Back to Journals » Clinical Pharmacology: Advances and Applications » Volume 18
Analyzing the Efficacy and Potential Risks of Nitrous Oxide for Pain Management During Labor: A Narrative Review
Authors Kichili N, Brown MK ![]() , Armer DS
, Armer DS ![]() , Mashaw SA, Gennuso SA, Ahmadzadeh S, Shekoohi S
, Mashaw SA, Gennuso SA, Ahmadzadeh S, Shekoohi S ![]() , Kaye AD
, Kaye AD
Received 1 November 2025
Accepted for publication 9 February 2026
Published 18 February 2026 Volume 2026:18 577932
DOI https://doi.org/10.2147/CPAA.S577932
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Khaled Deeb
Nikhita Kichili,1 Morgan K Brown,2 Devon S Armer,2 Sydney A Mashaw,2 Sonja A Gennuso,3 Shahab Ahmadzadeh,3 Sahar Shekoohi,3 Alan D Kaye3
1The University of Texas Medical Branch, Galveston, TX, USA; 2School of Medicine, Louisiana State University Heath Sciences Center, Shreveport, LA, USA; 3Department of Anesthesiology, Louisiana State University Health Sciences Center, Shreveport, LA, USA
Correspondence: Sahar Shekoohi, Email [email protected]
Abstract: Nitrous oxide has been used worldwide for labor analgesia for over a century. It offers a non-invasive, rapidly acting, and self-administered option for pain and anxiety management. The present investigation examines efficacy, safety, and limitations of nitrous oxide when compared to other labor analgesic modalities, including epidural anesthesia, intravenous opioids, and non-pharmacologic methods. Pharmacologically, nitrous oxide has both analgesic and anxiolytic effects via NMDA receptor inhibition, opioid receptor activation, and GABA-A modulation. While it can be less effective than epidurals in producing complete analgesia, studies demonstrate moderate pain relief, high maternal satisfaction, and preserved mobility. Safety considerations include common, mild adverse effects such as nausea, dizziness, and vomiting, with rare risks of hypoxia, especially when combined with other sedatives or in vitamin B12-deficient patients. Fetal exposure occurs via placental transfer, but it is rapidly cleared, with no consistent evidence of significant neonatal harm. In this regard, data on long-term neurodevelopmental outcomes is limited. Comparative studies suggest that nitrous oxide’s efficacy is like certain opioids but inferior to epidural analgesia, and it offers both patient autonomy and ease of administration. Barriers that prevent broader adoption of nitrous include limited availability in rural settings, equipment costs, and the need for proper scavenging systems. Future research should focus on optimizing delivery systems, exploring long-term neonatal safety, and defining nitrous oxides’s role in multimodal pain management. In summary, nitrous oxide represents a safe, flexible, and patient-centered analgesic option for labor, particularly for individuals who are looking for mobility, self-control, and a less invasive alternative to neuraxial anesthesia.
Keywords: nitrous oxide, labor analgesia, maternal satisfaction, multimodal pain managent, pregnancy
Introduction
Effective pain management during labor is a critical component of care, as the primary goals include reduced maternal distress, optimal labor experience, and good obstetric outcomes. Currently, there are various options available for managing labor pain. These include neuraxial methods like epidural analgesia and combined spinal-epidural analgesia, which are often seen as the most effective. Other options include systemic pharmacologic choices, such as intravenous (IV) opioids, as well as non-pharmacologic interventions such as breathing techniques, virtual reality, warm massages, and hydrotherapy.1 Although epidurals are the most effective method for providing pain relief during labor, they are invasive, restrict ambulation, and necessitate continuous monitoring. Conversely, IV opioids offer some pain relief but come with the potential for maternal sedation and respiratory depression in newborns.2
Nitrous oxide is an inhaled anesthetic and analgesic gas that has been used since the late 19th century in obstetrics, and self-administration devices initially were developed as early as the 1930s.1 It has been widely used for labor analgesia in many countries, such as the United Kingdom, Australia, and New Zealand, but its usage remains low in the United States.3 Nitrous oxide is used as both an anesthetic and analgesic in a 50% nitrous oxide /50% oxygen mixture, which is self-administered through a mask during expected contractions. It works by affecting N-methyl-D-aspartate (NMDA) receptors and endogenous opioid pathways to modulate pain perception, leading to quick onset and offset, anxiety relief, and mild labor pain relief.1
The interest in nitrous oxide for labor pain relief in the USA has been growing, as patients and healthcare workers are looking for alternative options that offer a balance for pain relief, mobility, and patient autonomy, while also minimizing risks for both mother and fetus.3,4 With this increased clinical interest in nitrous oxide, there is a need to assess its effectiveness, safety, and potential risks compared to other commonly used pain management methods.
This review will discuss the clinical applications of nitrous oxide for labor pain relief, the barriers to its widespread usage, its role in multimodal pain management, and future research directions and expanding implementation.
Pharmacokinetics of Nitrous Oxide
Mechanism of Action, Interaction with NDMA Receptor, and Opioid System
Nitrous oxide, commonly known as “laughing gas”, has both anesthetic and analgesic qualities. To reduce sensitivity to pain, nitrous oxide non-competitively inhibits the NMDA receptor. The NMDA receptor normally binds glutamate, the main excitatory neurotransmitter in the body.5 Nitrous oxide alters pain perception in the body by inhibiting excitatory neurotransmitter signals from being released. Additionally, nitrous oxide interacts with opioid receptors, leading to release of endogenous opioids and initiating downstream signaling cascades that cause analgesia and euphoria.6
Absorption, Distribution, Metabolism, and Excretion
Nitrous oxide is administered via inhalation, rapidly absorbed through the lung alveoli into the bloodstream. The onset of nitrous oxide effects occur within 2–5 minutes and is widely distributed throughout the body.2,7 Anaerobic bacteria in the gastrointestinal tract play a limited role in minimally metabolizing nitrous oxide before a majority is eliminated unchanged by lung exhalation.6
Implications for Sedation
Nitrous oxide alone is not potent enough for use in anesthetic procedures. The strength of inhaled pharmacological agents can be determined by the minimum alveolar concentration (MAC), which shows the relationship between dosage and response to nitrous stimuli.8 Nitrous oxide requires 104% concentration to reach one MAC value, where 50% of individuals would not respond to noxious stimuli. Therefore, additional agents are needed when using nitrous oxide for anesthesia to ensure adequate anesthesia for patients.9 When combined with other anesthetics, Nitrous oxide reduces the dose requirements of more potent medications. Nitrous oxide is beneficial for a number of reasons, including having minimal impact on hemodynamics as well as protecting airway and respiratory parameters in patients.10–12
Implications for Analgesia
While nitrous oxide is typically used in combination with other agents for general anesthesia, it can also be given on its own to provide pain relief. A 25% concentration of nitrous oxide is effective in alleviating pain symptoms.13 Nitrous oxide is a widely accepted form of pain management because it is relatively easy to administer, no fasting is required prior to administration, and it has a quick onset. These advantages make it suitable for diverse patient populations, including pediatric patients, and for urgent clinical scenarios.14
Maternal – Respiratory and Cardiovascular Effects
Nitrous oxide is an acceptable analgesic option to administer to patients in labor, as it allows for patient-controlled dosing, preservation of motor function, and faster onset compared to epidural anesthesia.15 However, more precautions need to be taken to ensure the safety of expecting mothers. Respiratory depression may occur, particularly when combined with other central nervous system depressants such as sedatives, opioids, and hypnotics.6 The diffusion hypoxia phenomenon possesses another potential risk on maternal lung physiology.When nitrous oxide is stopped, there is rapid diffusion of nitrous oxide back into the alveoli, displacing oxygen and potentially leading to hypoxemia.16 The risk of cardiovascular complications is elevated when myocardial ischemia is linked to the inhibition of methionine synthase by nitrous oxide.17 This inhibition leads to a significant rise in homocysteine levels, resulting in hyperhomocysteinemia, which in turn causes an increase in platelet aggregation, coagulation, and dysfunction of epithelial cells in a dose-dependent manner.18
Maternal – Implications for Labor with Comorbidities
Pregnant patients with comorbid conditions such as chronic hypertension or preeclampsia may have and increased susceptibility to experience adverse effects associated with nitrous oxide use. In these populations, elevated homocysteine levels could exacerbate negative cardiovascular effects.15 Caution is also warranted in patients with vitamin B12 or folate deficiencies, as nitrous oxide irreversibly oxidizes vitamin B12, an essential cofactor in the folate cycle. This disruption may impair purine synthesis and, with prolonged use or repeated exposure, contribute to DNA damage.19
Efficacy of Nitrous Oxide for Labor Analgesia
Mechanism of Pain Relief
Nitrous oxide produces analgesia through interactions with multiple neural pathways. It binds to opioid receptors and causes a release of endogenous opioids, specifically dynorphins, in the brain and also activates postsynaptic opioid receptors.20 Both effects reduce pain sensitivity and exhibit analgesic properties. Nitrous oxide also binds to the A-subunit of γ-aminobutyric acid type A (GABA-A) receptors, producing anxiolysis and mild sedative effects.6 This mechanism parallels that of benzodiazepines, which also bind to GABA-A receptors, resulting in similar sedative and hypnotic effects.
Clinical Effectiveness in Labor Pain Management – Patient Reported Pain Relief
Nitrous oxide is increasingly becoming a more popular alternative analgesic used in labor management and is considered safe in all three stages of labor and the postpartum period.21 Patient satisfaction, often linked to perceived pain relief, is a key measure of its clinical value. Several studies have been conducted to assess the pain levels of patients during childbirth. One study conducted at Babol University of Medical Sciences compared the use of nitrous oxide with an alternative medication for pain relief during labor.22 Out of the 49 patients who received nitrous oxide, 49% reported a positive experience.22 However, systematic reviews point out the lack of high-quality evidence in this area. Of the 58 studies on the effects of nitrous oxide on labor pain, only a few are considered to provide valuable data.1 Overall, the literature suggests that nitrous oxide may offer some relief from pain during labor, but further research is needed to confirm these findings.
Clinical Effectiveness in Labor Pain Management – Efficacy
Comparing nitrous oxide to other analgesic medications used in labor is another factor in determining its effectiveness. The clinical effectiveness of a drug depends on various factors such as concentration, adjunct medications, and delivery method.23 A Swedish postpartum study compared pain relief using nitrous oxide alone, epidural alone, and epidural with other modalities. 33% of patients who used nitrous oxide alone reported satisfactory pain relief.24 Other studies have shown that nitrous oxide is comparable to or slightly more effective than opioids for pain relief, but less effective than epidural.1 In a randomized trial comparing nitrous oxide to meperidine, there was no significant difference in pain scores P value of 0.89.25
Clinical Effectiveness in Labor Pain Management – Influence of Concentration and Duration
The concentration of nitrous oxide has been set since 2011 to a 50:50 ratio with oxygen using the Nitronox delivery system, which was the first nitrous oxide delivery system approved by the US FDA.23 It has been determined that patients can tolerate concentrations between 30–50% of N2O in the mixture.26 Standardizing the concentration has been a beneficial advancement to ensure safety. The peak nitrous oxide concentration in the body is within 60 seconds and should be administered prior to the start of contractions to ensure greatest pain relief.27 Researchers have faced challenges in determining the effectiveness of nitrous oxide due to the use of different concentrations and varying durations in studies.1,23 Additionally, there is a lack focus on the effects of the duration of nitrous oxide use, as most studies primarily test its efficacy.
Maternal Satisfaction and Preferences
Nitrous oxide is a beneficial alternative to patients in labor who prefer to self-administer medication and thus providing a greater sense of control to their pain.28,29 Patients who prefer the self-administration aspect of nitrous oxide favored not being confined to their bed, retaining feeling in their lower limbs, and having control over their medication.23 Researchers have explained satisfaction is hard to determine because it is multidimensional and complex.30 Notably, maternal preference for nitrous oxide is not solely due to analgesic effects.29 Personal expectations, involvement in decisions, quality of care received, and perceived control are some factors patients value when determining their satisfaction.31 Due to subjective patient preferences and tolerances, maternal satistisfaction cannot be objectively measured.
Limitations in Analgesic Efficacy
Although some patients prefer nitrous oxide over other pain relief methods, it often provides less pain relief compared to alternative modalities. Multiple studies comparing the use of nitrous oxide to intravenous medications for pain relief have shown that a significant percentage (40%) of women who used nitrous oxide during labor ended up switching to neuraxial analgesia.29 Additionally, a study found that majority of patients (80.9%) who opted for nitrous oxide during labor expressed a preference for a more comprehensive pain control method in future labors using a different medication.22 One of the main limitations in assessing the effectiveness of nitrous oxide is the variability in patient-reported outcomes, which are often subjective and use terms like “liked” or “loved”, making it difficult to objectively evaluate efficacy.29
Maternal and Fetal Safety Considerations/Risks
Short-Term Maternal Side Effects
As nitrous oxide gains popularity as a labor analgesic, it is crucial to evaluate the potential risks associated with its use. Nausea and vomiting are common occurrences during labor, but they are more prevalent among patients who use nitrous oxide.32 The frequency of vomiting varied based on the duration of nitrous oxide use, with 44% of women who continuously used nitrous oxide experiencing vomiting compared to 25% of women who used it intermittently.33
Nitrous oxide has the potential to induce hypoxia. In pregnant women, normal oxygen saturation is around 98% with values < 94% considered desaturation.34 Women often hyperventilate during contractions to enhance the effects of nitrous oxide, but this can be risky as it may result in excess carbon dioxide loss, increasing the risk of hypoventilation and hypoxia between contractions, particularly with a 50% nitrous oxide mixture compared to room air.4,35 Abrupt discontinuation or irregular breathing can also lead to diffusion hypoxia, as nitrous oxide rapidly displaces oxygen and carbon dioxide in the blood, causing oxygen desaturation.4,35 However, analyzing oxygen desaturation can be complex as it also occurs during unmedicated labor, and previous studies combing opioids with nitrous oxide have yielded mixed results.3
Long-Term Maternal Risks
Prolonged or high-concentrated exposure to nitrous oxide has the potential to cause neurological injury via demyelination.3 As a result, people may experience paresthesia, psychiatric symptoms, peripheral neuropathy, irritability, and mild memory impairment.36 Nitrous oxide is more likely to cause damage to those who are vitamin B12 deficient and who abuse the drug in large amounts.36
Nitrous oxide is self-administered through a mask, and specific precautions must be followed to ensure the safety of both patients and healthcare workers. The delivery system for nitrous oxide should include a demand valve and should be switched off when not in use by the patient. Additionally, the system should be equipped with scavenging equipment attached that utilizes negative pressure to capture exhaled nitrous oxide.3 These safety measures help protect healthcare workers from exposure to contaminated air, prevent patient overdoses, and reduce the risk of hypoxia.
Fetal Effects
Nitrous oxide crosses through the placenta, reaching 80% of the maternal concentration in nearly 15 minutes.4,37 Nitrous oxide does not pose a threat to the neonatal respiratory system due to the short half-life of less than 3 minutes.38 A study conducted during 2016–2017 assessed the fetal respiratory effects of nitrous oxide use during labor. Out of 463 participants, 31 neonates were admitted into ICU and 10 received an Apgar score < 7 after 5 minutes of birth.39 However, the researchers concluded that additional studies are necessary to assess the long-term effects of nitrous oxide on neonatal outcomes.39
Comparison to Other Drugs
Epidural anesthesia, opioids, and non-pharmacologic techniques are other analgesic modalities commonly used in labor. Epidural anesthesia is widely used due to its superior pain relief, anxiolytic effects, and low prevalence of hyperventilation. Additionally, newborns experience improved circulation due to vasodilation, enhanced oxygenation, and reduced metabolic acidosis.40 However, epidural anesthesia has slower analgesic onset, higher incidence of motor block and catheter failure, is less cost-efficient and can lead to assymetric nerve blockade, maternal hypotension and fetal bradycardia.40 Opioids provide quality pain control and maternal satisfaction, but are associated with higher rates of nausea, sedation, itching, and vomiting.41 Patients who prefer non-pharmacological options opt for relaxation or manual techniques for pain relief. Yoga, music therapy, and hypnosis are popular methods. Manual techniques include massages and cold or hot compresses.21 Non-pharmacologic options avoid drug-related risks but offer limited analgesia, functioning primarily as distraction or coping strategies.40
Comparison to Other Labor Analgesia Modalities
IV Opioids
Intravenous (IV) opioids, such as meperidine and remifentanil, are systemic analgesics used commonly for labor pain management. Opioids act on any of three main opioid receptors throughout the central nervous system: mu (μ), kappa (κ), and delta (δ). Systemic delivery of opioids enables them to act simultaneously across all receptor sites in the central nervous system, providing analgesia regardless of the specific receptor subtype engaged.21
A 2023 randomized controlled trial comparing nitrous oxide to IV meperidine found no significant difference in pain relief 20–30 minutes after administration. Measurements were recorded according to a visual analog scale (VAS) from 0 to 10 cm with 10 indicating greatest possible pain. Nitrous oxide was rated to have a VAS of 7.7 ± 2.3 cm vs meperidine which rated 7.6 ± 2.7 cm; P = 0.89, with similar maternal short-term pain relief.25 Nevertheless, both methods did not provide the same level of pain relief as epidural anesthesia. The study also reported no significant differences in adverse effects for both mother and child between the two analgesic methods.
However, a 2005 crossover trial comparing N2O to remifentanil found that remifentanil provided significantly greater pain relief (median pain score reduction of 1.5 vs 0.5 for N2O, P = 0.01), with most participants preferring remifentanil (14 out of 15 participants, P<0.001).42 Study findings also showed a higher incidence of sedation with remifentanil use and a lower maternal oxygen saturation, however these levels remained within safe ranges and no episodes of hypoxemia were reported.42
The use of opioids during labor is associated with nausea, vomiting, pruritus, sedation, and respiratory depression.21 Moreover, opioids can pass through the placenta and may cause decreased fetal heart rate, respiratory depression in newborns, lower Apgar scores, neurobehavioral changes, and difficulties with early breastfeeding.21 In contrast, nitrous oxide is quickly eliminated from both maternal and neonatal circulations, reducing the risk of prolonged exposure and making it a safe option for use during labor.
Epidural Analgesia
Epidural analgesia remains the gold standard for the management of pain during labor, consistently providing the most effective form of pain control during all stages of labor. Administration of an epidural involves the injection of an opioid analgesic and a local anesthetic into the lumbar epidural space of the patient. This cocktail of locally acting analgesic agents primarily affects the spinal nerve roots, blocking their function.43 Although epidurals yield higher rates of maternal satisfaction than other methods, they come with several significant drawbacks. Notably, epidurals are known to decrease mobility and have potential negative side effects such as hypotension, urinary retention, and intrapartum fever, especially when high doses of local anaesthetic agent is used.21
Nitrous oxide offers advantages over epidurals in having patient autonomy, ease of administration, and the benefits of rapid onset and offset for analgesic effects. As an inhaled agent, it is less invasive compared to an epidural and requires less patient monitoring. For patients with medical contraindications to neuraxial techniques or those seeking greater autonomy, nitrous oxide is a reasonable alternative.21
Non-Pharmacological Methods
The use of non-pharmacologic methods of pain management such as massage, hydrotherapy, warm compresses, and breathing is widespread but quantifiable research data on the efficacy of such methods is limited and variable. Despite this, some professional medical societies, including the American College of Obstetrics and Gynecology, the European Board and College of Obstetrics and Gynecology, and the World Health Organization, acknowledge these methods as an adjunct to pharmacologic management due to the high levels of patient satisfaction and minimal adverse events associated with their use.21
Related to the limited number of studies quantifying the efficacy of nitrous oxide and the highly subjective nature of many non-pharmacologic analgesic methods, an objective comparison between the two is difficult. While nitrous oxide may offer greater analgesic efficacy, non-pharmacologic approaches often result in higher patient satisfaction rates, particularly among patients that may value greater autonomy, minimally invasive intervention, or a personal reluctance to use more traditional medical interventions. These methods are likely best used in accompaniment with pharmacologic pain management.21 See Table 1.
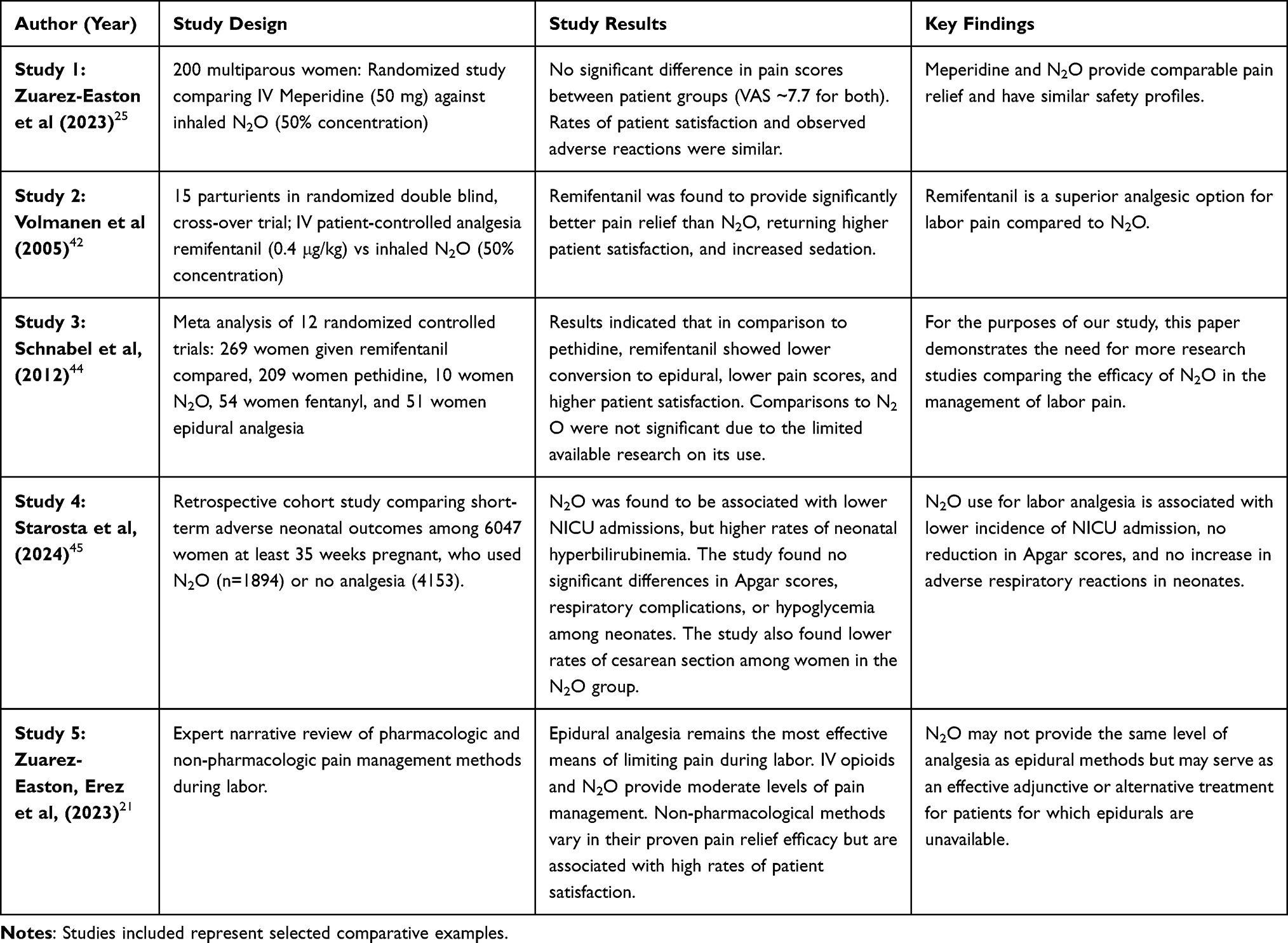 |
Table 1 Comparison of N2O to Other Labor Analgesia Modalities |
Discussion
Clinical Implications of Nitrous Oxide Use in Labor
Nitrous oxide has resurfaced as a potentially viable option for labor analgesia in recent years. It has been widely adopted in other countries since the 1880s as a labor analgesic, but use is infrequent in the United States.46 However, as women in the United States seek alternatives to invasive forms of pain control, its use has grown.47 Nitrous oxide offers a unique collection of benefits as an analgesic and anxiolytic, but it also comes with limitations to its use as a labor pain management option.20
Nitrous oxide is situated between non-pharmacologic approaches and more intensive pharmacologic options like IV opioids or epidural analgesia. Pain relief with nitrous oxide is minimal compared to the complete pain relief provided with epidural analgesia, but its ability to be self-administered via a mask provides patient autonomy and flexibility, as well as increased mobility that is typically limited by epidurals.23 Most of the benefit of nitrous oxide comes from its ability to decrease anxiety and help laboring individuals cope with contractions, particularly in early labor and in individuals who desire a less invasive approach.48 Nitrous oxide allows patients to further control their experience without lingering sedative effects.
Nitrous oxide has the additional benefit of its role in multimodal pain management, as it can be integrated with other non-pharmacologic or pharmacologic interventions to enhance patient comfort.49 For example, it may be used at the start of labor to bridge the gap while awaiting epidural placement, or it may also be used as a fallback analgesic in patients who have contraindications to epidural analgesia. Nitrous oxides’s ability to be combined with other modalities makes it an especially flexible tool in patient-centered care.
Challenges in Widespread Implementation
Despite the advantageous use of nitrous oxide in labor, widespread implementation faces challenges. Its availability is limited throughout healthcare settings; most major academic centers or large birthing centers can offer nitrous oxide as an option for birthing mothers, but rural hospitals, where approximately 18% of births occur, typically do not have the facilities to offer this as a treatment.3 The expenses associated with equipment and staff training, along with the necessary infrastructural modifications like adequate ventilation, may discourage institutions from implementing the practice to ensure the safety of personnel, mothers, and fetuses.4
Additionally, while nitrous oxide is known to be safe for use in dental settings, there is limited data on its long-term effects on newborns compared to epidural analgesia, which has a well established safety record for both mother and child.50 Nitrous oxide is quickly eliminated from the body, suggesting minimal risk to the fetus, but further research is necessary to examine any potential side effects, particularly on neurodevelopment.15
Future Directions in Labor Analgesia
In the future, there in potential for further research and improvement in various aspects of nitrous oxide as a method of labor analgesia. Currently, the delivery method of nitrous oxide relies on demand valves that require the laboring individual to both hold the mask on their face and synchronize their inhalations with contractions.51 This setup may inadvertently increase anxiety levels. Enhancements in mask design and real-time monitoring of inhalation and contractions could enhance patient comfort. Additionally, exploring more efficient and cost-effective scavenging systems could facilitate wider implemention in rural settings, reducing the risk of staff risk to overexposure and expanding access to this form of pain relief.52
Ongoing research is crucial to determine the safety and efficacy of Nitrou oxide as a multimodal treatment during labor. Studies examining nitrous oxide in conjunction with epidural analgesia as a standalone treatment are needed to establish its safety compared to standard of care. Understanding the impact of nitrous oxide on maternal and fetal outcomes, both neurologically and psychologically, could expedite its incorporation into care models.23 As patient preferences trend towards less pharmacological and more physiological births, nitrous oxide has the potential to play a more prominent role in individualized, patient-centered birth experiences through evidence-based integration into care models.
Other Medications
Additional methods of pharmacologic labor analgesia are sometimes used for patients who are unable or unwilling to use opioids. These therapies may include acetaminophen or non-steroidal anti-inflammatory drugs (NSAIDs). Intravenous acetaminophen is an effective and low-cost method for relieving post-operative pain at a comparable degree to opioids, with lower maternal side-effect profiles and no specialized monitoring requirements.21 NSAIDs inhibit prostaglandin production thereby reducing the body’s inflammatory response and relieving pain. However, while NSAIDs can relieve pain, they are generally avoided in labor due to limited analgesic benefit compared to opioids, as well as the risk for premature closure of the ductus arteriosus.21
Conclusion
Nitrous oxide shows potential as a cost-effective and lower risk alternative to traditional analgesia. Given the intensity of the pain associated with childbirth and the potential risks to both mother and child associated with its management, the efficacy and safety of available analgesic methods are critical considerations. Nitrous oxide is well established as a viable method of pain management in a variety of medical applications, including labor. While it may not provide complete pain relief like epidural analgesia, nitrous oxide has been found to demonstrate moderate effectiveness in reducing labor pain while allowing for increased mobility and autonomy during childbirth. It’s favorable safety profile and rapid onset and offset of action make it a suitable option for situations requiring immediate pain relief. The most commonly observed adverse effects of nitrous oxide use were mild, such as dizziness, nausea, and vomiting. However, more research is needed to fully establish nitrous oxides’s role in labor analgesia, including long-term maternal and neonatal outcomes, rare side effects, and strategies to enhance its efficacy. Exploring its use as part of a multimodal pain management plan may also help optimize patient comfort and satisfaction.
Compliance with Ethical Guidelines
This article is based on previous studies and contains no new studies with human participants or animals performed by any authors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding or sponsorship was received for this study or publication of this article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Likis FE, Andrews JC, Collins MR. et al. Nitrous oxide for the management of labor pain: a systematic review. Anesth Analg. 2014;118(1):153–10. doi:10.1213/ANE.0b013e3182a7f73c
2. Becker DE, Rosenberg M. Nitrous oxide and the inhalation anesthetics. Anesth Prog. 2008;55(4):2–124. doi:10.2344/0003-3006-55.4.124
3. Rooks JP. Safety and risks of nitrous oxide labor analgesia: a review. J Midwifery Womens Health. 2011;56(6):557–565. doi:10.1111/j.1542-2011.2011.00122.x
4. Rosen MA. Nitrous oxide for relief of labor pain: a systematic review. Am J Obstet Gynecol. 2002;186(5):S110–126. doi:10.1016/S0002-9378(02)70186-5
5. Jewett BE, Physiology TB. NMDA Receptor. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025. Available from: http://www.ncbi.nlm.nih.gov/books/NBK519495/.
6. Knuf K, Maani CV. Nitrous oxide. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025. Available from: http://www.ncbi.nlm.nih.gov/books/NBK532922/.
7. Khinda V, Rao D, Sodhi SP, Brar GS, Marwah N. Physiological effects, psychomotor analysis, cognition, and recovery pattern in children undergoing primary molar extractions under nitrous oxide sedation using two different induction techniques: a split-mouth randomized controlled clinical trial. Int J Clin Pediatr Dent. 2021;14(Suppl 2):S131–7. doi:10.5005/jp-journals-10005-2090
8. Lobo SA, Ojeda J, Dua A, Singh K, Lopez J. Minimum alveolar concentration. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025. Available from: http://www.ncbi.nlm.nih.gov/books/NBK532974/.
9. Zafirova Z, Sheehan C, Hosseinian L. Update on nitrous oxide and its use in anesthesia practice. Best Pract Res Clin Anaesthesiol. 2018;32(2):113–123. doi:10.1016/j.bpa.2018.06.003
10. Huang C, Johnson N. Nitrous oxide, from the operating room to the emergency department. Curr Emerg Hosp Med Rep. 2016;4(1):11–18. doi:10.1007/s40138-016-0092-3
11. Clark MS, Brunick AL. Handbook of Nitrous Oxide and Oxygen Sedation. St. Louis, Mo: Mosby; 1999:208.
12. Poonai N, Creene C, Dobrowlanski A, et al. Inhaled nitrous oxide for painful procedures in children and youth: a systematic review and meta-analysis. CJEM. 2023;25(6):508–528. doi:10.1007/s43678-023-00507-0
13. Gernez E, Lee GR, Niguet JP, Zerimech F, Bennis A, Grzych G. Nitrous oxide abuse: clinical outcomes, pharmacology, pharmacokinetics, toxicity and impact on metabolism. Toxics.;11(12):962. doi: 10.3390/toxics11120962.
14. Balice-Bourgois C, Anselmi L, Schild B, Zumstein-Shaha M, Mendoza-Sagaon M. Administration of nitrous oxide by medical assistants for painful procedures in outpatient pediatric settings. Child Basel Switz.;11(9):1091.
15. Vallejo MC, Zakowski MI. Pro-con debate: nitrous oxide for labor analgesia. BioMed Res Int. 2019;2019:4618798. doi:10.1155/2019/4618798
16. Buhre W, Disma N, Hendrickx J, et al. European society of anaesthesiology task force on nitrous oxide: a narrative review of its role in clinical practice. Br J Anaesth. 2019;122(5):587–604. doi:10.1016/j.bja.2019.01.023
17. Wrońska-Nofer T, Nofer JR, Jajte J, et al. Oxidative DNA damage and oxidative stress in subjects occupationally exposed to nitrous oxide (N(2)O). Mutat Res.;731(1–2):58–63. doi:10.1016/j.mrfmmm.2011.10.010
18. Badner NH, Drader K, Freeman D, Spence JD. The use of intraoperative nitrous oxide leads to postoperative increases in plasma homocysteine. Anesth Analg. 1998;87(3):711–713. doi:10.1213/00000539-199809000-00041
19. Misselbeck K, Marchetti L, Field MS, Scotti M, Priami C, Stover PJ. A hybrid stochastic model of folate-mediated one-carbon metabolism: effect of the common C677T MTHFR variant on de novo thymidylate biosynthesis. Sci Rep.;7(1):797. doi: 10.1038/s41598-017-00854-w.
20. Emmanouil DE, Quock RM. Advances in understanding the actions of nitrous oxide. Anesth Prog. 2007;54(1):9–18. doi:10.2344/0003-3006(2007)54[9:AIUTAO]2.0.CO;2
21. Zuarez-Easton S, Erez O, Zafran N, Carmeli J, Garmi G, Salim R. Pharmacologic and nonpharmacologic options for pain relief during labor: an expert review. Am J Obstet Gynecol. 2023;228(5):S1246–59. doi:10.1016/j.ajog.2023.03.003
22. Pasha H, Basirat Z, Hajahmadi M, Bakhtiari A, Faramarzi M, Salmalian H. Maternal expectations and experiences of labor analgesia with nitrous oxide. Iran Red Crescent Med J. 2012;14(12):792–797. doi:10.5812/ircmj.3470
23. Broughton K, Clark AG, Ray AP. Nitrous oxide for labor analgesia: what we know to date. Ochsner J. 2020;20(4):419–421. doi:10.31486/toj.19.0102
24. Ranta P, Jouppila P, Spalding M, Kangas-Saarela T, Hollmén A, Jouppila R. Parturients’ assessment of water blocks, pethidine, nitrous oxide, paracervical and epidural blocks in labour. Int J Obstet Anesth. 1994;3(4):193–198. doi:10.1016/0959-289X(94)90067-1
25. Zuarez-Easton S, Zafran N, Garmi G, Dagilayske D, Inbar S, Salim R. Meperidine compared with nitrous oxide for intrapartum pain relief in multiparous patients: a randomized controlled trial. Obstet Gynecol. 2023;141(1):4–10. doi:10.1097/AOG.0000000000005011
26. Stefani SJ, Hughes SC, Schnider SM, et al. Neonatal neurobehavioral effects of inhalation analgesia for vaginal delivery. Anesthesiology. 1982;56(5):351–355. doi:10.1097/00000542-198205000-00004
27. Maze M, Fujinaga M. Recent advances in understanding the actions and toxicity of nitrous oxide. Anaesthesia. 2000;55(4):311–314. doi:10.1046/j.1365-2044.2000.01463.x
28. Frost EA. A history of nitrous oxide. In: Eger E III, editor. Nitrous Oxide/N2O. New York, NY: Elsevier Inc; 1985:1–22.
29. Richardson MG, Raymond BL, Baysinger CL, Kook BT, Chestnut DH. A qualitative analysis of parturients’ experiences using nitrous oxide for labor analgesia: it is not just about pain relief. Birth. 2019;46(1):97–104. doi:10.1111/birt.12374
30. Berkowitz B. The patient experience and patient satisfaction: measurement of a complex dynamic. Online J Issues Nurs.;21(1):1. doi: 10.3912/OJIN.Vol21No01Man01.
31. Hodnett ED. Pain and women’s satisfaction with the experience of childbirth: a systematic review. Am J Obstet Gynecol. 2002;186(5):S160–172. doi:10.1016/S0002-9378(02)70189-0
32. Collado V, Nicolas E, Faulks D, Hennequin M. A review of the safety of 50% nitrous oxide/oxygen in conscious sedation. Expert Opin Drug Saf. 2007;6(5):559–571. doi:10.1517/14740338.6.5.559
33. Arthurs GJ, Rosen M. Self-administered intermittent nitrous oxide analgesia for labour. Enhancement of effect with continuous nasal inhalation of 50 per cent nitrous oxide (Entonox). Anaesthesia. 1979;34(4):301–309. doi:10.1111/j.1365-2044.1979.tb04926.x
34. Volmanen P, Akural EI, Raudaskoski T, Alahuhta S. Remifentanil in obstetric analgesia: a dose-finding study. Anesth Analg. 2002;94(4):913–917. (). doi:10.1097/00000539-200204000-00026
35. Carstoniu J, Levytam S, Norman P, Daley D, Katz J, Sandler AN. Nitrous oxide in early labor. Safety and analgesic efficacy assessed by a double-blind, placebo-controlled study. Anesthesiology. 1994;80(1):30–35. doi:10.1097/00000542-199401000-00008
36. Reynolds E. Vitamin B12, folic acid, and the nervous system. Lancet Neurol. 2006;5(11):949–960. doi:10.1016/S1474-4422(06)70598-1
37. Littleford J. Effects on the fetus and newborn of maternal analgesia and anesthesia: a review. Can J Anaesth J Can Anesth. 2004;51(6):586–609. doi:10.1007/BF03018403
38. Briggs GG, Freeman RK, Yaffe SJ. Drugs in Pregnancy and Lactation: A Reference Guide to Fetal and Neonatal Risk.
39. Nodine PM, Collins MR, Wood CL, et al. Nitrous oxide use during labor: satisfaction, adverse effects, and predictors of conversion to neuraxial analgesia. J Midwifery Womens Health. 2020;65(3):335–341. doi:10.1111/jmwh.13124
40. Coviello A, Iacovazzo C, Frigo MG, et al. Technical aspects of neuraxial analgesia during labor and maternity care: an updated overview. J Anesth Analg Crit Care.;5(1):6. doi:10.1186/s44158-025-00224-3
41. Grangier L, Martinez de Tejada B, Savoldelli GL, Irion O, Haller G. Adverse side effects and route of administration of opioids in combined spinal-epidural analgesia for labour: a meta-analysis of randomised trials. Int J Obstet Anesth. 2020;41:83–103. doi:10.1016/j.ijoa.2019.09.004
42. Volmanen P, Akural E, Raudaskoski T, Ohtonen P, Alahuhta S. Comparison of remifentanil and nitrous oxide in labour analgesia. Acta Anaesthesiol Scand. 2005;49(4):453–458. doi:10.1111/j.1399-6576.2005.00639.x
43. He FY, Wang S. Epidural analgesia for labor: effects on length of labor and maternal and neonatal outcomes. Eur Rev Med Pharmacol Sci. 2023;27(1):5.
44. Schnabel A, Hahn N, Broscheit J, et al. Remifentanil for labour analgesia: a meta-analysis of randomised controlled trials. Eur J Anaesthesiol. 2012;29(4):177–185. doi:10.1097/EJA.0b013e32834fc260
45. Starosta A, Lundsberg L, Culhane J, Partridge C, Grechukhina O, Son M. Association between intrapartum nitrous oxide for labor analgesia and short-term neonatal outcomes. Obstet Gynecol. 2024;143(5):677. doi:10.1097/AOG.0000000000005554
46. Collins MR, Starr SA, Bishop JT, Baysinger CL. Nitrous oxide for labor analgesia: expanding analgesic options for women in the United States. Rev Obstet Gynecol. 2012;5(3–4):e126–31.
47. Lim G, Facco FL, Nathan N, Waters JH, Wong CA, Eltzschig HK. A review of the impact of obstetric anesthesia on maternal and neonatal outcomes. Anesthesiology. 2018;129(1):192–215. doi:10.1097/ALN.0000000000002182
48. Collins M. Nitrous oxide utility in labor and birth: a multipurpose modality. J Perinat Neonatal Nurs. 2017;31(2):137. doi:10.1097/JPN.0000000000000248
49. Armstrong SL, Hayes LS, Berger AA. Management of labor pain: non-pharmacological and pharmacological interventions for pain control during childbirth. Curr Obstet Gynecol Rep.;13(3):222–235. doi: 10.1007/s13669-024-00397-8.
50. Hellams A, Sprague T, Saldanha C, Archambault M. Nitrous oxide for labor analgesia. JAAPA. 2018;31(1):41. doi:10.1097/01.JAA.0000527700.00698.8c
51. Kronberg JE, Thompson DEA. Is nitrous oxide an effective analgesic for labor? A qualitative systematic review. In: Evidence-Based Obstetric Anesthesia. John Wiley & Sons, Ltd; 2005. doi:10.1002/9780470988343.ch5.
52. Stewart LS, Collins M. Nitrous oxide as labor analgesia: clinical implications for nurses. Nurs Womens Health.;16(5):398–409. doi: 10.1111/j.1751-486X.2012.01763.x.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Nalbuphine as a Bridge to Delayed Epidural Analgesia: A Randomized Trial on First-Stage Labor Duration
Xu Y, Song C, Xu Y, Luo H, Chen K, Peng S, Guo L, Yu J
Drug Design, Development and Therapy 2026, 20:574810
Published Date: 7 February 2026