Back to Journals » International Journal of Women's Health » Volume 18
MRI-Based Classification Systems Combined with Serum CA125 for Predicting Symptom Recurrence After Ultrasound-Guided High-Intensity Focused Ultrasound Ablation Surgery for Adenomyosis: A Retrospective Cohort Study
Authors Tang Y, Tian HD, Chen XM, Wang H, Shen LM, Ni SQ ![]() , Su B, Jiang ZJ, Zhu LJ, Luo YX, Shi Q
, Su B, Jiang ZJ, Zhu LJ, Luo YX, Shi Q ![]()
Received 19 October 2025
Accepted for publication 30 March 2026
Published 17 April 2026 Volume 2026:18 575413
DOI https://doi.org/10.2147/IJWH.S575413
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Vinay Kumar
Ying Tang,1,2,* Hua-Dong Tian,1,* Xiao-Mei Chen,1,* Hang Wang,3,* Li-Ming Shen,1 Shang-Qi Ni,1 Bin Su,1 Zhi-Jun Jiang,4 Li-Juan Zhu,4 Yue-Xi Luo,1 Qiuling Shi2
1Department of Obstetrics and Gynecology, The Affiliated Nanchong Central Hospital of North Sichuan Medical College, Nanchong, Sichuan, People’s Republic of China; 2State Key Laboratory of Ultrasound in Medicine and Engineering, College of Biomedical Engineering, Chongqing Medical University, Chongqing, People’s Republic of China; 3Department of Obstetrics and Gynecology, Si Chuan Mian Yang 404 Hospital, Mian Yang, Sichuan, People’s Republic of China; 4Department of Radiology, The Affiliated Nanchong Central Hospital of North Sichuan Medical College, Nanchong, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yue-Xi Luo, Department of Obstetrics and Gynecology, The Affiliated Nanchong Central Hospital of North Sichuan Medical College, Nanchong, Sichuan, People’s Republic of China, Email [email protected] Qiuling Shi, State Key Laboratory of Ultrasound in Medicine and Engineering, College of Biomedical Engineering, Chongqing Medical University, Chongqing, People’s Republic of China, Email [email protected]
Background: The underlying mechanisms of symptom recurrence or established comprehensive predictive models have not yet elucidated. This study aimed to establish a prediction model for symptom recurrence following focused ultrasound ablation surgery (FUAS) in adenomyosis based on magnetic resonance imaging (MRI)-based classification system incorporating serum cancer antigen (CA) 125 levels.
Methods: We conducted a retrospective cohort study of 502 adenomyosis patients, divided into recurrence (n=133) and non-recurrence (n=369) groups. Patients were stratified by MRI lesion extent: ≥ 2/3 uterine wall involvement (n=446) vs < 2/3 (n=56). Symptom recurrence (dysmenorrhea and/or menorrhagia) was the primary outcome. Univariate and multivariate logistic regression identified predictors. Receiver operator characteristic curve analysis determined CA125 cutoffs. Kaplan–Meier curves and Cox regression assessed recurrence-free survival.
Results: Patients with ≥ 2/3 involvement had higher CA125 (57.9 vs 32.1 U/mL, P< 0.001). Recurrence group had higher CA125 (71.5 vs 51.14 U/mL, P< 0.001). Multivariate analysis identified CA125 (OR=1.002, 95% CI: 1.001– 1.004), diffuse grayscale changes (OR=0.632, 95% CI: 0.407– 0.981), and combined GnRH-a/LNG-IUS therapy (OR=0.504, 95% CI: 0.323– 0.785) as independent predictors. In the ≥ 2/3 subgroup, CA125 > 35 U/mL predicted shorter recurrence-free survival (37.7 vs 43.9 months, P=0.001). The combined model (CA125 ≥ 35 U/mL + lesion ≥ 2/3) yielded an AUC of 0.580 (95% CI: 0.533– 0.626).
Conclusion: A preoperative CA125 level ≥ 35 U/mL combined with MRI-based lesion extent ≥ 2/3 uterine wall involvement may effectively identify adenomyosis patients at high risk of post-FUAS recurrence. Further prospective studies are warranted.
Plain Language Summary: High CA125 level combined with MRI-based lesion extent ≥ 2/3 uterine wall involvement could better inform symptom recurrence of adenomyosis after FUAS.
Keywords: MRI, CA125, adenomyosis, symptom recurrence, focused ultrasound ablation surgery, risk prediction model
Introduction
Adenomyosis, a benign estrogen-dependent gynecological disorder predominantly affecting perimenopausal women (40–50 years), is pathologically characterized by the ectopic invasion of endometrial glands and stroma into the myometrium, typically manifesting as debilitating dysmenorrhea and menorrhagia.1,2 Recently, ultrasound-guided high-intensity focused ultrasound ablation (FUAS) has been recognized as a revolutionary non-invasive therapeutic modality for adenomyosis, providing significant advantages in uterine preservation while maintaining therapeutic efficacy.3 Despite these advancements, clinical observations suggest that approximately 20–30% of patients experience disease recurrence following FUAS treatment, with a median relapse interval of 12 months.4 This underscores the urgent need for reliable predictive biomarkers to optimize patient selection and guide treatment strategies. However, robust indicators for predicting post-FUAS symptom recurrence remain an unresolved challenge in clinical practice.
The tumor marker cancer antigen (CA) 125 has emerged as a potentially valuable biomarker in this context.5,6 A large number of studies have demonstrated that the serum CA125 level significantly elevates in adenomyosis patients compared with those with uterine fibroids (P<0.01),7,8 and particularly pronounced elevation could be observed in diffuse-type versus focal adenomyosis.5,9 Although preliminary evidence suggests that CA125 may have predictive value for symptom recurrence following FUAS,5 its standalone clinical utility has been limited by suboptimal sensitivity and specificity.5,8,9
Concurrently, advancements in magnetic resonance imaging (MRI) technology have established it as the gold standard for preoperative adenomyosis assessment prior to FUAS treatment.10,11 Contemporary high-resolution MRI enables precise evaluation of key pathological features including junctional zone thickness, lesion vascularity, and myometrial involvement patterns.11 Our previous study showed that based on classification of Kobayashi H criteria, patients had different clinical symptom stratified by myometrial involvement patterns.12,13 Recent investigations have begun to explore the prognostic potential of MRI characteristics, with particular attention being paid to their correlation with treatment outcomes.3,14 Nevertheless, current imaging-based studies have neither elucidated the mechanisms underlying symptom recurrence nor established comprehensive predictive models integrating both imaging and biochemical markers.
Given the complementary strengths of CA125 as a biomarker of inflammatory activity and MRI as a tool for detailed anatomical characterization, we hypothesized that combining these modalities would improve the prediction of symptom recurrence after FUAS. Therefore, this study aimed to investigate the combined predictive value of preoperative serum CA125 levels and MRI-based classification systems for symptom recurrence following FUAS in patients with adenomyosis. By developing a dual-modality prognostic framework, we sought to enable more accurate risk stratification, inform personalized therapeutic decisions, and ultimately improve long-term patient outcomes.
Methods
Study Design and Patients
In this retrospective cohort study, we analyzed 502 consecutive patients with MRI-confirmed adenomyosis treated with FUAS from June 2017 to March 2021. Patients were stratified into recurrence group (n=133) and non-recurrence group (n=369). In addition, our previous study showed Kobayashi H’s classification associated with symptom of adenomyosis,12 hence, patients were categorized into two subgroups based on the lesion size of uterine wall in MRI: the lesion size of uterine wall ≥2/3 group (n=446) and the lesion size of uterine wall <2/3 group (n=56).
Inclusion criteria: (1) MRI diagnosis of adenomyosis; (2) preoperative CA125 testing; (3) underwent FUAS; (4) complete follow-up data. Exclusion criteria: (1) coexisting uterine fibroids or malignancy; (2) inflammatory disease within 7 days; (3) previous treatment within 6 months; (4) incomplete data.
Assessments
The measurements of uterine and lesion dimensions across all meridians, conjugate zone thickness, and subcutaneous adipose tissue thickness were performed following the standardized protocols established by expert consensus. The MRI diagnostic criteria for adenomyosis were as follows: (1) a junctional zone maximum thickness (JZmax) exceeding 12 mm, (2) a JZmax-to-myometrial thickness ratio ≥40%, and (3) a difference in junctional zone maximum thickness >5 mm between the thickest and thinnest regions. Using a blinded assessment protocol, the quantitative measurements were independently performed by two imaging physicians (with ≥10 years of experience) and one obstetrician-gynaecologist (with ≥10 years of experience) with the title of deputy director or above.3,15 Inter-rater reliability was established upon concordance analysis, where consistent measurements between the first two physicians were directly adopted for data analysis. In cases of discrepancies in measurements, a third independent evaluator was consulted to resolve the differences, and the final consensus measurements were incorporated into the dataset after thorough discussion and agreement among all the three evaluators.3 The formula for calculating the uterine volume and lesion volume in adenomyosis was 0.52*long diameter*anteroposterior diameter*transverse diameter. The MRI-based classification systems of adenomyosis referred to two of our previous papers.3,12
Outcomes and Definitions
From August 2021 to December 2022, 502 patients were entered for follow-up observation, including whether dysmenorrhea and menorrhagia recurred, ie, whether dysmenorrhea recurred or not, and whether menorrhagia recurred or not.
The primary outcome was symptom recurrence, defined as patient-reported dysmenorrhea and/or menorrhagia occurring at least 12 months after a symptom-free interval of ≥3 months post-FUAS.5 Follow-up included on-site follow-up or telephone completion of questionnaires (for patients who lived far away and chose local follow-up).
MRI-Based Classifications for Adenomyosis
All pelvic MRI examinations were conducted using the 1.5 Tesla scanners with standardized protocols, including turbo spin-echo T2-weighted imaging and single-shot echo-planar diffusion-weighted imaging sequences, following the established methodology (Brown et al15). Two imaging physicians (ZJ, with 10 years of experience; JZ, with 11 years of experience) and one gynecologist (YT, with 11 years of experience) were invited to individually reclassify adenomyosis according to the classification of Kobayashi H criteria.12 The classification process followed rigorous methodology below: 1) each reviewer independently assessed all the cases; 2) initial concordance between any two reviewers was accepted for analysis; 3) discordant cases underwent tertiary review with consensus discussion; and 4) final classifications required agreement from at least two specialists. Quality Assurance Measures were as follows: 1) the classification schemes were detailed as previous study;12 2) every case underwent evaluation by at least two reviewers; 3) final determinations reflected the complete inter-rater consensus; and 4) validation procedures maintained identical standards across different cohorts.
Serum CA125 Test Before FUAS
Serum CA125 levels were quantified using a standardized two-step immunoassay at our central laboratory, with samples collected within 24 h pre-FUAS and transported at ambient temperature following the established protocols.5,6
FUAS Procedure
The FUAS treatment was performed using the JC200 Focused Ultrasound Tumor Therapeutic System (Chongqing Haifu Medical Technology Co., Ltd., China) in strict accordance with manufacturer’s guidelines.16 During the procedure, critical treatment parameters including sonication time and average power output were systematically recorded. The ablation volume was calculated using the ellipsoid volume formula (V = 4/3πABC), where A, B, and C were consistent with the lesion’s longitudinal, transverse, and anteroposterior diameters, respectively.17 Treatment efficacy was quantitatively assessed through the non-perfused volume (NPV) ratio, derived from the formula (NPV/adenomyosis volume) × 100%, by utilizing the dedicated analysis software provided by the manufacturer.18 To ensure measurement accuracy, three independent operators (ZJ, JZ, and YT) performed blinded assessments of both target lesion dimensions and non-enhanced regions.12 A consensus-based approach was implemented for result validation: concordant measurements from any two operators were accepted, while discordant results underwent tertiary review. All patients underwent the standardized 24-h post-procedural monitoring for immediate treatment evaluation and safety assessment.
Statistical methods
Continuous variables were indicated as mean ± standard deviation, while categorical data were presented as proportions. Body mass index (BMI) was dichotomized at 24 kg/m2.19 Comparative analyses between recurrence and non-recurrence groups were performed using independent samples t-tests for continuous variables (including age, BMI, serum CA125 levels, adipose tissue thickness, lesion-to-sacrococcygeal distance, uterine/lesion volumes, ablation parameters, and NPV) and by chi-square tests for categorical variables (dysmenorrhea/menorrhagia status, uterine position, and lesion location). Univariate and multivariate logistic regression were performed to identify predictors of recurrence (age, dysmenorrhea, CA125 levels, T2WI signal intensity, grayscale variation, and GnRH-a/LNG-IUS therapy) and symptom recurrence, stratified by lesion extent (≥2/3 vs <2/3 myometrial involvement). The results were reported as adjusted odds ratios (ORs) with 95% confidence intervals. Variables with P<0.10 in univariate analysis were entered into multivariate models. The predictive performance of preoperative CA125 was assessed using receiver operating characteristic (ROC) curve analysis, with optimal cutoff values determined for the overall cohort and lesion-size subgroups. Time-to-recurrence was analyzed using Kaplan–Meier curves and Cox proportional hazards regression. All analyses were conducted using SPSS 22.0 (IBM Corp.), with two-tailed P-value <0.05 indicating statistical significance.
Results
Clinicopathological Characteristics and Recurrence Analysis
The total cohort comprised 502 adenomyosis patients with a median follow-up period of 24 months (range, 2–51 months). Comparative analysis revealed significant differences between recurrence (n=133, 26.5%) and non-recurrence (n=369, 73.5%) groups (Table 1).5 Patients experiencing symptom recurrence demonstrated (1) significantly higher preoperative serum CA125 levels (median 71.5 vs 51.14 U/mL, P<0.001), (2) younger mean age (P<0.001), and (3) higher prevalence of clinically relevant features including dysmenorrhea (P<0.05), extensive myometrial involvement (≥2/3 uterine wall thickness, P<0.05), diffuse grayscale changes during FUAS (P<0.05), and receipt of FUAS monotherapy (P<0.05).
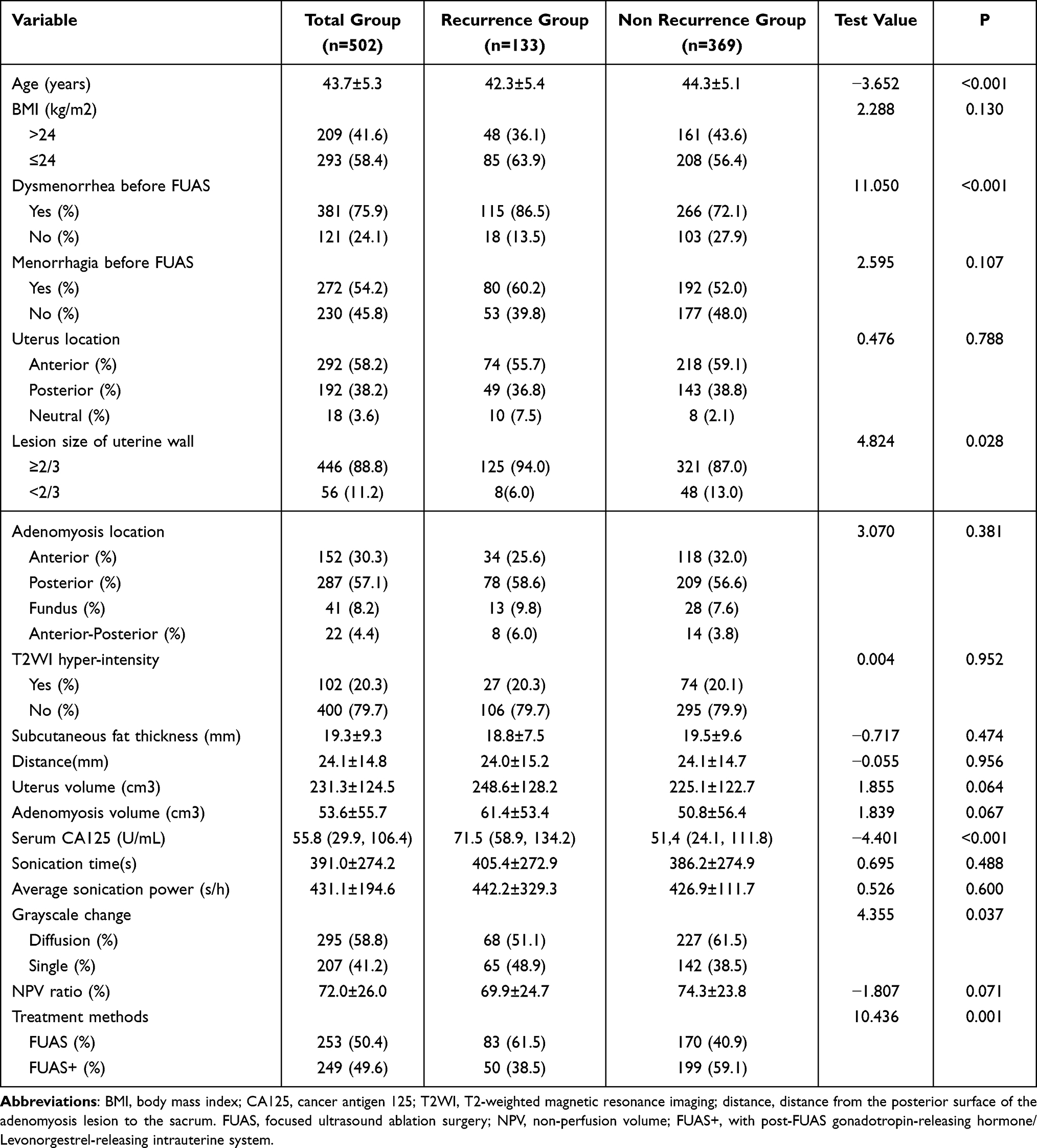 |
Table 1 Comparison of Clinical Features of Adenomyosis Between Recurrence Group and Non- Recurrence Group5 |
In the subgroup of patients with adenomyosis involving ≥2/3 of the uterine wall thickness, adenomyosis volume, uterus volume and serum CA125 levels were significantly higher than those in the subgroup of patients with adenomyosis involving <2/3 of the uterine wall thickness (Supplementary Table 1 and Table 2, P<0.05). The example of Kobayashi H’s classification was shown in Figure 1.
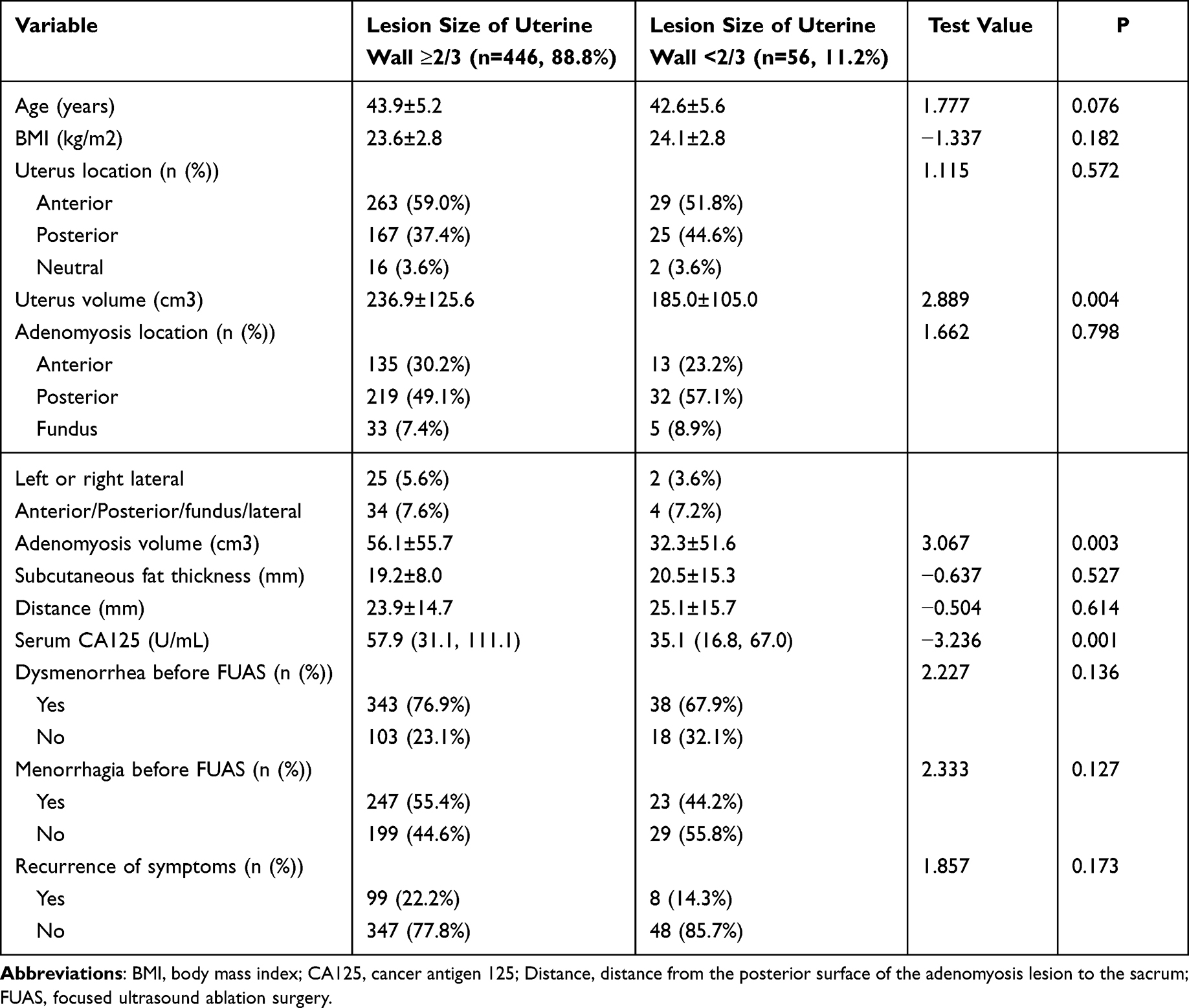 |
Table 2 Clinicopathological Features in Subgroups |
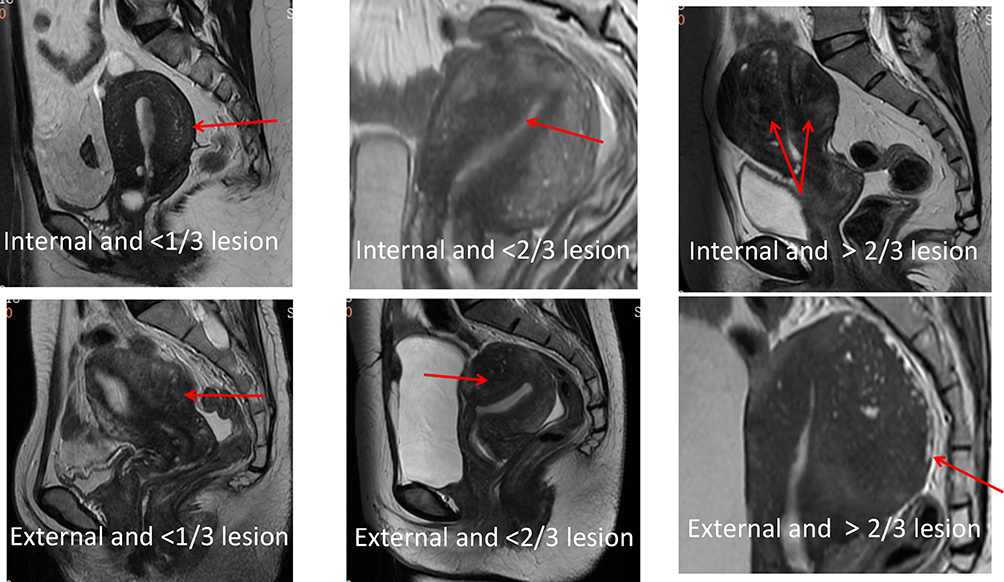 |
Figure 1 The example of Classification system 4 (red color arrow showed the lesion location based on MRI). |
Predictors of Symptom Recurrence
Univariate analysis identified younger age, dysmenorrhea, CA125 level, lesion extent ≥2/3, diffuse grayscale changes, and monotherapy as associated with recurrence (all P<0.05). Multivariate logistic regression confirmed CA125 (OR=1.002, 95% CI 1.001–1.004, P=0.012), diffuse grayscale changes (OR=0.632, 95% CI 0.407–0.981, P=0.041), and combination therapy (OR=0.504, 95% CI 0.323–0.785, P=0.002) as independent predictors in the total cohort (Table 3). In the ≥2/3 subgroup, CA125 remained predictive (OR=1.002, 95% CI 1.001–1.004, P=0.013) and combination therapy showed stronger protection (OR=0.553, 95% CI 0.350–0.874, P=0.011) (Table 4).
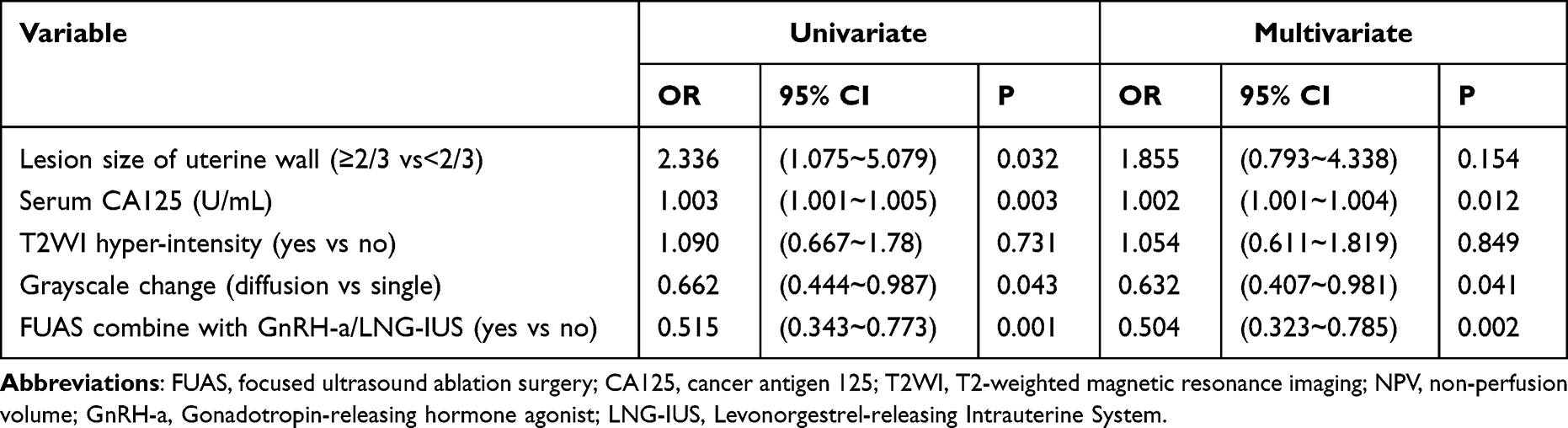 |
Table 3 Binary Logistic Regression Analysis of Symptom Recurrence in Total Cohort of Patients with Adenomyosis |
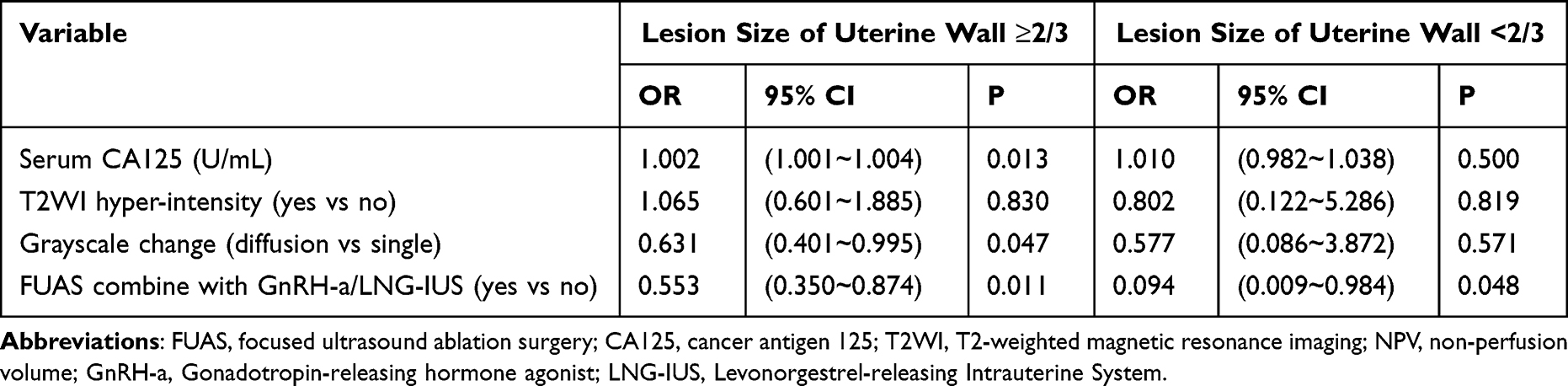 |
Table 4 Binary Logistic Regression Analysis of Symptom Recurrence in Subgroups Patients with Adenomyosis |
Predictive Value of CA125
In the ≥2/3 subgroup, preoperative CA125 predicted recurrence with an AUC of 0.580 (95% CI 0.533–0.626, P<0.001). The optimal cutoff was 57.1 U/mL (sensitivity 60.6%, specificity 58.6%). Using a clinically practical cutoff of 35 U/mL, sensitivity increased to 72.8% (specificity 38.9%) (Table 5 and Figure 2).
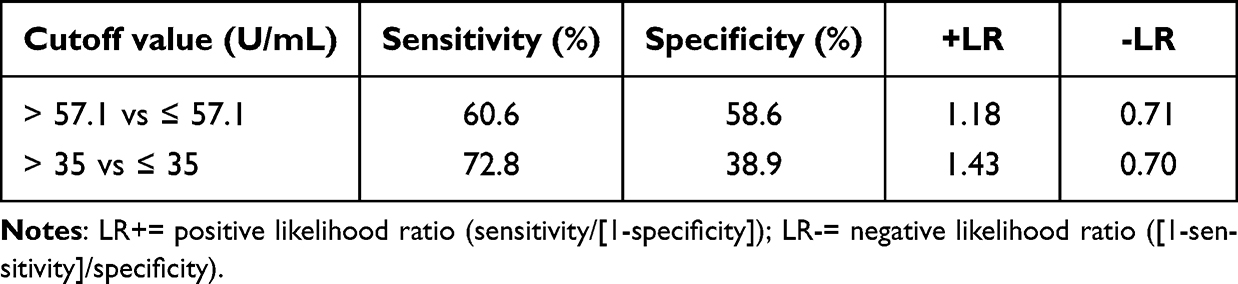 |
Table 5 Parameters of Different Cutoff Value of Serum CA125 in Patients with Lesion Size of Uterine Wall ≥2/3 |
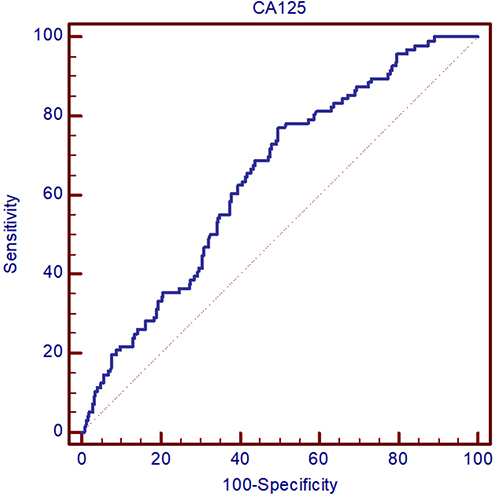 |
Figure 2 Receiver operating characteristic curve of CA125 predicting symptom recurrence in the ≥2/3 lesion subgroup. |
Recurrence-Free Survival
Multivariate Cox regression analysis showed that elevated preoperative CA125 levels were independently associated with earlier symptom recurrence in the total cohort (HR = 1.001, 95% CI: 1.001–1.003, P = 0.015 Table 6) and in the subgroup with extensive uterine wall involvement≥2/3(HR = 1.001, 95% CI: 1.000–1.002, P = 0.040 Table 6). Kaplan–Meier survival analysis further demonstrated that patients with preoperative CA125 levels >35 U/mL experienced significantly shorter median recurrence-free survival than those with CA125 ≤35 U/mL in the total cohort (38.5 vs 44.5 months, as shown in Figure 3A, P < 0.05). This difference was particularly pronounced in the subgroup with extensive uterine wall involvement (≥2/3), where the high-CA125 group had a median recurrence time of 37.7 months versus 43.9 months (P = 0.001, Figure 3B).
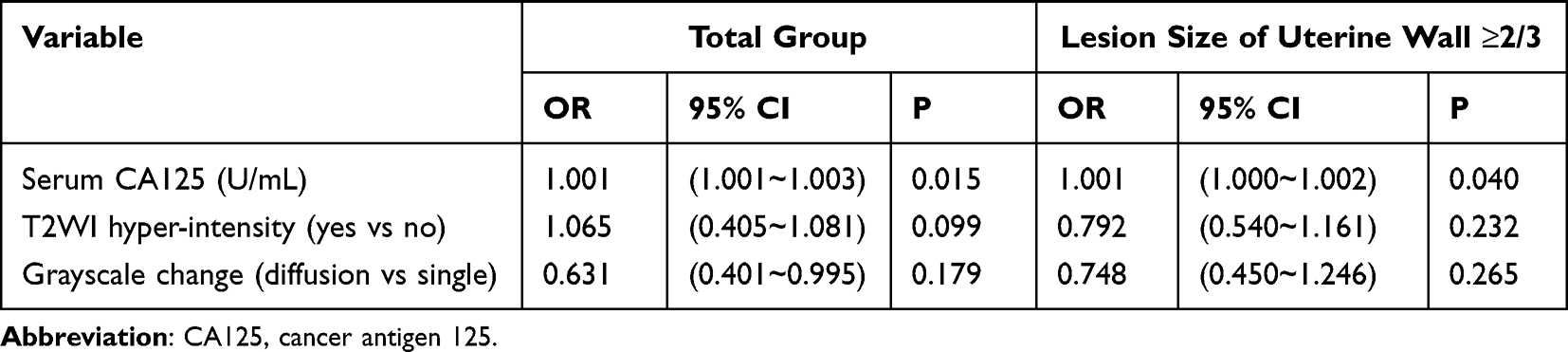 |
Table 6 Cox Regression Analysis of Symptom Recurrence in Patients with Adenomyosis |
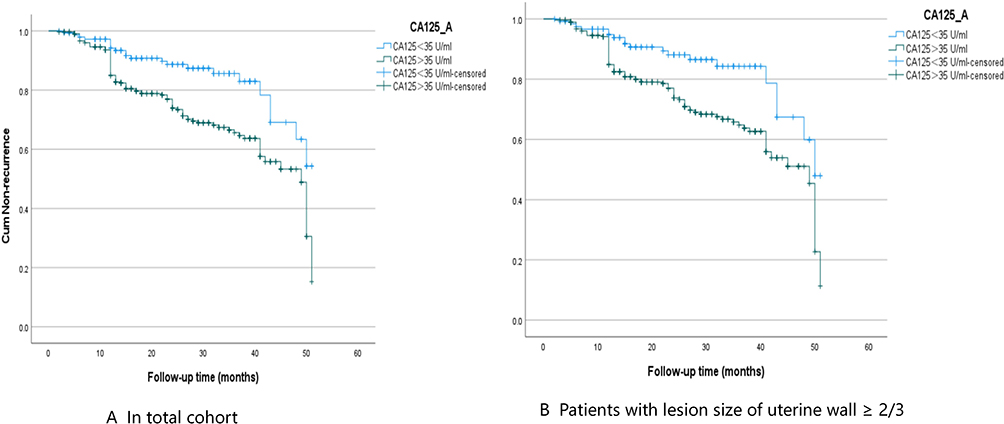 |
Figure 3 Kaplan–Meier curve of CA125 predicting symptom recurrence, (A) showed K-M curve of CA125 predicting symptom recurrence in total cohort, patients with CA125 >35 U/mL had shorter median recurrence-free survival (38.5 vs 44.5 months, P<0.05); (B) showed K-M curve of CA125 predicting symptom recurrence in the ≥2/3 lesion subgroup, patients with CA125 >35 U/mL had shorter median recurrence-free survival (37.7 vs 43.9 months, P=0.001). |
Discussion
This cross-sectional study identified preoperative serum CA125 as an independent predictive factor for symptomatic recurrence after FUAS in adenomyosis patients with extensive uterine involvement (lesion size ≥2/3 of uterine wall thickness on MRI). The clinically established cutoff of 35 U/mL exhibited a high sensitivity in predicting both recurrence incidence and shorter recurrence-free intervals, suggesting its utility as a practical biomarker for risk stratification in this patient subgroup. Moreover, these findings supported the incorporation of preoperative CA125 assessment, particularly when combined with MRI-based lesion characterization, into clinical decision-making for adenomyosis management.
Consistent with previous reports by Sheth et al,9 our study confirmed that elevated preoperative CA125 levels correlated with larger adenomyotic lesion volumes, particularly in external-type adenomyosis characterized by higher rates of pelvic adhesion and concurrent endometriosis. This patient subgroup typically presented with more pronounced inflammatory activity. Our findings revealed that when uterine wall involvement exceeded ≥2/3 thickness, patients with CA125 >35 U/mL (especially >57.1 U/mL) accompanied by severe dysmenorrhea,13 T2WI signal abnormalities, and diffuse grayscale changes during FUAS demonstrated significantly higher symptomatic recurrence rates. For patients demonstrating extensive uterine involvement (≥2/3 wall thickness) and elevated CA125 levels (>57.1 U/mL), a comprehensive therapeutic approach was recommended:1) during FUAS, application of maximal safe acoustic energy levels to achieve complete lesion ablation while maintaining appropriate safety margins; 2) implementation of adjuvant medical therapy, with either gonadotropin-releasing hormone agonists (GnRH-a) or a levonorgestrel-releasing intrauterine system (LNG-IUS), to enhance treatment efficacy; 3) for high-risk patients without immediate pregnancy plans, a sequential regimen of 4–6 cycles of GnRH-a therapy followed by LNG-IUS insertion was strongly recommended to optimize the long-term outcomes. These findings demonstrated that FUAS monotherapy might be insufficient for high-risk adenomyosis cases, underscoring the need for comprehensive, individualized treatment strategies incorporating both surgical and medical approaches to minimize the recurrence risk. However, CA125 elevation can occur in various benign and malignant conditions (eg, pregnancy, liver disease, autoimmune disorders).20,21 Thus, false positives should be considered when interpreting results.
Building upon our previous findings that Kishi Y’s classification system correlated with FUAS effectiveness,3,22 this study advanced the field by demonstrating that classification system 4, when used in combination with preoperative CA125 levels, provided the optimal predictive value for symptom recurrence. At first, the combination of CA125 ≥35 U/mL with MRI-documented lesion extent ≥2/3 uterine wall thickness effectively identified high-risk adenomyosis patients for post-FUAS recurrence (AUC=0.580, 95% CI: 0.533–0.62). This dual-parameter approach significantly improved the preoperative risk assessment compared with either biomarker alone (P<0.01), suggesting the biomarker utility in risk stratification and postoperative surveillance. Second, younger patients presenting with both extensive disease (≥2/3 involvement) and elevated CA125 levels (>57.1 U/mL) were associated with a higher recurrence risk, suggesting a distinct clinical phenotype requiring multimodal therapy, which might be beneficial for the comprehensive preoperative assessment of the optimal patient stratification and treatment planning, like the consideration of combination therapies for high-risk patients with extensive adenomyosis. Third, the predictive power of this combined model stemmed from the role of CA125 as an inflammatory mediator in adenomyosis pathogenesis. Emerging evidence had established inflammation as a pivotal driver for both the initiation and progression of adenomyosis,23 involving a complex interplay of genetic, hormonal, and inflammatory factors.24 Serum CA125, a cost-effective and clinically accessible biomarker, was a high-molecular-weight glycoprotein predominantly expressed by coelomic epithelial derivatives in the inflammatory environment.25 The up-regulation in adenomyosis patients reflected multiple pathological mechanisms, including inflammatory activation. Peritoneal irritation and increased endothelial permeability (often secondary to peritoneal stretching) triggered the substantial release of CA125 into the circulation, causing the increased preoperative level.7 The elevated CA125 levels might facilitate the ectopic endometrial migration and enhance the myometrial adhesion capacity, clinically manifesting as the increased pain severity and higher recurrence rates,12 especially in patients with MRI-documented lesion extent ≥2/3 uterine wall thickness. Besides, the reduction of post-FUAS CA125 level correlated with the diminished inflammatory activity, serving as a potential indicator of treatment response and disease burden alleviation. Thus, this multifunctional biomarker not only reflected both the inflammatory milieu and disease activity in adenomyosis, but also provided clinical utility in treatment monitoring and prognosis assessment.
Limitations
Although the integrated imaging-biomarker approach supports personalized management of adenomyosis—particularly in identifying candidates who may benefit from combined surgical and medical therapies—several inherent limitations of this study should be acknowledged. First, as a single-center retrospective study, the findings are subject to potential selection bias and may not be generalizable to broader populations. Second, postoperative CA125 levels were not measured, precluding analysis of dynamic changes before and after FUAS and limiting our ability to explore the relationship between CA125 kinetics and symptom recurrence. Additionally, CA125 is known to be elevated in various benign and malignant conditions20 (eg, pregnancy, liver disease, endometriosis),20,21 and the possibility of false-positive elevations cannot be entirely excluded, which may have influenced the predictive performance. Although the retrospective design does not permit causal inference, the observed association between preoperative CA125 and recurrence offers clinically useful information for risk stratification and postoperative surveillance. Third, despite rigorous follow-up efforts, the retrospective nature of the study led to incomplete data collection, partly due to the exclusion of patients from distant regions who could not attend on-site visits. Fourth, symptom recurrence was assessed based on patient-reported binary outcomes (presence or absence of dysmenorrhea and/or menorrhagia), without standardized severity grading, which may introduce reporting bias. Finally, the predictive model was not validated in an independent external cohort, and its performance may be overestimated. Future multicenter studies incorporating validated tools such as the Numerical Rating Scale (NRS) and including external validation cohorts are warranted to provide more robust evidence regarding the prognostic value of preoperative CA125 in adenomyosis.
Conclusions
Preoperative CA125 ≥35 U/mL combined with MRI lesion extent ≥2/3 uterine wall involvement may identify adenomyosis patients at high risk of post-FUAS recurrence. The combination of FUAS with GnRH-a and LNG-IUS might reduce recurrence risk. Further multicenter prospective studies are required to confirm these findings.
Abbreviations
MRI, Magnetic resonance imaging; FUAS, high-intensity focused ultrasound ablation; NPV, non-perfused volume; JZmax, junctional zone maximum; BMI, Body mass index; ORs, odds ratios; ROC, receiver operating characteristic; M, Kaplan-Meier; AUC, area under the curve; GnRH-a, gonadotropin-releasing hormone agonists; LNG-IUS, levonorgestrel-releasing intrauterine system; NRS, Numerical Rating Scale.
Data Sharing Statement
The datasets generated during this study are available from the corresponding author (Yue-xi Luo) upon reasonable request.
Ethics Statement
This retrospective cohort study was conducted in accordance with the Declaration of Helsinki and received ethical approval from the Institutional Review Board of the Affiliated Nanchong Central Hospital, North Sichuan Medical College (Approval No. 2021/104). Informed consent was waived due to the anonymized nature of the data.
Author Contributions
All authors made a significant contribution to the work reported, whether that was in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by National Key R&D Plan for Intergovernmental Cooperation, the Ministry of Science and Technology of China (Grant No.2022YFE0133100), Foundation of State Key Laboratory of Ultrasound in Medicine and Engineering (Grant No. 2024KFKT016), Sichuan Provincial Natural Science Foundation Project (Grant No. 26NSFSC0004), Nanchong Municipal Bureau of Science and Technology Project (Grant No. 25YYJCYJ007) and Sichuan Medical Science & Technology Innovation Research Association (Grant No. 2026YCYM002).
Disclosure
No potential conflict of interest was reported by the authors.
References
1. Vercellini P, Viganò P, Bandini V, et al. Association of endometriosis and adenomyosis with pregnancy and infertility. Fertil Sterility. 2023;119(5):727–12. doi:10.1016/j.fertnstert.2023.03.018
2. Dason ES, Maxim M, Sanders A, et al. Guideline No. 437: diagnosis and management of adenomyosis. J Obstet Gynaecol Can. 2023;45(6):417–29.e1. doi:10.1016/j.jogc.2023.04.008
3. Tang Y, Hu WH, Wang H, et al. Magnetic resonance imaging-based classification systems for informing better outcomes of adenomyosis after ultrasound-guided high-intensity focused ultrasound ablating surgery. J Magn Reson Imaging. 2024;59(5):1787–1797. doi:10.1002/jmri.28943
4. Liu X, Wang W, Wang Y, et al. Clinical predictors of long-term success in ultrasound-guided high-intensity focused ultrasound ablation treatment for adenomyosis: a retrospective study. Medicine. 2016;95(3):e2443. doi:10.1097/md.0000000000002443
5. Tang Y, Ming-Tao Y, Xiang RM, et al. Preoperative CA125 as a risk factor for symptom recurrence of adenomyosis after ultrasound-guided high-intensity focused ultrasound ablation surgery. Int J Hyperthermia. 2022;39(1):1164–1169. doi:10.1080/02656736.2022.2107716
6. Tang Y, Wen MB, Xiang RM, et al. Serum CA125 as a biomarker for dysmenorrhea in adenomyosis. Int J Gynaecol Obstet. 2023;163(1):131–139. doi:10.1002/ijgo.14832
7. Kil K, Chung JE, Pak HJ, et al. Usefulness of CA125 in the differential diagnosis of uterine adenomyosis and myoma. Eur J Obstet Gynecol Reprod Biol. 2015;185:131–135. doi:10.1016/j.ejogrb.2014.12.008
8. Jeng CJ, Ou KY, Long CY, et al. 500 cases of high-intensity focused ultrasound (hifu) ablated uterine fibroids and adenomyosis. Taiwanese J Obstetrics Gynecol. 2020;59(6):865–871. doi:10.1016/j.tjog.2020.09.013
9. Sheth SS, Ray SS. Severe adenomyosis and CA125. J Obstetrics Gynaecol. 2014;34(1):79–81. doi:10.3109/01443615.2013.832178
10. Harmsen MJ, Trommelen LM, de Leeuw RA, et al. Uterine junctional zone and adenomyosis: comparison of MRI, transvaginal ultrasound and histology. Ultrasound Obstet Gynecol. 2023;62(1):42–60. doi:10.1002/uog.26117
11. Bazot M, Daraï E. Role of transvaginal sonography and magnetic resonance imaging in the diagnosis of uterine adenomyosis. Fertil Sterility. 2018;109(3):389–397. doi:10.1016/j.fertnstert.2018.01.024
12. Tang Y, Jiang ZJ, Wen MB, et al. Magnetic resonance imaging-based Classifications for Symptom of Adenomyosis. Gynecol Obstetr Investigat. 2024;89(5):402–412. doi:10.1159/000535802
13. Su B, Huang JR, Wang H, et al. Combined magnetic resonance imaging with serum CA125 for dysmenorrhea in adenomyosis. Sci Rep. 2025. doi:10.21203/rs.3.rs-5025850/v1
14. Munro MG. Classification and reporting systems for adenomyosis. J Minimal Invasive Gynecol. 2020;27(2):296–308. doi:10.1016/j.jmig.2019.11.013
15. Brown MA. MR imaging of benign uterine disease. Magn Reson Imaging Clin N Am. 2006;14(4):439–53, v. doi:10.1016/j.mric.2007.01.006
16. Matlac DM, Tonguc T, Mutschler N, et al. Study protocol of a prospective, monocentric, single-arm study investigating the safety and efficacy of local ablation of symptomatic uterine fibroids with US-Guided High-Intensity Focused Ultrasound (HIFU). J Clin Med. 2023;12(18):5926. doi:10.3390/jcm12185926
17. Gong C, Wang Y, Lv F, et al. Evaluation of high intensity focused ultrasound treatment for different types of adenomyosis based on magnetic resonance imaging classification. Int J Hyperthermia. 2022;39(1):530–538. doi:10.1080/02656736.2022.2052366
18. Li J, Wang W, Liao L, et al. Analysis of the nonperfused volume ratio of adenomyosis from MRI images based on fewshot learning. Phys Med Biol. 2021;66(4):045019. doi:10.1088/1361-6560/abd66b
19. Yang PK, Chou CH, Chang CH, et al. Changes in peripheral mitochondrial DNA copy number in metformin-treated women with polycystic ovary syndrome: a longitudinal study. Reprod Biol Endocrinol. 2020;18(1):69. doi:10.1186/s12958-020-00629-5
20. Yin A, Chen Y, Zhang H, et al. Increased first-trimester CA125 levels associated with the development of preeclampsia. J Transl Med. 2025;24(1):97. doi:10.1186/s12967-025-07565-1
21. Baskiran DY, Sarigoz T, Baskiran A, Yilmaz S. The significance of serum tumor markers CEA, Ca 19-9, Ca 125, Ca 15-3, and AFP in patients scheduled for orthotopic liver transplantation: do elevated levels really mean malignancy? J Gastrointest Cancer. 2023;54(2):442–446. doi:10.1007/s12029-021-00798-5
22. Kishi Y, Suginami H, Kuramori R, et al. Four subtypes of adenomyosis assessed by magnetic resonance imaging and their specification. Am J Clin Exp Obstet Gynecol. 2012;207(2):114.e1–7. doi:10.1016/j.ajog.2012.06.027
23. Zhai J, Vannuccini S, Petraglia F, et al. Adenomyosis: mechanisms and pathogenesis. Semin Reprod Med. 2020;38(2–3):129–143. doi:10.1055/s-0040-1716687
24. Jin Z, Liu H, Xu C. Estrogen degrades Scribble in endometrial epithelial cells throughE3ubiquitin ligase HECW1 in the development of diffuse adenomyosis†. Biol Reprod. 2020;102(2):376–387. doi:10.1093/biolre/ioz194
25. Karam AK, Karlan BY. Ovarian cancer: the duplicity of CA125 measurement. Nat Rev Clin Oncol. 2010;7(6):335–339. doi:10.1038/nrclinonc.2010.44
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Endometriosis Severity and Risk of Preeclampsia: A Combined Mendelian Randomization and Observational Study
Zu Y, Xie Y, Zhang H, Chen L, Yan S, Wang Z, Fang Z, Lin S, Yan J
International Journal of Women's Health 2025, 17:923-935
Published Date: 27 March 2025
Predicting Glioma Recurrence Using 18F-FDG PET/CT, MRI, and Tumor Markers: A Combined Approach
Wei J
International Journal of General Medicine 2025, 18:2429-2438
Published Date: 5 May 2025
Uterine Anteroposterior Diameter as an Imaging Correlate of Dysmenorrhea Severity: Findings Across Symptom Based Clusters
Li J, Gao Y, Sun M, Chen C, Che J, Zhao T
International Journal of Women's Health 2026, 18:589366
Published Date: 16 March 2026