Back to Journals » Cancer Management and Research » Volume 17

Modified Glasgow Prognostic Score Incorporating CRP/Albumin Ratio and LDH Levels as Prognostic Indicators in Patients with Multiple Myeloma: A Retrospective Study
Authors Duran M ![]() , Begendi NK
, Begendi NK ![]()
Received 16 May 2025
Accepted for publication 9 September 2025
Published 16 September 2025 Volume 2025:17 Pages 2009—2021
DOI https://doi.org/10.2147/CMAR.S540819
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Harikrishna Nakshatri
Mustafa Duran, Nermin Keni Begendi
Department of Internal Medicine, Division of Hematology, Afyonkarahisar Health Sciences University, Afyonkarahisar, Türkiye
Correspondence: Mustafa Duran, Department of Internal Medicine, Division of Hematology, Afyonkarahisar Health Sciences University, Afyonkarahisar, Türkiye, Email [email protected]
Purpose: This study aimed to evaluate whether integrating the CRP/Albumin Ratio (CAR) and Lactate Dehydrogenase (LDH) levels into the Modified Glasgow Prognostic Score (mGPS) enhances its prognostic accuracy in patients with multiple myeloma (MM).
Patients and Methods: A single-center retrospective study was conducted on patients diagnosed with multiple myeloma (MM) at Afyonkarahisar Health Sciences University between 2017 and 2023. Demographic, clinical, and laboratory data including mGPS, CAR, LDH, and ISS staging were collected. Survival outcomes were assessed using Kaplan-Meier curves, and Cox regression models were used to determine prognostic factors.
Results: Among the 130 patients, the ISS score was the strongest predictor of mortality (HR = 1.63, 95% CI: 1.27– 2.09, p = 0.0001). mGPS 2 combined with LDH > 250 IU (HR = 1.96, 95% CI: 1.32– 2.92) and CAR > 0.51 (HR = 1.71, 95% CI: 1.16– 2.53) were independent risk factors. mGPS alone remained a consistent prognostic marker (HR = 1.42, 95% CI: 1.14– 1.77). One-year survival was 50.0% in the mGPS 2 group, dropping to 30.3% at two years. The mGPS 2 + LDH > 250 IU group had the poorest survival (39.5% to 23.3%), followed by the mGPS 2 + CAR > 0.51 group (44.9% to 28.6%). Median PFS was 28.0, 47.0, and 9.0 months in mGPS0, mGPS1, and mGPS2, respectively (p < 0.001), with mGPS2 showing significantly shorter PFS. mGPS2, CAR, LDH, and their combinations were independent predictors of progression. In mGPS2, OS and PFS declined steadily over 36 months, with the lowest long term PFS in the CAR elevated subgroup.
Conclusion: Integrating CAR and LDH into the mGPS offers a cost-effective and accessible approach to improve risk stratification in patients with MM. This enhanced model provides a comprehensive assessment of systemic inflammation and tumour burden, supporting its potential use in clinical decision making.
Keywords: modified Glasgow prognostic score, CRP/albumin ratio, lactate dehydrogenase, multiple myeloma
Introduction
Multiple myeloma (MM) is a haematological malignancy characterised by clonal proliferation of abnormal plasma cells in the bone marrow and extramedullary tissues, leading to various complications. Epidemiologically, MM accounts for approximately 1% of all cancers and 10% of haematological malignancies. In the United States, approximately 35,000 new cases are diagnosed annually, and nearly 13,000 deaths are attributed to the disease. The incidence of MM increases with age and is typically observed in individuals over 60 years old.1 In Turkey, multiple myeloma accounts for approximately 1% of all cancer cases. Among hematologic malignancies, its incidence is estimated to be around 2–3%.2 Mortality was recorded at 4.9 per 100,000 people in 2019, with an average 10-year survival rate of 33%.3
Prognosis in MM varies widely, and accurate risk stratification is essential for guiding treatment decisions. The International Staging System (ISS), and its revised versions (R-ISS and R2-ISS), remain the most widely used prognostic models. While ISS is simple (using beta-2 microglobulin and albumin levels) and widely applicable, R-ISS and R2-ISS require cytogenetic and molecular data (del(17p), t(4;14), t(14;16), 1q21, LDH) that may not be readily available in all clinical settings, particularly in resource limited environments.4 In 2022, the European Myeloma Network (EMN) introduced the Second Revision of the International Staging System (R2-ISS), which incorporates 1q21 gain in addition to the R-ISS criteria. R2-ISS integrates factors such as ISS stage, LDH (lactate dehydrogenase) levels, 1q21 gain, del(17p), and t(4;14), categorising patients into four risk groups and offering a more precise prognosis assessment. According to the report, the median Overall Survival (OS) and Progression-Free Survival (PFS) were found to be 109 and 68 months, respectively, in Stage II, while these values decreased to 37 and 19.9 months in Stage IV.5 The ISS is simple, cost-effective, and can be easily applied to every MM patient, whereas the R-ISS requires genetic analyses available only in advanced centers, making it more expensive and less accessible for all institutions. In the disease process, to improve prognostic prediction using more accessible parameters, various biochemical and inflammatory markers such as CRP, albumin, LDH, and the CRP/albumin ratio (CAR) have been evaluated in both solid and hematologic malignancies. The modified Glasgow Prognostic Score (mGPS), based on CRP and albumin levels, has been shown to predict survival in several cancers. Similarly, elevated LDH and high CAR values have been associated with worse outcomes in MM.6–10
Inflammation is the immune system’s response to harmful agents, initially serving as a protective mechanism but becoming one of the fundamental processes underlying various complications when it progresses uncontrollably. This cascade of responses can trigger numerous biological processes that are involved in the development and progression of cancer. Commonly used clinical biomarkers include CRP, albumin, fibrinogen, ferritin, and IL-6, which are widely utilised for prognostic evaluation of various diseases. The combined use of these markers improves the accuracy of prognostic predictions. One example is the GPS, which evaluates the systemic inflammatory response and nutritional status based on serum CRP and albumin levels and is frequently used in solid organ tumours.11 The mGPS utilises the same parameters as the original GPS but gives greater weight to the inflammatory component. For instance, patients with low albumin levels are still assigned a score of 0 if their CRP level is not elevated. This modification has been shown to better correlate with patient survival. The mGPS was calculated on a scale of 0, 1, or 2 as follows: CRP < 10 mg/L = 0, CRP > 10 mg/L = 1, and CRP > 10 mg/L with albumin < 35 g/L = 2. This studies have shown that in hepatocellular, colon, lung, and other solid organ cancers, patients with a high mGPS score of 2 have lower OS, PFS, and disease-free survival than those with lower mGPS.12–15 In one study, the GPS demonstrated prognostic value in newly diagnosed angioimmunoblastic T-cell lymphoma (AITL) patients, showing that those with higher scores were associated with worse survival, suggesting that GPS could serve as an independent prognostic factor in AITL patients.16 Additionally, in two multicenter studies, the impact of GPS at the time of diagnosis on survival in MM patients was evaluated, and it was found that patients with higher GPS scores had significantly lower OS and PFS values.17,18
Elevated LDH levels are indicative of an aggressive disease course and poorer outcomes. The prognostic significance of LDH lies in its role in tumour cell metabolism and cellular degradation. Empirical evidence has shown that the LDH concentration correlates with disease severity and cellular proliferation in MM. Increased LDH levels were associated with shorter OS and reduced treatment efficacy. Numerous studies have established that incorporating LDH into prognostic models enhances the accuracy of long-term survival prediction. This is particularly important in multifactorial risk assessment tools, such as the R-ISS, which improve prognostic accuracy and predictive capability.19,20
The CAR is a biomarker used to evaluate inflammatory processes in the body. Increased CRP and decreased albumin levels, which are considered acute-phase reactants, indicate the severity of inflammation and allow for the assessment of nutritional status. Although there are no definitive reference values, a CAR of generally between 0.5 and 1 is considered normal. A ratio >1 indicates high inflammation, while a ratio <0.5 suggests a lower inflammatory process.21,22 The prognostic significance of this ratio has been demonstrated, particularly in haematologic and solid organ cancers. Studies have shown that low ratios provide statistically significant advantages in OS and PFS in patients with acute myeloid leukemia (AML), MM, and myelofibrosis.23–25
Inflammation-based scores like mGPS, CAR, and LDH retain prognostic value independently of molecular profiling. Moreover, previous studies have not adequately assessed the combined utility of these markers in MM. Therefore, this study aims to evaluate the prognostic significance of mGPS in combination with CAR and LDH in MM patients, using data obtainable without advanced genetic testing. This approach could provide a more accessible and cost-effective risk stratification tool, especially for use in centers lacking molecular diagnostics.
Materials and Methods
This retrospective study included patients diagnosed with multiple myeloma at Afyonkarahisar Health Sciences University Faculty of Medicine Hospital, Department of Hematology between 2017 and 2023. A total of 130 patients were included in the study, of whom 81 were male and 49 were female. Inclusion criteria required a confirmed diagnosis according to the International Myeloma Working Group (IMWG) criteria, and included only patients without other organ malignancies, without rheumatologic diseases, and without signs of infection at the time of evaluation. Complete demographic, clinical, and laboratory data, and demographic variables including age, sex, and OS. Clinical data included the type of monoclonal immunoglobulin (IgG, IgA, or IgM), light chain subtype (kappa or lambda), bone marrow plasma cell infiltration percentage, and biochemical and haematological parameters, such as haemoglobin (Hgb) (g/dL), platelet count (Plt) (109/L), neutrophil count (Neu) (109/L), corrected serum calcium (ca) (mg/dL), serum creatinine (creatinine) (mg/dL), beta-2 microglobulin (β2-mg) (mg/L), LDH (U/L), and CRP (mg/L). Serum albumin levels (g/dL) and ISS stages (I, II, and III) were recorded. Disease-specific markers, including bone lesion presence and extent as determined by radiological imaging and erythrocyte sedimentation rate (ESR; mm/h), were also assessed.
Laboratory parameters were determined using standard clinical laboratory methods. Serum protein electrophoresis and immunofixation were used to identify monoclonal proteins and light chain subtypes. Bone marrow involvement was evaluated using aspirates and biopsy specimens. Imaging modalities such as X-ray, MRI, and PET-CT were employed to identify lytic bone lesions.
The CRP/albumin ratio (CAR) was calculated by dividing the serum CRP level (mg/L) by the serum albumin level (g/L), both obtained from patients’ laboratory data during the initial diagnostic workup for multiple myeloma. CAR was used as an integrated biomarker reflecting systemic inflammation and nutritional status. For statistical analysis, CAR was categorised according to the median value calculated from the study cohort to determine its prognostic relevance.
Patients were initially stratified into three prognostic categories based on the modified Glasgow Prognostic Score (mGPS 0, 1, or 2). Within the high-risk mGPS2 category, additional subgrouping was performed:
- mGPS2 + high CAR—patients with CAR values above the cohort median.
- mGPS2 + elevated LDH—patients with LDH > 250 IU.
Kaplan–Meier survival analysis and Cox proportional hazards regression were then applied to compare progression-free survival (PFS) and overall survival (OS) between these subgroups. This approach aimed to evaluate whether incorporating CAR or LDH into the mGPS2 classification could enhance prognostic stratification and improve the accuracy of survival probability estimation compared with mGPS alone.
The study was approved by the Afyonkarahisar Health Sciences University Faculty of Medicine Ethics Committee 2024/7, and written informed consent was obtained from all participants in accordance with the Declaration of Helsinki.
Modified Glasgow Prognostic Score
mGPS is a widely used inflammation-based prognostic system that incorporates CRP and serum albumin levels. In this scoring system, patients are assigned a score of 0, 1, or 2 based on the following criteria:
mGPS 0: CRP ≤ 10 mg/L, regardless of albumin level
mGPS 1: CRP > 10 mg/L and albumin ≥ 35 g/L
mGPS 2: CRP > 10 mg/L and albumin < 35 g/L
This score reflects both the systemic inflammatory response and the nutritional status of patients. It has been shown to correlate with disease progression and overall survival in various malignancies, including multiple myeloma. In our study, patients were stratified into mGPS groups to evaluate its prognostic significance in relation to CRP/Albumin ratio and LDH levels.
Statistical Analysis
Statistical analysis was performed to evaluate the prognostic significance of the various clinical and biochemical parameters. Descriptive statistics are expressed as mean ± standard deviation (SD) or percentages, as appropriate. Continuous variables between groups were compared using one-way ANOVA or Kruskal–Wallis test, depending on the distribution of the data. Categorical variables were analysed using the chi-square or Fisher’s exact tests. Kaplan-Meier survival analysis was performed to estimate overall survival (OS) across different groups, and the Log rank test was used to compare survival curves. Cox proportional hazards regression models were applied to assess the independent prognostic significance of the mGPS, ISS, CAR, LDH, and combined markers (mGPS + CAR > 0.51, mGPS + LDH > 250 IU). CAR, ROC curve analysis was performed. AUC was calculated to assess the overall discriminative ability of CAR. The optimal cut-off value was identified by maximizing the Youden-J index (J = sensitivity + specificity − 1), which provides the point that best balances sensitivity and specificity. Hazard ratios (HR) with 95% confidence intervals (CI) were calculated to quantify the strength of the associations.
Results
The demographic and clinical characteristics of the patients were analysed based on mGPS groups. A total of 130 patients were included in the study, of whom 81 were male and 49 were female. The demographic and clinical characteristics of the patients were analyzed according to the modified Glasgow Prognostic Score (mGPS) groups. The mean age of the study population was 68.2 ± 10.2 years, with no statistically significant differences between groups (p = 0.329) (Table 1). All patients received VCD, while VRD use was highest in mGPS1 (50%) and lowest in mGPS0 and mGPS2 (~36%). Lenalidomide maintenance was more common in mGPS2 (41.3%) versus mGPS0 and mGPS1 (16.7%). DRD and CRD regimens were also more frequent in mGPS1. ASCT rates were similar across groups (39–44%) (Table 2). Progressive and refractory disease were notably higher in mGPS2 (38.7% and 40%), while stable disease and remission were less frequent compared to lower mGPS categories. Ig G Kappa was the predominant monoclonal protein type (36.4%), followed by Ig G Lambda (21.5%) and Ig A Kappa (13.1%). A statistically significant difference was observed in the kappa-free light chain group (p = 0.029). CRP levels were significantly elevated in the mGPS 2 group (37.22 ± 35.86 mg/dL) compared to the mGPS 0 group (3.96 ± 2.62 mg/dL) (p < 0.001). Albumin levels were significantly lower in the mGPS 2 group (29.66 ± 4.21 g/L) compared to the mGPS 0 group (35.28 ± 7.37 g/L) (p < 0.001). CAR values exhibited significant variation between the groups (p < 0.001). The ISS stage distribution revealed that 57.3% of patients with Stage III disease had significantly poorer outcomes (p < 0.001). Statistically significant differences were observed in LDH, creatinine, calcium, haemoglobin, WBC count, and globulin levels among the subgroups. LDH (303.32 ± 172.70 U/L, p = 0.014) and creatinine (2.09 ± 2.08 mg/dL, p = 0.0076) levels were elevated in the mGPS 2 group, while haemoglobin levels were lower (9.85 ± 1.83 g/dL, p = 0.0110). β-2mg levels were elevated in mGPS 2 patients (14.29 ± 16.50 mg/L, p < 0.001). OS was lowest in the mGPS 2 group, with a mean of 20.67 ± 23.15 months (p = 0.007). These findings underscore the significant impact of the mGPS grouping on disease progression and clinical outcomes (Table 3).
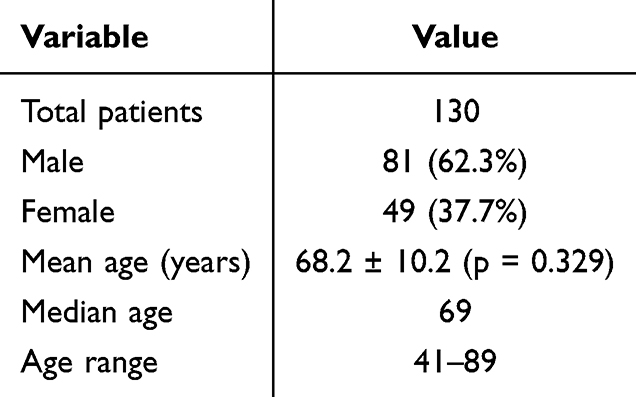 |
Table 1 Demographic Characteristics of the Study Population |
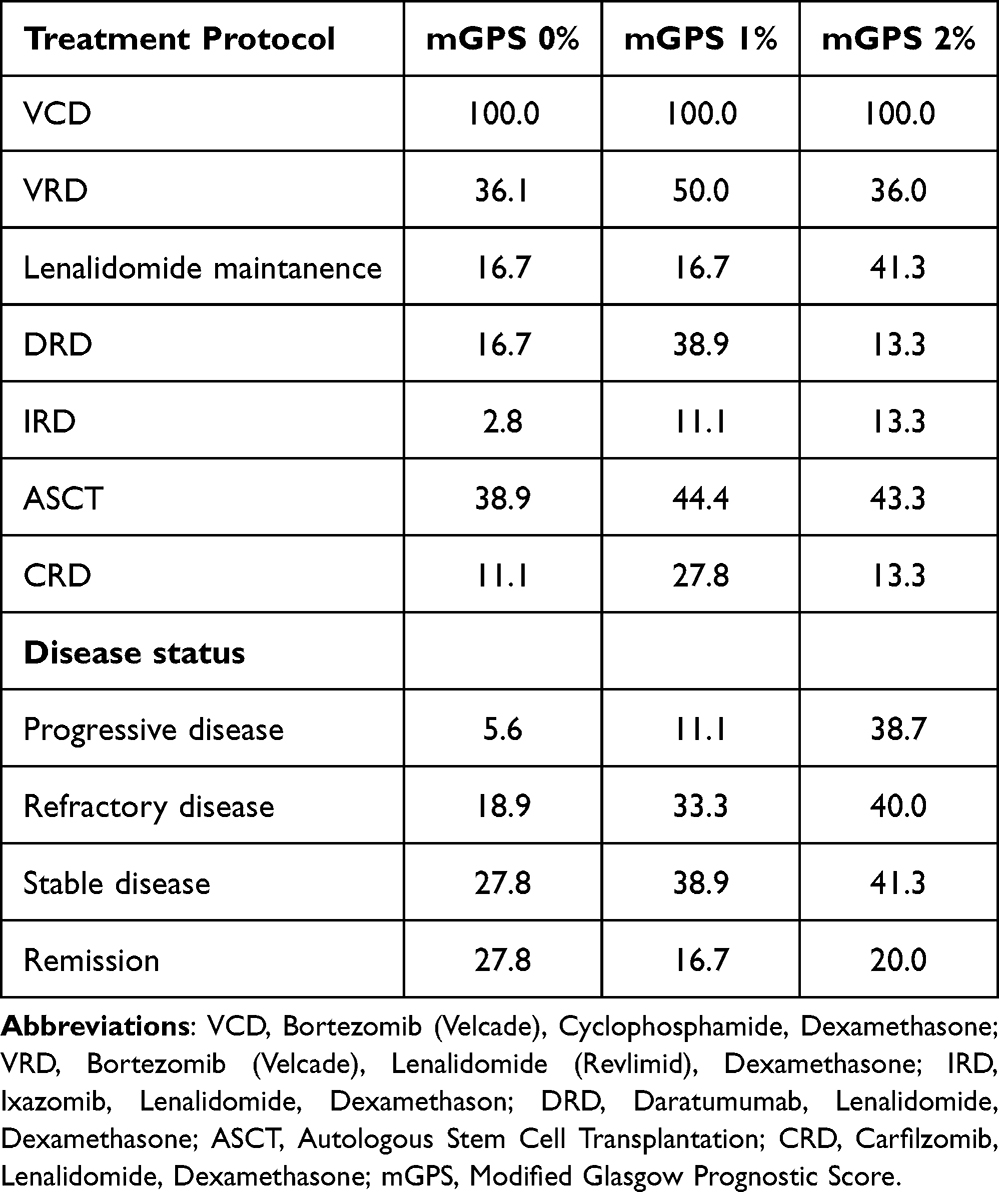 |
Table 2 Distribution of Treatment Protocols and Disease Status Across mGPS Categories |
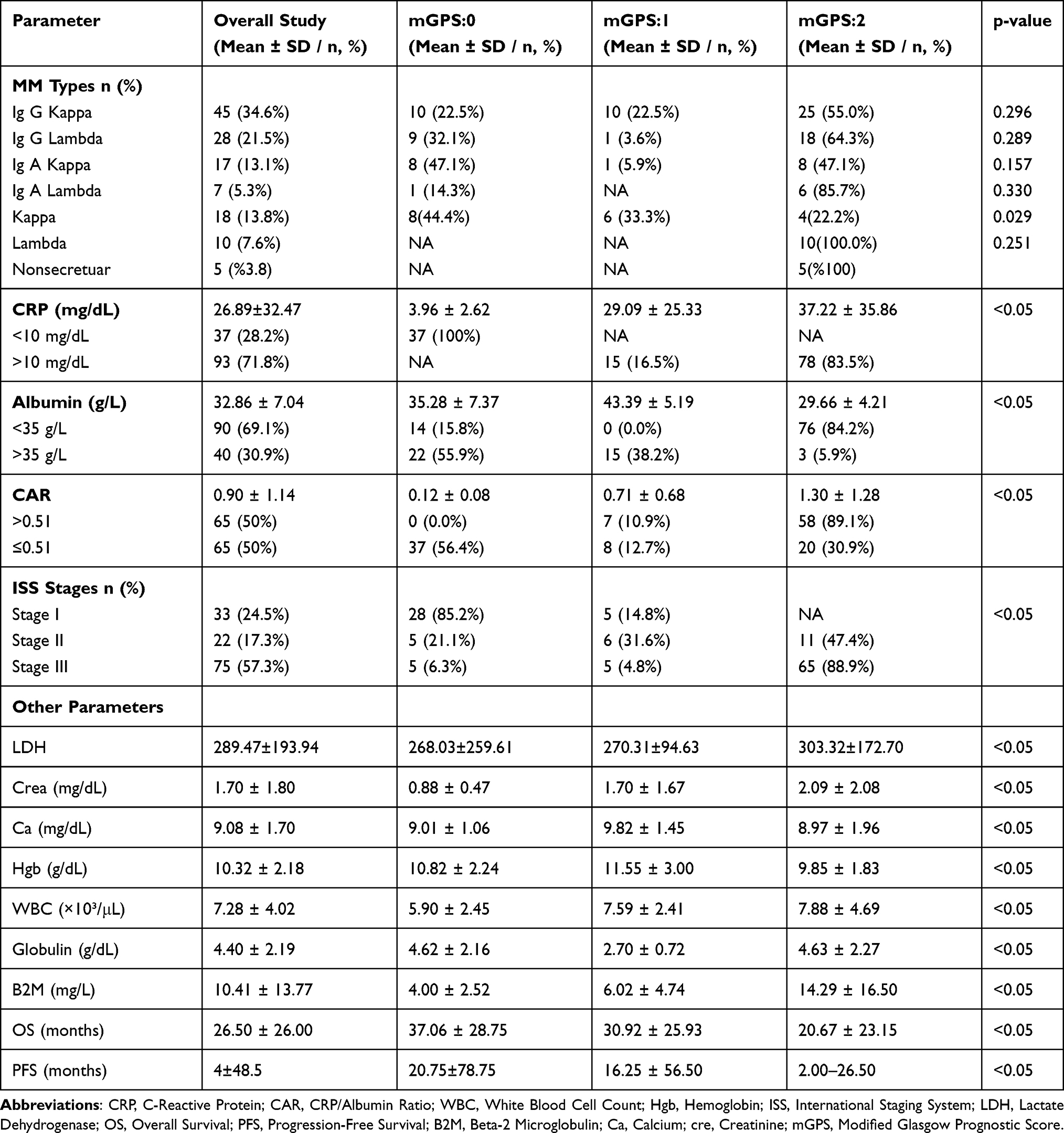 |
Table 3 Clinical and Laboratory Characteristics of the Study Population |
Kaplan-Meier analysis revealed notable findings: 12-month survival was 61.8%, dropping to 40.0% at 24 months and 29.1% at 36 months. The survival curve showed a steady decline that was most significant in the first 24 months. The median OS was 16.5 months, with a maximum follow-up of 91.0 months and mean follow-up of 26.5 months. Median survival times by mGPS were 29.0 months (mGPS 0), 26.0 months (mGPS 1), and 13.0 months (mGPS 2), indicating a significant decrease in survival with higher mGPS scores Median PFS was 18 months in all patients, 47.0 months in MGPS0, 28.0 months in MGPS1, and 9.0 months in MGPS2. Overall differences were significant (Kruskal–Wallis, p < 0.001). MGPS2 had significantly shorter PFS than MGPS0 and MGPS1 (p < 0.001 and p = 0.004, respectively); no difference was found between MGPS0 and MGPS1 (Figures 1 and 2) (p < 0.00)
 |
Figure 1 Survival Outcomes: OS (Overall Survival) and PFS (Progression-Free Survival) Kaplan–Meier Curves for the Study Populations. |
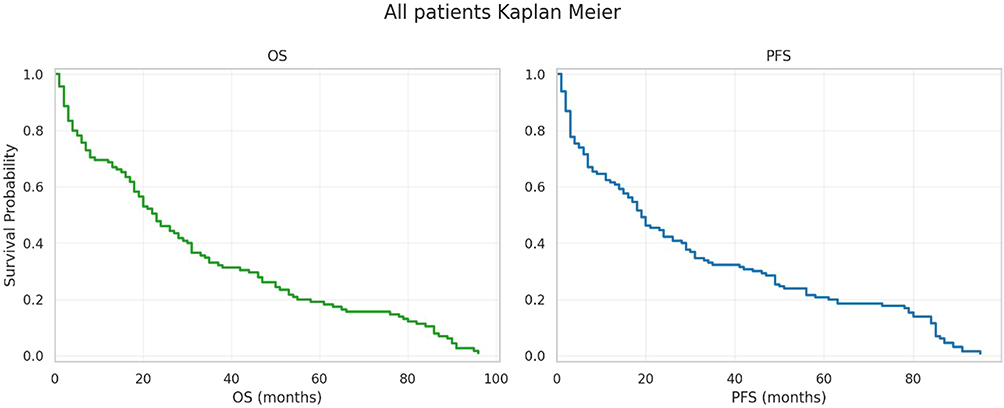 |
Figure 2 OS (Overall Survival) and PFS (Progression Free Survival) Kaplan Meier analysis by mGPS 0, 1, 2 group. |
The mGPS scoring system was enhanced with CAR > 0.51 and LDH > 250 IU to improve prognostic accuracy. These markers effectively identified high-risk patients, aiding in better risk stratification and survival prediction. The ISS score was the most significant survival predictor (HR = 1.63, 95% CI: 1.27–2.09, p = 0.0001), with a unit increase linked to a 63% higher mortality risk. mGPS 2 + LDH (HR = 1.96, 95% CI: 1.32–2.92, p = 0.0008) indicated poor survival, especially in patients with mGPS 2 and ROC analysis of CAR yielded an AUC of 0.91, indicating excellent discrimination. The optimal cut-off was 0.51, with 88% sensitivity and 84% specificity (Figure 3). CAR > 0.51, showing a 96% increased mortality risk. mGPS2 + CAR (HR = 1.71, 95% CI: 1.16–2.53, p = 0.0069) was an independent risk factor, with mGPS2 and LDH > 250 IU increasing mortality risk by 71%. mGPS remained a consistent outcome predictor (HR = 1.42, 95% CI: 1.14–1.77, p = 0.0019), with each unit increase linked to a 42% higher mortality risk. Combined markers, especially mGPS2 + LDH improved risk stratification, suggesting that patients with multiple highrisk features may need intensive management. Regular monitoring of these markers is crucial for predicting outcomes and guiding treatment decisions mGPS. For PFS CAR, LDH, and combined markers were significantly associated with increased risk of progression. Specifically, mGPS2 vs mGPS0 had HR 1.77 (95% CI 1.18–2.66, p = 0.006); CAR (per unit) HR 1.19 (95% CI 1.01–1.40, p = 0.038); LDH (per IU) HR 1.001 (95% CI 1.000–1.002, p = 0.046). Combined markers mGPS2 + CAR > 0.51 and mGPS2 + LDH > 250 IU were also significant (HR 2.09, p < 0.001 and HR 1.60, p = 0.010, respectively). These results indicate that patients with mGPS2 and combined high-risk markers had significantly shorter PFS (Table 4).
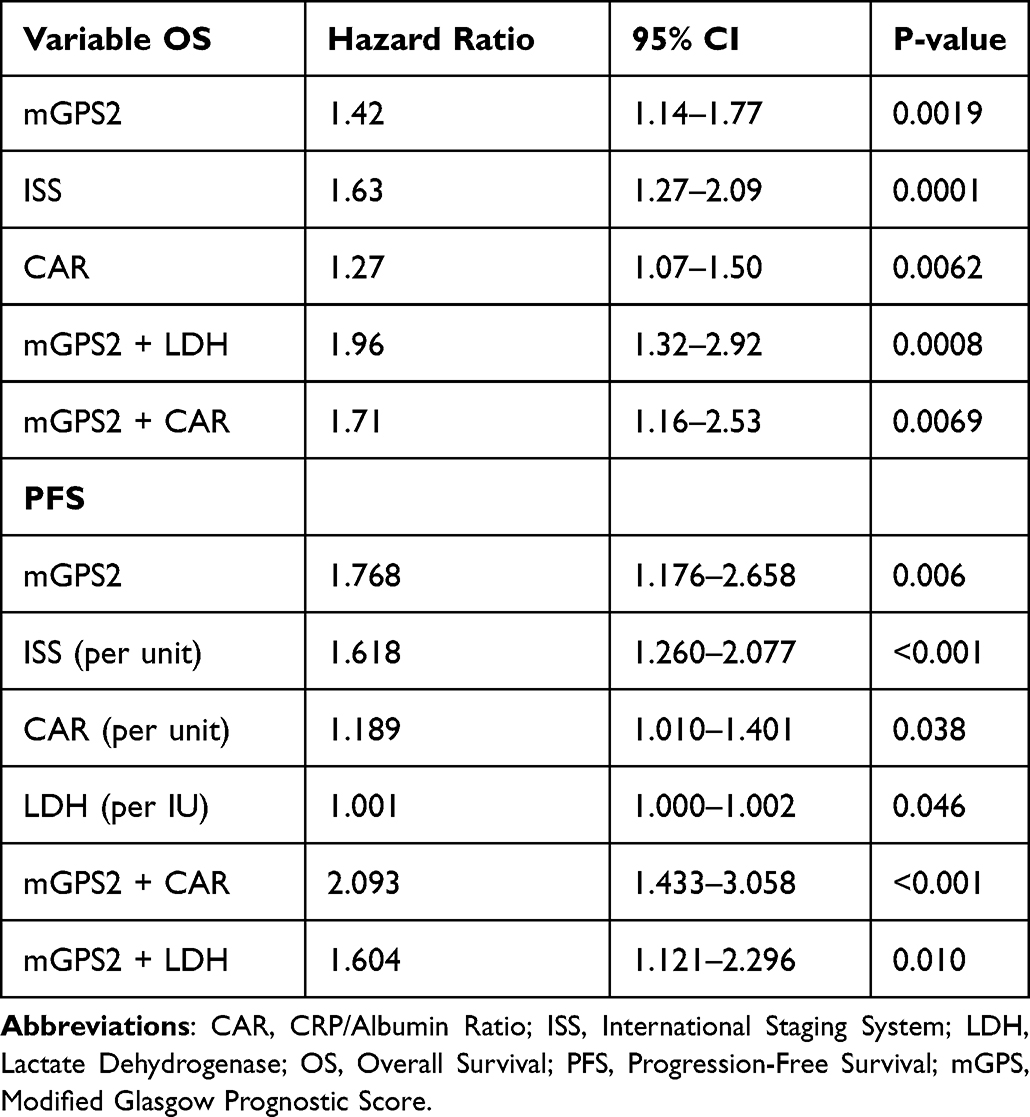 |
Table 4 Analysis Revealed the Prognostic Significance of mGPS, ISS, CAR, LDH, and Combined Markers (mGPS2 + CAR>0.51 and mGPS2 + LDH>250 IU) with OS and PFS |
 |
Figure 3 ROC curve analysis of CAR. |
The Log rank test results show that the comparison between “mGPS2” and “mGPS2 + LDH ≥ 250 IU” is statistically significant (p = 0.0359), with a median survival time 4 months shorter than the mGPS2 alone group. Adding elevated CAR (>0.51) to mGPS2 also indicated a negative impact on survival, although it was less pronounced than LDH elevation. In patients with mGPS2, the median PFS was 9 months (range: 0–89), 7.5 months in the mGPS2 + CAR group (range: 0–84), and 6 months in the mGPS2 + LDH group (range: 0–89), with no statistically significant differences (Figure 4).
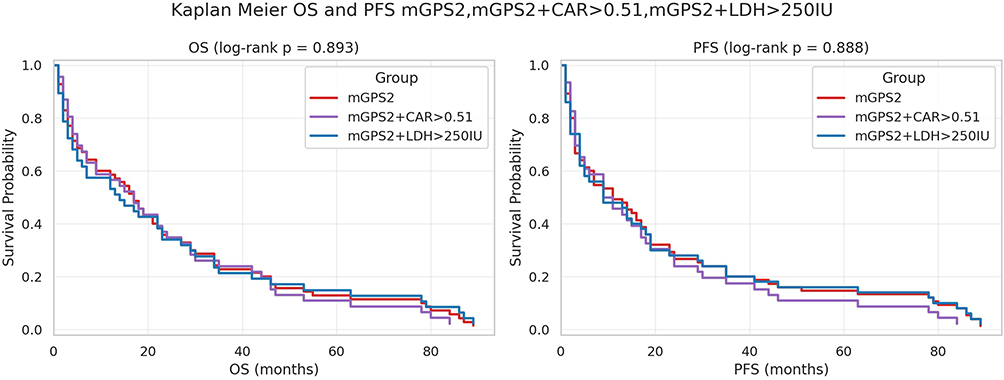 |
Figure 4 Impact of CAR (CRP/Albumin Ratio) and LDH on Survival Probability in Multiple Myeloma Patients: A Comparison of mGPS Models. |
Across all mGPS2 subgroups, both OS and PFS declined from 12 to 36 months. In the overall mGPS2 group, OS decreased from 50% at 12 months to 30.3% at 24 months and 21% at 36 months, while PFS declined from 48% to 25% and 19%. The mGPS2 + CAR > 0.51 subgroup showed OS of 44.9%, 29.6%, and 22% with corresponding PFS of 43%, 22%, and 15%, indicating comparatively lower long-term PFS. The mGPS2 + LDH > 250 subgroup showed OS of 39.5%, 23.5%, and 19% and PFS of 46%, 26%, and 18%. Overall, OS and PFS curves demonstrated progressive attrition through 36 months, with modest subgroup differences: numerically lower OS in the LDH-elevated group and the lowest 36‑month PFS in the CAR-elevated group. (p > 0.05) (Figure 5).
 |
Figure 5 Comparing the 12, 24, and 36 month survival rates across MGPS2, MGPS2 + CAR > 0.51 MGPS2 + LDH > 250 IU. |
Discussion
The role of systemic inflammatory processes in the development and progression of malignancies has become increasingly evident.26 Our study highlights the prognostic significance of inflammatory markers, specifically mGPS, CAR, mGPS + CAR, and mGPS + LDH, in patients with MM. Elevated CRP and reduced albumin levels have been associated with decreased PFS, OS, poor prognosis, high tumour burden, and immunosuppression, significantly reducing survival times.27,28
We found that the demographic, clinical, and biochemical characteristics of patients differed significantly across mGPS subgroups. Of the total 130 patients, 81 (62.3%) were male and 49 (37.7%) were female, with a mean age of 68.2 ± 10.2 years (median 69, range 41–89), and no significant age difference was observed between groups (Table 1) Treatment distribution patterns further underscored the clinical relevance of mGPS. While VCD was universally administered, regimens such as VRD, DRD, and CRD were more frequently used in mGPS1, and lenalidomide maintenance was disproportionately higher in mGPS2 (41.3%), possibly reflecting intensified maintenance strategies for high-risk patients. Nevertheless, progressive and refractory disease rates were highest in mGPS2 (38.7% and 40%, respectively), indicating that these patients were more likely to exhibit treatment resistance regardless of therapy type or intensity. ASCT utilization was comparable across mGPS categories, suggesting that transplant eligibility was not directly influenced by systemic inflammation; however, the inferior survival outcomes in mGPS2 patients despite receiving high intensity regimens highlight the prognostic independence of mGPS from treatment modality (Table 2). Specifically, patients in the mGPS 2 group exhibited significant differences in CRP, albumin, calcium, haemoglobin, platelet count, β2-microglobulin, LDH, and CAR parameters (Table 3). These parameters are well-established indicators of poor clinical outcomes, high tumour burden, and aggressive disease biology, corroborating the findings of previous studies. Our results are consistent with the existing literature, underscoring the validity of mGPS as a prognostic tool for MM.
A meta-analysis revealed a significant correlation between the high-sensitivity modified Glasgow prognostic score (HS-mGPS) and OS in cancer patients. Researchers have suggested lowering the CRP threshold from 10 mg/dL to 3 mg/dL to enhance the sensitivity and prognostic accuracy of HS-mGPS. Establishing an optimal CRP threshold is essential to ensure the effectiveness of this system. In our study, acknowledging minor influences on CRP, we chose to use the 10 mg/dL threshold.29,30
CRP is highly influenced by inflammation and is sensitive to baseline conditions such as patient age, tumour burden, histological features, disease stage, infections, chronic illnesses, medications, smoking, and alcohol consumption, leading to potential inconsistencies in CRP levels. Elevated CRP levels in infections and oncological and rheumatological diseases require careful assessment, particularly in immunosuppressed patients with MM, where infection must be ruled out. Incorporating albumin values in the mGPS and CAR calculations aids in distinguishing these conditions. The combined use of CRP and albumin levels has facilitated the development of prognostic models for MM patients, including CAR, albumin-to-monoclonal protein ratio, prognostic nutritional index, systemic immune-inflammation index, and mGPS.31,32
The mGPS and CAR are preferred because of their cost-effectiveness and ease of application in clinical settings, making them suitable for resource-limited environments. The mGPS is advantageous for rapid calculation and avoidance of delays from cytogenetic testing. By scoring and combining CRP and albumin levels, mGPS, along with CAR or LDH, can be beneficial in routine clinical practice. A study incorporating cytogenetic analyses into the mGPS showed enhanced predictive power for OS and PFS, especially for PFS. In a large study of patients with MM, GPS at diagnosis before autologous HSCT demonstrated significant prognostic value for OS (p < 0.0001) and PFS (p = 0.019), unlike inflammatory markers such as NLR and PLR. GPS is also proven to predict relapse and disease resistance after autologous stem cell transplantation.20
Our findings align with those of the initial seminal study, showing statistically significant differences in decreased OS duration among the MGPS groups (p = 0.007; Figures 1, 2 and 4). Disease stage and biochemical abnormalities significantly affected clinical outcomes. The markedly reduced OS in MGPS Two patients highlighted the need for individualised treatment strategies from the onset of therapy in this high-risk group. To avoid confounding CRP elevations due to infections, patients were evaluated for post-infection resolution, ensuring independent interpretation of the results. Recent studies have underscored the prognostic value of the mGPS in cancer outcomes. The observed survival decline, with a median OS of 16.5 months, reflects advanced malignancy progression, emphasising the need to stratify patients using prognostic markers, such as mGPS. Studies show higher mGPS scores correlate with poorer survival outcomes; for instance, one study reported significantly lower 5-year disease-free survival rates in patients with high mGPS scores compared to those with low scores (36.7% vs 76.6%).33 Similarly, the utility of mGPS in predicting survival in gastrointestinal cancer patients, showing that mGPS effectively stratifies patients into distinct risk categories with significant differences in survival outcomes.34 Our analysis showed an inverse relationship between median survival times and mGPS scores: 29.0 months for mGPS 0, 26.0 months for mGPS 1, and 13.0 months for mGPS 2 (Figure 2). These results highlight the role of systemic inflammation in cancer progression and outcomes, as indicated by mGPS. The Kaplan-Meier curve indicated a sharp decline in survival probabilities within the first 24 months, underscoring the need for early intervention and intensive management for patients with high mGPS scores. The statistically significant p-value (<0.005) across the mGPS groups confirmed the clinical utility of mGPS as a prognostic tool. Enhancing the mGPS with CAR and LDH marks a significant improvement in prognostic assessment, addressing the limitations of mGPS alone. Recent studies have suggested that a combination of inflammatory markers offers more accurate prognostic information.23,35,36
Higher mGPS categories, particularly mGPS2, were associated with significantly shorter progression-free survival, consistent with the established prognostic relevance of systemic inflammation in hematologic malignancies. The markedly reduced median PFS of 9 months in mGPS2 patients, compared with 47 and 28 months in mGPS0 and mGPS1, respectively, underscores the clinical utility of mGPS for risk stratification. In our study, the median CAR value was 0.51 (Table 3 and Figure 3). CAR > 0.51, as a high-risk marker, reflects systemic inflammation and nutritional status, whereas LDH > 250 IU indicates tumour burden and cellular turnover. The statistical significance of the ISS (HR = 1.63, 95% CI: 1.27–2.09, p = 0.0001) supports this enhanced approach (Table 4). The proposed prognostic model integrating CAR (>0.51) and LDH (>250 IU) with the mGPS is novel in oncology. Comparison of the mGPS:2 and mGPS:2 + LDH ≥ 250 IU groups revealed a significant difference in survival probabilities (p = 0.0359; Figure 3), indicating worse prognosis with LDH ≥ 250 IU in mGPS 2 patients. However, comparisons between mGPS:2 and mGPS:2 + CAR > 0.51 (p = 0.3839) and between mGPS:2 + CAR > 0.51 and mGPS:2 + LDH ≥ 250 IU (p = 0.1707) did not achieve statistical significance. Furthermore, the significant associations of CAR and LDH with PFS, both as continuous variables and in combination with mGPS2, suggest that integration of these biomarkers may enhance prognostic precision. Although mGPS2 + CAR > 0.51 and mGPS2 + LDH > 250 IU identified patients with numerically shorter PFS and OS, the lack of statistical significance in subgroup comparisons may reflect limited sample sizes or overlapping biological pathways underlying inflammation, nutritional status, and tumor, suggesting that LDH > 250 IU may indicate a trend towards worse survival without reaching statistical significance burden (Figures 1, 2 and 4). Additionally, when comparing the 1-year,2-year and 3-year survival expectations, the mGPS:2 + LDH group demonstrated a lower 2-year survival expectation than the other groups, although the difference was not statistically significant (Figure 5). Notably, CAR elevation appeared to correspond with the lowest 36-month PFS, whereas LDH elevation tended toward lower OS, indicating potentially distinct prognostic implications of these markers. Overall, our findings support the prognostic value of mGPS in multiple myeloma and suggest that incorporating CAR and LDH may refine risk assessment, warranting validation in larger, prospective cohorts. This lack of significance may be attributed to the limited sample size, characteristics of the patient population, and short 3-year follow-up period in our study. These findings highlight the prognostic importance of LDH levels in mGPS in 2 patients and suggest that LDH could serve as a valuable biomarker for risk stratification in this population. Inspired by the R-ISS, this model aimed to address the limitations of the existing prognostic tools by incorporating both inflammatory and tumour-specific markers. Thus, it offers several advantages, including improved risk stratification, more comprehensive assessment of disease burden, and enhanced survival predictions.
The strong statistical correlation in this model highlights its potential for clinical decision making and treatment planning. For example, options such as potent and highly effective monoclonal or bispecific antibodies can be considered in the selection of first-line treatment. Unlike the traditional mGPS, this enhanced system offers a multidimensional view of patient prognosis by integrating systemic inflammation, nutritional status, and tumour activity. This novel approach has not been explored previously, marking a pioneering effort to develop more accurate prognostic tools. Future research should analyse the survival curves for various marker combinations, compare this model with other prognostic systems using cytogenetic data, and explore its therapeutic implications. This study provides a robust foundation for further research.
Our study was a retrospective, single-centre investigation, with a limited sample size. A larger multicentre prospective study would provide more reliable results. Some patients lack cytogenetic examination data, but exploring the relationship between cytogenetic results and OS/PFS probability rates remains feasible and potentially valuable. The relationship between disease-specific mortality rate, event free survival, mGPS, and CAR could not be established results. Additionally, the other causes of death among the patients were not evaluated, nor were the outcomes of the treatments received. We believe that including a larger number of patients in future studies will yield more accurate and reliable results.
Conclusion
This study emphasised the prognostic value of systemic inflammatory markers, particularly mGPS, CAR, and LDH, in patients with MM. The integration of CAR > 0.51 and LDH > 250 IU with the mGPS provides more comprehensive risk stratification, allowing better prediction of OS and PFS. Our findings confirm the significant role of inflammation, as reflected by CRP and albumin levels, in the progression and outcomes of MM. The enhanced model, combining mGPS with CAR and LDH, addresses some limitations of traditional mGPS by incorporating indicators of tumor burden and systemic inflammation. Although the observed trends in survival outcomes, particularly for mGPS 2 patients with high LDH levels, did not always reach statistical significance, they highlighted the potential of this model for identifying high-risk patients. While ISS remains a strong predictor of survival, integrating mGPS2 with CAR and LDH enhances risk stratification, allowing for more precise identification of high-risk patients who may benefit from intensified treatment approaches. These findings suggest the need for individualized treatment strategies and closer monitoring, especially in resource-limited settings where cost-effective and accessible prognostic tools like mGPS are advantageous. Future studies with larger sample sizes, extended follow-up durations, and comparisons with genetic-based prognostic systems are essential to validate and refine this model. By improving risk stratification, this novel approach can guide treatment decisions, optimise patient management, and ultimately enhance clinical outcomes in patients with MM.
Abbreviations
MM, Multiple Myeloma; IMWG, International Myeloma Working Group; mGPS, Modified Glasgow Prognostic Score; GPS, Glasgow Prognostic Score; CAR, C-reactive Protein to Albumin Ratio; LDH, Lactate Dehydrogenase; CRP, C-reactive Protein; OS, Overall Survival; PFS, Progression-Free Survival; AHSCT, Autologe Hematopoietic Stem Cell Transplantation; R-ISS, Revised International Staging System; NLR, Neutrophil-to-Lymphocyte Ratio; PLR, Platelet-to-Lymphocyte Ratio; β2-M, Beta-2 Microglobulin; CI, Confidence Interval; HR, Hazard Ratio; SD, Standard Deviation.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Rajkumar SV. Multiple myeloma: 2024 update on diagnosis, risk-stratification, and management. Am J Hematol. 2024;99(9):1802–1824. doi:10.1002/ajh.27422
2. Republic of Turkey Ministry of Health, Public Health Directorate, Cancer Department. Turkey cancer statistics 2020. Ankara; 2021. Available from: https://hsgm.saglik.gov.tr/depo/birimler/kanserdb/Dokumanlar/Istatistikler/Turkiye_Kanser_Istatistikleri_2020.pdf.
3. Office for National Statistics. Population estimates for the UK, England and Wales, Scotland and Northern Ireland, provisional: mid-2019.
4. Palumbo A, Avet-Loiseau H, Oliva S, et al. Revised international staging system for multiple myeloma: a report from International Myeloma Working Group. J Clin Oncol. 2015;33(26):2863–2869. doi:10.1200/JCO.2015.61.2267
5. D’Agostino M, Mateos MV, Palumbo A, et al. Second Revision of the International Staging System (R2-ISS) for overall survival in multiple myeloma: a European Myeloma Network (EMN) report within the HARMONY project. J Clin Oncol. 2022;40(26):3406–3418. doi:10.1200/JCO.21.02614
6. Hu X, Dai X, Guo X, et al. Bone marrow fibrosis in newly diagnosed multiple myeloma and its correlation with clinicopathological factors. Diagn Pathol. 2024;19:99. doi:10.1186/s13000-024-01516-y
7. Liu Y, Zhang Z, Lin X, et al. Serum lactate dehydrogenase can be used as a factor for re-evaluating first-relapsed multiple myeloma. Acta Haematol. 2020;143(6):559–566. doi:10.1159/000505737
8. Qian J, Jin J, Luo H, et al. Analysis of clinical characteristics and prognostic factors of multiple myeloma: a retrospective single-center study of 787 cases. Hematology. 2017;22(8):472–476. doi:10.1080/10245332.2017.1309493
9. Mehra K, Ramasamy C, Perkit NR, et al. Significance of neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and monocyte-to-lymphocyte ratio in the prognosis of newly diagnosed multiple myeloma patients. Blood. 2023;142(suppl 1):6695. doi:10.1182/blood-2023-187731
10. Kastritis E, Terpos E, Roussou M, et al. Evaluation of the revised international staging system in an independent cohort of unselected patients with multiple myeloma. Haematologica. 2017;102(3):593–599. doi:10.3324/haematol.2016.145078
11. Pantano NDP, Rocha A, Simões C, et al. Validation of the modified Glasgow prognostic score in advanced cancer patients receiving palliative care. J Pain Symptom Manage. 2021;51(2):270–277. doi:10.1016/j.jpainsymman.2015.09.010
12. Lu L, Lin K, Zheng J, Wu H, Li D. Glasgow prognostic score and modified Glasgow prognostic score and survival in patients with hepatocellular carcinoma: a meta-analysis. BMJ Open. 2021;11(12):e053061. doi:10.1136/bmjopen-2021-053061
13. He L, Li H, Cai J, et al. Prognostic value of the Glasgow prognostic score or modified Glasgow prognostic score for patients with colorectal cancer receiving various treatments: a systematic review and meta-analysis. Cell Physiol Biochem. 2018;51(3):1237–1249. doi:10.1159/000495500
14. Tong T, Guan Y, Xiong H, Wang L, Pang J. A meta-analysis of Glasgow prognostic score and modified Glasgow prognostic score as biomarkers for predicting survival outcome in renal cell carcinoma. Front Oncol. 2020;10:1541. doi:10.3389/fonc.2020.01541
15. Igawa S, Yamamoto H, Yamada K, et al. The Glasgow prognostic score predicts survival outcomes in patients with extensive-stage small cell lung cancer. Oncology. 2023;101(11):695–704. doi:10.1159/000532087
16. Wang H. Glasgow prognostic score predicts prognosis in patients with angioimmunoblastic T-cell lymphoma. Blood. 2020;136(suppl 1):31–32. doi:10.1182/blood-2020-134351
17. Witte HM, Biersack H, Riecke A, et al. The integrated Glasgow prognostic- and cytogenetic risk score (CytoGPS) at diagnosis is a strong and independent predictor of survival in transplant-eligible patients with multiple myeloma. Blood. 2018;132(suppl 1):4509. doi:10.1182/blood-2018-99-117361
18. Witte HM, Bonorden B, Riecke A, et al. The Glasgow prognostic score at diagnosis is a predictor of clinical outcome in patients with multiple myeloma undergoing autologous haematopoietic stem cell transplantation. Cancers. 2020;12(4):921. doi:10.3390/cancers12040921
19. Dimopoulos MA, Kastritis E, Roussou M, et al. Elevated serum lactate dehydrogenase (LDH) should be included among the variables which define high-risk multiple myeloma. Blood. 2010;116(21):2969. doi:10.1182/blood.V116.21.2969.2969
20. Bal S, Choi K, Landau HJ, et al. Clinical outcomes of newly diagnosed multiple myeloma patients with elevated lactate dehydrogenase who underwent autologous hematopoietic stem cell transplantation. Blood. 2018;132(suppl 1):4623. doi:10.1182/blood-2018-99-120077
21. Kwan J, Tang ML. C-reactive protein and albumin ratio: a novel inflammatory index in predicting mortality. Crit Care Med. 2019;47(3):318–325.
22. Park JH, Kwon SH, Kim JY, et al. The C-reactive protein/albumin ratio as a predictor of mortality in critically ill patients. Crit Care. 2018;22(1):1–8. doi:10.1186/s13054-017-1923-7
23. Akhtar OS, Modi K, Kim J, et al. Simple score of albumin and CRP predicts high-grade toxicity in patients with multiple myeloma receiving CAR-T therapy. Transplant Cell Ther. 2024;30(3):
24. Dou L, Shi M, Song J, et al. The prognostic significance of C-reactive protein to albumin ratio in newly diagnosed acute myeloid leukemia patients. Cancer Manag Res. 2022;14:303–316. doi:10.2147/CMAR.S343580
25. Messerich NM, Uda NR, Volken T, et al. CRP/albumin ratio and Glasgow prognostic score provide prognostic information in myelofibrosis independently of MIPSS70: a retrospective study. Cancers. 2023;15(5):1479. doi:10.3390/cancers15051479
26. Nishida A, Andoh A. The role of inflammation in cancer: mechanisms of tumor initiation, progression, and metastasis. Cells. 2025;14(7):488. PMID: 40214442; PMCID: PMC11987742. doi:10.3390/cells14070488
27. Smith AB, Johnson CD, Williams EF. The role of C-reactive protein in kidney, bladder, and prostate cancers. Front Immunol. 2021;12:721989. doi:10.3389/fimmu.2021.721989
28. Chen X, Li L, Zhang W. Prognostic implications of alpha-fetoprotein and C-reactive protein in hepatocellular carcinoma patients undergoing hepatectomy: the PACE risk score. BMC Cancer. 2023;23:11693.
29. Wu TH, Tsai YT, Chen KY, et al. Utility of high-sensitivity modified Glasgow prognostic score in cancer prognosis: a systemic review and meta-analysis. Int J Mol Sci. 2023;24(2):1318. doi:10.3390/ijms24021318
30. Tsai YT, Fang KH, Hsu CM, et al. Prognostic role of high-sensitivity modified Glasgow prognostic score for patients with operated oral cavity cancer: a retrospective study. Front Oncol. 2022;12:825967. doi:10.3389/fonc.2022.825967
31. Wallington-Beddoe CT, Mynott RL. Prognostic and predictive biomarker developments in multiple myeloma. J Hematol Oncol. 2021;14(1):151. doi:10.1186/s13045-021-01162-7
32. Kádár K, Wolf K, Tábori J, et al. The albumin and monoclonal protein ratio as prognostic marker for multiple myeloma in the era of novel agents. Pathol Oncol Res. 2012;18(4):557–561. doi:10.1007/s12253-012-9506-z
33. Shimada A, Matsuda T, Sawada R, et al. The modified Glasgow prognostic score is a reliable predictor of oncological outcomes in patients with rectal cancer undergoing neoadjuvant chemoradiotherapy. Sci Rep. 2023;13(1):17111. PMID: 37816855; PMCID: PMC10564952. doi:10.1038/s41598-023-44431-w
34. Cotan H, Iaciu C, Nitipir C. Role of the Modified Glasgow Prognostic Score (mGPS) as a Prognostic Factor in Metastatic Colorectal Cancer. Cureus. 2024;16(7):e64916. PMID: 39156325; PMCID: PMC11330632. doi:10.7759/cureus.64916
35. Wang J, Shen N, Shen X, et al. Survival trends and prognostic factors of patients with newly diagnosed multiple myeloma accompanied with extramedullary disease. Ann Med. 2023;55(2):2281657. doi:10.1080/07853890.2023.2281657
36. Okura M, Ida N, Tanaka S, et al. Combination of highly sensitive C-reactive protein with R-ISS is a novel and powerful staging system in multiple myeloma. Blood. 2020;136(suppl 1):7–8. doi:10.1182/blood-2020-141200
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evaluation of Lactate Dehydrogenase and Alkaline Phosphatase as Predictive Biomarkers in the Prognosis of Hepatocellular Carcinoma and Development of a New Nomogram
Su K, Huang W, Li X, Xu K, Gu T, Liu Y, Song J, Qian K, Xu Y, Zeng H, Yang Y, Guo L, Han Y
Journal of Hepatocellular Carcinoma 2023, 10:69-79
Published Date: 14 January 2023