Back to Journals » Journal of Pain Research » Volume 16
The Effects of Different Puncture Points on Labor Analgesia Onset: Study Protocol for a Randomized Controlled Trial
Authors Zhou R ![]() , Peng Y
, Peng Y ![]() , Chen X
, Chen X ![]() , Xiong C, Zhai W, Zhang X
, Xiong C, Zhai W, Zhang X ![]() , Xia L, Zhou Y
, Xia L, Zhou Y
Received 7 June 2023
Accepted for publication 20 September 2023
Published 27 September 2023 Volume 2023:16 Pages 3289—3296
DOI https://doi.org/10.2147/JPR.S424540
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Jinlei Li
Rui Zhou,* Yanhua Peng,* Xuemeng Chen,* Chao Xiong, Wenhu Zhai, Xianjie Zhang, Leqiang Xia, Yukai Zhou
Department of Anesthesiology, Deyang People’s Hospital, Deyang City, Sichuan Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yukai Zhou, Department of Anesthesiology, Deyang People’s Hospital, NO. 173, Section 1 of Taishan North Road, Deyang City, Sichuan Province, People’s Republic of China, Tel +8618781054070, Email [email protected]
Purpose: Parturients suffer severe pain during the stages of labor, especially the first and second. Epidural anesthesia is an effective method to alleviate labor pain. L2-3, L3-4 and L4-5 spaces have been reported to be the recommendable puncture points owing to the adequate analgesia effect and high safety. However, the speed of pain alleviation via the three points has hardly been determined, which is of great importance to parturients. Thus, the aim of this study is to compare the onset time of parturients’ painless uterine contraction after epidural labor analgesia through different puncture points.
Study Design and Methods: It is a prospective, randomized, controlled, and subject- and assessor-blinded study. Totally, 150 subjects scheduled for vaginal delivery are going to be randomly assigned into the L2-3 and L3-4 group. Puncture point in L2-3 group is lumbar 2– 3 space, while in L3-4 group it is lumbar 3– 4 space. Analgesia initiation and maintenance are the same between the two groups. Primary outcome will be percentage of painless uterine contraction 15 min after epidural labor analgesia initiation. Secondary outcomes will be the sensory blocking level, motor blocking score, adverse effects of parturients, drug liquid consumption in unit interval, apgar score and degree of satisfaction of the parturients.
Discussion: This study estimates the onset time of parturients’ painless uterine contraction after epidural labor analgesia through L2-3 or L3-4 space. The results may provide a better choice to relieve labor pain as soon as possible.
Keywords: labor analgesia, epidural anesthesia, puncture points, rapid analgesia
Introduction
Pain throughout the labor stages torments parturients. Generally, analgesia methods to relieve labor pain include non-drug analgesia (such as mental comfort, percutaneous electrical stimulation, underwater labor, etc.), drug analgesia (N2O, demerol, diazepam, etc.), acupuncture analgesia and neuraxial anesthesia. However, lumbar epidural anesthesia is the most effective method with few severe adverse events,1 which is recommended by WHO.
According to human anatomical characteristics, intermittent epidural rapid infusion has a higher injection pressure, resulting in more uniform and broader drug distribution than continuous infusion.2 Castro et al3 confirmed that injected 0.5 mL, 1 mL, and 2 mL of contrast agent into the L4 nerve roots, 24%, 27%, and 33% of the subjects, respectively, achieved diffusion to adjacent nerve roots, and the range of nerve block increased with volume. Therefore, injection speed and capacity are the prerequisites for obtaining the ideal blocking range. Another factor to determine the level of sensory retardation is puncture point. L2-3, L3-4 and L4-5 spaces have been reported to be the recommendable puncture points according to the adequate analgesia effect and high safety.4,5 Nevertheless, there are few studies that focus on the onset time of painless uterine contraction after epidural analgesia through different puncture spaces. Does a higher puncture point lead to a faster relief of labor pain? It matters to parturients.
Dermatome T10 blocking is recognized as one of the standards for successful epidural labor analgesia.6,7 Considering L2-3 space is more closer to head, which facilitates solution to reach a higher level. Thus, we hypothesized that under fix volume and injection mode, a higher puncture point may help to reach a more rapid onset of sufficient analgesia.
Accordingly, we designed this prospective, randomized, controlled, and subject- and assessor- blinded study to compare the speed of parturients to reach painless uterine contraction status after epidural analgesia through a higher or lower puncture space. The primary outcome will be the percentage of painless uterine contraction 15 min after epidural labor analgesia initiation. The secondary outcomes will be the sensory blocking level, motor blocking score, adverse effects of parturients, drug liquid consumption in unit interval, apgar score and degree of satisfaction of the parturients.
Study Design
This is a prospective, randomized, controlled, and subject- and assessor-blinded study to investigate the relationship between onset speed of adequate labor analgesia and puncture space. The subjects will be recruited in Deyang People’s Hospital, Deyang city, Sichuan province, China. Table 1 shows the trial schedule in accordance with the SPIRIT statement. Figure 1 shows the patient flow chart. All researchers will be trained to participate in the study in a standard and uniform protocol.
 |
Table 1 Schedule of This Study |
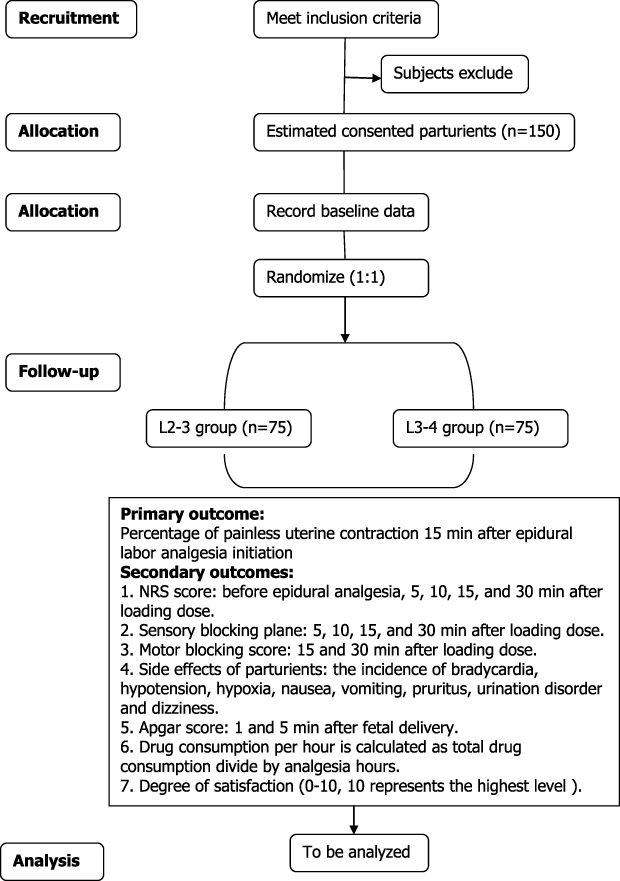 |
Figure 1 Flowchart of this study. Abbreviation: NRS, numerical rating scale. |
Registration and Ethics
This trial has been registered at Chinese Clinical Trial Registry, and the register number is ChiCTR2300070548. The study protocol (version 3.0) has been approved by the Ethics Committee of Deyang People’s Hospital, Deyang city, Sichuan province, China (2023–04-026-H01). This trial will be conducted in accordance with the Declaration of Helsinki.
Epidural analgesia executors will explain this study to the eligible parturients and show them the informed consent document. After signing related documents, parturients will be enrolled into the procedure, and they can withdraw at any moment.
Inclusion and Exclusion Criteria
The enrollment criteria include (1) parturients who are 22–40 years old, 150–170 cm height, 50–80 kg weight, with singleton, with gestational age ≥36 weeks, and assessed to deliver through vagina, (2) parturients whose American Society of Anesthesiologists (ASA) classification is II, (3) the cervical dilation is less than 5 cm, and (4) parturients who understand the research process and can cooperate to complete the trial.
The exclusion criteria are as follows: (1) The coagulation function is abnormal or platelet is less than 70 × 107/L, (2) The puncture area is infected, (3) Parturients are with a history of scoliosis, lumbar surgery, neurological dysfunction of the lower extremities, or poorly controlled psychosomatic disorders, (4) Sedatives are used before labor analgesia, (5) The interval time of uterine contraction is more than 5 min, (6) Numerical rating scale (NRS) score is less than 8 before labor analgesia.
Dropout Criteria
If patients meet one of the following situation, the follow-ups will be stopped: (1) failing to insert catheter in the intended point, (2) conversion to cesarean delivery, (3) the interval between two consecutive uterine contractions is more than 5 min after epidural analgesia, (4) labor analgesia failure, (5) severe complications, anesthetic accidents or anaphylaxis, and (6) withdrawal of the participants. Labor analgesic failure is considered as the NRS score is still more than 3 points and the blocking plane is lower than T10 15 min after an additional impact volume, or there is an asymmetric block.4 Sensory blocking level to cold is assessed bilaterally at the mid-clavicular line from caudal to cephalad, and the upper sensory blocking level is defined as where parturients first perceived cold sensation. Belly button level represents T10 plane.
Allocation and Blinding
Excel (Microsoft, USA) will be used to generate randomized sequence. According to the sequence, parturients who meet the inclusion and exclusion criteria will be allocated in a 1:1 ratio into the L2-3 group or L3-4 group. The allocation information is going to be concealed in opaque and sealed envelopes. Evaluation will be conducted once there is a request for labor analgesia. After qualification, one researcher will open an envelope, choose puncture points based on the information and go out of the room after puncture finished. Another researcher who is responsible for follow-ups will keep outdoors until the parturients turn back to a supine position. They will also take charge of dealing with underlying insufficient analgesia and side effects. The researchers who carry out puncture will be forbidden to participate in the consequent process. Thus, patients and observers will be blinded to grouping.
Intervention and Pain Management
Before puncture, an ultrasound machine will be used to identify the puncture points. According to grouping, one researcher will puncture through lumbar 2–3 space of parturients in L2-3 group, while lumbar 3–4 space in L3-4 group. A plastic conduit will be inserted 3 cm into the epidural space with the bevel of needle oriented cephalad. Then, verification of the conduit will be tested by withdrawing the plunger of the syringe and negative pressure test. After turning to supine position, the operator goes out and the other researcher gets in the room. Three milliliters of 2% lidocaine will be injected into epidural space. After a 5 min observation, a loading dose of 7 mL standard drug solution containing 0.1% ropivacaine and 0.5 ug/mL sufentanil will be administered by an electronic pump (Ren-206, Renxian Medical Technology Co., LTD, Jiangsu Province, China). Analgesia maintenance will be applied by a programmed intermittent bolus mode. The bolus is set as 9 mL and interval time is 40 min.8,9 For patient- controlled analgesia (PCA), the impact dose is set as 8 mL and the locking time is 15 min.
Fifteen minutes after the loading dose (7mL), if the NRS score is more than 3 points, an impact dose (8 mL) will be administered. Thirty minutes after the loading dose, if the NRS score is still more than 3 points, or there is an asymmetric block, it will be defined as an analgesia failure, and the parturient will be dropped out of this study. For these cases, we will take measures according to the specific circumstances, such as epidural top-ups, increasing the concentration of ropivacaine or sufentanil, adjusting the placement of epidural catheter, and re-siting catheter with the agreement of parturients.10 For successfully blocked parturients who undergo breakthrough pain (pain that parturients cannot bear), they can press the PCA button to initiate impact dose (8 mL). Then, the next programmed bolus will be triggered after 40 min. To avoid unilateral blocking, parturients are required to stay supine position when the impact dose or programmed dose is initiated.
The labor analgesia will withdraw when delivery is finished. If the myodynamia is inhibited too much to deliver, analgesia pump will be locked. After delivery is completed, the pump can be unlocked to inhibit pain from suturing of episiotomy or tear.
Outcomes
The objective of this trial is to determine which puncture point can lead to a faster relief (defined as NRS ≤ 3 points) of maternal pain.
Baseline Data and Expected Parameters
Demographic data including age, height, body weight, gestational week, blood pressure, heart rate and SPO2 will be recorded before epidural labor analgesia.
The data recorded during analgesia are as follows: NRS score, sensory blocking plane, motor blocking score (bromage scale: 0 represents no motor blocking, 1 represents unable to lift thigh, 2 represents unable to lift knee, 3 represents unable to lift ankle), bradycardia, hypotension, hypoxia, nausea, vomiting, pruritus, urination disorder, dizziness, apgar score, and drug consumption per hour.
Primary Outcomes
The primary outcome is the percentage of painless uterine contraction 15 min after epidural labor analgesia initiation. Painless uterine contraction is defined as an NRS score which is less than 4 points and no demands of additional analgesia when the uterine shrinks.
Secondary Outcomes
The secondary outcomes are as follows:
- NRS score: before epidural analgesia, 5, 10, 15, and 30 min after loading dose.
- Sensory blocking plane: 5, 10, 15, and 30 min after loading dose.
- Motor blocking score: 15 and 30 min after loading dose.
- Side effects of parturients: the incidence of bradycardia, hypotension, hypoxia, nausea, vomiting, pruritus, urination disorder and dizziness.
- Apgar score: 1 and 5 min after fetal delivery.
- Drug consumption per hour is calculated as total drug consumption divided by analgesia hours.
- Degree of satisfaction (0–10, 10 represents the highest level).
Sample Size Determination
The results of pilot test indicated that the percentages of painless uterine contraction 15 min after epidural labor analgesia initiation were 80.0% and 65.0% in L2-3 and L3-4 group, respectively. The sample size was determined by the model of Compare 2 Proportions: 2-Sample, 2-Sided Equality in http://www.powerandsamplesize.com/Calculators/. We hypothesized an alpha level of 0.05, a power level of 0.8, thus we estimated that 135 subjects were needed. Considering dropout, we decided to include 150 patients, namely 75 in each group.
Statistical Analysis
SPSS 23.0 (IBM, USA) will be applied to document data and conduct statistical analysis. Variables like demographics, main vital signs, NRS score, sensory blocking plane, motor blocking score, apgar score, and drug consumption per hour will be verified by the Kolmogorov–Smirnov test to identify the normality of data distribution. Normally distributed data will be described as mean ± standard deviation and abnormally distributed data as median (inter-quartile range). Independent t-test and Wilcoxon rank test will be used to compare differences between the two groups, respectively. Count data such as side effects will be described as percentage and be analyzed by the chi-square test or Fisher’s exact test. P < 0.05 is considered as statistically significant.
Adverse Event Report
Vital signs of parturients and fetal heart rate will be continuously monitored in the first half hour after epidural analgesia initiation. Following monitoring will be conducted if necessary. Adverse events of epidural analgesia will be regularly evaluated and recorded in the case report chart. The senior anesthesiologists will participate in the treatment. Comparison of adverse events between the groups will be conducted by the chi-square test or Fisher’s exact test.
Discussion
Neuraxial analgesia is regarded as the most effective method to relieve labor pain all over the world as it can inhibit breakthrough pain of uterine contraction.11 Epidural administration makes the blocking plane more manipulated than subarachnoid anesthesia, while low concentrated ropivacaine hardly impacts the nervus motorius of parturients, which makes epidural analgesia a most widespread approach for labor analgesia.1,12,13
Efforts have been input to improve the quality of epidural analgesia for labor. Programmed intermittent epidural boluses (PIEB) and dural puncture epidural (DPE) are the most recent advances in labor analgesia.14 PIEB has been evidenced to provide a better maintenance for labor analgesia with less drug consumption.12,13,15 This can be explained by that the higher injection pressure of intermittent bolus leads to more extensive diffusion of liquid than continuous infusion.2 The optimal time interval and bolus volume for different concentrations of ropivacaine of PIEB have also been well estimated.8,9,16,17 The time interval and bolus volume of this study are in accordance with these results. Song et al18 and Wang et al19 have demonstrated that DPE was related to a faster onset of analgesia than standard technique. However, Cappiello et al20 and Chau et al21 have failed to detect significant difference in the onset of analgesia between DPE and the standard. Though this could be explained by the diversity of puncture needle or the concentration of anesthetics, there are still works worth to do to improve quality of labor pain management.
Previous studies have regarded L2-3, L3-4 and L4-5 as accessible sites for the effectiveness in suppressing breakthrough pain during labor analgesia.4,5,13 Wu et al4 observed the influences of different puncture points combined with PIEB on breakthrough pain in labor analgesia, and results showed that at 20 min after analgesia initiation, NRS scores of parturients all declined to 0 in L2-3, L3-4 and L4-5 group. Regrettably, due to its long observation- interval, this study did not detect a more rapid relief of pain among the three groups. For miserable parturients, pain reduction even one minute faster matters. Since L2-3 space is more closer to head, this facilitates solution to reach a higher level. A higher puncture point may accelerate the onset of analgesic effects. As there are few related studies, we designed this clinical trial.
This study is designed as a single-center, double-blinded and randomized controlled clinical trial in order to investigate the onset speed of painless uterine contraction when conducting epidural analgesia through different puncture points. The parturients will be punctured through L2-3 or L3-4 spaces to insert a conduit. Initiation of analgesia will be achieved by an injection of 7 mL solution containing 0.1% ropivacaine and 0.5 ug/mL sufentanil. PIEB mode will be applied to maintain analgesic effects. According to the previous studies, time interval and bolus volume of PIEB are set as 40 min and 9 mL, respectively.8,9
Xiang et al22 initiating analgesia by 8 mL liquid mixture that containing about 0.1% ropivacaine and 0.5 ug/mL sufentanil, analyzed that onset time of standard epidural analgesia was 12.90 ± 1.95 min. In Fan’s study, 10 mL solution consisted of 0.1% ropivacaine and 0.5 ug/mL sufentanil provided adequate analgesia at 15 min.23 With comprehensive consideration, we choose 15 min as the primary endpoint. Considering an additional volume will be administered if the NRS score is still more than 3 points 15 min after initial dose, it is hard to compare the exact onset time of all participants. Thus, the percentage of sufficient analgesia 15 min after the initial volume is selected as the primary outcome, which is similar to a recent study.24
To eliminate the interference from unsuccessful cases, the NRS scores, sensory blocking level and blocking symmetry will be examined 30 min after initial dose. Yet, there is still no standard definition of epidural labor analgesia failure.10 Referring to a recent study, unsuccessful epidural labor analgesia is defined as that the NRS score is still more than 3 points and the blocking plane is lower than T10 15 min after an additional impact volume, or there is an asymmetric blocking.4 In order to decrease the rate of failure, we take some measures. Firstly, the operatives will be well trained, and they must have conducted epidural anesthesia for at least two years. Secondly, we will not recruit obese parturients, an ultrasound machine will be used to ensure the puncture points as well. Before puncture, we will detailedly teach parturients how to cooperate during the puncture process and give tips on analgesia maintenance. Lastly, to avoid asymmetric blocking caused by catheter inserted too deep, the epidural catheter will be placed only 3 cm into the epidural space.
Safety is also a crucial part of a successful labor analgesia. Though we conduct epidural analgesia in a standard way of which the security has been widely examined, we will observe side effects like the incidence of bradycardia, hypotension, hypoxia, nausea, vomiting, pruritus, urination disorder and dizziness. Because the fetal heart monitoring can be diverse in the whole stages of labor owing to the complex personal situation, and studies have shown that epidural analgesia has little statistical influence on fetal heart rate, we will not analyze it.5,19,24 However, we will collect the apgar score to evaluate the security of neonates.
Conclusion
This clinical trial is designed to investigate the onset speed of painless uterine contraction when conducting epidural analgesia through L2-3 or L3-4 space. If the results indicate that percentage of sufficient analgesia 15 min after the initial volume is significantly larger in L2-3 group, we promote L2-3 a better choice of puncture point for epidural labor analgesia.
Trial Status
This trial was registered at Chinese Clinical Trial Registry on 16 April, 2023 (identifier ChiCTR2300070548). The study protocol was approved by the Ethics Committee of Deyang People’s Hospital on 06 April, 2023 (reference number 2023-04-026-H01). The first subject was recruited on 16 April, 2023, and the deadline was estimated to be 11 April, 2024.
Acquisition of Data
Six months after the results being published, the data could be acquired from the corresponding author upon reasonable purpose.
Acknowledgments
This study is an investigator-initiated clinical trial of Deyang People’s Hospital. There are no funds supporting us. However, this work is supported by Department of Anesthesiology and Department of Obstetrics in Deyang People’s Hospital.
Disclosure
The authors declare that there are no conflicts of interest for this work.
References
1. Halliday L, Nelson SM, Kearns RJ. Epidural analgesia in labor: a narrative review. Int J Gynaecol Obstet. 2022;159(2):356–364. doi:10.1002/ijgo.14175
2. Hogan Q. Distribution of solution in the epidural space: examination by cryomicrotome section. Reg Anesth Pain Med. 2002;27(2):150–156. doi:10.1053/rapm.2002.29748
3. Castro WH, Grönemeyer D, Jerosch J, et al. How reliable is lumbar nerve root sheath infiltration? Eur Spine J. 1994;3(5):255–257. doi:10.1007/BF02226574
4. Wu C, Shi B, Jiang H. Clinical observation of regular intermittent epidural injection combined with different puncture points in suppressing breakthrough pain in labour analgesia. J Obstet Gynaecol. 2019;39(3):297–301. doi:10.1080/01443615.2018.1469604
5. Tan HS, Reed SE, Mehdiratta JE, et al. Quality of labor analgesia with dural puncture epidural versus standard epidural technique in obese parturients: a double-blind randomized controlled study. Anesthesiology. 2022;136(5):678–687. doi:10.1097/ALN.0000000000004137
6. Soetens FM, Meeuwis HC, Van der Donck AG, et al. Influence of maternal position during epidural labor analgesia. Int J Obstet Anesth. 2003;12(2):98–101. doi:10.1016/S0959-289X(02)00160-7
7. Sah N, Vallejo M, Phelps A, et al. Efficacy of ropivacaine, bupivacaine, and levobupivacaine for labor epidural analgesia. J Clin Anesth. 2007;19(3):214–217. doi:10.1016/j.jclinane.2006.11.003
8. Ran X, Zhou S, Cao K, et al. Optimization of programmed intermittent epidural bolus volume for different concentrations of ropivacaine in labor analgesia: a biased coin up-and-down sequential allocation trial. BMC Pregnancy Childbirth. 2022;22(1):590. doi:10.1186/s12884-022-04912-8
9. Zhou SQ, Wang J, Du WJ, et al. Optimum interval time of programmed intermittent epidural bolus of ropivacaine 0.08% with sufentanyl 0.3 μg/mL for labor analgesia: a biased-coin up-and-down sequential allocation trial. Chin Med J. 2020;133(5):517–522. doi:10.1097/CM9.0000000000000669
10. Guasch E, Iannuccelli F, Brogly N, et al. Failed epidural for labor: what now? Minerva Anestesiol. 2017;83(11):1207–1213. doi:10.23736/S0375-9393.17.12082-1
11. Süğür T, Kızılateş E, Kızılateş A, et al. Labor analgesia: comparison of epidural patient-controlled analgesia and intravenous patient-controlled analgesia. Agri. 2020;32(1):8–18. doi:10.14744/agri.2019.35403
12. Riazanova OV, Alexandrovich YS, Guseva YV, et al. A randomized comparison of low dose ropivacaine programmed intermittent epidural bolus with continuous epidural infusion for labour analgesia. Rom J Anaesth Intensive Care. 2019;26(1):25–30. doi:10.2478/rjaic-2019-0004
13. Roofthooft E, Barbé A, Schildermans J, et al. Programmed intermittent epidural bolus vs. patient-controlled epidural analgesia for maintenance of labour analgesia: a two-centre, double-blind, randomised study. Anaesthesia. 2020;75(12):1635–1642. doi:10.1111/anae.15149
14. Xiao F, Yao HQ, Qian J, et al. Determination of the optimal volume of programmed intermittent epidural bolus when combined with the dural puncture epidural technique for labor analgesia: a random-allocation graded dose-response study. Anesth Analg. 2023. doi:10.1213/ANE.0000000000006451
15. Munro A, MacCormick H, Aidemouni M, et al. A retrospective cohort comparison of programmed intermittent epidural bolus (PIEB) and continued epidural infusion (CEI) on delivery mode. Can J Anaesth. 2022;69(7):909–911. doi:10.1007/s12630-022-02268-3
16. Epsztein Kanczuk M, Barrett NM, Arzola C, et al. Programmed intermittent epidural bolus for labor analgesia during first stage of labor: a biased-coin up-and-down sequential allocation trial to determine the optimum interval time between boluses of a fixed volume of 10 mL of Bupivacaine 0.0625% with fentanyl 2 μg/mL. Anesth Analg. 2017;124(2):537–541. doi:10.1213/ANE.0000000000001655
17. Carvalho B, George RB, Cobb B, et al. Implementation of programmed intermittent epidural bolus for the maintenance of labor analgesia. Anesth Analg. 2016;123(4):965–971. doi:10.1213/ANE.0000000000001407
18. Song Y, Du W, Zhou S, et al. Effect of dural puncture epidural technique combined with programmed intermittent epidural bolus on labor analgesia onset and maintenance: a randomized controlled trial. Anesth Analg. 2021;132(4):971–978. doi:10.1213/ANE.0000000000004768
19. Wang J, Zhang L, Zheng L, et al. A randomized trial of the dural puncture epidural technique combined with programmed intermittent epidural boluses for labor analgesia. Ann Palliat Med. 2021;10(1):404–414. doi:10.21037/apm-20-2281
20. Cappiello E, O’Rourke N, Segal S, et al. A randomized trial of dural puncture epidural technique compared with the standard epidural technique for labor analgesia. Anesth Analg. 2008;107(5):1646–1651. doi:10.1213/ane.0b013e318184ec14
21. Chau A, Bibbo C, Huang CC, et al. Dural puncture epidural technique improves labor analgesia quality with fewer side effects compared with epidural and combined spinal epidural techniques: a randomized clinical trial. Anesth Analg. 2017;124(2):560–569. doi:10.1213/ANE.0000000000001798
22. Xiang B, Yang J, Lei X, et al. Adjuvant sufentanil decreased the EC50 of epidural ropivacaine for labor analgesia in healthy term pregnancy. Drug Des Devel Ther. 2021;15:2143–2149. doi:10.2147/DDDT.S307478
23. Fan M, Li J, Cao R, et al. Efficacy and safety of dexmedetomidine-ropivacaine versus sufentanil-ropivacaine for epidural labor analgesia: a randomized controlled trial. Ann Palliat Med. 2022;11(4):1410–1420. doi:10.21037/apm-22-264
24. Yi J, Li Y, Yuan Y, et al. Comparison of labor analgesia efficacy between single-orifice and multiorifice wire-reinforced catheters during programmed intermittent epidural boluses: a randomized controlled clinical trial. Reg Anesth Pain Med. 2023;48(2):61–66. doi:10.1136/rapm-2022-103723
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Nalbuphine as a Bridge to Delayed Epidural Analgesia: A Randomized Trial on First-Stage Labor Duration
Xu Y, Song C, Xu Y, Luo H, Chen K, Peng S, Guo L, Yu J
Drug Design, Development and Therapy 2026, 20:574810
Published Date: 7 February 2026