,89 and impact how OTs navigate their therapist identity within the hospital. Such an understanding contributes to sustaining the biomedicalization of OT knowledge and practice in the hospital,90 under the influence of medicine.
Chronic Illness Calls for Action Beyond Medicines’ Traditional Knowledge Base
Hospitals that are structured to respond to acute illness must also increasingly relate to and incorporate practices to accommodate chronically ill patients. In our study, patients with chronic hand manifestations are referred according to certain rules whereby RTs establish a diagnosis and OTs provide relevant treatment. Consultations are pre-planned in time and space and performed according to specific standards and procedures. Unlike in-hospital acute activities, hand OA accounts for a limited number of patients with specialized problems in outpatient services provision. Unforeseen occurrences rarely take place, and open disagreements over medical or therapeutic procedures are also rare. Contrary to Terpstra et al’s12 claim that RTs have a distinct and important role in hand OA treatment, our analysis showed that the work of RTs often ended with the establishment of a hand OA diagnosis, accompanied by shifting clinical responsibilities from RTs to OTs. The chronic nature of hand OA and the lack of relevant medical interventions call for action beyond medicines’ traditional knowledge base.46 In our study, OTs with less institutional power have developed a high level of expertise in hand OA management. Consequently, OTs increase their own possibilities through less status-based interaction when they enact tasks that are non-medical yet are in line with accepted international recommendations in rheumatology. This shows how OTs increase their authority base due to the limitations of medicine in providing a cure. Weber et al91 showed how power based on situational control can trump power based on social status. In our study, the social status of RTs could not influence the outcome of a chronic condition like OA. OTs were thus invited to frame a situation where they could become responsible for patient treatment, similar to a study of rheumatology clinical nurse specialists optimizing management of hand OA in secondary care.92 Hence, OTs circumvent ambiguity about the enactment of the task to enable patients to cope with the disease, thus precluding further negotiation. As such, their position to provide relevant interventions becomes an available resource that brings agentic power in planning and strategizing how to use what is available. Moreover, chronic conditions like hand OA enable stronger opportunities to complement each other’s professional worldviews and to equip OTs with the ability to act independently of the constraining power of social structure.
Crossing Professional Boundaries to Accommodate Patient Interests
In our study, the therapeutic-medical boundary was constructed within a larger social context where a united interprofessional aim to provide quality healthcare was central to task distribution and enactment. In healthcare, the person-centered approach is regarded as essential for health professionals in delivering high-quality services where an egalitarian patient–health professional relationship is the ideal.93,94 In our study, patients were transformed into boundary objects through the shared values and joint commitment of the two professional groups in responding to individual patient interests. Such arrangements were useful for everyday organization and routines in the hospitals.39 Our analysis align with a study by Apesoa-Varano95 where boundary crossing was enacted in the name of patient care. In situations where RTs instructed patients to do hand exercises, they justified the informal boundary-crossing as being in patient interests when OTs were not available, also contradicting a result of Apesoa-Varano95 where physicians never assisted other professional groups in enacting non-medical tasks due to their status.
Patient interests were also the main concern when OTs suspected a diagnosis other than hand OA and consequently entered the diagnostic territory of RTs. RTs did not perceive this practice to threaten their professional jurisdiction. On the contrary, quality of care was emphasized, and resonates with Fullerton et al’s96 study of a health rheumatology triage initiative where rheumatologists trusted therapists to identify patients with urgent needs to see rheumatologists in a timely manner. These professional practices show how doctors in our study perform therapeutic tasks and therapists in our study perform medical tasks within reason. Such task enactments that obscure formal jurisdictional boundaries allowed practitioners across groups to get things accomplished and make things work in the hospital.4,40 The shift in focus away from the professions themselves in order to respond to patient interests illustrates how tasks can be crossed without being significantly transformed when health professionals take person-centered action without claiming jurisdiction over new tasks in the workplace. Hence, the social order in the hospital is maintained. Status and prestige are sidelined when practitioners act in what they consider to be the best interests of their patients, surpassing clearly demarcated professional boundaries. Our analysis highlights the dominance of medicine over therapeutic dimensions of healthcare where OTs are appraised against a medical standard. It also emphasizes an interprofessional person-centered focus that contributes to a move towards patient interests rather than to narrowing clinical realities in the realm of medicine to a question of whether doctors or therapists should perform the task.
Limitations
Focusing on negotiated order theory enriched our data analysis, adding depth and consistency, while also limiting our insights into other aspects of negotiating professional tasks. By employing negotiated order theory, we recognize the challenges in capturing and interpreting meaning in interactions that are socially constructed and dynamic. Within such an ever-changing social order, implicit negotiations and tacit understandings are not easily recognized in our analysis. Regardless, such interpretivist approaches to health professional negotiations over tasks enable us to gain more insights into how both interactions and structures impact RTs and OTs experiences in enacting tasks. Thus, our analysis may be relevant beyond the therapeutic–medical boundary in rheumatology when we contextualize rather than generalize through producing illustrative accounts in telling one story, not the story about negotiating professional tasks.97 Our choice of methods and HJM not being a trained ethnographic observer influenced the moving of observations from ordinary and clinical looking to the rigor of systematically seeing.71 To enhance rigor through adequate preparation and in developing a clear purpose, HJM observed clinical hand OA consultations in a hospital not included in this study prior to data generation as part of practicing ethnographic skills.
Focusing on actions in structured clinical consultations due to ethical regulations limited our access to daily health professional interactions. Observing day-to-day activities in the hospital beyond clinical consultations would have allowed for a more comprehensive understanding and made proximity to participants less influenced by time and space limitations. Each interview and consultation were unique and our choice to analyze based on commonalities across settings over local variations led to some loss of nuances.69 HJM’s presence influenced participant actions, for example emphasizing certain tasks to provide a good impression of own practice.98 The health professional background of HJM facilitated trust and an understanding of clinical management and hand OA trajectories. However, reflexive practice was important to cast light on how ideas and assumptions about patients, health professionals, and healthcare interactions informed and influenced the research process.
Conclusion
Our study generates novel knowledge of doctor–therapist relations and seeks to provide an additional layer of understanding through negotiated order theory. We have drawn attention to the negotiated order perspective to explore how health professionals negotiate outpatient tasks. Overall, our analysis shows that RTs and OTs enact tasks in succession and do not share common tasks. Higher ranking doctors initiate patient inclusion into the hospital by classifying the problem, by establishing a diagnosis and by reasoning about the subsequent in-hospital trajectory rooted in a medical knowledge system. Henceforth, when medicine does not possess available treatment options for patients, doctors initiate the work of therapists. Through providing relevant therapeutic interventions that are entrenched in international recommendations in rheumatology, therapists take lead action in service delivery to equip patients with tools to cope with chronic illness. Hence, occupational therapists’ high level of expertise becomes central in directing and enhancing services for persons with hand OA. In our attention to order and to negotiation, we highlight that negotiations do not take place from equal power positions when status hierarchies and the knowledge criteria that portray them frame professional practices. At the same time, health professionals enact tasks in ways that are highly influenced by their workplace. In the arena of the workplace, they work together in concert despite professional differences in expertise, interests, and opinions when their patients are transformed into boundary objects in the process of providing relevant healthcare. We highlight the viewpoint that professionals negotiating tasks with each other is central for getting things accomplished, which demonstrates the dynamic connection between negotiations and order in negotiated order. By delegating tasks based on competence and expertise rather than professional titles, OTs and RTs can enhance interprofessional relationships, leverage each profession’s strengths, and work together to ensure that decisions and actions are aligned with the best interests and preferences of patients, while equalizing power dynamics.
Acknowledgments
The authors would like to thank all the participants for their time and insights. The overall project is funded by the Research Council of Norway (Grant 300823/H40).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Christensen K, Doblhammer G, Rau R, Vaupel JW. Ageing populations: the challenges ahead. The Lancet. 2009;374(9696):1196–1208. doi:10.1016/S0140-6736(09)61460-4
2. OECD. Elderly population. Available from: https://www.oecd-ilibrary.org/content/data/8d805ea1-en.
3. Ministry of Health and Care Services. Time to Act. Personnel in a Sustainable Health and Care Service. [Tid for Handling. Personellet I En Bærekraftig Helse- Og Omsorgstjeneste] NOU 2023:4; 2023.
4. Abbott A. The System of Professions: An Essay on the Division of Expert Labor. University of Chicago Press; 1988.
5. Freidson E. Professionalism: The Third Logic. Polity Press; 2001.
6. Johnson T. Professions and Power. Macmillan; 1972.
7. Ackroyd S. Sociological and organisational theories of professions and professionalism. In: Dent M, Bourgeault IL, Kuhlmann E, editors. The Routledge Companion to the Professions and Professionalism. Routledge; 2016.
8. Nancarrow SA, Borthwick AM. Dynamic professional boundaries in the healthcare workforce. Sociol Health Illn. 2005;27(7):897–919. doi:10.1111/j.1467-9566.2005.00463.x
9. Nancarrow S. Emerging allied health professions. In: Nancarrow S, Borthwick A, editors. The Allied Health Professions: A Sociological Perspective.
10. Edelaar L, Nikiphorou E, Fragoulis G, et al. 2019 EULAR recommendations for the generic core competences of health professionals in rheumatology. Ann Rheum Dis. 2020;79(1):53. doi:10.1136/annrheumdis-2019-215803
11. UEMS. Training requirements for the specialty of rheumatology: European standards of postgraduate medical specialist training. European Union of Medical Specialists 2014. Available from: https://www.uems.eu/__data/assets/pdf_file/0005/44438/UEMS-2014.21-European-Training-Requirements-Rheumatology-.pdf.
12. Terpstra SES, van de Stadt LA, Kloppenburg M. The management of hand osteoarthritis: the rheumatologist’s perspective. J Hand Ther. 2022;35(3):322–331. doi:10.1016/j.jht.2022.08.001
13. Dziedzic KS, Allen KD. Challenges and controversies of complex interventions in osteoarthritis management: recognizing inappropriate and discordant care. Rheumatology. 2018;57(suppl_4):iv88–iv98. doi:10.1093/rheumatology/key062
14. Tveter A, Nossum R, Eide R, et al. Short-term effect of occupational therapy intervention on hand function and pain in patients with thumb base osteoarthritis - Secondary analyses of a randomized controlled trial. Osteoarthritis and Cartilage. 2019;27:S85. doi:10.1016/j.joca.2019.02.121
15. Peck F, Kennedy S, McKirdy L. The Introduction of Practitioner-led Hand Clinics in South Manchester. Hand Ther. 2001;6(2):41–44. doi:10.1177/175899830100600201
16. Rose R-L, Probert S. Development and implementation of a hand therapy extended scope practitioner clinic to support the 18-week waiting list initiative. Hand Ther. 2009;14(4):95–104. doi:10.1258/ht.2009.009016
17. Burri RV. Doing Distinctions: boundary Work and Symbolic Capital in Radiology. Soc Stud Sci. 2008;38(1):35–62. doi:10.1177/0306312707082021
18. Liberati EG, Gorli M, Scaratti G. Invisible walls within multidisciplinary teams: disciplinary boundaries and their effects on integrated care. Soc Sci Med. 2016;150:31–39. doi:10.1016/j.socscimed.2015.12.002
19. Lamont M, Molnár V. The Study of Boundaries in the Social Sciences. Annu Rev Sociol. 2002;28(1):167–195. doi:10.1146/annurev.soc.28.110601.141107
20. Comeau-Vallée M, Langley A. The Interplay of Inter- and Intraprofessional Boundary Work in Multidisciplinary Teams. Organ Stud. 2019;41(12):1649–1672. doi:10.1177/0170840619848020
21. Star SL, Griesemer JR. Institutional Ecology, ‘Translations’ and Boundary Objects: amateurs and Professionals in Berkeley’s Museum of Vertebrate Zoology, 1907-39. Soc Stud Sci. 1989;19(3):387–420.
22. Star SL. This is Not a Boundary Object: reflections on the Origin of a Concept. Sci Technol Human Values. 2010;35(5):601–617. doi:10.1177/0162243910377624
23. Meier N. Collaboration in Healthcare Through Boundary Work and Boundary Objects. Qual Sociol Rev. 2015;11(3):60–82. doi:10.18778/1733-8077.11.3.05
24. Health Personnel Act [Lov om helsepersonell] 1999. Available from: https://lovdata.no/dokument/NL/lov/1999-07-02-64.
25. Freidson E. Profession of Medicine: A Study of the Sociology of Applied Knowledge. Dodd, Mead & Co.; 1970.
26. Freidson E. Professional Powers: A Study of the Institutionalization of Formal Knowledge. University of Chicago Press; 1986.
27. Larsen Ø. Mangfoldig medisin: Det medisinske fakultet, Universitetet i Oslo 175 år, 1814-1989. University of Oslo; 1989.
28. Haave P. [When state authorisation was introduced for medical doctors in Norway]. Da legene skulle autoriseres. Tidsskr nor Laegeforen. 2007;127(24):3267–3271.
29. Gran JT. Revmatologi. Tidsskr nor Laegeforen. 2006;1(126):114.
30. Brown CR, Criscione-Schreiber L, O’Rourke KS, et al. What Is a Rheumatologist and How Do We Make One? Arthritis Care Res. 2016;68(8):1166–1172. doi:10.1002/acr.22817
31. Dziedzic KS, Hill JC, Porcheret M, Croft PR. New Models for Primary Care Are Needed for Osteoarthritis. Phys Ther. 2009;89(12):1371–1378. doi:10.2522/ptj.20090003
32. Raastad A. Pionerenes fortellinger: Da ergoterapifaget var nytt i Norge.Kolofon; 2013.
33. Horghagen S, Josephsson S, Alasaker S. The use of craft activities as an occupational therapy treatment modality in Norway during 1952–1960. Occup Ther Int. 2007;14(1):42–56.
34. King R, Nilsskog G, Ness N. Aktuelle Artikler Om Ergoterapiens Historie.Ergoterapiutdanningen; 1995.
35. Mengshoel AM. Experiences of shifts in physiotherapy for patients with rheumatoid arthritis over time - An autoethnography. Physiother Theory Pract. 2023;1–11.
36. Salhani D, Coulter I. The politics of interprofessional working and the struggle for professional autonomy in nursing. Soc Sci Med. 2009;68(7):1221–1228. doi:10.1016/j.socscimed.2009.01.041
37. Album D, Johannessen LEF, Rasmussen EB. Stability and change in disease prestige: a comparative analysis of three surveys spanning a quarter of a century. Soc Sci Med. 2017;180:45–51. doi:10.1016/j.socscimed.2017.03.020
38. Nugus P. Re-structuring the negotiated order of the hospital. Sociol Health Illn. 2019;41(2):378–394. doi:10.1111/1467-9566.12838
39. Strauss A. The Hospital and its Negotiated Order. In: Freidson E, editor. The Hospital in Modern Society. The Free Press; 1963:147–169.
40. Strauss AL. Psychiatric Ideologies and Institutions. Transaction Publishers; 1964.
41. Strauss AL. Negotiations: Varieties, Contexts, Processes, and Social Order. Jossey-Bass; 1978.
42. Clarke AE. Straussian negotiated order theory c. 1960-present. In: Vom Lehn D, Ruiz-Junco N, Gibson W, editors. The Routledge International Handbook of Interactionism. Routledge; 2021:47–58.
43. Nugus P, Greenfield D, Travaglia J, Westbrook J, Braithwaite J. How and where clinicians exercise power: interprofessional relations in health care. Soc Sci Med. 2010;71(5):898–909. doi:10.1016/j.socscimed.2010.05.029
44. Håland E. Introducing the electronic patient record (EPR) in a hospital setting: boundary work and shifting constructions of professional identities. Sociol Health Illn. 2012;34(5):761–775. doi:10.1111/j.1467-9566.2011.01413.x
45. Allen D. The nursing-medical boundary: a negotiated order? Sociol Health Illn. 1997;19(4):498–520. doi:10.1111/j.1467-9566.1997.tb00415.x
46. Svensson R. The interplay between doctors and nurses—a negotiated order perspective. Sociol Health Illn. 1996;18(3):379–398. doi:10.1111/1467-9566.ep10934735
47. Strauss A. Cultural evolution: an interactionist perspective. Int Sociol. 1993;8(4):493–495. doi:10.1177/026858093008004006
48. Currie G, Dingwall R, Kitchener M, Waring J. Let’s dance: organization studies, medical sociology and health policy. Soc Sci Med. 2012;74(3):273–280. doi:10.1016/j.socscimed.2011.11.002
49. Holstein JA, Gubrium JF. Handbook of Constructionist Research. Guilford Press; 2008.
50. Mik-Meyer N. The Power of Citizens and Professionals in Welfare Encounters: The Influence of Bureaucracy, Market and Psychology. Social and Political Power. Manchester University Press; 2017.
51. Feiring M. Rehabilitation—Between management and knowledge practices: an historical overview of public action in Norwegian welfare reforms. Policy Soc. 2012;31(2):119–129. doi:10.1016/j.polsoc.2012.04.003
52. Romão VC, Fonseca JE. Major Challenges in Rheumatology: will We Ever Treat Smarter, Instead of Just Harder? Front Med. 2019;6. doi:10.3389/fmed.2019.00144
53. Directorate of Health. Clarification of responsibilities and task sharing between municipalities and the specialist health care in the rehabilitation area. [Avklaring av ansvars- og oppgavedeling mellom kommunene og spesialisthelsetjenesten på rehabiliteringsområdet]. (IS-1957). Oslo: Helsedirektoratet; 2012.
54. Kloppenburg M. Hand osteoarthritis—nonpharmacological and pharmacological treatments. Nat Rev Rheumatol. 2014;10(4):242–251. doi:10.1038/nrrheum.2013.214
55. Gravås EMH, Tveter AT, Nossum R, et al. Non-pharmacological treatment gap preceding surgical consultation in thumb carpometacarpal osteoarthritis - A cross-sectional study. BMC Musculoskelet Disord. 2019;20(1):180. doi:10.1186/s12891-019-2567-3
56. Zhang W, Doherty M, Leeb BF, et al. EULAR evidence-based recommendations for the diagnosis of hand osteoarthritis: report of a task force of ESCISIT. Ann Rheum Dis. 2009;68(1):8–17. doi:10.1136/ard.2007.084772
57. Kloppenburg M, Kroon FPB, Blanco FJ, et al. 2018 update of the EULAR recommendations for the management of hand osteoarthritis. Ann Rheum Dis. 2019;78(1):16. doi:10.1136/annrheumdis-2018-213826
58. Kjeken I, Bergsmark K, Haugen IK, et al. Task shifting in the care for patients with hand osteoarthritis. Protocol for a randomized controlled non-inferiority trial. BMC Musculoskelet Disord. 2021;22(1):194. doi:10.1186/s12891-021-04019-9
59. Eisenhardt KM. Building Theories from Case Study Research. Acad Manage Rev. 1989;14(4):532–550. doi:10.2307/258557
60. Malterud K, Siersma VD, Guassora AD. Sample Size in Qualitative Interview Studies: guided by Information Power. Qual Health Res. 2016;26(13):1753–1760. doi:10.1177/1049732315617444
61. Holstein JA, Gubrium JF. The Active Interview. SAGE; 1995.
62. Holstein JA, Gubrium JF. Postmodern Interviewing. Sage Publications; 2012.
63. Atkinson P, Coffey A. Revisiting the Relationship Between Participant Observation and Interviewing. In: Holstein JA, Gubrium JF, editors. Inside Interviewing: New Lenses, New Concerns. SAGE Publications Inc; 2003:414–428.
64. Emerson RM, Fretz RI, Shaw LL. Writing Ethnographic Fieldnotes.
65. Spradley JP. Participant Observation. Holt, Rinehart and Winston; 1980.
66. Wind G. Negotiated interactive observation: doing fieldwork in hospital settings. Anthropol Med. 2008;15(2):79–89. doi:10.1080/13648470802127098
67. Goldman J, Reeves S, Wu R, Silver I, MacMillan K, Kitto S. A sociological exploration of the tensions related to interprofessional collaboration in acute-care discharge planning. J Interprof Care. 2016;30(2):217–225. doi:10.3109/13561820.2015.1072803
68. Braun V, Clarke V. One size fits all? What counts as quality practice in (reflexive) thematic analysis? Qual Res Psychol. 2021;18(3):328–352. doi:10.1080/14780887.2020.1769238
69. Braun V, Clarke V. Thematic Analysis: A Practical Guide. SAGE; 2022.
70. Braun V, Clarke V. Reflecting on reflexive thematic analysis. Qual Res Sport Exerc Health. 2019;11(4):589–597. doi:10.1080/2159676X.2019.1628806
71. Patton MQ. Qualitative Research & Evaluation Methods.
72. Tavory I. Abductive Analysis: Theorizing Qualitative Research. University of Chicago Press; 2014.
73. Braun V, Clarke V. Toward good practice in thematic analysis: avoiding common problems and be(com)ing a knowing researcher. Int J Transgend Health. 2022;1–6. doi:10.1080/26895269.2022.2129597
74. Braun V, Clarke V. Conceptual and design thinking for thematic analysis. Qual Psychol. 2022;9(1):3–26. doi:10.1037/qup0000196
75. Freidson E. The Changing Nature of Professional Control. Annu Rev Sociol. 1984;10:1–20.
76. Vanstone M, Grierson L. Thinking about social power and hierarchy in medical education. Med Educ. 2022;56(1):91–97. doi:10.1111/medu.14659
77. Price S, Doucet S, Hall LM. The historical social positioning of nursing and medicine: implications for career choice, early socialization and interprofessional collaboration. J Interprof Care. 2014;28(2):103–109. doi:10.3109/13561820.2013.867839
78. Jutel A. ‘The expertness of his healer’: diagnosis, disclosure and the power of a profession. Health. 2019;23(3):289–305. doi:10.1177/1363459317745956
79. Allen D. The Invisible Work of Nurses: Hospitals, Organisation and Healthcare. Routledge; 2015.
80. Greenhalgh T. How to Read a Paper: The Basics of Evidence-Based Medicine and Healthcare.
81. Timmermans S, Kolker ES. Evidence-based medicine and the reconfiguration of medical knowledge. J Health Soc Behav. 2004;177–193.
82. Martin G, Bushfield S, Siebert S, Howieson B. Changing Logics in Healthcare and Their Effects on the Identity Motives and Identity Work of Doctors. Organ Stud. 2020;42(9):1477–1499. doi:10.1177/0170840619895871
83. Freidson E. Professionalization and the Organization of Middle-Class Labour in Postindustrial Society. Sociol Rev. 1972;20:47–59. doi:10.1111/j.1467-954X.1972.tb03209.x
84. Reeves S, Rice K, Conn LG, Miller KL, Kenaszchuk C, Zwarenstein M. Interprofessional interaction, negotiation and non-negotiation on general internal medicine wards. J Interprof Care. 2009;23(6):633–645. doi:10.3109/13561820902886295
85. Finn R. The language of teamwork: reproducing professional divisions in the operating theatre. Hum Relat. 2008;61(1):103–130. doi:10.1177/0018726707085947
86. Aas MH, Bonsaksen T. Exploring occupation-based practice among occupational therapists in hospitals and rehabilitation institutions. Scand J Occup Ther. 2022;1–11. doi:10.1080/11038128.2022.2059564
87. Cramer H, Hughes J, Johnson R, et al. ‘Who does this patient belong to?’ boundary work and the re/making of (NSTEMI) heart attack patients. Sociol Health Illn. 2018;40(8):1404–1429. doi:10.1111/1467-9566.12778
88. Cregård A. Inter-occupational cooperation and boundary work in the hospital setting. J Health Organ Manag. 2018;32(5):658–673. doi:10.1108/jhom-10-2016-0188
89. Fortune T. Occupational Therapists: is Our Therapy Truly Occupational or are We Merely Filling Gaps? Br J Occup Ther. 2000;63(5):225–230. doi:10.1177/030802260006300507
90. Turcotte P-L, Holmes D. From domestication to imperial patronage: deconstructing the biomedicalisation of occupational therapy. Health. 2021;1(3):58. doi:10.1177/13634593211067891
91. Weber CE, Kortkamp C, Maurer I, Hummers E. Boundary Work in Response to Professionals’ Contextual Constraints: micro-strategies in Interprofessional Collaboration. Organ Stud. 2022;43(9):1453–1477. doi:10.1177/01708406221074135
92. Kwok WY, Kloppenburg M, Beaart-van de Voorde LJ, Huizinga TW, Vliet Vlieland TP. Role of rheumatology clinical nurse specialists in optimizing management of hand osteoarthritis during daily practice in secondary care: an observational study. J Multidiscip Healthc. 2011;4:403–411. doi:10.2147/jmdh.S25269
93. Mead N, Bower P. Patient-centredness: a conceptual framework and review of the empirical literature. Soc Sci Med. 2000;51(7):1087–1110. doi:10.1016/S0277-9536(00)00098-8
94. McCormack B. A conceptual framework for person-centred practice with older people. Int J Nurs Pract. 2003;9(3):202–209. doi:10.1046/j.1440-172X.2003.00423.x
95. Apesoa-Varano EC. Interprofessional Conflict and Repair: a Study of Boundary Work in the Hospital. Sociol Perspect. 2013;56(3):327–349. doi:10.1525/sop.2013.56.3.327
96. Fullerton LM, Brooks S, Sweezie R, Ahluwalia V, Bombardier C, Gagliardi AR. Patient, Rheumatologist and therapist perspectives on the implementation of an Allied Health Rheumatology Triage (AHRT) initiative in Ontario Rheumatology Clinics. Pragmat Obs Res. 2020;1–12.
97. Malterud K. Qualitative research: standards, challenges, and guidelines. Lancet. 2001;358(9280):483–488. doi:10.1016/s0140-6736(01)05627-6
98. Maxwell JA. Qualitative Research Design: An Interactive Approach.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.