Back to Journals » Drug Design, Development and Therapy » Volume 20
Nalbuphine as a Bridge to Delayed Epidural Analgesia: A Randomized Trial on First-Stage Labor Duration
Authors Xu Y, Song C ![]() , Xu Y, Luo H, Chen K, Peng S, Guo L, Yu J
, Xu Y, Luo H, Chen K, Peng S, Guo L, Yu J ![]()
Received 16 October 2025
Accepted for publication 28 January 2026
Published 7 February 2026 Volume 2026:20 574810
DOI https://doi.org/10.2147/DDDT.S574810
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Yan Zhu
Yang Xu, Congzhong Song, Yuzeng Xu, Huijun Luo, Kai Chen, Song Peng, Liying Guo, Jing Yu
Department of Anesthesiology, Affiliated Xiaoshan Hospital, Hangzhou Normal University (Zhejiang Xiaoshan Hospital), Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Jing Yu, Department of Anesthesiology, Affiliated Xiaoshan Hospital, Hangzhou Normal University (Zhejiang Xiaoshan Hospital), Hangzhou, Zhejiang, People’s Republic of China, Email [email protected]
Purpose: The present study aimed to investigate whether nalbuphine-assisted delayed epidural analgesia, as compared with early epidural analgesia, exerts an effect on the duration of the first stage of labor in nulliparous women.
Patients and Methods: A total of 120 nulliparous women were enrolled in the final statistical analysis between July 2024 and March 2025. Participants were randomly allocated to either the Early Epidural Analgesia group (normal saline control, NS group) or the Delayed Epidural Analgesia group (nalbuphine-assisted, NB group). The primary outcome measure was the duration of the first stage of labor.
Results: The Kaplan-Meier survival curve analysis demonstrated that the duration of the first stage of labor was significantly shorter in the nalbuphine group than in the normal saline group (hazard ratio [HR] = 1.629, 95% confidence interval [CI]: 1.082– 2.455, P < 0.05), indicating a statistically significant difference. No between-group statistical differences were observed in the incidence of postpartum hemorrhage, oxytocin administration rate, labor induction methods, episiotomy rate, amniotic fluid contamination, maternal fever, nausea, vomiting, or cesarean section rate.
Conclusion: For nulliparous women, nalbuphine-assisted delayed epidural analgesia can shorten the duration of the first stage of labor compared with early epidural analgesia (administered at cervical dilation ≤ 3 cm).
Keywords: nalbuphine, epidural anesthesia, labor analgesia, first stage of labor, pregnancy
Introduction
Labor pain impacts maternal labor progression and maternal-neonatal health. Neuraxial analgesia, recognized internationally as the gold standard for labor pain relief due to its efficacy and safety,1–3 still faces debate regarding the optimal timing of epidural initiation (based on cervical dilation).4 The prevailing view holds that initiating analgesia early in labor (cervical dilation ≥2.0 cm) does not increase cesarean risk.5–8 However, clinical experience indicates that some parturients exhibit prolonged labor and inadequate active phase analgesia, leading to reduced delivery room turnover and inefficient resource utilization. In a prospective non-randomized study of 89 nulliparas, Simanauskaite9 observed that early epidural analgesia (initiated at cervical dilation < 3 cm) prolonged the first labor stage by 60–80 minutes and increased oxytocin augmentation rates to 44%, in contrast to 23% in the late-initiation group (3–7 cm cervical dilation).
Nalbuphine is a synthetic opioid agonist-antagonist that exerts targeted activity at κ-opioid receptors. Kim10 proposed that nalbuphine administration—irrespective of concomitant oxytocin use—shortens both the duration of cervical dilation and the active phase of the first stage of labor, with no adverse complications observed in parturients, fetuses, or neonates. At present, intravenous nalbuphine has been validated as a safe labor analgesia regimen, with a demonstrated trend toward reducing the time required for cervical dilation.10,11
Accordingly, we conducted a randomized controlled trial to investigate whether intravenous nalbuphine administration, followed by conversion to patient-controlled epidural analgesia (PCEA) at cervical dilation ≥ 4 cm, exerted an effect on the duration of the first stage of labor in nulliparous women, as compared with early epidural analgesia.
Materials and Methods
Study Participants
This randomized controlled trial was approved by the Ethics Committee of Zhejiang Xiaoshan Hospital (Approval No. K2024008), which conforms to the provisions of the Declaration of Helsinki (as revised in Tokyo 2004), and registered with the Chinese Clinical Trial Registry (www.chictr.org.cn, Registration No. ChiCTR2400086270). Written informed consent was obtained from all participants.
One hundred and twenty nulliparous women receiving labor analgesia at Zhejiang Xiaoshan Hospital between July 2024 and March 2025 were enrolled. Inclusion criteria: ASA physical status II; age 18–40 years; height 150–170 cm; weight ≤100 kg; cervical dilation ≤3 cm. Exclusion criteria: allergy to study drugs; spinal deformity; multiple gestation; contraindications to neuraxial blockade (coagulopathy, infection at puncture site); pregnancy complications (preeclampsia); patient refusal. Participants were excluded post-enrollment for: failed epidural placement; accidental subarachnoid or intravascular catheter placement; drug allergy; conversion to cesarean delivery.
Randomization and Blinding
A simple randomization method was adopted for participant allocation in this study. Specifically, computer-generated random numbers were sealed in sequentially numbered opaque envelopes. Prior to the initiation of labor analgesia, the attending anesthesiologist opened the envelopes in the exact order of patient recruitment to confirm the group assignment for each eligible nulliparous woman. All enrolled participants were then allocated to either the experimental group or the control group at a 1:1 ratio. After the administration of analgesia, the patient-controlled epidural analgesia (PCEA) pumps used by the participants were concealed in opaque black bags to maintain the blinding procedure. Owing to inherent limitations of the experimental design—given that the anesthesiologist was responsible for formulating and adjusting the analgesic regimen—blinding of the anesthesiologist was not feasible. However, strict single-blindness was maintained throughout the entire study duration: the participants, obstetricians in charge of labor management, and midwives providing intrapartum care were all unaware of the group allocation status of the participants. This design strictly adheres to the requirements of clinical trial methodology, minimizing the potential bias caused by unblinding to the greatest extent possible.
Study Procedure
After consent, intravenous access was established, and 10 mL/kg lactated Ringer’s solution was infused. Non-invasive blood pressure (NIBP), electrocardiography (ECG), and pulse oximetry (SpO2) were monitored continuously.
Epidural catheterization was performed by experienced attending anesthesiologists using a standardized technique (L2-L3 interspace, 18G Tuohy needle, loss-of-resistance to saline). The catheter was threaded 3–4 cm cephalad. After negative aspiration for blood/cerebrospinal fluid, a 3 mL test dose of 0.8% lidocaine was administered. Absence of signs of subarachnoid block or local anesthetic toxicity after 5 minutes, coupled with confirmed loss of cold sensation using an alcohol swab, verified correct epidural placement. The PCEA pump (PIEB mode) was connected using a solution of 0.075% ropivacaine with 2 μg/mL fentanyl. Settings: PIEB bolus 10 mL (rate 10 mL/min), patient-controlled bolus 10 mL, lockout interval 15 minutes, maximum hourly dose 30 mL, automated interval 60 minutes. The pump was placed in the opaque bag.
According to randomization: NS group: Received 10 mL intravenous saline followed by immediate PCEA activation. NB group: Received intravenous nalbuphine 5 mg (diluted to 10 mL). PCEA remained off. If the participant requested additional analgesia (second request), a cervical exam was performed. If dilation remained ≤3 cm, a second nalbuphine dose was administered (≥1 hour after first dose). PCEA was activated once dilation reached ≥4 cm or 1 hour after the second nalbuphine dose. Pain assessments were performed prior to analgesic administration, at 30, 60 minutes post-administration, and further at the point of full cervical dilation (10 cm). Sensory level (loss of cold sensation bilaterally) and motor block were assessed at 30 minutes. Subsequently, motor block, FHR, contractions, and vital signs were recorded every 2 hours until delivery. For both groups (once in the ≥4 cm phase for NB group): Asymmetric sensory level (2 dermatomal difference) prompted catheter withdrawal by 1 cm. Inadequate block height (bilateral sensory level < T10) was treated with a 5 mL epidural top-up (max 15 mL over 15 min). Breakthrough pain despite adequate sensory level (>T10 bilaterally) was treated with 10 mL epidural 1% lidocaine.
Outcome Measures
Primary outcome:
Duration of the first stage of labor.
Secondary outcomes:
Rate of breakthrough pain requiring lidocaine rescue; cesarean delivery rate; maternal vital signs; oxytocin usage (dose, frequency); neonatal Apgar scores at 1 and 5 minutes; duration of second and third stages; total labor duration; incidence of maternal adverse events (nausea/vomiting, fever, urinary retention, pruritus, lower limb numbness).
Sample Size Estimation
Based on preliminary data (NB group first stage: 463.20±246.00 min), a clinically significant difference of 2 hours was assumed. Using α=0.05, β=0.1, and an estimated dropout rate of 20%, PASS 11.0 software indicated 60 participants per group. Thus, the total sample size was set at 120.
Statistical Analysis
Quantitative data are presented as mean ± standard deviation, count, min/max, or median, Q1, Q3, 95% CI. Intergroup or intragroup comparisons employed normality testing. Normally distributed data used t-tests or paired t-tests; non-normal data used non-parametric tests or log-transformation followed by t-tests. Analysis of covariance (ANCOVA), interaction analysis, or stratified analysis was used for center/other factors. Generalized estimating equations (GEE) or repeated-measures ANOVA were used for center/time effects.
Qualitative data are presented as frequencies, percentages, or proportions. Intergroup or intragroup comparisons used Chi-square or Fisher’s exact tests. CMH Chi-square test was used for categorical/ordinal outcomes with center/other factors.
All hypothesis tests were two-sided (α=0.05), except non-inferiority tests.
Results
The study included a total of 135 female participants, of whom 15 were excluded (Figure 1). One hundred and twenty participants were randomized (60 per group). Six in the NS group had cesarean delivery and two withdrew due to severe pruritus. Eight in the NB group had cesarean delivery and one withdrew due to severe pruritus. Ultimately, 103 participants (NS: n=52, NB: n=51) were analyzed (Figure 1). The demographic characteristics of the patients are presented in Table 1. Statistical analysis revealed no significant differences among the groups in terms of age, height, weight, gestational age, cervical dilation, spontaneous/artificial/premature rupture of membranes (P > 0.05) (Table 1).
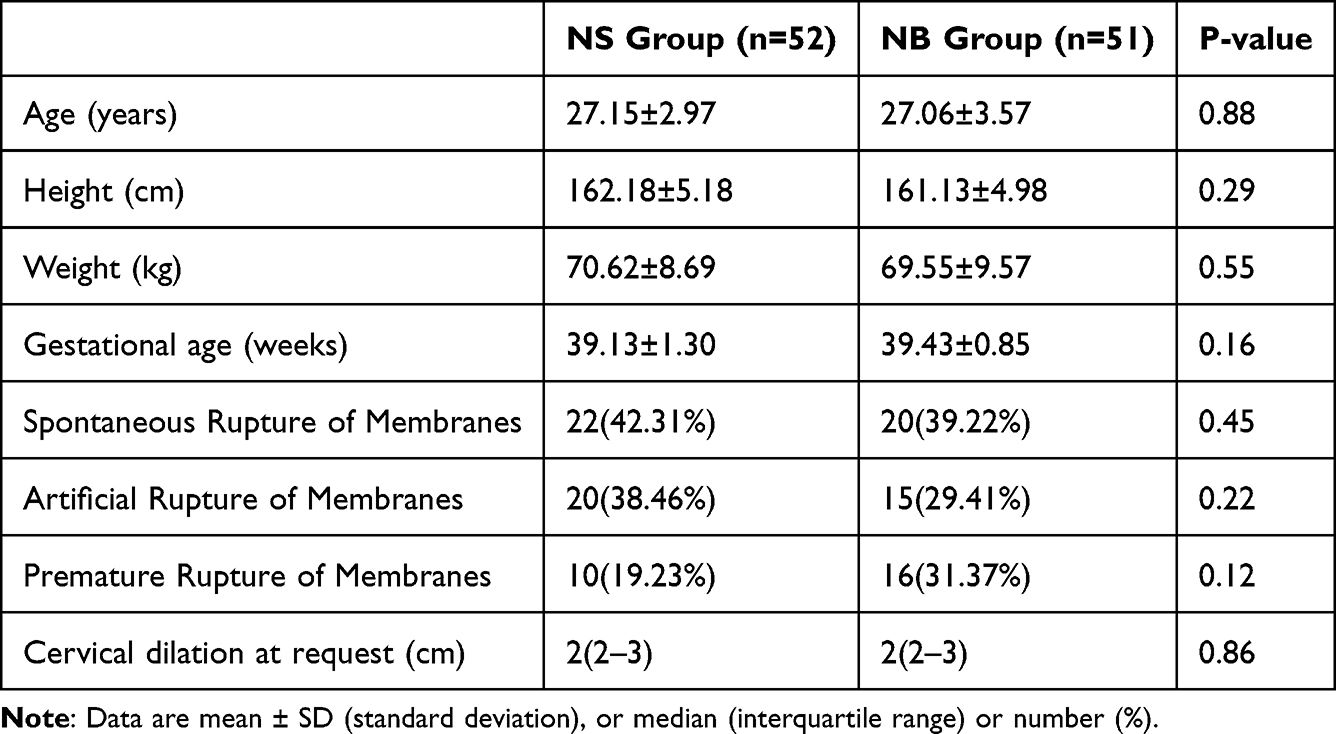 |
Table 1 Baseline Maternal Characteristics |
 |
Figure 1 Participant Flow Diagram (Image placeholder - Description: CONSORT-type flow diagram showing screening, randomization, allocation, follow-up, and analysis). |
The first stage duration was significantly longer in the NS group (636.08 ± 356.19 min vs 512.90 ± 215.21 min, P = 0.04). Total labor duration was also longer in the NS group (722.29 ± 356.97 min vs 598.96 ± 234.21 min, P = 0.04). No differences were found in second or third stage durations (Table 2). Box plot analysis showed the median first stage duration was shorter in the NB group (460 min, 95% CI 403.11–516.89 min, IQR 333 min) compared to the NS group (585 min, 95% CI 467.22–702.78 min, IQR 524 min). The NB group also showed less variability. (Figure 2). Kaplan-Meier survival analysis confirmed a significantly shorter first stage in the NB group (HR 1.629, 95% CI 1.082–2.455, P = 0.02) (Figure 3).
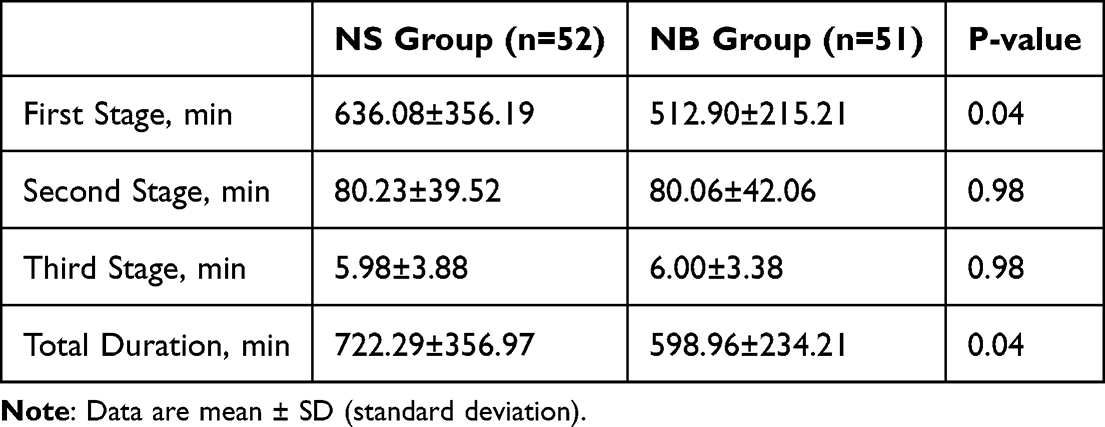 |
Table 2 Primary Labor Duration Outcomes |
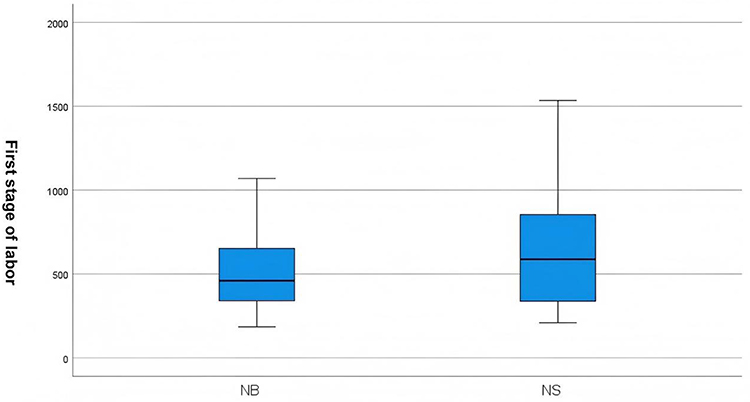 |
Figure 2 Box Plot of First Stage Duration (min) by Group (Image placeholder - Description: Box plot showing distribution, median, IQR, and outlier for NS and NB groups). |
 |
Figure 3 Kaplan-Meier Curve for Time to End of First Stage by Group (Image placeholder - Description: Survival curve showing proportion remaining in first stage over time, stratified by NS and NB groups). |
As shown in Table 3, patients in the nalbuphine group exhibited higher pain scores than those in the control group upon transitioning to epidural anesthesia. This discrepancy may stem from the fact that cervical dilation in the nalbuphine group had already reached 5 cm—rather than the preset 4 cm—at the time of patient-controlled epidural analgesia (PCEA) initiation. Fortunately, the pain scores recorded in the nalbuphine group remained within a clinically acceptable range.
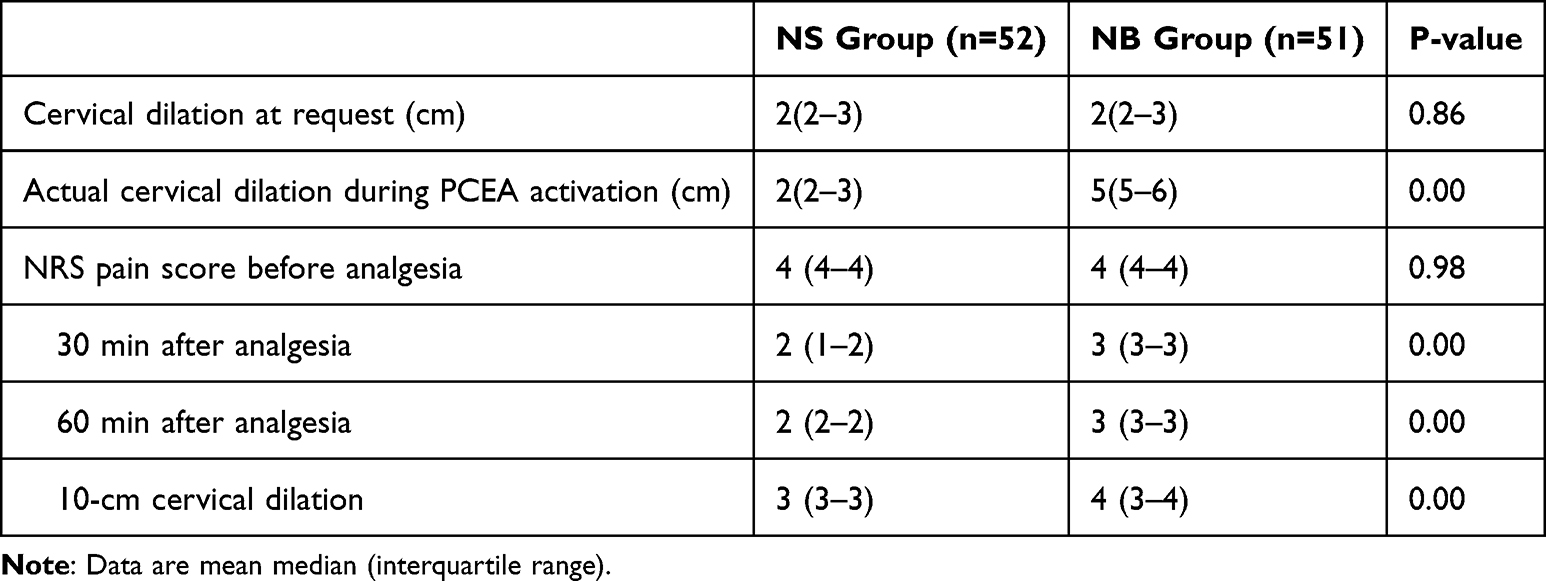 |
Table 3 Management of Analgesia |
No significant differences were observed in oxytocin usage (frequency or total dose), induction methods, episiotomy rate, meconium incidence, maternal fever, or neonatal birth weight (P > 0.05). One neonate in each group required NICU admission. The NS group neonate (Apgar 10/10) was transferred for low oxygenation index unresponsive to oxygen. The NB group neonate (Apgar 8/1 min → 9/5 min) was transferred for fetal distress. NICU transfer rates did not differ significantly (P > 0.05), though the lower Apgar in the NB group neonate warrants further investigation with larger samples regarding nalbuphine’s neonatal effects. Rates of nausea/vomiting and epidural rescue were similar. Pruritus was significantly more frequent in the NS group (15.4% vs 3.9%, P = 0.049), while dizziness was significantly more frequent in the NB group (1.9% vs 19.6%, P = 0.004). The cesarean rate was comparable (NS: 10.0% [6/60 randomized], NB: 13.3% [8/60 randomized], P = 0.570) (Table 4).
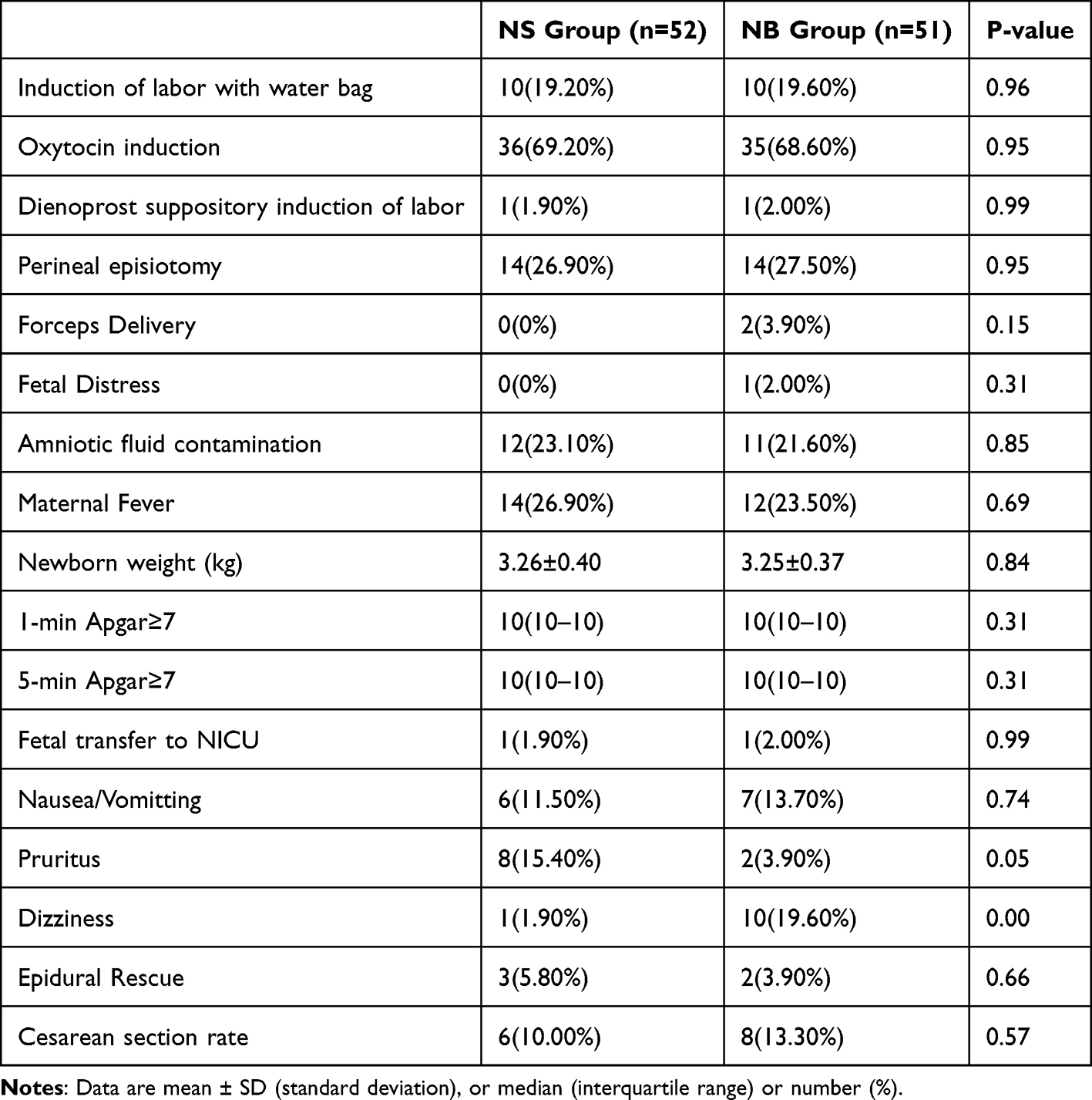 |
Table 4 Secondary Outcomes and Adverse Events |
Discussion
This prospective randomized controlled trial investigated the impact of early epidural analgesia on the first stage duration in nulliparas. The results indicate that initiating epidural analgesia early in labor (cervical dilation ≤3 cm) does not increase the cesarean delivery rate. However, compared to immediate epidural analgesia, utilizing intravenous nalbuphine during the latent phase (cervical dilation ≤3 cm) combined with delayed epidural initiation significantly shortened the first stage duration (HR 1.629, P < 0.05) without increasing maternal or neonatal complications. This finding offers a novel approach for nulliparas experiencing early labor dystocia but requiring analgesia.
For nulliparas, the timing of epidural initiation (based on cervical dilation) is considered a factor in the association between epidural analgesia and labor dystocia.5 Thorp suggested early epidural analgesia prolongs the first and second stages and significantly increases cesarean rates.12 Lieberman reported this risk could more than double.13 Zha found epidural initiation before 6 cm dilation was associated with longer labor compared to initiation after 6 cm. However, controversy exists.14 In a prospective RCT, Wong concluded that pain relief initiated early (≥2.0 cm dilation) does not increase cesarean risk.6 A large 5-year study from Nanjing Maternity Hospital suggested epidural analgesia initiated during the latent phase (≥1.0 cm) compared to delayed analgesia (≥4.0 cm) neither prolongs labor nor increases cesarean rates in nulliparas.8 American College of Obstetricians and Gynecologists (ACOG) guidelines state:1 “When feasible, maternal request is a sufficient medical indication for pain relief during labor”. Our findings align with the current consensus that early epidural analgesia (≤3 cm) does not increase cesarean risk. Crucially, we demonstrate that intravenous nalbuphine during the latent phase (≤3 cm) followed by delayed epidural initiation significantly shortens the first stage (HR 1.629, P < 0.05) without compromising safety. While individual parturients might accept a brief delay for pain relief, from an operational perspective (delivery room turnover, cost-effectiveness), initiating intravenous nalbuphine for eligible nulliparas followed by conversion to PCEA at ≥4 cm dilation appears advantageous. It addresses early pain needs, avoids prolonging labor, improves delivery room efficiency, and offers a new paradigm for comfortable labor analgesia.
Nalbuphine, a mixed opioid agonist-antagonist (κ-agonist, μ-partial antagonist), mitigates μ-agonist side effects like pruritus, shivering, and nausea/vomiting15,16. It is established as safe for intravenous labor analgesia.10 Based on this evidence, we employed intravenous nalbuphine for analgesia in parturients at ≤3 cm dilation. Notably, one case of fetal distress with lower Apgar scores occurred in the NB group. Unfortunately, this study did not collect umbilical artery blood gasses, neonatal behavioral neurological assessment (NBNA) scores, or neonatal neurobehavioral scale (NNNS) data. Therefore, potential effects of nalbuphine cannot be definitively excluded, warranting inclusion of more comprehensive neonatal assessment in future studies.
This study has limitations. While neuraxial analgesia has strong evidence and widespread use, clinical data on intravenous nalbuphine for labor analgesia remain relatively limited. Although existing evidence supports its safety, international guidelines lack consensus on optimal dosing. Our systematic review found 10 mg IV is common in Western studies. However, our preliminary single-center trial indicated a higher rate of dizziness and nausea/vomiting with 10 mg in an Asian population.17 Considering potential ethnic differences, we validated a 5 mg dose adjustment, achieving satisfactory analgesia with reduced adverse effects. Therefore, we used 5 mg IV nalbuphine. However, the overall sample size was modest. Determining the optimal dose that maintains efficacy without affecting labor progression requires further investigation.
This study excluded pregnant women with a BMI > 35 kg/m2, a trade-off between sample homogeneity and research feasibility in clinical research. On one hand, Severely obese pregnant women are prone to more comorbidities (eg, gestational diabetes, hypertensive and thrombotic disorders) and pregnancy complications, which introduce confounding variables that interfere with the assessment of core interventions or observational outcomes. On the other hand, from the perspective of research implementation, severely obese pregnant women pose greater challenges in terms of antenatal management, diagnostic procedures, and follow-up. Their higher risk of adverse pregnancy outcomes may also increase the study’s dropout rate and data missing rate, driving up the overall cost and difficulty of the research. However, this exclusion limits the study’s generalizability to obese obstetric populations.
The transition point was set at ≥4 cm; however, cervical exams were performed only upon maternal request (pain score >3), potentially leading to transition beyond 4 cm in practice. Finally, the lack of a pure intravenous analgesia control group makes it difficult to isolate the effect of epidural delay itself. Future multi-center studies with long-term maternal-neonatal outcome follow-up are needed.
Conclusion
Compared to delayed epidural analgesia following intravenous nalbuphine, initiating epidural labor analgesia early in labor (cervical dilation ≤3 cm) may prolong the first stage of labor in nulliparous women but does not increase the cesarean delivery rate. Utilizing intravenous nalbuphine during the latent phase followed by epidural analgesia at cervical dilation ≥4 cm offers an advantage in accelerating the first stage. This benefit extends beyond the biological metric of shortened labor, while accelerating delivery room turnover, providing an operationally feasible and potentially cost-effective clinical pathway. It suggests a new research direction for providing analgesia to parturients unable to receive neuraxial analgesia during the latent phase or experiencing uterine inertia, contributing to the development of a more precise labor analgesia system.
Data Sharing Statement
The datasets generated and analyzed during the current study are included in this published article. Due to the constraints of the ethical approval and the informed consent agreements with the participants, additional individual de-identified participant data will not be shared. Further raw data that support the findings of this study will be made available by the corresponding author, Jing Yu, upon reasonable request, starting from the date of publication and for a period of six months thereafter. Requests for data access can be directed to [email protected].
Ethics and Registration
Our clinical trial was approved by the Ethical Committee of Affiliated Xiaoshan Hospital, Hangzhou Normal University (Hangzhou, China) (Approval Number: K2024008), which conforms to the provisions of the Declaration of Helsinki (as revised in Tokyo 2004). This study was registered at the Chinese Clinical Trials Registry (ChiCTR), Protocol ID Number ChiCTR2400086270. Written informed consent was obtained from all participants involved.
Acknowledgments
The authors are grateful to the staff of the maternity and anesthesia departments at Affiliated Xiaoshan Hospital, Hangzhou Normal University, for their valuable contributions to this work, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Zhejiang Provincial Medical and Health Science and Technology Project (2024KY1442).
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Obstetrics. ACOG practice bulletin No. 209: obstetric analgesia and anesthesia. Obstet Gynecol. 2019;133(3):e208–9. doi:10.1097/AOG.0000000000003132.
2. Chajut E, Caspi A, Chen R, et al. In pain thou shalt bring forth children: the peak-and-end rule in recall of labor pain. Psychol Sci. 2014;25(12):2266–2271. doi:10.1177/0956797614551004
3. Anim-Somuah M, Smyth RM, Cyna AM, et al. Epidural versus non-epidural or no analgesia for pain management in labour. Cochrane Database Syst Rev. 2018;5(5):CD000331. doi:10.1002/14651858.CD000331.pub4
4. Sng BL, Leong WL, Zeng Y, et al. Early versus late initiation of epidural analgesia for labour. Cochrane Database Syst Rev. 2014;2014(10):CD007238. doi:10.1002/14651858.CD007238.pub2
5. Chen S, Ye S, Wu C, et al. Effects of epidural analgesia at 1 cm cervical dilatation on labor interventions in full-term primigravida: a retrospective cohort study. J Obstet Gynaecol Res. 2023;49(6):1545–1550. doi:10.1111/jog.15640
6. Wong CA, Scavone BM, Peaceman AM, et al. The risk of cesarean delivery with neuraxial analgesia given early versus late in labor. N Engl J Med. 2005;352(7):655–665. doi:10.1056/NEJMoa042573
7. Ohel G, Gonen R, Vaida S, et al. Early versus late initiation of epidural analgesia in labor: does it increase the risk of cesarean section? A randomized trial. Am J Obstet Gynecol. 2006;194(3):600–605. doi:10.1016/j.ajog.2005.10.821
8. Wang F, Shen X, Guo X, et al; Labor Analgesia Examining Group. Epidural analgesia in the latent phase of labor and the risk of cesarean delivery: a five-year randomized controlled trial. Anesthesiology. 2009;111(4):871–880. doi:10.1097/ALN.0b013e3181b55e65.
9. Simanauskaite A, Kavaliauskaite G, Kacerauskiene J. The impact of early epidural analgesia on the course of labor and delivery. Medicina. 2025;61(4):750. doi:10.3390/medicina61040750
10. Kim TH, Kim JM, Lee HH, et al. Effect of nalbuphine hydrochloride on the active phase during first stage of labour: a pilot study. J Obstet Gynaecol. 2011;31(8):724–727. doi:10.3109/01443615.2011.602139
11. Schoppmann S, Spiess D, Müller D, et al. Nalbuphine: a candidate for treatment of women overwhelmed with sudden, intense labor pain? J Matern Fetal Neonatal Med. 2022;35(25):6112–6114. doi:10.1080/14767058.2021.1906859
12. Thorp JA, Hu DH, Albin RM, et al. The effect of intrapartum epidural analgesia on nulliparous labor: a randomized, controlled, prospective trial. Am J Obstet Gynecol. 1993;169(4):851–858. doi:10.1016/0002-9378(93)90015-b
13. Lieberman E, Lang JM, Cohen A, et al. Association of epidural analgesia with cesarean delivery in nulliparas. Obstet Gynecol. 1996;88(6):993–1000. doi:10.1016/s0029-7844(96)00359-6
14. Zha Y, Gong X, Yang C, et al. Epidural analgesia during labor and its optimal initiation time-points: a real-world study on 400 Chinese nulliparas. Medicine. 2021;100(9):e24923. doi:10.1097/MD.0000000000024923
15. Jannuzzi RG. Nalbuphine for treatment of opioid-induced pruritus: a systematic review of literature. Clin J Pain. 2016;32(1):87–93. doi:10.1097/AJP.0000000000000211
16. Sun J, Zheng Z, Li YL, et al. Nalbuphine versus dexmedetomidine for treatment of combined spinal-epidural post-anesthetic shivering in pregnant women undergoing cesarean section. J Int Med Res. 2019;47(9):4442–4453. doi:10.1177/0300060519865063
17. Chestnut DH, McGrath JM, Vincent RD, et al. Does early administration of epidural analgesia affect obstetric outcome in nulliparous women who are in spontaneous labor? Anesthesiology. 1994;80(6):1201–1208. doi:10.1097/00000542-199406000-00006
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Effects of Different Puncture Points on Labor Analgesia Onset: Study Protocol for a Randomized Controlled Trial
Zhou R, Peng Y, Chen X, Xiong C, Zhai W, Zhang X, Xia L, Zhou Y
Journal of Pain Research 2023, 16:3289-3296
Published Date: 27 September 2023
Analyzing the Efficacy and Potential Risks of Nitrous Oxide for Pain Management During Labor: A Narrative Review
Kichili N, Brown MK, Armer DS, Mashaw SA, Gennuso SA, Ahmadzadeh S, Shekoohi S, Kaye AD
Clinical Pharmacology: Advances and Applications 2026, 18:577932
Published Date: 18 February 2026