Back to Journals » Infection and Drug Resistance » Volume 19
Molecular Epidemiology and Antifungal Susceptibility of Cryptococcus neoformans: A First Report of Clinical Isolates from Shanxi Province, China
Authors Li X, Guo X, Liu M, Song Z ![]() , Kang Y, Jing Y, Zhang R
, Kang Y, Jing Y, Zhang R ![]()
Received 28 January 2026
Accepted for publication 31 March 2026
Published 11 April 2026 Volume 2026:19 594240
DOI https://doi.org/10.2147/IDR.S594240
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Xia Li,1,* Xinyu Guo,2,* Mengying Liu,2 Ziping Song,2 Yuying Kang,2 Yukai Jing,1 Ruijun Zhang2
1Department of Clinical Laboratory, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, Taiyuan, 030032, People’s Republic of China; 2Department of Dermatology, Third Hospital of Shanxi Medical University, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Taiyuan, 030032, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yukai Jing, Department of Clinical Laboratory, Third Hospital of Shanxi Medical University, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, 99# Longcheng Street, Xiaodian District, Taiyuan, 030032, People’s Republic of China, Email [email protected] Ruijun Zhang, Department of Dermatology, Third Hospital of Shanxi Medical University, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, 99# Longcheng Street, Xiaodian District, Taiyuan, 030032, People’s Republic of China, Email [email protected]
Purpose: Cryptococcus neoformans is a critical fungal pathogen, and continuous surveillance of its molecular epidemiology and antifungal susceptibility is essential for clinical management. However, relevant data from many regions of China (including Shanxi Province) remain limited. This study aimed to provide the first molecular epidemiological description and antifungal susceptibility profile of C. neoformans clinical isolates from Shanxi Province, China, and to establish crucial baseline data for this region.
Patients and Methods: A retrospective analysis was conducted on all clinical isolates of C. neoformans (n=8) collected between 2014 and 2024 from a major regional hospital in Shanxi Province, China. All the isolates were subjected to molecular typing (serotype, mating type, genotype, and sequence type) and antifungal susceptibility testing.
Results: All 8 clinical isolates were identified as C. neoformans, with 100% consistency in key genetic features: serotype A, MATα mating type, VNI genotype, and ST5 sequence type. Antifungal susceptibility testing revealed low minimum inhibitory concentrations (MICs) for five common antifungals (fluconazole, amphotericin B, 5-fluorocytosine, itraconazole, voriconazole), with all 8 isolates (100%) falling within the wild-type epidemiological cut-off values (ECVs), notably, four of the eight strains (50%) showed higher MIC values (2 μg/mL) for fluconazole compared with the remaining isolates.
Conclusion: This study provides the first baseline data on the molecular epidemiology and antifungal susceptibility of C. neoformans in Shanxi Province. The exclusive presence of the susceptible ST5 lineage is consistent with the predominant pattern reported in China. These findings underscore the importance of establishing region-specific surveillance systems to monitor potential future shifts in the molecular epidemiology or antifungal resistance of C. neoformans, thereby supporting effective clinical management of related infections.
Keywords: Cryptococcus neoformans, molecular epidemiology, antifungal susceptibility, baseline data, Shanxi Province, China
Introduction
Cryptococcosis is a life-threatening fungal infection caused by Cryptococcus neoformans and Cryptococcus gattii species1 that mainly affect the central nervous system and lungs.2 Human infections typically occur through inhalation of airborne fungal spores originating from environmental reservoirs, such as pigeon droppings and eucalyptus trees.3,4 Cryptococcal meningitis is the most common form of the disease and disproportionately affects individuals with HIV infection. It is estimated that 152,000 cases of cryptococcal meningitis linked to HIV occur each year worldwide, with nearly 112,000 deaths resulting therefrom, constituting 19% of total AIDS-related mortalities globally.5 Owing to its substantial disease burden and high mortality, C. neoformans was designated by the World Health Organization (WHO) in 2022 as a pathogen of critical priority in the WHO fungal priority pathogens list,5,6 highlighting its significance to global public health.
The taxonomy of these pathogens has been substantially refined. The C. neoformans species complex encompasses two major haploid species: C. neoformans (serotype A, molecular type VNI/VNII), formerly known as C. neoformans var. grubii, which is the primary cause of cryptococcosis worldwide and predominantly affects immunocompromised populations, and C. deneoformans (serotype D, molecular type VNIV), synonymous with C. neoformans var. neoformans, which are widely distributed but most prevalent in Europe, can infect both immunocompromised and immunocompetent hosts.7 Conversely, the Cryptococcus gattii species complex (sensu lato) comprises five primary species: C. gattii (VGI), C. deuterogattii (VGII), C. bacillisporus (VGIII), C. tetragattii (VGIV), and other unnamed species (VGV),8 which are more frequently encountered in tropical and subtropical regions and are notable for causing severe diseases in immunocompetent hosts. In addition to haploid reproduction, Cryptococcus species can undergo hybridization, further contributing to genetic diversity. These taxonomic refinements provide an essential framework for interpreting the molecular epidemiological data from different geographic regions.
To date, several molecular methods have been applied for the detection of specific genetic sequences of members of the C. neoformans/ C. gattii species complex. This has enabled precise species identification and has revealed differences in geographic distribution, epidemiology, and antifungal susceptibility among species. In 2009, the International Society for Human and Animal Mycology (ISHAM) recommended multilocus sequence typing (MLST) as the preferred method to characterizing Cryptococcus strains.9 In China, the predominant Cryptococcus group is C. neoformans, genotype VNI, serotype A and ST5, which primarily infect individuals without no underlying disease.10 Early differential diagnosis and timely therapeutic intervention are pivotal for improving patient outcome. According to the Invasive Fungal Surveillance Net (CHIF-NET), approximately 10% of the strains analyzed in China exhibit reduced susceptibility or non-wild-type phenotypes to fluconazole (FCZ).11 Although most strains remained susceptible, this trend highlights the need for continued antifungal surveillance.12
Taiyuan, the capital of Shanxi Province in northern China, has a temperate continental monsoon climate that influences the regional fungal distribution and infection patterns. However, epidemiological data on Cryptococcus infections in this region are scarce. This knowledge gap creates critical clinical and public health challenges: local clinicians lack region-specific baseline data to guide empirical antifungal therapy and targeted surveillance, and the absence of Shanxi data limits a comprehensive understanding of national Cryptococcus epidemiological trends and geographic variations in drug susceptibility. In this study, we retrospectively analyzed clinical Cryptococcus isolates from a tertiary hospital in Shanxi Province between 2014 and 2024, characterizing their molecular features and antifungal susceptibility profiles. By contextualizing these regional findings with national data, we aimed to establish foundational baseline information to support evidence-based clinical management and targeted epidemiological surveillance of cryptococcosis in northern China.
Materials and Methods
Clinical Isolates Information
The clinical isolates investigated in this study were obtained from cerebrospinal fluid (CSF) or blood cultures of patients diagnosed with Cryptococcus infections at Shanxi Bethune Hospital between 2014 and 2024. The Shanxi Bethune Hospital, established in 2011, is a provincial tertiary teaching hospital that currently functions as a major regional referral center in northern China.
Documented clinical information included age, sex, symptomatology, diagnosis, medical history (encompassing underlying disorders and exposure to poultry), prognosis, timing of specimen collection, and outcomes of routine CSF and biochemical examinations. Our inclusion criteria were as follows: (1) clinical cases with specimens from sterile anatomical sites (eg, cerebrospinal fluid and blood) and no concurrent polymicrobial infection at the same site; (2) positive results of Cryptococcus culture; (3) inclusion of only one index isolate per patient (duplicate isolates were excluded), with all strains viably preserved and successfully recovered; and (4) availability of complete clinical and microbiological data (eg, comorbidities, demographics, and clinical outcomes).
Activation and Identification
Clinical specimens (CSF or blood) were initially processed using a BacT/ALERT 3D automated microbial detection system. For primary fungal isolation, the resulting isolates were inoculated on plates containing Sabouraud Dextrose Agar (SDA; 1% peptone, 4% dextrose, and 1.5% agar) (Autobio Diagnostics, Zhengzhou, Henan, China) and incubated at 35°C for 24–72 h.13 The isolates were identified as C. neoformans using MALDI-TOF mass spectrometry.14 They were preserved in cryovials filled with Brain Heart Infusion (BHI) broth containing 20% glycerol, which served as a cryoprotective agent. To obtain axenic cultures for downstream analyses, the resuscitated colonies were aseptically transferred to SDA plates, purified using the streak plate method, and subsequently incubated at 35°C for 48 h.
DNA Extraction
Fungal DNA was extracted using the QIAamp Mini Kit (Qiagen, Düsseldorf, Germany) according to the manufacturer’s instructions, with minor modifications.15 Specifically, a fungal colony was collected from the edge of a demarcated plate using an inoculation loop, and then transferred to a sterile microcentrifuge tube. The colony was resuspended in 180 μL Buffer ATL supplemented with 10 μL lysozyme and 50 mg glass beads, vortexed for 30 min, and incubated at 37°C for 30 min to facilitate cell wall disruption. Proteinase K and lysis buffer were added in accordance with the manufacturer’s standard protocol, followed by incubation at 56°C for 30 min, and heat inactivation at 95°C for 15 min. After supplementation with additional lysis buffer, mechanical bead beating, ultrasonication, and treatment with pre-chilled (4°C) ethanol,16 the resulting mixture was loaded onto a QIAamp Mini spin column. The column was washed twice as per the manufacturer’s instructions, and genomic DNA was eluted with 200 μL of elution buffer and stored at −20°C until further use.
Cryptococcus Variant Identification
To confirm the identity of the isolated fungal strains, the internal transcribed spacer (ITS) region of the ribosomal RNA (rRNA) gene was amplified using the universal primers ITS1 and ITS4 (Table 1). The resulting amplicons were bidirectionally sequenced on a 3730XL DNA Analyzer (Applied Biosystems, Foster City, CA, USA), and the obtained sequences were aligned and compared against reference sequences of Cryptococcus strains retrieved from the NCBI nucleotide database (http://blast.ncbi.nlm.nih.gov/Blast). This comparative sequence analysis enabled accurate determination of fungal variant types.17 The methodology is detailed in the Supplementary Methods 1.
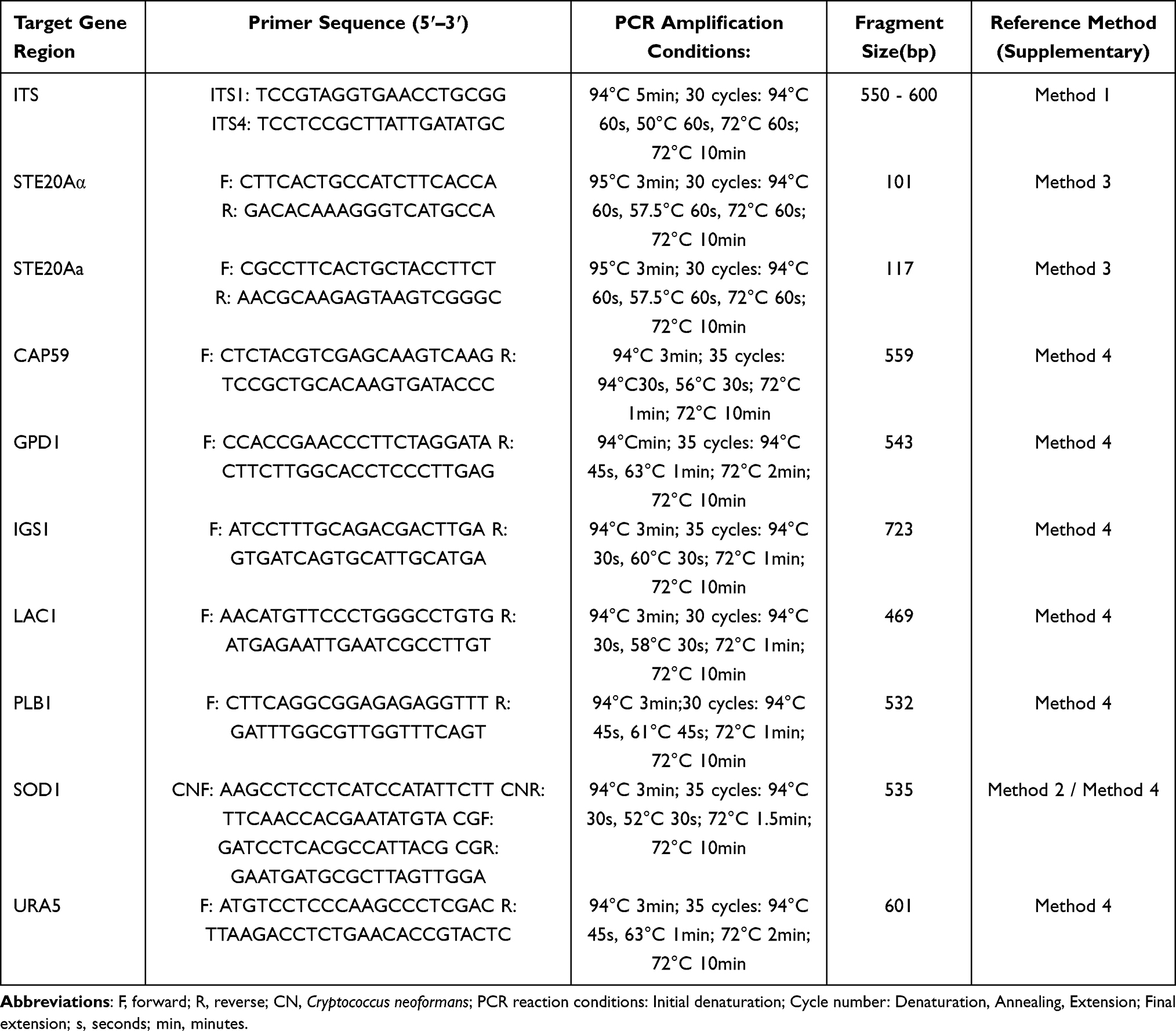 |
Table 1 Primer Information for Gene Amplification of Cryptococcus neoformans Species Used in This Study |
Cryptococcus Genotype Identification
To clarify the genotypic characteristics of the isolates, we amplified the superoxide dismutase 1 (SOD1) gene, which serves as a core molecular marker for cryptococcal genotyping.18–20 The sequences obtained were aligned with reference sequences from the following representative Cryptococcus strains: WM148 (serotype A, VNI), WM626 (serotype A, VNII), WM628 (serotype D, VNIII), WM629 (serotype AD, VNIV), WM179 (serotype B, VGI), WM178 (serotype B, VGII), WM175 (serotype B, VGIII), and WM779 (serotype C, VGIV),21 which are internationally recognized reference strains widely used in cryptococcosis research. The detailed methodology is provided in the Supplementary Methods 2.
Cryptococcus Mating Type Identification
The mating type was determined using a multiplex PCR assay with primers (Table 1) targeting the pheromone-encoding sequences within the MAT loci of Cryptococcus, where the MATα-specific target was the α-pheromone-encoding sequence in the MATα locus, and the MATa-specific target was the a-pheromone-encoding sequence in the MATa locus. These genes were specific to α and a mating types, respectively, as previously described.20,22,23 The amplified MAT locus-specific PCR products were subjected to electrophoresis on 1% agarose gels for the initial validation. Specifically, the well-characterized Cryptococcus neoformans reference strain H99 (MATα) was used as a positive control to confirm PCR specificity, whereas a no-template control (NTC) was included to rule out potential cross-contamination or reagent contamination. To further substantiate the mating-type assignments, the PCR amplicons were subjected to Sanger sequencing and the resulting sequences were aligned and compared against the H99 reference allele (GenBank accession number: AF542529.2) using the NCBI BLAST database, focusing on sequence identity and coverage to ensure reliable genotype assignment. The detailed methodology is provided in the supplementary Methods 3.
Cryptococcus MLST Identification
Seven housekeeping genes (CAP59, GDP1, LAC1, PLB1, URA5, IGS1, and SOD1) of Cryptococcus were amplified according to the ISHAM consensus MLST protocol for Cryptococcus species,21 consistent with previous studies on Chinese clinical isolates.20,24 The procedures are described in detail in Supplementary Methods 4. The sequences were submitted to the MLST online database (http://mlst.mycologylab.com) for analysis.
Phylogenetic Analysis
The sequences of seven housekeeping genes from clinical isolates and reference strains (one strain chosen per distinct sequence type and genotype archived in the MLST database) were concatenated using the BioEdit software to generate integrated sequence datasets for subsequent analyses. ClustalW was used for sequence alignment. Phylogenetic trees were constructed using MEGA 11.0, based on the neighbor-joining method with 1000 bootstrap replications.
National Comparison of Cryptococcus
A comprehensive literature review of global peer-reviewed studies published in the last 25 years was conducted, focusing on reports that detailed the number of C. neoformans isolates and confirmed their typing by MLST. The gathered data were used to generate provincial maps, illustrate strain distribution, and refine the evolutionary tree of the system.
Antifungal Susceptibility Testing
Before testing, the isolates were sub-cultured on SDA at 35 °C for 48 h to guarantee optimal growth conditions. Subsequently, the turbidity of the fungal suspensions was measured using a McClure turbidimeter to standardize the inoculum concentration in the susceptibility assay. Minimum inhibitory concentrations (MICs) of amphotericin B (AMB), 5-fluorocytosine (5FC), fluconazole (FCZ), itraconazole (ITR), and voriconazole (VCZ) were determined using the BioMérieux ATB FUNGUS 3 system. The experimental procedures, including sample preparation, reagent mixing, and signal measurement, were performed in strict accordance with the manufacturers’ protocols. After 48 h of incubation at 35°C, the strips were visually examined. Candida Krusei (ATCC6258) and Candida parapsilosis (ATCC22019) served as quality control specimens. Owing to the absence of well-established breakpoints specifically for Cryptococcus within the CLSI framework, epidemiological cutoff values (ECVs) were used to categorize the isolates as either wild-type or non-wild-type based on a comparison with the MICs. ECVs were established in CLSI document M59.25 Specifically, for C. neoformans (VNI) species, the ECVs were 0.5 µg/mL for AMB, 8 µg/mL for 5FC and FCZ, and 0.25 µg/mL for ITR and VCZ.26 Strains with MICs surpassing these thresholds were classified as non-wild type, indicating potential antifungal resistance.27
Results
Patient Characteristics
To date, fewer than 50 cases of cryptococcosis have been diagnosed at our hospital. Because patients with severe conditions were transferred to tertiary medical centers in Beijing or other provinces during the early stage of hospital establishment and because fungal cultures had already been completed for some patients before their admission to our hospital, with clinical isolates preserved at the referring institutions, a total of eight clinical isolates were retrieved from the Laboratory Department of Shanxi Bethune Hospital, Shanxi Province. Each isolate represented a unique patient, and no duplicate isolates were included. Fundamental clinical data were documented for all patients. All the isolates were identified as C. neoformans (formerly C. neoformans var. grubii). The patients were predominantly male (n=5, 62.5%) and all were middle-aged or older. Seven isolates were obtained from cerebrospinal fluid (CSF), and one isolate (specimen No. 6) was recovered from blood. The clinical diagnoses included cryptococcal meningitis simplex (CM) (n=5, 62.5%), cryptococcal pneumonia simplex (PC) (n=1, 12.5%), and multisite disseminated infection (n=2, 25%). None of the patients had a history of poultry exposure. Intracranial pressure data were not available for this cohort. Routine cerebrospinal fluid examination revealed elevated protein concentrations and decreased glucose levels in most cases, consistent with the typical laboratory findings of cryptococcal meningitis. The CSF chloride levels were generally within the normal range, which is in accordance with previous reports.28 The reference values for CSF protein, glucose, and chloride in adults are 0.15–0.45 g/L, 2.5–4.4 mmol/L, and 120–130 mmol/L, respectively. A summary of the clinical manifestations of the patients is presented in Table 2.
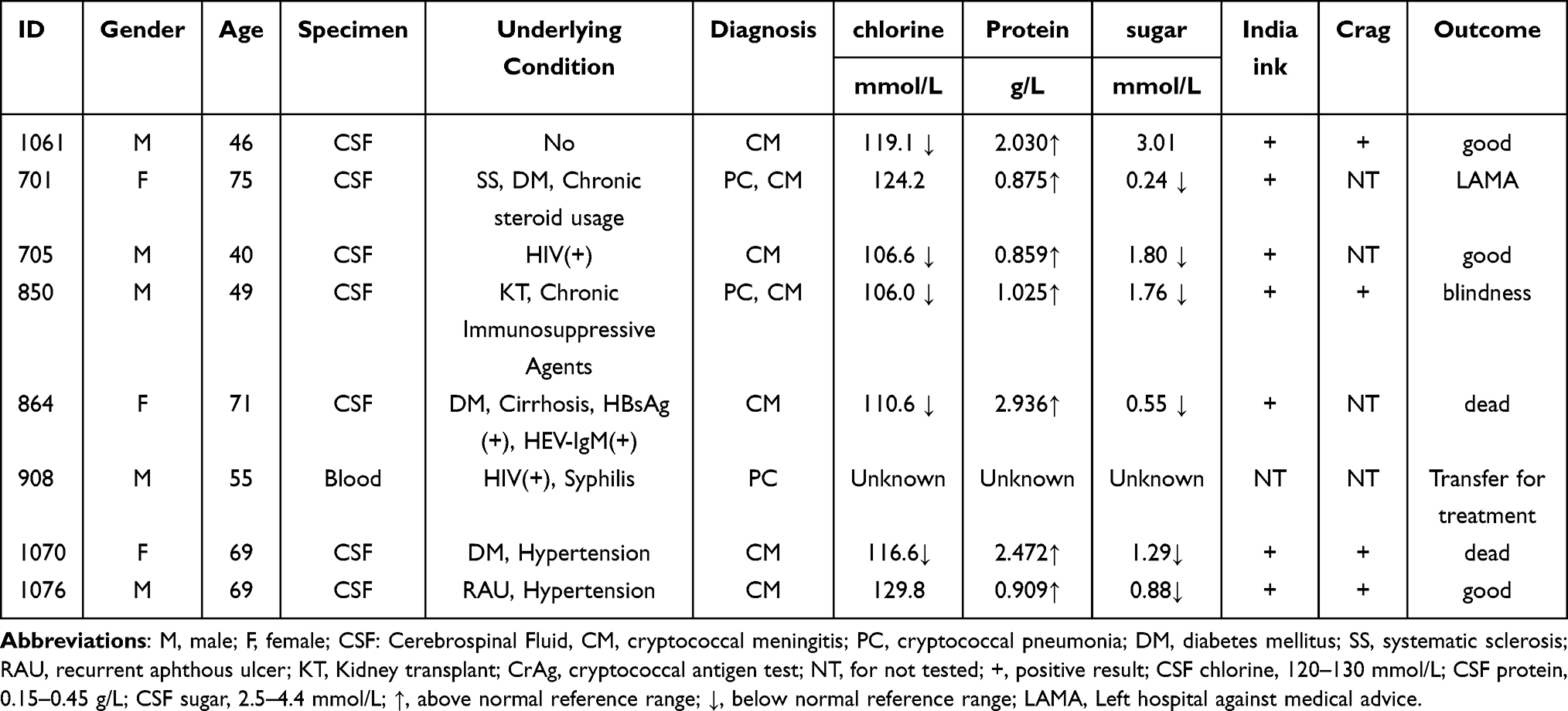 |
Table 2 Clinical Aspects of Eight Patients with Cryptococcosis |
Cryptococcus Genotypes
Multilocus sequence analysis was performed on all eight clinical isolates to determine species identity, involving amplification of the ITS region of rRNA, mating-type markers, and housekeeping genes. All isolates were identified as C. neoformans, exhibiting α-mating type (confirmed by PCR, Figure S1), VNI molecular type, and ST5 sequence type. These findings indicated a significant level of genetic uniformity across the study area. Consistent with the PCR typing results, BLAST analysis of the mating-type sequences against the reference strain H99 in the NCBI database revealed a sequence identity ranging from 94.92% to 98.33%. This high level of sequence homology further validated the accuracy and robustness of the MATα typing results. Detailed genotype data are summarized in Table 3.
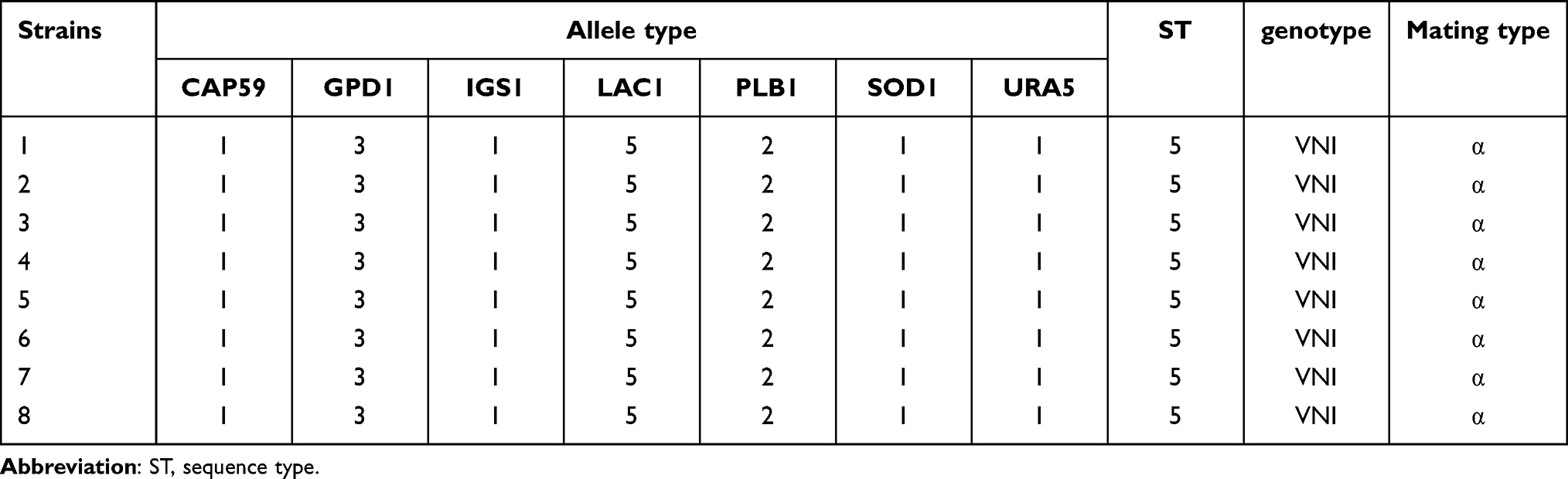 |
Table 3 Allele Type Numbers for MLST Loci and MLST Sequence Type Numbers for 8 Isolates of Cryptococcus neoformans |
Phylogenetic Tree Analysis
Phylogenetic analysis was performed using MLST data acquired in this study, along with data previously documented in China. Our findings revealed that the C. neoformans isolates from Shanxi Province belong exclusively to the ST5 lineage (Table 3). In contrast, previous studies have reported substantial genetic diversity of C. neoformans across China, with more than 40 sequence types identified to date, including ST2, ST4, ST5, ST6, ST31, ST32, ST38, ST43, ST53, ST57, ST63, ST69, ST77, ST79, ST81, ST 93, ST139, ST174, ST185, ST186, ST191, ST194, ST195, ST202, ST226, ST230, ST237, ST265, ST278, ST289, ST295, ST296, ST297, ST298, ST319, ST324, ST337, ST359, ST360, ST534, ST535, ST536, ST537, ST538, ST539, ST653, ST656, ST657, and ST658 (Figure 1).9,14,18,20,26,28–33 Despite this diversity, ST5 remains the dominant clinical lineage in most regions of China (Table 4). This distribution is similar to that observed in Hong Kong, Korea, and Japan, and no significant differences were noted across different immunized populations.34–36 The results of the phylogenetic tree analysis (Figure 1) demonstrated that the VNI genotype occupied the primary branches of the evolutionary tree, exhibiting rich diversity of sequence types. These strains formed tightly clustered groups within the tree, confirming that VNI was the predominant molecular type of C. neoformans in China. Among these, 8 strains of C. neoformans from Shanxi Province clustered with multiple ST types in China, and all (100%) clustered with the VNIc subcluster.
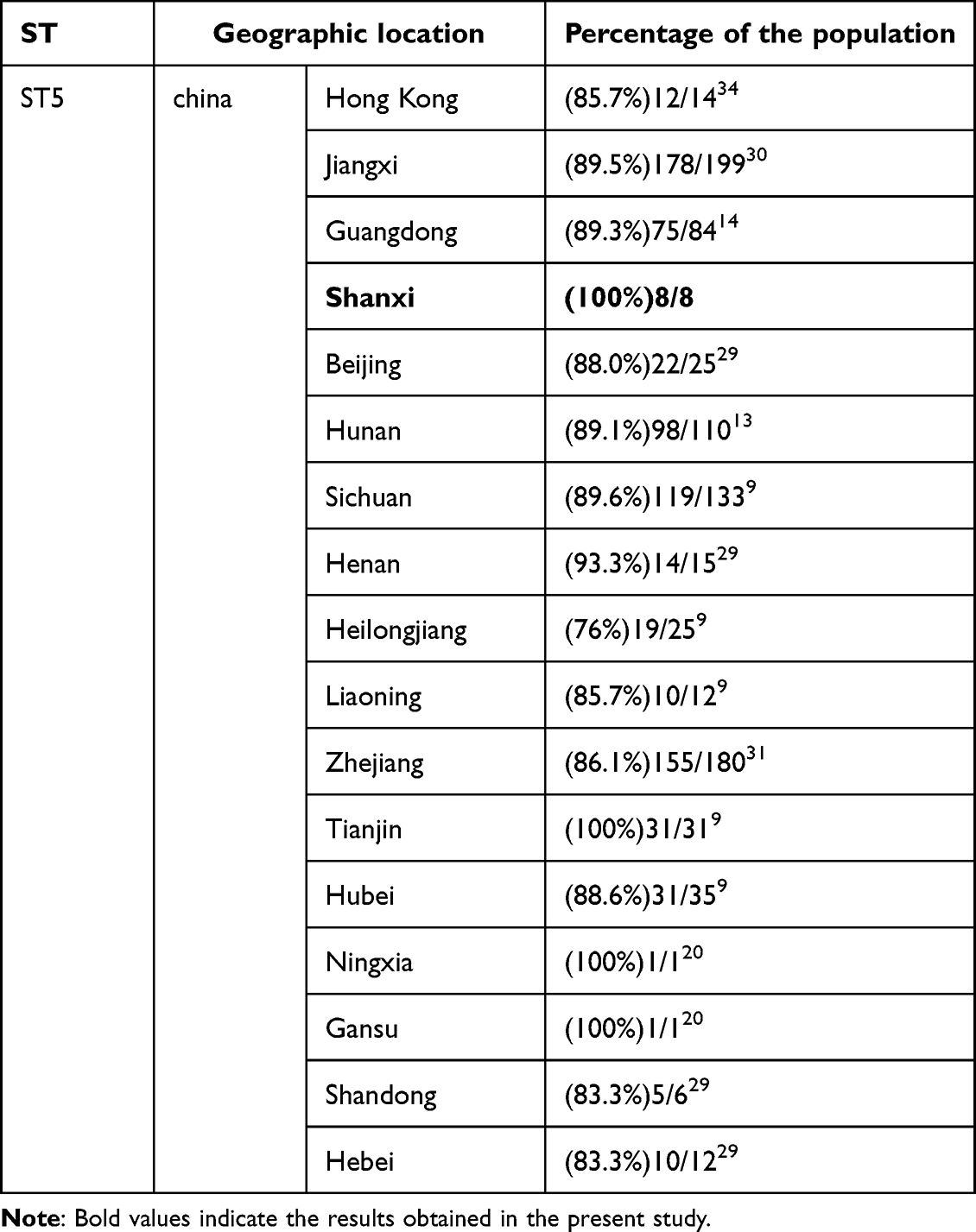 |
Table 4 Summary Distributions of Sequence Types Identified in Shanxi Province in Other Parts of China |
 |
Figure 1 Phylogenetic tree of ST types reported nationwide and strains found in this study. The black triangles represent standard strains of C. neoformans, red circles represent strains found in Shanxi Province, and the remainder represent strains already reported in China. Standard strains refer to well-characterized, internationally recognized reference strains with confirmed sequence types (STs), which were included as controls to validate the accuracy of the phylogenetic analysis. |
National Epidemiology of C. neoformans in China
An analysis of reported C. neoformans cases in China over the past 25 years has revealed significant geographical disparities. As shown in Figure 2, the incidence of infection was substantially higher in the southern provinces than in the northern regions and was similarly higher in the coastal areas than in the inland areas.
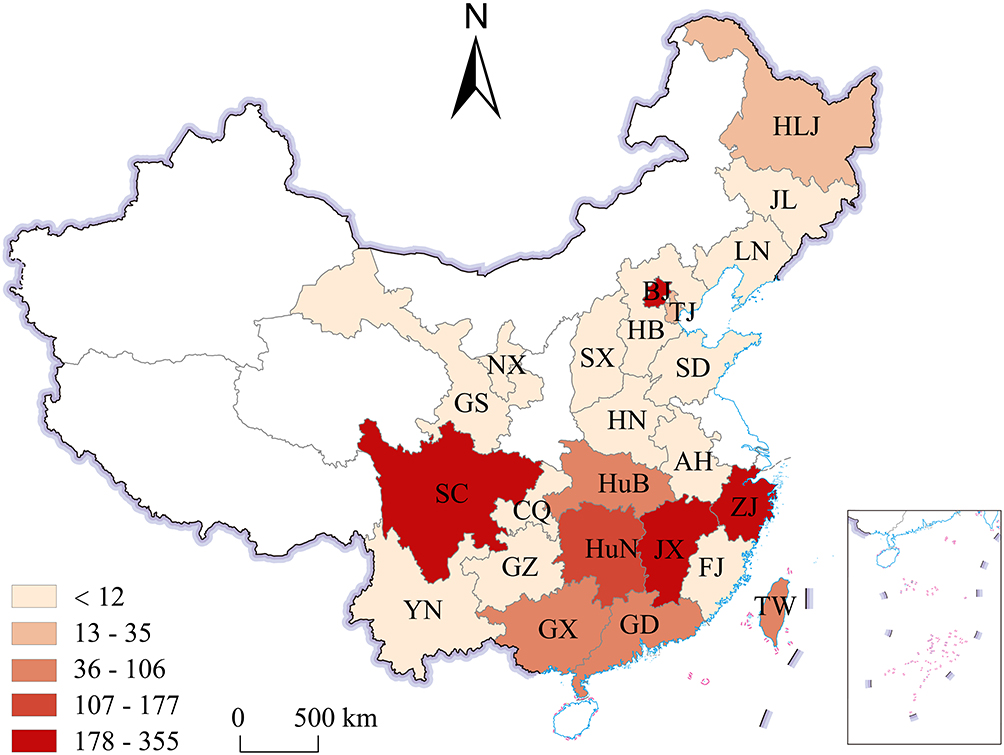 |
Figure 2 Geographic distribution of reported Cryptococcus neoformans clinical isolates in China (2000–2024).Geographic distribution of documented Cryptococcus neoformans clinical isolates in China. Number and geographic distribution of the documented clinical isolates of Cryptococcus neoformans in China since 2000. Scale key: The colored gradient indicates the number of Cryptococcus neoformans clinical isolates per provincial administrative region, with numerical ranges corresponding to isolate counts as follows: <12 isolates, 13–35 isolates, 36–106 isolates, 107–177 isolates, 178–355 isolates. Abbreviations on the map correspond to the following provinces/regions (isolate count in parentheses): SX(Shanxi):8, GD(Guangdong):93, SC(Sichuan):355, HLJ(Heilongjiang):27, LN(Liaoning):19, TJ(Tianjin):34, BJ(Beijing):232, HuB(Hubei):41, TW(Taiwan):99, JX(Jiangxi):318, ZJ(Zhejiang):182, GX(Guangxi):92, HuN(Hunan):108, HN(Henan):12, HB(Hebei):12, FJ(Fujian):3, SD(Shandong):4, AH(Anhui):2, JL(Jilin):2, GZ(Guizhou):2, NX(Ningxia):1, GS(Gansu):1, YN(Yunnan):1, CQ(Chongqing):1. This map is based on the standard map with the map review number GS(2023)2767 from the Standard Map Service Website of the Ministry of Natural Resources, and the base map has not been modified. |
Antifungal Susceptibility Testing
The in vitro antifungal susceptibility test implemented for the eight Cryptococcus strains revealed that the range of the MIC distribution was relatively narrow. This implied that the strains within this region were susceptible to the antifungal agents 5FC, AMB, FCZ, ITR, and VCZ. Representative raw images of microdilution plates used for antifungal susceptibility testing are shown in Figure S2. All strains were categorized as wild-type, in line with ECVs derived from prior investigations. Nevertheless, strains 2, 6, 7, and 8 demonstrated relatively higher MICs for FCZ than other strains. MIC data are presented in Table 5.
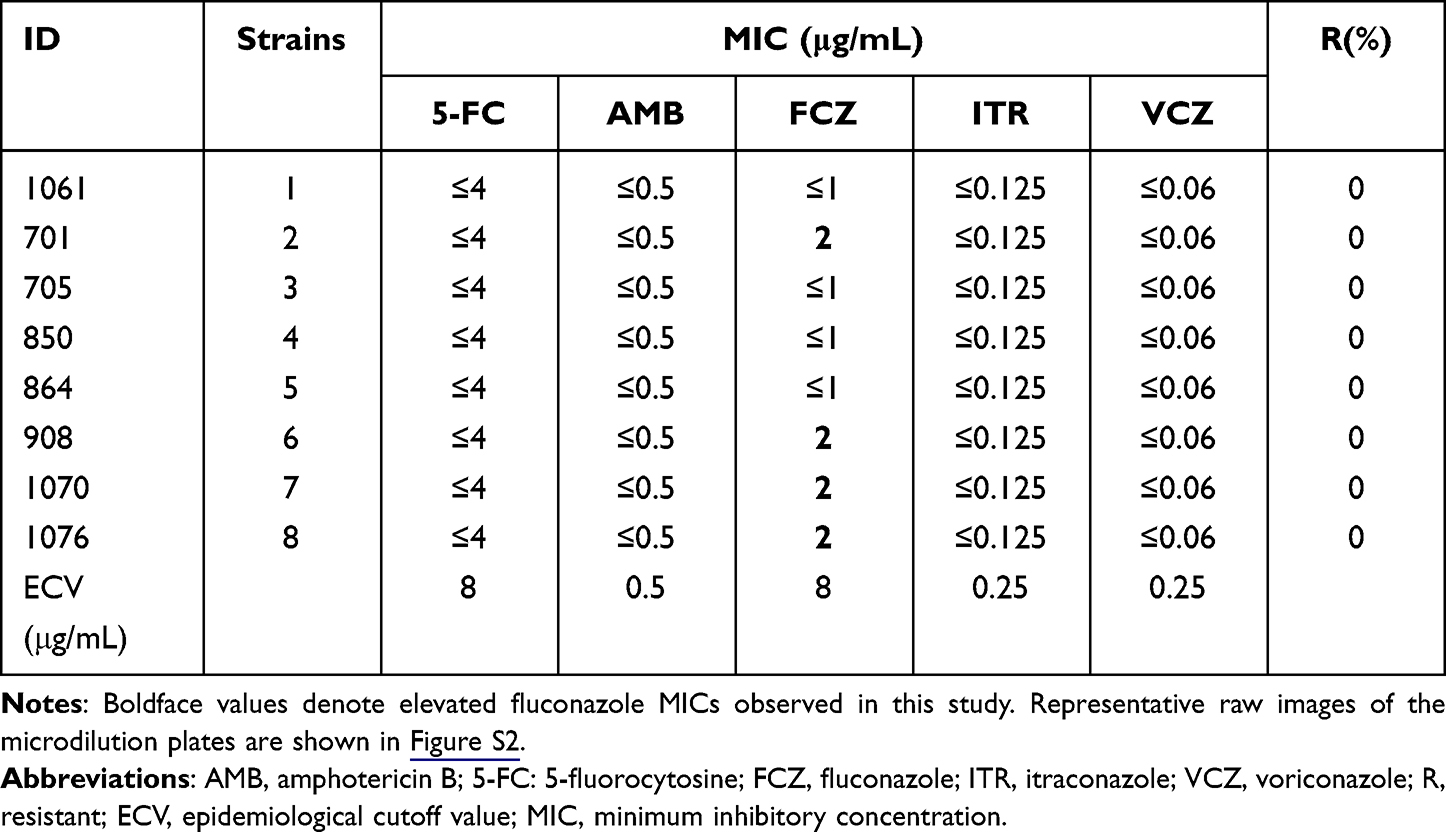 |
Table 5 Antifungal Susceptibility Data of 8 Isolates Recovered in the Study |
Discussion
This study provides the first molecular epidemiological and antifungal susceptibility profile of C. neoformans in the Shanxi Province, northern China, thereby addressing an important regional knowledge gap. Several novel findings emerged from this investigation, offering new insights into both the local and national cryptococcal epidemiology.
Predominance of the VNI/ST5 Lineage
Accurate typing of Cryptococcus is crucial to advance our understanding of this pathogen.9 A striking feature of this study was that all eight Shanxi isolates shared the same molecular profile (VNI, serotype A, MATα, and ST5) (Table 3). Notably, phylogenetic analysis of our cohort confirmed that the VNI genotype (corresponding to Cryptococcus neoformans serotype A) dominates clinical Cryptococcus isolates in China. As illustrated in Figure 1, the vast majority of the Chinese clinical isolates clustered within the VNI clade, further validating its epidemiological predominance. Based on phylogenetic analysis, all VNI genotypes in this region (n=8, 100%) clustered with the VNIc subgroup, consistent with previous reports from China,37 and no distinct internal sublineage differentiation has been identified.
Within the context of the VNI lineage, our study documented a 100% detection rate ST5 in a regional cohort. This proportion is comparable to or exceeds the ST5 rates reported in major northern Chinese medical centers. Specifically, a large multicenter study analyzing 305 clinical C. neoformans isolates via MLST reported an ST5 prevalence of 100% at the Peking University First Hospital, 95.7% at the Peking Union Medical College Hospital, and 100% at the Tianjin Medical University General Hospital. Notably, these ST5 prevalence rates in northern regions (including Shanxi) were significantly higher than those observed in southern Chinese regions included in the same multicenter investigation.5,9,28,29 The highly concentrated genotype distribution observed in Shanxi may reflect a regional clonal structure that is potentially influenced by local ecological conditions or founder effects, although this interpretation remains speculative and is constrained by the limited sample size. Comparable trends have been observed in other East Asian countries, including South Korea and Japan, where ST5 prevalence reached 96% and 88.6%, respectively,36,38 suggesting that the VNI/ST5 lineage may be well-adapted in East Asia.
Within the VNI/ST5 lineage, haploid MATα strains exhibited overwhelming predominance. In China, MATα strains of C. neoformans are predominant, and this mating type is closely associated with virulence. Several studies have demonstrated that these strains possess an enhanced ability to cross the blood-brain barrier and cause severe infections.14,39 A multicenter study covering six major regions in China reported that MATα accounted for 89.6% of the isolates.10 In the current study, all isolates were identified as MATα, which is consistent with the national data. However, given the limited number of isolates analyzed, the current data do not allow for meaningful assessment of regional differences in strain virulence, and further research is needed to evaluate the pathogenic potential of isolates from the Shanxi Province.40
Early Signals of Rising Fluconazole MICs
According to global guidelines for the diagnosis and Management of Cryptococcosis,41 the primary antifungal agents used to treat cryptococcal infections in China include 5-FC, AMB, FCZ, ITR, and VCZ. Among these, the combination of AMB with FCZ and 5-FC is the most cost-effective, and FCZ is administered for a prolonged duration throughout the course of cryptococcal infection treatment. Antifungal susceptibility testing showed that all isolates were susceptible to first-line antifungal agents, with MIC values remaining below established ECVs. However, four isolates exhibited elevated MICs (2 μg/mL) for fluconazole, potentially reflecting an early shift toward reduced susceptibility. This pattern parallels the trends observed in southwestern China and Taiwan, where MICs for FCZ showed a gradual upward trajectory.32,42 Similarly, national surveillance data indicate that resistance to FCZ is rising, increasing from 10.5% in 2010 to 34% in 2014.11
Although a one-dilution difference in fluconazole MICs was observed among isolates, all values remained within the wild-type range, and no statistically meaningful associations with clinical outcomes or temporal trends could be assessed owing to the limited sample size. Nevertheless, systematic surveillance is essential for detecting potential shifts in antifungal susceptibility patterns over time.
Clinical Characteristics and Potential Prognostic Disparities
Age and sex appeared to be associated with clinical outcomes in this small cohort. Consistent with national data, most patients were middle-aged or older males.43 However, a notable trend emerged: both fatal cases occurred in older females, whereas all favorable outcomes were observed in male patients, including those aged <60 years. In addition, all three female patients presented with CM. These observations suggest that sex and age may influence clinical outcomes, which is consistent with recent reports of higher mortality among older female patients.44 Consistently, elevated cerebrospinal fluid protein levels and reduced glucose concentrations were observed, whereas chloride levels generally remained within the normal range, which is consistent with previous reports.28 The limited sample size (n = 8) restricts further analysis of genotype-phenotype correlations; nevertheless, the observed clinical pattern suggests that host factors warrant further investigation in northern China.
Contrasting HIV Association and Host Risk Profiles
Although HIV infection remains the predominant risk factor for cryptococcosis globally, most cases in China occur among HIV-negative individuals. The proportion of HIV-positive cryptococcosis cases in China ranges from 12.9% to 24.7%,45 significantly lower than that in Europe (80%), America (86%), and Africa (69%).46–48 In this study, two of eight patients (25%) tested positive for HIV, and these two patients were diagnosed with CM and PC, respectively. The eight patients, seven of whom were diagnosed with CM, and the majority of these cases were identified in negative. Consistent with previous studies in China, an extremely high proportion (approximately 85%) of CM cases were identified in HIV-negative patients.49 This situation contrasts with those observed in other countries. A plausible explanation for this discrepancy lies in the severe under-reporting of CM cases in China’s HIV-infected population, as previously speculated.49 Differences in reported HIV associations across regions may partially reflect variations in hospital-admission patterns and study settings. Most HIV-negative patients in this cohort had other recognized risk factors, including diabetes and renal transplantation. Only one HIV-negative patient had no identifiable immunosuppressive condition, which is a lower proportion than that reported in earlier Chinese studies.10 These findings highlight the heterogeneity of the risk profiles among HIV-negative patients and the importance of broad clinical vigilance.
Implications for Transmission
Our 25-year synthesis of national molecular epidemiological data confirmed that the incidence of C. neoformans is higher in southern China than in northern China, and in coastal regions than in inland regions (Figure 2). This distribution is likely driven by multiple factors. The warm, humid subtropical and tropical climates in these areas provide favorable conditions for environmental survival and propagation of C. neoformans. They remain widely distributed in soil, decayed wood, and pigeon excreta.50 Although none of the patients reported bird exposure, the infection likely resulted from environmental inhalation of fungal spores.51 Molecular epidemiological studies have demonstrated considerable genotypic diversity among environmental isolates, with numerous novel genotypes identified in pigeon droppings.52 These genotypic disparities likely reflect the adaptive evolution of organisms across the ecological niches. Environmental studies in northern China have indicated that ST31 frequently dominates environmental niches, whereas ST5 predominates clinical isolates,53 potentially reflecting host-selective adaptation. The intrinsic differences between ST5 and ST31, including variations in virulence and host susceptibility, may contribute to their distinct clinical and environmental distribution.
Limitations
This study has several limitations. First, the absence of environmental sampling precluded the identification of the ecological factors underlying the observed ST5 homogeneity. Second, the small sample size limited genotype–phenotype analyses and prevented further investigation of ecological or epidemiological factors associated with the predominance of the ST5 lineage in this region. Third, incomplete intracranial pressure data and the lack of immunological markers, such as anti-GM-CSF antibody testing,28,54,55 constrained the exploration of host-pathogen interactions.
Future Directions and Conclusion
Given the predominance of ST5 in Shanxi and its potential implications for antifungal resistance, future studies should prioritize establishing a China-wide MLST network. This would enable the establishment of a correlation between genotype distribution (eg, ST5 prevalence in Shanxi vs. southern provinces) and antifungal resistance trends, ultimately supporting the development of region-specific strategies for cryptococcosis management.
Conclusion
This study established the first baseline data on the molecular epidemiology and antifungal susceptibility of C. neoformans in Shanxi Province. The exclusive presence of the susceptible ST5 lineage is consistent with the predominant pattern reported in China. These findings carry several clinical implications. First, the occurrence of C. neoformans infection in immunocompetent individuals highlights that cryptococcosis should not be overlooked in patients without classical risk factors. Second, the predominance of ST5 and the generally low MIC values to antifungal agents support the continued use of standard antifungal therapy in our region. However, the observation of a trend toward higher fluconazole MIC values in some isolates underscores the importance of ongoing antifungal susceptibility monitoring, particularly in refractory infections. Third, our observations suggest that delayed diagnosis may contribute to poor clinical outcomes, emphasizing the importance of early diagnostic intervention. These findings underscore the importance of establishing region-specific surveillance systems to monitor potential future shifts in the molecular epidemiology or antifungal resistance of C. neoformans, thereby supporting effective clinical management of related infections.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Shanxi Bethune Hospital (Approval Number: YXLL-2024-169). The patients’ information was anonymized before the data analysis. The Ethics Committee waived the need for written informed consent from the participants and conducted the study in accordance with the Declaration of Helsinki.
Acknowledgments
We thank Tsingke Biotechnology Co., Ltd. (Anhui, China) for their assistance with the PCR amplification and Sanger sequencing. The authors have reviewed and edited the manuscript and take full responsibility for its content.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by the Foundation Research Program of the Shanxi Province (grant number 202303021221196) and the Shanxi Provincial Committee for the Administration of Overseas Scholars.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Kwon-Chung KJ, Bennett JE, Wickes BL, et al. The case for adopting the “species complex” nomenclature for the etiologic agents of Cryptococcosis. mSphere. 2017;2(1). doi:10.1128/mSphere.00357-16
2. Litvintseva AP, Thakur R, Vilgalys R, Mitchell TG. Multilocus sequence typing reveals three genetic subpopulations of Cryptococcus neoformans var. grubii (serotype A), including a unique population in Botswana. Genetics. 2006;172(4):2223–14. doi:10.1534/genetics.105.046672
3. Botts MR, Hull CM. Dueling in the lung: how Cryptococcus spores race the host for survival. Curr Opin Microbiol. 2010;13(4):437–442. doi:10.1016/j.mib.2010.05.003
4. Kakizaki MIT, Melhem MDSC. CRYPTOCOCCOSIS: a bibliographic narrative review on antifungal resistance. Anais da Academia Brasileira de Ciencias. 2023;95(suppl 1):e20220862. doi:10.1590/0001-3765202320220862
5. Rajasingham R, Govender NP, Jordan A, et al. The global burden of HIV-associated cryptococcal infection in adults in 2020: a modelling analysis. Lancet Infect Dis. 2022;22(12):1748–1755. doi:10.1016/s1473-3099(22)00499-6
6. Casalini G, Giacomelli A, Antinori S. The WHO fungal priority pathogens list: a crucial reappraisal to review the prioritisation. Lancet Microbe. 2024;5(7):717–724. doi:10.1016/s2666-5247(24)00042-9
7. Hagen F, Khayhan K, Theelen B, et al. Recognition of seven species in the Cryptococcus gattii/Cryptococcus neoformans species complex. Fungal Genet Biol. 2015;78:16–48. doi:10.1016/j.fgb.2015.02.009
8. Montoya MC, Magwene PM, Perfect JR. Associations between Cryptococcus Genotypes, phenotypes, and clinical parameters of human disease: a review. J Fungi. 2021;7(4):260. doi:10.3390/jof7040260
9. Fan X, Xiao M, Chen S, et al. Predominance of Cryptococcus neoformans var. grubii multilocus sequence type 5 and emergence of isolates with non-wild-type minimum inhibitory concentrations to fluconazole: a multi-centre study in China. Clin Microbiol Infect. 2016;22(10):887.e1–887.e9. doi:10.1016/j.cmi.2016.07.008
10. Feng X, Yao Z, Ren D, Liao W, Wu J. Genotype and mating type analysis of Cryptococcus neoformans and Cryptococcus gattii isolates from China that mainly originated from non-HIV-infected patients. FEMS Yeast Res. 2008;8(6):930–938. doi:10.1111/j.1567-1364.2008.00422.x
11. Xiao M, Chen SC-A, Kong F, et al. Five-year China Hospital Invasive Fungal Surveillance Net (CHIF-NET) study of invasive fungal infections caused by noncandidal yeasts: species distribution and azole susceptibility. Infect Drug Resist. 2018;11:1659–1667. doi:10.2147/idr.S173805
12. Dao A, Kim HY, Garnham K, et al. Cryptococcosis-a systematic review to inform the World Health Organization Fungal Priority Pathogens List. Med Mycol. 2024;62(6). doi:10.1093/mmy/myae043
13. Li Y, Zou M, Yin J, Liu Z, Lu B. Microbiological, epidemiological, and clinical characteristics of patients with Cryptococcal Meningitis at a Tertiary Hospital in China: a 6-year retrospective analysis. Front Microbiol. 2020;11:1837. doi:10.3389/fmicb.2020.01837
14. Wang P, Li Y, Gao L, et al. In vitro characterization and molecular epidemiology of Cryptococcus spp. isolates from non-HIV patients in Guangdong, China. Front Microbiol. 2023;14:1295363. doi:10.3389/fmicb.2023.1295363
15. Kumar M, Mugunthan M. Evaluation of three DNA extraction methods from fungal cultures. Med J Armed Forces India. 2018;74(4):333–336. doi:10.1016/j.mjafi.2017.07.009
16. Griffiths LJ, Anyim M, Doffman SR, Wilks M, Millar MR, Agrawal SG. Comparison of DNA extraction methods for Aspergillus fumigatus using real-time PCR. J Med Microbiol. 2006;55(Pt 9):1187–1191. doi:10.1099/jmm.0.46510-0
17. Katsu M, Kidd S, Ando A, et al. The internal transcribed spacers and 5.8S rRNA gene show extensive diversity among isolates of the Cryptococcus neoformans species complex. FEMS Yeast Res. 2004;4(4–5):377–388. doi:10.1016/s1567-1356(03)00176-4
18. Chen Y-H, Yu F, Bian Z-Y, et al. Multilocus sequence typing reveals both shared and unique Genotypes of Cryptococcus neoformans in Jiangxi Province, China. Sci Rep. 2018;8(1):1495. doi:10.1038/s41598-018-20054-4
19. Chowdhary A, Hiremath SS, Sun S, Kowshik T, Randhawa HS, Xu J. Genetic differentiation, recombination and clonal expansion in environmental populations of Cryptococcus gattii in India. Environ Microbiol. 2011;13(7):1875–1888. doi:10.1111/j.1462-2920.2011.02510.x
20. Wu S-Y, Lei Y, Kang M, Xiao Y-L, Chen Z-X. Molecular characterisation of clinical Cryptococcus neoformans and Cryptococcus gattii isolates from Sichuan province, China. Mycoses. 2015;58(5):280–287. doi:10.1111/myc.12312
21. Meyer W, Aanensen DM, Boekhout T, et al. Consensus multi-locus sequence typing scheme for Cryptococcus neoformans and Cryptococcus gattii. Med Mycol. 2009;47(6):561–570. doi:10.1080/13693780902953886
22. Chaturvedi S, Rodeghier B, Fan J, McClelland CM, Wickes BL, Chaturvedi V. Direct PCR of Cryptococcus neoformans MATalpha and MATa pheromones to determine mating type, ploidy, and variety: a tool for epidemiological and molecular pathogenesis studies. J Clin Microbiol. 2000;38(5):2007–2009. doi:10.1128/jcm.38.5.2007-2009.2000
23. Yan Z, Li X, Xu J. Geographic distribution of mating type alleles of Cryptococcus neoformans in four areas of the United States. J Clin Microbiol. 2002;40(3):965–972. doi:10.1128/jcm.40.3.965-972.2002
24. Wang Y, Li Z, Liu Y, Ding Y, Wang Z. Molecular epidemiology and distribution of Cryptococcus neoformans in human immunodeficiency-positive patients in China. J Int Med Res. 2024;52(12):3000605241286992. doi:10.1177/03000605241286992
25. CLSI. Epidemiological Cutoff Values for Antifungal Susceptibility Testing. 2nd Ed. CLSI Supplement M59. Wayne, PA: Clinical and Laboratory Standards Institute; 2018.
26. Zhou Z, Zhu C, Ip M, et al. Molecular epidemiology and antifungal resistance of Cryptococcus neoformans from human immunodeficiency virus-negative and human immunodeficiency virus-positive patients in Eastern China. Front Microbiol. 2022;13:942940. doi:10.3389/fmicb.2022.942940
27. Bandalizadeh Z, Shokohi T, Badali H, et al. Molecular epidemiology and antifungal susceptibility profiles of clinical Cryptococcus neoformans/Cryptococcus gattii species complex. J Med Microbiol. 2020;69(1):72–81. doi:10.1099/jmm.0.001101
28. Xu X, Du P, Wang H, et al. Clinical characteristics, Cryptococcus neoformans genotypes, antifungal susceptibility, and outcomes in human immunodeficiency virus-positive patients in Beijing, China. J Int Med Res. 2021;49(5):3000605211016197. doi:10.1177/03000605211016197
29. Dou H-T, Xu Y-C, Wang H-Z, Li T-S. Molecular epidemiology of Cryptococcus neoformans and Cryptococcus gattii in China between 2007 and 2013 using multilocus sequence typing and the DiversiLab system. Eur J Clin Microbiol Infect Dis. 2015;34(4):753–762. doi:10.1007/s10096-014-2289-2
30. Yang C, Bian Z, Blechert O, et al. High prevalence of HIV-related Cryptococcosis and increased resistance to Fluconazole of the Cryptococcus neoformans complex in Jiangxi Province, South Central China. Front Cell Infect Microbiol. 2021;11:723251. doi:10.3389/fcimb.2021.723251
31. Zhang J, Wang Z, Chen Y, et al. Antifungal susceptibility and molecular characteristics of Cryptococcus spp. based on whole-genome sequencing in Zhejiang Province, China. Front Microbiol. 2022;13:991703. doi:10.3389/fmicb.2022.991703
32. Wu S-Y, Kang M, Liu Y, et al. Molecular epidemiology and antifungal susceptibilities of Cryptococcus species isolates from HIV and non-HIV patients in Southwest China. Eur J Clin Microbiol Infect Dis. 2021;40(2):287–295. doi:10.1007/s10096-020-04013-4
33. Dai -F-F, Yu Y-H, Lu -X-X. Multi-locus sequence typing-based genetic analysis, antifungal resistance, and clinical prognosis of Cryptococcus neoformans infections in HIV-infected patients in Northern China. Am JTrop Med Hyg. 2024;111(6):1184–1191. doi:10.4269/ajtmh.24-0242
34. Khayhan K, Hagen F, Pan W, et al. Geographically structured populations of Cryptococcus neoformans Variety grubii in Asia correlate with HIV status and show a clonal population structure. PLoS One. 2013;8(9):e72222. doi:10.1371/journal.pone.0072222
35. Umeyama T, Ohno H, Minamoto F, et al. Determination of epidemiology of clinically isolated Cryptococcus neoformans strains in Japan by multilocus sequence typing. Jpn J Infect Dis. 2013;66(1):51–55. doi:10.7883/yoken.66.51
36. Park SH, Choi SC, Lee KW, Kim M-N, Hwang SM. Genotypes of Clinical and Environmental Isolates of Cryptococcus neoformans and Cryptococcus gattii in Korea. Mycobiology. 2015;43(3):360–365. doi:10.5941/myco.2015.43.3.360
37. Chen J, Varma A, Diaz MR, Litvintseva AP, Wollenberg KK, Kwon-Chung KJ. Cryptococcus neoformans strains and infection in apparently immunocompetent patients, China. Emerg Infect Dis. 2008;14(5):755–762. doi:10.3201/eid1405.071312
38. Mihara T, Izumikawa K, Kakeya H, et al. Multilocus sequence typing of Cryptococcus neoformans in non-HIV associated cryptococcosis in Nagasaki, Japan. Med Mycol. 2013;51(3):252–260. doi:10.3109/13693786.2012.708883
39. Lin X, Heitman J. The biology of the Cryptococcus neoformans species complex. Ann Rev Microbiol. 2006;60:69–105. doi:10.1146/annurev.micro.60.080805.142102
40. Barchiesi F, Cogliati M, Esposto MC, et al. Comparative analysis of pathogenicity of Cryptococcus neoformans serotypes A, D and AD in murine cryptococcosis. J Infect. 2005;51(1):10–16. doi:10.1016/j.jinf.2004.07.013
41. Chang CC, Harrison TS, Bicanic TA, et al. Global guideline for the diagnosis and management of cryptococcosis: an initiative of the ECMM and ISHAM in cooperation with the ASM. Lancet Infect Dis. 2024;24(8):e495–e512. doi:10.1016/s1473-3099(23)00731-4
42. Chen Y-C, Chang T-Y, Liu J-W, et al. Increasing trend of fluconazole-non-susceptible Cryptococcus neoformans in patients with invasive cryptococcosis: a 12-year longitudinal study. BMC Infect Dis. 2015;15:277. doi:10.1186/s12879-015-1023-8
43. Guess TE, Rosen JA, McClelland EE. An overview of sex bias in C. neoformans infections. J Fungi. 2018;4(2):49. doi:10.3390/jof4020049
44. Tsai W-C, Lien C-Y, Lee -J-J, et al. The clinical characteristics and therapeutic outcomes of cryptococcal meningitis in elderly patients: a hospital-based study. BMC Geriatr. 2019;19(1):91. doi:10.1186/s12877-019-1108-0
45. Tian Y, Wang J, Shen Y, et al. Characteristics and prognostic risk factors of patients with sequence type 5 lineage-associated cryptococcosis in China. Inter J Infect Dis. 2023;128:244–253. doi:10.1016/j.ijid.2023.01.015
46. Moosa MY, Coovadia YM. Cryptococcal meningitis in Durban, South Africa: a comparison of clinical features, laboratory findings, and outcome for human immunodeficiency virus (HIV)-positive and HIV-negative patients. Clinl Infect Dis. 1997;24(2):131–134. doi:10.1093/clinids/24.2.131
47. Hajjeh RA, Conn LA, Stephens DS, et al; Cryptococcal Active Surveillance Group. Cryptococcosis: population-based multistate active surveillance and risk factors in human immunodeficiency virus-infected persons. J Infect Dis. 1999;179(2):449–454. doi:10.1086/314606
48. Dromer F, Mathoulin S, Dupont B, Laporte A; French Cryptococcosis Study Group. Epidemiology of cryptococcosis in France: a 9-year survey (1985-1993. Clinl Infect Dis. 1996;23(1):82–90. doi:10.1093/clinids/23.1.82
49. Chen M, Xu N, Xu J. Cryptococcus neoformans meningitis cases among China’s HIV-infected population may have been severely under-reported. Mycopathologia. 2020;185(6):971–974. doi:10.1007/s11046-020-00491-4
50. Ellabib MS, Aboshkiwa MA, Husien WM, D’Amicis R, Cogliati M. Isolation, Identification and Molecular Typing of Cryptococcus neoformans from Pigeon Droppings and other environmental sources in Tripoli, Libya. Mycopathologia. 2016;181(7–8):603–608. doi:10.1007/s11046-016-9996-4
51. Takahara DT, Lazéra M, Wanke B, et al. First report on Cryptococcus neoformans in pigeon excreta from public and residential locations in the metropolitan area of Cuiabá, State of Mato Grosso, Brazil. Rev Inst Med Trop Sao Paulo. 2013;55(6):371–376. doi:10.1590/s0036-46652013000600001
52. Chen M, Wang Y, Li Y, et al. Genotypic diversity and antifungal susceptibility of environmental isolates of Cryptococcus neoformans from the Yangtze River Delta region of East China. Med Mycol. 2021;59(7):653–663. doi:10.1093/mmy/myaa096
53. Dou H, Wang H, Xie S, Chen X, Xu Z, Xu Y. Molecular characterization of Cryptococcus neoformans isolated from the environment in Beijing, China. Med Mycol. 2017;55(7):737–747. doi:10.1093/mmy/myx026
54. Arango-Franco CA, Rojas J, Firacative C, et al. Autoantibodies Neutralizing GM-CSF in HIV-Negative Colombian Patients Infected with Cryptococcus gattii and C. neoformans. J Clin Immunol. 2024;44(7):163. doi:10.1007/s10875-024-01757-y
55. Saijo T, Chen J, Chen SC-A, et al. Anti-granulocyte-macrophage colony-stimulating factor autoantibodies are a risk factor for central nervous system infection by Cryptococcus gattii in otherwise immunocompetent patients. mBio. 2014;5(2):e00912–14. doi:10.1128/mBio.00912-14
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Molecular Epidemiology of Group B Streptococcus Isolates from Pregnant Women with Premature Rupture of Membranes in Fuzhou, China
Liang B, Chen H, Yu D, Zhao W, Cai X, Qiu H, Xu L
Infection and Drug Resistance 2023, 16:269-278
Published Date: 14 January 2023
Cryptococcosis in Southern China: Insights from a Six-Year Retrospective Study in Eastern Guangdong
Bilal H, Zhang D, Shafiq M, Khan MN, Chen C, Khan S, Wang Q, Cai L, Awais M, Hu H, Zeng Y
Infection and Drug Resistance 2023, 16:4409-4419
Published Date: 6 July 2023