Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Monitoring Ototoxicity in Cancer Patients Undergoing Platinum-Based Chemotherapy and Radiation in Saudi Arabia: Challenges and Solutions
Authors AlJasser A ![]()
Received 9 September 2025
Accepted for publication 22 October 2025
Published 5 November 2025 Volume 2025:18 Pages 7159—7173
DOI https://doi.org/10.2147/JMDH.S566255
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Charles V Pollack
Arwa AlJasser
Department of Rehabilitation Sciences, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia
Correspondence: Arwa AlJasser, Department of Rehabilitation Sciences, College of Applied Medical Sciences, King Saud University, P.O. Box 10219, Riyadh, Saudi Arabia, Email [email protected]
Purpose: Platinum-based chemotherapy and radiotherapy are cornerstone treatments for many cancers but carry a high risk of ototoxicity, leading to hearing loss, tinnitus, and balance dysfunction. Despite the benefits of monitoring in reducing long-term consequences, global uptake remains poor. This study provides the first national-level insight into ototoxicity monitoring for cancer patients in Saudi Arabia, aiming to identify service gaps and propose solutions to guide healthcare planning.
Methods: Twenty-five oncology centers were evaluated. Data were collected via phone interviews with oncologists and audiologists, providing a comprehensive understanding of monitoring in clinical practice.
Results: Findings highlight a concerning reality: institutions often fail to support even the most basic elements of ototoxicity monitoring. Practices varied considerably in the absence of formal policies, even within the same institution, depending on audiology service availability and oncologists’ referral approaches. Adult referrals were rare, pediatric monitoring was inconsistent, and long-term follow-up was limited. Barriers included inadequate audiological resources, staff shortages, insufficient multidisciplinary coordination, limited audiologists’ knowledge, and lack of guidelines.
Conclusion: As decision-makers seek reliable national data to guide policies aligned with Vision 2030 health transformation goals, this study proposes policy-based solutions to strengthen ototoxicity monitoring and expand access to hearing rehabilitation services in Saudi Arabia. The study has inspired a collaborative initiative—currently being explored by the author with audiologists and oncologists across health sectors—to promote internal monitoring protocols in capable institutions and lay the groundwork for a future national ototoxicity monitoring program.
Keywords: hearing loss, cancer, survivorship, policy, audiology, multidisciplinary healthcare
Introduction
Ototoxicity refers to damage to the inner ear or auditory nerve, leading to cochlear hearing loss, tinnitus, or balance dysfunction.1 Cancer patients receiving antitumor therapies, particularly platinum-based chemotherapy and radiation therapy, are at high risk of experiencing ototoxicity.
Platinum-based chemotherapy drugs, including cisplatin, carboplatin, and oxaliplatin, are well documented to cause ototoxicity in both pediatric and adult populations.2 Cisplatin is the most ototoxic of this group and among the most ototoxic medications in clinical practice, often causing hearing loss and persistent tinnitus in many patients.3 Carboplatin, while less ototoxic, can still cause significant cochlear damage at high cumulative doses.4,5 Hearing loss from oxaliplatin is rare.6,7 Beyond hearing loss, platinum drugs may also cause vestibular dysfunction, unsteadiness, dizziness, and difficulty focusing on objects while in motion (oscillopsia).8,9 Hearing loss caused by platinum-based drugs usually begins in the high frequencies, worsens with cumulative doses, and may spread to lower frequencies.10–13 Reported adult incidence remains unreliable due to the absence of standardized monitoring. Persistent tinnitus occurs in about 60% and hearing loss in 18% of young testicular cancer patients treated with cisplatin,14 while up to 80% of young men with germ cell cancer develop hearing loss ranging from mild to profound.³ In children, cisplatin-induced ototoxicity has been reported in 26–90% of cases.15
Ototoxicity is also associated with radiation therapy (also known as radiotherapy), which is commonly used for brain, head, and neck tumors and is the first-line treatment for nasopharyngeal cancer.16,17 Because of the complex anatomy of this region, it is difficult to protect the ears and surrounding structures, making radiation-induced ototoxicity a frequent complication. Damage may occur to the cochlea, auditory nerve, or middle and external ear.18 Reported ototoxicity ranged from 0–43% with radiation alone and 17–88% with chemoradiation.19
While ototoxicity monitoring is commonly understood as the process of detecting hearing changes at the earliest stage, it equally encompasses the objective of initiating prompt intervention.9 In the absence of effective, approved preventive or therapeutic interventions that do not compromise anticancer efficacy,20 systematic monitoring of the auditory and vestibular effects of chemotherapy and radiation is essential, as many patients receiving ototoxic drugs may not recognize hearing loss until communication difficulties emerge. This suggests that damage to the frequency range essential for understanding speech has likely already occurred. Likewise, symptoms such as dizziness may only be reported after significant vestibular system damage has taken place.11
Untreated hearing loss can hinder patients’ ability to comprehend important health and treatment-related information21 and has been linked to a higher risk of hospital readmissions.22 Addressing hearing loss is therefore particularly crucial during periods of critical illness.11 Hearing loss, although not life-threatening, can significantly impact communication and quality of life23 and limit employment opportunities.24 Addressing hearing loss can have significant advantages in reducing the risk of developing dementia by enhancing cognitive function and daily living skills.25 Children with any degree of hearing loss, from mild to severe, are at risk of experiencing delays in language development. This can have negative effects on their education, social outcomes, and self-esteem.13,15,24,26 In 2020 Pearson et al27 interviewed adults who had undergone chemotherapy and found that ototoxicity significantly reduced quality of life, particularly due to social difficulties and anxiety about worsening hearing or tinnitus. They recommended better hearing monitoring, patient education, and routine screenings during and after treatment, along with increasing awareness among both patients and healthcare providers to ensure early detection, timely intervention, and long-term support.
Although ototoxicity monitoring guidelines have existed for decades, international adoption of audiological practices remains low.28, A 2023 review of international guidelines reported that limitations in the protocols issued by the American Speech-Language-Hearing Association (ASHA)40 and the American Academy of Audiology (AAA),9 such as impracticality in clinical settings and the absence of clear definitions for significant hearing changes or concrete monitoring intervals, may partly explain the low global adoption of audiological ototoxicity monitoring practices. The authors emphasized the need for further studies to clarify specific barriers to implementing real-world ototoxicity monitoring practices.28
Few studies have explored ototoxicity monitoring practices with the aim of identifying challenges and developing solutions. In the United States, research has largely focused on adherence to national guidelines11,29 supported by well-established monitoring programs, advanced audiology services, and widespread postgraduate training programs—resources that very few countries share. While such studies are valuable, their findings are often shaped by the resources, organization, and workflows of individual institutions. Other investigations have typically been limited to single centers; such approaches often fail to capture real-world challenges or provide practical, implementable solutions needed for establishing comprehensive national programs. For example, a single-center Italian study suggested that establishing a national monitoring program would facilitate early detection and rehabilitation of ototoxic hearing loss. This highlighted the value of national monitoring programs for early detection and rehabilitation of ototoxic hearing loss.30 However, a recent US study reported that while such programs improved baseline testing, follow-up and rehabilitation rates remained low, underscoring the need for context-specific and sustainable surveillance strategies.31
Collectively, these findings highlight the need for national-level evaluations across different countries and regions, as challenges and solutions may vary not only between countries but also across regions within the same country. Some barriers, such as the absence of clear guidelines, may be shared internationally, whereas others are likely to be unique to specific healthcare systems, regional infrastructures, or cultural contexts. Saudi Arabia, which covers most of the Arabian Peninsula, is experiencing a sharp rise in cancer incidence, with rates approaching global levels.32 Cancer care has expanded across health sectors, and survival rates are now comparable to those in Western countries.33,34 This progress should shift the focus toward improving survivors’ quality of life and reducing long-term toxicities, yet research on ototoxicity monitoring is lacking.
This study aims to:
- gain insight into the national practice patterns of ototoxicity monitoring at institutions treating patients with cancer, to identify audiology service gaps, barriers, facilitators, and possible solutions; and
- develop recommendations to enhance ototoxicity monitoring and improve access to hearing rehabilitation services in Saudi Arabia.
This paper provides important information for decision-makers at a critical time. Under Vision 2030, Saudi Arabia launched the National Transformation Program in 2016.35 The healthcare sector is undergoing major reforms to build a more inclusive, efficient, and interconnected system. The strategy emphasizes insurance-based funding, greater private sector involvement, improved access to services, modernized facilities, and expanded investment.36 As decision-makers increasingly seek reliable data and international benchmarks to guide policy, this creates an opportune moment to integrate evidence-based strategies for strengthening cancer care and ototoxicity monitoring in line with global best practices.
Materials and Methods
This study utilized a cross-sectional survey design to evaluate current national practices in ototoxicity monitoring for cancer patients receiving platinum-based chemotherapy or radiotherapy across the Kingdom of Saudi Arabia. The study was approved by the Institutional Review Board, College of Medicine, King Saud University, Riyadh, Saudi Arabia (Reference No. 24/1377/IRB).
Questionnaires
Development and Validity
Two versions of the structured questionnaire were developed by the author: one for oncologists and a parallel version for audiologists. Both were informed by a review of relevant literature, expert input, and clinical practice guidelines from professional audiology organizations. The questionnaires aimed to assess the extent of ototoxicity monitoring implementation, variations in practice, access to services, protocols in use, service gaps, and perceived challenges, with the goal of proposing solutions to improve ototoxicity monitoring systems in oncology settings nationally.
Most items were close-ended with multiple selection options, including check-all-that-apply formats and Likert-style frequency scales, supplemented by “Other” and comment fields for elaboration. This dual-respondent design enabled a comprehensive understanding of ototoxicity monitoring in clinical practice. Face validity was assessed by a subgroup of four professionals (two oncologists and two audiologists), and following consensus on clarity and relevance, both versions were approved for data collection.
Content
The primary questionnaire targeted medical and radiation oncologists in hospitals or cancer centers providing platinum-based chemotherapy or radiotherapy. It began with eligibility confirmation and collected information on center characteristics, including region, healthcare sector, patient population, and cancer treatments offered. It also examined the availability of audiology services, the presence of ototoxicity monitoring programs, internal policies or guidelines, and the stage of implementation.
The questionnaire further explored real-world practices, such as pre-treatment counseling on ototoxic effects, the frequency and consistency of monitoring for pediatric and adult patients, testing locations, referral systems, and appointment scheduling processes. Finally, it identified perceived challenges and barriers to implementation and captured oncologists’ views on systemic issues, including the need for a national monitoring program and the role of audiologists in multidisciplinary care.
The parallel version of the questionnaire was administered to representatives from audiology departments where services were available. It included matched sections for cross-validation with oncologist responses as well as items specific to audiologists’ clinical roles. These covered protocols for baseline and follow-up assessments, diagnostic tests used, counseling practices, and whether standard criteria to define ototoxic shifts or grading scales were used. The questionnaire also assessed the availability of audiological equipment, including portable tools for bedside testing, and explored perceived challenges and barriers to current practice (see Supplementary Materials for the two versions of the questionnaire).
Participating Centers and Representatives
Specialized cancer care centers were identified across the five geographical regions of Saudi Arabia. The Ministry of Health is the largest provider of healthcare in the Kingdom, accounting for approximately 60% of services. Other governmental organizations – such as King Faisal Specialist Hospital and Research Center, Armed Forces Hospitals, National Guard Hospitals, University Hospitals, and Security Forces Hospital – provide 16%, while the private sector accounts for 24%.37 In cancer care, however, governmental organizations play the dominant role, and private sectors contribution is minimal; therefore, it was excluded from this study.
Representatives of evaluated centers were identified through professional networks, with recruitment facilitated by referrals and supported by the collaboration of colleagues and professionals. Direct communication occurred via email, WhatsApp, and phone calls, with a brief explanation of the study’s purpose. Participants chose to remain anonymous to prevent disclosure of their institutions. After obtaining informed consent, questionnaires were completed during scheduled phone calls. This approach allowed respondents to elaborate on their answers and provide additional clarifying information for a more comprehensive understanding. At the end of each call, responses were summarized and reviewed with the participant to ensure accuracy.
Oncology representatives from 25 cancer centers agreed to participate in the study. These representatives were practicing medical or radiation oncologists in cancer centers providing platinum-based chemotherapy or radiotherapy and therefore were directly involved in patient care at their respective institutions. For centers offering both chemotherapy and radiotherapy services, two representatives were interviewed—a medical oncologist and a radiation oncologist—to reflect the common practices of each discipline. In most centers, one medical oncology representative participated, along with a radiation oncologist when applicable. However, in three large centers with higher patient volumes, a total of four oncology representatives (two medical and two radiation oncologists) were interviewed. In total, 45 oncologists participated in the study. Audiologists from 17 centers were interviewed. In most centers, one clinical audiologist served as the representative, whereas in four centers with established audiology departments within the same facility, two audiologists were interviewed. In total, 21 audiologists participated. The majority held a bachelor’s degree in audiology, while a smaller number had completed postgraduate studies abroad.
Although not all cancer care centers in the Kingdom participated, the dataset from these 25 centers—representing approximately 82% of all cancer care centers in Saudi Arabia—is considered comprehensive. It includes representation from all five geographical regions and encompasses a variety of healthcare sectors. This range extends from large, nationally recognized cancer centers to smaller centers with limited oncology services and lower patient volumes. See Table 1 for the characteristics of the evaluated cancer care centers.
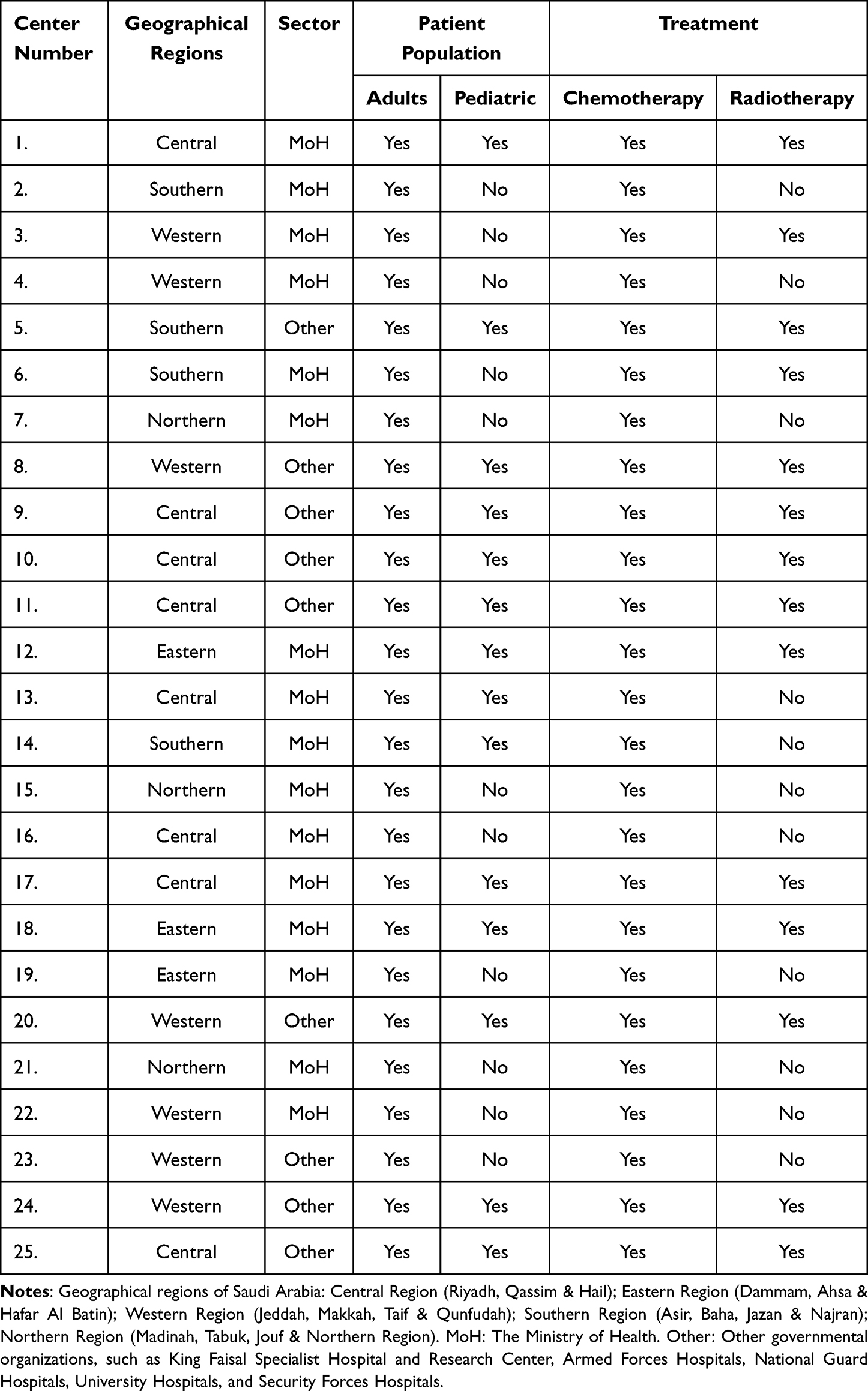 |
Table 1 Characteristics of the Evaluated Cancer Care Centers |
Results
It is worth noting that, in the absence of formal ototoxicity monitoring policies between oncology and audiology departments across all evaluated centers, practices varied considerably, even within the same institution. This variation was occasionally observed by the author during data collection, particularly in larger centers where more than one representative was interviewed. When discrepancies arose, the author verified the information with the respondents. In all such cases, inconsistencies reflected individual differences in practice between oncologists or among audiologists within the same center. The author therefore reported the most commonly conducted practices for each center, while acknowledging that actual practices at any given time may differ and may be slightly better or worse than described.
Table 2 provides a summary of the main descriptive results, while additional important details are described in the Results section.
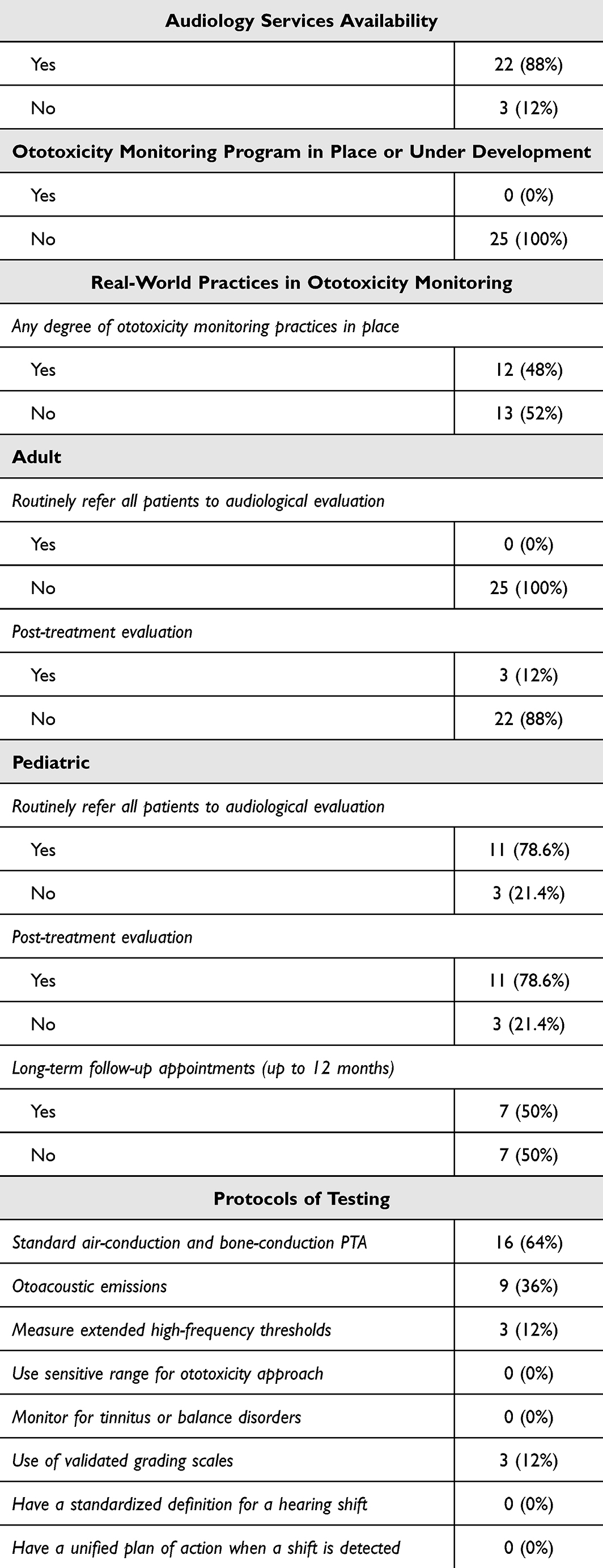 |
Table 2 Summary of the Main Descriptive Results |
Audiology Services Availability
Oncologists from three (12%) centers reported that there are no audiology services available within their facilities, or that they are not aware of such services. In the remaining centers, the availability and scope of audiology services varied widely. These ranged from a lack of full-time audiologists to basic services embedded within otolaryngology clinics, to standalone audiology outpatient clinics, and in some cases, fully equipped departments that included cochlear implant centers. In centers where audiology services were available, they were typically located in separate buildings within the same institution, most commonly near the otolaryngology outpatient clinics.
Ototoxicity Monitoring Programs, Policies, and Implementation Stage
Currently, there is no ototoxicity monitoring program in place or under development at any of the evaluated centers. However, two (8%) audiology departments located within hospitals that host cancer centers reported ongoing efforts to develop an internal policy aimed at improving ototoxicity monitoring practices for cancer patients. Additionally, audiologists from four (16%) other audiology departments indicated the existence of a brief protocol that is informally followed within the department. Nevertheless, these protocols are not formalized, institutionally approved, or sufficiently detailed to be considered official clinical guidelines.
Real-World Practices in Ototoxicity Monitoring
Pretreatment Counselling
Oncologists across all centers reported informing patients or caregivers about potential ototoxic effects before treatment, although the depth of counseling varied. In some facilities, risks were only briefly referenced in the general treatment consent form, alongside other potential side effects, while others provided more detailed verbal discussions. Ototoxicity risk was more frequently addressed with patients receiving cisplatin or those undergoing radiotherapy for head and neck cancers. No centers provided written materials or information on rehabilitation options. When provided, pre-treatment counseling was conducted solely by oncologists; no center reported involvement of audiologists in this process.
Referral to Audiological Evaluation
Oncologists at 13 (52%) of the evaluated centers reported that no routine ototoxicity monitoring practices were in place. In these centers, referrals to audiology were only considered when patients presented with hearing-related symptoms, and such referrals were rare. According to audiologists in the departments serving these centers, referred patients were managed as new cases for assessment and treatment rather than as individuals requiring ototoxicity monitoring. In the remaining 12 (48%) centers, ototoxicity monitoring practices were reported; however, the frequency and consistency of these practices varied and were largely influenced by patient population (adult vs pediatric), the individual approach of the oncologist, availability of audiology appointment slots, cancer type, and the specific antitumor therapies used.
None of the evaluated centers routinely refer all adult patients receiving chemotherapy or radiotherapy for baseline audiological assessments, nor do they conduct regular follow-up monitoring during treatment. Nine centers (36%) reported routinely referring head and neck cancer patients, particularly those with nasopharyngeal carcinoma or requiring radiotherapy, for audiological assessment. In these centers, some oncologists also refer patients who are receiving cisplatin. Monitoring primarily involved baseline evaluations before or shortly after treatment, with ongoing monitoring rarely practiced. Post-treatment evaluations were uncommon and typically occurred only when oncologists considered rehabilitation necessary. Three centers (12%) occasionally conduct post-treatment assessments for head and neck cancer patients, where audiologists provide long-term follow-up for up to 12 months after treatment. However, many patients missed these appointments.
Monitoring changes in hearing for pediatric patients was generally more consistent and frequent than for adults across most centers that serve both populations. However, in three centers (21.4%), routine referrals to audiology were not conducted, with two of these centers (14.3%) lacking audiology services. In the remaining 11 centers (78.6%), baseline assessments were usually performed unless the patient’s clinical status prevented testing. Follow-up monitoring prior to each treatment dose was limited and inconsistent, whereas post-treatment evaluations were conducted more frequently. In only seven centers (50%), audiologists reported providing long-term follow-up appointments for up to 12 months, but none extended beyond this period. However, many pediatric patients miss these appointments, and no tracking systems are in place to ensure continued monitoring.
Protocols, Equipment, and Location of Testing
In all centers that reported conducting hearing evaluations for cancer patients receiving antitumor therapies, the protocols used for baseline, during-treatment (if conducted), and post-treatment assessments involved similar test batteries. These typically include tympanometry, bilateral standard air-conduction and bone-conduction pure-tone audiometry (PTA) at 0.25, 0.5, 1, 2, 4, and 8 kHz, with some centers also testing at 3 and 6 kHz, and speech reception thresholds, along with word recognition testing. Auditory brainstem response is used to estimate thresholds in infants and young children unable to provide reliable behavioral responses. Otoacoustic emissions (OAEs) are commonly included in the test battery. Depending on equipment availability, centers use either distortion-product OAEs (measured up to 8 or 10 kHz) or transient-evoked OAEs.
Audiologists in only three centers (12%) reported routinely measuring extended high-frequency (EHF) PTA thresholds. Notably, the absence of EHF testing in other centers was not always due to equipment limitations; audiologists in some facilities acknowledged having access to high-frequency audiometers but still did not incorporate EHF testing into their routine protocols. None of the participating audiologists reported using the behavioral Sensitive Range for Ototoxicity (SRO) approach.38 Similarly, no centers monitored for ototoxicity-related tinnitus or balance disorders, nor did they employ self-report measures for hearing, tinnitus, or quality of life.
All testing was conducted in audiology clinics, as portable equipment was unavailable in most centers. Only three centers (12%) reported having portable equipment (tympanometer, standard audiometer, and diagnostic OAE system) and considered bedside testing for patients with limited responsiveness, although this was not common practice.
Shift Definition, Grading Scales, and Outcome Reporting
None of the evaluated centers used a consistent or standardized definition for identifying an ototoxic hearing shift, nor was there a unified plan of action when a shift was detected. Conducting a validating retest before making clinical recommendations was reported by audiologists in only one center (4%). In general, participating audiologists in centers where ototoxicity monitoring for cancer patients was implemented routinely documented threshold shifts, of any magnitude, at a single frequency or two or more adjacent frequencies in the audiology notes for review by the referring oncologist.
Audiologic management, follow-up appointments, and counseling regarding rehabilitative options – such as hearing aids and communication strategies – were typically provided to patients when clinically indicated. The use of validated grading scales was uncommon. Only three centers (12%) reported routine use: two (8%) used the International Society of Pediatric Oncology (SIOP) Boston Ototoxicity Scale for pediatric patients, and one (4%) used the Common Terminology Criteria for Adverse Events (CTCAE) for both pediatric and adult patients.
Access and Scheduling
In all evaluated centers, audiologists only had access to patients requiring ototoxicity monitoring if they were referred by oncologists. Scheduling of monitoring tests was managed jointly by oncology and audiology clinics, depending on appointment availability. In three centers (12%), audiology departments reported that oncology referrals were prioritized, allowing patients to be accommodated as walk-ins for urgent cases.
Limitations and Challenges in Implementing Effective Monitoring
The key challenges limiting the implementation and the feasibility of timely and consistent ototoxicity monitoring were identified through both the multiple-choice responses and elaborative comments provided by participating oncologists and audiologists. The following themes emerged.
Audiology Service Availability and Audiologist Shortage
This was a central concern shared by both oncologists and audiologists. In several centers, particularly those located outside major cities, oncologists reported significant barriers due to the limited availability of audiology services, lack of essential equipment for ototoxicity monitoring, or the absence or shortage of full-time audiologists. Larger institutions, which are typically in the main cities and host major cancer centers, were more likely to have established audiology departments. These departments often serve ENT clinics, traditional audiology outpatient caseloads, newborn hearing screening referrals, and cochlear implant programs. However, even in these better-resourced centers, audiologists reported considerable challenges due to staff shortages and limited availability of sound booths.
Most participating audiologists described a high clinical workload, which makes it challenging to consistently monitor all adult cancer patients and to provide timely, repeated assessments for pediatric patients. Scheduling constraints and competing service demands, where audiologists are often stretched across multiple services, further hinder the implementation of consistent ototoxicity monitoring for all at-risk patients.
Insufficient Multidisciplinary Teamwork and Coordination
Another frequently reported limitation, identified by most participating oncologists and audiologists, was the lack of effective multidisciplinary collaboration. A common concern was the absence of dedicated coordinators to manage key aspects of ototoxicity monitoring, including referral processes, access to patients and follow-ups, communication of outcomes, and interdepartmental coordination. The lack of an integrated care model was identified as a major barrier to implementing consistent and timely monitoring practices.
Lack of Guidelines for Ototoxicity Monitoring Protocols
A primary challenge reported by the majority of participating audiologists was the absence of formal guidelines or structured protocols for ototoxicity monitoring. The lack of clear policies to guide essential elements – the selection of diagnostic tests, recommended test frequency, criteria for defining hearing shifts, use of grading scales, and standardized methods for documentation and reporting – was identified as a major barrier to implementing effective monitoring practices.
It is worth noting that the majority of participating audiologists, particularly those with only a bachelor’s degree in audiology and no postgraduate studies abroad, reported limited familiarity with ototoxic medications, recommended practices such as the SRO screening method, available grading scales, and international ototoxicity monitoring guidelines. This gap was largely attributed to the insufficient coverage of ototoxicity during their undergraduate studies.
Compromised Clinical Status of Cancer Patients
A less frequently reported but significant barrier was the physical and cognitive condition of some patients undergoing chemotherapy or radiotherapy, particularly those in critical condition. In such cases, the compromised clinical status made it difficult to transport patients to audiology clinics, often located in separate buildings or distant departments, or to conduct comprehensive behavioral hearing assessments.
Oncologists’ Perspectives
Participating oncologists were invited to share their perspectives on key issues related to ototoxicity monitoring, including the potential role of audiologists, and to highlight areas they believed would most improve current practices.
Need for a National Ototoxicity Monitoring Program
All oncologists agreed on the need for a structured ototoxicity monitoring policy for patients receiving chemotherapy or radiotherapy. However, views differed regarding the scale at which such a program should be implemented. The majority, particularly those from centers with limited or no audiology services, believed that meaningful progress would not be possible without a national program formally supported by the Saudi Ministry of Health and other health sectors. In contrast, a few oncologists from large institutions with well-established audiology departments felt that, while a national program should remain the long-term goal, adopting standardized internal policies within their institutions could still provide noticeable improvements in current practices, even if not fully sufficient. Notably, over 94% of participating oncologists believed the initiative for establishing a national program should originate from audiologists, as part of a collaborative, multidisciplinary effort. None disagreed, while the remaining respondents were uncertain (neither agreeing nor disagreeing).
Role of Audiologists in Multidisciplinary Care
All participating oncologists emphasized that audiologists should take a more active role in raising awareness about the signs and symptoms of ototoxicity – such as hearing loss, tinnitus, and imbalance – and their impact on communication and overall quality of life. This awareness should be directed not only to healthcare providers, including oncologists and nurses, but also to patients and caregivers. The majority (over 90%) also believed that audiologists should be more involved in pre-treatment counseling, working alongside oncologists to educate patients and caregivers about the potential risks of ototoxicity and the rehabilitative options available. None of the oncologists disagreed with this view; however, those who did not fully agree expressed concerns about the depth and style of counseling, noting that it should be delivered carefully so as not to discourage patients or create hesitation in accepting the therapy plan recommended by the oncologist.
Discussion
Current State of Ototoxicity Monitoring for Cancer Patients
This study provides the first national-level insight into the real-world practices of ototoxicity monitoring for cancer patients undergoing platinum-based chemotherapy and radiotherapy in Saudi Arabia. The findings from the evaluated centers reveal a substantial gap in the delivery of structured, consistent, and protocol-driven audiological care for both adult and pediatric cancer patients at risk of ototoxicity. No formal ototoxicity monitoring programs or endorsed internal policies between oncology and audiology departments were reported to be in place or under development. The existing informal protocols mentioned in a few audiology departments lacked institutional support and clinical standardization.
In adult oncology, routine referrals for audiological evaluation – whether prior to, during, or after cessation of treatment – were nearly absent. Referrals infrequently occurred only after patients reported symptoms, and in some centers, were limited to subgroups such as head and neck cancer patients. Monitoring for other high-risk adult patients, including those receiving cisplatin, remained an exception rather than the norm. Although these adult cancer centers did not treat pediatric patients, it is worth noting that some institutions consider individuals as young as 14 years old as adults in their oncology protocols.
Pediatric ototoxicity monitoring practices were generally somewhat better than those for adults. However, this was not consistent across all centers, as several institutions either lacked on-site audiology services or did not refer all pediatric patients for hearing evaluations. In centers where stronger practices existed, baseline and follow-up assessments were more common, though inconsistent, during treatment cycles.
The level of ototoxicity monitoring services was clearly influenced by the presence of an established audiology department within the same facility. However, even in institutions with such departments, comprehensive and consistent monitoring was not guaranteed. Most prioritized a single baseline evaluation rather than full-cycle monitoring. As audiologists do not have direct access to oncology patients, the implementation of consistent monitoring schedules relied entirely on oncologists’ referral decisions. Post-treatment assessments were more common in pediatric than adult settings. Follow-up appointments, when scheduled, did not extend beyond 12 months post-treatment. Missed follow-up appointments were frequent, with no tracking systems in place to ensure continuity of care. Gaps in the routinely used protocols by audiologists were also identified. EHF audiometry, a critical component of early ototoxicity detection,39 was rarely performed, even when equipment was available. The SRO method, a patient-specific high-frequency screening strategy38,39,41 recommended by ASHA (1994)40 and AAA (2009),9 was not used at any center. Additionally, standardized definitions for hearing shifts, documentation protocols, and predefined action plans were largely absent. The use of validated grading scales was inconsistent, despite their importance for identifying intervention needs and long-term outcome tracking.13
Current practices appear to focus on detecting clinically significant hearing loss only after it has progressed to the lower frequencies that affect speech comprehension and daily communication. This approach leans more towards making decisions about rehabilitation rather than prioritizing the proactive early detection necessary to prevent or minimize auditory damage. Moreover, the absence of structured end-of-treatment evaluations and long-term follow-up for adults and pediatric patients poses a significant risk of undetected hearing loss, particularly since platinum-related ototoxic effects may continue to progress after therapy has concluded. For example, it was found that audiograms showed grade 2 ototoxicity in 11% of patients shortly after treatment, rising markedly to 44% in evaluations conducted more than two years post-treatment.42
Challenges and Barriers to Effective Ototoxicity Monitoring in Practice
Understanding the barriers within current practices is essential for identifying the next steps toward improving ototoxicity monitoring and for developing feasible solutions. Several recurring challenges emerged from this study.
One major challenge is the limited availability of audiology services and the shortage of audiologists, particularly outside major cities in Saudi. Many oncology departments lack access to dedicated audiology units or essential equipment required for comprehensive ototoxicity monitoring. Even large institutions with established audiology departments face constraints such as limited staffing, insufficient sound booths, lack of portable equipment, and high clinical workloads, that hinder consistent monitoring for both adult and pediatric patients.
Weak interdisciplinary collaboration and the absence of structured referral and follow-up policies were also highlighted. Referral pathways are often unclear, and audiologists are unable to access patients without a formal referral. Referral decisions largely depend on individual oncologists’ practices, resulting in inconsistencies within and across institutions.
Another significant barrier is the lack of guidelines and standardized protocols. The absence of unified monitoring protocols, validated grading systems, and documentation standards creates inconsistencies and uncertainty in clinical practice. Many audiologists also reported limited familiarity with international recommendations, reflecting insufficient coverage of ototoxicity in undergraduate training.
Patient-related factors, including compromised clinical status and logistical constraints, were also reported. The clinical condition of some patients undergoing chemotherapy or radiotherapy, combined with the physical separation of audiology and oncology services and the lack of portable testing equipment, often impede timely and comprehensive assessments, especially for critically ill patients.
Facilitators, Recommendations, and Proposed Solutions
A primary aim of this study was to identify facilitators and propose recommendations to enhance the monitoring and management of ototoxicity across cancer care centers in Saudi Arabia. Rather than evaluating adherence to international guidelines, the study focused on understanding current practices and challenges. The recommendations and possible solutions presented in this study reflect the author’s perspective, informed by professional experience in audiology in Saudi Arabia, relevant international literature, reported challenges requiring solutions, and insights gained from oncologists’ perspectives.
- Strengthen audiology services nationwide: Establish new audiology departments in underserved regions and expand staffing levels in existing units to ensure equitable access to care. Prioritize investment in essential diagnostic equipment, including portable testing solutions, to facilitate timely ototoxicity monitoring. While the focus of this paper is on improving ototoxicity monitoring practices for cancer patients, these measures will also strengthen nationwide audiology service coverage, support early detection and intervention, and address broader audiological care needs of the Saudi population. Achieving these objectives will require strategic infrastructure development, targeted workforce training, and sustainable resource allocation.
- Address workforce shortages: Audiology is a relatively new field in Saudi Arabia, with the first bachelor’s program established at King Saud University in 1985. The program only began graduating cohorts annually from 1998 and remained the sole source of audiologists until 2016, when a second program opened in Riyadh.43 Two more programs were launched in Jeddah and Abha in 2021, with their first graduates in 2025.44 No postgraduate M.Sc. program currently exists in Saudi. However, the number of programs is expected to increase in the next few years, so the longstanding shortage of audiologists, particularly outside the capital city, is expected to ease as more graduates enter the workforce.
- Empower audiologists in counseling and awareness roles: Audiologists should actively engage in patient and caregiver education, pre-treatment counseling, and oncology team training. Oncologists highlighted their role in raising awareness about ototoxicity symptoms, impact, and rehabilitative solutions. None of the evaluated centers provided written counseling; therefore, written handouts should be developed to complement verbal counseling. Evidence shows that combining both formats improves patient knowledge, satisfaction, and standardization of care.45 Strengthening counseling practices and educating patients and caregivers could reduce missed follow-up appointments and increase the likelihood of patients seeking help and adhering to prescribed interventions.11,46
- Promote self-referral and direct access models: Building on their counseling role, audiologists should encourage patients and caregivers to seek audiological care independently of oncologist referrals, particularly when symptoms arise. Counseling should also stress the importance of end-of-treatment evaluations and follow-up beyond one year. Patients should have long-term access to local audiology services, including eligibility for no-cost annual hearing screenings and hearing aid support where needed. These measures would promote earlier detection and timely intervention.27
- Expand digital and remote solutions: Although not yet widely implemented, tele-audiology and remote hearing assessment tools hold strong future potential. With advancements in artificial intelligence, these solutions are expected to expand access for patients in remote or underserved areas and should therefore be considered in future planning.47 Validated Arabic self-report questionnaires should also be developed and used routinely to quickly assess patient needs and guide further testing.
- Establish a centralized tracking and data-sharing system: To improve continuity of care, a centralized tracking and data-sharing system should be established to record, monitor, and share ototoxicity-related outcomes across oncology and audiology teams. Such a system would facilitate coordinated management, enable earlier identification of at-risk patients, and support the development of databases to inform research and policy planning.
- Review and enhance audiology curricula: Study findings revealed knowledge gaps among audiologists holding only a bachelor’s degree without postgraduate training abroad. As most Saudi audiologists fall into this category, undergraduate programs should be reviewed to ensure graduates are equipped with the knowledge on ototoxicity, including the pharmacology of ototoxic medications, international best practices, and guideline-driven monitoring protocols, counseling strategies and interdisciplinary collaboration.
- Develop clear and concise guidelines: Poor global uptake of audiological ototoxicity monitoring is partly due to the absence of clear, practical, and time-efficient guidance.11,28 To improve uptake, simplified national guidelines should be developed, drawing on the pragmatic elements of the ASHA (1994) and AAA (2009) recommendations, while ensuring they are adaptable to local resource availability and clinical workflows. Guidelines should remain flexible for updates in line with international evidence, but must start with a practical, resource-sensitive framework that delivers measurable improvements. Overly theoretical policies risk poor implementation, whereas realistic approaches will support adoption, build momentum, and lay the foundation for future enhancements.
- Establish a national ototoxicity monitoring program: Insights from oncologists and audiologists underscore the urgent need for a structured, standardized program to ensure consistent, coordinated, and equitable services across all cancer care centers. A Ministry-led program – modeled on the successful rollout of the Universal Newborn Hearing Screening program (UNHS) launched in 2016–48 should be established, led by audiologists in partnership with oncologists and pharmacists. Aligning with Vision 2030 health transformation goals, this program would integrate preventive audiology services into cancer care, ensuring early detection, coordinated management, and improved survivor quality of life. An initiative toward this goal has already been set in motion by the author in collaboration with senior clinical audiologists and oncologists from diverse healthcare sectors. While initially focused on cancer care, the program could later expand to include patients receiving other ototoxic medications.
- Pilot institutional policies while scaling nationally: In the absence of immediate national implementation, institutions with existing capacity should adopt internal monitoring protocols and tracking systems as a first step. Drawing on the UNHS model, phased in from 2016 in major hospitals and expanded nationwide by 2018,48 a similar phased approach would support systematic adoption, capacity building, and eventual national coverage. Strengthening collaboration between oncology and audiology teams will be vital to ensure consistent, effective monitoring practices.
Study Limitations
This study is limited by its cross-sectional and descriptive design, which restricts evaluation of the long-term sustainability of monitoring and follow-up practices. The study timeframe, while sufficient for descriptive outcomes, naturally limits assessment of evolving practices over time. Although the dataset covers approximately 82% of cancer care centers in Saudi Arabia, the exclusion of a few centers may introduce minor potential for selection or response bias.
Conclusion
- By documenting current practices and challenges, this study proposes recommendations to strengthen ototoxicity monitoring and expand access to hearing rehabilitation services, while providing a foundation for evidence-based policy and program development in Saudi Arabia.
- Raising awareness among both patients and healthcare providers is essential to ensure early detection, timely intervention, and long-term support.
- Prioritizing the implementation of the recommended solutions to strengthen and standardize ototoxicity monitoring practices is crucial to improving the quality of life of cancer patients and survivors and minimizing long-term consequences.
- While tailored to the local context, the core elements may be transferable to other countries with similar healthcare systems where formal ototoxicity monitoring programs are absent. Future international efforts should prioritize the updating of existing guidelines to address current weaknesses that hinder implementation.
Abbreviations
AAA, The American Academy of Audiology; ASHA, The American Speech-Language-Hearing Association; EHF, Extended high-frequency; OAEs, Otoacoustic Emissions; PTA, Pure-Tone Audiometry; SRO, Sensitive Range for Ototoxicity
Acknowledgments
The author gratefully acknowledges the contributions of the oncologists and audiologists who participated in this study and generously shared their time, insights, and expertise. The author would like to thank Ongoing Research Funding Program, (ORFFT-2025-102-1), King Saud University, Riyadh, Saudi Arabia for financial support.
Disclosure
The author declares no conflicts of interest in this work.
References
1. Ganesan P, Schmiedge J, Manchaiah V, Swapna S, Dhandayutham S, Kothandaraman PP. Ototoxicity: a challenge in diagnosis and treatment. J Audiol Otol. 2018;22(2):59–68. doi:10.7874/jao.2017.00360
2. Baguley DM, Prayuenyong P. Looking beyond the audiogram in ototoxicity associated with platinum-based chemotherapy. Cancer Chemother Pharmacol. 2020;85:245–250.
3. Frisina RD, Wheeler HE, Fossa SD, et al. Comprehensive audiometric analysis of hearing impairment and tinnitus after cisplatin-based chemotherapy in survivors of adult-onset cancer. J Clin Oncol. 2016;34(23):2712–2720. doi:10.1200/JCO.2016.66.8822
4. Obermair A, Speiser P, Thomas M, et al. Prediction of toxicity but not of clinical course by determining carboplatin exposure in patients with epithelial ovarian cancer treated with a combination of carboplatin and cisplatin. Int J Oncol. 1998;13(5):1023–1030. doi:10.3892/ijo.13.5.1023
5. Hartmann JT, Lipp HP. Toxicity of platinum compounds. Expert Opin Pharmacother. 2003;4(6):889–901. doi:10.1517/14656566.4.6.889
6. Dreisbach L, Ho M, Reid E, Siegel J. Effects of oxaliplatin, carboplatin, and cisplatin across treatment on high-frequency objective and subjective auditory measures in adults. Perspect ASHA Spec Interest Groups. 2017;2:17–36. doi:10.1044/persp2.SIG6.17
7. Hijri FZ, Arifi S, Ouattassi N, Mellas N, El Mesbahi O. Oxaliplatin-induced ototoxicity in adjuvant setting for colorectal cancer: unusual side effect. J Gastrointest Cancer. 2014;45:106–108. doi:10.1007/s12029-013-9489-3
8. Handelsman JA. Vestibulotoxicity: strategies for clinical diagnosis and rehabilitation. Int J Audiol. 2017.
9. American Academy of Audiology (AAA). Position Statement and Clinical Practice Guidelines: ototoxicity Monitoring. 2009. Available from: http://www.audiology.org.
10. Blakley BW, Myers SF. Patterns of hearing loss resulting from cis-platinum therapy. Otolaryngol Head Neck Surg. 1993;109:385–391. doi:10.1177/019459989310900302
11. Konrad-Martin D, Poling GL, Garinis AC, et al. Applying US. national guidelines for ototoxicity monitoring in adult patients: perspectives on patient populations, service gaps, barriers and solutions. Int J Audiol. 2018;57(sup4):S3–S18. doi:10.1080/14992027.2017.1398421
12. Ding D, Allman BL, Salvi R. Review: ototoxic characteristics of platinum antitumor drugs. Anat Record. 2012;295(11):1851–1867. doi:10.1002/ar.22577
13. Brock PR, Freyer KR, Campbell DR, Steyger KC, Blakley PS, Neuwelt EA. Platinum-induced ototoxicity in children: a consensus review on mechanisms, predisposition, and protection, including a new international society of pediatric oncol. boston ototoxicity scale. J Clin Oncol. 2012;30(19):2408–2417. doi:10.1200/JCO.2011.39.1110
14. Bokemeyer C, Berger C, Hartmann JT, et al. Analysis of risk factors for cisplatin-induced ototoxicity in patients with testicular cancer. Br. J. Cancer. 1998;77:1355–1362. doi:10.1038/bjc.1998.226
15. Knight KR, Kraemer DF, Neuwelt EA. Ototoxicity in children receiving platinum chemotherapy: underestimating a commonly occurring toxicity that may influence academic and social development. J Clin Oncol. 2005;23(34):8588–8596. doi:10.1200/JCO.2004.00.5355
16. Wei WI, Sham JS. Nasopharyngeal carcinoma. Lancet. 2005;365:2041–2054. doi:10.1016/S0140-6736(05)66698-6
17. Honore HB, Bentzen SM, Møller K, Grau C. Sensori-neural hearing loss after radiotherapy for nasopharyngeal carcinoma: individualized risk estimation. Radiother Oncol. 2002;65:9–16. doi:10.1016/S0167-8140(02)00173-1
18. Wakisaka H, Yamada H, Motoyoshi K, Ugumori T, Takahashi H, Hyodo M. Incidence of long-term ipsilateral and contralateral ototoxicity following radiotherapy for nasopharyngeal carcinoma. Auris. Nasus Larynx. 2011;38(1):95–100. doi:10.1016/j.anl.2010.03.012
19. Theunissen EA, Bosma SC, Zuur CL, et al. Sensorineural hearing loss in patients with head neck cancer after chemoradiotherapy and radiotherapy: a systematic review of the literature. Head Neck. 2015;37:281–292. doi:10.1002/hed.23551
20. Chattaraj A, Syed MP, Low CA, Owonikoko TK. Cisplatin-Induced Ototoxicity: a concise review of the burden, prevention, and interception strategies. JCO Oncol Pract. 2023;19(5):278–283. doi:10.1200/OP.22.00710
21. Amalraj S, Starkweather C, Nguyen C, Naeim A. Health literacy, communication, and treatment decision-making in older cancer patients. Oncol. 2009;23(4):369–375.
22. Genther DJ, Betz J, Pratt S, et al. Association between hearing impairment and risk of hospitalization in older adults. J Am Geriatr Soc. 2015;63(6):1146–1152. doi:10.1111/jgs.13456
23. Punch JL, Hitt R, Smith SW. Hearing loss and quality of life. J Commun Disord. 2019;78:33–45. doi:10.1016/j.jcomdis.2019.01.001
24. Graydon K, Waterworth C, Miller H, et al. Global burden of hearing impairment and ear disease. J Laryngol Otol. 2019;133(1):18–25.
25. Dawes P, Munro KJ. Hearing loss and dementia: where to from here? Ear Hear. 2024;45(3):529–536. doi:10.1097/AUD.0000000000001494
26. Tomblin JB, Ambrose M, Walker SE, Oleson EA, Moeller MP, Moeller MP. Language outcomes in young children with mild to severe hearing loss. Ear Hear. Ear and Hearing. 2015;36:76S–91S. doi:10.1097/AUD.0000000000000219
27. Pearson SEC, Shabbir C, Shabbir M, Baguley DM. M. et al. The impact of chemotherapy-induced inner ear damage on quality of life in cancer survivors: a qualitative study. J Cancer Surviv. 2022;16:976–987. doi:10.1007/s11764-021-01089-5
28. Lester GMW, Timmer WJ, B BH, Ladwa RM. Audiological ototoxicity monitoring guidelines: a review of current evidence and appraisal of quality using the AGREE II tool. Int. J Audiol. 2023;1–6.
29. Santucci NMG, Ivory B, Kuhn R, Stephen MA, Aizenberg D. Insight into the current practice of ototoxicity monitoring during cisplatin therapy. J Otolaryngol Head Neck Surg. 2021;50(1). doi:10.1186/s40463-021-00506-0
30. Gambacorta VO, Faralli E, Gullà M, et al. Practice of monitoring cisplatin-induced ototoxicity by audiology, ENT, and oncology specialists: a survey-based study in a single italian medical center. Audiol Res. 2023;13:779–790. doi:10.3390/audiolres13050069
31. Patel JB, Liu J, Urdang K, et al. Ototoxicity monitoring: the evolution of a protocol for head and neck cancer patients. OTO Open. 2025;9.
32. Jazieh ARD, Alkaiyat OB, Zaatreh M, et al. Cancer incidence trends from 1999 to 2015 and contributions of various cancer types to the overall burden: projections to 2030 and Extrapolation of Economic Burden in Saudi Arabia. Cancer Manage Res. 2019;11,9665–9674.
33. Aseafan MD, AlAhwal E, Souissi M, AlEid R, AlEid R, Bazarbashi S. Populationbased survival for cancer patients in Saudi Arabia for the years 2005–2009. Sci Rep. 2022;12. doi:10.1038/s41598-021-04374-6
34. Gazette S, Al-Fayyadh M. (2023). King Faisal Specialist Hospital and Research Center (KFSH&RC) CEO. hospital’s transformation and future plans Interview. Available online: https://www.saudigazette.com.sa/article/631595. (
35. Vision 2030. (n.d.-a). National Transformation Program: strategic objectives. Available from: https://vision2030.gov.sa/en.
36. Vision 2030. (n.d.-b). Health Sector Transformation Program. Kingdom of Saudi Arabia Vision 2030. Available from: https://www.vision2030.gov.sa/en/vision-2030/vrp/health-sector-transformation-program/.
37. Ministry of Investment Saudi Arabia. Healthcare Sector Overview; 2025.
38. Vaughan NESAF, A. Henry J, A. Henry J, A. Henry J, Henry JA, Henry JA. An efficient test protocol for identification of a limited, sensitive frequency test range for early detection of ototoxicity. J Rehabil Res Dev. 2002;39:567–574.
39. Dreschler WA, van der Hulst RJ, Tange RA, Urbanus NA. Role of high-frequency audiometry in the early detection of ototoxicity. II Clinical Aspects Audiology. 1989;28(4):211–220.
40. American Speech-Language-Hearing Association (ASHA). Guidelines for the audiologic management of individuals receiving cochleotoxic drug therapy. ASHA. 1994;36:11–19.
41. Konrad-Martin D, Hulswit J. Sensitivity Range for Ototoxicity (SRO): Screening Method to Improve Access”. VA RR&D National Center for Rehabilitative Auditory Research (NCRAR; 2020.
42. Bertolini PML, Mercier G, Raquin MA, Izzi G, Corradini N, Hartmann O. Platinum compound-related ototoxicity in children: long-term follow-up reveals continuous worsening of hearing loss. J Pediatric Hematol Oncol. 2004;26,649–655.
43. Saudi Commission for Health Specialties. Saudi Higher Diploma in Clinical Audiology: training program curriculum. Available from: https://scfhs.org.sa/sites/default/files/2022-02/Audiology-updated.pdf.
44. Alakeel A. The Practice of Speech-Language Pathology in Saudi Arabia. Arab J Appl Linguist. 2022;7(1):86–98.
45. Sandford JA, Tyndall J. Written and verbal information versus verbal information only for patients being discharged from acute hospital settings to home. Cochrane Database Syst Rev. 2003.
46. Knudsen LVÖ, Nielsen M, Naylor C, Kramer SE. Factors influencing help seeking, hearing aid uptake, hearing aid use and satisfaction with hearing aids: a review of the literature. Trends Amplif. 2010;14(3):127–154. doi:10.1177/1084713810385712
47. D’Onofrio KL, Zeng FG. Tele-audiology: current state and future directions. Front digital health. 2022;3.
48. Alaql FAM. Realization of a successful universal newborn hearing screening program in Saudi Arabia. J Paediatr Neonatal Med. 2021;3(4):147.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Reasons for Emergency Department Visit, Outcomes, and Associated Factors of Oncologic Patients at Emergency Department of Jimma University Medical Centre
Workina A, Habtamu A, Zewdie W
Open Access Emergency Medicine 2022, 14:581-590
Published Date: 28 October 2022
The Use of Chatbots in Oncological Care: A Narrative Review
Wang A, Qian Z, Briggs L, Cole AP, Reis LO, Trinh QD
International Journal of General Medicine 2023, 16:1591-1602
Published Date: 1 May 2023
Psychometric Properties of the Peruvian Version of the MOS Scale for Social Support in Cancer Patients and Convergent Network with Quality of Life
Ramos-Vera C, Calle D, Collacso Fiesta H, Lamilla LL, Serpa-Barrientos A, Saintila J
Patient Preference and Adherence 2023, 17:1999-2011
Published Date: 14 August 2023
Evaluating the Outcomes in Patients with Colorectal Cancer Using the Malnutrition Universal Screening Tool: A Systematic Review
Muntean C, Blidari AR, Faur AM, Curca RO, Feier CVI
Journal of Multidisciplinary Healthcare 2024, 17:4277-4289
Published Date: 3 September 2024