Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Multidisciplinary Student Groups Support Digital Education as a Public Health Precautional Action to Prevent Spread of COVID-19 Infection: A Mixed Methods Study
Authors Almendingen K ![]() , Skotheim T, Ervik B, Magnus EM
, Skotheim T, Ervik B, Magnus EM
Received 14 February 2022
Accepted for publication 26 May 2022
Published 21 June 2022 Volume 2022:15 Pages 1369—1382
DOI https://doi.org/10.2147/JMDH.S362365
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Kari Almendingen,1 Torhild Skotheim,2 Bjørn Ervik,3 Ellen Merethe Magnus3
1Department of Nursing and Health Promotion, Faculty of Health Sciences, Oslo Metropolitan University, Oslo, Norway; 2Department of Primary and Secondary Teacher Education, Faculty of Education and International Studies, Oslo Metropolitan University, Oslo, Norway; 3Section for Analysis and Quality of Education, Department of Academic Affairs, Division for Education and Library, Oslo Metropolitan University, Oslo, Norway
Correspondence: Kari Almendingen, Department of Nursing and Health Promotion, Faculty of Health Sciences, Oslo Metropolitan University, Oslo, Norway, Tel +4790158165, Email [email protected]
Background: Health personnel had greater odds of contracting COVID-19 during its first wave in Norway, compared with all working-age individuals. Students in health care, but also in social care and teacher education programs may be exposed to the risk of being infected themselves and to infect others through their mandatory practical training. Online education may reduce their risk of becoming patients and spreaders both in their private lives and during their mandatory training.
Aim: To explore the extent to which unvaccinated professional students fear transmission of SARS-CoV-2 from fellow students and from public transportation during the third wave.
Materials and Methods: In this cross-sectional study, 3148 students in health care, social care, and teacher education programs and 32 supervisors completed online questionnaires consisting of open and closed questions (mixed methods) after participating in digital interprofessional learning (IPL) small-group seminars (49.6% and 65% response rates, respectively). On a 6-point Likert scale (0– 5), all means concerning fear were around 3, with overlapping confidence intervals. Fear of infecting high-risk individuals seemed higher than fear of contracting the virus themselves. High levels of loyalty to and trust in state and health authorities were expressed. Medical-related terminology was frequently used, such as the one-meter distance rule, infection tracking, national guidelines, and hand sanitizer, which implies high levels of health literacy. They expressed strong support for online course delivery (mean 4.5) ahead of practical training as a precautionary public health action.
Conclusion: These students did not have high levels of fear of contracting the virus from other students or public transport. They expressed a higher fear of infecting others than being infected themselves. The major implication for the public and the educational system is that students, even in a country with low death rates, support digital education as a public health precautional action to prevent the spread of infection.
Keywords: students, COVID-19, fear, health literacy, public health, education, distance, nurses
Plain Language Summary
- COVID-19 research has revealed fears related to contracting the virus.
- Health, social, and teacher education students may be exposed to the risk of SARS-CoV-2 infection during mandatory practical training in welfare services.
- This mixed methods cross-sectional study was conducted at the beginning of the third wave of infection among unvaccinated professional students in Norway.
- The professional students did not have high levels of fear of contracting the coronavirus from other students and public transport. Their fear of infecting high-risk individuals seemed higher than their fear of contracting the virus themselves.
- Medical-related terminology was frequently used by students, implying a high degree of health literacy.
- High levels of loyalty to and trust in state and health authorities were expressed.
- Based on outliers with high levels of fear, there is a need to explore whether the traditional suitability assessment for professional students will ensure patient safety in the post-pandemic health care.
- Even after one year of partial or total pandemic lockdown, the responders expressed support for online education as a precautionary action as part of public health practice.
Introduction
A cohort study,1 covering the entire Norwegian population during the first and the second waves of the COVID-19 pandemic in Norway, found that health professionals had at least two times higher risk of contracting the virus during the first wave. During the second wave, childcare workers, preschool teachers, and primary school teachers had approximately 1.1–2 times greater odds of being infected. Public transport (bus, streetcar, and taxi) drivers showed up to twice the risk of contracting the virus faced by others of working age in both waves.1 At the end of the second wave, Norway reported few COVID-19-associated deaths and little severe disease as compared to most other countries.2
Confronted with the rising third wave COVID-19 cases, vaccination of high-risk individuals had just begun.3 Neither teachers, health or social care providers nor professional students undergoing their mandatory practical training were vaccinated.4 To attempt halting the third wave, restrictions were tightened on January 4, 2021.3 Some of the precautionary measures were asking people to work and study from their homes. Crowded public transportation was considered a risk factor in transmitting the virus and should thus be avoided. Digital teaching was reintroduced in all upper secondary schools, colleges, and universities.
The COVID-19 disease has been a source of fear globally.5–7 This may be not only a direct result of the virus but also due to lack of preparedness in different parts of the society (such as health care and education), fast spread of the coronavirus, high mortality rates, lack of a treatment and measures taken to prevent its spread.6–8 A systematic review and meta-analysis of the fear of COVID-19 found that the highest and lowest means of fear had been found in Asia and Australia based on continent, and in hospital staff and college students based on target population, respectively.6 There is, however, no universal definition or understanding of fear, or more specifically, of fear of COVID-19, which makes such cross-cultural, cross-gender, and cross-country research difficult.5,9
Infection control guidelines may decrease the spread of infectious disease, but it may also increase fear.10 Fear-based approaches can be effective in preventing diseases; on the other hand, high levels of fear may be negative to health.6,10,11 Fear has a negative relationship with ageing, knowledge about COVID-19, and education level.12 In contrast to science, technology, engineering, and mathematics (STEM) students, health care, social care, and teacher education students’ mandatory practical training in welfare services form a major part of their degree programs. Professional students may therefore have a higher risk of being both potential patients and spreaders of the COVID-19 disease compared with STEM students. On the other hand, well informed and educated students can act as advocates for disease prevention, by talking to others about how to prevent the spread of viruses, and thus reduce fear at a public health level. Previous pandemics has shown that failing to involve stakeholders in decision-making can lead to fear, a lack of trust, and negatively impact morale.11,13
The present study utilizes data from an ongoing interprofessional learning (IPL) study14 among professional students attending nine different Health, Social and Teacher Education study programs at the largest state university in Norway. The students’ perception of health risks to themselves and potential transmission of the virus to persons in high-risk groups may be of importance in the preparedness in higher education for a similar situation as the COVID-19 pandemic. The current student groups were selected because the exposure these students would have had to other students if they had met physically was similar for all students and difficult to ensure if the respondents had been chosen in another manner.
In this mixed methods study, our purpose is to explore the extent to which unvaccinated professional students (according to age and educational background) fear transmission of SARS-CoV-2 from fellow students and from public transportation during the third wave of the COVID-19 pandemic.
Materials and Methods
Design and Sampling
This mixed methods study is based on data from an annual cross-sectional study on students attending a mandatory interprofessional learning (IPL) course delivered on January 4–7, 2021 at Oslo Metropolitan University (OsloMet) in Norway. The study design has been presented previously in details.14–17 In short, undergraduate students participated in the annual IPL seminars, structured as a combination of synchronous group discussions and the use of digital learning materials (used both synchronously and asynchronously) delivered in the learning management system (LMS) Canvas. Digital learning materials were made available through the LMS Canvas prior to the IPL course, according to a flipped classroom approach.18 The IPL course is part of an educational intervention (Interprofessional Interaction with Children and Youth [INTERACT]) and aims to meet the demands for better coordination of services to children, better interaction among professionals, and better cooperation between children/young people and professionals. The IPL course was delivered as a hybrid course in 2019 and 2020, and the deliveries and learning outcomes have been found satisfactory.15,16 Due to the high student volume, it was decided that the course would be fully digitalized in 2021. The student evaluation of the fully digital course delivery will be presented in a separate paper (in preparation).
Participants
The student participants comprised those in the first, second, or third year of a bachelor’s degree in the following education programs: Early Childhood Education, Primary and Lower Secondary Teacher Education, Teacher Education in Art and Design, Physiotherapy, Social Education, Nursing, Social Work, Child Welfare, and Occupational Therapy. The supervisors were recruited from the staff, master’s degree students, and professionals working in the field.16 They represented a wide age range, different educational, work and supervision background.
Online Evaluation Survey
Because the Norwegian government enforced strict measures in the capital city and all higher education institutions on short notice, to take effect on January 4, 2021, the authors designed this study and developed the survey questions during the prior weekend (January 2–3). No pilot test could be performed due to the short time frame. The study questions were fitted to the anonymous self-administered online questionnaires described in a previous study.14 The students and the supervisors were asked the following identical closed-ended questions:
‘If in the current situation, you had to meet physically on campus to take the ILP course in interprofessional groups (not digitally), to what extent would you then be afraid of being infected by the coronavirus … from students attending 1) health care education programs in particular?, 2) social care education programs in particular?, 3) teacher education programs in particular?; 4) other students?, 5) public transport to/from campus? 6) Do you agree that the ILP course in January 2021 is offered digitally (as opposed to at campus) due to the infection pressure? (on a scale of 0–5, where 0 = “completely disagree” and 5 = “completely agree”). ‘Both the students and the supervisors could respond on a 6-point Likert scale (from 0 = “completely disagree” to 5 = “completely agree”).
Both the students and the supervisors were asked this identical open-ended question: “If you wish, please elaborate on your answer regarding physical attendance on campus and the risk of infection in interprofessional student groups.” The responders simply wrote their text answers on a computer or their mobile. The open-ended responses were used to explore and understand the participants’ experiences and perspectives.
Additionally, they were asked about their demographic data (age group and educational background). The student questionnaire was provided as an internet link embedded in the students’ LMS, whereas the supervisor (post) questionnaire was distributed via email. One reminder was sent to increase the response rate.
Data Analysis
Descriptive statistics were used to present the demographic data and the mean, standard error of the mean (SEM), and 95% confidence interval (CI) outcome variables. The analyses were stratified by study programs dichotomized to teacher education programs (Early Childhood Education and Care, Primary and Lower Secondary Teacher Education, and Teacher Education in Art and Design), social care education programs (Social Work and Child Welfare), and health care education programs (Physiotherapy, Mensendieck Physiotherapy, Nursing, and Occupational Therapy), as well as by age, dichotomized to ≤25 or >25 years. Due to the exploratory nature of the study, no adjustment was made for multiple hypothesis testing. Due to the low number of supervisors (n = 32), and heterogenous backgrounds (representing each group and profession, and with a wide age range), we have not carried out statistical analyses for the supervisors’ responses similarly to the students’ responses. Statistical analyses were performed using Microsoft Excel and the Statistical Package for the Social Sciences (SPSS), version 27. The open-ended responses were analyzed by NVivo software using the function autocodes, stop words, word clouds, text search, and word three. Manual coding was also applied to assess thematic saturation. The use of NVIVO was supplemented by the open-ended responses being imported from Excel to Word. Word was used to grouping the text responses into themes, under the headings shown under the results. This implies that only responses relevant to the present study aim, were reported. Only rich quotes relevant to the present aim are presented verbatim in this paper; the rest of the responses are paraphrased here. Quotes are presented together with data on student number (nr), age category, major, and year of study.
Ethics
The Ethical Guidelines for Research at OsloMet were followed.19 According to the criteria of the Norwegian Centre for Research Data (NSD),20 the study was considered completely anonymous, with no sociodemographic information beyond the participants’ age and gender, and thus not subject to reporting requirements (NSD reference number 741,649). The data were collected from an anonymous online survey using Nettskjema,21 in line with ethical guidelines.19 All the participants were over 18 years old and received written information about the study beforehand on LMS Canvas. The respondents’ voluntary participation and anonymity were emphasized, and they were informed about the study’s purpose and how the data would be used. The participants informed consent included publication of anonymized responses. Answering the questionnaire was considered informed consent to participate. The study complies with the Declaration of Helsinki.
Results
Demographic Characteristics
The response rate was 49.6% (Table 1). Among all participating students, 38%, 19%, and 43% were enrolled in health care, social care, and teacher education programs, respectively. Approximately 2/3 of the students were aged 25 or younger.
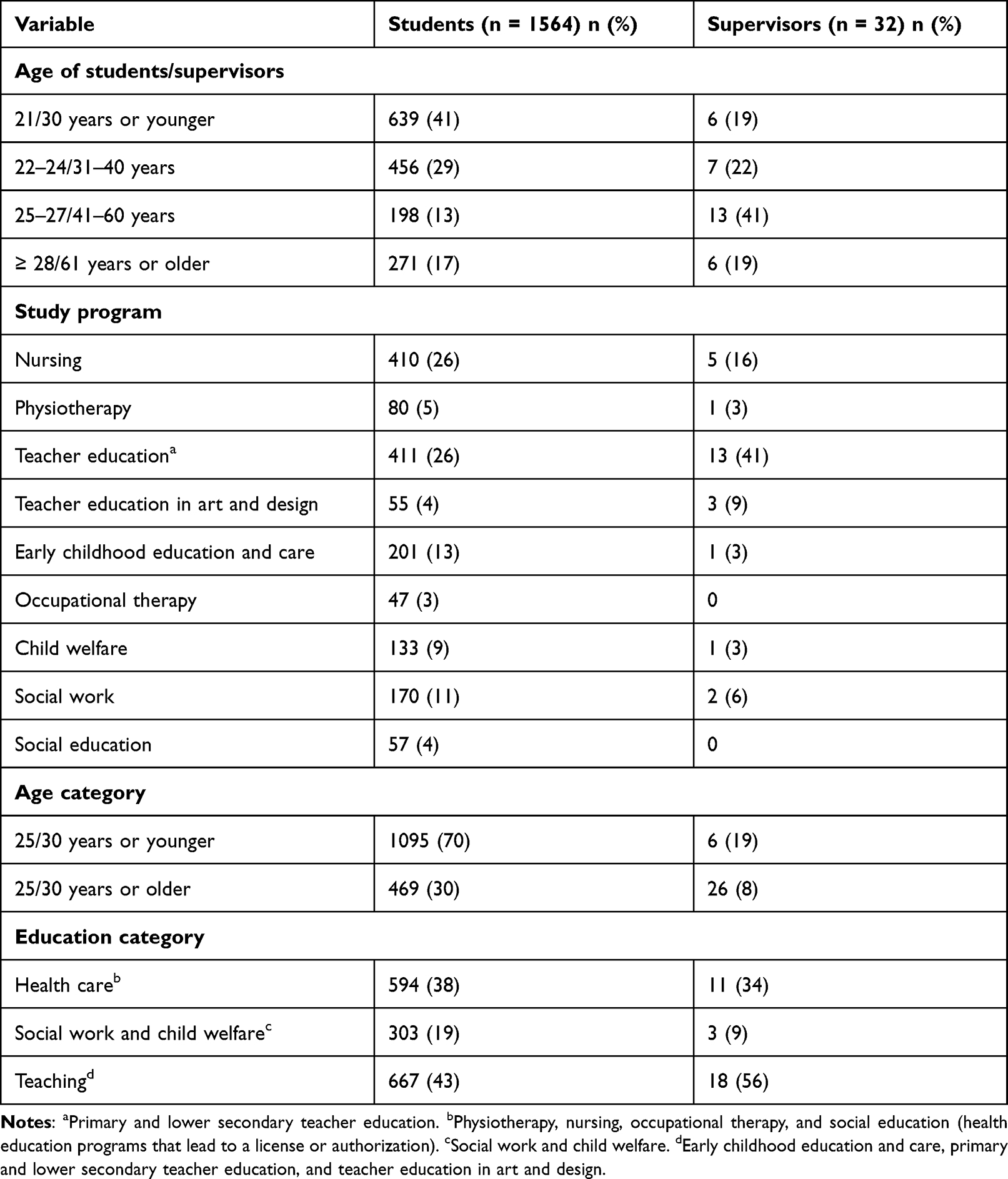 |
Table 1 Characteristics of Students in a Large-Scale Blended Interprofessional Learning Course Delivered in 2019 (Post-2019) and in 2020 (Pre- and Post-2020). Numbers are Stated as Frequencies and Percentages |
More than half of the supervisors (n = 32, 65% response rate) were educated as teachers or child welfare service providers, and 65% were aged 41 or older.
Students
Regarding the fear of transmission from other students and from public transport, the means were around 3 (on a scale of 0–5) (Table 2), and the CIs overlapped. When stratified by educational background, the students showed no differences in their fear of transmission from other students or from public transport. Accordingly, none of the differences among the groups is statistically significant.
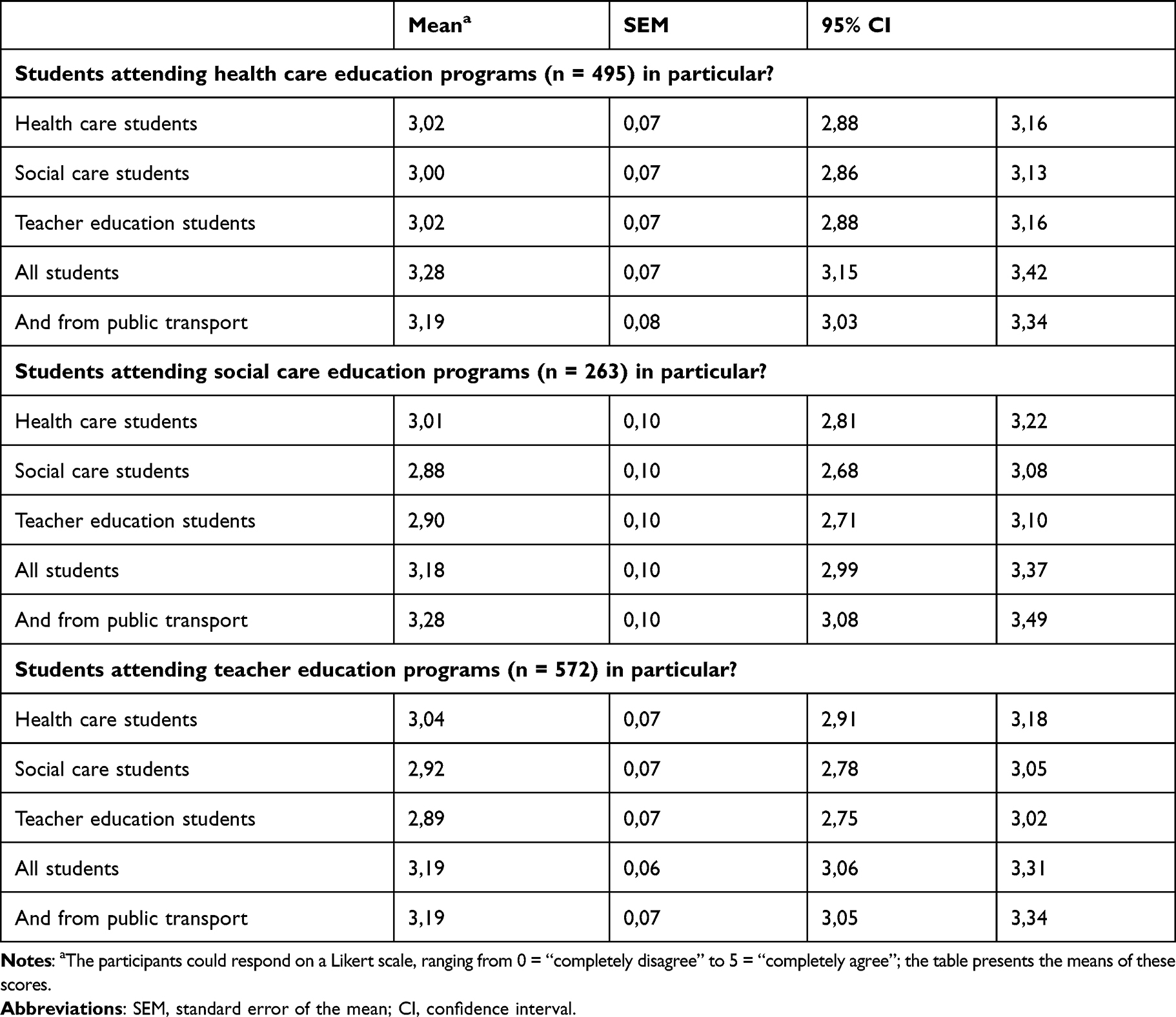 |
Table 2 Stratified by Education: If in the Current Situation, You Had to Meet Physically on Campus to Take the Mandatory Interprofessional Course (Not Digitally), to What Extent Would You Then Be Afraid of Being Infected by the Coronavirus from |
Regarding the means, only the students aged 25 or younger had a slightly but not significantly higher fear of transmission from other students (Table 3). No differences were found when the students were stratified by academic-year level (data not shown).
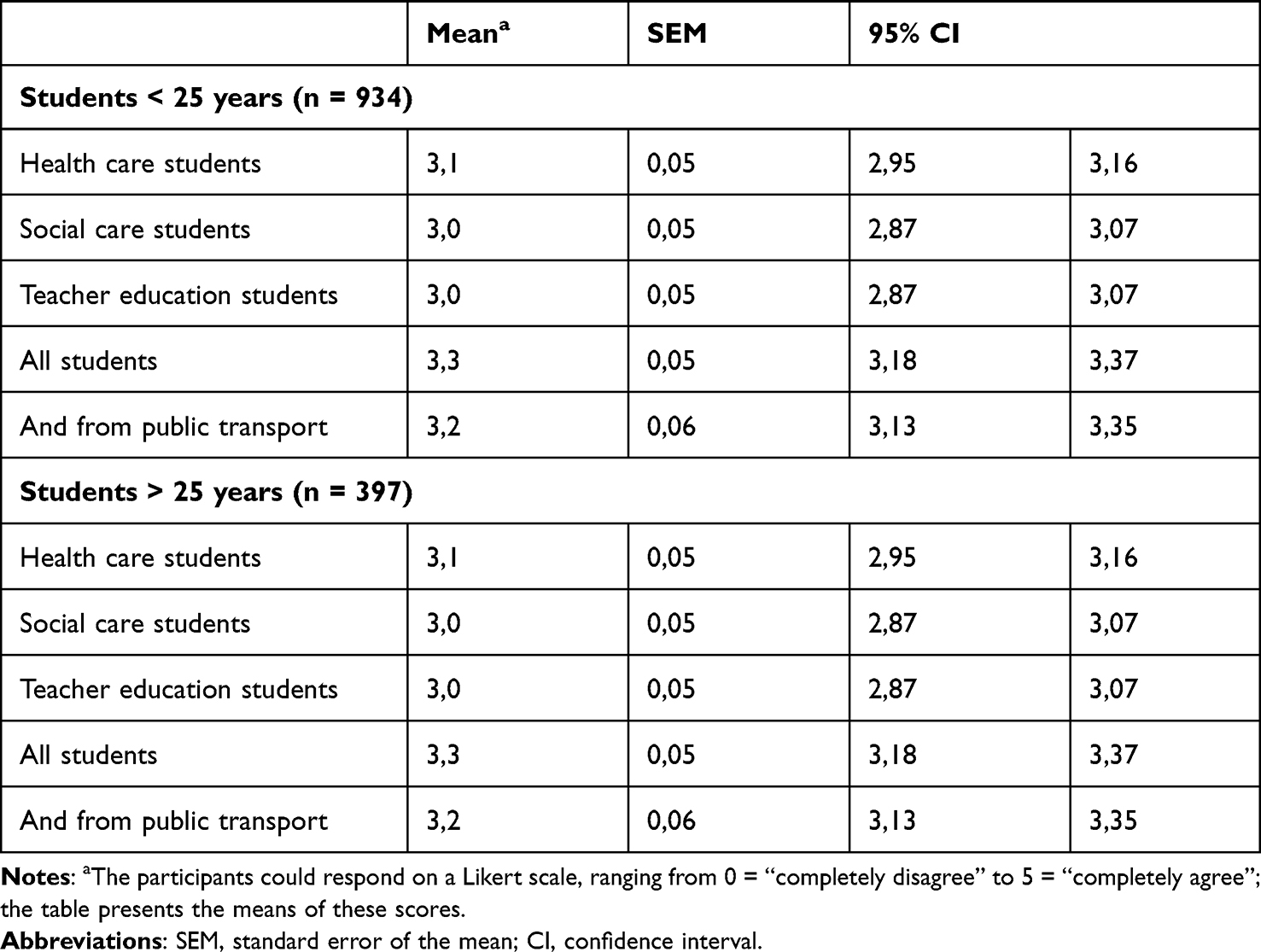 |
Table 3 Stratified by Age: If in the Current Situation, You Had to Meet Physically on Campus to Take the Mandatory Interprofessional Course (Not Digitally), to What Extent Would You Then Be Afraid of Being Infected by the Coronavirus from |
The results shown in Tables 2 and 3 indicate that neither age nor educational background affected the students’ fear of becoming infected from fellow students and, thus, indicate that, in a future similar situation, the need for distinguishing the students according to age and educational programme is probably neglectable.
Most of the students completely agreed (score of 4 or 5) on the digital course delivery, instead of the on-campus delivery (Table 4). The support for digital delivery was slightly higher among the teacher education students than among the health care and the social science students; however, all CIs overlapped.
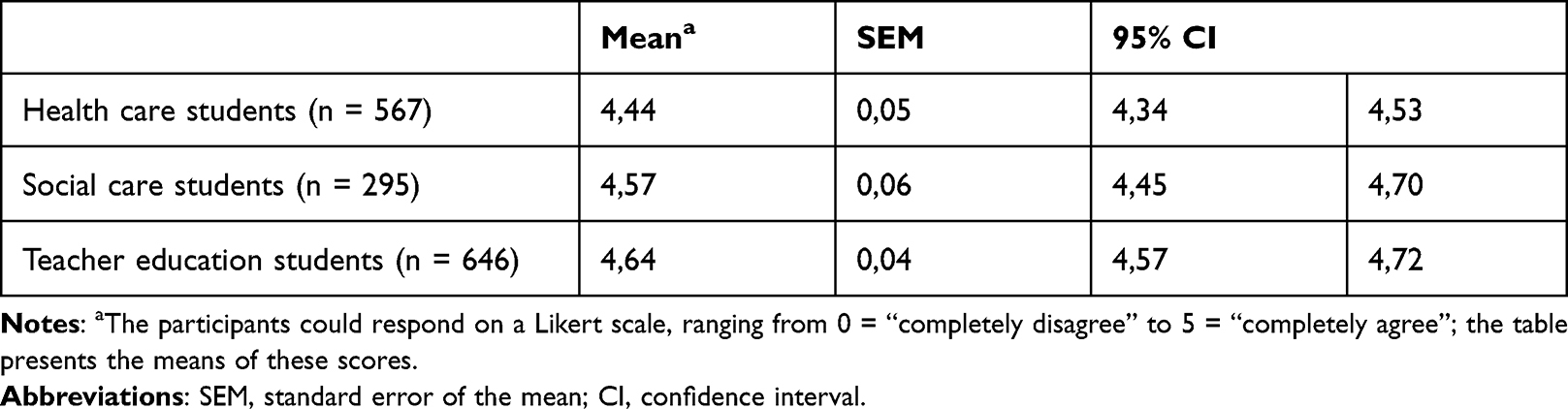 |
Table 4 Do You Agree That the Interprofessional Learning Course in 2021 is Offered Digitally (as Opposed to at Campus) Due to the Infection Pressure? (on a Scale of 0–5, Where 0 = “Completely Disagree” and 5 = “Completely Agree”) |
The students were invited to elaborate on their answers concerning physical education and risk of infection in an open question (“If you wish, please elaborate on your answer regarding physical attendance on campus and the risk of infection in interprofessional student groups.”). The following main themes were identified from the 176 students who responded:
Loyalty and trust (80).
Fear of contracting Covid 19 (27).
Fear of transmitting COVID-19 to high-risk individuals (8).
Challenges with digital IPL activities (23).
In addition,10 students reported preference for digital IPL, and 28 students provide comments that did not fit into any of the five categories. Some of the comments could be classified in more than one of the five categories. In such cases, the main theme of the comment was used to assign the comment.
Loyalty and Trust
The students expressed high levels of loyalty to and trust in the Norwegian government, the Norwegian Directorate of Health, and the Norwegian Institute of Public Health. The terminology communicated by the state authorities as part of the official news and press releases (eg, 1-meter distance rule, infection tracking, infection control, national guidelines, fines, voluntary work, hand sanitizer, and cohort) was frequently used. One student said:
There is a good reason why the government has introduced digital education after Christmas. If all students who have traveled during Christmas were to gather on campus for two days in close collaboration and then meet other students in their own programs afterwards, the virus could possibly spread quickly (nr. 121, age category: 20–24 years, second year student, Teacher Education.)
The students expressed a high level of general trust in all student groups. Some students strongly opposed to the idea that students pursuing other professions could pose a higher risk of spreading the virus than others, represented by these two quotes:
I think that all students are equally responsible and that everyone knows the rules so that everyone has worn a face mask or at least kept more than 1-meter distance from each other. (nr. 43, age category: 21 years or younger, first year student, Nursing)
I do not think that the risk is directly greater because you collaborate across education programs and student groups, but the risk increases based on how many people are together. (nr. 29, age category: 21 years of younger, first year student, Social Education)
Some students also expressed the opinion that the measures were too restrictive and provided that the infection-control measures were followed, they had no fear of COVID-19. Two students explained:
On a general basis, I think that the restrictions around COVID-19 are too strict according to the costs they entail socially, financially, psychologically, and obviously in the form of a reduced teaching offer for students at OsloMet. (nr. 31, age category: 28 years or older, first year student, Teacher Education)
If you relate to small groups and keep your distance, I think that meeting physically would have been OK. (nr. 161, age category: 25–27 years, third year student, Early Childhood Education and Care)
A high level of trust and loyalty was overall reflected also in the responses that included public transport. A high number of passersby and dense crowds using public transportation were highlighted as unnecessary risks when the infection pressure in the capital was high, as illustrated in these quotes:
Even though the infection control routines on campus are excellent, that isn’t necessarily so in public transport. (nr. 139, age category: 22–24 years, third year student, Child Welfare)
On the other hand, I think that it would have been wrong to take public transport because then you increase the pressure and the risk of infection there – and there may have been people from societally beneficial functions who also take the same public transport. (nr. 176, age category: 22–24 years, third year student, Occupational Therapy)
The loyalty and trust were also expressed through dilemmas. The students preferred on-campus activities but accepted the digital IPL course delivery due to the pandemic. They considered it safe to meet physically in the small IPL groups on campus but felt that public transport should be avoided due to the crowd of strangers.
Fear of Contracting Covid-19
Although fear of contracting the Covid-19 virus was not predominant among the students, some students elaborated on fear of becoming infected. One student said:
I am not worried about one particular group of students passing on the virus. I am worried about contraction the virus form anyone. (nr. 68, age 22–24 years, first year student, Early Childhood Education and Care)
Another student said:
I would not have attended if we were to meet physically. (nr. 20, age category 22–24 years, first year student, Social Work)
Fear of COVID-19 to High-Risk Individuals
Although they were not afraid of being infected themselves, they did not want to infect others. One student said:
I’m not afraid of being infected, but I’m afraid I’ll infect someone who may become seriously ill. (nr. 145, age category: 25–27 years, third year student, Social Work)
Some students were worried because they had next-of-kin in high-risk groups or were high-risk individuals themselves. The high infection levels in the capital city of Oslo and the lack of social distancing due to crowding (both on campus and in public transportation) were repeated in the responses, as illustrated in these quotes:
I’m not afraid of infection from any of the professions but from young people who have stayed indoors for a year. (nr. 131, age category: 22–24 years, second year student, Teacher Education)
Personally, I am not afraid of being infected with corona, but for the sake of other students, my own family, and especially vulnerable groups, the only right thing to do is to carry out [the course delivery] digitally as much as possible, as the situation is now. (nr. 74, age category: 28 years or older, first year student, Child Welfare)
Challenges with Digital IPL Activities
Although not explicitly asked, some unsolicited students stated that in-person education provided higher learning outcomes, higher motivation, and less physical challenges than digital education. Online supervision was also mentioned as inferior to face-to-face supervision on campus. One student recounted:
Physical attendance would have made a big difference because then we would have had more guidance, someone to be able to ask questions more impulsively, not demand so much from the participants. We would also have learned more if a person had talked about interprofessional collaboration rather than watching videos. Since we could not watch the videos together due to technical errors, then the seminar felt as individual work that we had to carry out and then present our opinions to the student group. (nr. 22, age category: 21 years or younger, first year student, Teacher Education)
Some students commented that it was more difficult to get to know new peers from other education programs online compared with face-to-face meetings on campus. Others cited the group dynamics as better in the virtual group work than in face-to-face settings. One student said:
Now everyone could see one another, and everyone got to talk; last year, a few students dominated the group, and the rest were present just because they had to be. (nr. 127, age category: 21 years or younger, second year student, Teacher Education)
Supervisors
The supervisors consisted of 32 persons with very different backgrounds (educational and work experience) and age.
Regarding fear of transmission from health care students, social care students, teacher education students, and all students, as well as from public transport, 59%, 53%, 53%, 81%, and 81% of the supervisors, respectively, all supervisors answered with scores of 3–5. Nearly all (97%) agreed on the digital delivery instead of the on-campus delivery (only scores between 3 and 5) (data not shown due to the low number of supervisors). None of the supervisors used the scores 0 or 2.
Of the 32 supervisors, 9 (28%) answered the open-ended question regarding the course delivery mode. The supervisors agreed about the digital IPL course delivery with reference to the authorities, students’ possible fear of infection, and higher course sustainability due to the high student volume. Two supervisors said that infection control was not discussed during their supervision. Some supervisors noted that although the digital delivery went well, meeting people face-to-face was also fine. There was a dilemma between the fear of infection when meeting face-to-face and the burden of being unable to meet physically on campus. Two supervisors thought that the delivery could have been face-to-face on campus:
I think that meeting physically with 8 people would be fine if a separate area for each group had been accepted by everyone. (nr. 17, age category 41–60 years, Teacher Education)
I find that students are not very worried about infection. That’s understandable to me. (nr. 29, age category: 61 years or older, Teacher Education)
Discussion
The students in our study did not have high levels of fear of being infected by the coronavirus. Their fear of infecting high-risk individuals seemed higher than their fear of being infected themselves. The qualitative responses are suggestive of not only high levels of loyalty to and trust in the authorities but also high levels of health literacy. The major implication of this study for higher education is that these professional students strongly support digital education as a public health precautional action to prevent spread of infection.
Our data are in accordance with the results from a large Norwegian national survey among Norwegian students.22 In general, a low proportion (16%) of the students worried about being infected themselves. However, 40% of the students worried that someone in their immediate family would be infected.22 Our data are also consistent with the results of a survey among 71,000 adult Norwegians in the autumn of 2020, showing that 72% had confidence in the pandemic-related information provided by the government.23 Similarly, in that survey, 74% responded that they trusted the information provided by health authorities.23 The present data also confirm the results of a survey among Norwegian adolescents during the first wave, in which almost half (49%) were satisfied or very satisfied with the information provided about COVID-19, 12% were dissatisfied or very dissatisfied, and 39% were neither satisfied nor dissatisfied.24 The majority (52%) were not concerned about becoming infected with COVID-19.24 In another study among adolescents during the first wave in an urban area of Norway, only 7% worried about becoming infected, while 53% worried about infection among their family members.25 The Norwegian strategy aims to be based on transparency, and in this context, confidence is earned through openness.26
At the onset of the third wave of the pandemic in Norway, public transportation had to be avoided.3 One study comparing Norway and Austria found a negative impact on public transportation during both the first and the second waves of the pandemic, with less patronage loss in Norway.27 Our study’s results, with data from the third wave, support the conclusion of the cited study,27 suggesting a “fresh-fear” effect27,28 during the first wave. In Taiwan, the outbreaks of the SARS epidemic in 2003 resulted in an unprecedented reduction in the use of public transport.28
It appeared that the students linked the risk of infection to a slightly greater extent to contact with peers (STEM students) other than fellow professional students and to the use of public transport to and from campus. The difference, which is admittedly small and uncertain, can be attributed to the perceived higher risks of taking public transport to and from the university, as well as mingling with strangers on campus, than meeting other university students in small IPL groups on campus.
The dilemma about the risk of becoming infected when meeting face-to-face versus the burden of being unable to meet physically on campus was also expressed. Studies have shown negative consequences of working or studying from the home office.4,22,29–32 Some studies have reported that students experience a reduced quality of life, academic stress, financial insecurity, and increased levels of physical problems during the pandemic.22,25,30,33–36. Blended learning on campus, according to the flipped classroom model, was implemented in most Norwegian universities’ during the autumn 2020. Confronted with the rising third wave of COVID-19 cases, we did not know if students with high levels of fear (fear for oneself and fear for infecting others) would choose not to attend courses on campus even at a slightly elevated risk level, thus neither learning their curriculum well, nor working-life relevant coping strategies and problem solving in times of crisis. A scoping review of studies on different groups in populations from other parts of the world, with data collected from the first wave of the pandemic, found that females were at higher risk of the fear of COVID-19 infection.7 We did not ask the respondents to indicate their gender because of the low number of male students in some of the education programs included in this study. For ethical reasons, we could not ask the students explicitly about their private lives or other sensitive questions.
Although the health care students in our study probably had a higher level of medical knowledge than the other students,37,38 the responses were similar across educational groups. Overall, health literacy was probably high among these students compared with that of a large and representative sample of the Norwegian population39 and possibly, compared with the participants studied in a scoping review including studies from very different countries and settings.7
Studies on the fear of transmission, designed to target the first outbreaks of the pandemic,7,9,29,33–36,38,40–45 might have stronger impacts due to the “fresh-fear” effect compared with studies capturing subsequent waves.28 Additionally, the results of studies using headings that included words such as “fear” (eg, the “Fear of COVID-19 Questionnaire”5) may not be comparable to studies using more neutral wordings, such as that used in the present study. Moreover, a study investigating “The Fear of COVID-19 Scale” across 48 countries found the scale suitable for cross-cultural research but limited when examining correlates and predictors of fear of COVID-19.5
A higher fear of infecting high-risk individuals than their fear of being infected themselves was also found by other studies.9,22 One year into COVID-19 education disruption, these students still agreed to digital IPL delivery due to the high infection pressure. Nonetheless, a few of the students in our study did express high levels of fear. A student posing a potential danger to the lives, physical and mental health, rights and safety of kindergarten children and pupils or patients, clients, and users is unsuitable for the profession.46 The advice and imposed actions due to the pandemic might exacerbate the problems experienced by people with a preexisting anxiety-related disorder.8 From meta studies it has been found that the fear of COVID-19 is associated with a wide range of mental health problems among the general population.47 The pandemic will most probably induce a change in professional education, with a permanent rise in distance learning and digital multidisciplinary collaboration. Educators are not trained to evaluate students’ suitability in the context of new future scenarios that may arise due to changes in higher education, or in the society. There is a need to explore whether the traditional suitability assessments for professional students46 will ensure patient safety in the post-pandemic health care.
These students were young adults in the second year of the pandemic, with their education disrupted. The study indicated that students adapted quickly to the regulations and stayed loyal to them even though it affected their everyday life, which is also found by others.48 Fear of COVID-19 can be modulated through governments’ public policies, such as precautionary actions as part of public health practice,13,49,50 and by providing effective training programs for different populations.6 Higher education must follow regulations and deliver education with high learning outcome and high quality, even during lockdown due to the COVID-19. Delivering safe education through precautional actions. such as delivering online IPL courses during the pandemic, requires many considerations but may contribute to reducing infection pressure and 1maintaining public health, and hopefully also moderate levels of fear.49,50
Limitations and Strengths
When the presented data were collected, Norway was in the beginning of the third wave of the Covid-19 pandemic and the inhabitants were plunged back into strict preventive measures.3 Self-selection bias cannot be excluded, as participants with strong opinions in either direction might have responded, yet the diversity of our sample enhances the robustness of our findings. If participants with strong opinions responded (both directions), then the average was not affected. One limitation is using a questionnaire which was not pre-tested or validated in the studied population prior to use. However, due to time constraints following the lockdown due to the third wave, it was not possible to perform pre-testing or validation of the instruments used in the present study. The data was collected because the researchers seized the opportunity to add the present study as an addition to an ongoing questionnaire survey.14,17 Retrospectively, we realize that the closed-ended question about “all other students” was unclear on whether it should be interpreted as “other than myself” or “other than the three groups mentioned above” (ie, students who were not required to meet physically at their practicum places and thus, might have a higher risk of being infected than those only working from their home office). Nevertheless, regardless of the interpretation, we do not think that this affects our findings. Some students may not depend on public transport because they either live close to the campus or have access to a car. If these students answered with a score of 0 or did not answer at all, an underestimation might have occurred. The response rates were higher than in those of our cross-sectional studies before the pandemic, 14–16 and also higher than the response rates in the national student survey in Norway (Studiebarometeret) among 74000 Norwegian students, which was 44% in 2020 and 41% in 2021.51 Although the low response rate, which was in line with a declining response rate for surveys in general, might threaten the validity and generalizability of the results, a high response rate does not guarantee sample quality.
Our study’s major strengths include the anonymous data collection, the large sample size, the different educational backgrounds of the participants, and the mixed-method design. The combined use of both closed and open questions in a mixed methods design enabled different perspectives to be captured and adds strength to the study. Regarding the supervisors, although their sample size is too small to draw any reliable conclusions, their responses were similar to the student responses. The fact that the responses to the open questions were in line with the scores on the closed questions lends credibility to our results.
Future Studies
The scoping review found that health care workers, women, younger adults, divorcees, urban residents, those with mental health problems, and so on, had an increased risk of fear at the beginning of the pandemic.7 However, the included studies are based on different population groups globally that are very different from the students in our study. The low mortality rate in Norway compared with many other countries26,44,52 may have influenced the present responses, and future studies should compare countries with high and low death rates. Although no universal definition or understanding of fear exists, predictors of fear of the coronavirus in the general population were previously found to be health anxiety, regular media use, social media use, and risks for loved ones in one study with data collected from the beginning of the pandemic.9 We suggest an approach using open-ended responses in qualitative interviews to obtain knowledge and understanding about the topic of the fear of COVID-19 among professional students in future studies.
Conclusion
Unvaccinated professional students did not report high levels of fear of infection from fellow students or fellow passengers using public transportation at the beginning of the third wave of the pandemic. They seemed more worried that someone in their immediate family or high-risk individuals would be infected with COVID-19 than being infected themselves. The findings support high levels of loyalty to and trust in the government and governmental institutions. The results from this mixed methods study did not vary with age and educational background. The major implication of the current study for the public and the educational system is that students, even in a rich country with low death rate, support digital education as a public health precautional action to prevent spread of infection.
Acknowledgments
First and foremost, we thank the participants. We also express our gratitude to the academic and the administrative staff at Oslo Metropolitan University for their contributions to this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Magnusson K, Nygård K, Methi F, Vold L, Telle K. Occupational risk of COVID-19 in the first versus second epidemic wave in Norway, 2020. Eurosurveillance. 2021;26(40):2001875. doi:10.2807/1560-7917.ES.2021.26.40.2001875
2. Coronavirus cases. Reported cases and deaths by country or territory. Worldometer COVID-19 data. Available from: https://www.worldometers.info/coronavirus/?utm_campaign=homeAdUOA?Si.
3. Norwegian Ministries. Timeline: news from Norwegian Ministries about the coronavirus disease covid-19; 2022. Available from: https://www.regjeringen.no/en/topics/koronavirus-covid-19/timeline-for-news-from-norwegian-ministries-about-the-coronavirus-disease-covid-19/id2692402/.
4. Norwegian Institute of Public Health. Coronavirus – facts, advice and measures. Available from: https://www.fhi.no/en/op/novel-coronavirus-facts-advice/?chapter=89992.
5. Sawicki AJ, Żemojtel-Piotrowska M, Balcerowska JM, et al. The fear of COVID-19 scale: its structure and measurement invariance across 48 countries. Psychol Assess. 2022;34(3):294–310. doi:10.1037/pas0001102
6. Luo F, Ghanei Gheshlagh R, Dalvand S, Saedmoucheshi S, Li Q. Systematic review and meta-analysis of fear of COVID-19. Systematic review. Front Psychol. 2021;12. doi:10.3389/fpsyg.2021.661078
7. Quadros S, Garg S, Ranjan R, Vijayasarathi G, Mamun MA. Fear of COVID 19 infection across different cohorts: a scoping review. Front Psychiatry. 2021;12. doi:10.3389/fpsyt.2021.708430
8. Shafran R, Rachman S, Whittal M, Radomsky A, Coughtrey A. Fear and anxiety in COVID-19: preexisting anxiety disorders. Cogn Behav Pract. 2021;28(4):459–467. doi:10.1016/j.cbpra.2021.03.003
9. Mertens G, Gerritsen L, Duijndam S, Salemink E, Engelhard IM. Fear of the coronavirus (COVID-19): predictors in an online study conducted in March 2020. J Anxiety Disord. 2020;74:102258. doi:10.1016/j.janxdis.2020.102258
10. Demirtaş-Madran HA. Accepting restrictions and compliance with recommended preventive behaviors for COVID-19: a discussion based on the key approaches and current research on fear appeals. Front Psychol. 2021;12:558437. doi:10.3389/fpsyg.2021.558437
11. Stolow JA, Moses LM, Lederer AM, Carter R. How fear appeal approaches in COVID-19 health communication may be harming the global community. Health Educ Behav. 2020;47(4):531–535. doi:10.1177/1090198120935073
12. Cerda AA, García LY. Factors explaining the fear of being infected with COVID-19. Health Expect. 2022;25(2):506–512. doi:10.1111/hex.13274
13. Crosby L, Crosby E. Applying the precautionary principle to personal protective equipment (PPE) guidance during the COVID-19 pandemic: did we learn the lessons of SARS? Can J Anaesth. 2020;67(10):1327–1332. doi:10.1007/s12630-020-01760-y
14. Almendingen K, Šaltytė Benth J, Molin M. Large scale blended learning design in an interprofessional undergraduate course in Norway: context description and supervisors’ perspective. MedEdPublish. 2021;10(1). doi:10.15694/mep.2021.000162.1
15. Almendingen K, Molin M, Šaltytė Benth J. Large-scale blended learning design in an undergraduate interprofessional course in Norway: students’ perspectives from an exploratory study. J Res Interprof Pract Educ. 2021;11(1):1–26. doi:10.22230/jripe.2021v11n1a319
16. Almendingen K, Nilsen B, Kvarme L, Saltyte Benth J. Core competencies for interprofessional collaborative practice among teacher education, health and social care students in a large scaled blended learning course. J Multidiscip Healthc. 2021;14:2249–2260. doi:10.2147/JMDH.S325086
17. Foss C, Guldbrandsen LM, Løndal K, Ulleberg I, Ødegaard NB, Øien I. Constructing Interprofessional Education: the case of INTERACT (Interprofessional Interaction with Children and Youth). presented at: its 21 4th conference on interdisciplinary teamwork skills for the 21st century; 2018. Available from: https://www.ntnu.no/videre/konferanse/Its21/abstractbook.pdf.
18. Evans L, Vanden Bosch ML, Harrington S, Schoofs N, Coviak C. Flipping the classroom in health care higher education: a systematic review. Nurse Educ. 2019;44(2):74–78. doi:10.1097/nne.0000000000000554
19. Oslo Metropolitan University (OsloMet). Ethical guidelines for research at Oslo Metropolitan University (OsloMet). Available from: https://ansatt.oslomet.no/documents/585743/53632647/Ethical+Guidelines+for+Reserach+at+OsloMet/3dccee65-e17e-04f6-34d3-a8e58f280c88.
20. Database for statistics on higher education (DBH). Available from: https://dbh.nsd.uib.no/statistikk/rapport.action?visningId=234&visKode=false&admdebug=false&columns=arstall!8!finmodkode&index=1&formel=999&hier=insttype!9!instkode!9!progkode!9!emnekode&sti=¶m=arstall%3D2020!9!Semester%3D3!9!dep_id%3D1!9!nivakode%3DB3!8!B4!8!HK!8!YU!8!AR!8!LN!8!M2!8!ME!8!MX!8!HN!8!M5!8!PR.
21. Nettskjema. University of Oslo. Available from: https://www.uio.no/english/services/it/adm-services/nettskjema/.
22. Sivertsen B. Studentenes Helse- og Trivselsundersøkelse (SHoT).Tilleggsundersøkelse 2021; 2021. Available from: https://tidliginnsats.forebygging.no/globalassets/shot_rapport2021.pdf.
23. Norsk koronamonitor S. Høy tillit til myndighetene. Available from: https://opinion.no/2020/11/hoy-tillit-til-myndighetene/.
24. Kaiser S, Kyrrestad H, Martinussen M. Adolescents’ experiences of the information they received about the coronavirus (Covid-19) in Norway: a cross-sectional study. Child Adolesc Psychiatry Ment Health. 2021;15(1):30. doi:10.1186/s13034-021-00384-4
25. Lehmann S, Skogen JC, Haug E, et al. Perceived consequences and worries among youth in Norway during the COVID-19 pandemic lockdown. Scand J Public Health. 2021;49:1403494821993714.
26. Brean A. Openness and trust. Tidsskr nor Laegeforen. 2020;140(18). doi:10.4045/tidsskr.20.0997
27. Rasca S, Markvica K, Ivanschitz BP. Impacts of COVID-19 and pandemic control measures on public transport ridership in European urban areas – the cases of Vienna, Innsbruck, Oslo, and Agder. Transp Res Interdiscip Perspect. 2021;10:100376. doi:10.1016/j.trip.2021.100376
28. Wang K-Y. How change of public transportation usage reveals fear of the SARS virus in a city. PLoS One. 2014;9(3):e89405. doi:10.1371/journal.pone.0089405
29. Almendingen K, Morseth MS, Gjølstad E, Brevik A, Tørris C. Student’s experiences with online teaching following COVID-19 lockdown: a mixed methods explorative study. PLoS One. 2021;16(8):e0250378. doi:10.1371/journal.pone.0250378
30. Fretheim A, Helleve A, Løyland B, et al. Relationship between teaching modality and COVID-19, well-being, and teaching satisfaction (Campus & Corona): a cohort study among students in higher education. medRxiv. 2021;2021:21254388. doi:10.1101/2021.03.26.21254388
31. Nicola M, Alsafi Z, Sohrabi C, et al. The socio-economic implications of the coronavirus pandemic (COVID-19): a review. Int J Surg. 2020;78:185–193. doi:10.1016/j.ijsu.2020.04.018
32. Sahu P. Closure of universities due to coronavirus disease 2019 (COVID-19): impact on education and mental health of students and academic staff. Cureus. 2020;12(4):e7541–e7541. doi:10.7759/cureus.7541
33. Beisland EG, Gjeilo KH, Andersen JR, et al. Quality of life and fear of COVID-19 in 2600 baccalaureate nursing students at five universities: a cross-sectional study. Health Qual Life Outcomes. 2021;19(1):198. doi:10.1186/s12955-021-01837-2
34. Van de Velde S, Buffel V, van der Heijde C, et al. Depressive symptoms in higher education students during the first wave of the COVID-19 pandemic. An examination of the association with various social risk factors across multiple high- and middle-income countries. SSM Popul Health. 2021;16:100936. doi:10.1016/j.ssmph.2021.100936
35. Studiebarometeret 2020 –Hovedtendenser Studiebarometeret 2020; 2021. Available from: https://docplayer.me/203118062-Rapport-studiebarometeret-2020-hovedtendenser.html.
36. Solberg E, Hovdhaugen E, Gulbrandsen M, Scordato L, Svartefoss SM, Eide T. Et akademisk annerledesår Konsekvenser og håndtering av koronapandemien ved norske universiteter og høgskoler; 2021. Available from: https://nifu.brage.unit.no/nifu-xmlui/bitstream/handle/11250/2737339/NIFUrapport2021-9.pdf?sequence=4&isAllowed=y.
37. Grüner S, Krüger F. Infodemics:Do healthcare professionals detect Corona-related false news stories better than students? PLoS One. 2021;16(3):e0247517. doi:10.1371/journal.pone.0247517
38. Ikhlaq A, Bint-E-Riaz H, Bashir I, Ijaz F. Awareness and attitude of undergraduate medical students towards 2019-novel corona virus. Pak J Med Sci. 2020;36(S4):S32–S36. doi:10.12669/pjms.36.COVID19-S4.2636
39. Le C, Finbråten HS, Pettersen KS, Joranger P, Guttersrud Ø. Health literacy in the Norwegian population. English summary; 2021. Available from: https://www.helsedirektoratet.no/rapporter/befolkningens-helsekompetanse/Health%20Literacy%20in%20the%20Norwegian%20Population.%20English%20summary.pdf/_/attachment/inline/a08fec5e-16c7-435e-abf8-e2f0ba05cc84:c576b33bcd3eb386c58124a817bc3b01fde33df8/Health%20Literacy%20in%20the%20Norwegian%20Population.%20English%20summary.pdf.
40. Berge LI, Gedde MH, Husebo BS, Erdal A, Kjellstadli C, Vahia IV. Age and emotional distress during COVID-19: findings from two waves of the Norwegian citizen panel. Int J Environ Res Public Health. 2021;18(18):9568. doi:10.3390/ijerph18189568
41. Bjørknes R, Sandal GM, Mæland S, Haug E, Lehmann S. ‘We are unlikely to return to the same world, and I do not want it to destroy my future.’ Young people’s worries through the outbreak of the COVID-19 pandemic. Child Fam Soc Work. 2022;27:246–253. doi:10.1111/cfs.12878
42. Burdzovic Andreas J, Brunborg GS. Self-reported mental and physical health among Norwegian adolescents before and during the COVID-19 pandemic. JAMA Network Open. 2021;4(8):e2121934–e2121934. doi:10.1001/jamanetworkopen.2021.21934
43. Afshin A, Sur PJ, Fay KA, et al. Health effects of dietary risks in 195 countries, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2019;393(10184):1958–1972. doi:10.1016/S0140-6736(19)30041-8
44. Harris SM, Sandal GM. COVID-19 and psychological distress in Norway: the role of trust in the healthcare system. Scand J Public Health. 2021;49(1):96–103. doi:10.1177/1403494820971512
45. Myhr A, Naper LR, Samarawickrema I, Vesterbekkmo RK. Impact of COVID-19 pandemic lockdown on mental well-being of Norwegian adolescents during the first wave—socioeconomic position and gender differences original research. Front Public Health. 2021;9(1331). doi:10.3389/fpubh.2021.717747
46. Oslo Metropolitian University. Suitability assessment. Oslo Metropolitian University. Available from: https://minside.oslomet.no/en/web/student/suitability-assessment.
47. Şimşir Z, Koç H, Seki T, Griffiths MD. The relationship between fear of COVID-19 and mental health problems: a meta-analysis. Death Stud. 2021;1–9. doi:10.1080/07481187.2021.1889097
48. Prati G, Mancini AD. The psychological impact of COVID-19 pandemic lockdowns: a review and meta-analysis of longitudinal studies and natural experiments. Psychol Med. 2021;51(2):201–211. doi:10.1017/S0033291721000015
49. Goldstein BD. The precautionary principle also applies to public health actions. Am J Public Health. 2001;91(9):1358–1361. doi:10.2105/ajph.91.9.1358
50. Martuzzi M, Tickner JA; World Health Organization. The Precautionary Principle: Protecting Public Health, the Environment and the Future of Our Children. Regional Office for Europe: World Health Organization; 2004.
51. Studiebarometeret 2020 –Hovedtendenser. In Norwegian. Available from: https://www.nokut.no/globalassets/studiebarometeret/2021/hoyere-utdanning/studiebarometeret-2020_hovedtendenser_1-2021.pdf.
52. Askim J, Bergström T. Between lockdown and calm down. Comparing the COVID-19 responses of Norway and Sweden. Local Gov Stud. 2021;1–21. doi:10.1080/03003930.2021.1964477
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.