Back to Journals » Infection and Drug Resistance » Volume 16
Cryptococcosis in Southern China: Insights from a Six-Year Retrospective Study in Eastern Guangdong
Authors Bilal H ![]() , Zhang D, Shafiq M
, Zhang D, Shafiq M ![]() , Khan MN
, Khan MN ![]() , Chen C, Khan S, Wang Q
, Chen C, Khan S, Wang Q ![]() , Cai L, Awais M, Hu H, Zeng Y
, Cai L, Awais M, Hu H, Zeng Y ![]()
Received 20 April 2023
Accepted for publication 27 June 2023
Published 6 July 2023 Volume 2023:16 Pages 4409—4419
DOI https://doi.org/10.2147/IDR.S417968
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Hazrat Bilal,1 Dongxing Zhang,2,3 Muhammad Shafiq,4 Muhammad Nadeem Khan,5 Canhua Chen,6 Sabir Khan,1 Qian Wang,1,7 Lin Cai,1 Muhammad Awais,8 Haibin Hu,9 Yuebin Zeng1,10
1Department of Dermatology, Second Affiliated Hospital of Shantou University Medical College, Shantou, 515041, People’s Republic of China; 2Department of Dermatology, Meizhou Dongshan Hospital, Meizhou, Guangdong Province, 514023, People’s Republic of China; 3Department of Dermatology, Meizhou People’s Hospital, Meizhou, Guangdong Province, 514023, People’s Republic of China; 4Department of Cell Biology and Genetics, Shantou University Medical College, Shantou, People’s Republic of China; 5Faculty of Biological Sciences, Department of Microbiology, Quaid-I-Azam University, Islamabad, 45320, Pakistan; 6Clinical Laboratory, Meizhou People’s Hospital, Meizhou, Guangdong Province, 514023, People’s Republic of China; 7Department of Medical-Surgical and Experimental Sciences University of Sassari Neurology Unit, Azienda Ospedaliera Universitaria (AOU), Sassari, Italy; 8Department of Environmental Science and Engineering, Kunming University of Science and Technology, Kunming, Yunnan, People’s Republic of China; 9The First Clinical Medical college, Guangdong Medical University, Zhanjiang, 523808, People’s Republic of China; 10Department of Dermatology, West China Second University Hospital, Sichuan University, Chengdu, Sichuan, 610021, People’s Republic of China
Correspondence: Yuebin Zeng, Tel +8618607549813, Email [email protected]
Objective: Cryptococcosis is a fatal infection that can affect both immunocompetent and immunocompromised patients, and it is little understood in China’s various regions. This research aimed to look at the epidemiology, risk factors, and antifungal susceptibility pattern of Cryptococcus neoformans in eastern Guangdong, China.
Methods: A six-year (2016– 2022) retrospective study was conducted at Meizhou People’s Hospital, China. Demographical, clinical, and laboratory data of cryptococcal patients were collected from hospital records and statistically analyzed using the chi-square and ANOVA tests.
Results: Overall, 170 cryptococcal infections were recorded, of which meningitis accounted for 78 (45.88%), cryptococcemia for 50 (29.41%), and pneumonia for 42 (24.7%). The number of cases increased 8-fold during the study duration. The median age of patients was 58 years (Inter quartile range: 47– 66), and the high proportion of cases was from the male population (n = 121, 71.17%). The underlying diseases were identified only in 60 (35.29%) patients, of which 26 (15.29%) were severely immunocompromised, and 26 (15.29%) others were mildly immunocompromised. A statistically significant difference was reported for chronic renal failure, and anemia (p < 0.05) persisted in cases of three infection types. A high number of non-wild type (NWT) isolates were found against amphotericin B (n=13/145, 8.96%), followed by itraconazole (n=7/136, 5.15%) and voriconazole (n=4/158, 2.53%). Only six isolates (3.79%) were multidrug-resistant, four of which were from cryptococcemia patients. Compared to meningitis and pneumonia, cryptococcemia revealed a higher percentage of NWT isolates (p < 0.05).
Conclusion: In high-risk populations, cryptococcal infections require ongoing monitoring and management.
Keywords: cryptococcosis, Cryptococcus neoformans, epidemiology, risk factors, antifungal susceptibility
Introduction
Cryptococcosis is a severe fungal infection caused by various encapsulated yeast species known as Cryptococcus.1 It is an opportunistic infection that frequently affects people with weakened immune systems, such as those with HIV/AIDS, solid organ or bone marrow transplant recipients, or people with other immune-compromising illnesses like malignancies and diabetes. Cryptococcus genus includes ten species, of which seven are pathogenic to animals and humans. Among these, Cryptococcus neoformans and Cryptococcus gattii are the two main species that cause cryptococcosis in humans, with C. neoformans being the most prevalent species globally.2 Meningitis, pneumonia, fungemia, endocarditis, and skin lesions are the clinical infections induced by Cryptococcus species. It is also known to cause severe morbidity and mortality worldwide.3
Every year, an estimated 223,100 new cases of cryptococcal meningitis are diagnosed worldwide, resulting in approximately 181,100 deaths.4 Similarly, the prevalence of cryptococcal infections in China is comparatively significant, and their burden varies in different geographic locations.5 Due to the lack of a proper surveillance system, the exact burden for the whole country is still to determine.6 However, some studies reported up to 43% mortality rate of C. neoformans in the Chinese population. The disease is most commonly documented in HIV-infected people, although it can also develop in non-HIV patients with other immunosuppressive conditions like organ transplants and malignancies.7,8
Antifungal agents are the cornerstone of cryptococcosis treatment. A combination of amphotericin B and 5-flucytosine is advised as a first-line treatment for patients with severe illness.9,10 Following that, fluconazole consolidation therapy is administered to finish a 10- to 12-week course of treatment.11 However, the rise of drug-resistant strains and the toxicities associated with antifungal drugs necessitate antifungal susceptibility testing.12,13 Based on their antifungal resistance mechanisms and hazardous properties, the WHO classified C. neoformans at the top of the critical fungal priority group (https://www.who.int/publications/i/item/9789240006355, accessed on 22 February 2023). The testing can help in selecting the best antifungal treatment and stop the emergence of drug resistance.12,13
The clinical traits, risk factors, and antifungal susceptibility patterns of cryptococcal infections have not been extensively studied in China.14,15 Therefore, a retrospective analysis of patients diagnosed with cryptococcosis in a Chinese hospital during the last six years would provide valuable insights into the disease’s epidemiology and management. The research could aid in identifying disease risk factors and determining antifungal susceptibility patterns of isolates. The findings could help in the development of effective strategies for the prevention and treatment of cryptococcosis in China and around the world, where it is still a significant public health issue.
Methods
This retrospective study was conducted at Meizhou People’s Hospital located in Meizhou city, eastern Guangdong, South China and included all identified cryptococcal disease cases from January 2016 to December 2022. The hospital is a tertiary (A) level hospital containing 3600 beds and providing healthcare service to around 20 million people in the region.16 The study received ethical approval from the hospital, which adhered to the standards of the Helsinki Declaration (Letter number: 2021-C-106). Hospital electronic health records were used to collect patient demographics and clinical data, including age, gender, specimen source, department location, baseline, clinical features of cryptococcal disease, HIV serology, and antifungal drug susceptibility test results.
Definition
The diagnosis of cryptococcal disease was based on World Health Organization guidelines (https://www.who.int/publications/i/item/9789240052178, accessed on 22 February 2023). This study classified cryptococcal cases based on specimen source and showed clinical features. Cryptococcal meningitis has been identified in cases where Cryptococcus neoformans has been isolated from cerebrospinal fluid (CSF) samples, and patients have experienced symptoms such as headache, fever, stiff neck, nausea, vomiting, photophobia, and confusion. The cases where C. neoformans was cultured from respiratory specimens or patients who developed symptoms such as cough, shortness of breath, fever, chest pain, and sputum production were classified as cryptococcal pneumonia. Finally, cryptococcal fungemia was classified for cases where C. neoformans was isolated from the blood, and the patients experienced symptoms such as fever, chills, headache, fatigue, and an altered mental state and did not show any symptoms of meningitis and pneumonia.1
Laboratory Isolation and Identification of Cryptococcus Species
During the study duration, 773,800 patients visited the hospital, of which 170 cases were of cryptococcosis. The species were isolated from different specimen types, like CSF, blood, tissue biopsy, BAL fluid, urine, sputum, ascites fluid, and pus. One species was counted from each patient specimen, and only the first positive culture was selected for the patients having repeated positive cultures. According to routine laboratory protocols, all the samples were first cultured on Sabouraud Dextrose Agar as selective media and then overnight enriched on Brain Heart Agar at 35 °C to identify the species of each patient sample. A single mucoid creamy colony was picked from each plate and viewed under a microscope at 400X magnification. MALDI-TOF MS (Bruker Daltonik, Bremen, Germany) was used to confirm species according to the manufacturer’s instructions. The identification process was performed using the Bruker library program Spectra (version 4.0.0.1, which contained 5627 entries) preinstalled on Bruker Biotyper (version 3.1; Bruker.1). The manufacturer’s recommended rating standards were used to determine the level of identification: Rating 2.000 or more indicated species-level identification, a score between 1700 and 1999 indicated genus-level identification, and a score below 1700 indicated that the species could not be identified.
Antifungal Susceptibility Testing
Antifungal susceptibility testing (AST) was performed using the ATB fungal 3 kit (bioMérieux SA, France) according to the manufacturer’s instructions. The tested antifungal drugs were fluconazole, itraconazole, voriconazole, 5-flucytosine, and amphotericin B. Candida parapsilosis ATCC 22019 and Candida krusei ATCC 6258 were used as quality control strains to ensure the accuracy of the results. The results were interpreted as wild type (WT) or non-wild type (NWT) based on the epidemiological cut-off values set by clinical and laboratory standards institutes guidelines for Cryptococcus species.17
Statistical Analysis
Patient demographics and clinical data were obtained from electronic medical records of the hospital surveillance system and documented in an Excel spreadsheet (2016). Qualitative data were presented as absolute numbers and relative percentages, while quantitative data were expressed as median and interquartile ranges. The characteristics of the three types of cryptococcal infections (meningitis, mycosis, and pneumonia) were analyzed using the chi-square test for categorical variables and ANOVA for continuous variables, with p-values less than 0.05 being considered statistically significant. Data analysis and visualization were done with GraphPad Prism v.8.0.2.
Results
Distribution of Cryptococcus Species
A total of 170 cryptococcal infections caused by C. neoformans were reported in the six-year study duration. The most number of cases were reported in the year 2021 (n = 56, 32.94%), followed by 2018 (n = 40, 23.53%) and 2020 (n = 17.65%), while only 7 (4.17%) cases were reported in 2016. Fluctuations in the number of cases from year to year were reported; however, an 8-fold increase occurred from 2016 to 2021. Regarding the hospital’s different departments, a large number of cases were reported from ICU (n = 67, 39.41%), followed by neurology (n = 43, 25.29%), while only 3 (1.76%) cases were reported from pediatrics and only one (0.59%) from surgery department. A total of 78 (45.88%) species were isolated from CSF, 50 (30%) from blood, and only one (0.59%) from the pus sample. The complete presentation of cases from different hospital departments and sample sources is depicted in Figure 1.
 |
Figure 1 The number of cryptococcal cases detected from different departments and sample sources during the study duration (2016 to 2021). *Other departments represent 4 cases in hepatology, 3 cases (each) from pediatrics and general practice departments, and 1 case (each) from surgery, hematology, stomatology, and cardiology. |
Demographic and Clinical Characteristics
Out of 170 cases, the total number of male cases was comparatively higher than female cases at the ratio of 121:49. Most of the cases occurred in older populations; the median age of the study population was 58 at the range of 5 years to 91 years. Among different age groups, no cases in neonatal and infants were detected, while only 9 cases (5.29%) were detected in children (ages: 2–17). The highest cases (n = 49, 28.82%) were detected in the senior age group of 61 to 70 years (Figure 2).
 |
Figure 2 Distribution of cryptococcal cases based on different age groups and gender during the study duration (2016 to 2021). |
Based on sample sources and clinical manifestations, three types of cryptococcal infection were identified in the study population. Among these, the highest number of cases was reported for cryptococcal meningitis (n = 78, 45.88%), followed by cryptococcal fungemia (n = 50, 29.41%) and then cryptococcal pneumonia (n = 42, 24.7%). The proportion of male cases was higher in all three cryptococcal infection types than in females. According to the X2 test comparison, there was no statistically significant difference in the distribution of the three infections by gender (p > 0.05). For cryptococcal pneumonia, a high number of cases were reported in the age group 51 to 60 (n = 15/42, 35.71%), followed by the age group 41 to 50 (n = 11/42, 26.19%). While for cryptococcal meningitis and fungemia, a high number of cases were reported in the age group 51 to 60, which are n = 25/78 (32.05%) and 15/50 (30%), respectively. The statistically significant difference in the distribution of infections for the age groups 51 to 60 and 71 to 80 was reported in the current study (p < 0.05).
Only 60 (35.29%) cases were reported having underlying diseases among the total cryptococcal cases. Of these, 12 (7.05%) patients had autoimmune disorders, of which 8 (4.7%) had systemic lupus erythematosus, and 4 (2.35%) had rheumatoid arthritis. Similarly, chronic renal failure was reported in 11 (6.47%) cases, followed by 8 (4.7%) cases each for cancer and diabetes and 7 (4.11%) cases for liver cirrhosis. None of the cryptococcosis patients was HIV positive in the current study. According to the X2 test comparing underlying status distribution in three infection types, a statistically significant difference was reported for chronic renal failure and anemia (p<0.05). Chronic renal failure was present in 10% of the patients with cryptococcal fungemia and 9.52% with cryptococcal pneumonia. Similarly, the results showed that anemia was more common in patients with cryptococcal fungemia (6%) than in patients with cryptococcal meningitis (0%) or pneumonia (0%). However, the distribution of some underlying conditions, such as autoimmune disorders, malignancy, diabetes, liver cirrhosis, cardiac diseases, and benign prostatic hyperplasia, was not statistically significant in three cryptococcal infection types (p > 0.05).
Among the clinical manifestations, the fever was found in high proportion among three types of cryptococcal infections (64–70%). However, some other manifestations were associated with specific infection types, like headache (n = 74, 94.87%), neck stiffness (n = 40, 51.28%), and altered mental status (n = 23, 29.48%) were found in high proportion in cryptococcal meningitis. Similarly, fatigue (n = 22, 44%) was associated with cryptococcal fungemia, while cough (n = 36, 85.71%) and shortness of breath (n = 23, 54.76%) were found in high numbers in cryptococcal pneumonia. The X2 test comparing the distribution of clinical manifestations in three different infection types revealed that, except fever, all others were statistically different (p < 0.05). The patient demographic data, underlying conditions, and clinical symptoms for each of the three forms of cryptococcal infections are presented in Table 1.
 |
Table 1 Demographical and Clinical Characteristics Associated with Cryptococcal Meningitis, Cryptococcal Fungemia, and Cryptococcal Pneumonia During the Six-Year Study Duration |
Antifungal Susceptibilities Profiles
Among the tested antifungal agents, a high number of NWT isolates were reported against amphotericin B (n = 13/145, 8.96%), followed by itraconazole (n = 7/136, 5.15%) and voriconazole (n = 4/158, 2.53%), while only 2 (4.11%) isolates showed resistance against fluconazole (Figure 3). In the overall tested isolates, only six (3.79%) isolates were MDR and showed resistance to two or more than two antifungal agents.
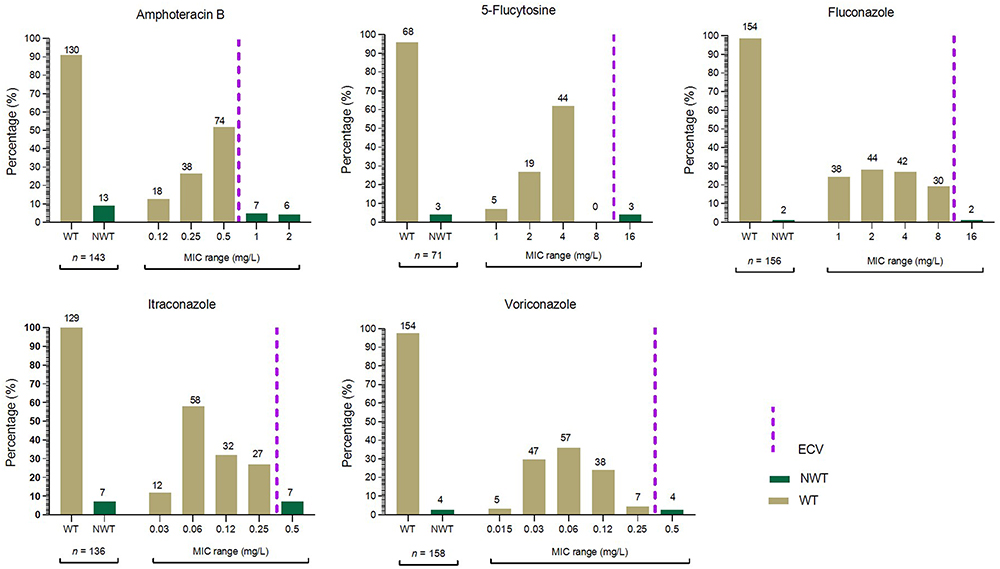 |
Figure 3 The distribution of WT/NWT and MIC ranges of different antifungal agents against the tested C. neoformans isolates tested in the current study. The brown bars indicate WT isolates, while the green bars are for NWT, and the purple line shows the ECVs for each antifungal agent according to CLSI guidelines (M57s). The ECV for amphotericin B is 0.5 mg/L, for 5-flucytosine and fluconazole is 8 mg/L, and for itraconazole, and voriconazole is 0.25 mg/L. |
Furthermore, we analyze the antifungal susceptibilities in different cryptococcal infection types (Table 2). The results showed that four of the six MDR isolates were from cryptococcal fungemia. The X2 statistic for MDR was 3.912, indicating that there may be some association between cryptococcal fungemia and the emergence of MDR isolates; however, the p-value of 0.1414 indicates that this association is not statistically significant. Moreover, the findings demonstrated that resistance to amphotericin B was associated with cryptococcal fungemia at a considerably more significant proportion (22.22%) than the other types of infection (p-value = 0.0009). Similarly, resistance to 5-flucytosine occurred at a greater rate in cryptococcal pneumonia infection (12.5%), but the association was only marginally significant (p-value = 0.041).
 |
Table 2 Antifungal Susceptibilities Profiles of C. neoformans Causing Cryptococcal Meningitis, Fungemia, and Pneumonia |
Discussion
In the current study, 170 cryptococcosis cases were reported in the past six years, of which 45.88% were meningitis, 29.41% were fungemia, and 24.7% were pneumonia. Typically, Cryptococcus is transmitted by inhalation route and causes pneumonia and fungemia, and has a proclivity to spread to the brain, where it manifests as meningitis.18 Cryptococcal meningitis is the globally predominately reported cryptococcosis followed by pneumonia and then cryptococcemia.19,20 The current study found meningitis in most in number compared to other infection types, the same as the earlier finding from China.14,21 However, the high proportion of fungemia than pneumonia is a matter of concern. As cryptococcemia is a severe threat to the immunocompromised population, early detection and treatment are critical for better outcomes.22 C. neoformans caused all cases; no C. gattii was detected in the present study. The studies showed that C. neoformans is predominantly reported worldwide and mainly infects immunosuppressed individuals, while the C. gattii is endemic to only a few regions of the world and infects immune-competent individuals.23,24
The cryptococcal infection in this study was found in high proportion in the male population compared to female, 121:49. A total of 71.7% of cases were detected from the male population, which is inconsistent with the previous findings, ie, 60.9% from Hunan, China, 75.6% from Wuhan, China, 73% from Beijing China, 79.6% from Colombia, and 69% from Brazil.14,18,25–27 The high proportion in the male population might be due to their lifestyle and weak immune system compared to the female population.19 In the present study, the median age of patients was 58 (IQR; 47–66). Specifically, for cryptococcal meningitis and fungemia, 32.05% and 30% of cases were reported in the age group 61 to 70 years, respectively. The high proportion of cases in the elderly population is similar to earlier findings from China, India, and Taiwan.14,19,28 The elderly population is more vulnerable to infections because of age-related changes in the immune system, increased risk for underlying conditions, and increased immunosuppressive medication.19 For cryptococcal pneumonia, 35.71% and 26.19% cases were reported in the age group 51 to 60 and 41 to 50, respectively. Comparatively to the other two types of infections, cryptococcal pneumonia is found in all adult age group patients.29 A previous 20-year retrospective study from China reported a mean age of 49.3 (SD: 14.3) for cryptococcal pneumonia patients.24 The occurrence of cryptococcal pneumonia in all age patients is solely related to the subject’s weakened immune systems.30
Both immunocompetent and immunocompromised persons can develop cryptococcosis.31 Patients with cryptococcal infections may have predisposing factors that vary geographically and alter over time.20,32 HIV/AIDS is considered a leading risk factor for cryptococcosis globally. However, in the current study, no cryptococcosis patients were HIV/AIDS positive. Other risk factors, like immunosuppressive therapy, advanced age, severe underlying status, solid organ transplant, hematological malignancies, prolonged corticosteroid treatment, and other immunocompromised statuses, may contribute to cryptococcosis.33 In the current study, as mentioned in Table 1, most cases are in advanced age, and severe underlying diseases are reported, which might be the reason for possible immunosuppressive statuses and the cause of cryptococcosis. Similar to our study, some previous studies reported extra-pulmonary cryptococcoses in HIV-negative patients from different world regions.34–37 Moreover, in 64.71% of patients, no apparent underlying diseases were reported. This is nearly similar to previous studies from China, in which 71% and 60% of cases showed no apparent risk factor.38,39 In the present study, 26 (15.29%) cases were severely immunocompromised (Cancer (n = 8, 4.7%), autoimmune disorder (n = 12, 7.06%), hematological malignancies (n = 6, 3.53%)) and 26 (15.29%) cases were mildly immunocompromised (chronic renal failure (n = 11, 6.47%), diabetes (n = 8, 4.7%), liver cirrhosis (n = 7, 4.11%)). The degree of immunosuppression is undetermined for the other 8 underlying statuses of patients. In previously published studies, both these severe and mildly immunosuppressive states showed an increased risk of cryptococcosis in patients.40–45
Cryptococcosis is highly fatal if not diagnosed and treated promptly. Its clinical manifestation is frequently ambiguous.27 In the current study, fever (n = 113, 66.47%) was found in high proportion, followed by headache (n = 98, 57.64%) and neck stiffness (n = 56, 32.94%), while in six cases (3.52%), chest pain and seizures were reported. Studies revealed that various cryptococcal infections showed different clinical manifestations.46 According to our data, except for the fever, all other clinical manifestations significantly varied with the type of infection. In cryptococcal meningitis, the headache was found in high proportion, followed by neck stiffness and fever, similar to the previously published report.47 Fever is a well-known clinical presentation of cryptococcemia, which is reported in our study (n = 35/50, 70%). While in cryptococcal pneumonia, the cough, shortness of breath, and chest pain were predominant clinical presentations.24
The advent of C. neoformans with resistance or high MICs exceeding ECVs is also causing concern. Antifungal susceptibility indicated species-specific differential sensitivity, although acquired resistance remained unusual.48 In the present study, six isolates were MDR, of which four were reported in cryptococcal fungemia, indicating the severity of cryptococcemia.49 The high numbers of NWT isolates were reported against amphotericin B (8.96%), similar to a previous study reported from China, in which 8.6% of isolates were NWT. However, the proportion of NWT isolates against 5-flucytosine and fluconazole in the present study is lower than the previously published literature from China.14,50 Worldwide, the estimated prevalence of 5-flucytosine NWT C. neoformans isolates is 1–2% but may exceed up to 7% in some studies, and same like in our study, the 4.11% isolates were 5-flucytosine NWT.51
Nonetheless, another study from Zhejiang, China, reported only 2% fluconazole NWT isolates, which is closer to our finding (1.29% of isolates).52 In our finding, the itraconazole and voriconazole NWT C. neoformans isolates were 5.15% and 2.53%, respectively. A rise in azole resistance among C. neoformans is pervasive worldwide. According to the ARTEMIS DISK Global Antifungal Surveillance Project, azole resistance in C. neoformans developed gradually between 1997 and 2007 from 7.3% to 11.7%.53 Significantly, azole-resistant isolates of C. neoformans were uncommon in the United Kingdom and the United States; nevertheless, isolates from Spain, Africa, Cambodia, and were reported to be becoming more resistant.54 In line with this, reports from Taiwan and Uganda for the past ten years show a rise in azole minimum inhibitory concentrations (MIC) and a decrease in azole susceptibility among C. neoformans isolates.55 The proportion of NWT isolates in the current study and published literature varies depending on several factors, such as the method used for AST determination, the study population and their underlying conditions, and the geographical distribution of C. neoformans isolates.56–58
The limitation of the current study is its retrospective design, which is based on the available records, and some variables might be missing to finalize a concrete conclusion. Furthermore, the data was collected from a single center which might vary from the other center, indicating that the results might not apply to all locations. However, the current study is the first of its kind, which will provide baseline information for future research work and guidelines for healthcare workers to manage cryptococcosis in the regions.
Conclusion
The study provides important insights into the distribution and clinical characteristics of Cryptococcus species infections over six years. The results indicate that C. neoformans was the predominant species causing cryptococcal infections, while meningitis was found in high proportion, followed by fungemia and pneumonia. A total of 8-fold increase in cryptococcosis occurred during the study duration. A high number of cases were reported in the male population and senior elderly age group, indicating their immunocompromised status and vulnerability to get infections. Underlying diseases were present in a minority of cases, with autoimmune disorders and chronic renal failure being the most common and all of the cases were HIV negative. A total of 6 MDR isolates were reported, with a high proportion of NWT isolates against amphotericin B. Overall, the isolates recovered from fungemia cases were more resistant than meningitis and pneumonia. The study highlights the need for continued surveillance and management of cryptococcal infections, especially in high-risk populations.
Data Sharing Statement
All the data are presented in the manuscript; any raw data can be available by request to first author (email: [email protected]).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of Meizhou People’s Hospital (protocol code; 2021-C-106 and date of approval; 25-12-2021).
Patient Consent Form
Patient consent was waived due to the retrospective nature of study and information was collected from the hospital record as a secondary data, and no personal image or figure of patients is included in this study.
Acknowledgments
All the authors are thankful to the Second Affiliated Hospital of Shantou University Medical College, Shantou China for supporting this work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest.
References
1. Rathore SS, Sathiyamoorthy J, Lalitha C, Ramakrishnan J. A holistic review on Cryptococcus neoformans. Microb Pathog. 2022;166:105521. doi:10.1016/j.micpath.2022.105521
2. Ashton PM, Thanh LT, Trieu PH, et al. Three phylogenetic groups have driven the recent population expansion of Cryptococcus neoformans. Nat Commun. 2019;10(1):2035. doi:10.1038/s41467-019-10092-5
3. McGuire CN, Walter DJ, Wopperer SB. Cryptococcus neoformans endocarditis in an immunocompetentpatient a case report. BMC Cardiovasc Disord. 2022;22(1):565. doi:10.1186/s12872-022-02997-9
4. Rajasingham R, Smith RM, Park BJ, et al. Global burden of disease of HIV-associated cryptococcal meningitis: an updated analysis. Lancet Infect Dis. 2017;17(8):873–881. doi:10.1016/s1473-3099(17)30243-8
5. Chen M, Xu Y, Hong N, et al. Epidemiology of fungal infections in China. Front Med. 2018;12(1):58–75. doi:10.1007/s11684-017-0601-0
6. Zhou LH, Jiang YK, Li RY, et al. Risk-based estimate of human fungal disease burden, China. Emerg Infect Dis. 2020;26(9):2137–2147. doi:10.3201/eid2609.200016
7. Liu L, Guo L, Liu Y, et al. Clinical characteristics and prognosis of pediatric cryptococcosis in Beijing Children’s Hospital, 2002–2014. Eur J Pediatr. 2017;176(9):1235–1244. doi:10.1007/s00431-017-2974-0
8. Jiang YK, Wu JQ, Zhao HZ, et al. Genetic influence of Toll-like receptors on non-HIV cryptococcal meningitis: an observational cohort study. EBioMedicine. 2018;37:401–409. doi:10.1016/j.ebiom.2018.10.045
9. Liu J, Liu J, Su X, et al. Amphotericin B plus fluorocytosine combined with voriconazole for the treatment of non-HIV and non-transplant-associated cryptococcal meningitis: a retrospective study. BMC Neurol. 2022;22(1):274. doi:10.1186/s12883-022-02803-1
10. Iyer KR, Revie NM, Fu C, Robbins N, Cowen LE. Treatment strategies for cryptococcal infection: challenges, advances and future outlook. Nat Rev Microbiol. 2021;19(7):454–466. doi:10.1038/s41579-021-00511-0
11. Molloy SF, Kanyama C, Heyderman RS, et al. Antifungal combinations for treatment of cryptococcal meningitis in Africa. N Engl J Med. 2018;378(11):1004–1017. doi:10.1056/NEJMoa1710922
12. Albehaijani SHI, Macreadie I, Morrissey CO, Boyce KJ. Molecular mechanisms underlying the emergence of polygenetic antifungal drug resistance in msh2 mismatch repair mutants of Cryptococcus. JAC Antimicrob Resist. 2022;4(2):dlac033. doi:10.1093/jacamr/dlac033
13. Hoy MJ, Park E, Lee H, et al. Structure-guided synthesis of FK506 and FK520 analogs with increased selectivity exhibit in vivo therapeutic efficacy against Cryptococcus. mBio. 2022;13(3):e0104922. doi:10.1128/mbio.01049-22
14. Li Y, Zou M, Yin J, Liu Z, Lu B. Microbiological, epidemiological, and clinical characteristics of patients with cryptococcal meningitis at a tertiary hospital in china: a 6-year retrospective analysis. Front Microbiol. 2020;11:1837. doi:10.3389/fmicb.2020.01837
15. Fang W, Fa Z, Liao W. Epidemiology of Cryptococcus and cryptococcosis in China. Fungal Genet Biol. 2015;78:7–15. doi:10.1016/j.fgb.2014.10.017
16. Bilal H, Zhang D, Shafiq M, et al. Six-year retrospective analysis of epidemiology, risk factors, and antifungal susceptibilities of candidiasis from a tertiary care hospital in South China. Microbiol Spectr. 2023:e00708–e00723. doi:10.1128/spectrum.00708-23
17. Clinical and Laboratory Standards Institute. Epidemiological cutoff values for antifungal susceptibility testing. In: CLSI Supplement M57s.
18. Cao W, Jian C, Zhang H, Xu S. Comparison of clinical features and prognostic factors of cryptococcal meningitis caused by Cryptococcus neoformans in patients with and without pulmonary nodules. Mycopathologia. 2019;184(1):73–80. doi:10.1007/s11046-018-0263-8
19. Tsai WC, Lien CY, Lee JJ, et al. The clinical characteristics and therapeutic outcomes of cryptococcal meningitis in elderly patients: a hospital-based study. BMC Geriatr. 2019;19(1):91. doi:10.1186/s12877-019-1108-0
20. O’Halloran JA, Powderly WG, Spec A. Cryptococcosis today: it is not all about HIV infection. Curr Clin Microbiol Rep. 2017;4(2):88–95. doi:10.1007/s40588-017-0064-8
21. Zhao T, Xu X, Wu Y, et al. Comparison of amphotericin B deoxycholate in combination with either flucytosine or fluconazole, and voriconazole plus flucytosine for the treatment of HIV-associated cryptococcal meningitis: a prospective multicenter study in China. BMC Infect Dis. 2022;22(1):677. doi:10.1186/s12879-022-07665-z
22. Martins-Santana L, Rezende CP, Rossi A, Martinez-Rossi NM, Almeida F. Addressing microbial resistance worldwide: challenges over controlling life-threatening fungal infections. Pathogens. 2023;12(2):293.
23. Skolnik K, Huston S, Mody CH. Cryptococcal lung infections. Clin Chest Med. 2017;38(3):451–464. doi:10.1016/j.ccm.2017.04.007
24. Hou X, Kou L, Han X, Zhu R, Song L, Liu T. Pulmonary cryptococcosis characteristics in immunocompetent patients-A 20-year clinical retrospective analysis in China. Mycoses. 2019;62(10):937–944. doi:10.1111/myc.12966
25. Gao LW, Jiao AX, Wu XR, et al. Clinical characteristics of disseminated cryptococcosis in previously healthy children in China. BMC Infect Dis. 2017;17(1):359. doi:10.1186/s12879-017-2450-5
26. Escandón P, Lizarazo J, Agudelo CI, Castañeda E. Cryptococcosis in Colombia: compilation and analysis of data from laboratory-based surveillance. J Fungi. 2018;4(1):32. doi:10.3390/jof4010032
27. Alves Soares E, Lazera MDS, Wanke B, et al. Mortality by cryptococcosis in Brazil from 2000 to 2012: a descriptive epidemiological study. PLoS Negl Trop Dis. 2019;13(7):e0007569. doi:10.1371/journal.pntd.0007569
28. Madhavan A, Sachu A, Samuel A, Vasudevapanicker J. Cryptococcal antigen prevalence in HIV patients from a tertiary care centre in South India. Iran J Microbiol. 2022;14(5):740–745. doi:10.18502/ijm.v14i5.10970
29. Thambidurai L, Prabhuradhan R, Singhvi P, Ilanchezhian S, Ramachandran R, Shankar H. Cryptococcal pneumonia: the great mimicker. BJR Case Rep. 2017;3(2):20150358. doi:10.1259/bjrcr.20150358
30. Diniz-Lima I, Fonseca L, Silva-Junior E, et al. Cryptococcus: history, epidemiology and immune evasion. Appl Sci. 2022;12(14):7086. doi:10.3390/app12147086
31. Lahiri S, Manjunath N, Bhat M, et al. Clinical insights and epidemiology of central nervous system infection due to Cryptococcus neoformans/gattii species complexes: a prospective study from South India. Med Mycol. 2020;58(5):600–608. doi:10.1093/mmy/myz097
32. Ellis J, Bangdiwala AS, Cresswell FV, et al. The changing epidemiology of HIV-associated adult meningitis, Uganda 2015–2017. Open Forum Infect Dis. 2019;6(10):ofz419. doi:10.1093/ofid/ofz419
33. Patel D, Kale P, Khillan V, Sarin SK. P406 Rise in HIV negative Cryptococcal infection in liver disease patient: epidemiology, risk factor, antifungal susceptibility profile from tertiary care hepatobiliary center. Med Mycol. 2022;60(Supplement_1):myac072P406. doi:10.1093/mmy/myac072.P406
34. Chippa VM, Chenna S, Gujarathi R, Candula N. Disseminated Cryptococcosis in an HIV-negative patient with liver cirrhosis and asplenia: a rare but dreadful disease. Cureus. 2023;15(4):e37243. doi:10.7759/cureus.37243
35. Adzic-Vukicevic T, Cevik M, Poluga J, et al. An exceptional case report of disseminated cryptococcosis in a hitherto immunocompetent patient. Rev Inst Med Trop Sao Paulo. 2020;62:e3. doi:10.1590/s1678-9946202062003
36. Xie X, Xu B, Yu C, et al. Clinical analysis of pulmonary cryptococcosis in non-HIV patients in south China. Int J Clin Exp Med. 2015;8(3):3114–3119.
37. Kohno S, Kakeya H, Izumikawa K, et al. Clinical features of pulmonary cryptococcosis in non-HIV patients in Japan. J Infect Chemother. 2015;21(1):23–30. doi:10.1016/j.jiac.2014.08.025
38. Chen J, Varma A, Diaz MR, Litvintseva AP, Wollenberg KK, Kwon-Chung KJ. Cryptococcus neoformans strains and infection in apparently immunocompetent patients, China. Emerg Infect Dis. 2008;14(5):755–762. doi:10.3201/eid1405.071312
39. Liu K, Ding H, Xu B, et al. Clinical analysis of non-AIDS patients pathologically diagnosed with pulmonary cryptococcosis. J Thorac Dis. 2016;8(10):2813–2821. doi:10.21037/jtd.2016.10.36
40. Diniz-Lima I, da Fonseca LM, Dos Reis JS, et al. Non-self glycan structures as possible modulators of cancer progression: would polysaccharides from Cryptococcus spp. impact this phenomenon? Braz J Microbiol. 2023;54(2):907–919. doi:10.1007/s42770-023-00936-0
41. Essien F, Westbrook M, Wolfley G, Patterson S, Carrol M. “When Cryptococcus strikes and lupus is found”: a unique covert unveiling of systemic lupus erythematosus presenting as subacute meningitis. Ther Adv Chronic Dis. 2022;13:20406223221102784. doi:10.1177/20406223221102784
42. Marr KA, Sun Y, Spec A, et al. A multicenter, longitudinal cohort study of cryptococcosis in human immunodeficiency virus-negative people in the United States. Clin Infect Dis. 2020;70(2):252–261. doi:10.1093/cid/ciz193
43. Dudiki N, Tigas E, Jones E. The entity of cryptosarc-cryptococcosis in sarcoid. B61 fungal infection cases. Am Thorac Soc. 2020:A3956. doi:10.1164/ajrccm-conference.2020.201.1_MeetingAbstracts.A3956
44. Nsenga L, Kajjimu J, Olum R, et al. Cryptococcosis complicating diabetes mellitus: a scoping review. Therap Adv Infect Dis. 2021;8:20499361211014769. doi:10.1177/20499361211014769
45. Zhou QH, Hu CQ, Shi Y, et al. Cryptococcosis in patients with liver cirrhosis: death risk factors and predictive value of prognostic models. Hepatobil Pancr Dis Int. 2021;20(5):460–468. doi:10.1016/j.hbpd.2021.06.006
46. Lao M, Li C, Li J, Chen D, Ding M, Gong Y. Opportunistic invasive fungal disease in patients with type 2 diabetes mellitus from Southern China: clinical features and associated factors. J Diabetes Investig. 2020;11(3):731–744. doi:10.1111/jdi.13183
47. Qu J, Lv X. Cryptococcal meningitis in apparently immunocompetent patients. Crit Rev Microbiol. 2022;1–11. doi:10.1080/1040841x.2022.2159786
48. Zhou Z, Zhu C, Ip M, et al. Molecular epidemiology and antifungal resistance of Cryptococcus neoformans from human immunodeficiency virus-negative and human immunodeficiency virus-positive patients in Eastern China. Front Microbiol. 2022;13:942940. doi:10.3389/fmicb.2022.942940
49. Chan KS, Lai CC, Yu WL, Chao CM. COVID-19 associated with cryptococcosis: a new challenge during the pandemic. J Fungi. 2022;8(10):1111. doi:10.3390/jof8101111
50. Fan X, Xiao M, Chen S, et al. Predominance of Cryptococcus neoformans var. grubii multilocus sequence type 5 and emergence of isolates with non-wild-type minimum inhibitory concentrations to fluconazole: a multi-centre study in China. Clin Microbiol Infect. 2016;22(10):
51. Bermas A, Geddes-McAlister J. Combatting the evolution of antifungal resistance in Cryptococcus neoformans. Mol Microbiol. 2020;114(5):721–734. doi:10.1111/mmi.14565
52. Fu Y, Xu M, Zhou H, Yao Y, Zhou J, Pan Z. Microbiological and clinical characteristics of cryptococcemia: a retrospective analysis of 85 cases in a Chinese hospital. Med Mycol. 2020;58(4):478–484. doi:10.1093/mmy/myz089
53. Pfaller MA, Diekema DJ, Gibbs DL, et al. Results from the ARTEMIS DISK Global Antifungal Surveillance Study, 1997 to 2007: 10.5-year analysis of susceptibilities of noncandidal yeast species to fluconazole and voriconazole determined by CLSI standardized disk diffusion testing. J Clin Microbiol. 2009;47(1):117–123. doi:10.1128/jcm.01747-08
54. Chen YC, Chang TY, Liu JW, et al. Increasing trend of fluconazole-non-susceptible Cryptococcus neoformans in patients with invasive cryptococcosis: a 12-year longitudinal study. BMC Infect Dis. 2015;15(1):277. doi:10.1186/s12879-015-1023-8
55. Smith KD, Achan B, Hullsiek KH, et al. Increased antifungal drug resistance in clinical isolates of Cryptococcus neoformans in Uganda. Antimicrob Agents Chemother. 2015;59(12):7197–7204. doi:10.1128/aac.01299-15
56. Bongomin F, Oladele RO, Gago S, Moore CB, Richardson MD. A systematic review of fluconazole resistance in clinical isolates of Cryptococcus species. Mycoses. 2018;61(5):290–297. doi:10.1111/myc.12747
57. Bilal H, Shafiq M, Hou B, et al. Distribution and antifungal susceptibility pattern of Candida species from mainland China: a systematic analysis. Virulence. 2022;13(1):1573–1589. doi:10.1080/21505594.2022.2123325
58. Bilal H, Hou B, Shafiq M, Chen X, Shahid MA, Zeng Y. Antifungal susceptibility pattern of Candida isolated from cutaneous candidiasis patients in eastern Guangdong region: a retrospective study of the past 10 years. Front Microbiol. 2022;13:981181. doi:10.3389/fmicb.2022.981181
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Scoping Review on the Status of Female Breast Cancer in Asia with a Special Focus on Nepal
Dhakal R, Noula M, Roupa Z, Yamasaki EN
Breast Cancer: Targets and Therapy 2022, 14:229-246
Published Date: 26 August 2022
Burden of Metabolic Syndrome Among a Low-Income Population in China: A Population-Based Cross-Sectional Study
Bao J, Wang L, Hu P, Liu J, Tu J, Wang J, Li J, Ning X
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2713-2723
Published Date: 3 September 2022
Clinical Features of Human Brucellosis and Risk Factors for Focal Complications: A Retrospective Analysis in a Tertiary-Care Hospital in Beijing, China
Zhang Z, Zhang X, Chen X, Cui X, Cai M, Yang L, Zhang Y
International Journal of General Medicine 2022, 15:7373-7382
Published Date: 19 September 2022
Prevalence and Associated Factors of Urinary Tract Infection in Patients with Diabetic Neuropathy: A Hospital-Based Cross-Sectional Study
Wang X, Wang Y, Luo L, Tan L, Cai W, Chen L, Ren W
Diabetes, Metabolic Syndrome and Obesity 2023, 16:1261-1270
Published Date: 3 May 2023
Prevalence, Risk Factors, and Impact on Life of Female Urinary Incontinence: An Epidemiological Survey of 9584 Women in a Region of Southeastern China
Wang Q, Que YZ, Wan XY, Lin CQ
Risk Management and Healthcare Policy 2023, 16:1477-1487
Published Date: 9 August 2023