Back to Journals » Drug Design, Development and Therapy » Volume 20
Moringa oleifera Lamk. as a Promising Adjunct Therapeutic Candidate: A Narrative Review of Human Studies and Published Case Reports
Authors Sianipar EA, Sumiwi SA, Susilawati Y ![]() , Levita J
, Levita J ![]()
Received 4 December 2025
Accepted for publication 31 January 2026
Published 10 February 2026 Volume 2026:20 586556
DOI https://doi.org/10.2147/DDDT.S586556
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Solomon Tadesse Zeleke
Erlia Anggrainy Sianipar,1,2,* Sri Adi Sumiwi,3,* Yasmiwar Susilawati,4,* Jutti Levita3,*
1Doctoral Program in Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Department of Pharmacy, School of Medicine and Health Sciences, Atma Jaya Catholic University of Indonesia, Jakarta, Special Capital Region of Jakarta, Indonesia; 3Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 4Department of Biology Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, West Java, Indonesia
*These authors contributed equally to this work
Correspondence: Jutti Levita, Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, West Java, Indonesia, Email [email protected]
Abstract: Moringa oleifera Lamk. a highly valued multipurpose plant, has gained increasing attention owing to its diverse pharmacological properties, including immunomodulatory, antioxidant, and antidiabetic effects. This narrative review evaluates published human studies and case reports from 2015 to 2025 to assess the efficacy and safety of M. oleifera and the underlying mechanisms of its pharmacological effects. A narrative review was chosen over a systematic review because it is flexible, broad-focused, and interpretive, and thus is suitable for mapping emerging fields. A total of 22 clinical trials and nine case reports met the inclusion criteria. This review focuses on five major clinical themes: immunological and nutritional effects, metabolic and endocrine disorders, inflammatory and oxidative stress-related diseases, maternal and child health outcomes, and other clinical applications. Evidence from human studies indicates consistent improvements in immune function, glycemic control, and antioxidant status, particularly among individuals with HIV infection, prediabetes, and malnutrition. Maternal supplementation also enhances the vitamin A content and nutritional outcomes in infants. Mechanistically, these effects are linked to the immune system (modulation of cytokine activity, activation of AMP-activated protein kinase, and antioxidant activity) and to metabolic pathways (inhibition of α-glucosidase and dipeptidyl peptidase IV). Although it is generally well tolerated, rare hypersensitivity and thrombotic events have been reported. Collectively, M. oleifera shows promising potential as a safe and accessible functional food and a nutraceutical or adjunct therapeutic candidate for immune and metabolic disorders, thus warranting further standardized, large-scale randomized controlled trials to confirm its long-term efficacy and safety.
Keywords: antidiabetic, antioxidant, drumstick tree, horseradish tree, immunomodulator, metabolic disorders
Introduction
Moringa oleifera Lamk. (family Moringaceae), a fast-growing subtropical tree, natively edible to the Indian subcontinent, has gained remarkable global recognition for its exceptional nutritional and medicinal values.1 For centuries, nearly every part of the tree, especially the leaves, has been used for food and traditional medicine to combat many diseases. The leaves are rich in essential vitamins, minerals, and bioactive phytochemicals such as polyphenols, flavonoids (kaempferol glycosides, malonyl glucosides, rutinosides, quercetin, myricetin, epicatechin, and rutin), phenolic acids (caffeic acid, chlorogenic acid, coumaric acid, gallic acid, and ellagic acid), and sulfur compounds (glucosinolates and isothiocyanates). These compounds are largely responsible for the diverse pharmacological effects of M. oleifera, including notable antidiabetic, anti-inflammatory, and antioxidant properties.2
The therapeutic relevance of M. oleifera has become increasingly important in light of the global rise in chronic non-communicable diseases, particularly type 2 diabetes mellitus (T2DM). Diabetes mellitus now represents one of the most pressing global health challenges. According to the International Diabetes Federation, an estimated 589 million adults worldwide are living with DM by 2024, a number projected to reach 853 million by 2050.3 This dramatic increase places immense economic and social strain on healthcare systems, especially in resource-limited regions where access to affordable treatment remains difficult. In this context, M. oleifera offers a locally available, low-cost, and potentially effective nutritional product and complementary therapy. Nutritional products are regulated less stringently than medication.1,4 The Indonesian Food and Drug Authority, in the BPOM Rule number 26/2021, requires that all registered nutritional products include nutrition facts on their labels to guarantee food safety.5 The European Union in the Regulation (EU) No 609/2013 of the European Parliament on Food Intended for Infants and Young Children, Food for Special Medical Purposes, and Total Diet Replacement for Weight Control assists food manufacturers in complying with food safety regulations.6
Extensive preclinical research supports the blood sugar–lowering properties of M. oleifera through multiple mechanisms, including enhanced insulin sensitivity, improved pancreatic β-cell function, and reduced intestinal glucose absorption.7 These findings make M. oleifera a strong candidate for further development as a nutraceutical. However, translating these promising laboratory results into consistent clinical outcomes remains a challenge. Although small-scale human studies have shown encouraging effects on post-prandial blood glucose levels, results vary across populations, disease stages, and study designs. Key questions also remain: the optimal dosage, formulation of raw powder versus extract, and long-term benefits on important clinical measures, such as glycosylated hemoglobin A1c (HbA1c), inflammatory markers, and cardiovascular risk.8
To address these gaps, it is essential to evaluate the available clinical studies and clarify the therapeutic potential and safety of M. oleifera; therefore, the purpose of this narrative review is to examine published human studies and case reports on M. oleifera supplementation. Specifically, this review aimed to (1) assess the clinical efficacy and safety profile of M. oleifera across key health domains, including metabolic/endocrine, inflammatory, immunological/nutritional, maternal/child health and others; (2) explore the mechanistic insights underlying the observed clinical effects; and (3) identify current limitations and propose directions for future research to close the existing knowledge gap.
Methods
The search was conducted using major scientific databases such as PubMed, Scopus, and Google Scholar, covering studies published from January 2015 to November 2025. The search combined terms such as “Moringa oleifera,” “human studies,” “clinical trial,” “case report,” “diabetes,” “hyperglycemia,” “dyslipidemia,” “inflammation,” “oxidative stress,” “anemia,” “hematological,” “lactation,” and “galactagogue.”
The inclusion criteria were as follows: (1) human clinical studies (randomized controlled trials, controlled trials or RCTs, cohort studies) and case reports; (2) studies investigating the therapeutic, nutritional, and functional effects of M. oleifera (any plant part or extract); (3) publications written in English; and (4) publication period within the last 10 years to ensure relevance and data currency. The exclusion criteria were as follows: in vitro or animal studies, systematic reviews/meta-analyses (used for background information and contextual discussion only, and not primary data extraction), and studies lacking primary clinical data or sufficient methodological detail.
A total of 312 articles were identified through the database searches. After removing duplicates (n = 84) and screening titles and abstracts (n = 228), 43 full-text articles were assessed for eligibility. Following full-text evaluation, 31 studies met the inclusion criteria, comprising 22 human clinical trials (summarized in Table 1) and eight case reports (summarized in Table 2).
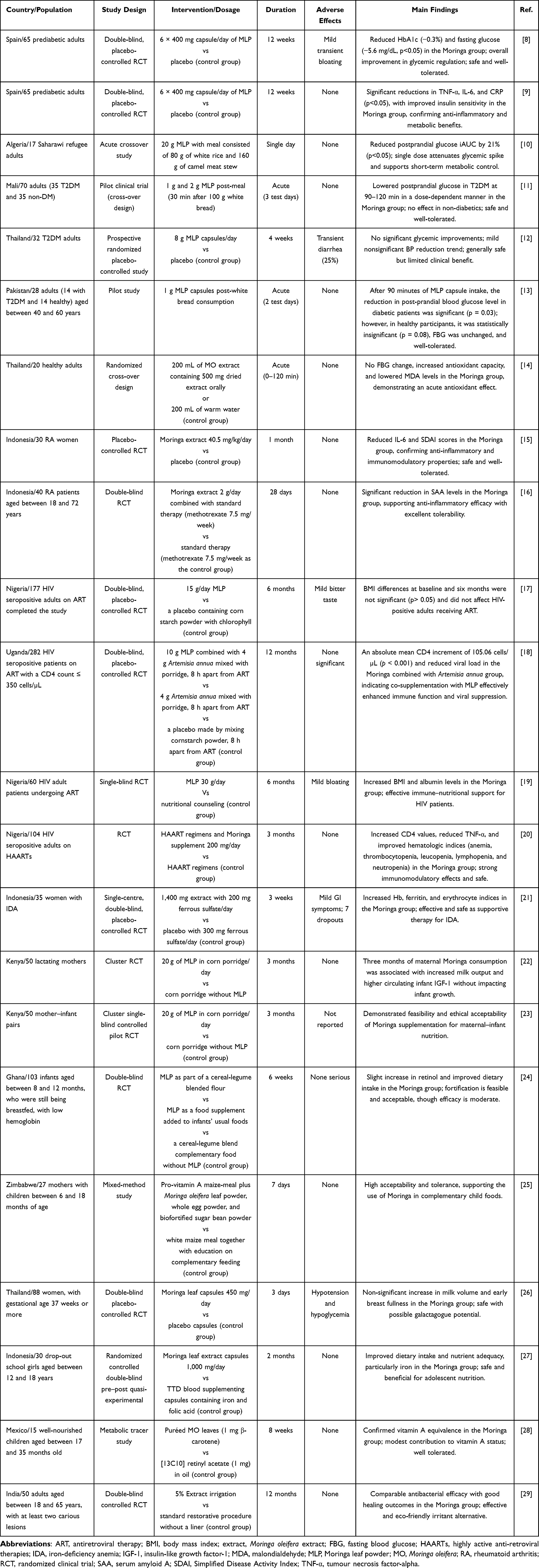 |
Table 1 Published Human Clinical Studies on Moringa oleifera |
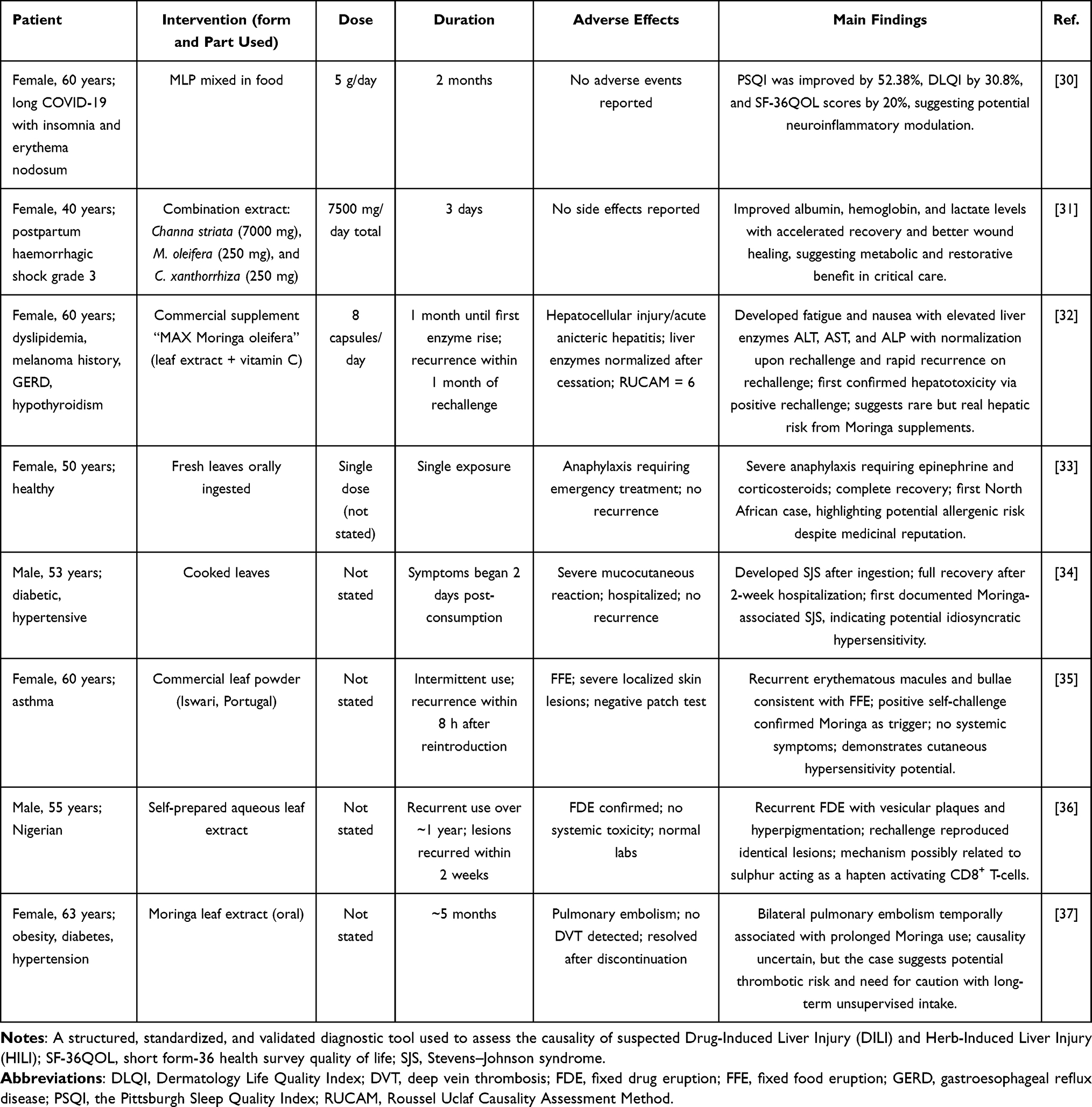 |
Table 2 Published Case Reports on Moringa oleifera |
Clinical Evidence
Clinical evidence for M. oleifera therapy in humans is rapidly accumulating, largely driven by its traditional use and robust preclinical pharmacological data. An analysis of the current literature reveals that its clinical application is largely supported by RCTs and pilot clinical studies, reflecting a focused effort to validate its use in specific health domains. The findings, while largely positive with respect to safety and efficacy in targeted areas, underscore the need for greater standardization across interventions.
Metabolic and Endocrine Disorders
Cumulative clinical evidence supports the role of M. oleifera in improving metabolic function and glycemic control. The therapeutic potential of M. oleifera in T2DM and related metabolic disorders is a primary focus of human research, with its efficacy showing a clear dependence on the stage of disease and the duration of intervention.
Two RCTs in Spain, with 65 prediabetic adults, were conducted by Gómez-Martínez et al (2021) and Díaz-Prieto et al (2022), with participants receiving 2.4 g/day of leaf powder M. oleifera capsules for 12 weeks demonstrated significant improvements in both fasting blood glucose (FBG) by −5.6 mg/dL and long-term glycemic marker, glycosylated hemoglobin (HbA1c) by −0.3%, with p < 0.05 compared to placebo, significantly lowered tumor necrosis factor-alpha (TNF-α), interleukin-6 (IL-6), and C-reactive protein (CRP). These findings indicate anti-inflammatory effects, probably mediated by the isothiocyanates and polyphenolic compounds of M. oleifera, and suggest a significant role for M. oleifera in the preventive or early management phase of T2DM.8,9
Complementary findings by Leone et al (2018), in an acute crossover study of 17 Saharawi adults, where a single 20 g dose of M. oleifera leaf powder administered with a carbohydrate-based meal resulted in a reduced postprandial glucose incremental area under the curve by 21% (p < 0.05), confirm its capacity for blunting glycemic excursions.10 Together, these results not only show the metabolic potential of M. oleifera but have also been used as a botanical adjunct in the management of early glucose dysregulation and chronic low-grade inflammation. A favorable safety profile and functional food adaptability are advantages that enhance the translational relevance of preventive metabolic health strategies.
Conversely, in patients with established T2DM, a higher dose (8 g/day) of leaf capsules administered for a shorter duration (4 weeks) failed to produce significant differences in FBG or HbA1c (0.2–0.3%) compared to controls.11 This contrasting result highlights a potential limitation in M. oleifera’s ability to reverse established chronic metabolic damage within a short timeframe. However, the acute efficacy of M. oleifera is well-supported, and a pilot study demonstrated that ingestion of the powder resulted in a significant reduction in post-prandial blood glucose (PPG) at the 90- and 120-minute marks in diabetic patients, confirming its role as an effective agent for mitigating post-prandial glucose excursions. Across all of these metabolic trials, M. oleifera was consistently well-tolerated, with no serious adverse events reported, reinforcing its safety profile.12,13
Inflammatory and Oxidative Stress-Related Diseases
The therapeutic potential of M. oleifera as an anti-inflammatory and antioxidant agent is robustly supported by its phytochemical profile; however, human evidence distinguishes between its acute and chronic effects. The most direct validation of its antioxidant capacity comes from acute studies. A randomized crossover trial demonstrated that a single 500 mg dose of M. oleifera leaf extract rapidly and significantly enhanced plasma antioxidant status, by using ferric-reducing antioxidant power (FRAP) and trolox equivalent antioxidant capacity (TEAC) within 30 min, concurrently reducing the lipid peroxidation marker, malondialdehyde (MDA).14 This functional association confirms that the M. oleifera supplement provides immediate cellular defense against systemic oxidative stress without altering the glucose levels.
Beyond acute protection, recent clinical trials have validated the direct anti-inflammatory action of M. oleifera in chronic disease models. Studies focusing on patients with rheumatoid arthritis (RA), which is a chronic autoimmune inflammatory disorder, have provided compelling evidence. A trial administering 40.50 mg/kg body weight/day of Moringa extract for one month alongside standard therapy resulted in a significant decrease in both interleukin-6 (IL-6) levels and the simplified disease activity index (SDAI) scores in the intervention group.15 The reduction in IL-6, a pivotal pro-inflammatory cytokine, indicates genuine modulation of key inflammatory pathways. This is further supported by a separate study on RA patients that investigated Moringa’s effect on serum amyloid A (SAA), an acute phase reactant.16 Collectively, these findings move Moringa’s status from a general antioxidant nutraceutical to a complementary immunomodulatory agent capable of influencing specific inflammatory biomarkers and improving clinical disease activity, although further large-scale, long-term RCTs remain necessary.
Hematological, Nutritional, and Immunological Effects
The clinical validation of M. oleifera demonstrated its multifaceted efficacy in enhancing nutritional status and supporting the immune system, particularly in vulnerable populations. The use of M. oleifera as a nutritional fortifier is strongly justified by its composition, especially in the treatment of iron-deficiency anemia. A study confirms that supplementing with Moringa leaf powder significantly improved key hematological parameters: achieving a statistically significant increase in both hemoglobin (Hb) and ferritin levels in anemic women of reproductive age compared to control groups.17 This efficacy is often superior to that predicted by the iron content alone, primarily attributed to the synergistic effect of vitamin C, which substantially enhances non-heme iron absorption. The robust nutritional profile and safety margin underscore its clinical relevance as an accessible public health intervention for anemia. Furthermore, in chronic disease management, such as people living with HIV (PLWH) receiving highly active antiretroviral therapy (HAART), low-dose Moringa supplementation (20 mg daily for three months) has been shown to improve hematological abnormalities, underscoring its role as a crucial, accessible micronutrient source.18 Crucially, across all trials, the supplementation was deemed safe and well-tolerated, with only mild, transient gastrointestinal effects reported.
M. oleifera has been demonstrated to be a promising immunomodulatory and nutritional adjuvant for PLWH undergoing antiretroviral therapy, based on compelling evidence from several African RCTs. Supplementation (15 to 30 g/day M. oleifera leaf powder for six months) consistently led to a significant increase in both CD4+ T-cell count and body mass index (BMI) in PLWH compared to placebo.19,20 A meta-analysis published in 2025 further consolidated these findings, confirming that Moringa supplementation in PLWH is effective in improving immunological indices (CD4+ counts) and hematological abnormalities.21 Critically, a 12-month, three-arm RCT in Uganda showed that 10 g/day of M. oleifera leaf powder (alone or combined with Artemisia annua) resulted in significant increases in CD4+ counts and notable decreases in viral load compared to controls.22 Across all studies, Moringa was consistently safe and well-tolerated, establishing it as an effective and accessible phytotherapeutic adjuvant for improving immune recovery and nutritional status in PLWH, especially in resource-limited settings.
Maternal and Child Health Outcomes
Several trials have been conducted to assess the applications of M. oleifera to improve maternal and infant nutrition, micronutrient status, and lactation outcomes. Attia et al (2024) conducted a cluster-RCT in Kenya among 50 lactating mothers, showing that a daily intake of 20 g of M. oleifera leaf powder over three months resulted in significantly higher α-carotene concentrations in breast milk, but did not affect serum retinol levels. The supplementation was well-tolerated, confirming its nutritional safety during lactation.23 A related pilot study, Mogaka et al (2022), confirmed the feasibility of Moringa supplementation among mother–infant pairs and strong community acceptance; thus, it was highly applicable in practice for rural maternal–child health programs.24 In Ghana, Boateng et al (2018) conducted an RCT among 103 infants (8–12 months) using complementary foods fortified with M. oleifera leaf powder (5–35 g/day) for six weeks. Although improvements in blood retinol levels did not reach statistical significance, fortified foods improved overall nutrient adequacy and were well accepted by infants and caregivers.25 Complementary formative work by Chagwena et al (2023) in Zimbabwe gave assurance of high acceptability of Moringa-enriched porridge for both mothers and children; mean sensory scores were in the range 4.4–4.9/5, while no adverse gastrointestinal events were recorded.26 Fungtammasan and Phupong (2021) from Thailand, in turn, showed a trend towards increased breast milk volume after Moringa administration of 900 mg/day for three days, and a rapid onset of breast fullness, although not statistically significant. There were no observed side effects, establishing its ethnopharmacological use as a galactagogue.27 Another positive observation by Suhartini et al (2021) was that supplementation daily with 1000 mg of Moringa extract over two months among Indonesian adolescent girls increased the dietary adequacy of nutrient intake significantly (p < 0.001), indicating its potential role in correcting undernutrition among adolescents.28 Together, these findings point out M. oleifera as one important, versatile nutritional intervention that has the potential to enhance micronutrient density, dietary adequacy, and lactation outcomes among nutritionally vulnerable populations.
Other Clinical Applications
Lopez-Teros et al (2021) investigated the vitamin A equivalence of M. oleifera leaves in 12 Mexican children using a stable isotope tracer and determined that 21 μg β-carotene from Moringa is equivalent to 1 μg retinol.29 This ensured moderate bioefficacy and very good tolerance. Anumula et al (2023) studied, in dental therapeutics, the effects of 5% M. oleifera leaf extract irrigation compared with sodium hypochlorite (NaOCl) in root canal treatment in a double-blind RCT for 12 months in India.38 Identical antibacterial and healing results were obtained for both groups, proving Moringa to be a nontoxic, safe, ecologically friendly alternative irrigant. These new applications extend the clinical applicability of M. oleifera, with the support of micronutrient intake in dental medicine.
General synthesis throughout all human clinical trials, M. oleifera showed positive effects upon immune restoration, glycemic regulation, nutritional adequacy, and functional health outcomes with very minimal undesirable side effects. The convergence of evidence across geographically and demographically distinct populations underlines its global applicability as a safe, plant-based nutraceutical. While the available evidence strongly supports its adjuvant use in HIV care, states of prediabetes, and maternal and child nutrition, additional multicenter randomized trials with standardized formulations and long-term follow-up are needed to define optimal dosing, mechanisms of action, and population-specific benefits.
The use of M. oleifera as a galactagogue (lactogenic or milk booster) represents the most clinically validated and consistent therapeutic approach in human studies. Multiple clinical trials have confirmed that M. oleifera leaf supplementation leads to a significant enhancement in the volume of breast milk output and an elevation of serum prolactin levels in postpartum mothers experiencing lactation insufficiency.39 Robust evidence fully supports its widespread traditional use and has established it as a first-line natural agent for promoting breastfeeding. However, more traditional uses of M. oleifera for wound healing, renal protection, and hepatic support are hardly represented in current human clinical research on the plant. To date, these indications lack the high-quality clinical data necessary for translation into evidence-based medical practice and therefore represent a clear priority in research.
Case Reports
Therapeutic Case Reports and Functional Improvements
Several clinical case reports have highlighted the therapeutic benefits of M. oleifera, even under complex or treatment-resistant conditions.
In a 2025 report by Rajanna and Kumari, a 60-year-old woman with chronic insomnia related to COVID-19 and erythema nodosum experienced a significant improvement after taking M. oleifera leaf powder as a standalone therapy. She received 5 g daily for two months, resulting in a 52% improvement in sleep quality (Pittsburgh Sleep Quality Index) and a 31% increase in her overall quality of life scores (p < 0.05). Notably, she did not take any other sleep medications during this period, suggesting that M. oleifera played a central role in her recovery. The authors proposed that bioactive flavonoids such as quercetin and kaempferol may have contributed to these effects by modulating gamma-aminobutyric acid-ergic (GABAergic) activity and reducing oxidative stress. This case is the first to describe M. oleifera as an effective monotherapy for long-term COVID-related neuroinflammation, broadening its potential use beyond nutrition and aligning with existing trial data that demonstrate its immune and anti-inflammatory properties.30
Another case, reported by Rahardjo in 2024, involved a critically ill postpartum woman who developed grade 3 hemorrhagic shock from a retained placenta. She was treated with a combination of M. oleifera, Channa striata, and Curcuma xanthorrhiza (7,500 mg/day for three days). This therapy led to rapid improvements in albumin, hemoglobin, and lactate levels, along with improved wound healing and recovery—without any adverse effects. While the benefit cannot be attributed solely to Moringa, this report underscores its potential contribution to restoring metabolic balance and tissue repair under severe stress. It also supports evidence from clinical trials showing M. oleifera to enhance immune and nutritional markers, particularly in patients with HIV or malnutrition.31
Rare and Adverse Reactions: Uncommon but Clinically Significant
Although M. oleifera is generally recognized as safe and non-toxic, its widespread use as a food source and dietary supplement has been linked to a growing number of isolated case reports describing rare, yet potentially serious, adverse reactions. These documented cases were classified into three major categories: hypersensitivity reactions, hepatic injury, and prothrombotic events.
A 2022 case report by Secundino et al identified M. oleifera as a rare but clinically evident cause of herb-induced liver injury (HILI). The patient was a 60-year-old woman who developed fatigue and elevated liver enzymes one month after taking M. oleifera capsules. Based on a Roussel Uclaf Causality Assessment Method (RUCAM) score of R > 8, the liver injury was classified as hepatocellular. After discontinuation, her liver function normalized; however, symptoms recurred with marked hepatic enzyme elevation (alanine transaminase or ALT, 1080 U/L, and aspartate transaminase or AST, 591 U/L) upon self-reintroduction of the supplement. This report indicates that M. oleifera may trigger acute anicteric hepatitis, a presentation previously unreported in the major DILI/HILI registries.34
M. oleifera has demonstrated the capacity to act as a potent allergen and immune-trigger, leading to reactions ranging from life-threatening immunoglobulin E (IgE)-mediated responses to severe immune-mediated dermatological syndromes. In a severe case that occurred in Tunisia, immediate anaphylaxis was reported in a 50-year-old woman who consumed fresh M. oleifera leaf. The systemic reaction, characterized by angioedema, hypotension, and respiratory distress, was confirmed to be IgE-mediated by elevated serum tryptase and positive skin tests. The patient recovered fully after emergency treatment. This case underscores that, while M. oleifera is often praised for its anti-inflammatory and anti-allergic effects, it can paradoxically trigger life-threatening allergic responses in certain individuals. Therefore, clear allergen labeling of commercial M. oleifera products is warranted.33
Witharana et al (2018) documented an extremely rare severe cutaneous adverse reaction (SCAR) in Sri Lanka. A 53-year-old man developed Stevens–Johnson syndrome (SJS) two days after consuming cooked M. oleifera leaf. The patient exhibited painful lesions affecting the skin, mouth, and genitals, highlighting the potential of common herbs to provoke severe immune-mediated reactions. After two weeks of hospital treatment, including corticosteroids and supportive care, the patient recovered completely. It should be noted that herbs such as M. oleifera can, in very rare cases, provoke severe immune-mediated reactions unrelated to dose or contamination.34
Several studies have linked M. oleifera to recurrent, well-demarcated, and fixed eruptions. One proposed mechanism involves the high sulfur content in leaf extracts, which may act as a hapten to activate CD8+ effector/memory T-cells. The diagnosis of fixed drug eruption (FDE) and fixed food eruption (FFE) is often confirmed by positive self-challenge (rechallenge) or oral provocation tests.35,36
A rare but serious event involving bilateral pulmonary embolism (PE) was reported in 2022 (Ebhohon & Miller) in a 63-year-old woman with pre-existing cardiovascular risk factors (diabetes and hypertension), after approximately five months of continuous M. oleifera leaf extract use. The condition resolved after cessation and initiation of anticoagulant therapy. Although a definitive causation could not be established, the strong temporal association and absence of other common risk factors raise the possibility of a metabolic or prothrombotic interaction. This case serves as a critical reminder of the potential dose-unrelated risks associated with unsupervised, long-term M. oleifera use, particularly in individuals with underlying cardiovascular-related diseases.37
Taken together, these reports portray M. oleifera as a plant with dual clinical identities: a promising therapeutic agent with strong antioxidant and anti-inflammatory potential, yet capable of triggering rare but serious adverse effects in sensitive individuals. The positive cases, such as improved sleep, enhanced recovery, and immune support, align with findings from controlled trials that consistently show M. oleifera to be safe, well-tolerated, and beneficial for metabolic and immune functions. In contrast, the few adverse reports appeared to be idiosyncratic, likely reflecting individual susceptibilities rather than inherent toxicities. From a clinical and regulatory perspective, these findings highlight the importance of pharmacovigilance, standardized formulations, and post-market monitoring for identifying rare hypersensitivity or thrombotic reactions. They also emphasize that healthcare providers should exercise caution when recommending M. oleifera supplements, especially for patients with existing cardiovascular, metabolic, or autoimmune conditions.
Discussion
This narrative review compiled and evaluated clinical evidence from 22 human clinical trials and 8 case reports on M. oleifera published over the past decade. Collectively, the evidence supports M. oleifera as a safe, accessible functional food and a potential adjunct therapy, particularly for managing metabolic disorders, inflammation, and malnutrition. However, while enthusiasm for its therapeutic potential is warranted, it must be balanced with an awareness of the current methodological limitations, including the lack of standardized preparations, variable dosing regimens, and the difficulty in translating preclinical results into consistent clinical outcomes.
Clinical Efficacy in Metabolic and Inflammatory Disorders
The most consistent clinical evidence highlights M. oleifera in modulating glycemic and inflammatory biomarkers, especially among individuals with prediabetes or early metabolic dysregulation. RCTs by Gómez-Martínez et al (2021) and Díaz-Prieto et al (2022) reported significant reductions in HbA1c, fasting blood glucose, and pro-inflammatory cytokines (TNF-α and IL-6), along with improved insulin sensitivity.8,9 However, several reviews have reported inconsistent or limited efficacy in patients with advanced T2DM. This discrepancy may reflect differences in pancreatic β-cell reserves.40,41 In earlier disease stages, when pancreatic β-cell function is preserved, the bioactive compounds of M. oleifera, acting as insulin secretagogues and peroxisome proliferator-activated receptor-gamma (PPAR-γ) activators, can enhance insulin signaling and glucose uptake. In contrast, in advanced T2DM, extensive β-cell loss in the islets of Langerhans may limit its restorative potential.42 Thus, M. oleifera appears to be more effective as a preventive or adjunctive intervention than as a standalone therapy for established diabetes.
The multifaceted benefits of this plant are likely driven by nutraceutical synergy, a cooperative effect among its diverse bioactive components such as quercetin, kaempferol, niazimicin, and essential micronutrients.43 Together, these compounds act on multiple metabolic pathways, including α-glucosidase inhibition, oxidative stress reduction, and nuclear factor-kappaB (NF-κB) suppression. This multi-target action represents a key strength of phytotherapy and underscores the need for network pharmacology studies to map the interactions between these compounds and their biological targets.
Mechanistic Translation and the Standardization Challenge
The clinical benefits of M. oleifera are biologically plausible and supported by a multi-target mechanism of action. The antidiabetic activity of M. oleifera is mainly attributed to its rich profile of bioactive compounds, particularly phenolic acids, flavonoids, and isothiocyanates. Mechanistically, these compounds modulate glucose homeostasis through the inhibition of α-glucosidase and dipeptidyl peptidase-IV (DPP-IV), thereby slowing intestinal glucose absorption and enhancing incretin activity.44 Additional mechanisms include improved insulin sensitivity, enhanced insulin secretion, and regulation of glycolytic and gluconeogenic enzymes.42 Furthermore, M. oleifera leaf extracts strengthen cellular antioxidant defenses, boosting catalase, superoxide dismutase, and glutathione, while reducing pro-inflammatory cytokines such as TNF-α, IL-1β, and IL-6 through modulation of the nuclear factor-kappaB (NF-κB) signaling pathway.41,45 These mechanisms underpin the observed improvements in oxidative and inflammatory biomarkers across multiple clinical trials.
Despite these promising mechanistic insights, the lack of standardization remains the most significant barrier to consistent clinical translation. The therapeutic yield of key phytochemicals such as gallic acid, kaempferol, and isothiocyanates depends heavily on factors like plant part used, solvent type, extraction method (eg, cold and hot extraction vs ultrasound-assisted extraction), and processing temperature.46 For instance, a crucial group of active compounds in M. oleifera are glucosinolates, which are converted by the enzyme myrosinase into highly bioactive isothiocyanates.47 These molecules modulate the Keap1/Nrf2 pathway, a master regulator of cellular antioxidant defense.45 However, the stability of these compounds depends heavily on processing methods. Excessive heat or boiling can deactivate myrosinase, thus preventing glucosinolate conversion and reducing its bioavailability.46
The choice of extraction solvent also influences the therapeutic profile of the bioactive compounds. Water-based extractions capture polar compounds (eg, phenolic acids), while organic solvents like ethanol or methanol extract non-polar flavonoids such as kaempferol.44 To overcome this issue, future trials must transition from crude or uncharacterized leaf powders to standardized, chemically profiled extracts with quantified marker compounds (eg, ≥10% total polyphenols or quantified glucosinolate levels).40 Only through such standardization can reproducible efficacy, dose–response relationships, and mechanistic clarity be achieved.
Safety, Toxicology, and Pharmacovigilance
In general, M. oleifera leaf preparations are validated as safe and well-tolerated in clinical studies, consistent with high LD50 values reported in preclinical studies.48 However, safety evaluations must move beyond the absence of reported adverse events in clinical trials and address the potential for harm arising from factors outside the trial protocol, specifically focusing on adulteration and HILI.
While preclinical studies often demonstrate the hepatoprotective qualities of M. oleifera extracts (eg, against bisphenol A-induced damage), M. oleifera also contains secondary metabolites, such as the alkaloids moringinin and moringin.9 Moringin has demonstrated hypoglycaemic effects, anti-inflammatory, antitumor, and mitigating neurodegenerative diseases such as Parkinson’s and Alzheimer’s diseases.49 This alkaloid defends cerebral tissue and prevents severe damage induced by focal ischemia/reperfusion,50 and was thought to contribute to the hypoglycemic activity of the plant.44 Furthermore, the clinical significance of rare case reports of severe adverse drug reactions (ADRs), such as Stevens–Johnson syndrome, cannot be dismissed.51 These severe immunological or cutaneous reactions may not be due to the natural constituents themselves, but rather to individual hypersensitivity, the concentration of toxic metabolites in less-used plant parts (eg, root, bark), or, most critically, adulteration or contamination with heavy metals or synthetic pharmaceuticals in uncertified supplements, or during processing or transportation, may lead to a pervasive problem in the global herbal market.
Therefore, although M. oleifera leaves are safe as food or nutraceutical supplements, their usage as concentrated nutraceuticals requires regulatory supervision and thorough quality control and post-market surveillance. Future studies must prioritize establishing a global safety benchmark by conducting large-scale, long-term human toxicological trials for longer than six months, and integrating pharmacovigilance data to identify rare adverse events and batch-specific safety concerns. This rigorous approach is essential for granting M. oleifera the status of a scientifically validated and safe phytomedicine.
Conclusion
M. oleifera demonstrates clinically relevant metabolic, antioxidant, and anti-inflammatory benefits, and is grounded in well-characterized biochemical mechanisms. Its safety profile remains favorable, and its affordability enhances its public health relevance in resource-limited settings. The clinical significance of rare case reports of severe ADRs, such as Stevens–Johnson syndrome, should not be ignored, pointing to the need for thorough monitoring and careful care of the patients, particularly elderly or vulnerable patients. However, methodological variability and extract standardization remain key obstacles that prevent its formal recognition as clinically validated phytomedicine. Future research should focus on conducting large-scale, multicenter RCTs using standardized extracts with defined phytochemical profiles. Performing pharmacokinetic and pharmacodynamic studies to clarify absorption, metabolism, and drug–herb interactions has also been suggested. Additionally, implementing long-term safety and pharmacovigilance frameworks to monitor rare adverse events will provide health benefits and safety guarantees for vulnerable patients. Such efforts are critical for translating M. oleifera from a traditional remedy to a scientifically substantiated, globally accepted functional nutritional or phytotherapeutic agent. Moreover, for vulnerable patients and patients with comorbidities, a risk-based approach focusing on patient safety, product quality, and potential interactions with prescription medication should be managed.
Acknowledgments
The authors thank the Rector of Universitas Padjadjaran and the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology. This narrative review is a preliminary study of the first author in the Doctorate Program in Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, West Java, Indonesia.
Funding
The article processing charge is funded by Universitas Padjadjaran through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology, and managed under the EQUITY Program (document contract number 4303/B3/DT.03.08/2025 and 3927/UN6. RKT/HK.07.00/2025).
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Pareek A, Pant M, Gupta MM, et al. Moringa oleifera: an updated comprehensive review of its pharmacological activities, ethnomedicinal, phytopharmaceutical formulation, clinical, phytochemical, and toxicological aspects. Int J Mol Sci. 2023;24(3):2098. doi:10.3390/ijms24032098
2. Kou X, Li B, Olayanju JB, Drake JM, Chen N. Nutraceutical or pharmacological potential of Moringa oleifera lam. Nutrients. 2018;10(3):343. doi:10.3390/nu10030343
3. International Diabetes Federation. IDF diabetes atlas 2025. Available from: https://diabetesatlas.org/resources/idf-diabetes-atlas-2025/.
4. Khan MAB, Hashim MJ, King JK, Govender RD, Mustafa H, Al Kaabi J. Epidemiology of type 2 diabetes: global burden of disease and forecasted trends. J Epidemiol Glob Health. 2020;10(1):107–14. doi:10.2991/jegh.k.191028.001
5. The Indonesian food and drug authority (Badan pengawas obat dan makanan) rule no. 26/2021. Available from: https://peraturan.bpk.go.id/Details/223934/peraturan-bpom-no-26-tahun-2021.
6. Stolwijk NN, Bosch AM, Bouwhuis NJ, et al. Food or medicine? A European regulatory perspective on nutritional therapy products to treat inborn errors of metabolism. J Inherited Metab Dis. 2023;46(6):1017–1028. doi:10.1002/jimd.12677
7. Watanabe S, Okoshi H, Yamabe S, Shimada M. Moringa oleifera Lam. in diabetes mellitus: a systematic review and meta-analysis. Molecules. 2021;26(12):3513. doi:10.3390/molecules26123513
8. Gómez-Martínez S, Díaz-Prieto LE, Vicente Castro I, et al. Moringa oleifera leaf supplementation as a glycemic control strategy in subjects with prediabetes. Nutrients. 2021;14(1):57. doi:10.3390/nu14010057
9. Díaz-Prieto LE, Gómez-Martínez S, Vicente-Castro I, et al. Effects of Moringa oleifera lam. supplementation on inflammatory and cardiometabolic markers in subjects with prediabetes. Nutrients. 2022;14(9):1937. doi:10.3390/nu14091937
10. Leone A, Bertoli S, Di Lello S, et al. Effect of Moringa oleifera leaf powder on postprandial blood glucose response: in vivo study on Saharawi people living in refugee camps. Nutrients. 2018;10(10):1494. doi:10.3390/nu10101494
11. Sissoko L, Diarra N, Nientao I, et al. Moringa oleifera leaf powder for type 2 diabetes: a pilot clinical trial. Afr J Tradit Complement Altern Med. 2023;17(2):29–36. doi:10.21010/ajtcan.v17i2.2
12. Taweerutchana R, Lumlerdkij N, Vannasaeng S, Akarasereenont P, Sriwijitkamol A. Effect of Moringa oleifera leaf capsules on glycemic control in therapy-naïve type 2 diabetes patients: a randomized placebo-controlled study. Evid-Based Complement Alternat Med. 2017;2017:6581390. doi:10.1155/2017/6581390
13. Amer M, Fatima SA, Gondal HHUUR, et al. Impact of Moringa oleifera on the post-prandial blood glucose level among adults in Rawalpindi, Pakistan. Int J Community Med Public Health. 2023;10(10):3545–3549. doi:10.18203/2394-6040.ijcmph20233083
14. Ngamukote S, Khannongpho T, Siriwatanapaiboon M, Sirikwanpong S, Dahlan W, Adisakwattana S. Moringa oleifera leaf extract increases plasma antioxidant status associated with reduced plasma malondialdehyde concentration without hypoglycemia in fasting healthy volunteers. Chin J Integr Med. 2016;1–6. doi:10.1007/s11655-016-2515-0
15. Prabowo NA, Nurudhin A, Werdiningsih Y, Putra DD, Putri DP, Widyastuti R. Moringa oleifera extract decreases interleukin 6 levels and disease activity in rheumatoid arthritis patients. Bangladesh J Med Sci. 2023;22(2):416–421. doi:10.3329/bjms.v22i2.65006
16. Nugroho YA, Sidharta BRA, Wardhani LO, Suparyatmo J, Pramudianti MD. SAA as inflammatory marker in rheumatoid arthritis: study on standard therapy and moringa extract. Indones J Clin Pathol Med Lab. 2023;29(3):239–244. doi:10.24293/ijcpml.v29i3.2028
17. Gambo A, Gqaleni N. Does Moringa oleifera lam. Leaves supplementation have an impact on the weight and bone mass index of people living with HIV on antiretroviral therapy? A double-blind randomized control trial. J Public Health Afr. 2022;13(3):2126. doi:10.4081/jphia.2022.2126
18. Twinomujuni SS, Atukunda EC, Mukonzo JK, Nicholas M, Roelofsen F, Ogwang PE. Evaluation of the effects of Artemisia annua L. and Moringa oleifera lam. on CD4 count and viral load among PLWH on ART: a double-blind randomized controlled clinical trial. AIDS Res Ther. 2024;21:22. doi:10.1186/s12981-024-00609-4
19. Tshingani K, Donnen P, Mukumbi H, Duez P, Dramaix-Wilmet M. Impact of Moringa oleifera lam. Leaf powder supplementation versus nutritional counseling on the body mass index and immune response of HIV patients on antiretroviral therapy: a single-blind randomized control trial. BMC Complement Altern Med. 2017;17:420. doi:10.1186/s12906-017-1920-z
20. Aprioku JS, Robinson O, Obianime AW, Tamuno I. Moringa supplementation improves immunological indices and hematological abnormalities in seropositive patients receiving HAARTs. Afr Health Sci. 2022;22(2):1–11. doi:10.4314/ahs.v22i2.2
21. Suzana D, Suyatna FD, A A, Andrajati R, Sari SP, Mun’im A. Effect of Moringa oleifera leaves extract against hematology and blood biochemical value of patients with iron deficiency anemia. J Young Pharm. 2017;9(1s):s79–84.
22. Attia SL, Owuor PM, Odhiambo SA, et al. Effect of maternal Moringa oleifera leaf supplementation on maternal and infant nutritional status and human milk output: a pilot single-blinded cluster-randomized trial. Curr Dev Nutr. 2025;9(11):107568. doi:10.1016/j.cdnut.2025.107568
23. Mogaka JN, Owuor PM, Odhiambo S, et al. Investigating the impact of Moringa oleifera supplemented to Kenyan breastfeeding mothers on maternal and infant health: a cluster randomized single-blinded controlled pilot trial protocol. JPGN Rep. 2022;3(3):e237. doi:10.1097/PG9.0000000000000237
24. Boateng L, Ashley I, Ohemeng A, Asante M, Steiner-Asiedu M. Improving blood retinol concentrations with complementary foods fortified with Moringa oleifera leaf powder: a pilot study. Yale J Biol Med. 2018;91(2):83–94.
25. Chagwena DT, Fernando S, Tavengwa NV, et al. Formulation and acceptability of local nutrient-dense foods for young children: a formative study for the child health, agriculture and integrated nutrition (CHAIN) trial in rural Zimbabwe. Matern Child Nutr. 2024;20(2):e13605. doi:10.1111/mcn.13605
26. Fungtammasan S, Phupong V. The effect of Moringa oleifera capsule in increasing breastmilk volume in early postpartum patients: a double-blind, randomized controlled trial. PLoS One. 2021;16(4):e0248950. doi:10.1371/journal.pone.0248950
27. Hadju V, Samricard R, Unde A, Bahar B. Moringa oleifera capsule and diet in young women with dropout school. Gaceta Sanitaria. 2021;35(2):S211–5. doi:10.1016/j.gaceta.2021.10.023
28. Lopez-Teros V, Ford JL, Green MH, et al. Use of a “Super-child” approach to assess the vitamin A equivalence of Moringa oleifera leaves, develop a compartmental model for vitamin a kinetics, and estimate vitamin a total body stores in young Mexican children. J Nutr. 2017;147(12):2356–2363. doi:10.3945/jn.117.256974
29. Anumula L, Ramesh S, Chinni SK, Punamalli P, Kolaparthi VSK. Clinical assessment of Moringa oleifera as a natural crosslinker for enhanced dentin bond durability: a randomized controlled trial. Cureus. 2023;15(10):e46304. doi:10.7759/cureus.46304
30. Rajanna M, Kumari VG. The effect of Moringa powder supplementation on quality of sleep in a patient of long COVID-19 syndrome insomnia with pre-existing erythema nodosum: a case report. Sleep Vigil. 2025. doi:10.1007/s41782-025-00317-7
31. Rahardjo TM, Suryawan A, Rumouw NRA, Santoso H, Faustin AJM. The effect of Channa striata, Moringa oleifera, and Curcuma xanthorrhiza extract on accelerating recovery in a ventilated patient with hemorrhagic shock grade 3 due to prolonged retained placenta: a case report. J Med Case Rep. 2024;18:120. doi:10.1186/s13256-024-04360-2
32. Secundino C, Nunes V, de Gameleira SSL, Schinoni MI, Schinono ML, Parana R. Hepatic injury induced by Moringa oleifera with rechallenge. Online J Complement Alt Med. 2022;7(3). doi:10.33552/OJCAM.2022.07.000665
33. Ichrak B. Anaphylaxis to Moringa oleifera in North Africa: a case report and review of the literature. Clin Case Rep. 2022;10(8):e6193. doi:10.1002/ccr3.6193
34. Witharana EW, Wijetunga WM, Wijesinghe SK. Stevens - Johnson syndrome (SJS) following Murunga leaf (Moringa oleifera) consumption. Ceylon Med J. 2018;63(4):188–189. doi:10.4038/cmj.v63i4.8771.
35. Amsler E, Mahevas T, Soria A, Barbaud A. Fixed food eruption to Moringa oleifera. Contact Dermatitis. 2023;89(4):301–302. doi:10.1111/cod.14383.
36. Olanrewaju FO, Onayemi O, Olasode OA, Oripelaye MM. Fixed drug eruption induced by Moringa oleifera leaf extracts: a case report. Our Dermatol Online. 2017;8(4):413–416. doi:10.7241/ourd.20174.117
37. Ebhohon E, Miller D. Moringa oleifera leaf extract induced pulmonary embolism-a case report. Int J Emerg Med. 2022;15(1):16. doi:10.1186/s12245-022-00419-3
38. Jin D, Jin S, Zhou T, et al. Effects of Moringa oleifera supplementation on immune and nutritional biomarkers in adults living with HIV: a systematic review and meta-analysis. Front Nutr. 2025;12:1667158. doi:10.3389/fnut.2025.1667158
39. Nova E, Redondo-Useros N, Martínez-García RM, Gómez-Martínez S, Díaz-Prieto LE, Marcos A. Potential of Moringa oleifera to improve glucose control for the prevention of diabetes and related metabolic alterations: a systematic review of animal and human studies. Nutrients. 2020;12(7):2050. doi:10.3390/nu12072050
40. da Silva Parente TSJ, Sarandy MM, de Araújo ERD, Gonçalves RV, Zucolotto SM. Effect of Moringa oleifera on inflammatory diseases: an umbrella review of 26 systematic reviews. Front Pharmacol. 2025; (16):1572337. doi:10.3389/fphar.2025.1572337
41. Pauzan P. Profile anti-inflammatory mechanisms of moringa leaves: a review of preclinical and clinical studies. J Biol Tropis. 2025;25(3):2605–2613. doi:10.29303/jbt.v25i3.9244
42. Krawczyk M, Burzynska-Pedziwiatr I, Wozniak LA, Bukowiecka-Matusiak M. Evidence from a systematic review and meta-analysis pointing to the antidiabetic effect of polyphenol-rich plant extracts from Gymnema montanum, Momordica charantia and Moringa oleifera. Curr Issues Mol Biol. 2022;44(2):699–717. doi:10.3390/cimb44020049
43. Gopalakrishnan L, Doriya K, Kumar DS. Moringa oleifera: a review on nutritive importance and its medicinal application. Food Sci Hum Wellness. 2016;5(2):49–56. doi:10.1016/j.fshw.2016.04.001
44. Azad SB, Ansari P, Azam S, et al. Anti-hyperglycaemic activity of Moringa oleifera is partly mediated by carbohydrase inhibition and glucose-fibre binding. Biosci Rep. 2017;37(3):BSR20170059. doi:10.1042/bsr20170059
45. Mthiyane FT, Dludla PV, Ziqubu K, et al. A review on the antidiabetic properties of Moringa oleifera extracts: focusing on oxidative stress and inflammation as main therapeutic targets. Front Pharmacol. 2022;13:940572. doi:10.3389/fphar.2022.940572
46. Fitri ZA, Ahmadi F, Islam MA, Ponnampalam EN, Dunshea FR, Suleria HAR. A systematic review of extraction methods, phytochemicals, and food applications of Moringa oleifera leaves using PRISMA methodology. Food Sci Nutr. 2025;13(4):e70138. doi:10.1002/fsn3.70138
47. Fahey J. Moringa oleifera: a review of the medical evidence for its nutritional, therapeutic, and prophylactic properties. Part 1. Trees Life J. 2005;1. doi:10.1201/9781420039078.ch12
48. Adedapo A, Mogbojuri O, Emikpe B. Safety evaluations of the aqueous extract of the leaves of Moringa oleifera. J Med Plants Res. 2009;3:586–591.
49. Borgonovo G, De Petrocellis L, Schiano Moriello A, et al. Moringin, A stable isothiocyanate from Moringa oleifera, activates the somatosensory and pain receptor TRPA1 channel in vitro. Molecules. 2020;25(4):976. doi:10.3390/molecules25040976
50. Galuppo M, Giacoppo S, Iori R, et al.4(α-L-rhamnosyloxy)-benzyl isothiocyanate, a bioactive phytochemical that defends cerebral tissue and prevents severe damage induced by focal ischemia/reperfusion. J Biol Regul Homeost Agents. 2015;29(2):343–356.
51. Sagrera A, Montenegro T, Borrego L. Cutaneous toxicity due to Moringa oleifera. Actas Dermo-Sifiliográficas Engl Ed. 2021;112(10):953–954. doi:10.1016/j.ad.2020.03.011
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Herbal Medicines as Complementary Therapy for Managing Complications in COVID-19 Patients with Diabetes Mellitus
Adha SA, Afifah NN, Latarissa IR, Iftinan GN, Kusuma ASW, Febriyanti RM, Barliana MI, Lestari K
Diabetes, Metabolic Syndrome and Obesity 2025, 18:135-146
Published Date: 16 January 2025
N-Acetylcysteine as a Potential Immunomodulator in Tuberculosis: Evidence of IL-2 Elevation in a Pilot Study
Yudhawati R, Husodo S, Aini FN
Journal of Inflammation Research 2025, 18:14381-14390
Published Date: 16 October 2025