Back to Journals » Infection and Drug Resistance » Volume 15
Multidrug-Resistant Tuberculosis Treatment Outcome and Associated Factors at the University of Gondar Comprehensive Specialized Hospital: A Ten-Year Retrospective Study
Authors Belachew T ![]() , Yaheya S, Tilahun N, Gebrie E, Seid R, Nega T
, Yaheya S, Tilahun N, Gebrie E, Seid R, Nega T ![]() , Biset S
, Biset S ![]()
Received 7 March 2022
Accepted for publication 27 May 2022
Published 3 June 2022 Volume 2022:15 Pages 2891—2899
DOI https://doi.org/10.2147/IDR.S365394
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Teshome Belachew,1 Seid Yaheya,2 Nehemia Tilahun,2 Eshet Gebrie,2 Rim Seid,2 Tilahun Nega,3 Sirak Biset1
1Department of Medical Microbiology, School of Biomedical and Laboratory Sciences, University of Gondar, Gondar, Ethiopia; 2School of Biomedical and Laboratory Sciences, University of Gondar, Gondar, Ethiopia; 3University of Gondar Comprehensive Specialized Hospital, Gondar, Ethiopia
Correspondence: Sirak Biset, Tel +251-911-598-568, Email [email protected]
Background: Multidrug-resistant tuberculosis (MDR-TB) remains a public health crisis and a health security threat worldwide. Poor public health infrastructure, inefficient infection control and mismanagement of TB treatment are among the reasons for the continuous emergence and spread of drug-resistant TB (DR-TB). The final treatment outcome is the most direct measurement of TB control programs. Therefore, this study sought to determine the proportions and predictors of TB treatment outcomes among MDR/RR-TB treated patients.
Methods: A 10-year, 2011 to 2021, hospital-based retrospective cohort study was conducted at the University of Gondar Comprehensive Specialized Hospital. The records of 408 MDR-TB patients, 389 with treatment outcome and 19 on treatment, were collected using a structured checklist.
Results: A total of 389 patients with a recorded MDR/RR-TB treatment outcome were included. The treatment success rate was 77.12%, with 58.35% cured and 18.76% treatment completed. The proportion of death rate, treatment default loss to follow-up, treatment failure, and unknown treatment outcome was 9.25%, 6.94%, 3.1%, and 3.6%, respectively. Regarding the patient category, the most successful treatment outcome (83.5%) came from patients diagnosed with relapse cases, followed by new cases (81.8%). An unsuccessful treatment outcome was significantly associated with patients aged > 44 years (AOR, 3.3, 95% CI = 1.55– 6.99).
Conclusion and Recommendations: This study indicated that nearly 23% of MDR/RR-TB patients had unsuccessful treatment outcomes and being older was significantly correlated with these outcomes. For better outcomes, it is recommended to strengthen combined treatment adherence interventions and evaluate treatment regimens and administration options. A prospective cohort study may be required to investigate the full range of potential causes of unfavorable outcomes.
Keywords: tuberculosis treatment outcome, multidrug-resistant tuberculosis, rifampicin resistance, Ethiopia
Background
Tuberculosis (TB) is one of the top causes of morbidity and mortality worldwide, particularly in developing countries.1,2 TB caused by Mycobacterium tuberculosis (MTB), a bacterium that can survive harsh environments mainly due to the presence of an unusually thick, lipid-rich cell envelope,3,4 infects approximately 1/4 of the world’s population.5 Although, the global incidence and death rates of TB have decreased in recent years,5,6 meeting the WHO End TB Strategy targets is becoming increasingly difficult.7 The emergence of drug-resistant (DR) MTB strains is an impediment to effective TB control programs,5,6,8 which could explain the setback.2,9,10 DR-TB, responsible for roughly one-third of all antimicrobial resistance deaths worldwide,11 is a public health crisis that poses a threat to global health security. In 2019, around 1.5 million DR-TB cases were reported worldwide.5 Both mismanagement of TB treatment and person-to-person transmission are the primary reasons for the continued emergence and spread of DR-TB.8,12,13
Multidrug-resistant TB (MDR-TB), TB resistant to at least isoniazid and rifampicin, and rifampicin-resistant (RR) TB, TB resistant to rifampicin with or without resistance to other first-line anti-TB drugs, are the most common types of DR-TB.14 According to the reports, up to 90% of RR-TB cases are resistant to isoniazid.15 As a result, in countries with limited MDR-TB laboratory diagnostic capacity, RR-TB is utilized as a surrogate marker for MDR-TB.16 Globally, 3–4% of new and 18–21% of previously treated cases are diagnosed with MDR/RR-TB.5,6 However, in Ethiopia, the prevalence of RR-TB and MDR-TB in 2019 was 1.1% and 1.03% among new and 7.5% and 6.52% among previously treated TB cases, respectively.16 Globally, an estimated of nearly half a million new cases of MDR/RR-TB emerge each year, requiring regimens that include second-line drugs, which are less effective, more expensive, and more toxic than the first-line drugs.5,14,17
Even though the annual number of people taking treatment for MDR/RR-TB has increased in recent years, only 482,683 peoples with MDR/RR-TB were treated between 2018 and 2020, which is equivalent to 32% of the five-year (2018–2022) treatment target of 1.5 million.6 The worldwide MDR/RR-TB treatment success rate (TSR) has also increased in recent years. For example, it was 56% in 2016, 57% in 2017 and 59% in 2018.5,6,18 In 2018, the average TSR in the African region was 69%, which was higher than in the European region (56%). In Ethiopia, it was >75%, which was one of the highest among high-burden countries.6
Most of the 30 high-burden countries for TB, HIV-associated TB, and RR-TB to be used by WHO in the years 2021–2025 are from Africa,6 where factors that usually affect TB treatment outcomes, such as poverty, undernutrition, and chronic infectious diseases are prevalent.19 In Ethiopia, factors such as low body mass index (BMI), comorbidities, previous anti-TB drug exposure, older age, anemia, and treatment delay were reported as the causes of poor treatment outcomes.20–22 As far as the literature is concerned, there has been little work done on treatment outcomes and associated factors of MDR/RR-TB in the study area.
Materials and Methods
A hospital-based retrospective cohort study was undertaken from June to September 2021 at the University of Gondar Comprehensive Specialized Hospital (UoGCSH), Gondar, Ethiopia. This teaching hospital provides outpatient and inpatient services for more than five million residents in North Gondar and its surrounding areas. This hospital offers curative, rehabilitative, educational, and promotional services. It has more than 518 beds, with different health service-providing departments, including the MDR-TB treatment center. UoGCSH is one of Ethiopian’s treatment initiating centers (TICs) for DR-TB since 2010, but the only one in the North Gondar zone, which has many treatment follow-up centers (TFCs). Patients with MDR-TB initiate their treatments in the UoGCSH, while stable patients follow the treatment under a directly observed therapy (DOT) program in the nearby TFCs as ambulatory outpatients. However, all information on patients who were registered for MDR-TB treatment was captured at the UoGCSH.
Study Population
We included all patients who had MDR/RR-TB treatment outcomes registered on MDR-TB registration books from 2011 to 2021. Patients receiving MDR-TB treatment were excluded from the inferential statistics.
Data Collection Tools
We collected the data from registration books of patients with MDR/RR-TB using a structured checklist. There were three data collectors and two supervisors. Patient information, including age, sex, BMI, treatment outcomes, history of TB drug use, HIV status or other comorbidities, patient category, site of TB infection, laboratory results, types of DR-TB, and year of diagnosis, were obtained from MDR/RR-TB registration book.
Treatment Outcomes
Treatment outcomes were defined and classified according to the WHO guidelines23,24
Cured: A patient with bacteriologically confirmed TB at the beginning of treatment who completed treatment as recommended by the national policy, with evidence of bacteriological response and no evidence of failure. Treatment completed: A patient who completed treatment as recommended by the national policy, whose outcome does not meet the definition for cure or treatment failure. Died: A patient who died before starting treatment or during the course of treatment. Treatment failed: A patient whose treatment regimen needed to be terminated or permanently changed to a new regimen or treatment strategy. Lost to follow-up: A patient who did not start treatment or whose treatment was interrupted for 2 consecutive months or more. Not evaluated: A TB patient for whom no treatment outcome is assigned. Successful treatment outcomes: include cured patients and those who completed treatment.
Data Quality Control
We used different methods to ensure that the collected data had the required quality. For instance, we used a structured data collection checklist and regular communication with the hospital staff. Finally, we checked the collected data and cleaned manually and entered into SPSS version 20 for analysis.
Data Processing and Analysis
Descriptive statistics were used to calculate frequencies and percentages of variables. Continuous variables were summarized using their mean and standard deviations. The magnitude of the association between different variables and MDR/RR-TB was assessed using bivariable and multivariable analyses. Variables with a p-value <0.20 during bivariate analysis were taken to the multivariate analysis to check whether there was an association of MDR/RR-TB with factors and expressed by an adjusted odds ratio at 95% confidence interval. Finally, results were presented in tables, texts, and graphs.
Result
Demographic Characteristics
A total of 408 MDR/RR-TB patients, 389 with treatment outcomes and 19 on treatment, were registered at the UoGCSH between 2011 and 2021. The highest number of patients enrolled into the treatment was in 2013 (72/408; 17.6%), followed by 2014 (50/408; 12.3%), 2012 (45/408; 11%), and 2017 (42/408; 10.3%). Most of the MDR/RR-TB patients were male (251/408; 61.5%). The age distribution of the patients ranged from 1 to 73 years, with a mean and standard deviation of 32.4 and ± 12.55 years. Majority of the patients were aged between 25 and 44 (224/408; 54.9%), followed by <25 years (111/408; 27.2%) (Table 1). Of the total registered MDR/RR-TB patients, 19/408; 4.7% were on treatment and thus excluded in the analysis part.
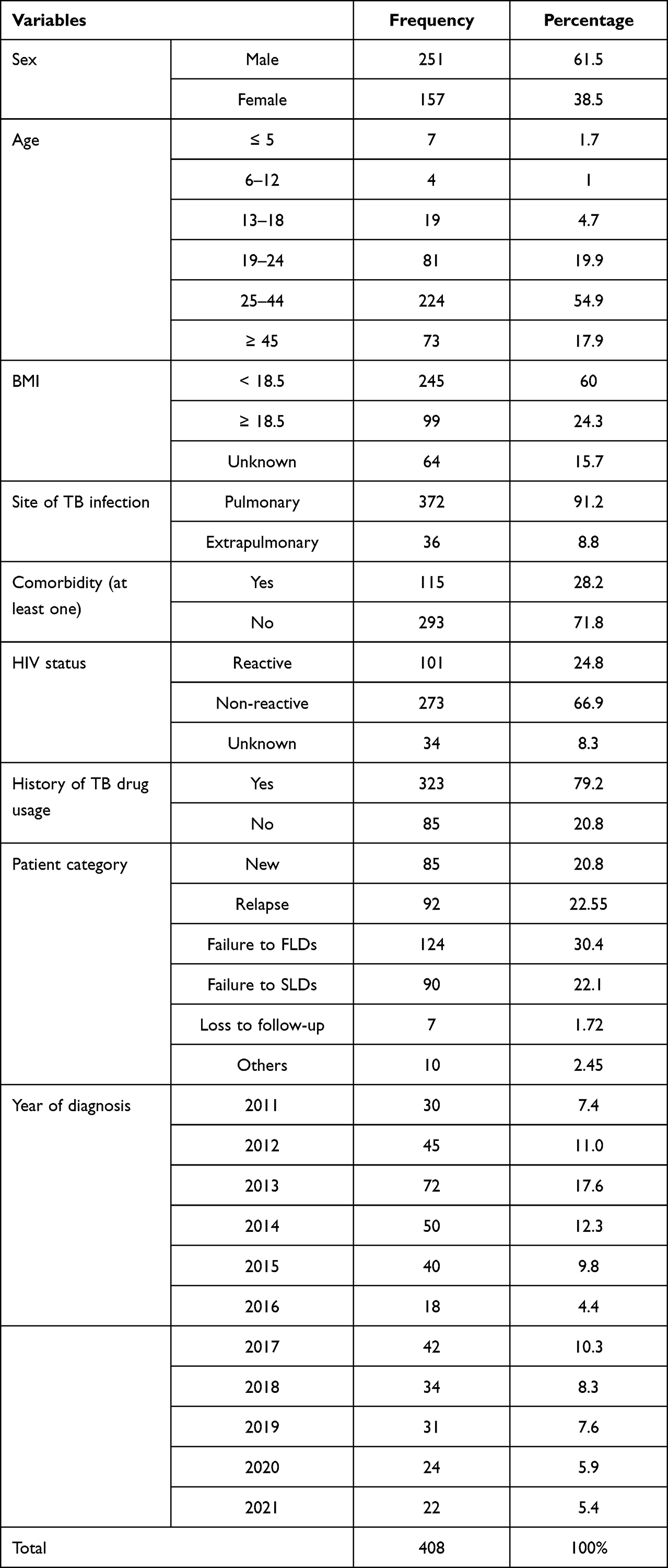 |
Table 1 Socio-Demographic and Clinical Characteristics of MDR/RR-TB Patients Treated at the UoGCSH, Between 2011 and 2021 (N = 408) |
Clinical Characteristics
Most of the patients (245; 60%) were suffered from malnutrition, their body mass index (BMI) ratio was below the normal range (18.5–24.9). Majority of the patients had pulmonary TB (PTB) (372; 91.2%) and previous TB treatment (318; 77.9%). About 101 (24.8%) of the MDR/RR-TB patients were HIV positive, and 34 (8.3%) of the patients were with unknown HIV status. The HIV prevalence among those with known status was 101/374 (27%). More than half of the patients (214; 52.5%) were started MDR/RR-TB treatment after failure to TB drug treatment, followed by relapse (92; 22.55%) and newly diagnosed (85; 20.8%) cases. Of the 408 patients, 124 (30.4%) and 90 (22.1%) had previous exposure to first-line drugs (FLDs) and second-line drugs (SLDs), respectively (Table 1).
MDR/RR-TB Treatment Outcomes
Of the 389 registered MDR/RR-TB patients with treatment outcomes, the majority (227; 58.35%) were cured, followed by completed (73; 18.76%). The overall treatment success rate was 300/389 (77.12%). Thirty-six (9.25%) treated patients died and treatment failure was observed in 12 (3.1%) cases. From the total unsuccessful MDR/RR-TB treatment outcome cases, 14 (3.6%) were with treatment outcomes that could not be evaluated (Table 2).
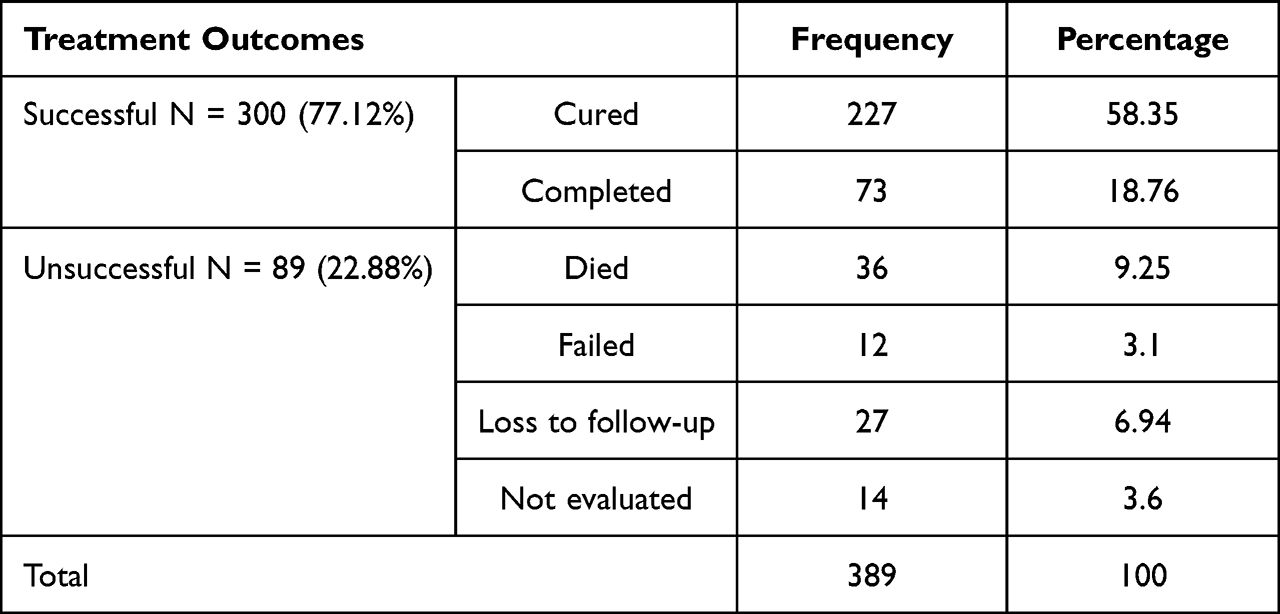 |
Table 2 Treatment Outcomes Among Patients Who Had Received Treatment for MDR/RR-TB at the UoGCSH, Between 2011 and 2021 (N = 389) |
Factors Associated with MDR/RR-TB Treatment Outcomes
Possible factors affecting the MDR/RR-TB treatment outcome were assessed using the bi-variable and multivariable logistic regression model. In bivariable analysis, variables like age, BMI, and patient category had a p-value of <0.2 and thus eligible for the multivariable analysis. According to the multivariable analysis result, treatment outcomes of TB were affected by the age of the patient. Patients aged above 44 years were 3.3 times more likely to have unsuccessful treatment outcomes than those aged less than 25 years [AOR, 3.292; 95% CI (1.551–6.988)]. There was also a higher proportion of unsuccessful treatment outcome among patients with comorbidities, HIV infection, and history of anti-TB drug use than their counterparts (Table 3).
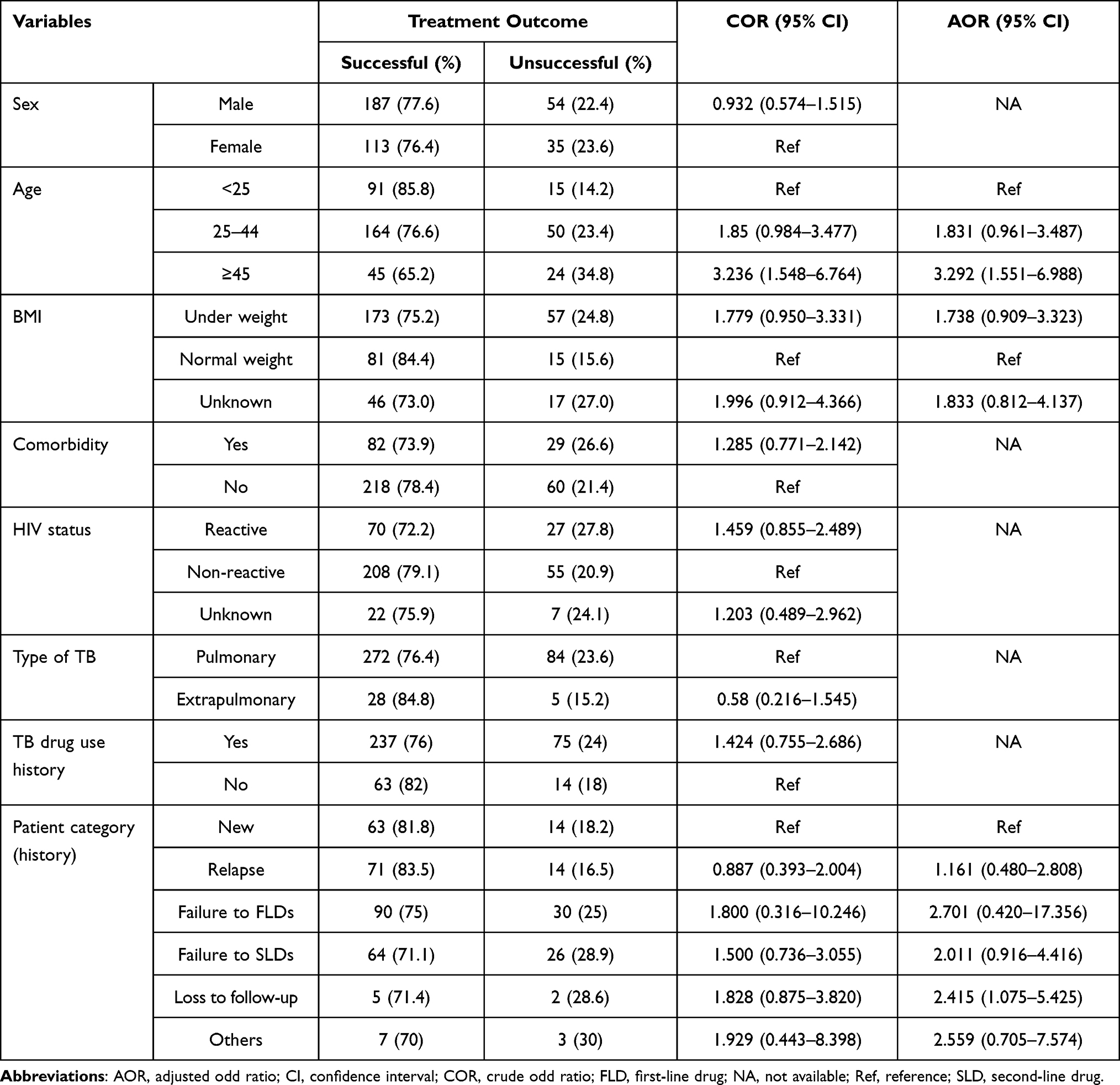 |
Table 3 Bivariable and Multivariable Analyses of Factors Associated with MDR-TB Treatment Outcomes at the UoGCSH, from 2011 to 2021. (N = 389) |
Discussion
In the past 20 years, there has been a significant decrease in TB incidence and an estimated number of annual TB deaths. Globally, because of TB treatment, more than estimated 63 million deaths have been averted since 2000.5 Since TB treatment success is one of the most important indicators in WHO’s End TB Strategy, tracking treatment outcomes over time is substantial.25
The current study found a 77.12% (95% CI = 73.0–81.5) MDR/RR-TB TSR, which is in agreement with the 75.7% national TSR report (from 2009 to 2019) by Habteyes Tola.21 Other retrospective studies conducted in Addis Ababa (2011–2016)26 and Southern-Ethiopia (2014–2019)27 also reported similar findings, 76.9% and 76.32%, respectively. However, according to a review paper published in 2020, the overall pooled TSR in Ethiopia was 63.82%, which was less than the current report.22 Our finding was also higher than results reported in Northeast Ethiopia, 64.4%,28 Northwest Ethiopia, 63%,29 and a systematic review by Setegn Eshetie, 59.2%.30 This huge gap in TSR may be due to differences in the study area, study protocol, or study populations used to calculate the success rate. For instance, in the above two studies,29,30 patients on treatment were included in the TSR calculation, but we excluded them in the current study.
The mortality rate in the current study was 9.25% (95% CI = 6.2–12.3), which is in agreement with a report from Southern Ethiopia, 9.37%.27 However, it was lower than other individual reports in Ethiopia.22,28–31 The current result was even lower than death rates reported using nationwide data. For instance, according to the 2018 published review32 and a retrospective study from Ethiopia,21 about 14.3% and 12.8% death rates, respectively, were reported among MDR/RR-TB treated patients. The presence of patients with unknown outcomes (3.6%) may have resulted in an underestimation of the mortality rate in this study. Those patients are more likely to have negative outcomes, including death, because they no longer visit the healthcare system unless they have been transferred out.
Another notable finding in this study was the significant association between unsuccessful MDR/RR-TB treatment outcome and older age (>44 years). This was also reported by other studies in Ethiopia21,22,33 and abroad.34,35 The presence of underlying malignant conditions, immunosuppressive therapies, malnutrition, and other age-related health conditions make elderly population susceptible to TB disease and its complications.36–38
In this study, patients with a low BMI, comorbidities, HIV infection, a history of past anti-TB drug usage, and pulmonary TB had a higher proportion of unfavorable treatment outcomes than their counterparts. The association, however, was not statistically supported. A study conducted from a teaching and referral hospital in Wolayta Sodo, Ethiopia, reported similar findings.39 However, studies in Ethiopia and abroad reported that undernutrition,31,33 HIV infection,21,26 and history of anti-TB drug use40 were risk factors for unsuccessful treatment outcomes such as treatment failure and death. In the present study, there were a considerable number of patients with unknown HIV and BMI status, which may have underestimated the frequency of HIV infection and BMI, respectively. As a result, unknown status may have an impact on the association of treatment outcome with the variables. The UoGCSH is currently working on the implementation of electrical medical recording (digital data management), and we anticipate that the above difficulties will be addressed as a result of this type of initiative.
We acknowledge that our study has limitations. The major limitation was attributable to the use of secondary data, we could not access the full range of factors for treatment outcomes. For instance, patient data on sociodemographic, behavioral, and clinical factors, such as the presence or absence of pregnancy, were missing in patient records. Furthermore, the presence of unknown status for some variables, such as HIV infection and BMI, may affect our analysis of their relationship with treatment outcomes.
Conclusion and Recommendations
Although the TSR seen in this study was better than other reports in Ethiopia and abroad, there were still significant numbers of lost to follow-up and death cases. Thus, it is recommended to strengthen combined treatment adherence interventions to reduce the number of deaths and loss to follow-up cases in MDR/RR-TB patients. Furthermore, regular evaluation of treatment regimens and treatment administration options can be substantial in reducing unfavorable treatment outcomes.14 A prospective cohort study may be required to investigate the full range of potential causes of unfavorable outcomes.
Abbreviations
BMI, body mass index; CI, confidence interval; COVID-19, coronavirus disease 2019; DOT, directly observed therapy; DR-TB, drug-resistant tuberculosis; FLDs, first-line drugs; HIV, human immunodeficiency virus; MDR-TB, multidrug-resistant tuberculosis; MTB, Mycobacterium tuberculosis; RR-TB, rifampicin-resistant tuberculosis; SLDs, second-line drugs; SPSS, Statistical Package for Social Sciences; TB, tuberculosis; TSR, treatment success rate; UoGCSH, University of Gondar Comprehensive Specialized Hospital; WHO, World Health Organization.
Data Sharing Statement
All data generated or analyzed during this study were included in this article. Data that support the findings of this study are also available from the corresponding author upon reasonable request.
Ethical Approval and Consent to Participate
Before the commencement of the study, we obtained ethical clearance from the University of Gondar, School of Biomedical and Laboratory Sciences ethical review committee (Ref. No/SBMLS/2894/2021; July 2021), and an official letter of co-operations was provided to UoGCSH. Before data collection, we explained the study objectives to the heads of the hospital director and laboratory personnel who worked in the hospital. Since we used secondary data for this study, we did not require the patient’s informed consent. We conducted the study following the Declaration of Helsinki.41 To ensure confidentiality of information from participant’s record, we did not record any personal identifiers on the data collection sheet, and secured data from participant records were not available to anyone except for the investigators.
Acknowledgments
We thank all the Medical Microbiology staff working at the University of Gondar, School of Biomedical and Laboratory Science, College of Medicine and Health Sciences for their unreserved support. We would like to thank the UoGCSH, and its staff working at the TB treatment center for their support during the data collection period.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Furin J, Cox H, Pai M. Tuberculosis. Lancet. 2019;393(10181):1642–1656. doi:10.1016/S0140-6736(19)30308-3
2. Zaman K. Tuberculosis: a global health problem. J Heal Popul Nutr. 2010;28(2):111.
3. Friedman LN, Dedicoat M, Davies PD. Clinical Tuberculosis.
4. Allué-Guardia A, García JI, Torrelles JB. Evolution of drug-resistant mycobacterium tuberculosis strains and their adaptation to the human lung environment. Front Microbiol. 2021;12. doi:10.3389/fmicb.2021.612675
5. World Health Organization. Global tuberculosis report 2020 [Internet]. World Health Organization; 2020 [
6. World Health Organization. Global tuberculosis report 2021 [Internet]. Geneva: World Health Organization; 2021 [
7. World Health Organization. The end TB strategy [Internet]. World Health Organization; 2015 [
8. Singh R, Dwivedi SP, Gaharwar US, Meena R, Rajamani P, Prasad T. Recent updates on drug resistance in Mycobacterium tuberculosis. J Appl Microbiol. 2020;128(6):1547–1567. doi:10.1111/jam.14478
9. Lange C, Chesov D, Heyckendorf J, Leung CC, Udwadia Z, Dheda K. Drug-resistant tuberculosis, an update on disease burden, diagnosis and treatment. Respirology. 2018;23(7):656–673. doi:10.1111/resp.13304
10. Mariandyshev A, Eliseev P. Drug-resistant tuberculosis threatens WHO’s End-TB strategy. Lancet Infect Dis. 2017;17(7):674–675. doi:10.1016/S1473-3099(17)30246-3
11. Pai M, Memish ZA. Antimicrobial resistance and the growing threat of drug-resistant tuberculosis. J Epidemiol Glob Health. 2016;6(2):45. doi:10.1016/j.jegh.2016.02.001
12. World Health Organization. Tuberculosis, multidrug-resistant tuberculosis (MDR-TB) [Internet]. World Health Organization; 2018 [
13. Kendall EA, Fofana MO, Dowdy DW. The burden of transmitted multi-drug resistance among epidemics epidemics of tuberculosis, a transmission model. Lancet Respir Med. 2015;3(12):963–972. doi:10.1016/S2213-2600(15)00458-0
14. World Health Organization. WHO consolidated guidelines on tuberculosis. Module 4, treatment - drug-resistant tuberculosis treatment. [Internet]. Geneva: World Health Organization; 2020 [
15. Lecai J, Mijiti P, Chuangyue H, et al. Predictors and trends of MDR/RR-TB in Shenzhen China: a retrospective 2012–2020 period analysis. Infect Drug Resist. 2021;14:4481–4491. doi:10.2147/IDR.S335329
16. Federal Ministry of Health of Ethiopia. Guidelines for Clinical and Programmatic Management of TB, TB/ HIV, DR-TB and Leprosy in Ethiopia.
17. World Health Organization. WHO consolidated guidelines on drug-resistant tuberculosis treatment [Internet]. Geneva: World Health Organization; 2019 [
18. World Health Organization. Global tuberculosis report 2019. Geneva: World Health Organization; 2019.
19. Olupot-Olupot P, Namuyodi D, Obbo JSO, Meadway J. Multidrug resistant tuberculosis (MDR-TB) in emerging economies in Sub-Saharan Africa, clinicians’ public health concerns. J Public Heal Emerg. 2017;1:43. doi:10.21037/jphe.2017.03.01
20. Jaleta KN, Gizachew M, Gelaw B, Tesfa H, Getaneh A, Biadgo B. Rifampicin-resistant Mycobacterium tuberculosis among tuberculosis-presumptive cases at University of Gondar Hospital, northwest Ethiopia. Infect Drug Resist. 2017;10:185–192. doi:10.2147/IDR.S135935
21. Tola H, Holakouie-Naieni K, Mansournia MA, et al. National treatment outcome and predictors of death and treatment failure in multidrug-resistant tuberculosis in Ethiopia, a 10-year retrospective cohort study. BMJ Open. 2021;11(8):e040862. doi:10.1136/bmjopen-2020-040862
22. Alemu A, Bitew ZW, Worku T. Poor treatment outcome and its predictors among drug-resistant tuberculosis patients in Ethiopia, a systematic review and meta-analysis. Int J Infect Dis. 2020;98:420–439. doi:10.1016/j.ijid.2020.05.087
23. World Health Organization. Meeting report of the WHO expert consultation on drug-resistant tuberculosis treatment outcome definitions [Internet]. Geneva; 2021 [
24. World Health Organization. Definitions and reporting framework for tuberculosis – 2013 revision [Internet]. Geneva: World Health Organization; 2013 [
25. World Health Organization. Implementing the End TB Strategy, the essentials [Internet]. Geneva: World Health Organization; 2015 [
26. Aragaw N, Teferi M, Ali O, et al. Treatment outcomes and predictors of outcome in Multidrug Resistance Tuberculosis (MDR-TB) cohort of patients in Addis Ababa, Ethiopia. Am J Heal Res. 2021;9(5):204. doi:10.11648/j.ajhr.20210905.19
27. Bogale L, Tsegaye T, Abdulkadir M, Akalu TY. Unfavorable treatment outcome and its predictors among patients with multidrug-resistance tuberculosis in southern Ethiopia in 2014 to 2019, a multi-center retrospective follow-up study. Infect Drug Resist. 2021;14:1343–1355. doi:10.2147/IDR.S300814
28. Baye AM, Demisis Sarhie W, Endalew BT. Treatment outcomes of multi-drug-resistant tuberculosis and its determinants in Boru Meda Hospital, Northeast Ethiopia. J Infect Dis Ther. 2018;06(01). doi:10.4172/2332-0877.1000350
29. Alene KA, Viney K, McBryde ES, Tsegaye AT, Clements ACA. Treatment outcomes in patients with multidrug-resistant tuberculosis in north-west Ethiopia. Trop Med Int Heal. 2017;22(3):351–362.
30. Eshetie S, Alebel A, Wagnew F, Geremew D, Fasil A, Sack U. Current treatment of multidrug resistant tuberculosis in Ethiopia, an aggregated and individual patients’ data analysis for outcome and effectiveness of the current regimens 11 Medical and Health Sciences 1117 Public Health and Health Services. BMC Infect Dis. 2018;18(1):1–0.
31. Wakjira MK, Sandy PT, Mavhandu-Mudzusi AH. Treatment outcomes of patients with MDR-TB and its determinants at referral hospitals in Ethiopia. PLoS One. 2022;17(2):e0262318. doi:10.1371/journal.pone.0262318
32. Eshetie S, Alebel A, Wagnew F, Geremew D, Fasil A, Sack U. Current treatment of multidrug resistant tuberculosis in Ethiopia, an aggregated and individual patients’ data analysis for outcome and effectiveness of the current regimens. BMC Infect Dis. 2018;18(1),486. doi:10.1186/s12879-018-3401-5
33. Kassa GM, Tadesse A, Gelaw YA, et al. Predictors of mortality among multidrug-resistant tuberculosis patients in central Ethiopia, a retrospective follow-up study. Epidemiol Infect. 2020;15(148):e258. doi:10.1017/S0950268820002514
34. Murali S, Krishnamoorthy Y, Knudsen S, et al. Comparison of profile and treatment outcomes between elderly and non-elderly tuberculosis patients in Puducherry and Tamil Nadu, South India. PLoS One. 2021;16(8):e0256773. doi:10.1371/journal.pone.0256773
35. Van LH, Phu PT, Vinh DN, et al. Risk factors for poor treatment outcomes of 2266 multidrug-resistant tuberculosis cases in Ho Chi Minh City, a retrospective study. BMC Infect Dis. 2020;20(1),164. doi:10.1186/s12879-020-4887-1
36. Byng-Maddick R, Noursadeghi M. Does tuberculosis threaten our ageing populations? BMC Infect Dis. 2016;16(1),119. doi:10.1186/s12879-016-1451-0
37. Schaaf HS, Collins A, Bekker A, Davies PDO. Tuberculosis at extremes of age. Respirology. 2010;15(5),747–763. doi:10.1111/j.1440-1843.2010.01784.x
38. Rajagopalan S. Tuberculosis and aging: a global health problem. Clin Infect Dis. 2001;33(7),1034–1039. doi:10.1086/322671
39. Teferi MY, Didana LD, Hailu T, Woldesenbet SG, Bekele S, Mihret A. Tuberculosis treatment outcome and associated factors among tuberculosis patients at Wolayta Sodo Teaching and Referral Hospital, Southern Ethiopia, a retrospective study. J Public Health Res. 2021;10:
40. Ali MH, Alrasheedy AA, Kibuule D, Godman B, Hassali MA, Ali HMH. Assessment of multidrug-resistant tuberculosis (MDR-TB) treatment outcomes in Sudan; findings and implications. Expert Rev Anti Infect Ther. 2019;17(11),927–937. doi,10.1080/14787210.2019.1689818
41. World Medical Association. Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310,45.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Nomogram for the Prediction of Unfavorable Treatment Outcome Among Multi-Drug Resistant Tuberculosis Patients in North West Ethiopia: An Application of Prediction Modelling
Anley DT, Akalu TY, Merid MW, Tsegaye T
Infection and Drug Resistance 2022, 15:3887-3904
Published Date: 21 July 2022