Back to Journals » Journal of Inflammation Research » Volume 18
N-Acetylcysteine as a Potential Immunomodulator in Tuberculosis: Evidence of IL-2 Elevation in a Pilot Study
Authors Yudhawati R ![]() , Husodo S, Aini FN
, Husodo S, Aini FN
Received 5 June 2025
Accepted for publication 10 October 2025
Published 16 October 2025 Volume 2025:18 Pages 14381—14390
DOI https://doi.org/10.2147/JIR.S542396
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Yuhan Xing
Resti Yudhawati,1– 3 Septiardhi Husodo,1– 3 Faradila Nur Aini3
1Department of Pulmonology and Respiratory Medicine, Faculty of Medicine, Universitas Airlangga, Surabaya, 60132, Indonesia; 2Department of Pulmonology and Respiratory Medicine, Universitas Airlangga Teaching Hospital, Surabaya, 60015, Indonesia; 3Department of Pulmonology and Respiratory Medicine, Dr. Soetomo General Academic Hospital, Surabaya, 60286, Indonesia
Correspondence: Resti Yudhawati, Department of Pulmonology and Respiratory Medicine, Faculty of Medicine, Universitas Airlangga – Universitas Airlangga Teaching Hospital – Dr. Soetomo General Academic Hospital, Jl. Prof. Dr. Moestopo 47, Surabaya, 60132, Indonesia, Email [email protected]
Purpose: Aimed to investigate the potential of N-acetylcysteine (NAC) as an adjunctive immunomodulatory therapy to support the host immune response against Mycobacterium tuberculosis by enhancing interleukin-2 (IL-2) production.
Patients and Methods: A quasi-experimental study was conducted on the effect of NAC administration on IL-2 levels in patients newly diagnosed with pulmonary tuberculosis at Universitas Airlangga Teaching Hospital, Indonesia. Participants who met the inclusion criteria were subsequently divided into two groups: treatment group (received 600 mg every 12 hours of NAC therapy, n = 15) and control group (did not receive NAC therapy, n = 15). Enzyme-linked immunosorbent assay (ELISA) was used to analyze IL-2 levels in both groups, which were subsequently compared using statistical analysis.
Results: Analysis of IL-2 levels before treatment with NAC revealed no significant difference between the treatment and control groups. The treatment group exhibited a significant increase in IL-2 levels after NAC administration (p=0.023). The median IL-2 level in the treatment group increased from 243.7 to 386.62 ng/L after two weeks of NAC administration, whereas in the control group, it decreased from 303.6 to 285.89 ng/L. The comparison test analysis of delta IL-2 levels also showed a significant difference between the treatment and control group (p = 0.025), with the median value of delta IL-2 levels in the treatment group being 147.0 ng/L and − 24.7 ng/L in the control group.
Conclusion: This preliminary study demonstrated that IL-2 levels significantly increased with NAC supplementation, suggesting an enhanced immune response and its potential as an adjunct to standard tuberculosis therapy.
Keywords: N-acetylsistein, IL-2, tuberculosis, immunomodulator, antioxidant
Introduction
Tuberculosis (TB) is an infectious disease that is responsible for significant health issues worldwide as one of the leading causes of death from a single infectious agent following 3 years in which it was replaced by coronavirus disease (COVID-19), and caused nearly double the number of deaths as human immunodeficiency virus (HIV)/AIDS.1 According to the Global Tuberculosis Report 2024 by World Health Organization (WHO), TB affects 10.8 million people, including 6.0 million males, 3.6 million females, and 1.3 million children, with a mortality rate of 1.25 million in 2023.2 The host immune response is essential in regulating Mycobacterium tuberculosis (M. tb) infection, with interleukin-2 (IL-2) serving as a key cytokine in T-cell activation and proliferation.3
The reduction in immune function observed in active TB is attributed to the depletion of IL-2 supply.4 IIL-2 is a pro-inflammatory cytokine produced by T cells (Th1) that contributes significantly to the immunopathogenesis of M. tb infection.5 IL-2 stimulates the proliferation and differentiation of CD4+ and CD8+ T cells, natural killer (NK) cells, and B lymphocytes via a positive feedback loop. IL-2 exerts autocrine effects on CD4+ and CD8+ T cells, promoting CD4+ T cell differentiation toward Th1 and enhancing CD8+ T cell activity and memory formation. In addition, IL-2 acts in a paracrine manner to augment NK cell cytotoxic activity.6 However, IL-2 is rapidly used by activated T cells in active TB, resulting in its depletion. An imbalance in the number or function of T cells caused by this depletion can disturb the formation of granulomas, allowing M. tb to evolve into active TB.4,7 The description above reflects the typical immune response in TB patients. In patients who have previously received TB therapy or in retreatment cases, there is a notable decrease in TNaive cells, together with a reduction in effector T cell activity, particularly in Th1 cytokine production.8,9
Recent studies have suggested that NAC, a known antioxidant and mucolytic agent, may also possess immunomodulatory properties.10,11 NAC may help improve the efficiency of IL-2 production by T cells without worsening the existing immune imbalance. Its role is more immunomodulatory rather than immunostimulatory. By reducing oxidative stress, NAC can contribute in restoring impaired T-cell function and enable a more stable and sustained production of IL-2.12,13 However, to the best of our knowledge, although studies on NAC in TB cases exist, none have specifically investigated its potential effect on cytokine profiles, particularly IL-2 in humans. Existing evidence coming from other conditions besides TB,14 or performed in animal models, both in vitro and in vivo. According to an in vitro study by Guerra et al,15 administration of 20 mM NAC resulted in a positive effect on the treatment of IL-2 and IL-12 in 23 samples. The study revealed a glutathione (GSH)-related pathway that enhances NK cell function against TB infection by inhibiting the growth of M. tb strains (H37Rv) by threefold.16 NAC elevates intracellular GSH, thereby boosting the immune activity of NK cells and macrophages and potentially enhancing immunity against M. tb through increased IL-2 production.4 In contrast, the absence of NAC resulted in no significant increase in IL-2 levels. Increasing cellular GSH through various cytokines and NAC has been demonstrated to improve the effects on NK cells while reducing M. tb proliferation. In addition, NAC reduces the production of IL-10, a cytokine that promotes mycobacterial proliferation, as well as pro-inflammatory cytokines such as IL-1, IL-6, and TNF-α, which are known to aggravate oxidative stress.17–19 Therefore, this study makes an attempt to translate the findings of the above laboratory studies into real clinical conditions.
Considering the high prevalence of pulmonary TB in Indonesia and the absence of prior human studies evaluating the effect of NAC on IL-2 levels, this pilot study is the first to assess the effect of NAC supplementation on IL-2 concentrations in patients with newly diagnosed pulmonary TB. This study investigated the potential of NAC to enhance IL-2 production, with the aim of providing preliminary evidence for its role as an adjunctive immunomodulatory therapy to support the host immune response against M. tb.
Materials and Methods
Study Design and Subjects Characteristics
This quasi-experimental study on the effect of NAC administration on IL-2 levels in patients with newly diagnosed pulmonary TB employed a pre- and post-control group design. The subjects were patients diagnosed with new cases of pulmonary TB between May and August 2024 at the Universitas Airlangga Teaching Hospital, Surabaya, Indonesia. Consecutive sampling was implemented while complying with the inclusion and exclusion criteria, and the treatment and control groups were randomized using a simple randomization method.
Inclusion criteria included adults aged 18 years and older; new cases of bacteriologically confirmed pulmonary TB patients based on GeneXpert MTB/RIF assay result who had not initiated anti-TB therapy; and willingness to participate in the study by completing an informed consent form. Participants who met the inclusion criteria were subsequently divided into two groups: treatment group (who received an additional 600 mg every 12 hours of NAC therapy) and control group (who did not receive any additional NAC therapy). Pregnant and lactating women, individuals infected with HIV, those suffering from autoimmune diseases or currently using immunosuppressive drugs, individuals with severe chronic comorbidities such as cancer, and individuals who 2 weeks prior to study consumed antioxidant supplements were excluded. The following criteria were used to drop out participants: non-compliance with the administration of anti-tuberculosis medications and NAC (<100%), absence of IL-2 levels due to patients not attending the final assessment after two weeks of NAC administration, and allergy to NAC.
Questionnaire
A pre-tested questionnaire was used to collect information on demographic characteristics (name, age, address, gender, phone number, occupation), medical history (clinical complaints or symptoms, current comorbidity history, history of TB disease, history of TB treatment, history of antioxidant supplements consumption, family medical history, history of drug allergies), special conditions (eg, pregnancy), and history of contact with TB patients. Physical examination was conducted, including weight, height, vital signs (blood pressure, pulse, temperature, and respiration rate), and head, neck, thorax, abdomen, and extremity examinations. All participants were interviewed face to face.
Plano Test Examination
Planotest kit (Sensitif – PT Danpac Pharma, Jakarta, Indonesia) was used for all female samples to detect pregnancy, which is an exclusion criterion. Urine was collected for this test and the pregnancy test strip was dipped into a specific line. The outcomes of the strips were evaluated after 2–3 minutes.
Monitoring and Evaluation of Treatment Adherence
Each participant was supplied with a self-monitoring card to assess patient adherence to NAC administration (600 mg every 12 h) and to standard anti-TB treatment by marking each dose taken daily on the card. Regular follow-up phone calls were made to reinforce and monitor participants’ adherence. The participants received reminders about the dosing schedules and were encouraged to report any missed doses or adverse events during the call to improve compliance and reduce recall bias.
Examination of Interleukin-2 Levels
Venous blood samples of 10 cc were collected from the patients using a 5-cc spuit and subsequently divided into two blood vials, each containing 5 cc. The samples were placed in a cool box and transported to the KALGen INNOLAB Laboratory for centrifugation and storage. Blood sampling was performed twice: first, on day 1 before receiving NAC and anti-TB treatment, and secondly on day 15.
IL-2 levels were measured at the KALGen INNOLAB Laboratory using the Human Interleukin 2 ELISA Kit obtained from Bioassay Technology Laboratory Co., Ltd., Wuhan, China (Cat. No. E0094Hu), following the manufacturer’s instructions. The blood samples were allowed to clot at room temperature for 10–20 minutes before centrifugation at 3000 rpm for 20 minutes. The resulting serum samples were aliquoted and stored at 2°C until further analysis. Prior to the assay, all the reagents and samples were stored at room temperature. Standard and serum samples were added in duplicate to a 96-well microplate precoated with a monoclonal antibody specific for human IL-2. After incubation with the biotinylated detection antibody, streptavidin-HRP was added to bind to the biotinylated IL-2 antibody. After incubation, unbound streptavidin-HRP was thoroughly washed. Following the washing step, the substrate solution was added and the color developed in proportion to the amount of Human IL-2. The plate was then incubated in the dark at 37°C for 15–20 minutes. The reaction was stopped by adding stop solution, and absorbance was measured at 450 nm using a microplate reader.
Ethics Statement
Written informed consent for publication was obtained from study participants. Informed consent for adults who are not capable of giving informed consent due to age, physical incapacity, or local ethical requirements, consent was obtained from a parent, legal guardian, or next of kin. The study was performed in accordance with the ethical principles of the Declaration of Helsinki and was approved by the Institutional Review Board of the Universitas Airlangga Teaching Hospital (registration number: 058/KEPK/2024).
Statistical Analysis
Data were recorded on data collection sheets that were arranged, processed, and analyzed using computer software. IBM SPSS Statistics V.30 program was used to analyze the data. The statistical analysis used to test the difference in IL-2 levels between the treatment and control group was an independent t-test for normally distributed data and the Mann–Whitney test for data that were not normally distributed. IL-2 was analyzed before and after NAC administration using the paired t-test analysis test for normally distributed data and Wilcoxon test for data that were not normally distributed.
Results
Characteristics of Research Subjects
Thirty subjects who met the inclusion and exclusion criteria were subsequently divided into two groups: 15 in the treatment group and 15 in the control group. The general characteristics of the study participants, including gender, age, and comorbidities, are presented in Table 1. The majority of the subjects in each group were male: 10 (66.7%) in the treatment group and 11 (73.3%) in the control group. The distribution of the gender between the two group according to the chi-squared test was not significantly different (p=1.000) (Table 1).
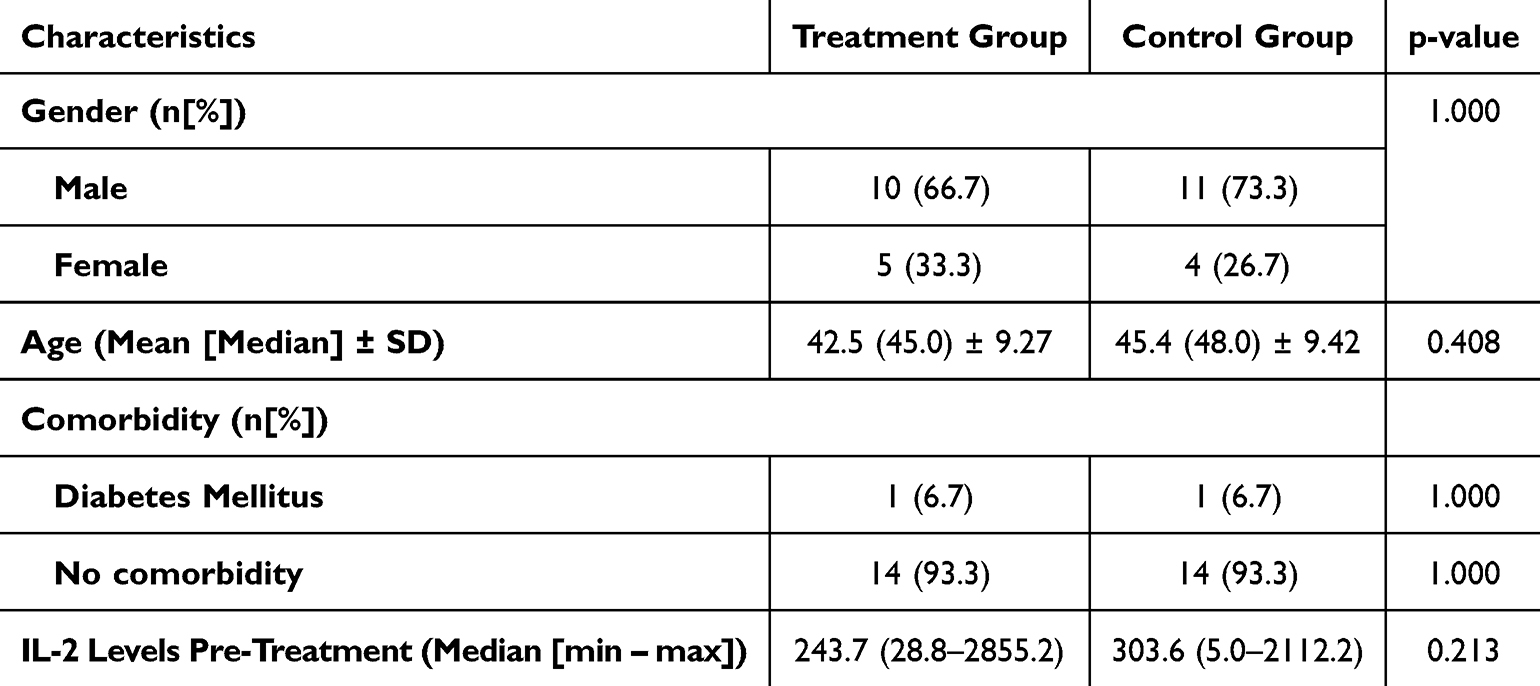 |
Table 1 Characteristics of the Subjects |
A normality test using the Shapiro–Wilk method of age distribution indicated that the data were normally distributed. The mean (median) ± SD age distribution in both group is presented in Table 1. According to the chi-square test, the age distribution between the treatment and control group was not significantly different (p>0.05) (Table 1).
Most subjects reported no comorbidities. Only 2 subjects had diabetes mellitus as a comorbidity, with 1 subject (6.7%) in each group. Similarly, no significant differences were observed in the comorbidity distribution (p>0.05). Additionally, analysis of IL-2 levels prior to NAC treatment revealed no significant differences between the treatment and control group (Table 1).
IL-2 Levels in the Treatment and Control Groups Pre- and Post-NAC Treatment
The data obtained from the normality test of IL-2 levels using the Shapiro–Wilk method indicated that all variables, including delta IL-2 and IL-2 levels before and after the intervention, were not normally distributed. Consequently, the data analysis in this study employed the non-parametric Wilcoxon signed-rank test and Mann–Whitney U-test.
The median IL-2 levels in the treatment group prior to NAC and control group prior to NAC treatment in new cases of pulmonary TB patients were 243.7 ng/L and 303.6 ng/L, respectively (Table 2).
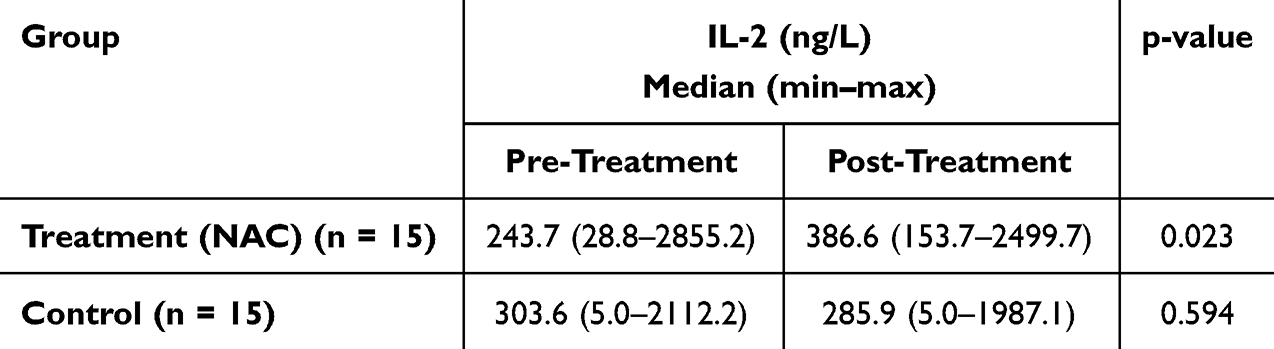 |
Table 2 IL-2 Levels in the Treatment and Control Groups Pre- and Post-NAC Treatment |
The median IL-2 level in the treatment group increased to 386.62 ng/L after two weeks of NAC administration, whereas it decreased to 285.89 ng/L, as presented in the control group (Table 2).
The treatment group exhibited a statistically significant increase in IL-2 levels following administration of NAC (p=0.023). In contrast, no significant differences were observed in the control group (p=0.594) (Table 2). Figure 1 shows that the median IL-2 level following NAC administration was higher than that before NAC administration.
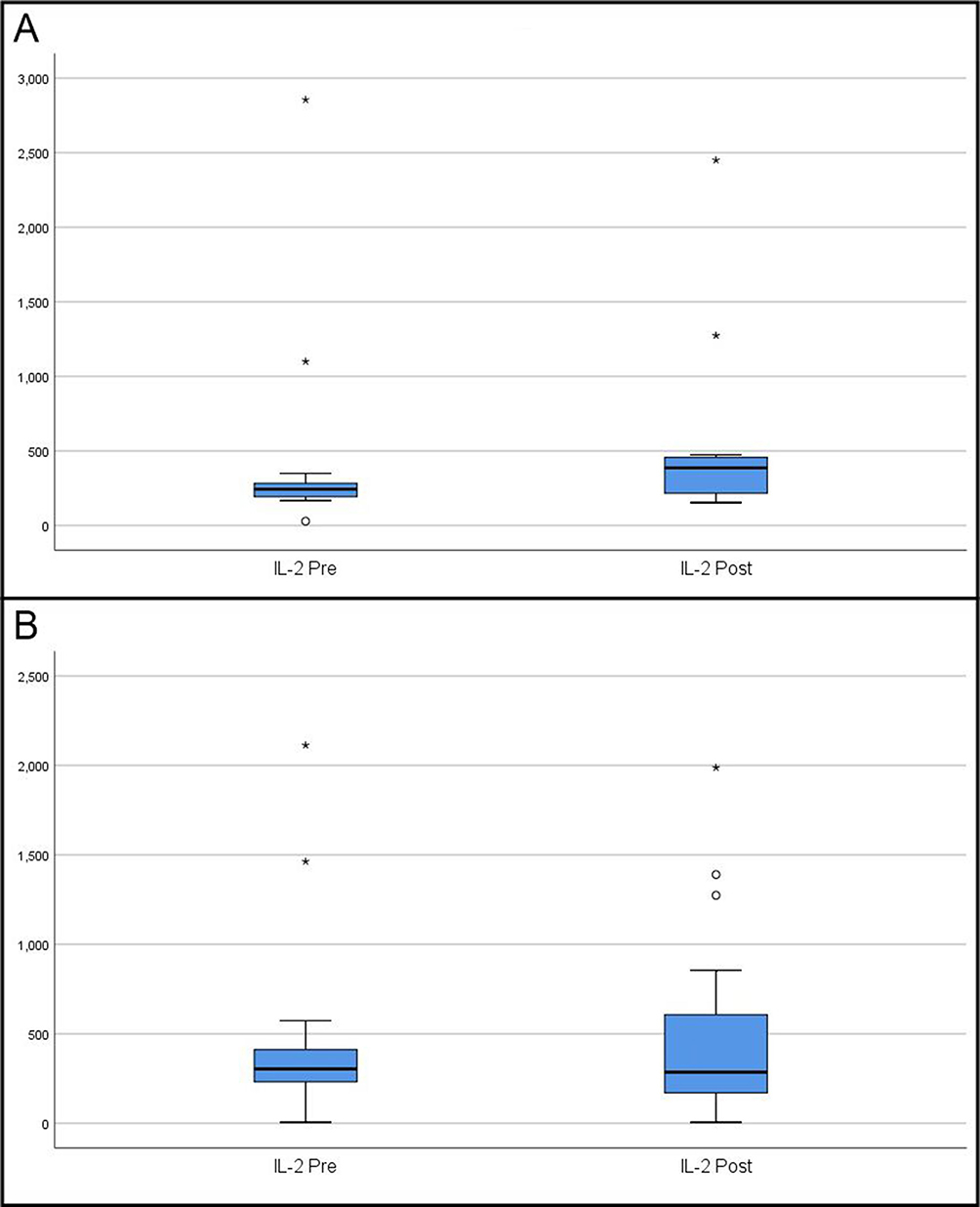 |
Figure 1 Interleukin-2 (IL-2) levels in new pulmonary tuberculosis cases before (Pre) and after (Post) N-acetylcysteine (NAC) administration in (A) Treatment group: the median IL-2 level increased significantly after two weeks of NAC (p = 0.023). (B) Control group: the median IL-2 level decreased with no significant change (p = 0.594). Boxplots represent the median (horizontal line), interquartile range (box), and minimum–maximum values within 1.5× IQR (whiskers). *Indicates extreme outliers (values > 3× IQR). oIndicates moderate outliers (values > 1.5× but < 3× IQR). |
Comparative Analysis of IL-2 Levels Between Treatment and Control Groups
The delta value of IL-2 level was calculated by subtracting the values obtained after and before NAC treatment. The median delta IL-2 levels in the treatment group were 147.0 ng/L, while a decrease observed in control group with a median delta value of −24.7 ng/L (Table 3). Analysis of the delta value of IL-2 levels between the treatment and control groups revealed a significant difference (p=0.025), indicating that NAC administration positively influenced IL-2 levels. Comprehensive data outcomes are presented in Table 3 and Figure 2.
 |
Table 3 Comparison Test Analysis of Delta IL-2 Levels in the Treatment Group and Control Group |
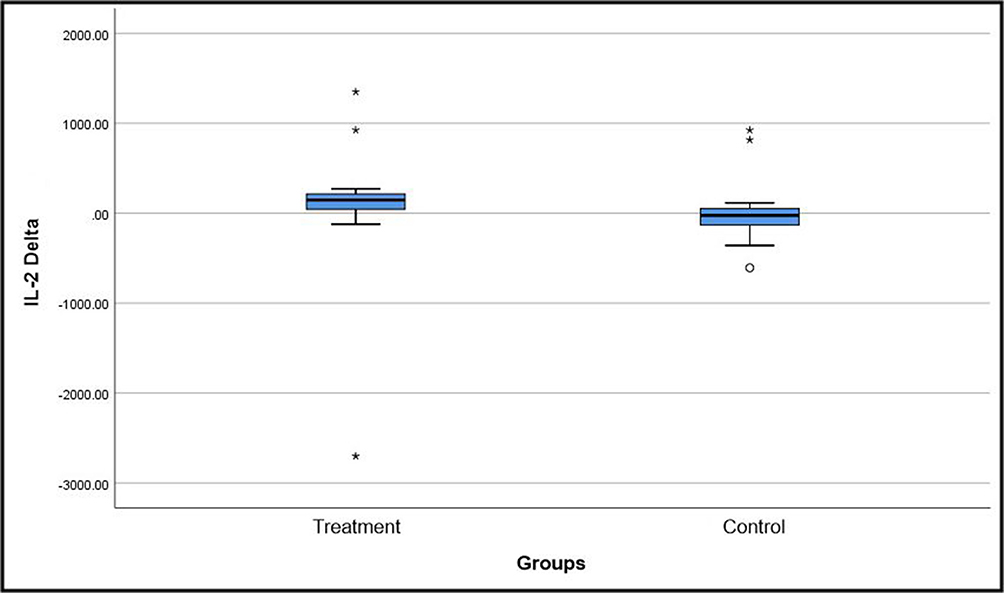 |
Figure 2 Changes in interleukin-2 (IL-2) levels (Delta = Post – Pre) in new pulmonary tuberculosis patients. The treatment group showed a significant overall increase after NAC, while the control group exhibited no meaningful change. Significant difference (p=0.025) observed in the delta value of IL-2 levels between the treatment and control groups. *Indicates extreme outliers (values > 3× IQR). oIndicates moderate outliers (values > 1.5× but < 3× IQR). |
Evaluation of Treatment-Related Adverse Effects
The reported side effects after administration of 600 mg NAC every 12 h for 14 days in the treatment groups were mild gastrointestinal disturbances, including nausea and abdominal discomfort, which occurred in only one subject (6.7%). The reported side effects were mild and lasted only for one day, and discontinuation of the treatment was not required.
Discussion
The IL-2 levels observed over two weeks after NAC administration showed that the median IL-2 levels were higher in the treatment group than in the control group. These results are consistent with those of previous in vitro study that demonstrated a beneficial role of NAC in the treatment of active TB. The study reported that 10 mM NAC therapy, which elevated IFN-γ, IL-12, and IL-2 levels in vitro. This finding shows that cytokine balance is important for proper immune response against M. tb, and the proper ratio and proportion of the type of cytokines is crucial for the correct and efficient response against TB.19 Study by Viora et al,20 supported these results by showing upregulated secretion of IL-1β, IL-2, IL-12, and IL-15 in phytohaemagglutinin (PHA)-stimulated peripheral blood mononuclear cells (PBMC) treated with NAC. The production of IL-2 by CD4-positive cells from diabetic NOD donor mice was also reported to be significantly enhanced by NAC in vitro.21
Comparative analysis of IL-2 levels in both group monitored over two weeks showed that the group receiving NAC therapy experienced a significant increase in IL-2 levels. On the other hand, in the control group, the IL-2 levels relatively decreased, indicating that there was not enough additional stimulus to enhance the cellular immune response during the two-week monitoring period. NAC predominantly increases IL-2 by acting as an antioxidant, which restores cellular redox balance, enhances T cell activation and function, and influences IL-2 gene transcription by regulating signalling pathways such as NF-κB. This theory aligns with the literature, indicating that NAC consists of several important functional groups, including acetyl group (-COCH3), carboxylate group (-COOH), amine group (-NH2), and thiol group (-SH). The thiol group is the most critical component of NAC biological activity. The free thiol group is responsible for the direct antioxidant activity of NAC due to the capability of reacting with reactive oxygen and nitrogen species (RONS). In experimental settings, NAC rapidly interacts with hydroxyl radicals (●OH), nitrogen dioxide (●NO2), carbon trioxide ion (CO3●–), and thiyl radical (RS●), as well as nitroxyl (HNO), the reduced and protonated form of nitric oxide (●NO).22,23 Literature also mentioned that NAC, as a potent antioxidant, potentially acts as an immunomodulator that is directly linked to its ability to increase levels of intracellular cysteine with a subsequent increase in GSH, consequently reducing oxidative stress in immune cells.23 NAC according to the literature, is a low-molecular-weight thiol compound, in which deacetylation results in elevated levels of intracellular cysteine. Cysteine may be a limiting factor in GSH synthesis, and NAC has been demonstrated to elevate GSH levels in some cell types.24 The precise metabolic mechanism of NAC increases the intracellular pool of GSH and directly scavenges oxidants remains unclear. Literature suggests that NAC is transported into cells and then hydrolyzed, consequently inducing the synthesis of GSH.25
The elevated levels of intracellular GSH and regulation of NF-κB by NAC, results in the inflammation and oxidation reduction.26 NAC treatment in vivo and in vitro induced a Th1 response by elevating the intracellular GSH level in antigen-presenting cells.27 GSH supplementation also increased Th1 cytokines, such as IL-2, IL-12, IFN-γ, and TNF-α.28 NAC enhances T cells by activating the PI3K/Akt pathway and suppressing Foxo1, while also reducing ROS levels through the indirect increase of small hydrophobic proteins. GSH has been demonstrated to stimulate T cell growth and metabolism. Thiol-mediated regulation of IL-2 secretion is essential for T cell proliferation. T cell proliferation requires reduced thiols but not necessarily GSH.24,29,30
IL-2, a multipotent cytokine synthesized after antigen activation, which is essential for the immune response, may play a critical role against M. tb. Identified in the supernatants of activated T cells, and is capable of mediating human T cell growth and proliferation, IL-2 additionally enhances CD8+ T cell and NK cell cytolytic activity, while also modulating T cell differentiation programs in response to antigen. Specifically, it promotes the differentiation of naïve CD4+ T cells into T helper-1 (Th1) and T helper-2 (Th2) cells, concurrently inhibiting the differentiation of T helper-17 (Th17) and T follicular helper (Tfh) cells.30,31 The adaptive immune system is primarily composed of T lymphocytes (T cells), which are responsible for mediating cell-based immune responses to maintain the health of the host and prevent the development of a variety of diseases.32 Progressive impairment of M. tb-specific T-cell responses can result from chronic M. tb infection. This impairment is inversely proportional to the mycobacterial load and can be partially restored during anti-mycobacterial therapy.33 M. tb-specific CD4+ and CD8+ T cells ex vivo exhibit reduced production of IFN-γ, TNF-α, and IL-2, as predicted from exhausted T cells.34,35 A meta-analysis study investigated IL-2, IL-5, IL-13, IFN-γ, IL-10, and TNF-α in 14 studies with 982 subjects to assist the distinction between active TB and latent tuberculosis infection (LTBI), and IL-2 with the highest overall accuracy.36 This was also supported by another systematic review and meta-analysis that included 58 reports, accounting for 9291 participants, showing that IL-2 level after stimulation with latent antigen is a potential biomarker for differentiating TB from LTBI.37 These facts demonstrate that IL-2 may serve as a biomarker in tuberculosis patients and is significant in the immunological response to tuberculosis infection.
In this study, the adverse effects that manifested after NAC administration for two weeks were classified as minor, specifically gastrointestinal. Literatures indicate that the toxic effects of NAC are only observed at very high doses, above 6 g/kg when administered orally and above 2 g/kg when administered intravenously. When administered orally, NAC is rapidly absorbed and metabolized in the intestine and liver. Following oral treatment, the maximum plasma concentration (Cmax) occurs within 1–2 h.23,38 The side effects of NAC range from mild to severe, depending on the formulation and dosage. However, multicenter studies have demonstrated that both intravenous and oral NAC are associated with minimal side effects. In oral administration, the most common side effects were gastrointestinal symptoms, such as nausea, vomiting, and diarrhea, as well as rhinorrhea, itching, and erythema.23,38 Additionally, moderate side effects, including gastrointestinal reactions, such as dyspepsia, diarrhea, sweating, and erythema, have been reported in other literature when NAC was administered orally at a dose of 150 mg/kg. Compared with intravenous administration, oral administration induces significantly fewer adverse effects.39,40 Notably, the adverse effects may also be attributed to the anti-TB drug treatment received by the subjects; therefore, further analysis is required.
Maintaining or increasing IL-2 levels may be essential for enhancing treatment outcomes and accelerating recovery, considering the critical function of IL-2 in regulating the cellular immune response against M. tb. These findings support our initial hypothesis that NAC supplementation has the potential to improve the immunological status of newly diagnosed TB patients by acting as an immunomodulator via the upregulation of IL-2 production. However, it should be noted that this study did not examine IL-2 levels in healthy individuals; therefore, baseline values cannot be compared between patients with active TB and healthy individuals. Therefore, inclusion of healthy controls in future studies is required to provide baseline reference values. Additionally, there was no control over the consumption of foods containing natural NAC, which may have independently affected the IL-2 levels. Future study may include a brief dietary questionnaire identify the consumption of foods containing antioxidants and foods rich in L-cysteine, with examples of such foods provided. This is a pilot study with a short observation period. Further research should consider conducting clinical trials with longer duration and larger sample sizes, while also exploring dose–response relationships and the role of NAC at different phases of TB treatment. This study evaluated only one immunological marker (IL-2) while not addressing any clinical outcomes (eg, improvement in symptoms; weight gain), microbiological outcomes (eg, sputum smear or culture conversion), or radiological outcome. Future research is needed to assess clinical, microbiologic, as well as radiological end points and investigate other cytokines as well as broader immunologic profiles in an effort to more fully elucidate the immunomodulatory effect of NAC.
Conclusion
A significant elevation in IL-2 levels was observed in patients receiving NAC supplementation, indicating an improvement in immunological response. These findings suggest that NAC may be beneficial as an adjunctive agent to standard anti-TB therapy for newly diagnosed pulmonary TB cases. Nevertheless, as this study presents preliminary results and exploratory investigation, further well-designed large-scale clinical trials are required to verify these observations before definitive clinical recommendations can be made.
Abbreviations
AFB, acid-fast bacillus; GSH, glutathione; HIV, human immunodeficiency virus; IL-, interleukin-; LTBI, latent tuberculosis infection; M. tb, Mycobacterium tuberculosis; NAC, N-acetylcysteine; NK, natural killer; PBMC, peripheral blood mononuclear cell; TB, tuberculosis; Tfh, T follicular helper; Th, T helper-.
Data Sharing Statement
All data underlying the results are available as part of the article and no additional source data are required.
Acknowledgments
We would like to show our gratitude to the patients and their guardians of our research. We would also thank the members of the Department of Pulmonology and Respiratory Medicine, Medical Faculty of Airlangga University for their helpful discussions and contributions. We are also immensely grateful to Nimas Roro Gayatri for helping with the editing and proofreading process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. World Health Organization (WHO). Tuberculosis. Available from: https://www.who.int/news-room/fact-sheets/detail/tuberculosis.
2. World Health Organization (WHO). Global Tuberculosis Report; 2024. Available from: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2024.
3. Zhuang L, Li L, Yang L, Ye Z, Gong W. Mycobacterium tuberculosis: immune response, biomarkers, and therapeutic intervention. MedComm. 2024;5(1):e419. doi:10.1002/mco2.419
4. Allen M, Bailey C, Cahatol I, et al. Mechanisms of control of Mycobacterium tuberculosis by NK cells: role of glutathione. Front Immunol. 2015;6:508. doi:10.3389/fimmu.2015.00508
5. Qiu X, Wang H, Tang Y, et al. Is interleukin-2 an optimal marker for diagnosing tuberculosis infection? A systematic review and meta-analysis. Ann Med. 2020;52(7):376–385. doi:10.1080/07853890.2020.1800073
6. Liao W, Lin JX, Leonard WJ. Interleukin-2 at the crossroads of effector responses, tolerance, and immunotherapy. Immunity. 2013;38(1):13–25. doi:10.1016/j.immuni.2013.01.004
7. Romero-Adrian TB, Leal-Montiel J, Fernández G, Valecillo A. Role of cytokines and other factors involved in the Mycobacterium tuberculosis infection. World J Immunol. 2015;5(1):16–50. doi:10.5411/wji.v5.i1.16
8. Petrone L, Peruzzu D, Altera AMG, et al. Therapy modulates the response to T cell epitopes over the spectrum of tuberculosis infection. J Infect. 2024;89(6):106295. doi:10.1016/j.jinf.2024.106295
9. Yao X, Cai H, Chen J, et al. Increased long-term central memory T cells in patients with retreatment pulmonary tuberculosis. Front Immunol. 2025;16:1545537. doi:10.3389/fimmu.2025.1545537
10. Amaral EP, Conceição EL, Costa DL, et al. N-acetyl-cysteine exhibits potent anti-mycobacterial activity in addition to its known anti-oxidative functions. BMC Microbiol. 2016;16(1):251. doi:10.1186/s12866-016-0872-7
11. Shiozawa A, Kajiwara C, Ishii Y, Tateda K. N-acetyl-cysteine mediates protection against Mycobacterium avium through induction of human β-defensin-2 in a mouse lung infection model. Microbes Infect. 2020;22(10):567–575. doi:10.1016/j.micinf.2020.08.003
12. Eylar E, Rivera-Quinones C, Molina C, Báez I, Molina F, Mercado CM. N-acetylcysteine enhances T cell functions and T cell growth in culture. Int Immunol. 1993;5(1):97–101. doi:10.1093/intimm/5.1.97
13. Sahasrabudhe SA, Terluk MR, Kartha RV. N-acetylcysteine pharmacology and applications in rare diseases-repurposing an old antioxidant. Antioxidants. 2023;12(7):1316. doi:10.3390/antiox12071316
14. Emet S, Memis D, Pamukçu Z. The influence of N-acetyl-L-cystein infusion on cytokine levels and gastric intramucosal pH during severe sepsis. Crit Care. 2004;8(4):R172–R179. doi:10.1186/cc2866
15. Guerra C, Johal K, Morris D, et al. Control of Mycobacterium tuberculosis growth by activated natural killer cells. Clin Exp Immunol. 2012;168(1):142–152. doi:10.1111/j.1365-2249.2011.04552.x
16. Venketaraman V, Millman A, Salman M, et al. Glutathione levels and immune responses in tuberculosis patients. Microb Pathog. 2008;44:255–261. doi:10.1016/j.micpath.2007.09.002
17. Magalhães LS, Melo EV, Damascena NP, et al. Use of N-acetylcysteine as treatment adjuvant regulates immune response in visceral leishmaniasis: pilot clinical trial and in vitro experiments. Front Cell Infect Microbiol. 2022;12:1045668. doi:10.3389/fcimb.2022.1045668
18. Cazzola M, Calzetta L, Facciolo F, Rogliani P, Matera MG. Pharmacological investigation on the anti-oxidant and anti-inflammatory activity of N-acetylcysteine in an ex vivo model of COPD exacerbation. Respir Res. 2017;18:26. doi:10.1186/s12931-016-0500-y
19. Guerra C, Morris D, Sipin A, et al. Glutathione and adaptive immune responses against mycobacterium tuberculosis infection in healthy and HIV infected individuals. PLoS One. 2011;6:E28378. doi:10.1371/journal.pone.0028378
20. Viora M, Quaranta M, Straface E, Vari R, Masella R, Malorni W. Redox imbalance and immune functions: opposite effect of oxidized low-density lipoproteins and N-acetylcysteine. Immunol. 2001;104:431–438. doi:10.1046/j.1365-2567.2001.01334.x
21. Yim CY, Hibbs JB, McGregor JR, Galinsky RE, Samlowski WE. Use of N-acetyl cysteine to increase intracellular glutathione during the induction of antitumor responses by IL-2. J Immunol. 1994;152:5796–5805. doi:10.4049/jimmunol.152.12.5796
22. Samuni Y, Goldstein S, Dean OM, Berk M. The chemistry and biological activities of N-acetylcysteine. Biochim Biophys Acta. 2013;1830:4117–4129. doi:10.1016/j.bbagen.2013.04.016
23. Tenório MCDS, Graciliano NG, Moura FA, Oliveira ACM, Goulart MOF. N-acetylcysteine (NAC): impacts on human health. Antioxidants. 2021;10(6):967. doi:10.3390/antiox10060967
24. Hadzic T, Li L, Cheng N, Walsh SA, Spitz DR, Knudson CM. The role of low molecular weight thiols in T lymphocyte proliferation and IL-2 secretion [published correction appears in J Immunol. 2006 May 1;176(9):5682]. J Immunol. 2005;175(12):7965–7972. doi:10.4049/jimmunol.175.12.7965
25. Irie J, Shimada A, Oikawa Y, Shigihara T, Saruta T. N-acetyl-cysteine accelerates transfer of diabetes into non-obese diabetic scid mice. Diabetologia. 2004;47(10):1803–1809. doi:10.1007/s00125-004-1529-x
26. Paschalis V, Theodorou AA, Margaritelis NV, Kyparos A, Nikolaidis MG. N-acetylcysteine supplementation increases exercise performance and reduces oxidative stress only in individuals with low levels of glutathione. Free Radic Biol Med. 2018;115:288–297. doi:10.1016/j.freeradbiomed.2017.12.007
27. Peterson JD, Herzenberg LA, Vasquez K, Waltenbaugh C. Glutathione levels in antigen-presenting cells modulate Th1 versus Th2 response patterns. Proc Natl Acad Sci USA. 1998;95:3071–3076. doi:10.1073/pnas.95.6.3071
28. Ly J, Lagman M, Saing T, et al. Liposomal glutathione supplementation restores TH1 cytokine response to mycobacterium tuberculosis infection in HIV-infected individuals. J Interferon Cytokine Res. 2015;35(11):875–887. doi:10.1089/jir.2014.0210
29. Mak TW, Grusdat M, Duncan GS, et al. Glutathione primes T cell metabolism for inflammation [published correction appears in Immunity. 2017 Jun 20;46(6):1089-1090. doi: 10.1016/j.immuni.2017.06.009.]. Immunity. 2017;46(4):675–689. doi:10.1016/j.immuni.2017.03.019
30. Kalyanaraman B. NAC, NAC, Knockin’ on Heaven’s door: interpreting the mechanism of action of N-acetylcysteine in tumor and immune cells. Redox Biol. 2022;57:102497. doi:10.1016/j.redox.2022.102497
31. Zhou X, Xing J, Tang X, Sheng X, Chi H, Zhan W. Interleukin-2 (IL-2) interacts with IL-2 receptor beta (IL-2Rβ): its potential to enhance the proliferation of CD4+ T lymphocytes in flounder (Paralichthys olivaceus). Front Immunol. 2020;11:531785. doi:10.3389/fimmu.2020.531785
32. Sun L, Su Y, Jiao A, Wang X, Zhang B. T cells in health and disease. Signal Transduct Target Ther. 2023;8(1):235. doi:10.1038/s41392-023-01471-y
33. Lombardi A, Villa S, Castelli V, Bandera A, Gori A. T-cell exhaustion in mycobacterium tuberculosis and nontuberculous mycobacteria infection: pathophysiology and therapeutic perspectives. Microorganisms. 2021;9(12):2460. doi:10.3390/microorganisms9122460
34. Day CL, Abrahams DA, Lerumo L, et al. Functional capacity of Mycobacterium tuberculosis-specific T cell responses in humans is associated with mycobacterial load. J Immunol. 2011;187(5):2222–2232. doi:10.4049/jimmunol.1101122
35. Shen L, Gao Y, Liu Y, et al. PD-1/PD-L pathway inhibits M.tb-specific CD4+ T-cell functions and phagocytosis of macrophages in active tuberculosis. Sci Rep. 2016;6:38362. doi:10.1038/srep38362
36. Wei Z, Li Y, Wei C, et al. The meta-analysis for ideal cytokines to distinguish the latent and active TB infection. BMC Pulm Med. 2020;20:248. doi:10.1186/s12890-020-01280-x
37. Jeong JH, Shim SR, Han S, Hwang I, Ihm C. Diagnostic performance of biomarkers for differentiating active tuberculosis from latent tuberculosis: a systematic review and Bayesian network meta-analysis. Front Microbiol. 2024;15:1506127. doi:10.3389/fmicb.2024.1506127
38. Pedre B, Barayeu U, Ezeriņa D, Dick TP. The mechanism of action of N-acetylcysteine (NAC): the emerging role of H2S and sulfane sulfur species. Pharmacol Ther. 2021;228:107916. doi:10.1016/j.pharmthera.2021.107916
39. Yudhawati R, Prasanta N. The role of N-acetyl sistein in pulmonary tuberculosis. J Respirasi. 2020;6(1):27. doi:10.20473/jr.v6-I.1.2020.27-34
40. Mapamba DA, Sauli E, Mrema L, et al. Impact of N-acetyl cysteine (NAC) on tuberculosis (TB) Patients – a systematic review. Antioxidants. 2022;11(11):2298. doi:10.3390/antiox11112298
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.