Back to Journals » Infection and Drug Resistance » Volume 16
Molecular Epidemiology and Characterization of Multidrug-Resistant MRSA ST398 and ST239 in Himachal Pradesh, India
Authors Patil S ![]() , Dong S
, Dong S ![]() , Sharma D, Lopes BS, Hanafiah A
, Sharma D, Lopes BS, Hanafiah A ![]() , Chen X, Wen F
, Chen X, Wen F
Received 3 March 2023
Accepted for publication 15 April 2023
Published 20 April 2023 Volume 2023:16 Pages 2339—2348
DOI https://doi.org/10.2147/IDR.S409037
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Sandip Patil,1,2 Shaowei Dong,2 Devender Sharma,3,4 Bruno Silvester Lopes,5,6 Alfizah Hanafiah,7 Xiaowen Chen,2 Feiqiu Wen1,2
1Department of Haematology and Oncology, Shenzhen Children’s Hospital, Shenzhen, People’s Republic of China; 2Paediatric Research Institute, Shenzhen Children’s Hospital, Shenzhen, People’s Republic of China; 3Department of Microbiology, Himachal Dental College, Sundar Nagar, Himachal Pradesh, India; 4School of Biotechnology, Shoolini University, Solan, Himachal Pradesh, India; 5School of Health and Life Sciences, Teesside University, Middlesbrough, TS1 3BA, UK; 6National Horizons Centre, Teesside University, Darlington, DL1 1HG, UK; 7Department of Medical Microbiology and Immunology, Faculty of Medicine, Universiti Kebangsaan Malaysia, Kuala Lumpur, Malaysia
Correspondence: Feiqiu Wen, Department of Haematology and Oncology, Shenzhen Children’s Hospital, Shenzhen, Guangdong, People’s Republic of China, Tel +86-755-83009888, Email [email protected]
Aim: Methicillin-resistant Staphylococcus aureus (MRSA) is a common cause of severe and difficult-to-treat infections in humans and animals. We aimed to identify the predominant lineages of methicillin-resistant S. aureus in Himachal Pradesh, India, to understand the genomic epidemiology along with the genotypic and phenotypic characteristics.
Methods: We isolated 250 S. aureus from two district hospitals in Himachal Pradesh, India. Methicillin-Resistant S. aureus (MRSA) isolates were subjected to MLST, SCCmec typing, and resistance as well as virulence determinants were determined by PCR and sequencing. Bio-typing was also performed for source tracking.
Results: A 17.6% (44/250) of isolates were classified as MRSA by both the MRSA detection kit and disc diffusion methods. Antimicrobial Susceptibility Testing of MRSA isolates (n = 44) showed high resistance to oxacillin (77.27%), erythromycin (77.27%), tetracycline (75%), cefoxitin (65.9%), and gentamicin (61.36%), while low resistance was observed for teicoplanin (36.36%), vancomycin and levofloxacin (31.81%) and fusidic acid (18.18%). All isolates were sensitive to linezolid, quinupristin-dulfopristin, dalbavancin, and cefazoline. The SCCmec-II was observed in 20.45% of isolates, SCCmec-I in 11.36%, SCCmec-III in 9%, SCCmec-IV in 40.9% and SCCmec-V in 18.18%. The mecA gene was present in all isolates (n = 44) and 50% also had the vanA gene. 35% of isolates had the lukS-PV/lukf-PV toxin gene and 11.36% had the co-existence of mecA, vanA, and lukS-PV/lukf-PV. The major strain was ST398 (39%) followed by ST239 (27%), ST217 (16%), ST121 (11%), and ST338 (7%). The MRSA isolates produced staphylokinase and β-hemolysis but were negative for bovine plasma coagulation tests.
In Conclusion: The predominant MRSA clones in Himachal Pradesh, India, were hospital-associated multi-drug resistant-MRSA ST239 with PVL and community-associated MRSA ST398.
Keywords: MRSA, molecular epidemiology, antimicrobial resistance, SCCmec, vanA, lukS-PV/lukf-PV
Introduction
Increasing antibiotic resistance is a worrisome trend being observed worldwide. Methicillin-resistant Staphylococcus aureus (MRSA) was first reported in the United Kingdom (UK) in 1961 and has since been reported throughout the world as a nosocomial pathogen.1 A steady increase in the occurrence of MRSA strains has been reported in hospitals globally including in India.2,3 MRSA is a notorious pathogen that can withstand and develop resistance against the available empirical drugs of choice.4 The availability of sensitive and specific methods for the accurate detection of antibiotic resistance in these bacteria has become an important tool in clinical diagnosis. Since phenotypic typing methods cannot discriminate accurately and are highly dependent on growth conditions.5 The use of molecular typing is, therefore, warranted.6 The mecA gene, a structural determinant that encodes penicillin-binding protein 2a (PBP2a) is considered one of the useful molecular markers of putative MRSA.7 The methicillin resistance is primarily attributed to overexpression of PBP2a which has a low affinity to β-lactam antibiotics. However, some other mechanisms are also responsible for methicillin resistance such as the efflux pumps.8 Vancomycin was considered to be the best alternative for the treatment of MRSA.9 However, several reports globally reveal the emergence of vancomycin-resistant S. aureus (VRSA) which was first reported in Japan in 1996.10 The resistance was believed to be due to the thickened cell wall in which many vancomycin molecules were trapped. The trapped molecules clog the peptidoglycan meshwork which acts as a physical barrier towards further incoming vancomycin molecules resulting in complete resistance to vancomycin (MIC ≥ 32 µg/mL). The USA first reported on VRSA in 2002 which was recovered from a foot wound of a diabetic patient receiving long-term vancomycin therapy.11 Vancomycin-resistant S. aureus (VRSA) confers resistance as a result of plasmid-borne vanA which is part of an operon encoding enzymes that result in modification or elimination of the vancomycin-binding site.12 Since 2002, VRSA has been reported globally in countries such as India, Pakistan, Portugal, and USA.13 S. aureus is armed with the virulence genes such as lukS-PV/lukf-PV which produces the Panton-Valentine Leukocidin (PVL) which has a key role in the pathogenesis and is linked with community-associated MRSA (CA-MRSA) and has more virulence potential compared to the hospital-associated MRSA (HA-MRSA).14 This gene encodes for a pore-forming cytotoxin which is responsible for tissue necrosis and leukocyte destruction. The virulence gene is frequently present in CA-MRSA and is associated with various virulence factors, such as PVL-stable markers of CA-MRSA cases worldwide. Both Staphylococcal chromosomal cassette mecA (SCCmecA) and detection of the PVL production are useful tools for the molecular characterization of HA- MRSA and CA-MRSA isolates.15 In conclusion, multi-drug resistant (MDR) MRSA with vanA/lukS-PV/lukf-PV spread Asian countries including India in the past couple of years show a predominance of major clones such as ST239, and ST5 (HA-MRSA) while ST59, ST338, ST30, and ST72 which are associated with CA-MRSA.16 Although there have been few epidemiological studies of MRSA from other provisions of India published but knowledge of the entire MRSA population and clone dissemination in hospital settings from north India is still quite limited.17 The genotypic characteristics of MRSA clones are valuable for understanding MRSA evolution and dissemination. MRSA profiling in a targeted area is crucial in monitoring its emergence and spread and informing prevention strategies. During the past years, molecular methods have overcome the traditional phenotypic methods regarding the characterization of MRSA. However, sources of S. aureus can be identified by using the simplified complement genotyping system published by Devriese which is cost-effective.18 The present study aims to understand the molecular epidemiology and investigate the antimicrobial resistance profile of MRSA in less populated areas of Himachal Pradesh, India.
Materials and Methods
Isolates Identification
A total of 250 clinical isolates were recovered from suspected cases of S. aureus infections, including vomiting, diarrhea, bacteremia, surgical site infections, and fever, from specimens such as pus, urine, catheter-associated infections, and blood, at the Indira Gandhi Medical College in Shimla and the Solan district hospital in Solan, Himachal Pradesh. The isolates were collected in batches over 12 months from January 2012 to December 2012. These isolates were collected as part of routine hospital procedures and transported in a tryptic soy broth medium and were processed further in the microbiology laboratory at Shoolini University, Solan, India. Only verbal consent was obtained because this study was retrospective in nature, and written consent was waived by the Ethics Committee of Shoolini University. All experiments were conducted as per the institution’s biosafety regulations act. The research was approved by the Institute Ethics Committee (IEC) of Shoolini university as communicated through letter no. SUIEC/12/03, dated March 19th, 2012 which is compliant with international ethical standards. The details of the isolates were obtained from the hospital’s electronic data record. The bacterial isolates were cultured on blood agar and mannitol salt agar and initially were identified based on colony characteristics, pigment production (golden yellow on blood agar), Gram staining, and type of hemolysis on blood agar, and various biochemical tests such as indole, methyl red/Voges-Proskauer (MR-VP), mannitol fermentation, coagulase, catalase, and oxidase tests.19 They were further confirmed using the 16S rRNA PCR and sequencing.20
MRSA Detection and Antimicrobial Susceptibility
All confirmed 250 S. aureus isolates were tested for MRSA by using the oxacillin MIC strip (Hi-media, Mumbai, India) test and MRSA detection kit where MRSA strains produced a colour change from pink to yellow with agglutination, test was performed as per the manufacturer’s instructions (Hi-media). In addition, the VRSA phenotype was detected by using the broth dilution methods, with log2 dilutions ranging from 8 to 0.016 mg/L as described previously.21 The confirmed MRSA isolates (n = 44) were tested for susceptibility against commonly used antibiotics by disc method as per Clinical and Laboratory Standards Institute (CLSI) guidelines.21 The antibiotic discs used were oxacillin (1µg), cefoxitin (30 µg), erythromycin (15µg), clindamycin (2µg), tetracycline (30µg), gentamicin (10µg), fusidic acid (30µg), mupirocin (5µg), linezolid (30µg), teicoplanin (30µg), ciprofloxacin (5µg), levofloxacin (5µg), daptomycin (50µg), trimethoprim/sulfamethoxazole (1.25/23.75µg), quinupristin-dalfopristin, dalbavancin (15 µg), and ceftaroline (30µg) (Hi-media, Mumbai, India) and dalbavancin susceptibility was performed by the broth dilution method. S. aureus ATCC 29213 was a positive control and S. aureus ATCC 25923 was used as the quality control strain. The 24-hour-old MRSA cultures were adjusted to a concentration of approximately 1–2×108 colony-forming units (CFU) per millilitre using a 5% MacFarland standard. The standardized cultures were then spread onto Muller-Hinton agar plates using a glass spreader. Plates were incubated at 37°C for 24 hrs and the zone of inhibitions was recorded. All antimicrobial susceptibility results were interpreted according to CLSI instructions.22
Isolation of Genomic DNA (gDNA)
A total of 44 MRSA was selected for molecular characterization, and genomic DNA (gDNA) was extracted from the overnight growth culture, 1.5mL of sample in nutrient broth was centrifuged at 10,000 rpm for 7min. The cell pellet was suspended in 150µL of 50mM Tris-HCl (pH8.0), 10mM EDTA, and 7% sucrose with lysozyme lysostaphin (5 mg/mL) lysostaphin (20 µg/mL) and further incubated at 37°C for 10 min. The resulting protoplast was lysed with sodium dodecyl sulfate (1.25%) for 10 min on ice and thereafter two phenol-chloroform extractions were performed. gDNA was recovered from the supernatant after centrifugation at 12,000 rpm for 5 min. The purity of eluted gDNA was assessed by reviewing OD ratios collected during routine spectrophotometry. Pure gDNA was assessed for an A260/280 of 1.8–1.9 and was stored at −20°C until further use.
Genetic Characterization
The standard PCR assay was performed to detect the presence of resistance encoding genes: mecA, vanA, and lukS-PV/lukf-PV using specific primers described earlier,23 Staphylococcal cassette chromosome mec (SCCmec) typing was performed using the primers described in Table 1. The PCR total reaction volume was 45µL which included 1µL target DNA (20 ng/µL), 4.5 µL of 10x buffer (Intron) with 1.5mM of MgCl2, 200 µM of dNTPs (1µL each), 50pmol of each primer (1µL each), and 0.5µL (1.5 units) of Taq DNA polymerase (Intron). The initial denaturation of the target DNA was carried out at 94°C for 3 minutes followed by 30 cycles of amplification. Each cycle consists of denaturation at 94°C for one minute. The annealing temperature for mecA was 55°C, for vanA was 54°C, and for lukS-PV/lukf-PV was 58°C, all for 45 seconds. After the annealing step, the extension step was carried out at 72°C for one minute. The final extension was carried out at 72°C for 5 min. The amplified product was electrophoresed in 1.8% agarose gel at a constant current of 20mA and the band pattern was visualized by ethidium bromide 0.4 μg/mL on a UV transilluminator. The purified PCR products of were sequenced commercially (Xcelaris Lab, Ahmedabad) and further all DNA sequences were compared with published sequences by the NCBI-BLAST program - https://blast.ncbi.nlm.nih.gov/Blast.cgi (last accessed, 15/05/2013).
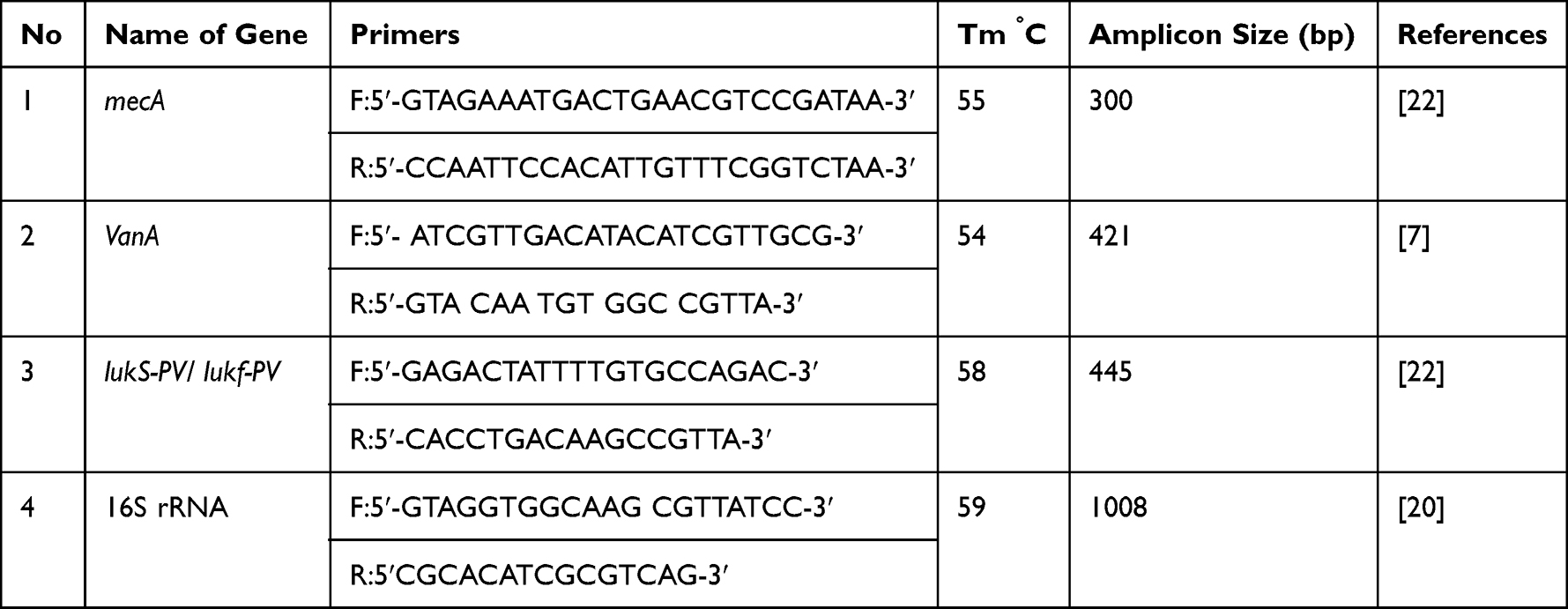 |
Table 1 Primers Used in the Present Study for the Detection of Different Genes |
Multi-Locus Sequence Typing
The 44 MRSA isolates were characterized by MLST analysis to provide a detailed picture of the epidemiology of MRSA in Himachal Pradesh. The PCR assay was carried out for MLST using previously reported primers (Supplemental File 1).24 PCR was performed at initial denaturation at 95°C for 5 min, followed by 30 cycles of annealing at 55°C, and a final extension step at 72°C for 5 min. The purified PCR products were sequenced commercially (Xcelaris Lab, Ahmedabad). The sequences were analyzed, and the ST of each isolate was assigned according to the MLST database https://pubmlst.org/organisms/staphylococcus-aureus. The associated clonal complexes (CC) were determined by the eBURST analyses (last accessed date 12/05/2013), which are used to determine cluster-related STs.
Biotyping
Bio-typing was performed according to the simplified system previously described by Devriese25 using four tests that include staphylokinase production with bovine fibrinogen (Hi-media, Mumbai, India), Hemolysis on sheep blood agar was studied, coagulation of bovine plasma for a duration of 6 hrs was performed, and crystal violet growth types on Tryptose agar (HI-media) were studied. The results were analyzed based on Devrie guidelines and biotypes (source of isolates) were assigned to each MRSA isolate.
Results
Staphylococcus aureus was isolated from four different specimens that include Pus samples 61% (n = 152), urine 17% (n = 43), Blood 14% (n = 35), and catheter-associated 8% (n = 20). Of the 250 isolates, 68%, (n = 170) were isolated from the males while 32%, (n = 80) were from females. The chi-square statistical test was X2=15.567, and P-value was 0.0013 indicating a significantly high rate of infection reported in male patients compared to females. All 250 isolates were further confirmed by 16S rRNA sequencing.
MRSA Detection and Antimicrobial Susceptibility
Of the 250 S. aureus, 17.6% (n = 44) isolates showed methicillin-resistant phenotype, which was confirmed by the MRSA detection kit (Hi-media K-058) which showed a change in colour from pink to yellow indicating a positive result, further tested by using the oxacillin MIC strip (Hi-media, Mumbai) shows 16.6% (n = 34). Antimicrobial susceptibility results of 44 MRSA isolates show the highest resistance to oxacillin, erythromycin 77.27%, (n = 34) each, followed by tetracycline 75% (n = 33), clindamycin 68.18% (n = 30), cefoxitin 65.90% (n = 29), gentamycin 61.35% (n = 27), ciprofloxacin 59.09% (n = 26), teicoplanin 36.36% (n = 16), vancomycin, levofloxacin 31.81% (n = 14). A lower resistance was observed for fusidic acid 18.11%, (n = 8) followed by Mupirocin 15.90% (n = 7), Sulfamethoxazole/trimethoprim 13.63% (n = 6), and Daptomycin 11.36% (n = 5). We found that all MRSA isolates were sensitive to linezolid, quinupristin-dalfopristin, dalbavancin, and ceftaroline. The antimicrobial susceptibility results showed multi-drug resistance phenotypes, in 54.54% (n = 24) isolates as these had resistance to at least 3 or more antibiotic classes. As a comparative analysis, no significant difference was found between the oxacillin disc (Strip) method and the MRSA kit method. Vancomycin resistance phenotype was seen in 31.81% (n=14/44) isolates that had a MIC of at least >32 ug/mL. The antimicrobial susceptibility test result was shown in heatmap format in Figure 1.
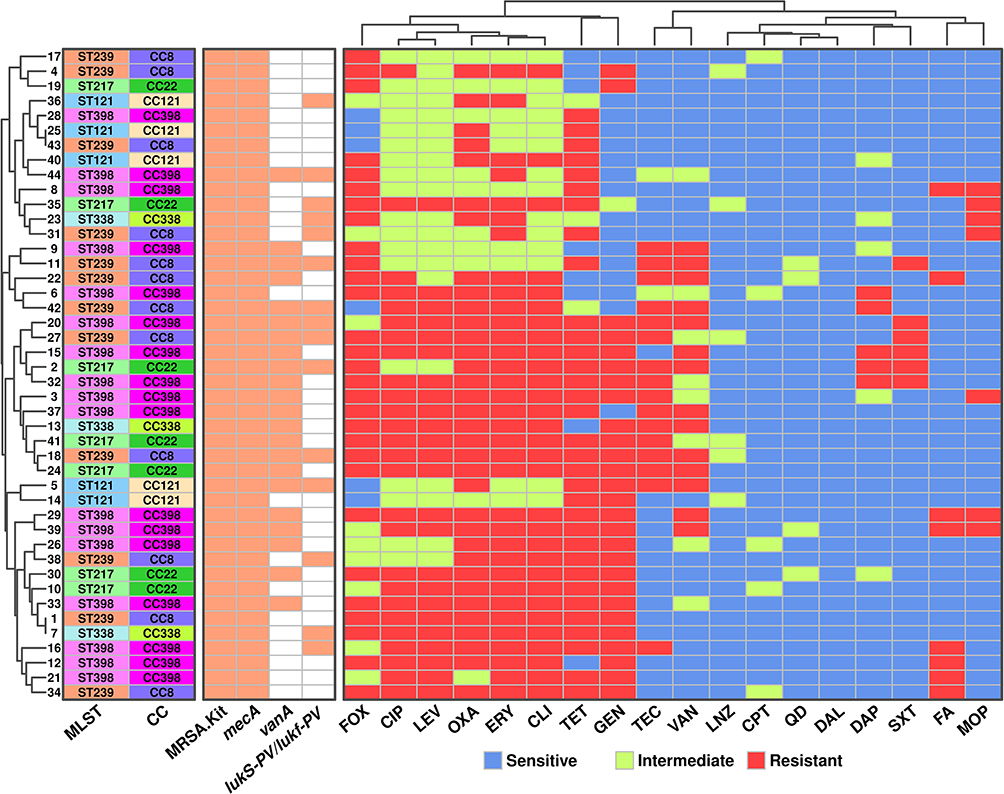 |
Figure 1 Phylogenic analysis between antimicrobial susceptibility, molecular sequences typing and resistance determinant. Abbreviations: ST, Sequence type; CC, clonal complex; OXA, oxacillin; FOX, cefoxitin; ERY, erythromycin; CLI, clindamycin; TET, tetracycline; GEN, gentamicin; FA, fusidic acid; MOP, mupirocin; LNZ, linezolid; TEC, teicoplanin; CIP, ciprofloxacin; LNZ, levofloxacin; DAP, daptomycin; SXT, trimethoprim/sulfamethoxazole; QD, quinupristin-dalfopristin; DAL, dalbavancin; CPT, ceftaroline. Note: White box indicates negative results. |
Molecular Characterization
The PCR assay results showed that all 44 isolates were positive for the presence of mecA which encodes a penicillin-binding protein (PBP2a) with low affinity to virtually all β-lactams. The staphylococcal cassette chromosome mec (SCCmec) typing results revealed that most isolates had SCCmec-II 61%, (n = 27) while SCCmec-V was seen in 30%, (n = 13) and SCCmec-IV in 9%, (n = 4) of the isolates (Figure 2). The SCCmec results revealed that CA-MRSA 59.09%, (n = 26) is more prevalent than HA-MRSA 40.90%, (n = 18) at Himachal (Figure 2). Among 44 tested MRSA 50% (n = 22) MRSA isolates harboured the vanA gene that mainly causes glycopeptide resistance. In addition, lukS-PV/lukf-PV was observed in 34% (n = 15) MRSA isolates. The co-existence of mecA, VanA and lukS-PV/lukf-PV was observed in the 18.18% (n = 8) isolates. The co-existence of the resistance determinant and resistance phenotype is represented in Figure 1.
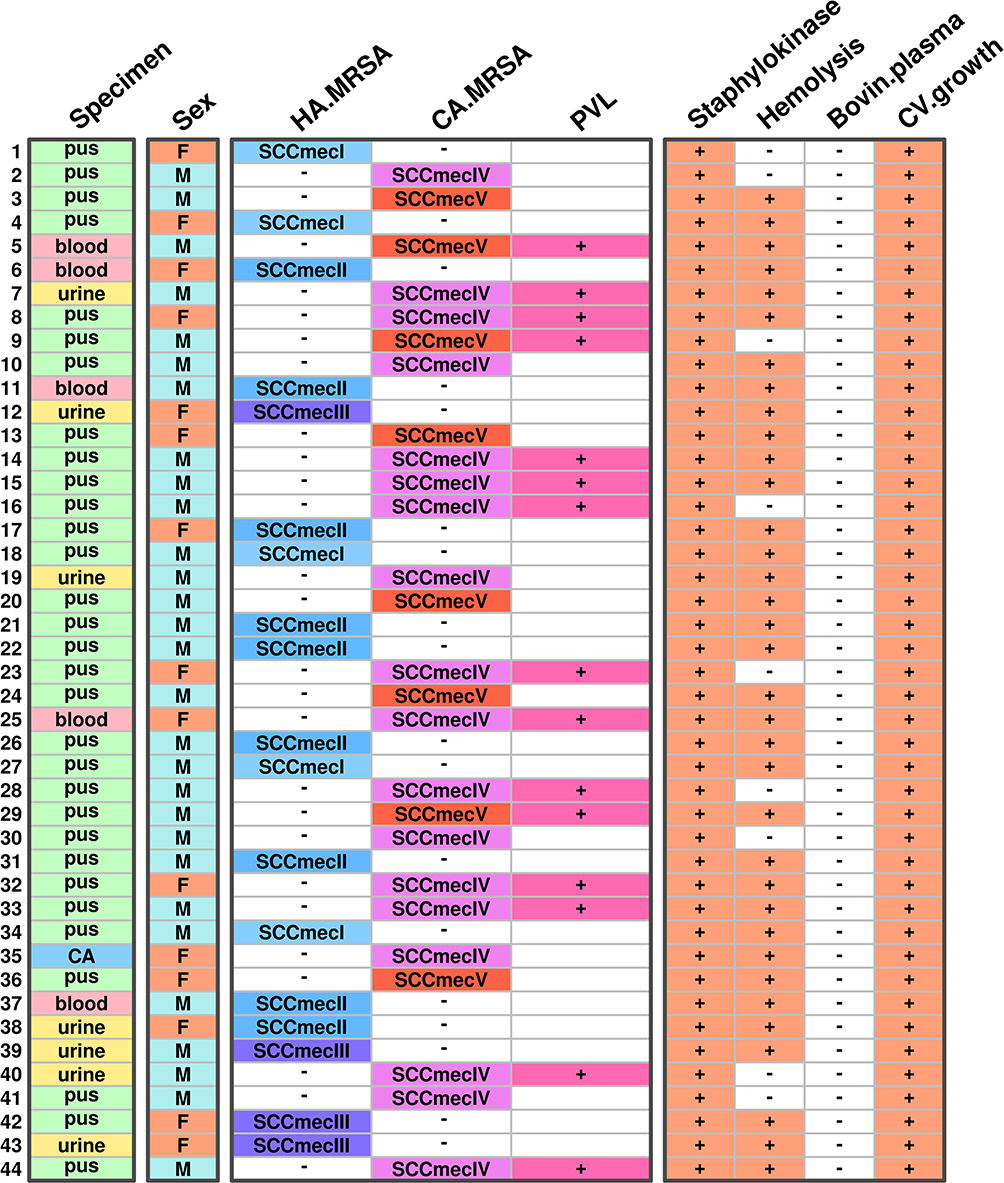 |
Figure 2 MRSA host specific, specimen and associated infection classification with PVL production. Abbreviations: F, Female; M, Male; HA.MRSA, Hospital associated methicillin resistant Staphylococcus aureus; CA.MRSA, Community associated methicillin resistant Staphylococcus aureus; PVL, Panton–Valentine leukocidin. |
Sequence Typing
A total of 5 STs were detected in the 44 MRSA isolates screened. These were dominated by ST398 39% (n = 17), followed by ST239 seen in 27% of isolates (n = 12), ST217 in 16% (n = 7), ST121 in 11% (n = 5), and ST338 (n = 3) in only 7% of the isolates. We determined the clonal complex of each ST type and also analyzed the direct relation between ST types and antimicrobial resistance. We observed type ST 398 and ST338 clones showed MDR phenotype but ST121 showed a lower resistance phenotype (Figure 1).
Host-Specific Bio-Typing
The 44 MRSA strains were investigated for bio-typing and results showed that all isolates were able to produce the staphylokinase but only 80% (n = 35) showed hemolysis on blood agar plates. Bovin plasma coagulation tests were negative for all 44 MRSA but all showed a positive result for crystal violate growth. The present results revealed that major isolates were from man host-specific 79.54% (n = 35) while a few 20.45% (n = 9) isolates were from animal-specific hosts Figure 2. Among animal-specific hosts isolates (n = 8) are associated with CA-MRSA and one isolate is associated with HA-MRSA. We have established the correlation between the bio-typing, and associate infection with PVL production represented in Figure 2.
Discussion
Methicillin-resistant S. aureus (MRSA) is a significant pathogen that has emerged over the last four decades, transmitted in both hospitals and communities, and leading cause of bacteremia, endocarditis, skin and soft tissue infections, bone and joint infections, and hospital-acquired infections.26 Genetically diverse MRSA is primarily characterized by the serial emergency of epidemic human host clones which are CC130, CC425, CC121, CC8 and CC97.27 Although prevalence has declined, attention is particularly necessary as this remains a formidable clinical threat.28 Regular surveillance with accurate detection of such MRSA strains is therefore important so that appropriate antimicrobial therapy may be given to the patients, understand the evolution for the control of the nosocomial spread and preventive measures of these strains. The results of the present study have provided insight into the distribution and types of MRSA clones ST239 and ST398 which were found in the rural area of Himachal Pradesh, India during 2012–2013. The isolates belonged to diverse genetic backgrounds with 59.09% and 40.90% of the MRSA isolates belonging to the CA-MRSA and HA-MRSA genotypes respectively. This is consistent with the global trends.29 Our study found that 18% (n=44) of 250 strains tested positive for MRSA using both the MRSA detection kit and the antibiotic disc diffusion method. In India, MRSA prevalence varies in different regions with 25% reported in West India, 50% in Central India, and 70% in South India. In South Asia, MRSA prevalence is 61% in Pakistan, 14% in Malaysia, and 40% in Hong Kong as per the respective national and regional antimicrobial surveillance reports.30–33 The strains in this study were bacteriophage typed at the National Bacteriophage Typing Center in New Delhi, and they were comparable to previous genotype studies.34 The study found a higher rate of MRSA infection in male patients compared to female patients, which is consistent with previous studies that have shown significant (p<0.001) male dominance for MRSA.35 This higher rate of MRSA in male patients is attributed to the fact that male (gender factor) patients possess more risk factors for MRSA infection. The antimicrobial susceptibility results revealed that MRSA is associated with multi-drug resistance, meaning it is resistant to many common antibiotics. The highest resistance was found for oxacillin, erythromycin, tetracycline, clindamycin, cefoxitin, gentamicin, ciprofloxacin and teicoplanin. This means these drugs may not be used for treatment but 100% susceptibility was observed for linezolid, quinupristin-dalfopristin, dalbavancin and ceftaroline. The low MICs and high susceptibility rate observed for Fusidic acid, Mupirocin, Sulfamethoxazole/trimethoprim and Daptomycin indicate hopeful antibiotic treatment for MRSA infections in the current setting. A similar susceptibility pattern was observed in human-origin isolates as well as livestock isolates and suggested that linezolid last drug of choice for MDR-MRSA.36 We have concerns regarding the co-existence of the MRSA and VRSA phenotype, which was seen in 5.6% (14 out of 250) of our cases, as it is higher than the rates seen in Europe (1.1%) and America (3.6%). To the best of our knowledge, we did not find similar data from India. However, it is in line with findings from other studies conducted in India and Ethiopia. Further investigation may be needed to determine the reasons for these differences.37,38 The mecA gene was found in all MRSA samples studied. SCCmec-II was the most common type of MRSA followed by SCCmec-V and -IV. This pattern of SCCmec-II dominance has been reported in Algeria, but not in India.39 SCCmec-II is usually associated with hospital-acquired MRSA (59.09%) while SCCmec-IV and -V are linked to community-acquired MRSA (40.90%). The SCCmec typing results suggest a mix of CA-MRSA and HA-MRSA genotypes in the hospital, indicating a shift in epidemiology with community-associated SCCmec genotypes which are now more associated with hospital infections. The virulence gene lukS-PV/lukf-PV was found in 34% (15/44) of MRSA isolates. The PVL production has been linked to CA-MRSA harbouring SCCmec type IV, V, VI, VII, and VIII epidemiologically.40 The CA-MRSA with PVL was observed at a lower rate in Japan, whereas it was higher in Colombia at 92%, Saudi Arabia at 76%, and 48% reported in overall India.39 Our study found MRSA ST239 SCCmec-II to be highly prevalent in Himachal Pradesh, similar to a report from Kolkata, India (66% of MRSA belonging to ST239).41 Our results indicate a higher proportion of MRSA ST239 SCCmec-II compared to a previous study in Korea, which reported a prevalence of 0.5%.42 ST239-SCCmec-III is the major HA-MRSA clone prevailing in various geographical regions including Asia, in contrast ST239-SCCmec-II, is rarely reported around the world.43 The high prevalence of MRSA ST239 SCCmec- II in two districts of Himachal Pradesh does not represent the entire country. Further large-scale studies and surveillance are required, as our analysis was based on only 44 MRSA isolates. Our study also found MRSA ST398 to be the second major group in Himachal Pradesh. Some studies suggest that farm animals may be the reservoir for ST398 and that it can be transmitted to humans.43 In support of these, we have observed that few ST398 clones show animal-specific hosts biotype. Our study found ST398 in Himachal Pradesh due to many people working on farms and with animals so may be transmitted from animal sources. However, the study does not suggest that companion animals play a significant role in the transmission of MRSA-ST398, as there is a lack of data on their colonization. Our results showed the majority of MRSA ST239 isolates PVL. A total of 50% of ST239 MRSA with PVL has been reported in Egypt which was from human and cow hosts.44 The diversity of human and animal strains was found to be comparable, based on their genetic background. These results suggest that the host is not the main factor influencing the diversity of this clone and that ST239-MRSA strains of the same origin may have undergone distinct evolutionary mechanisms in order to survive. The high level of diversity among these strains presents a formidable array of defense mechanisms and poses challenges to both prevention methods and therapies. It is noteworthy that the clonal diversity of MRSA has resulted in the detection of SCCmec-II in various genetic sequence types, indicating its ability to potentially transfer genetic sequences between the clones of MRSA. The origin of S. aureus strains was identified using a biotyping method, which was mostly used for food samples, but we applied it to human isolates in this study. It showed that isolates were human host-specific (59.09%) or animal (40.90). Other reports have suggested poultry-based strain transmission.45 The study has several limitations that must be taken into account when interpreting the results. The small sample size of only 250 participants and the inclusion of only two district hospitals may limit the generalizability of the findings to other populations. Additionally, the lack of diversity in the sample could further limit the generalizability of the findings. Finally, MRSA spa typing and agar typing, pulsed-field gel electrophoresis and whole genome sequence are other important to provide a comprehensive understanding of the characteristics of MRSA. Future research with larger, more representative samples is needed to confirm and extend the findings and to better understand the epidemiology, risk factors, and treatment of MRSA infection.
Conclusion
In conclusion, this is the first study that highlights the prevalence of Methicillin-resistant S. aureus (MRSA) in the rural areas of Himachal Pradesh, India, during 2012–2013. The isolates belonged to diverse genetic backgrounds, with 59.09% and 40.90% of the MRSA isolates belonging to the CA-MRSA and HA-MRSA genotypes, respectively. MRSA prevalence varies in different regions of India, with 17.6% of 250 strains tested positive for MRSA in this study. The antimicrobial susceptibility results revealed that MRSA is associated with multi-drug resistance, meaning it is resistant to many common antibiotics. The study found a higher rate of MRSA infection in male patients compared to female patients, and MRSA is associated with co-existing with the VRSA phenotype in 5.6% of the cases. The study suggests a mix of CA-MRSA and HA-MRSA genotypes in the hospital, indicating a shift in epidemiology with community-associated SCCmec genotypes that are now more associated with hospital infections. The virulence gene lukS-PV/lukf-PV was found in 34% of MRSA isolates, and MRSA ST239 SCCmec-II was highly prevalent in Himachal Pradesh, followed by MRSA ST398. Further large-scale studies and surveillance are required to better understand the prevalence and genetic diversity of MRSA in India.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and was approved by the Institutional Ethics Committee of Shoolini University, Solan with the reference number SUIEC/12/03, which adheres to international ethical standards. All experiments were conducted in compliance with the biosafety regulations of the university. As this study was retrospective in nature, written consent was waived by the Ethics Committee of Shoolini University. The study did not use any personal patient information, and all data were kept confidential and in accordance with the revised Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Shenzhen Fund for Guangdong Provincial High-Level Clinical Key Specialties (No. SZGSP012); Shenzhen Key Medical Discipline Construction Fund (No. SZXK034).
Disclosure
The authors declare no conflict of interest.
References
1. Gregory TV, Ellis K, Valeriani R, et al. MoWa: a disinfectant for hospital surfaces contaminated with methicillin-resistant Staphylococcus aureus (MRSA) and other nosocomial pathogens. Front Cell Infect Microbiol. 2021;11:676638. doi:10.3389/fcimb.2021.676638
2. Lohan K, Sangwan J, Mane P, Lathwal S. Prevalence pattern of MRSA from a rural medical college of North India: a cause of concern. J Family Med Prim Care. 2021;10:752–757. doi:10.4103/jfmpc.jfmpc_1527_20
3. Ghia CJ, Waghela S, Rambhad G. A systemic literature review and meta-analysis reporting the prevalence and impact of methicillin-resistant Staphylococcus aureus infection in India. Infect Dis. 2020;13:1178633720970569.
4. Rae N, Jarchow-MacDonald A, Nathwani D, Marwick CA. MRSA: treating people with infection. BMJ Clin Evid. 2016;2016:0922.
5. Van Belkum A, Tassios PT, Dijkshoorn L, et al. Guidelines for the validation and application of typing methods for use in bacterial epidemiology. Clin Microbiol Infect. 2007;13(S–3):1–46. doi:10.1111/j.1469-0691.2007.01786.x
6. Dendani Chadi Z, Dib L, Zeroual F, Benakhla A. Usefulness of molecular typing methods for epidemiological and evolutionary studies of Staphylococcus aureus isolated from bovine intramammary infections. Saudi J Biol Sci. 2022;29:103338. doi:10.1016/j.sjbs.2022.103338
7. Kashef MT, Helmy OM. Development of a multiplex polymerase chain reaction-based DNA lateral flow assay as a point-of-care diagnostic for fast and simultaneous detection of MRSA and vancomycin resistance in bacteremia. Diagnostics. 2022;12:2691. doi:10.3390/diagnostics12112691
8. Fishovitz J, Hermoso JA, Chang M, Mobashery S. Penicillin-binding protein 2a of methicillin-resistant Staphylococcus aureus. IUBMB Life. 2014;66:572–577. doi:10.1002/iub.1289
9. Bush LM. Best alternative to vancomycin for serious methicillin-resistant Staphylococcus aureus infections: let’s just say it. Clin Infect Dis. 2011;53:965–966. doi:10.1093/cid/cir528
10. Shariati A, Dadashi M, Moghadam MT, van Belkum A, Yaslianifard S, Darban-Sarokhalil D. Global prevalence and distribution of vancomycin-resistant, vancomycin-intermediate and heterogeneously vancomycin-intermediate Staphylococcus aureus clinical isolates: a systematic review and meta-analysis. Sci Rep. 2020;10:12689. doi:10.1038/s41598-020-69058-z
11. McGuinness WA, Malachowa N, DeLeo FR. Vancomycin resistance in Staphylococcus aureus. Yale J Biol Med. 2017;90:269–281.
12. de Niederhäusern S, Bondi M, Messi P, et al. Vancomycin-resistance transferability from VanA enterococci to Staphylococcus aureus. Curr Microbiol. 2011;62:1363–1367. doi:10.1007/s00284-011-9868-6
13. Hu Q, Peng H, Rao X. Molecular events for promotion of vancomycin resistance in vancomycin intermediate Staphylococcus aureus. Front Microbiol. 2016;7:1601. doi:10.3389/fmicb.2016.01601
14. Fujita Y, Matsudera S, Watanabe S, et al. Extensive subcutaneous abscess due to panton-valentine leucocidin-positive community-associated methicillin-resistant Staphylococcus aureus in an infant. Tohoku J Exp Med. 2022;258:303–307. doi:10.1620/tjem.2022.J086
15. Fanelli F, Chieffi D, Cho GS, et al. First genome-based characterisation and Staphylococcal enterotoxin production ability of methicillin-susceptible and methicillin-resistant Staphylococcus aureus strains isolated from ready-to-eat foods in Algiers (Algeria). Toxins. 2022;14:731. doi:10.3390/toxins14110731
16. Chen CJ, Huang YC. New epidemiology of Staphylococcus aureus infection in Asia. Clin Microbiol Infect. 2014;20:605–623. doi:10.1111/1469-0691.12705
17. Singhal T, Rodrigues C, Soman R, et al. Treatment of MRSA infections in India: clinical insights from a Delphi analysis. Indian J Med Microbiol. 2022;40:35–45. doi:10.1016/j.ijmmb.2021.11.005
18. Hata E, Katsuda K, Kobayashi H, Ogawa T, Endo T, Eguchi M. Characteristics and epidemiological genotyping of Staphylococcus aureus isolates from bovine mastitic milk in Hokkaido, Japan. J Vet Med Sci. 2005;68:165–170. doi:10.1292/jvms.68.165
19. Kateete DP, Kimani CN, Katabazi FA, et al. Identification of Staphylococcus aureus: dNase and Mannitol salt agar improve the efficiency of the tube coagulase test. Ann Clin Microbiol Antimicrob. 2010;9:23. doi:10.1186/1476-0711-9-23
20. Gumaa MA, Idris AB, Bilal NE, Hassan MA. First insights into molecular basis identification of 16s ribosomal RNA gene of Staphylococcus aureus isolated from Sudan. BMC Res Notes. 2021;14:240. doi:10.1186/s13104-021-05569-w
21. Hegstad K, Giske CG, Haldorsen B, et al. Performance of the EUCAST disk diffusion method, the CLSI agar screen method, and the Vitek 2 automated antimicrobial susceptibility testing system for detection of clinical isolates of Enterococci with low- and medium-level VanB-type vancomycin resistance: a multicenter study. J Clin Microbiol. 2014;52:1582–1589. doi:10.1128/JCM.03544-13
22. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing. CLSI Supplement M100.
23. Abimanyu N, Krishnan A, Murugesan S, Subramanian GK, Gurumurthy S, Krishnan P. Use of triplex PCR for rapid detection of PVL and differentiation of MRSA from methicillin resistant coagulase negative Staphylococci. J Clin Diagn Res. 2013;7:215–218. doi:10.7860/JCDR/2013/4523.2731
24. Enright MC, Day NP, Davies CE, Peacock SJ, Spratt BG. Multilocus sequence typing for characterization of methicillin-resistant and methicillin-susceptible clones of Staphylococcus aureus. J Clin Microbiol. 2000;38:1008–1015. doi:10.1128/JCM.38.3.1008-1015.2000
25. Devriese LA. A simplified system for biotyping Staphylococcus aureus strains isolated from different animal species. J Appl Bacteriol. 1984;56:215–220. doi:10.1111/j.1365-2672.1984.tb01341.x
26. Kourtis AP, Hatfield K, Baggs J, et al. Vital signs: epidemiology and recent trends in methicillin-resistant and in methicillin-susceptible Staphylococcus aureus bloodstream infections—United States. MMWR Morb Mortal Wkly Rep. 2019;68:214–219. doi:10.15585/mmwr.mm6809e1
27. Yebra G, Harling-Lee JD, Lycett S, et al. Multiclonal human origin and global expansion of an endemic bacterial pathogen of livestock. Proc Natl Acad Sci U S A. 2022;119:e2211217119. doi:10.1073/pnas.2211217119
28. Hindy JR, Quintero-Martinez JA, Lee AT, et al. Incidence trends and epidemiology of Staphylococcus aureus bacteremia: a systematic review of population-based studies. Cureus. 2022;14:e25460. doi:10.7759/cureus.25460
29. Mediavilla JR, Chen L, Mathema B, Kreiswirth BN. Global epidemiology of community-associated methicillin resistant Staphylococcus aureus (CA-MRSA). Curr Opin Microbiol. 2012;15:588–595. doi:10.1016/j.mib.2012.08.003
30. Sivaraman GK, Gupta SS, Visnuvinayagam S, et al. Prevalence of S. aureus and/or MRSA from seafood products from Indian seafood products. BMC Microbiol. 2022;22:233. doi:10.1186/s12866-022-02640-9
31. Tasneem U, Majid M, Mehmood K, et al. Co-occurrence of antibiotic resistance and virulence Genes in Methicillin-Resistant Staphylococcus aureus (MRSA) Isolates from Pakistan. Afr Health Sci. 2022;22:486–495. doi:10.4314/ahs.v22i1.57
32. Institute for Medical Research. Antibiotic Resistance Surveillance Report 12 October 2020. Kuala Lumpur, Malaysia: Institute for Medical Research; 2020.
33. Centre of Health Protection, Department of Health, The Government of Hong Kong Special Administration Region, Statistics. Available from: https://www.chp.gov.hk/en/statistics/data/10/100044/6864.html.
34. Patil S, Sharma PC. Bacteriophage typing and plasmid profiling of methicillin-resistant of Staphylococcus aureus strains isolated from human clinical cases in Himachal Pradesh. Asian J Pharm. 2013;3:866–869.
35. Humphreys H, Fitzpatick F, Harvey BJ. Gender differences in rates of carriage and bloodstream infection caused by methicillin-resistant Staphylococcus aureus: are they real, do they matter and why? Clin Infect Dis. 2015;61:1708–1714. doi:10.1093/cid/civ576
36. Matuszewska M, Murray GGR, Ba X, Wood R, Holmes MA, Weinert LA. Stable antibiotic resistance and rapid human adaptation in livestock-associated MRSA. Elife. 2022;11:e74819. doi:10.7554/eLife.74819
37. Shah S, Rampal R, Thakkar P, Poojary S, Ladi S. The prevalence and antimicrobial susceptibility pattern of gram-positive pathogens: three-year study at a Tertiary Care Hospital in Mumbai, India. J Lab Physicians. 2021;14:109–114. doi:10.1055/s-0041-1731136
38. Tefera S, Awoke T, Mekonnen D. Methicillin and vancomycin resistant Staphylococcus aureus and associated factors from surgical ward inpatients at Debre Markos Referral Hospital, Northwest Ethiopia. Infect Drug Resist. 2021;14:3053–3062. doi:10.2147/IDR.S324042
39. Aouati H, Hadjadj L, Aouati F, et al. Emergence of methicillin-resistant Staphylococcus aureus ST239/241 SCCmec-III Mercury in Eastern Algeria. Pathogens. 2021;10:1503. doi:10.3390/pathogens10111503
40. Funaki T, Yasuhara T, Kugawa S, et al. SCCmec typing of PVL-positive community-acquired Staphylococcus aureus (CA-MRSA) at a Japanese hospital. Heliyon. 2019;5:e01415. doi:10.1016/j.heliyon.2019.e01415
41. Jain S, Chowdhury R, Datta M, Chowdhury G, Mukhopadhyay AK. Characterization of the clonal profile of methicillin resistant Staphylococcus aureus isolated from patients with early post-operative orthopedic implant based infections. Ann Clin Microbiol Antimicrob. 2019;18:8. doi:10.1186/s12941-019-0307-z
42. Chong YP, Kim ES, Park SJ, et al. Accessory gene regulator (agr) dysfunction in Staphylococcus aureus bloodstream isolates from South Korean patients. Antimicrob Agents Chemother. 2013;57:1509–1512. doi:10.1128/AAC.01260-12
43. Abd El-Hamid MI, Sewid AH, Samir M, et al. Clonal Diversity and Epidemiological Characteristics of ST239-MRSA Strains. Front Cell Infect Microbiol. 2022;12:782045. doi:10.3389/fcimb.2022.782045
44. Witte W, Strommenger B, Stanek C, Cuny C. Methicillin-resistant Staphylococcus aureus ST398 in humans and animals, Central Europe. Emerg Infect Dis. 2007;13(2):255–258. doi:10.3201/eid1302.060924
45. Blaiotta G, Fusco V, von Eiff C, Villani F, Becker K. Biotyping of enterotoxigenic Staphylococcus aureus by enterotoxin gene cluster (egc) polymorphism and spa typing analyses. Appl Environ Microbiol. 2006;72:6117–6123. doi:10.1128/AEM.00773-06
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Bacterial Etiology and Antimicrobial Resistance Pattern of Pediatric Bloodstream Infections in Beijing, 2015–2019
Lyu ZY, Zhen JH, Meng QY, Zhou W, An JY, Dong F
Infection and Drug Resistance 2023, 16:6297-6308
Published Date: 25 September 2023
Hospital Air and Healthcare Personnel as Reservoirs of Drug-Resistant Bacteria in Tertiary Care Settings in Pakistan
Ahmad N, Imran MF, Ahmed RT, Suleman MM, Riaz M, Sheikh AS, Chiang MH
Infection and Drug Resistance 2026, 19:571281
Published Date: 6 March 2026