Back to Journals » Neuropsychiatric Disease and Treatment » Volume 22
Modifying Neuropsychiatric and Motor Trajectories in Huntington’s Disease Through an Integrated Neurobehavioral Clinic Model
Authors Khan S ![]() , Velez Figueroa L
, Velez Figueroa L ![]() , Selvadurai C
, Selvadurai C ![]() , Deshpande AR, Najmivarzaneh F, Lindbergh CA
, Deshpande AR, Najmivarzaneh F, Lindbergh CA ![]()
Received 27 February 2026
Accepted for publication 14 May 2026
Published 17 June 2026 Volume 2026:22 605644
DOI https://doi.org/10.2147/NDT.S605644
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Taro Kishi
Shakaib Khan,1 Luis Velez Figueroa,1 Chindhuri Selvadurai,2 Ajit Rajendra Deshpande,1 Fatemeh Najmivarzaneh,2 Cutter A Lindbergh1
1Department of Psychiatry, University of Connecticut Health Center, Farmington, CT, USA; 2Department of Neurology, University of Connecticut Health Center, Farmington, CT, USA
Correspondence: Shakaib Khan, Department of Psychiatry, University of Connecticut Health Center, 263 Farmington Ave., Farmington, CT, 06030, USA, Tel +1-860-679-3265, Email [email protected]
Introduction: Huntington’s disease (HD) is a progressive neurodegenerative disorder characterized by worsening motor dysfunction, cognitive decline, and psychiatric symptoms. Psychiatric symptoms in HD arise from progressive frontostriatal circuit dysfunction and often precede motor manifestations, contributing significantly to disability and functional decline. In the absence of disease-modifying therapies, clinical care focuses on symptom management and functional preservation.
Methods: This was a retrospective pre-post chart review comparing longitudinal clinical outcomes before and after implementation of a multidisciplinary clinic model in HD patients (N = 56) using an observational study design. Differences were analyzed using paired-samples t-tests, with effect sizes reported as Cohen’s d. Depressive and anxiety symptoms were measured using the Patient Health Questionnaire-9 (PHQ-9) and Generalized Anxiety Disorder-7 (GAD-7), respectively. Motor symptoms were assessed using the Unified Huntington’s Disease Rating Scale (UHDRS) motor subscale. Cognitive symptoms were measured using the Montreal Cognitive Assessment (MoCA).
Results: Anxiety and depression symptom trajectories showed increased stability after initiation of the multidisciplinary clinic (ds = − 0.008 and 0.133, respectively) compared to worsening trajectories prior to initiation (ds = 0.309 and 0.366, respectively). About 64– 67% of patients were responders post-clinic relative to only 33– 43% pre-clinic. Motor symptom severity significantly decreased following integrated clinic model implementation (d = − 0.341), representing deviation from the expected progressive trajectory of manifest HD. Cognitive performance remained stable across follow-up intervals.
Discussion: Our findings suggest that multidisciplinary integrated care may favorably influence motor and psychiatric symptom trajectories in HD, supporting the value of a coordinated, team-based approach to managing this complex disorder. While observed effects were not particularly large, in the context of a progressive neurodegenerative condition, modest improvement or even stabilization in symptoms represents a clinically meaningful deviation from the expected course of decline. However, conclusions and generalizability are limited by the modest sample size and retrospective observational design.
Plain Language Summary: Huntington’s disease is a progressive inherited brain disorder that causes worsening movement difficulties, cognitive decline, and severe emotional and behavioral symptoms. There are currently no treatments that can stop or slow the underlying disease process, which means care focuses on managing symptoms and preserving independence. Although multidisciplinary care bringing together neurology, mental health, and social support within a coordinated clinic visit is widely recommended, there is little quantitative evidence showing whether this approach meaningfully alters how symptoms evolve over time.
In this study, we evaluated patients with Huntington’s disease before and after the implementation of an integrated clinic model that combined neurological, psychiatric, and social care in a single structured visit. We examined changes in movement, mood, anxiety, and cognitive functioning over extended follow-up periods. After the integrated model was introduced, movement symptoms improved and emotional symptoms stabilized, contrasting with worsening patterns observed before the clinic redesign. Cognitive performance remained stable.
While observational in design, these findings suggest that coordinated, team-based care may do more than simply support patients; it may influence measurable symptom trajectories in a progressive brain disorder. This work provides important evidence that system-level changes in care delivery can have meaningful clinical impact in Huntington’s disease.
Keywords: Huntington’s disease, integrated care models, neurodegenerative disorders, anxiety, depression
Background
Huntington’s disease (HD) is a hereditary neurodegenerative disorder caused by an expansion of Cytosine-Adenine-Guanine (CAG) trinucleotide repeats in the huntingtin (HTT) gene located on chromosome 4p16.3 that encodes the Huntingtin protein.1 The abnormal polyglutamine expansion in the huntingtin protein results in progressive neurodegeneration, primarily affecting the striatum (caudate and putamen), although the brain is globally affected.2,3 Pathologically, 90% of the striatum’s medium spiny neurons (MSN) degenerate.4 The disease is inherited in an autosomal dominant manner and disease onset and severity correlate with CAG repeat length. Earlier age of onset and more severe disease are correlated with great number of CAG repeats.5 The disease typically manifests between ages 30 and 50, with symptoms in 3 major domains: motor, psychiatric and cognitive.4 Life expectancy is estimated to be within 20 years from time of diagnosis.1
Motor manifestations are hallmark features of HD. In early disease, motor symptoms include progressive, hyperkinetic involuntary movements such as chorea. Later in the disease course, symptoms progress to hypokinesia, bradykinesia and dystonia.4 The balance of hyperkinesia and hypokinesia varies from patient to patient and makes progression unique. Dysarthria and dysphagia are common symptoms and lead to increased morbidity and mortality, with aspiration pneumonia being a leading cause of death.6
Psychiatric symptoms often precede motor onset by many years and can include depression, apathy, irritability, agitation, anxiety, paranoia, delusions and hallucinations.7 It is estimated that up to 73–98% of patients will have a major psychiatric disorder which is linked to more rapid decline in the independence scale (IS).7–11 Depression symptoms are common and are reported by up to 50% of patients during the course of their illness.12 Depression has been linked to more rapid decline in functional capacity.11 In HD, completed suicides have been reported to be as high as 13%, a seven-to-twelve-fold increase compared to the general population.3 Neurobiologically, many of these psychiatric manifestations reflect disruption of frontostriatal circuits, including degeneration of medium spiny neurons within the caudate and putamen and impaired connectivity between the prefrontal cortex and basal ganglia. Dysfunction within these cortico-striatal-thalamo-cortical loops is associated with affective dysregulation, apathy, impulsivity, and executive dysfunction, underscoring that psychiatric symptoms in HD are intrinsic neurologic features rather than secondary psychological reactions to illness.
Cognitive difficulties in HD include progressive impairment in attention, executive functioning, social cognition (eg, emotion recognition), and cognitive slowing. Hallmark neurocognitive symptoms of HD include apathy, anosognosia, and disinhibition, which are symptoms shared by many other cognitive and psychiatric conditions.12 Anosognosia can be prevalent in all stages of disease which can create tension and conflict within the family, leading to interference with medical care.13
HD manifests with complex symptoms, ranging from psychiatric disorders to various motor symptoms and cognitive deficits. These occur with varying severity and progress overtime. There is no FDA approved disease modifying or curative treatment to date and mainstay of treatment is symptom management with a goal to maintain function as long as possible. Multidisciplinary teams—composed of professionals including movement disorder specialists, mental health providers, social workers and speech language pathologist—are often assumed to be the gold standard to meet the complex needs of patients and their families.14 However, a multidisciplinary approach is costly and resource-intensive. Although multidisciplinary care is widely recommended for HD, longitudinal real-world data using validated clinical outcome measures remain limited. Few studies have quantitatively examined whether integrated clinic models are associated with measurable changes in symptoms trajectories over time. This study addresses this gap by using a within-subject pre-post design to examine motor, psychiatric, and cognitive symptom trajectories before and after implementation of an integrated neurobehavioral clinic model.
Methods
Study Design and Setting
This study employed a retrospective, within-subject pre-post observational design comparing longitudinal clinical trajectories before (5/2018 to 7/2023) and after implementation (7/2023 to 6/2025) of the multidisciplinary clinic model in a single-site academic medical center setting. The clinic received designation as a Huntington’s Disease Society of America (HDSA) Center of Excellence in January 2024. Huntington’s Disease Society of America is a disease-centered organization which confers special recognition to clinical centers, Huntington’s Disease Center of Excellence (HD CoE), in the US for HD.15
This study was reviewed and approved as exempt research by the Institutional Review Board at UConn Health (Protocol Number: [26X-082-1]) because it falls under secondary research for which consent is not required due to the retrospective nature of the review and the data were recorded by the investigator in such a manner that the identity of subjects cannot readily be ascertained, the investigator does not contact subjects, and the investigator does not re-identify subjects. Subject privacy was upheld. All data was anonymized and stored on a secure network drive with access restricted to key study personnel. This project conforms to the standards set forth by the Declaration of Helsinki.
We implemented a structured multidisciplinary neurobehavioral clinic model integrating movement disorders neurology, psychiatry, and social work within a single coordinated visit. The model included a 2-hour coordinated visit with the movement disorders neurology, psychiatry, and social work, followed by an interdisciplinary case conference to generate a unified care plan. Appointments were divided into 1 hour with the neurologist, 30 minutes with psychiatry and 30 minutes with social work in synchronized visits.
During each visit, movement disorder neurologists conducted structured motor assessments and optimized pharmacologic management of chorea and related motor manifestations. Psychiatric providers evaluated mood, anxiety, suicidality, and behavioral dysregulation, with targeted psychotropic adjustments including antidepressants, antipsychotics, and VMAT-2 inhibitors when indicated. Given the overlapping pharmacologic roles of dopamine-modulating agents in HD, medication adjustments were coordinated across neurology and psychiatry.
Following each clinic session, an interdisciplinary case conference was conducted to integrate findings and to generate a coordinated treatment plan.
Participants
All individuals with a diagnosis of HD receiving care in the HD CoE were included in the analytic sample if they had at least two longitudinal time points within either the pre-implementation or post-implementation period. No additional exclusion criteria were applied.
Outcome Measures
We used the Patient Health Questionnaire 9 (PHQ-9) to measure depression, the Generalized Anxiety Disorder 7 (GAD-7) for anxiety, the United Huntington’s Disease Rating Scale (UHDRS) for movement monitoring, and the Montreal Cognitive Assessment (MoCA) for cognition. The UHDRS is 30-question, clinician administered rating scale used to monitor movement symptoms in HD.16 The PHQ-9 is a 9-question self-report tool used to screen for presence and severity of depression.17 The GAD-7 is a 7-question self-report tool used to screen for presence and severity of anxiety.18 The MoCA is a 30-point screening tool designed to detect cognitive impairment.19
Data Collection Procedures
To determine the effects of the multidisciplinary intervention on clinical trajectories, data from four visits (timepoints) were used in statistical analyses. Visits 1 and 2 occurred prior to implementation of the multidisciplinary clinic whereas visits 3 and 4 occurred after implementation of the multidisciplinary clinic. In cases where there were more than two time points available, the first and last scores during pre-implementation and post-implementation were used to maximize follow-up duration. The average time interval between visits was 20.84 months.
Sample sizes differed across outcomes based on available data. Prior to implementation of the multidisciplinary model, UHDRS motor assessments were not consistently documented at each visit. Following implementation, standardized UHDRS motor evaluation was embedded into clinic workflow, resulting in improved measurement completeness post-implementation. All available data for each analysis were used to maximize representativeness.
Statistical Analysis
Paired-samples t-tests (p < 0.05 two-sided significance level) were conducted to compare rates of change in each outcome measure (PHQ-9, GAD-7, UHDRS, and MoCA) from visit 1 to visit 2 (pre-clinic) and from visit 3 to visit 4 (post-clinic). The assumptions underlying the use of paired-samples t-tests (eg, dependent variable on a continuous scale, random sampling, normal distribution of differences between paired values, no extreme outliers in difference scores, etc) were generally met in our analyses.20 However, we acknowledge the potential for parametric analyses, including t-tests, to be less robust to potential violations of assumptions when the analytic sample is small.21 Accordingly, for any statistical analysis that contained fewer than 30 subjects (n < 30), we also conducted a non-parametric alternative, the Wilcoxon Signed Rank Test, to confirm that our findings held.21 The non-parametric analyses yielded the same pattern of results as the parametric analyses in all such instances. Accordingly, only results from parametric analyses (paired-samples t-tests) are reported below.
For all analyses, effect sizes are reported as Cohen’s d. Patients were categorized as “responders” if symptom severity improved or remained stable across the observation interval. In progressive neurodegenerative disorders, stabilization represents deviation from expected clinical decline and therefore constitutes a clinically meaningful outcome. Medication adjustments were not controlled analytically as they represent an inherent component of the multidisciplinary intervention.
Regarding our handling of missing data, we included all available data (ie, every subject with at least one paired observation) in our analyses to maximize representativeness. We elected not to apply imputation methods to avoid introducing additional imputation-related model assumptions, which may not be met in smaller sample sizes.22,23 Further, the use of imputation methods has potential to introduce artificial differences into the data and our goal was to preserve the interpretability of observed within-subject changes in a “real world” clinical setting.22,23
Power Considerations
A paucity of research has quantitatively examined the extent to which multidisciplinary integrated care clinics are associated with measurable changes in clinical outcomes in HD. This makes it challenging to estimate effect sizes based on prior literature. Further, the sample size for the present study was constrained by the study design (retroactive chart review) and nature of the study population (rare neurodegenerative disorder). These factors complicate traditional sample size and power calculations. Nonetheless, we present power analyses for a range of effect sizes to help guide interpretation of our results. All power analyses were performed in G*Power and based on a paired-samples t-test with a two-sided significance level of 0.05.24,25 These power analyses indicated the following: a sample size of 34 would yield ≥80% power to detect a medium effect size (Cohen’s d = 0.5); a sample size of 21 would yield ≥80% power to detect a medium-to-large effect size (Cohen’s d = 0.65); and a sample size of 15 would yield ≥80% power to detect a large effect size (Cohen’s d = 0.8). While the sample size for most of our analyses were adequately powered (ie, ≥80%) to detect a medium or medium-to-large effect, for some outcome measures (eg, MoCA scores) the available sample size was smaller and should be interpreted accordingly given the potential for Type II error.
Results
Baseline demographic characteristics of the sample are described in Table 1. Briefly, there were 56 subjects, they were in their mid-50s on average with more females (74%) than males. The sample was predominately white (88%). Disease stage distribution and CAG repeat length were not uniformly available in retrospective documentation and therefore were not included in subgroup analyses.
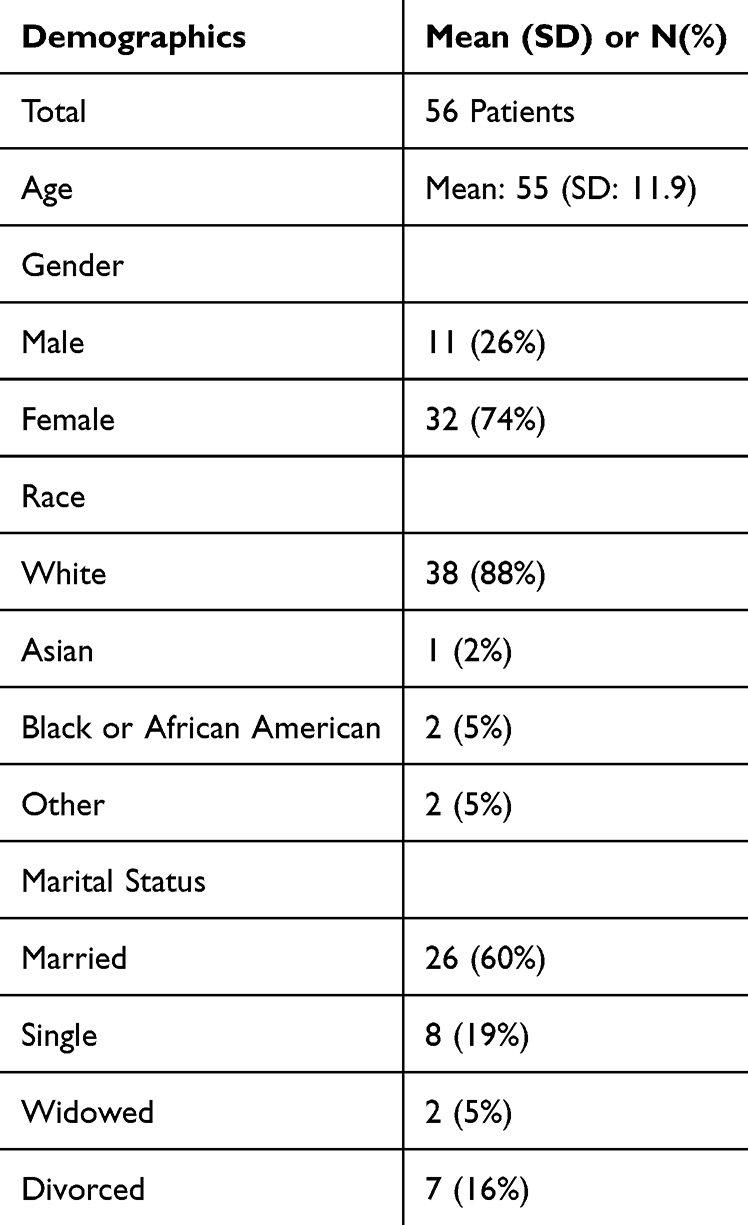 |
Table 1 Demographics |
Table 2 presents descriptive statistics of the clinical outcome measures at each of the four timepoints (visits 1–4). As detailed in Table 2, the analytic sample varied in size across outcome measures due to variability in longitudinal documentation inherent to retrospective rare-disease cohorts. All available paired observations were included in each analysis to maximize representativeness while preserving within-subject comparisons.
 |
Table 2 Descriptive Statistics of Clinical Outcomes |
Depression Trajectories
Prior to clinic implementation, PHQ-9 scores increased significantly from visit 1 to visit 2 [t(34) = 2.165, p = 0.038, d = 0.366], reflecting worsening depressive symptoms over time. Following implementation of the multidisciplinary clinic, PHQ-9 scores did not significantly change from visit 3 to visit 4 [t(34) = 0.785, p = 0.438, d = 0.133], indicating a stabilization of depressive symptoms severity. Descriptively, 64% met responder criteria (stable or improved depressive symptoms over time) post-clinic compared to 43% pre-clinic. In the context of a progressive neurodegenerative disorder, the absence of continued worsening represents deviation from the prior trajectory observed in the same cohort.
Anxiety Trajectories
GAD-7 scores evidenced a trend toward worsening anxiety from visit 1 to visit 2 prior to initiation of the multidisciplinary clinic, though this was not statistically significant [t(29) = 1.692, p = 0.101, d = 0.309]. There was non-significant change in GAD-7 scores from visit 3 to visit 4, indicating stability in anxiety over time following the multidisciplinary clinic [t(35) = −0.051, p = 0.960, d = −0.008]. Descriptively, 67% of the sample were responders (stable or improved anxiety symptoms over time) post-clinic compared to only 33% pre-clinic.
Motor Trajectories
Pre-implementation UHDRS motor scores did not significantly change between visit 1 to visit 2 [t(6) = 0.386, p = 0.713, d = 0.146], though interpretation is limited by small sample size (n = 7 with paired date). Following implementation, UHDRS motor scores significantly decreased from visit 3 to visit 4, indicating improved motor symptoms over time after initiation of the multidisciplinary clinic [t(35) = −2.044, p = 0.049, d = −0.341], indicating reduction in motor severity over time. Descriptively, 69% of the sample met responders criteria post-clinic compared to 43% pre-clinic. Given that longitudinal natural history studies of manifest HD typically demonstrate progressive motor worsening over comparable intervals, the observed stabilization and reduction in UHDRS motor scores post-implementation warrant further investigation.
Cognitive Trajectories
MoCA scores did not significantly change pre-clinic from visit 1 to visit 2 [t(10) = 0.787, p = 0.450, d = 0.237]. Similarly, MoCA scores also did not significantly change post-clinic from visit 3 to visit 4 [t(10) = −0.747, p = 0.473, d = −0.255]. Mean score changes across intervals were less than one point, suggesting absence of clinically meaningful short-term cognitive decline.
Discussion
The primary aim of this study was to examine whether implementation of a structured multidisciplinary neurobehavioral clinical model was associated with changes in longitudinal motor, psychiatric, and cognitive trajectories in individuals with Huntington’s disease (HD). Following clinic implementation, depressive and anxiety symptoms stabilized, and motor severity demonstrated statistically significant improvement, with a majority of patients meeting responder criteria across domains. In the context of HD, a progressive frontostriatal neurodegenerative disorder in which gradual symptom worsening is expected over time, these findings suggest deviation from prior trajectory patterns observed within the same cohort. Motor symptoms showed significant longitudinal improvements post-clinic, with a majority (69%) of the sample classified as responders. Cognitive functioning remained stable across follow-up. These findings are notable in the context of HD, a progressive neurodegenerative disorder in which symptom worsening is typically expected over comparable intervals.26 In this setting, stabilization or modest improvement represents a clinically meaningful deviation from the anticipated disease course.
Huntington’s disease is characterized by progressive degeneration of medium spiny neurons within the striatum and disruption of cortico-striatal-thalamo-cortical circuits that subserve motor control, executive functioning, and affective regulation. The convergence of motor, psychiatric, and cognitive symptoms reflects shared circuit-level dysfunction rather than isolated domains of pathology. In the absence of disease-modifying therapies, clinical management is necessarily focused on optimizing symptomatic control and preserving functional capacity. The present findings contribute quantitative evidence suggesting that integrated, team-based care favorably influences symptom trajectories across multiple domains.
Current FDA approved treatments for HD focus on symptom management alone and have not been shown to modify disease course.27 Prior treatments that have been unsuccessfully attempted for disease modification for HD include cholinesterase inhibitors, such as donepezil for memory, chorea, and quality of life (QoL).28,29 Conventional treatment for Huntington’s disease remains symptomatic and typically includes VMAT-2 inhibitors or dopamine-blocking agents for chorea, antidepressants or anxiolytics for mood and anxiety symptoms, antipsychotics or mood stabilizers for irritability and behavioral dysregulation, and supportive interventions including physical therapy, speech-language pathology, nutrition, social work, and caregiver support.30 The side effect profile for approved medications is very extensive, from fatigue, weight gain, depression and suicidality, so a multidisciplinary non-pharmacological approach may avoid some of these pitfalls.27 These services are often delivered in parallel rather than through a single coordinated model. The present study does not establish superiority over conventional care because it was observational and lacked a parallel control group. However, the findings suggest that coordinated multidisciplinary care may offer advantages over fragmented care by allowing synchronized medication adjustment, measurement-based monitoring, and rapid interdisciplinary communication. Several mechanisms may explain the observed stabilization and improvement. Synchronized neurology and psychiatry assessment may reduce fragmented medication changes, especially for dopamine-modulating agents that affect both motor and behavioral symptoms. Measurement-based care may allow earlier detection of worsening symptoms. Social work and caregiver involvement may improve adherence, access to resources, safety planning, and continuity of care. Together, these mechanisms may help explain why integrated care could influence psychiatric and motor trajectories even in the absence of disease-modifying treatment. Future work would benefit from incorporating neuroimaging data to elucidate neural mechanisms of clinical symptom trajectories and treatment response, including potential changes to brain white matter and functional connectivity, as has been done by other research groups.31,32
Interpretation of outcomes in rare neurodegenerative diseases warrants particular attention to clinical relevance alongside statistical significance. In such contexts, reliance solely on p-values may obscure clinically meaningful change. The progressive and heterogeneous nature of HD—combined with symptom overlap between neurodegeneration and psychiatric burden (eg, fatigue, psychomotor slowing)—further complicates the interpretation of standardized symptom scales. Within this framework, the observed effect sizes for psychiatric and motor symptoms (d = 0.13–0.36), though modest, gain greater importance. Notably, cognitive performance did not significantly decline following clinic implementation, and the magnitude of change on the MoCA (<1 point) was not clinically meaningful. In our cohort, MoCA scores did not show meaningful longitudinal decline, a pattern that aligns with prior longitudinal work indicating that brief cognitive screening tools such as the MoCA may lack sensitivity to detect short-term cognitive change in manifest HD despite capturing cross-sectional impairment. Specifically, in a 12-month study comparing brief cognitive tests to comprehensive neuropsychological measures, MoCA demonstrated reasonable cross-sectional validity but was less effective than the UHDRS cognitive component at reflecting short-term change in HD patients over a 12-month interval.33
Motor symptoms demonstrated significant improvement following multidisciplinary clinic implementation. Motor severity, as measured by the UHDRS motor subscale, significantly decreased following clinic implementation. In natural history cohorts of manifest HD, motor scores typically worsen over comparable intervals, reflecting progressive striatal degeneration. Against this expected trajectory, the observed reduction in motor severity may reflect improved pharmacologic coordination, earlier adjustment of dopamine-modulating agents, and mitigation of behavioral exacerbators that amplify functional impairment. While causal inference cannot be established, the directional shift in motor trajectory warrants further prospective investigation. Reductions in both depressive and anxiety symptoms were observed over the intervention period. Both PHQ-9 and GAD-7 reflect moderate effect sizes. Although the average reductions in PHQ-9 and GAD-7 scores fell just below commonly accepted thresholds for minimally clinically important differences (MCID) typically 4–5 points for PHQ-9 and 3–4 points for GAD-7—the observed effect sizes suggest that a meaningful subset of participants likely experienced symptom changes perceptible in daily functioning. Psychiatric symptoms in HD are increasingly recognized as intrinsic manifestations of frontostriatal circuit dysfunction rather than purely reactive phenomena. Depression and anxiety have been associated with accelerated functional decline and reduced quality of life. The observed stabilization of depressive and anxiety trajectories following clinic implementation may reflect coordinated psychotropic optimization, systematic suicide risk assessment, and structured psychosocial support embedded within neurologic care. In progressive neurodegenerative conditions, interruption of psychiatric worsening may indirectly influence adherence, engagement, and overall functional outcomes. Depression and anxiety are highly prevalent in HD, with reported lifetime rates ranging from 40% to 60%, and they substantially reduce quality of life while influencing the trajectory of cognitive and motor symptoms.26,34 Prior studies demonstrate that multidisciplinary models and integrated psychiatric care can effectively address the complex emotional and behavioral manifestations of HD, improving coping, adherence, and psychosocial functioning.35,36
Several interrelated mechanisms may underlie the observed patterns. Synchronized evaluation by neurology and psychiatry likely reduced fragmented medication adjustments, particularly for dopamine-modulating agents with dual motor and behavioral effects. Also, embedding measurement-based care (PHQ-9, GAD-7, UHDRS, MoCA) within clinical workflow enabled early detection of symptom shifts and timely intervention. The inclusion of social work and caregiver engagement is commonly stated to help but limited empirical evidence is available to demonstrate the benefit of a multidisciplinary approach. Together, these system-level modifications allowed for a proactive, individualized approach, one that may be uniquely suited to the fluctuating course and psychosocial complexity of HD, and that demonstrates potential to shift clinical trajectories even in the absence of statistically large effects.
Limitations
The observational pre–post design precludes causal inference, as improvements could reflect regression to the mean, spontaneous remission, or unmeasured confounders such as concurrent life events or medication adjustments. The modest sample size limits statistical power and generalizability, and the possibility of false negative findings (Type II error) cannot be ruled out, particularly for outcome measures (eg, MoCA scores) in which fewer subjects were available for analyses. The lack of external validation also limits confidence in generalizability. In a similar vein, the stability of cognitive outcomes should be interpreted with caution given the potential for skewed distributions (eg, ceiling effects), as well as limited sample heterogeneity, though it is encouraging that we obtained the same pattern of results when applying non-parametric statistical techniques to the data. Future studies are warranted in larger sample sizes, ideally with a control group, to replicate our findings before drawing definitive conclusions. While we acknowledge that replication may be limited by variability in clinical implementation practices, as well as differences in chosen outcome measures, our goal was to assess the potential effects of multidisciplinary integrated care in a “real world” clinical setting, as opposed to a tightly regulated research trial. It will be informative to see whether our findings hold in other clinics who adhere to core tenets of multidisciplinary integrated care but may have different implementation practices and outcome measures. It is possible that treatment effects will be enhanced or attenuated in such cases. Measurement overlap between psychiatric symptoms and neurodegenerative features may have influenced symptom ratings. Of note, treatment heterogeneity, including variation in pharmacologic regimens, psychotherapy exposure, and caregiver engagement, was not controlled for and may have influenced outcomes. Additionally, absence of a parallel non-intervention control cohort limits the ability to distinguish intervention effects from natural variability or regression to the mean.
Conclusion
In a progressive neurodegenerative condition with limited therapeutic options, multidisciplinary integrated care offers meaningful clinical benefit. Prior research has demonstrated that care models that incorporate psychiatry, neurology, social work, and psychotherapy may enable earlier detection and more effective treatment of psychiatric comorbidities but empirical evidence of outcomes is lacking.37 By demonstrating stabilization or improvement in psychiatric and motor symptom trajectories using validated longitudinal measures, this study provides preliminary quantitative evidence that a structured multidisciplinary clinic model may influence measurable motor and psychiatric trajectories in Huntington’s disease. These preliminary findings suggest that a structured multidisciplinary clinic model may be associated with stabilization or improvement in psychiatric and motor symptom trajectories in Huntington’s disease. While the observational design precludes causal inference, the results provide quantitative support for further prospective evaluation of integrated neurobehavioral care models in HD. Controlled studies are needed to determine whether coordinated multidisciplinary care produces durable benefits beyond conventional symptomatic management.
Data Sharing Statement
Data used for this manuscript will not be shared as participants did not provide consent for it to be shared publicly.
Ethics Approval and Informed Consent
This study was reviewed and approved as exempt research by the Institutional Review Board at UConn Health (Protocol Number: [26X-082-1]) because it falls under secondary research for which consent is not required due to the retrospective nature of the review and the data were recorded by the investigator in such a manner that the identity of subjects cannot readily be ascertained, the investigator does not contact subjects, and the investigator does not re-identify subjects. Subject privacy was upheld. All data was anonymized and stored on a secure network drive with access restricted to key study personnel. This project conforms to the standards set forth by the Declaration of Helsinki.
Funding
This work is supported by the Department of Psychiatry at University of Connecticut Health Center. There was no external funding source.
Disclosure
The authors have no conflicts of interest or competing interest related to this work. The authors declare that this manuscript is original work and has not been published previously, nor is it currently under consideration for publication elsewhere. All authors have read and approved the final manuscript and agree to its submission.
References
1. Walker FO. Huntington’s disease. Lancet. 2007;369:218–10. doi:10.1016/S0140-6736(07)60111-1
2. Gil JM, Rego AC. Mechanisms of neurodegeneration in Huntington’s disease. Eur J Neurosci. 2008;27:2803–2820. doi:10.1111/j.1460-9568.2008.06310.x
3. Wetzel HH, Gehl CR, Dellefave L, et al. Suicidal ideation in Huntington disease: the role of comorbidity. Psychiatry Res. 2011;188:372–376. doi:10.1016/j.psychres.2011.05.006
4. Ajitkumar A, Lui F, De Jesus O. Huntington disease. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025.
5. Duyao M, Ambrose C, Myers R, et al. Trinucleotide repeat length instability and age of onset in Huntington’s disease. Nat Genet. 1993;4:387–392. doi:10.1038/ng0893-387
6. Pizzorni N, Pirola F, Ciammola A, et al. Management of dysphagia in Huntington’s disease: a descriptive review. Neurol Sci. 2020;41:1405–1417. doi:10.1007/s10072-020-04265-0
7. Peixoto C, Rego D, Bicho M, et al. Psychiatric symptoms in huntington’s disease. Eur Psychiatry. 2021;64:S254–S255. doi:10.1192/j.eurpsy.2021.682
8. Paulsen JS, Nehl C, Hoth KF, et al. Depression and stages of Huntington’s disease. J Neuropsychiatry Clin Neurosci. 2005;17:496–502. doi:10.1176/jnp.17.4.496
9. Paoli RA, Botturi A, Ciammola A, et al. Neuropsychiatric burden in Huntington’s disease. Brain Sci. 2017;7:67. doi:10.3390/brainsci7060067
10. Thompson JC, Harris J, Sollom AC, et al. Longitudinal evaluation of neuropsychiatric symptoms in Huntington’s disease. J Neuropsychiatry Clin Neurosci. 2012;24:53–60. doi:10.1176/appi.neuropsych.11030057
11. Marder K, Zhao H, Myers RH, et al. Rate of functional decline in Huntington’s disease. Neurology. 2000;54:452. doi:10.1212/WNL.54.2.452
12. Bates GP, Dorsey R, Gusella JF, et al. Huntington disease. Nat Rev Dis Primers. 2015;1:15005. doi:10.1038/nrdp.2015.5
13. Boll TJ, Heaton R, Reitan RM. Neuropsychological and emotional correlates of Huntington’s chorea. J Nerv Mental Dis. 1974;158:61. doi:10.1097/00005053-197401000-00008
14. Mühlbӓck A, van Walsem M, Nance M, et al. What we don’t need to prove but need to do in multidisciplinary treatment and care in Huntington’s disease: a position paper. Orphanet J Rare Dis. 2023;18:19. doi:10.1186/s13023-023-02622-8
15. Bardakjian TM, Klapper J, Carey A, et al. Addressing the value of multidisciplinary clinical care in Huntington’s disease: a snapshot of a New Huntington’s Disease Center. J Huntingtons Dis. 2019;8:501–507. doi:10.3233/JHD-190355
16. Huntington HS. Unified Huntington’s disease rating scale: reliability and consistency. Mov Disord. 1996;11:136–142. doi:10.1002/mds.870110204
17. Kroenke K, Spitzer RL, Williams JBW. The PHQ-9. J Gen Intern Med. 2001;16:606–613. doi:10.1046/j.1525-1497.2001.016009606.x
18. Dhira TA, Rahman MA, Sarker AR, et al. Validity and reliability of the Generalized Anxiety Disorder-7 (GAD-7) among university students of Bangladesh. PLoS One. 2021;16:e0261590. doi:10.1371/journal.pone.0261590
19. Daniel B, Agenagnew L, Workicho A, et al. Psychometric properties of the Montreal Cognitive Assessment (MoCA) to detect major neurocognitive disorder among older people in ethiopia: a validation study. NDT. 2022;18:1789–1798. doi:10.2147/NDT.S377430
20. Verma JP, Abdel-Salam A-SG. Testing Statistical Assumptions in Research. Hoboken: John Wiley & Sons; 2019.
21. Vrbin CM. Parametric or nonparametric statistical tests: considerations when choosing the most appropriate option for your data. Cytopathology. 2022;33(6):663–667. doi:10.1111/cyt.13174
22. Fleming TR. Addressing missing data in clinical trials. Ann Intern Med. 2011;154:113–117. doi:10.7326/0003-4819-154-2-201101180-00010
23. Jakobsen JC, Gluud C, Wetterslev J, et al. When and how should multiple imputation be used for handling missing data in randomised clinical trials - a practical guide with flowcharts. BMC Med Res Methodol. 2017;17:162. doi:10.1186/s12874-017-0442-1
24. Faul F, Erdfelder E, Lang A-G, et al. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39:175–191. doi:10.3758/BF03193146
25. Faul F, Erdfelder E, Buchner A, et al. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav Res Methods. 2009;41:1149–1160. doi:10.3758/BRM.41.4.1149
26. van Lonkhuizen PJC, Frank W, Heemskerk A-W, et al. Quality of life, health-related quality of life, and associated factors in Huntington’s disease: a systematic review. J Neurol. 2023;270:2416–2437. doi:10.1007/s00415-022-11551-8
27. Ferguson MW, Kennedy CJ, Palpagama TH, et al. Current and possible future therapeutic options for Huntington’s disease. J Cent Nerv Syst Dis. 2022;14:11795735221092517. doi:10.1177/11795735221092517
28. Vattakatuchery JJ, Kurien R. Acetylcholinesterase inhibitors in cognitive impairment in Huntington’s disease: a brief review. World J Psychiatry. 2013;3:62–64. doi:10.5498/wjp.v3.i3.62
29. Cubo E, Shannon KM, Tracy D, et al. Effect of donepezil on motor and cognitive function in Huntington disease. Neurology. 2006;67:1268–1271. doi:10.1212/01.wnl.0000238106.10423.00
30. Nagarajan E, Sanmugam DL. Huntington disease treatment & management: approach considerations, pharmacologic treatment, nonpharmacologic treatment. 2025. Available from: https://emedicine.medscape.com/article/1150165-treatment#d10.
31. Liu X, Wei Z, Li L, et al. Effect of continuous esketamine infusion on brain white matter microstructure in patients with major depression: a diffusion tensor imaging study. J Affective Disorders. 2025;372:173–181. doi:10.1016/j.jad.2024.12.002
32. Li L, Shi Q, Fang B, et al. Functional connectivity changes in primary motor cortex subregions of patients with obstructive sleep apnea. Brain Behav. 2025;15:e70698. doi:10.1002/brb3.70698
33. Toh EA, MacAskill MR, Dalrymple-Alford JC, et al. Comparison of cognitive and UHDRS measures in monitoring disease progression in Huntington’s disease: a 12-month longitudinal study. Transl Neurodegener. 2014;3:15. doi:10.1186/2047-9158-3-15
34. Dale M, van Duijn E. Anxiety in Huntington’s disease. J Neuropsychiatry Clin Neurosci. 2015;27:262–271. doi:10.1176/appi.neuropsych.14100265
35. The varied roles of neuropsychology in a multidisciplinary clinic for Huntington’s disease. ABPP; 2025. Available from: https://abpp.org/newsletter-post/the-varied-roles-of-neuropsychology-in-a-multidisciplinary-clinic-for-huntingtons-disease/.
36. Zadegan SA, Ramirez F, Reddy KS, et al. Treatment of depression in Huntington’s disease: a systematic review. JNP. 2024;36:283–299. doi:10.1176/appi.neuropsych.20230120
37. Țenea-Cojan Ș-T, Dinescu V-C, Gheorman V, et al. Exploring multidisciplinary approaches to comorbid psychiatric and medical disorders: a scoping review. Life. 2025;15:251. doi:10.3390/life15020251
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Subjective Sleep Disruption and Mood Disorders are Associated with the Risk of Chronic Pain in Patients with Obstructive Sleep Apnea
Liu L, Li X, Xue P, Wu M, Zeng S, Dai Y, Zhou J
Nature and Science of Sleep 2022, 14:2023-2032
Published Date: 7 November 2022
Vitamin B12, Folate, Homocysteine, Inflammatory Mediators (Interleukin-6, Tumor Necrosis Factor-α and C-Reactive Protein) Levels in Adolescents with Anxiety or Depressive Symptoms
Tan Y, Zhou L, Huang J, Chen X, Wu Y, Song X, Wang J, Hu H, Yang Q
Neuropsychiatric Disease and Treatment 2023, 19:785-800
Published Date: 7 April 2023
AI Technology panic—is AI Dependence Bad for Mental Health? A Cross-Lagged Panel Model and the Mediating Roles of Motivations for AI Use Among Adolescents
Huang S, Lai X, Ke L, Li Y, Wang H, Zhao X, Dai X, Wang Y
Psychology Research and Behavior Management 2024, 17:1087-1102
Published Date: 12 March 2024
Longitudinal Problematic Social Media Use in Students and Its Association with Negative Mental Health Outcomes
Shannon H, Bush K, Shvetz C, Paquin V, Morency J, Hellemans KGC, Guimond S
Psychology Research and Behavior Management 2024, 17:1551-1560
Published Date: 8 April 2024
Mushrooms, Microdosing, and Mental Illness: The Effect of Psilocybin on Neurotransmitters, Neuroinflammation, and Neuroplasticity
Kinderlehrer DA
Neuropsychiatric Disease and Treatment 2025, 21:141-155
Published Date: 29 January 2025