Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Molecular Pathways of Diabetic Kidney Disease Inferred from Proteomics
Received 10 October 2022
Accepted for publication 6 December 2022
Published 12 January 2023 Volume 2023:16 Pages 117—128
DOI https://doi.org/10.2147/DMSO.S392888
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Gian Paolo Fadini
Lan Wei,1 Yuanyuan Han,2 Chao Tu1
1Department of Internal Medicine, The Third Affiliated Hospital of Soochow University, Changzhou, People’s Republic of China; 2Institute of Medical Biology, Chinese Academy of Medical Sciences and Peking Union Medical College, Yunnan Key Laboratory of Vaccine Research and Development on Severe Infectious Diseases, Kunming, People’s Republic of China
Correspondence: Chao Tu, Department of Internal Medicine, The Third Affiliated Hospital of Soochow University, 185 Juqian Road, Changzhou, 213000, People’s Republic of China, Email [email protected]
Abstract: Diabetic kidney disease (DKD) affects an estimated 20– 40% of type 2 diabetes patients and is among the most prevalent microvascular complications in this patient population, contributing to high morbidity and mortality rates. Currently, changes in albuminuria status are thought to be a primary indicator of the onset or progression of DKD, yet progressive nephropathy and renal impairment can occur in certain diabetic individuals who exhibit normal urinary albumin levels, emphasizing the lack of sensitivity and specificity associated with the use of albuminuria as a biomarker for detecting diabetic kidney disease and predicting DKD risk. According to the study, a non-invasive method for early detection or prediction of DKD may involve combining proteomic analytical techniques such second generation sequencing, mass spectrometry, two-dimensional gel electrophoresis, and other advanced system biology algorithms. Another category of proteins of relevance may now be provided by renal tissue biomarkers. The establishment of reliable proteomic biomarkers of DKD represents a novel approach to improving the diagnosis, prognostic evaluation, and treatment of affected patients. In the present review, a series of protein biomarkers that have been characterized to date are discussed, offering a theoretical foundation for future efforts to aid patients suffering from this debilitating microvascular complication.
Keywords: diabetic kidney disease, proteomics, diagnostic biomarkers, therapeutic targets
Introduction
Diabetic kidney disease (DKD) is a common microvascular complication that impacts 20–40% of individuals diagnosed with type 2 diabetes, resulting in high rates of morbidity and mortality. DKD is diagnosed based on the detection of persistent proteinuria, an albumin creatinine ratio greater than 30 mg/g creatinine, a reduction in the estimated glomerular filtration rate (eGFR), and the progressive deterioration of kidney function.1,2 Persistent hyperglycemia in individuals with diabetes can drive the increased synthesis of extracellular matrix (ECM) proteins, enhanced cell proliferation, and the dysfunction of endothelial cells together with tubular atrophy, interstitial fibrosis, and the thickening of the glomerular and tubular basement membrane as a consequent of inflammation, oxidative stress, and advanced glycation end product (AGE) production.3 DKD development is further driven by the increased accumulation of protein within the renal extracellular matrix, the expansion of the mesangial matrix, glomerular hyperfiltration, tubulointerstitial fibrosis, and the aggravated thickening of the glomerular basement membrane. Injury to glomerular podocytes can also contribute to DKD incidence.1
Both a reduction in eGFR and albuminuria are considered relatively non-specific biomarkers of DKD given that they are also altered in the context of many other chronic glomerular diseases, with 60% of nephron function already being absent with eGFR values falling to the threshold of 60 mL/min/1.73 m2.4 Given that DKD is a prevalent cause of end-stage renal disease (ESRD), it is critical that reliable biomarkers that can guide the diagnosis and treatment of this condition be defined. Both urinary albumin (UALB) and β2-microglobulin (Uβ2m) have been leveraged as biomarkers of glomerular and tubular injury,5 yet these levels and eGFR changes are only evident after substantial glomerular damage has taken place. However, many patients exhibit histopathological alterations in renal structures prior to the onset of microalbuminuria.6 While these changes can be detected through renal biopsy, enabling the more robust diagnosis and monitoring of affected patients, the utility of this approach is limited by the inherent invasivity of biopsy procedures. As such, there is a pressing need for the establishment of new, non-invasive biomarkers that can gauge the risk of future DKD onset or detect this disease while in its earliest stages.
Certain urinary and plasma protein biomarkers have been linked to the pathophysiology of many forms of renal disease, and some of these biomarkers have even been successfully implemented in clinical settings. The kidneys directly produce urine. It is relatively simple and non-invasive to collect urine protein because it is so stable. It can be a useful biomarker and is difficult to degrade.7,8 Blood samples are also easy to collect, serving as an optimal sample type for efforts to diagnose early-stage DKD.8–10 Proteins found in renal tissue allow for the monitoring of biomolecules’ effects on tissues. As proteomic indicators of DKD, they are currently becoming more and more well-known.11 Indeed, the proteome has long been regarded as an ideal focus for efforts to understand the molecular etiology of disease and to define prognostic or diagnostic biomarkers associated with particular disease states. The use of blood, urine, and renal tissue proteomic analyses to non-invasively detect and monitor DKD has emerged as an increasingly important field that can clarify the pathophysiological mechanisms underlying DKD while identifying key targets for future efforts to prevent subsequent disease progression.12 The systematic examination of these proteomic targets offers more comprehensive insight into DKD and other complex metabolic diseases while also providing a foundation to design prognostic tools and targeted therapies. DKD biomarkers have been the subject of numerous transcriptomics and metabonomics investigations in the past. Lei et al conducted work on transcriptomics,13 and Mu et al conducted experiments on metabonomics.14 Proteomics is the topic of this essay. This article primarily examines and discusses the most recent developments in the proteome analysis of urine, blood, and kidney tissue samples for the purpose of identifying potential specific biomarkers for the diagnosis of DKD.
Proteins and Proteomics
The proteome is a catch-all term that refers to all proteins produced by a given tissue, cell, or organism. A range of proteomic techniques have been leveraged to date to characterize the proteome or the expression of particular protein subsets, including low molecular mass polypeptides. Protein-based biomarkers of DKD have been explored through enzyme-linked immunosorbent assay (ELISAs), 2-way gel electrophoresis (2-DE),15 equivalent labeling for relative and absolute quantification (iTRAQ),16,17 tandem mass labeling (TMT) and mass spectrometry, unlabeled approaches, and biochip analyses.18 Proteomic analyses can enable the establishment of DKD-specific biomarkers through analyses of patient urine, blood, or renal tissue samples,19,20 with advances in the underlying techniques having made the robust and routine screening of biofluid samples increasingly feasible, potentially enabling the detection of novel targets for the treatment of DKD.21 These biomarkers also have the potential to advance current understanding of the mechanistic basis for DKD-related injury and to provide new diagnostic, monitoring, and classification options to support the individualized treatment of affected patients.22 Labeled and unlabeled mass spectrometry methods, which may simultaneously screen thousands of target proteins, are currently the most widely used proteomic tools for locating biomarkers relevant to DKD diagnosis and prognosis.
Urinary Protein Biomarkers of DKD
In addition to being easy to collect in a non-invasive manner, urine can remain stable for years in storage such that even archived urine samples can be used to screen for DKD-related biomarkers.23 Urinary proteomics analyses thus offer an opportunity to define small proteins and peptides characteristic of pathophysiological shifts associated with early-stage DKD. In one study, a proteomic biosignature consisting of 273 different urinary protein fragments known as the CKD273 classified was shown to be capable of differentiating between diabetic kidney disease patients and individuals with other forms of chronic renal disease.24 The CKD273 classifier is a more accurate predictor of the incidence rate of DKD and can aid in the diagnosis, monitoring, and prognosis assessment of DKD patients. As it can detect individuals at risk of developing DKD, it can also help protect these patients from adverse renal outcomes.25 Limonte et al determined that high urinary levels of the lysosomal proteolytic enzyme cathepsin D are linked to intracellular protein degradation, autophagy, and apoptotic cell death.26 Elevated urinary cathepsin D levels are closely associated with rapid eGFR declines, tubular atrophy, tubulointerstitial inflammation, and fibrosis.27 Ahn et al determined that urinary proteomic analyses are more reliable than measurement of albuminuria alone as a tool to predict DKD patient prognosis, with a proteomic biosignature comprised of ACP2, CTSA, GM2A, MUC1, and SPARCL1 offering substantial clinical utility.28 Chen et al determined that β2-microglobulin and Clara-cell protein are protein biomarkers associated with DKD that can aid in predicting the incidence of this condition and associated risks.
ITRAQ, TMT, etc. are technologies that can detect proteins in a specific way.29 Through the use of a 2D-DIGE-MALDIQ-TOF strategy and related techniques, Patel et al were able to detect novel DKD-related protein biomarkers in at-risk individuals corresponding to the processes of renal tubulointerstitial fibrosis and tubulointerstitial fibrosis, including apolipoprotein A1, α-1microglobulin, and zinc α-2 glycoprotein.30,31 Guo et al discovered that - 1-antitrypsin - 1-acid glycoprotein, ceruloplasmin, prostate stem cell antigen, APOA4 and other apolipoprotein AIV are prospective protein biomarkers of DKD in 23 diabetic patients and 16 healthy volunteers.32 Liao et al also observed a significant increase in urinary haptoglobin (Hp) levels in DKD patients, allowing for the more accurate diagnosis and prognostic assessment of individuals with this disease.33 Urinary retinol-binding protein 4 (uRBP4) and SH3 domain-binding glutamic acid-rich-like protein 3 (uSH3BGRL3) protein levels are closely associated with eGFR.34 Through an SDS-PAGE approach, Araumi et al determined that urinary afamin (uAFM), uRBP4, and uSH3BGRL3 levels were elevated in DKD patients relative to individuals without renal damage, underscoring their potential utility as diagnostic biomarkers in this context.20,35,36 Fan et al have also demonstrated that haptoglobin (HPT) and α-1-microglobulin / bicunin precursor (AMBP) are two protein biomarkers that can effectively differentiate between healthy individuals and diabetic patients who are or are not affected by DKD. Urinary proteomic techniques can aid in the non-invasive diagnosis of DKD and the identification of patients considered at high risk.37
The low molecular weight protein RBP is filtered by the glomeruli and ultimately reabsorbed via the proximal tubules, and has been found to offer substantial diagnostic utility in DKD patients who exhibit pronounced albuminuria. Al-Rubeaan et al reported the increased excretion of urinary transferrin, RBP, and serum osteopontin with diabetic kidney disease development, emphasizing the value of these biomarkers when diagnosing type 2 diabetic kidney disease.38 Urinary L-FABP is a recently detected urinary protein biomarker used for early DKD detection, and Panduru et al reported higher urinary L-FABP levels in DKD patients relative to controls in a manner associated with disease severity. Urinary L-FABP thus represents a specific, sensitive protein biomarker capable of guiding early DKD diagnosis.39 Nucleated cells produce the low molecular mass protein cystatin C (CST3), and cysteine aminotransferase activity can be used as a metric for kidney function in diabetic individuals with higher CST3 levels in urine being indicative of renal tubular damage. Through a CE-MS approach, Garg et al determined that urinary CST3 levels were significantly elevated in DKD patients relative to controls (P < 0.05), supporting the diagnostic utility of this protein (P < 0.05), indicating that urinary CST3 has diagnostic value.40 A DKD-related proteomic classifier consisting of collagen fragments, α-microglobulin, β 2-microglobulin (β 2MG), A1AT, uromodulin, and other peptides has also shown promise as a tool for identifying type 2 diabetes patients at a high risk of DKD.41 For further details regarding these urinary protein biomarkers, see Table 1.
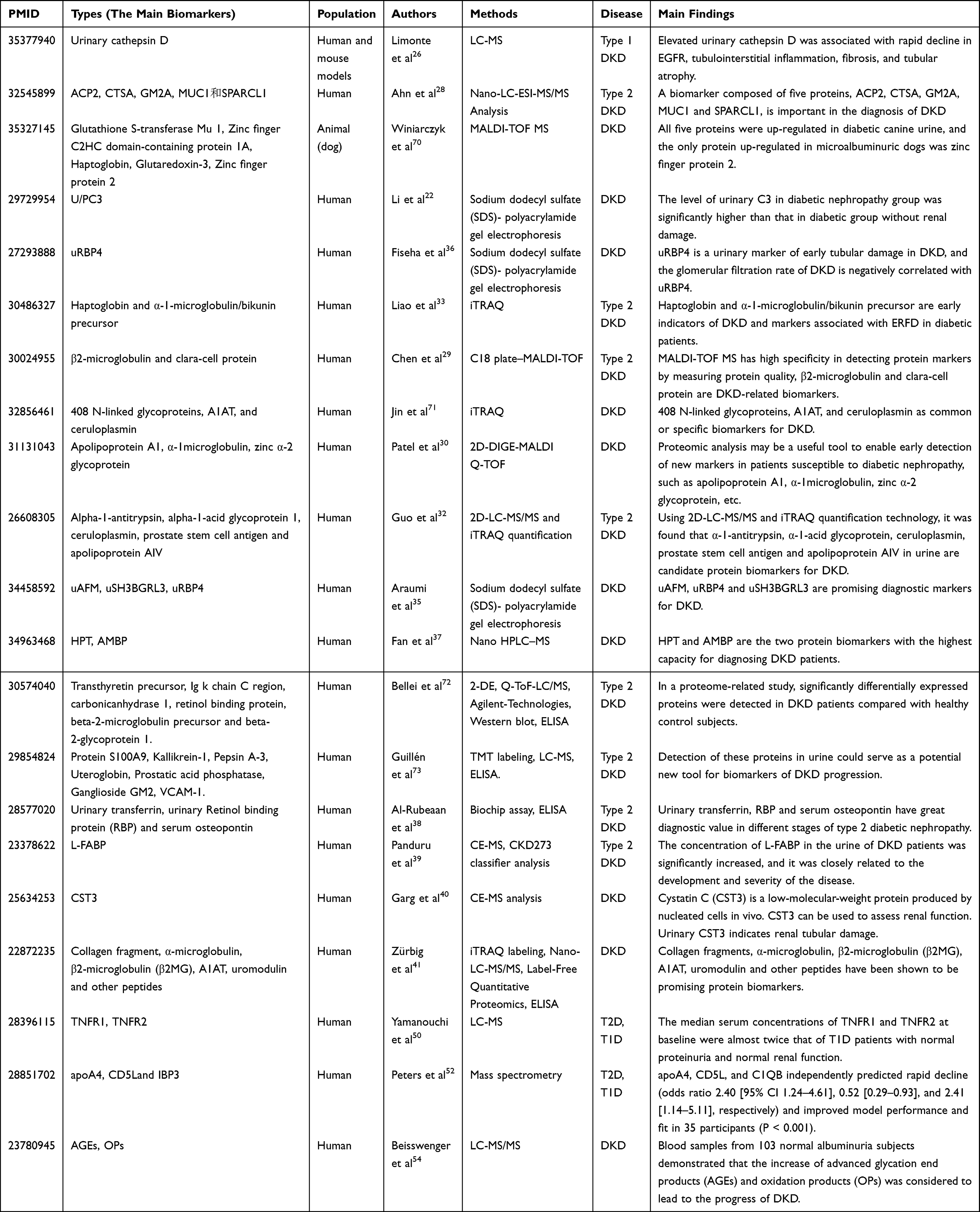 |
Table 1 Biomarkers of Urine Proteomics in DKD |
Blood-Based Protein Biomarkers of DKD
Tubular cells are activated in response to high glucose levels, resulting in the secretion of inflammatory mediators and ECM components that contribute to tubular thinning and cell damage. Glomerular injury-associated proteinuria can act as a stressor that adversely impacts proximal renal tubular cells, driving inflammatory mediator secretion and renal damage. Blood can be kept stable in storage for a number of years and can be used to check for DKD-related biomarkers. Circulating biomarkers can offer insight into kidney damage in patients diagnosed with diabetes,42 offering new potential means of guiding patient diagnosis, treatment, and prognostic assessment.43 Plasma u/PC3 levels in the serum of DKD patients have been shown to be elevated as compared to diabetic individuals free of renal damage, emphasizing the potential diagnostic utility of this serum biomarker.35 Chiang et al determined that SH3BGRL3 can function as an epidermal growth factor receptor conjugate, and that there is a significant positive correlation between uSH3BGRL3 levels and eGFR such that it can serve as a DKD-related biomarker.34 Caseiro et al further detected increases in MMP-9, neutrophil gelatinase-associated lipocalin (NGAL), aminopeptidase N, azurocidin, and kallikrein 1 activity in type 1 DKD patients as compared to healthy individuals, suggesting that this protein biosignature may offer value in this type of DKD.44 Moresco et al also confirmed that circulating NGAL levels correspond to renal tubular function, and a positive correlation has been reported between serum NGAL concentrations and proteinuria whereas these levels are negatively correlated with eGFR.45 The lipocalin protein family member β-trace protein (β-TP), also known as lipoprotein prostaglandin D2 synthase (L-PGDS), is reportedly an independent and reliable serum protein biomarker that responds to eGFR levels more reliably than do anhydride or cystatin.46 Lu et al employed Q-Exactive mass spectrometry and proteomic iTRAQ techniques which ultimately revealed that DKD patient serum exhibited higher concentrations of gelatin, collectin-11, protein tyrosine phosphatase type J receptor (PTPRJ), and protein kinase anchoring protein-7 (AKAP-7), supporting their possible diagnostic value.43 The circulating glycoprotein Hp is primarily produced in the liver, and plasma Hp levels are significantly higher in individuals with DKD. Plasma gelatin protein (PGSN) is primarily produced by skeletal muscle, smooth muscle, and the myocardium. Piktel et al determined that PGSN can promote PKC activation, thereby contributing to renal reactive oxygen species (ROS) production, inflammation, and DKD development.47 DKD patients exhibit higher PGSN levels than do controls, emphasizing the potential value of this protein as a diagnostic biomarker in this pathological context.48 Yang et al reported that serum levels of the inflammatory cytokine tumor necrosis factor-α (TNFα) are significantly correlated with early glomerular dysfunction and early-stage DKD.49 Yamanouchi et al discovered that 221 individuals with type 2 diabetes and 279 patients with type 1 diabetes had higher serum levels of the tumor necrosis factor receptors (TNFR) 1 and 2. End-stage renal disease(ESRD), T2D, and T1D were all highly correlated with TNFR. According to the study, this indicator had an 85% predictive value and a 72% sensitivity.50,51 In Phase II of the diabetes study, Peters et al used mass spectroscopy on 35 community patients. They discovered that the participants’ plasma levels of apolipoprotein (apo) A-IV (apoA4), CD5 antigen like (CD5L), and insulin-like growth factor binding protein 3 (IBP3) independently predicted rapid decline (odds ratio 2.40 [95% CI 1.24–4.61], 0.52 [0.29–0.93], and 2.41 [1.14–5 (P < 0.001). New plasma biomarkers (apoA4, CD5L, and IBP3) have been discovered by recent study that may help predict the rapid loss in renal function in type 2 diabetic patients. Among these, the increase in ApoA4 level is a precursor to mild to moderate DKD, the increase in IBP3 level is connected to low baseline EGFR, and the inhibitor of apoptosis of CD5L or macrophage protein is related to immunological and inflammatory response.52,53 Beisswenger et al performed an LC-MS/MS investigation on blood samples from 103 people with normal albuminuria diabetes and discovered that the progression of DKD was thought to be accompanied by an increase in advanced glycation end products (AGEs) and oxidation products (OPs).54 El-Asrar et al found soluble CD40 ligand (CD40L) to represent a promising plasma protein biomarker associated with progressive DKD that can participate in endothelial injury and inflammatory activity.55 In a separate analysis, Kobayashi et al detected an independent association between the LAYN, DLL1, MAPK11, MATN2, Endostatin, and ROR1 proteins and the risk of chronic renal failure owing to their role in the progression of DKD, emphasizing their promise as targets for renoprotective therapeutic interventions.27 Niewczas et al additionally determined that plasma TNF-R1 and TNF-R2 play roles in renal inflammation and can predict the decline in renal function that is associated with DKD incidence.56 For further details regarding blood-based protein biomarkers of DKD characterized to date, see Table 2.
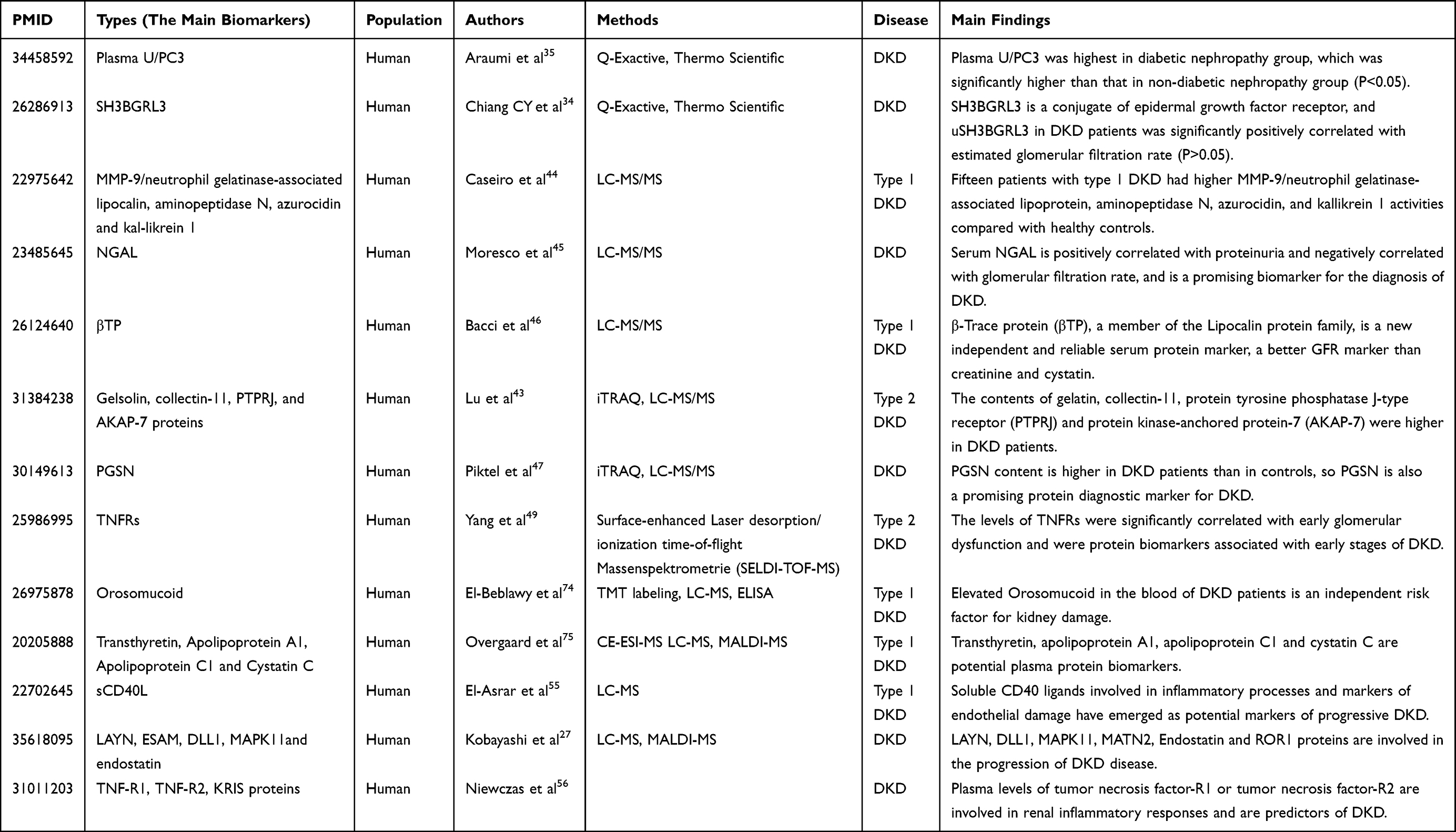 |
Table 2 Biomarkers of Blood Proteomics in DKD |
Renal Tissue Protein Biomarkers of DKD
Recent advances in proteomic techniques have enabled the routine assessment of proteins in urine, plasma, and kidney tissue samples, allowing for the more in-depth interrogation of the mechanistic basis for DKD progression.57 Renal protein levels may reflect the actual pathogenesis of tubular atrophy, glomerular injury, and tubulointerstitial fibrosis. To aid in the characterization of renal proteomic profiles, high-throughput matrix-assisted laser desorption/ionization imaging MS has been leveraged to analyze the proteins present in tissue sections.58 Renal tissue proteomic analyses can detect biomarkers of glomerular injury such as albumin, as well as renal tubular injury-related proteins including α1MG, β2MG, RBP4, N acetyl β D glucosaminidase (NAG), alkaline phosphatase (ALP), gamma-glutamyltransferase (GGT), liver type fatty acid binding protein (LFABP), NGAL, and renal injury molecule 1 (KIM1).59 Moresco et al determined that the transmembrane glycoprotein Kim-1 is specifically expressed on proximal tubular cells on the apical membrane, serving as a reliable biomarker of proximal tubule injury that is closely linked to the extent of renal tubulointerstitial injury and fibrosis, offering a tool to diagnose early-stage DKD.45 Vaidy et al observed elevated NAG and Kim-1 levels in type 1 diabetes patients with microalbuminuria, with these levels being even higher in patients with albuminuria, emphasizing the link between these protein biomarkers and type 1 diabetes-related DKD.60 The 25 kDa lipocalin family member NGAL is often studied as a sensitive, specific biomarker for renal tubular injury that can predict DKD development.61 Regucalcin is a mediator of cellular Ca21 homeostasis, oxidative stress regulation, and ascorbic acid biosynthesis. Using a 2D-DGE and MS-based approach, Zubiri et al compared the proteomic profiles of renal tissue samples from rats with early-stage DKD and observed significant decreases in regucalin levels in tissues from DKD model rats relative to controls.62,63 The matrix protein TIMP3 (tissue inhibitor of metalloproteinases) can inhibit proteolytic enzyme activity and receptor activation in the ECM. DKD has been shown to be associated with TIMP3 downregulation.64 Rossi et al employed differential proteomic analyses of renal tissues from 6-week-old wild-type (WT) and Timp3−/− mice using a nano-liquid chromatography-electrospray ionization-tandem mass spectrometry (nLC-ESI-MSE) approach, observing significant TIMP3 downregulation in DKD mice consistent with its possible relevance as a therapeutic target in this disease.65 The cell adhesion molecule periostin (POSTN) has also been posited to serve as a protein-based marker of diabetes-related renal damage, with elevated glomerular POSTN concentrations in patients with type 2 diabetes even before the onset of significant proteinuria such that it may hold value as a protein marker of early-stage renal injury.66 Increased glomerular ECM protein deposition is a primary mechanism governing the pathogenesis of DKD, contributing to higher glomerular membrane ECM accumulation that ultimately contributes to glomerular membrane dilatation and glomerulosclerosis.67 LC-MS/MS and iTRAQ techniques have both been used to compare renal tissues from DKD and nondiabetic patients. Nakatani et al determined that both nephronectin and apolipoprotein E are important mediators of renal extracellular matrix development, while renal connexin is an integrin α8β1 ligand associated with diabetic glomerulosclerosis onset and progression. Further studies of these and other targets in patient renal tissues may aid in further understanding of DKD.68 Fugmann et al further determined that significant renal Vanin-1 and cystatin C upregulation were evident in their model system, corresponding to proinflammatory and cytoprotective effects, while uromodulin was downregulated in diabetic model rates such that these proteins may offer value as therapeutic targets in DKD.69 For further details regarding known renal tissue protein biomarkers of DKD, see Table 3.
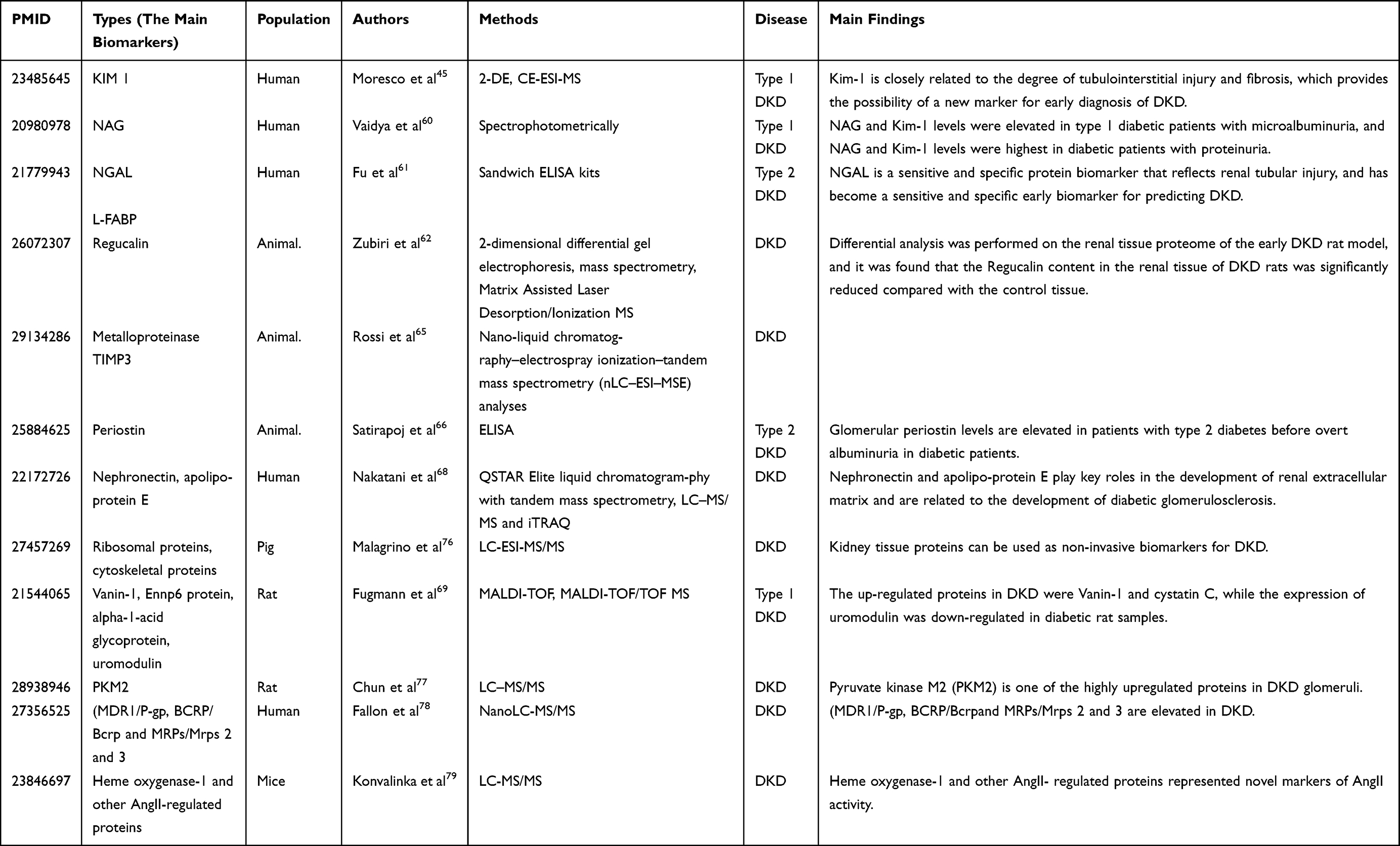 |
Table 3 Biomarkers of Renal Proteomics in DKD |
Conclusions and Outlook
As the studies discussed herein emphasize, there is growing interest in the use of alternative biomarkers other than urinary albumin and creatinine when detecting early-stage DKD, including protein-based biomarkers present in urine, blood, and renal tissue samples. Proteomic technologies offer an increasingly robust means of detecting low-abundance proteins related to the progressive pathogenesis of kidney injury.
Numerous biomarkers discovered thus far have demonstrated strong diagnostic potential, including urine-based CKD273 proteomic biomarkers, which have demonstrated excellent potential. In the clinic, more and more diagnostics are now available, allowing for the independent and accurate prediction of microalbuminuria associated with DKD. These proteomic biomarker analyses are often simpler and less invasive than standard diagnostic techniques, potentially reducing the need for renal biopsy procedures as the primary means of diagnosing DKD. These strategies also offer a theoretical foundation for more reliably treating this disease and preventing its progression. Despite such promise, however, proteomics-based biomarker panels are not routinely applied in most clinical chemistry laboratories. Further research focused on these proteomic biomarkers will guide the early and noninvasive diagnosis of DKD, allow for more reliable patient monitoring, and support better patient outcomes at many levels. We anticipate that further research efforts centered on the role of targeted proteomics in diabetic kidney disease will yield novel breakthroughs in this field with clear clinical value.
Ethics Statement
This review does not involve animal or human trials, therefore it does not require ethical review.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This review is supported by Yunnan Fundamental Research Projects (grant NO. 202001AT070145, 202101AT070288) and Changzhou Health Commission Youth Project (grant NO. QN202206).
Disclosure
The authors report no conflicts of interest in this review.
References
1. Liu S, Gui Y, Wang MS, et al. Serum integrative omics reveals the landscape of human diabetic kidney disease. Mol Metab. 2021;54:101367. doi:10.1016/j.molmet.2021.101367
2. Tofte N, Lindhardt M, Adamova K, et al. Early detection of diabetic kidney disease by urinary proteomics and subsequent intervention with spironolactone to delay progression (PRIORITY): a prospective observational study and embedded randomised placebo-controlled trial. Lancet Diabetes Endocrinol. 2020;8:301–312. doi:10.1016/S2213-8587(20)30026-7
3. Gordin D, Shah H, Shinjo T, et al. Characterization of glycolytic enzymes and pyruvate kinase M2 in type 1 and 2 diabetic nephropathy. Diabetes Care. 2019;42:1263–1273. doi:10.2337/dc18-2585
4. Uyy E, Suica VI, Boteanu RM, et al. Diabetic nephropathy associates with deregulation of enzymes involved in kidney sulphur metabolism. J Cell Mol Med. 2020;24:12131–12140. doi:10.1111/jcmm.15855
5. Shah IM, Mackay SP, McKay GA. Therapeutic strategies in the treatment of diabetic nephropathy - a translational medicine approach. Curr Med Chem. 2009;16:997–1016. doi:10.2174/092986709787581897
6. Nicholas SB. Use of urinary proteomics in diagnosis and monitoring of diabetic kidney disease. Lancet Diabetes Endocrinol. 2020;8:261–262. doi:10.1016/S2213-8587(20)30067-X
7. Klein J, Ramirez-Torres A, Ericsson A, et al. Urinary peptidomics provides a noninvasive humanized readout of diabetic nephropathy in mice. Kidney Int. 2016;90:1045–1055. doi:10.1016/j.kint.2016.06.023
8. Shao C, Wang Y, Gao Y. Applications of urinary proteomics in biomarker discovery. Sci China Life Sci. 2011;54:409–417. doi:10.1007/s11427-011-4162-1
9. Greco V, Piras C, Pieroni L, et al. Direct assessment of plasma/serum sample quality for proteomics biomarker investigation. Methods Mol Biol. 2017;1619:3–21.
10. Overgaard AJ, Thingholm TE, Larsen MR, et al. Quantitative iTRAQ-based proteomic identification of candidate biomarkers for diabetic nephropathy in plasma of type 1 diabetic patients. Clin Proteomics. 2010;6:105–114. doi:10.1007/s12014-010-9053-0
11. Cefalu WT, Bakris G, Blonde L, Boulton A, DAlessio D, Groot M. Standards of medical care in diabetes-2017: summary of Revisions. Diabetes Care. 2017;40:S4–S5. doi:10.2337/dc17-S003
12. Aluksanasuwan S, Plumworasawat S, Malaitad T, et al. High glucose induces phosphorylation and oxidation of mitochondrial proteins in renal tubular cells: a proteomics approach. Sci Rep. 2020;10:5843. doi:10.1038/s41598-020-62665-w
13. Lei L, Bai Y, Fan Y, et al. Comprehensive diagnostics of diabetic nephropathy by transcriptome RNA sequencing. Diabetes Metab Syndr Obes. 2022;15:3069–3080. doi:10.2147/DMSO.S371026
14. Mu X, Yang M, Ling P, et al. Acylcarnitines: can they be biomarkers of diabetic nephropathy? Diabetes Metab Syndr Obes. 2022;15:247–256. doi:10.2147/DMSO.S350233
15. Shen L, Zhao D, Chen Y, et al. Comparative proteomics analysis of serum proteins in gestational diabetes during early and middle stages of pregnancy. Proteomics Clin Appl. 2019;13:e1800060. doi:10.1002/prca.201800060
16. Moulder R, Bhosale SD, Goodlett DR, et al. Analysis of the plasma proteome using iTRAQ and TMT-based isobaric labeling. Mass Spectrom Rev. 2018;37(5):583–606. doi:10.1002/mas.21550
17. Bringans SD, Ito J, Stoll T, et al. Comprehensive mass spectrometry based biomarker discovery and validation platform as applied to diabetic kidney disease. EuPA Open Proteom. 2017;14:1–10. doi:10.1016/j.euprot.2016.12.001
18. Frantzi M, Latosinska A, Fluhe L, et al. Developing proteomic biomarkers for bladder cancer: towards clinical application. Nat Rev Urol. 2015;12:317–330. doi:10.1038/nrurol.2015.100
19. Geyer PE, Holdt LM, Teupser D, et al. Revisiting biomarker discovery by plasma proteomics. Mol Syst Biol. 2017;13:942. doi:10.15252/msb.20156297
20. Siwy J, Zurbig P, Argiles A, et al. Noninvasive diagnosis of chronic kidney diseases using urinary proteome analysis. Nephrol Dial Transplant. 2017;32:2079–2089. doi:10.1093/ndt/gfw337
21. Beasley-Green A. Urine proteomics in the era of mass spectrometry. Int Neurourol J. 2016;20:S70–75. doi:10.5213/inj.1612720.360
22. Li XQ, Chang DY, Chen M, et al. Complement activation in patients with diabetic nephropathy. Diabetes Metab. 2019;45:248–253. doi:10.1016/j.diabet.2018.04.001
23. Yang J, Liu D, Liu Z. Integration of metabolomics and proteomics in exploring the endothelial dysfunction mechanism induced by serum exosomes from diabetic retinopathy and diabetic nephropathy patients. Front Endocrinol. 2022;13:830466. doi:10.3389/fendo.2022.830466
24. Lindhardt M, Persson F, Zurbig P, et al. Urinary proteomics predict onset of microalbuminuria in normoalbuminuric type 2 diabetic patients, a sub-study of the DIRECT-Protect 2 study. Nephrol Dial Transplant. 2017;32(11):1866–1873. doi:10.1093/ndt/gfw292
25. Khan NU, Lin J, Liu X, et al. Insights into predicting diabetic nephropathy using urinary biomarkers. Biochim Biophys Acta Proteins Proteom. 2020;1868:140475. doi:10.1016/j.bbapap.2020.140475
26. Limonte CP, Valo E, Drel V, et al. Urinary proteomics identifies cathepsin D as a biomarker of rapid eGFR decline in type 1 diabetes. Diabetes Care. 2022;45:1416–1427. doi:10.2337/dc21-2204
27. Kobayashi H, Looker HC, Satake E, et al. Results of untargeted analysis using the SOMAscan proteomics platform indicates novel associations of circulating proteins with risk of progression to kidney failure in diabetes. Kidney Int. 2022;102:370–381. doi:10.1016/j.kint.2022.04.022
28. Ahn HS, Kim JH, Jeong H. et al. Differential urinary proteome analysis for predicting prognosis in type 2 diabetes patients with and without renal dysfunction. Int J Mol Sci. 2020:21. doi:10.3390/ijms22010021
29. Chen CJ, Liao WL, Chang CT, et al. Urine proteome analysis by C18 plate-matrix-assisted laser desorption/ionization time-of-flight mass spectrometry allows noninvasive differential diagnosis and prediction of diabetic nephropathy. PLoS One. 2018;13:e0200945. doi:10.1371/journal.pone.0200945
30. Patel DN, Kalia K. Characterization of low molecular weight urinary proteins at varying time intervals in type 2 diabetes mellitus and diabetic nephropathy patients. Diabetol Metab Syndr. 2019;11:39. doi:10.1186/s13098-019-0430-1
31. Chebotareva N, Vinogradov A, McDonnell V, et al. Urinary protein and peptide markers in chronic kidney disease. Int J Mol Sci. 2021;23(1):22. doi:10.3390/ijms23010022
32. Guo Z, Liu X, Li M, et al. Differential urinary glycoproteome analysis of type 2 diabetic nephropathy using 2D-LC-MS/MS and iTRAQ quantification. J Transl Med. 2015;13:371. doi:10.1186/s12967-015-0712-9
33. Liao WL, Chang CT, Chen CC, et al. Urinary proteomics for the early diagnosis of diabetic nephropathy in Taiwanese patients. J Clin Med. 2018;7:483.
34. Chiang CY, Pan CC, Chang HY, et al. SH3BGRL3 protein as a potential prognostic biomarker for urothelial carcinoma: a novel binding partner of epidermal growth factor receptor. Clin Cancer Res. 2015;21:5601–5611. doi:10.1158/1078-0432.CCR-14-3308
35. Araumi A, Osaki T, Ichikawa K, et al. Urinary and plasma proteomics to discover biomarkers for diagnosing between diabetic nephropathy and minimal change nephrotic syndrome or membranous nephropathy. Biochem Biophys Rep. 2021;27:101102. doi:10.1016/j.bbrep.2021.101102
36. Fiseha T, Tamir Z. Urinary markers of tubular injury in early diabetic nephropathy. Int J Nephrol. 2016;2016:4647685. doi:10.1155/2016/4647685
37. Fan G, Gong T, Lin Y, et al. Urine proteomics identifies biomarkers for diabetic kidney disease at different stages. Clin Proteomics. 2021;18:32. doi:10.1186/s12014-021-09338-6
38. Al-Rubeaan K, Siddiqui K, Al-Ghonaim MA, et al. Assessment of the diagnostic value of different biomarkers in relation to various stages of diabetic nephropathy in type 2 diabetic patients. Sci Rep. 2017;7(1):2684. doi:10.1038/s41598-017-02421-9
39. Panduru NM, Forsblom C, Saraheimo M, et al. Urinary liver-type fatty acid-binding protein and progression of diabetic nephropathy in type 1 diabetes. Diabetes Care. 2013;36:2077–2083. doi:10.2337/dc12-1868
40. Garg V, Kumar M, Mahapatra HS, et al. Novel urinary biomarkers in pre-diabetic nephropathy. Clin Exp Nephrol. 2015;19(5):895–900. doi:10.1007/s10157-015-1085-3
41. Zurbig P, Jerums G, Hovind P, et al. Urinary proteomics for early diagnosis in diabetic nephropathy. Diabetes. 2012;61:3304–3313. doi:10.2337/db12-0348
42. Canadas-Garre M, Anderson K, McGoldrick J, et al. Proteomic and metabolomic approaches in the search for biomarkers in chronic kidney disease. J Proteomics. 2019;193:93–122. doi:10.1016/j.jprot.2018.09.020
43. Lu H, Deng S, Zheng M, et al. iTRAQ plasma proteomics analysis for candidate biomarkers of type 2 incipient diabetic nephropathy. Clin Proteomics. 2019;16(1):33. doi:10.1186/s12014-019-9253-1
44. Caseiro A, Ferreira R, Quintaneiro C, et al. Protease profiling of different biofluids in type 1 diabetes mellitus. Clin Biochem. 2012;45:1613–1619. doi:10.1016/j.clinbiochem.2012.08.027
45. Moresco RN, Sangoi MB, De Carvalho JA, et al. Diabetic nephropathy: traditional to proteomic markers. Clin Chim Acta. 2013;421:17–30. doi:10.1016/j.cca.2013.02.019
46. Bacci MR, Cavallari MR, de Rozier-Alves RM, et al. The impact of lipocalin-type-prostaglandin-D-synthase as a predictor of kidney disease in patients with type 2 diabetes. Drug Des Devel Ther. 2015;9:3179–3182. doi:10.2147/DDDT.S82100
47. Piktel E, Levental I, Durnas B, et al. Plasma gelsolin: indicator of inflammation and its potential as a diagnostic tool and therapeutic target. Int J Mol Sci. 2018;20(1):19. doi:10.3390/ijms20010019
48. Cheng Y, Hu X, Liu C, et al. Gelsolin inhibits the inflammatory process induced by LPS. Cell Physiol Biochem. 2017;41:205–212. doi:10.1159/000456043
49. Yang Y, Zhang S, Lu B, et al. Predicting diabetic nephropathy by serum proteomic profiling in patients with type 2 diabetes. Wien Klin Wochenschr. 2015;127:669–674. doi:10.1007/s00508-014-0679-1
50. Yamanouchi M, Skupien J, Niewczas MA, et al. Improved clinical trial enrollment criterion to identify patients with diabetes at risk of end-stage renal disease. Kidney Int. 2017;92:258–266. doi:10.1016/j.kint.2017.02.010
51. Saulnier PJ, Gand E, Velho G, et al. Association of circulating biomarkers (Adrenomedullin, TNFR1, and NT-proBNP) with renal function decline in patients with type 2 diabetes: a French prospective cohort. Diabetes Care. 2017;40:367–374. doi:10.2337/dc16-1571
52. Peters KE, Davis WA, Ito J, et al. Identification of novel circulating biomarkers predicting rapid decline in renal function in type 2 diabetes: the Fremantle diabetes study Phase II. Diabetes Care. 2017;40:1548–1555. doi:10.2337/dc17-0911
53. Peters KE, Xu J, Bringans SD, et al. PromarkerD predicts renal function decline in type 2 diabetes in the Canagliflozin Cardiovascular Assessment Study (CANVAS). J Clin Med. 2020;9(10):3212. doi:10.3390/jcm9103212
54. Beisswenger PJ, Howell SK, Russell GB, et al. Early progression of diabetic nephropathy correlates with methylglyoxal-derived advanced glycation end products. Diabetes Care. 2013;36(10):3234–3239. doi:10.2337/dc12-2689
55. El-Asrar MA, Adly AA, Ismail EA. Soluble CD40L in children and adolescents with type 1 diabetes: relation to microvascular complications and glycemic control. Pediatr Diabetes. 2012;13:616–624. doi:10.1111/j.1399-5448.2012.00881.x
56. Niewczas MA, Pavkov ME, Skupien J, et al. A signature of circulating inflammatory proteins and development of end-stage renal disease in diabetes. Nat Med. 2019;25:805–813. doi:10.1038/s41591-019-0415-5
57. Barutta F, Bellini S, Canepa S, et al. Novel biomarkers of diabetic kidney disease: current status and potential clinical application. Acta Diabetol. 2021;58(7):819–830. doi:10.1007/s00592-020-01656-9
58. Blutke A. Opening a treasure chest: glomerular proteome analyses of formalin-fixed paraffin-embedded kidney tissue in the investigation of diabetic nephropathy. Nephrol Dial Transplant. 2012;27(5):1695–1698. doi:10.1093/ndt/gfs082
59. Hoyer KJR, Dittrich S, Bartram MP, et al. Quantification of molecular heterogeneity in kidney tissue by targeted proteomics. J Proteomics. 2019;193:85–92. doi:10.1016/j.jprot.2018.03.001
60. Vaidya VS, Niewczas MA, Ficociello LH, et al. Regression of microalbuminuria in type 1 diabetes is associated with lower levels of urinary tubular injury biomarkers, kidney injury molecule-1, and N-acetyl-beta-D-glucosaminidase. Kidney Int. 2011;79:464–470. doi:10.1038/ki.2010.404
61. Fu WJ, Xiong SL, Fang YG, et al. Urinary tubular biomarkers in short-term type 2 diabetes mellitus patients: a cross-sectional study. Endocrine. 2012;41:82–88. doi:10.1007/s12020-011-9509-7
62. Zubiri I, Posada-Ayala M, Benito-Martin A, et al. Kidney tissue proteomics reveals regucalcin downregulation in response to diabetic nephropathy with reflection in urinary exosomes. Transl Res. 2015;166:474–484 e474. doi:10.1016/j.trsl.2015.05.007
63. de la Cuesta F, Barderas MG, Calvo E, et al. Secretome analysis of atherosclerotic and non-atherosclerotic arteries reveals dynamic extracellular remodeling during pathogenesis. J Proteomics. 2012;75:2960–2971. doi:10.1016/j.jprot.2011.12.005
64. Mi H, Poudel S, Muruganujan A, et al. PANTHER version 10: expanded protein families and functions, and analysis tools. Nucleic Acids Res. 2016;44(D1):D336–D342. doi:10.1093/nar/gkv1194
65. Rossi C, Marzano V, Consalvo A, et al. Proteomic and metabolomic characterization of streptozotocin-induced diabetic nephropathy in TIMP3-deficient mice. Acta Diabetol. 2018;55:121–129. doi:10.1007/s00592-017-1074-y
66. Satirapoj B, Tassanasorn S, Charoenpitakchai M, et al. Periostin as a tissue and urinary biomarker of renal injury in type 2 diabetes mellitus. PLoS One. 2015;10:e0124055. doi:10.1371/journal.pone.0124055
67. Jung CY, Yoo TH. Pathophysiologic mechanisms and potential biomarkers in diabetic kidney disease. Diabetes Metab J. 2022;46:181–197. doi:10.4093/dmj.2021.0329
68. Nakatani S, Wei M, Ishimura E, et al. Proteome analysis of laser microdissected glomeruli from formalin-fixed paraffin-embedded kidneys of autopsies of diabetic patients: nephronectin is associated with the development of diabetic glomerulosclerosis. Nephrol Dial Transplant. 2012;27:1889–1897. doi:10.1093/ndt/gfr682
69. Fugmann T, Borgia B, Revesz C, et al. Proteomic identification of vanin-1 as a marker of kidney damage in a rat model of type 1 diabetic nephropathy. Kidney Int. 2011;80:272–281. doi:10.1038/ki.2011.116
70. Winiarczyk D, Winiarczyk M, Michalak K, et al. Urinary proteome differences in canine diabetes with and without the presence of microalbuminuria. Animals. 2022;12(6):748. doi:10.3390/ani12060748
71. Jin J, Gong J, Zhao L, et al. iTRAQ-based comparative proteomics analysis reveals specific urinary biomarkers for various kidney diseases. Biomark Med. 2020;14(10):839–854. doi:10.2217/bmm-2019-0556
72. Bellei E, Monari E, Bergamini S, et al. Urinary proteomics in biomarker discovery of kidney-related disorders: diabetic nephropathy and drug-induced nephrotoxicity in chronic headache. EJIFCC. 2018;29:290–297.
73. Guillen-Gomez E, Bardaji-de-quixano B, Ferrer S, et al. Urinary proteome analysis identified neprilysin and VCAM as proteins involved in diabetic nephropathy. J Diabetes Res. 2018;2018:6165303. doi:10.1155/2018/6165303
74. El-Beblawy NM, Andrawes NG, Ismail EA, et al. Serum and urinary orosomucoid in young patients with type 1 diabetes: a link between inflammation, microvascular complications, and subclinical atherosclerosis. Clin Appl Thromb Hemost. 2016;22:718–726. doi:10.1177/1076029616637185
75. Overgaard AJ, Hansen HG, Lajer M, et al. Plasma proteome analysis of patients with type 1 diabetes with diabetic nephropathy. Proteome Sci. 2010;8:4. doi:10.1186/1477-5956-8-4
76. Malagrino PA, Venturini G, Yogi PS, et al. Proteome analysis of acute kidney injury - Discovery of new predominantly renal candidates for biomarker of kidney disease. J Proteomics. 2017;151:66–73. doi:10.1016/j.jprot.2016.07.019
77. Chun N, Wyatt CM, He JC. Identification of a protective proteomic signature and a potential therapeutic target in diabetic nephropathy. Kidney Int. 2017;92:780–781. doi:10.1016/j.kint.2017.08.002
78. Fallon JK, Smith PC, Xia CQ, et al. Quantification of four efflux drug transporters in liver and kidney across species using targeted quantitative proteomics by isotope dilution NanoLC-MS/MS. Pharm Res. 2016;33:2280–2288. doi:10.1007/s11095-016-1966-5
79. Konvalinka A, Zhou J, Dimitromanolakis A, et al. Determination of an angiotensin II-regulated proteome in primary human kidney cells by stable isotope labeling of amino acids in cell culture (SILAC). J Biol Chem. 2013;288:24834–24847. doi:10.1074/jbc.M113.485326
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Neutrophil Extracellular Traps in Diabetic Kidney Disease: Mechanisms of Pathogenesis and Emerging Therapeutic Strategies
Wang B, Zhang R, Liu X, Shang Y, Jin T, Gao C, Yang N, Jin J, He Q
Drug Design, Development and Therapy 2026, 20:583077
Published Date: 21 February 2026
Trimethylamine N-Oxide Combined with Phenylacetylglutamine as Potential Biomarkers for Diabetic Kidney Disease
Xiong G, Fang Q, Wu H, Zhang D, Wang J, Qin Y, Chen Z, Wu Y, Lei Y, Cui Y, Chen L, Li X, Li Y, Ouyang D
Diabetes, Metabolic Syndrome and Obesity 2026, 19:592052
Published Date: 29 May 2026