Back to Journals » Journal of Inflammation Research » Volume 15
Modified Glasgow Prognostic Score is Better for Predicting Oncological Outcome in Patients with Soft Tissue Sarcoma, Compared to High-Sensitivity Modified Glasgow Prognostic Score
Authors Nakamura T ![]() , Asanuma K, Hagi T, Sudo A
, Asanuma K, Hagi T, Sudo A
Received 8 April 2022
Accepted for publication 16 June 2022
Published 11 July 2022 Volume 2022:15 Pages 3891—3899
DOI https://doi.org/10.2147/JIR.S369993
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Tomoki Nakamura, Kunihiro Asanuma, Tomohito Hagi, Akihiro Sudo
Department of Orthopedic Surgery, Mie University Graduate School of Medicine, Tsu City, Mie, 514-8507, Japan
Correspondence: Tomoki Nakamura, Department of Orthopaedic Surgery, Mie University Graduate School of Medicine, 2-174 Edobashi, Tsu City, Mie, 514-8507, Japan, Tel +81592315022, Fax +81592315211, Email [email protected]
Background: Inflammation plays a critical role in the development, progression, clinical presentation, and diagnosis of tumours. We compared the usefulness of the high-sensitivity modified Glasgow prognostic score (HS-mGPS) and mGPS in predicting oncological outcomes in patients with soft tissue sarcomas (STSs) who underwent primary surgical tumour resection.
Methods: Between 2002 and 2018, 144 patients were included in the study. The mean age of the patients was 63 years. The mean follow-up period was 76 months.
Results: The disease-specific survival (DSS) at five years was 71.5% in all patients. When patients were divided into three groups according to the HS-mGPS and mGPS, those with a score of 1 or 2 had a poorer DSS than those with a score of 0, respectively. When we compared the survival rate among the 98 patients with both HS-mGPS and mGPS of 0 and 21 patients with HS-mGPS of 1 and mGPS of 0, there was no significant difference in the prognosis. In multivariate analysis, larger tumour size and higher mGPS remained significant.
Conclusion: mGPS is a reliable system for identifying patients at high risk for death in patients with STSs.
Keywords: soft tissue sarcoma, modified Glasgow prognostic score, high-sensitivity modified Glasgow prognostic score, oncological outcome, C-reactive protein, albumin
Introduction
Soft tissue sarcoma (STS) is a rare and heterogeneous tumour.1 The incidence of STS is fewer than 6 per 100,000 cancer cases, accounting for 1–2% of all cancer cases in adults.1 Lung metastasis develops in 20–50% of STS patients, and the subsequent prognosis is poor.2 Inflammation plays a critical role in the development, progression, clinical presentation, and diagnosis of tumours.3,4 In cancer patients, inflammation is closely related to nutrition; inflammation induces malnutrition by increasing catabolism and impairing nutrient absorption; conversely, malnutrition promotes the severity of inflammation.5,6 Therefore, the combination of hypoalbuminaemia (< 3.5 g/dl) and elevated C-reactive protein (CRP) (> 1.0 mg/dl) levels, which is used to calculate the Glasgow prognostic score (GPS), is an important indicator.7 The modified GPS (mGPS) highlights the importance of CRP; when CRP is elevated, patients with normal albumin levels are assigned a score of 1.8 Recently, some authors have suggested that a lower threshold for CRP (> 0.3 mg/dl) may enhance the prognostic value of mGPS in patients with cancer, and a high-sensitivity modified GPS (HS-mGPS) has been proposed.9 Previous studies have shown the utility of the HS-mGPS in predicting the survival of patients with STSs,10,11 although the relationship between mGPS and survival in patients with STSs has not been reported due to the high threshold of CRP levels. In this study, we compared the usefulness of the HS-mGPS and mGPS in predicting oncological outcomes in patients with STSs who underwent primary surgical tumour resection with a minimum of one year follow-up after surgery.
Materials and Methods
Data Source
This study was approved by Mie University Hospital (H2020-224). Informed consent was obtained from all the patients. procedures followed were in accordance with the Helsinki Declaration of 1975, as revised in 1983. Data from 2002 to 2018 were retrospectively reviewed. Patients presenting with recurrent disease, metastases, and those referred for additional resection after a previous inappropriate excision were excluded from this study. We further excluded dermatofibrosarcoma protuberans and well-differentiated liposarcoma. Finally, 144 patients (88 men and 56 women) were included in the study. The mean age of the patients was 63 years (range 21–89 years). The tumours were located in the thigh (n = 60), leg (n = 18), buttock (n = 12), upper arm (n = 10), chest wall (n = 9), back (n = 9), forearm (n = 5), inguinal lesion (n = 5), and other sites (n = 16), including three retroperitoneal lesions. The mean follow-up period was 76 months (range 1–203 months). All patients underwent pretreatment staging with CT scans of the lungs to exclude metastases. The histological diagnosis and grade of the tumour were determined using the French Federation of Cancer Centers Sarcoma Group grading system. Serum albumin and CRP levels were obtained prior to treatment inclusing surgery, radiotherapy, and chemotherapy for all patients and were measured using a Denka Seiken X-2 autoanalyzer (Denka Seiken Co., Ltd., Tokyo, Japan). mGPS score was calculated as previously described.8 Briefly, patients with both hypoalbuminaemia (< 3.5 g/dl) and an elevated CRP level (> 1.0 mg/dl) were allocated a score of 2. Those who had only an elevated CRP level were assigned a score of 1. The remaining patients were allocated a score of 0. Further, the HS-mGPS was calculated as described previously.9 Briefly, patients with both hypoalbuminaemia (< 3.5 g/dl) and an elevated CRP level (> 0.3 mg/dl) were allocated a score of 2. Those who had only an elevated CRP level were assigned a score of 1. The remaining patients were allocated a score of 0. The primary purpose of this study was to elucidate the role of the mGPS and HS-mGPS in predicting oncological outcomes in patients with STS.
Statistical Analyses
Statistical associations between the clinicopathological variables were evaluated using the
Kruskal–Wallis rank-sum test for quantitative data and chi-square test for qualitative data. Survival time was measured from the date of surgery of the primary tumour to the date of sarcoma-related death or the last follow-up. Disease-free time was measured from the date of surgery of the primary tumour to the date of local recurrence and/or metastasis. Survival curves were generated using the Kaplan-Meier method and compared using the Log rank test. Univariate and multivariate analyses were performed using Cox proportional hazards regression models. Variables with a p-value < 0.05 in the univariate analyses were included in the multivariate analysis.
All statistical analyses were performed using the EZR graphical user interface (Saitama Medical Center, Jichi Medical University, Saitama, Japan) for R (R Foundation for Statistical Computing, Vienna, Austria), which is a modified version of R Commander designed to add statistical functions frequently used in biostatistics.
Results
The mean tumour size was 8.9 cm (range, 2–30 cm). The depth of the tumours was superficial in 29 patients and deep in 115 patients. Thirteen patients had grade 1 STSs, 44 had grade 2, and 87 had grade 3 STSs. The STSs were classified histologically as follows: 31 malignant fibrous histiocytomas (MFH) or undifferentiated pleomorphic sarcomas (UPS), 30 liposarcomas (15 myxoid type, 13 dedifferentiated type, and 2 pleomorphic type), 29 myxofibrosarcomas, 23 leiomyosarcomas, 8 malignant peripheral nerve sheath tumours, 7 synovial sarcomas, and 16 other STSs. All patients underwent primary surgical tumour resection. A total of 10 patients (7%) received adjuvant radiotherapy postoperatively, and 32 patients (22%) received perioperative chemotherapy. Radiotherapy was administered to patients having tumours with inadequate margin. Serum levels of albumin and CRP were measured before chemotherapy in these patients. The mGPS varied from 0 to 2. A total of 119 patients (82.6%) had a score of 0, 19 (13.2%) had a score of 1, and 6 (4.2%) had a score of 2. The HS-mGPS varied from 0 to 2. A total of 98 patients (68%) had a score of 0, 39 (27.1%) had a score of 1, and 7 (4.9%) had a score of 2. Therefore, of the 119 patients with an mGPS of 0, 21 patients had an HS-mGPS of 1. The relationship between the mGPS, HS-mGPS, and clinicopathological variables is shown in Table 1. The tumour size was related to the scoring system.
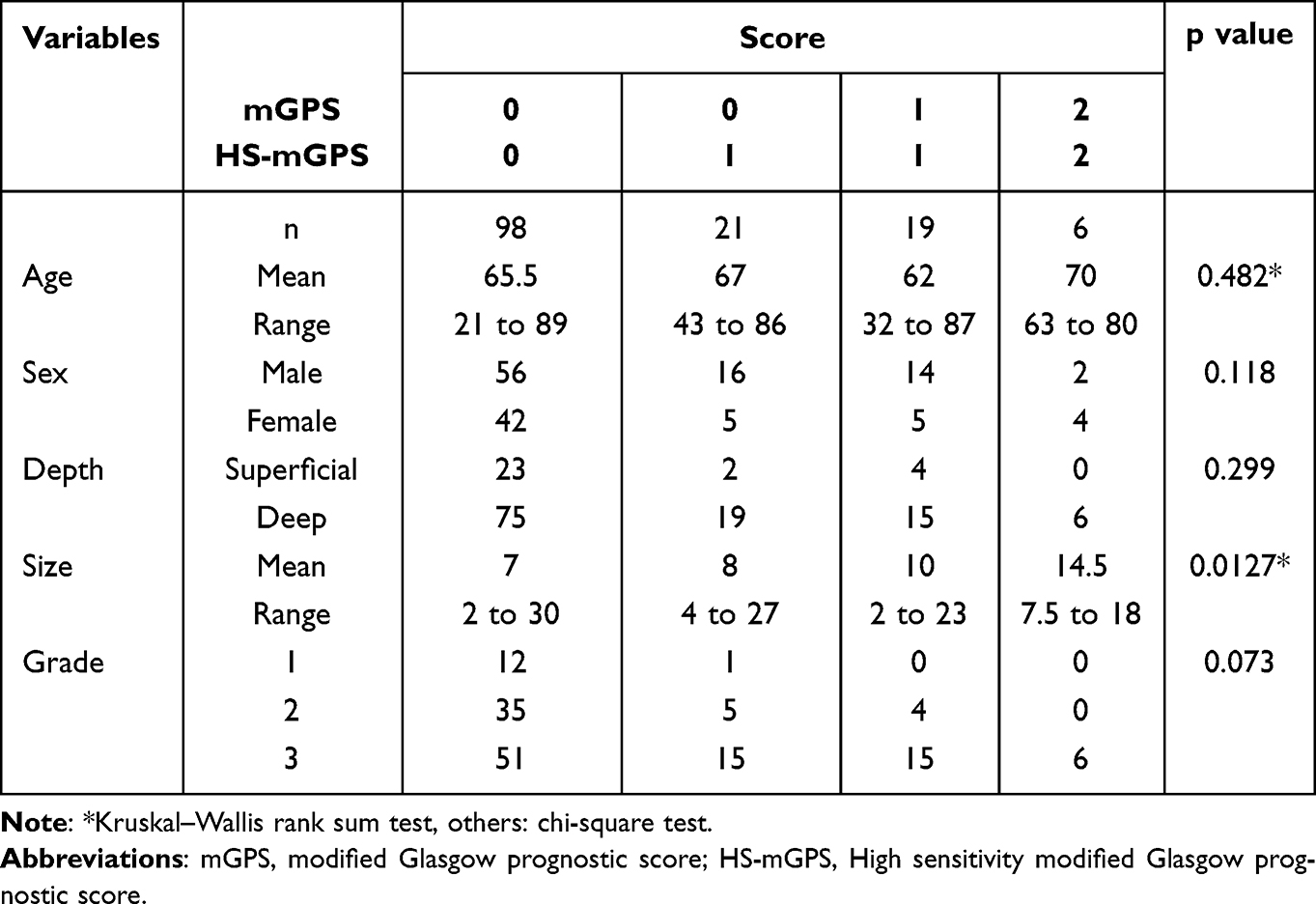 |
Table 1 The Relationship Between mGPS, HS-mGPS and Clinical Date |
Disease-Specific Survival and Prognostic Variables
At the final follow-up, 92 patients (63.9%) were alive, while 44 (30.6%) had died of STSs, and 8 (5.5%) had died of other causes. The disease-specific survival (DSS) at five years was 71.5% (95% confidence interval (CI), 62.7–78.6). When patients were divided into three groups according to the HS-mGPS, those with a score of 1 or 2 had a poorer DSS than those with a score of 0 (p = 0.00174 and p < 0.0001, respectively, Log rank test) (Figure 1). The 5-year DSS rates were 82.7% (95% CI, 72.9–89.3) for those with a score of 0, compared with 51.6% (95% CI, 33.6–67) and 28.6% (95% CI, 4.1–61.2), respectively, for those with scores of 1 and 2. There was a marginally significant difference in the prognosis between patients with scores of 1 and 2 (p = 0.0592, Log rank test). Next, when the patients were divided into three groups according to the mGPS, those with a score of 1 or 2 had a poorer DSS than those with a score of 0 (p < 0.0001 and p < 0.0001, respectively, Log rank test). There was no significant difference in the prognosis between patients with scores of 1 and 2 (p = 0.185, Log rank test) (Figure 2). Finally, when we compared the survival rate among the 98 patients with both HS-mGPS and mGPS of 0 and 21 patients with HS-mGPS of 1 and mGPS of 0, there was no significant difference in the prognosis (p = 0.402, Log rank test) (Figure 3). Patients with an mGPS of 1 or 2 had a poorer DSS than the 98 patients with both HS-mGPS and mGPS of 0 (p < 0.0001 and p < 0.0001, respectively, Log rank test), and 21 patients with HS-mGPS of 1 and mGPS of 0 (p = 0.0336 and p < 0.0001, respectively, Log rank test). In univariate analysis, larger tumour size, grade 3 STSs, and higher mGPS were independent prognostic variables for predicting DSS. In multivariate analysis, larger tumour size and higher mGPS remained significant (Table 2).
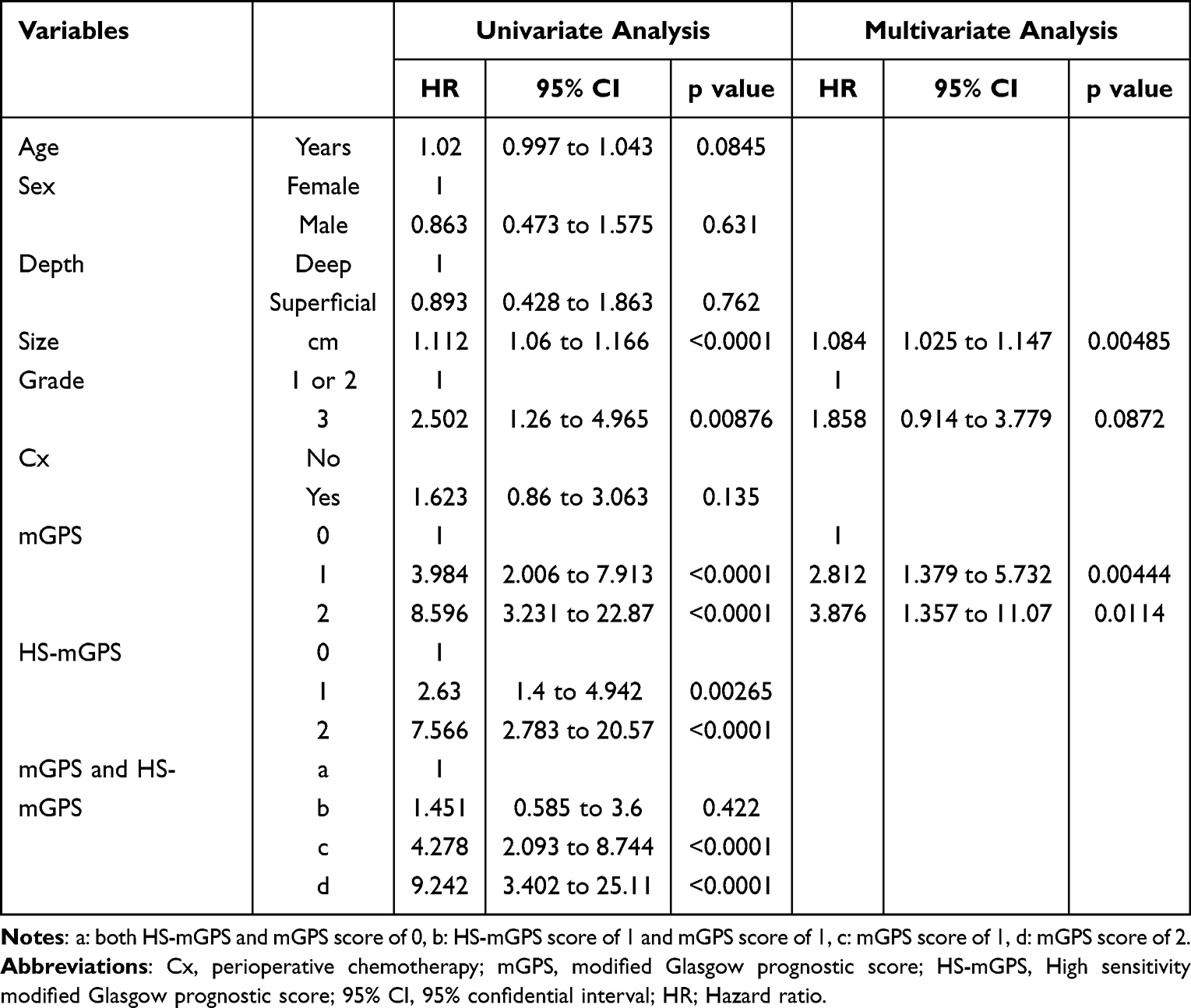 |
Table 2 The Prognostic Factors for Disease Specific Survival in 144 Patients |
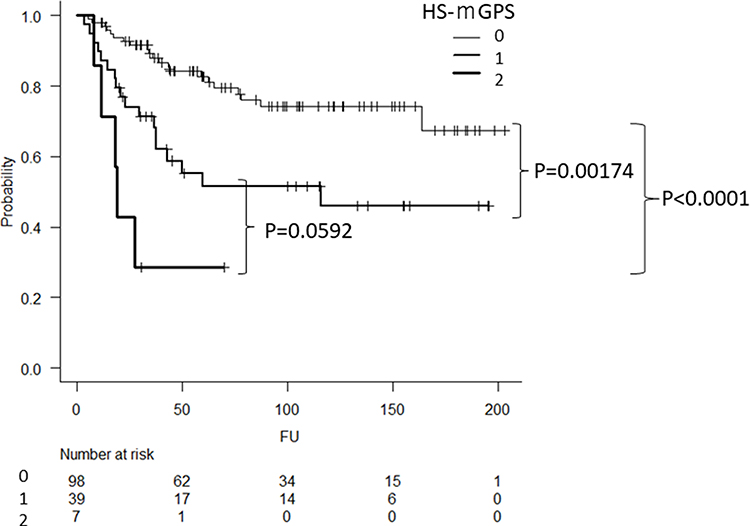 |
Figure 1 Kaplan-Meier curve showing the disease-specific survival according to the HS-mGPS score. |
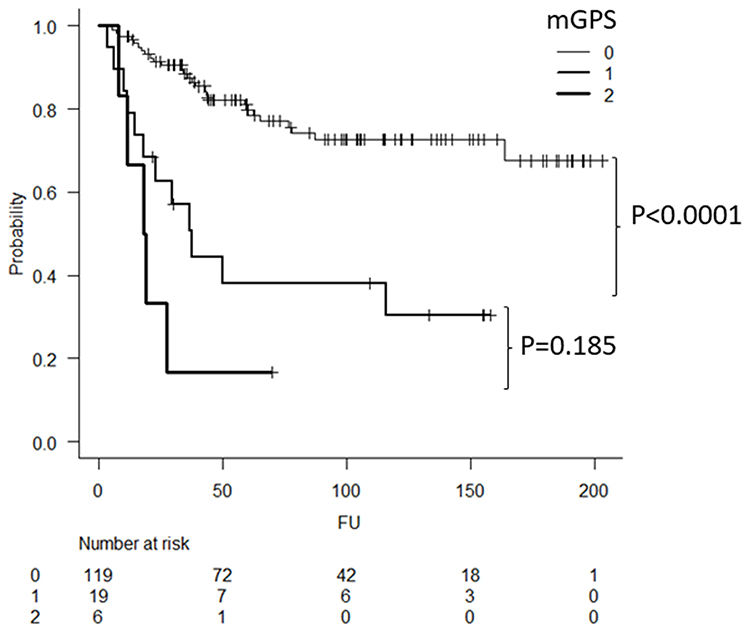 |
Figure 2 Kaplan-Meier curve showing the disease-specific survival according to the mGPS score. |
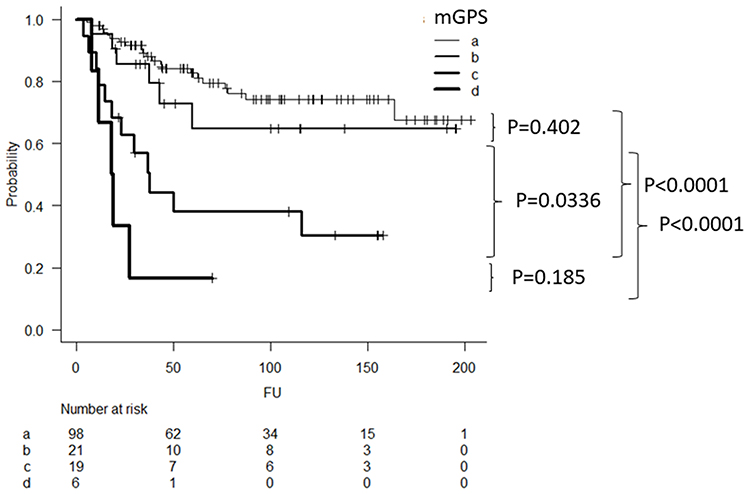 |
Figure 3 Kaplan-Meier curve showing disease specific survival. (a: patients who had both HS-mGPS and mGPS score of 0, b: patients who had HS-mGPS score of 1 and mGPS score of 1, c: patients who had mGPS score of 1, d: patients who had mGPS score of 2). |
Disease-Free Survival and Prognostic Variables
As an initial relapse, a total of 30 patients (20.8%) developed local recurrence. A total of 46 patients (31.9%) developed metastases. The disease-free survival (DFS) rate at 5 years was 53.6% (95% CI, 45–61.6). When the patients were divided into three groups according to the HS-mGPS, those with a score of 1 or 2 had a poorer DFS than those with a score of 0 (p = 0.00314, p < 0.0001, respectively, Log rank test) (Figure 4). The 5-year DFS rate was 63.7% (95% CI, 53–72.6) for those with a score of 0, compared with 35.9% (95% CI, 21.4–50.6) and not reached for those with scores of 1 and 2. There was no significant difference in the prognosis between patients with scores of 1 and 2 (p = 0.0835, Log rank test). Next, when patients were divided into three groups according to the mGPS, those with a score of 1 or 2 had a poorer DFS than those with a score of 0 (p < 0.0001 and p < 0.0001, respectively, Log rank test). There was no significant difference in the prognosis between patients with scores of 1 and 2 (p = 0.135, Log rank test) (Figure 5). The 5-year DFS rate was 62.5% (95% CI, 52.9–70.7) for those with a score of 0, compared with 15.8% (95% CI, 3.92–34.9) and not reached, respectively, for those with a score of 1 and 2. Finally, when we compared survival among the 98 patients with HS-mGPS and mGPS of 0 and 21 patients with HS-mGPS of 1 and mGPS of 0, there was no significant difference in the prognosis (p = 0.859, Log rank test) (Figure 6). Patients with an mGPS of 1 or 2 had a poorer DSS than the 98 patients with both HS-mGPS and mGPS of 0 (p < 0.0001 and p < 0.0001, respectively, Log rank test), and 21 patients with HS-mGPS of 1 and mGPS of 0 (p = 0.00263 and p < 0.0001, respectively, Log rank test) (Figure 6). In univariate analysis, larger tumour size, higher age, grade 3 STSs, and higher mGPS were independent prognostic variables for predicting DSS. In the multivariate analysis, all the variables remained significant (Table 3).
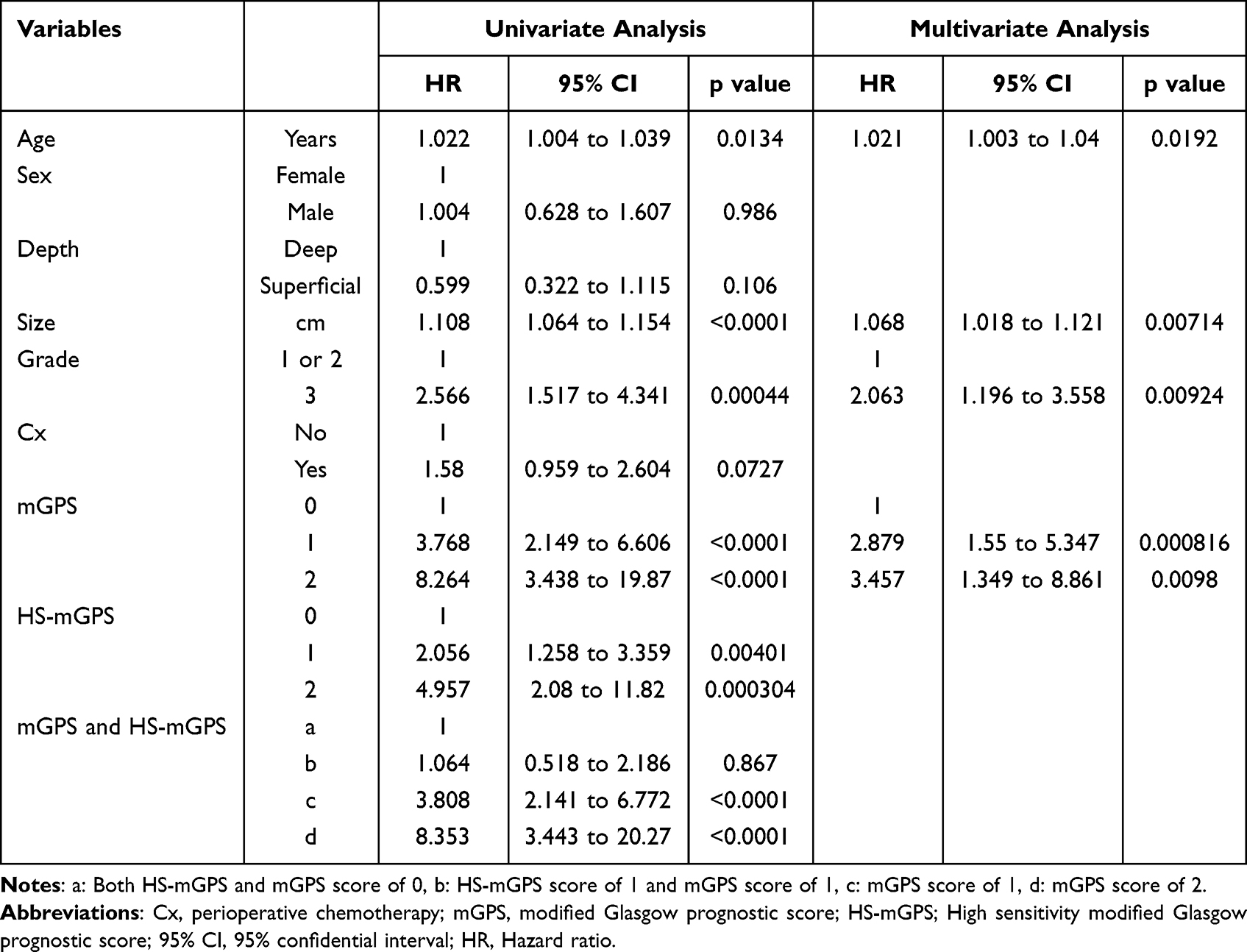 |
Table 3 The Prognostic Factors for Disease-Free Survival in 144 Patients |
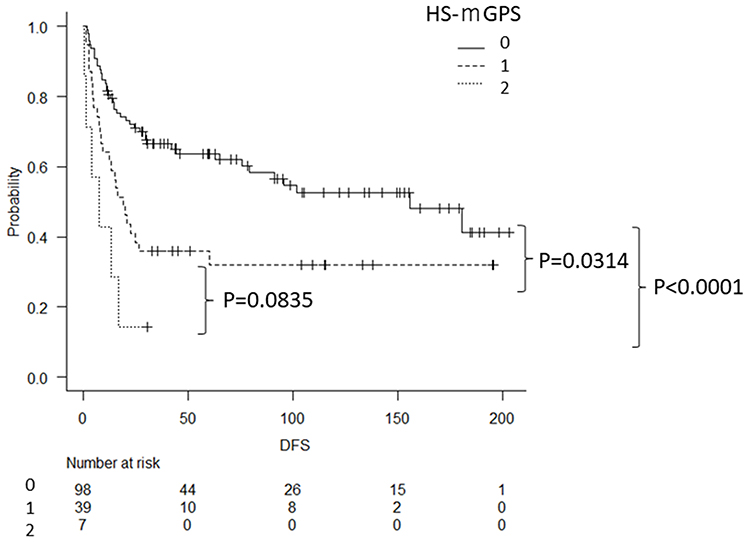 |
Figure 4 Kaplan-Meier curve showing the disease-free survival according to the HS-mGPS score. |
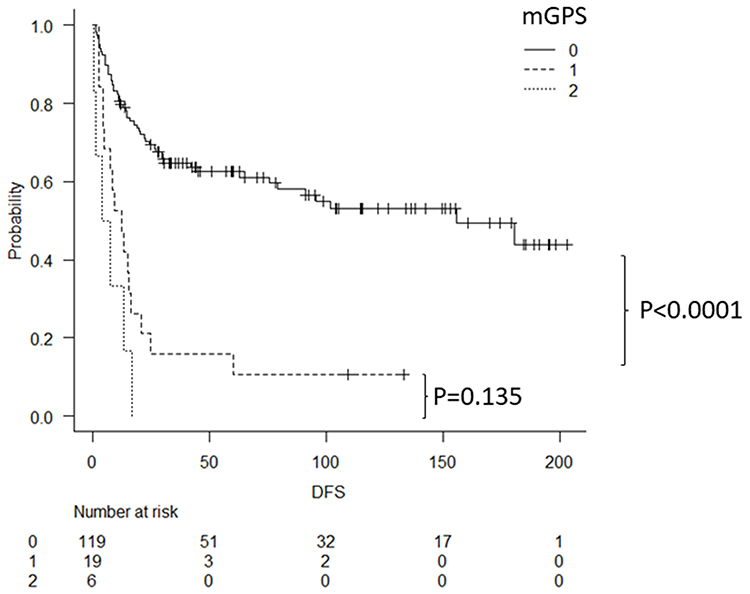 |
Figure 5 Kaplan-Meier curve showing the disease-free survival according to the mGPS score. |
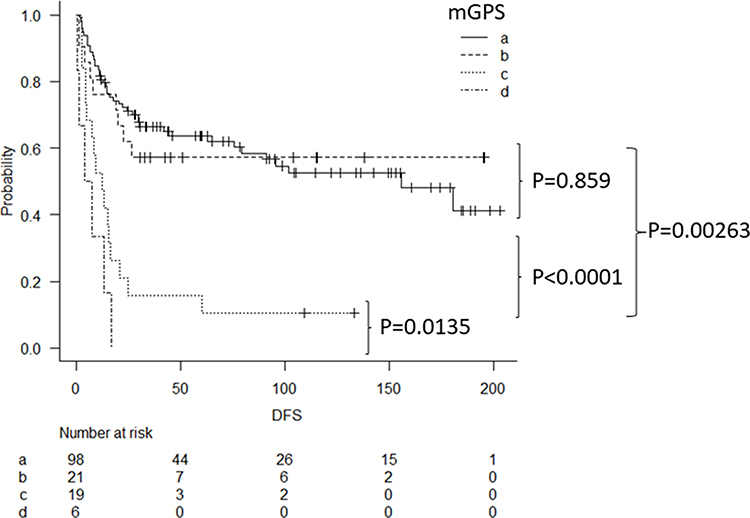 |
Figure 6 Kaplan-Meier curve showing disease-free survival. (a: patients who had both HS-mGPS and mGPS score of 0, b: patients who had HS-mGPS score of 1 and mGPS score of 1, c: patients who had mGPS score of 1, d: patients who had mGPS score of 2). |
Discussion
The association between systemic inflammation and poor prognosis has previously been reported in patients with STSs.10–14 In the cancer microenvironment, inflammation contributes to the promotion of cancer cell proliferation, invasion, and metastatic spread.3,4 As a systemic inflammation marker, CRP is a reliable marker for predicting oncological outcomes in several cancers, including STS.12–15 Additionally, serum albumin levels are a leading indicator of nutritional status, and serum albumin levels likely decrease secondarily to a systemic inflammatory response.5,6,16 GPS or mGPS has been shown to provide additional prognostic information in patients with several types of cancers.7,8 However, the ability of mGPS to predict poor prognoses is restricted because only a few patients show abnormal mGPS when a CRP cut-off value of 1.0 mg/dl is used. Therefore, subsequent studies further refined mGPS to HS-mGPS using a lower threshold for CRP to enhance the predictive ability of inflammation-based prognostic systems in cancer patients.9–11,17,18 When a lower cut-off value for CRP in the HS-mGPS scoring system was used, the number of patients with abnormal scores increased. In this study, 46 patients (31.9%) had HS-mGPS of 1 or 2, although only 25 (17.4%) had an mGPS of 1 or 2. Hou et al reported that the HS-mGPS was an independent predictor of survival in 454 patients with STSs.11 In their cohort, only 77 (17%) patients had an mGPS of 1 or 2. However, when the HS-mGPS was used, 152 patients (33.5%) had HS-mGPS of 1 or 2. They used HS-mGPS for further analysis to elucidate the prognostic variables due to the small number of patients with abnormal mGPS scores. Nakamura et al reported that only 31 of 139 patients (22.3%) with STSs had HS-mGPS of 1 or 2, and they concluded that HS-mGPS was a useful scoring system for predicting oncological outcomes.10 In this study, we also found that HS-mGPS is a useful scoring system for predicting DSS and DFS. However, we wondered if patients with low abnormal levels of CRP (HS-mGPS of 1 and mGPS of 0) had poor oncological outcomes; we found that these patients did not have poorer DSS and DFS than those with normal CRP levels. These results suggest that mGPS may be a better predictor of survival and relapse than HS-mGPS in patients with STSs who underwent primary surgical tumour resection. We emphasise that patients with an mGPS of 1 or 2 are at risk of relapse and death. Recently, Spence et al reported that prognosis of localized STS strongly correlates with mGPS, as an increasing score was associated with a poorer outcome at international multicentre study.19 Although there were no reports comparing mGPS and HS-mGPS, mGPS may become a common tool for predicting survival in patients with STS. We also found that tumour size, tumour histological grade, and age were related to survival and/or relapse. When patients have an mGPS of 0, the variables that have been reported as prognostic variables should be taken into consideration during the follow-up after surgery.20
This study has some limitations. First, we focused on the preoperative assessment of the scoring system and its derivatives, without evaluating the postoperative changes. Second, although all patients had pretreatment staging with CT scans of the chest and routine blood tests to rule out the presence of metastases or inflammatory disease, other chronic conditions were not taken into consideration because of the lack of information. Third, we cannot focus the individual histology due to the limitation of the number of this study. Finally, the retrospective nature of the study is another limitation. However, we believe that mGPS is a reliable system for identifying patients at high risk for death and relapse in patients with STSs.
Ethics
This study was approved by the institutional review boards of the authors’ affiliated institutions (1310).
Disclosure
The authors report no conflicts of interest in this study.
References
1. Clark MA, Fisher C, Judson I, Thomas JM. Soft-tissue sarcomas in adults. N Engl J Med. 2005;353:701–711. doi:10.1056/NEJMra041866
2. Nakamura T, Asanuma K, Takao M, et al. Clinical outcome in patients with soft tissue sarcoma who received metastasectomy and/or radiofrequency ablation: Tokai Musculoskeletal Oncology Consortium study. Cancer Manag Res. 2021;13:8473–8480. doi:10.2147/CMAR.S333721
3. Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflammation. Nature. 2008;454(7203):436–444. doi:10.1038/nature0720
4. Diakos CI, Charles KA, McMillan DC, Clarke SJ. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014;15(11):e493–e503. doi:10.1016/S1470-2045(14)70263-3
5. Baracos VE, Martin L, Korc M, et al. Cancer-associated cachexia. Nat Rev Dis Primers. 2018;4(1):17105. doi:10.1038/nrdp.2017.105
6. Eckart A, Struja T, Kutz A, et al. Relationship of nutritional status, inflammation, and serum albumin levels during acute illness: a Prospective Study. Am J Med. 2020;133(6):713–722.e7. doi:10.1016/j.amjmed.2019.10.031
7. Forrest LM, McMillan DC, McArdle CS, et al. Evaluation of cumulative prognostic scores based on the systemic inflammatory response in patients with inoperable non-small-cell lung cancer. Br J Cancer. 2003;89(6):1028–1030. doi:10.1038/sj.bjc.6601242
8. McMillan DC, Crozier JE, Canna K, et al. Evaluation of an inflammation-based prognostic score (GPS) in patients undergoing resection for colon and rectal cancer. Int J Colorectal Dis. 2007;22(8):881–886. doi:10.1007/s00384-006-0259-6
9. Takeno S, Hashimoto T, Shibata R, et al. The high-sensitivity modified Glasgow prognostic score is superior to the modified Glasgow prognostic score as a prognostic predictor in patients with resectable gastric cancer. Oncology. 2014;87(4):205–214. doi:10.1159/000362601
10. Nakamura T, Matsumine A, Asanuma K, et al. The value of high-sensitivity modified Glasgow prognostic score in predicting the survival of patients with a soft-tissue sarcoma. Bone Joint J. 2015;97-B(6):847–852. doi:10.1302/0301-620X.97B.35098
11. Hou T, Guo T, Nie R, et al. The prognostic role of the preoperative systemic immune-inflammation index and high-sensitivity modified Glasgow prognostic score in patients after radical operation for soft tissue sarcoma. Eur J Surg Oncol. 2020;46(8):1496–1502. doi:10.1016/j.ejso.2020.05.026
12. Nakamura T, Matsumine A, Matsubara T, et al. Clinical significance of pretreatment serum C-reactive protein level in soft tissue sarcoma. Cancer. 2012;118(4):1055–1061. doi:10.1002/cncr.26353
13. Nakamura T, Grimer R, Gaston C, et al. The value of C-reactive protein and comorbidity in predicting survival of patients with high grade soft tissue sarcoma. Eur J Cancer. 2013;49(2):377–385. doi:10.1016/j.ejca.2012.09.004
14. Wang X, Liu S, Zhao X, et al. The value of C-reactive protein as an independent prognostic indicator for disease-specific survival in patients with soft tissue sarcoma: a meta-analysis. PLoS One. 2019;14(7):e0219215. doi:10.1371/journal.pone.0219215
15. Errani C, Cosentino M, Ciani G, et al. C-reactive protein and tumour diagnosis predict survival in patients treated surgically for long bone metastases. Int Orthop. 2021;45(5):1337–1346. doi:10.1007/s00264-020-04921-2
16. McMillan DC, Watson WS, O’Gorman P, et al. Albumin concentrations are primarily determined by the body cell mass and the systemic inflammatory response in cancer patients with weight loss. Nutr Cancer. 2001;39(2):210–213. doi:10.1207/S15327914nc392_8
17. Hirahara N, Matsubara T, Kaji S, et al. Glasgow prognostic score is a better predictor of the long-term survival in patients with gastric cancer, compared to the modified Glasgow prognostic score or high-sensitivity modified Glasgow prognostic score. Oncotarget. 2020;11(45):4169–4177. doi:10.18632/oncotarget.27796
18. Ando K, Sakamoto S, Saito S, et al. Prognostic value of high-sensitivity modified Glasgow prognostic score in castration-resistant prostate cancer patients who received docetaxel. Cancers. 2021;13(4):773. doi:10.3390/cancers13040773
19. Spense S, Doonan J, Farhan-Alanie OM, et al. Does the modified Glasgow prognostic score aid in the management of patients undergoing surgery for soft-tissue sarcoma?: An international multicentre study. Bone Joint J. 2022;104-B(1):168–176. doi:10.1302/0301-620X.104B1.BJJ-2021-0874.R1
20. Callegaro D, Miceli R, Bonvalot S, et al. Development and external validation of two nomograms to predict overall survival and occurrence of distant metastases in adults after surgical resection of localised soft-tissue sarcomas of the extremities: a retrospective analysis. Lancet Oncol. 2016;17(5):671–680. doi:10.1016/S1470-2045(16)00010-3
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Role of Albumin in the Diagnosis of Neonatal Sepsis Over the Last 11 Years: A Retrospective Study
Shi J, Lu ZQ, Lin QM, Zeng W, Gu PJ, Yu Q, Long J, Huang DG, Dai YH
Journal of Inflammation Research 2023, 16:2855-2863
Published Date: 19 July 2023
Prognostic Significance of C-Reactive Protein to Albumin Ratio in Predicting Long-Term Mortality Among Patients with Acute Heart Failure
Zuo R, Zhang J, Liu Q, Jia N
Journal of Inflammation Research 2025, 18:15501-15510
Published Date: 4 November 2025
Clinical Prognostic Value of C-Reactive Protein-Albumin-Lymphocyte Index (CALLY) in Patients with Stage III Breast Cancer
Zhu M, Cheng R, Zhang K, Yue C, Guan S, Chen L, Wang J, Wang Y, Zhang B
Breast Cancer: Targets and Therapy 2025, 17:1293-1305
Published Date: 22 December 2025
The Association Between C-Reactive Protein-to-Albumin Ratio and in-Hospital Mortality in Patients with Klebsiella pneumoniae Bloodstream Infection: A Retrospective Cohort Study
Huang Y, Ao T, Hu M, Zhen P
Journal of Inflammation Research 2026, 19:588368
Published Date: 22 April 2026