Back to Journals » Infection and Drug Resistance » Volume 19
mNGS-Supported Interpretation of Staphylococcus pettenkoferi Bloodstream Infection After Intracerebral Hemorrhage: A Case Report
Authors Li Q, Wang X, Zhang S, Wang H, Li X, Zhao F
Received 27 March 2026
Accepted for publication 18 May 2026
Published 20 May 2026 Volume 2026:19 611927
DOI https://doi.org/10.2147/IDR.S611927
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Qingjun Li,1,2,* Xiaoyu Wang,3,* Shiwei Zhang,4 He Wang,3 Xia Li,1 Feipeng Zhao1
1School of Basic Medical Sciences, Mudanjiang Medical University, Mudanjiang, People’s Republic of China; 2Department of Anesthesiology, Daqing People’s Hospital, Daqing, People’s Republic of China; 3First Clinical Medical School, Mudanjiang Medical University, Mudanjiang, People’s Republic of China; 4Department of Neurosurgery, Daqing People’s Hospital, Daqing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xia Li; Feipeng Zhao, Email [email protected]; [email protected]
Purpose: Staphylococcus pettenkoferi is an uncommon coagulase-negative staphylococcus whose recovery from blood may be difficult to interpret because of the frequent contamination associated with this bacterial group. We report a case in which peripheral-blood metagenomic next-generation sequencing (mNGS) and repeated blood cultures supported clinically significant bloodstream infection after intracerebral hemorrhage.
Patients and Methods: We described the clinical course, imaging findings, microbiological results, and antimicrobial management of an 85-year-old man admitted to the intensive care unit after intracerebral hemorrhage with intraventricular extension. Peripheral-blood mNGS and two sets of peripheral blood cultures were obtained during early fever evaluation.
Results: Peripheral-blood mNGS, performed on samples obtained immediately after ICU admission and before neurosurgical intervention or intracranial device placement, detected S. pettenkoferi within 24 h. At 72 h, both peripheral blood culture sets yielded the same organism. Concordant results from mNGS and repeated peripheral blood cultures, together with the clinical context, supported clinically significant bloodstream infection rather than simple contamination. The respiratory tract was considered a presumed source in the setting of clinically suspected aspiration-related pulmonary infection, although it was not microbiologically confirmed.
Conclusion: This case highlights the need for cautious interpretation of uncommon coagulase-negative staphylococci recovered from blood. Peripheral-blood mNGS may provide early etiologic support, but conventional blood culture remains essential for confirmation and antimicrobial susceptibility testing.
Plain Language Summary: Staphylococcus pettenkoferi is a rare type of staphylococcal bacterium. When this type of bacterium is found in blood samples, doctors may have difficulty deciding whether it represents a true bloodstream infection or contamination from the skin during blood collection.
We report the case of an 85-year-old man who was admitted to the intensive care unit after intracerebral hemorrhage. He developed fever early during treatment, and chest imaging suggested an aspiration-related lung infection. A blood metagenomic next-generation sequencing test detected Staphylococcus pettenkoferi within 24 hours. The same bacterium was later found in two separate sets of peripheral blood cultures.
Because the same organism was detected by different methods and in repeated blood samples, the finding was interpreted as a clinically significant bloodstream infection rather than simple contamination. The respiratory tract was considered a presumed source, although this could not be proven microbiologically.
This case shows that uncommon coagulase-negative staphylococci should not always be dismissed as contaminants when they are found in blood. Careful interpretation of the patient’s condition, repeated blood culture results, and early molecular testing may help doctors make more timely and appropriate antimicrobial decisions.
Keywords: blood culture, bloodstream infection, case report, coagulase-negative staphylococci, metagenomic next-generation sequencing, Staphylococcus pettenkoferi
Introduction
Bloodstream infection remains an important cause of morbidity and mortality worldwide, particularly in older adults and critically ill patients, in whom delayed pathogen identification may compromise timely antimicrobial management.1,2 In routine clinical practice, blood culture remains the cornerstone of diagnosis because it confirms organism viability and enables antimicrobial susceptibility testing. However, its diagnostic yield may be limited by prior antibiotic exposure, low-level bacteremia, and the time required for organism recovery and identification.3,4
Metagenomic next-generation sequencing (mNGS) has emerged as a culture-independent diagnostic tool that can detect microbial nucleic acids directly from clinical samples. In recent years, it has been increasingly used as an adjunctive method in difficult infectious syndromes, particularly when early etiologic clarification is clinically important or when conventional microbiological methods are inconclusive.5–8 Even so, mNGS does not replace conventional culture. Its results must be interpreted together with the clinical presentation, specimen type, and standard microbiological findings, because it cannot independently distinguish infection from colonization or contamination and does not provide phenotypic antimicrobial susceptibility data.5–8
Coagulase-negative staphylococci (CoNS) are among the organisms most frequently recovered from blood cultures, but their clinical significance is often difficult to determine because they are also common skin commensals and frequent contaminants.9,10 This challenge becomes even greater when an uncommon CoNS species is isolated. Staphylococcus pettenkoferi, first described as a distinct species in 2007, is a relatively rare CoNS that has only occasionally been reported in clinically significant human infection.11,12 Published reports have linked this organism to bacteremia and device-associated infection, but the total number of well-documented clinical cases remains limited, and its pathogenic role may still be underestimated in routine practice.13–15
In critically ill patients, distinguishing true bloodstream infection from culture contamination is particularly important because both underrecognition and overinterpretation may lead to inappropriate management. Repeated recovery of the same organism, concordant microbiological findings, and close correlation with the clinical course are therefore essential when evaluating the significance of uncommon CoNS isolates.16,17 In this context, earlier adjunctive methods may have practical value when interpreted cautiously and confirmed by standard microbiological techniques.
Here, we report an elderly patient with intracerebral hemorrhage who developed early fever in the setting of clinically suspected aspiration-related pulmonary infection, in whom blood mNGS detected S. pettenkoferi before routine blood cultures became positive. The same organism was subsequently recovered from two sets of peripheral blood cultures, supporting true bloodstream infection rather than simple contamination, while the respiratory tract remained the presumed rather than proven source. This case is clinically relevant for two reasons: first, it shows that an uncommon coagulase-negative staphylococcus should not be dismissed automatically as a contaminant when repeated sampling and concordance between microbiological findings and the clinical course support true infection; second, it illustrates how blood mNGS may provide early etiologic support while conventional blood culture remains essential for confirmation and susceptibility testing.
Case Presentation
An 85-year-old man developed sudden nausea, projectile vomiting, and right-sided limb weakness while working. He had no documented history of major chronic cardiometabolic disease and no preceding fever or respiratory symptoms. At initial hospital presentation, non-contrast cranial CT showed hemorrhage in the left thalamic/basal ganglia region with intraventricular extension (Figure 1). Vital signs were as follows: BP, 185/93 mmHg; T, 36.5°C; RR, 25 breaths/min; HR, 75 beats/min; and SpO2, 95% with supplemental oxygen. His consciousness was impaired. Lung auscultation revealed coarse breath sounds with scattered rales.
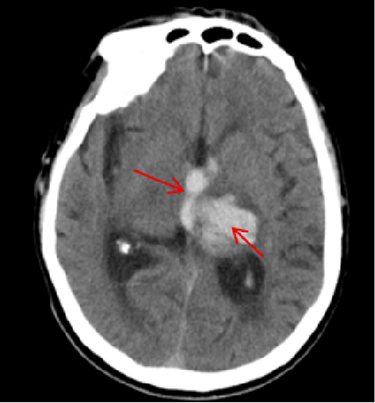 |
Figure 1 Brain CT obtained before ICU admission. The scan shows patchy hyperdense hemorrhage in the left thalamic/basal ganglia region with increased density in the ventricular system, consistent with intraventricular extension of the hematoma. The red arrows indicate the intracerebral hematoma and intraventricular blood. |
Before transfer to the ICU, repeat brain CT confirmed left thalamic hemorrhage with intraventricular extension and no significant midline shift (Figure 1). Chest CT demonstrated increased bilateral lung markings, focal hyperlucent areas with cystic or bullous change, and posterior patchy opacities suggestive of early aspiration-related inflammatory or infectious consolidation (Figure 2). Aspiration-related pulmonary infection was suspected clinically on the basis of impaired consciousness, preceding projectile vomiting, abnormal lung auscultation with scattered rales, hypoxemia, early fever during ICU care, and dependent posterior patchy opacities on chest CT. No respiratory specimen confirmed S. pettenkoferi as a pulmonary pathogen; therefore, the respiratory tract was considered a presumed rather than microbiologically proven source. Laboratory testing before ICU admission showed neutrophils accounting for 76.2% and lymphocytes for 18.5% of the total leukocyte count, decreased serum albumin (37 g/L), and hypoxemia with mild respiratory alkalosis on arterial blood gas analysis (PaCO2 36.7 mmHg, PaO2 59.9 mmHg, and PaO2/FiO2 285 mmHg). The initial working diagnoses included intracerebral hemorrhage with intraventricular extension, obstructive hydrocephalus, type I respiratory failure, and aspiration-related pulmonary infection. The patient was admitted to the ICU for neurosurgical management and organ support. Initial peripheral blood samples for mNGS and two sets of blood cultures were obtained immediately after ICU admission, before neurosurgical intervention or placement of any intracranial drainage device; no external ventricular drainage, intracranial pressure monitoring catheter, or other intracranial drainage device was in place at that time.
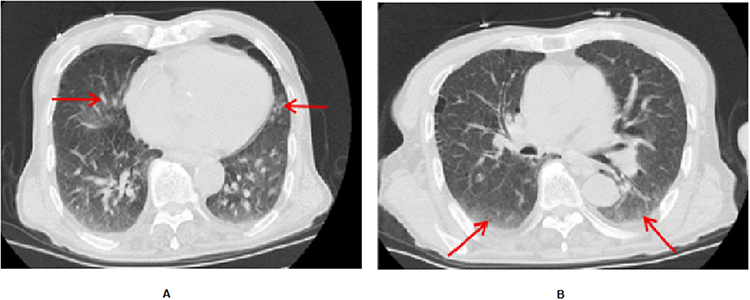 |
Figure 2 Chest CT obtained before ICU admission. (A) Scattered cystic lucencies without visible pulmonary vascular markings, suggestive of localized emphysematous or bullous change. The red arrows indicate the cystic or bullous changes. (B) Curvilinear patchy opacities in the posterior lung fields, raising concern for early aspiration-related inflammatory or infectious consolidation. The red arrows indicate the posterior patchy pulmonary opacities. |
Microbiological Evaluation and Antimicrobial Therapy
Fever developed early during ICU care, with a peak temperature of 38.4°C, in the setting of clinically suspected aspiration-related pulmonary infection. Because bloodstream infection was suspected, two sets of peripheral blood cultures and peripheral-blood metagenomic next-generation sequencing (mNGS) were obtained immediately after ICU admission and before escalation of antimicrobial therapy. The mNGS assay was performed directly on peripheral blood and yielded a result earlier than routine culture-based testing.
Empiric ampicillin/sulbactam was initiated after the initial blood samples had been obtained. Within 24 h of admission, blood mNGS detected Staphylococcus pettenkoferi. At 72 h, the same organism was recovered from both sets of peripheral blood cultures. Species identification and antimicrobial susceptibility testing were performed in the hospital clinical microbiology laboratory. Species identification was conducted using MALDI-TOF MS, and susceptibility testing was performed using standard phenotypic methods, including cefoxitin screening for methicillin susceptibility. In view of the persistent fever, the compatible clinical context, and the concordant microbiological findings from blood mNGS and two peripheral blood-culture sets, the isolate was considered clinically significant rather than a contaminant. At that stage, no infectious focus other than the respiratory tract was identified. The episode was therefore managed as clinically significant bloodstream infection, with the respiratory tract considered a presumed source in the setting of clinically suspected aspiration-related pulmonary infection after intracerebral hemorrhage. In response to persistent fever, clinically suspected aspiration-related pulmonary infection, and concern for possible polymicrobial infection, antimicrobial therapy was empirically broadened to piperacillin plus ertapenem by the treating team. This regimen reflected real-world ICU management before complete microbiological clarification and was not intended to represent definitive targeted or preferred therapy for S. pettenkoferi alone. Antimicrobial management was reassessed according to the clinical course and follow-up microbiological results. Detailed microbiological identification results are summarized in Table 1.
 |
Table 1 Microbiological Identification of Staphylococcus Pettenkoferi in This Case |
During prolonged ICU care, a later, separate healthcare-associated bloodstream infection caused by methicillin-resistant coagulase-negative staphylococci was identified approximately two weeks after ICU admission. This later episode involved different CoNS species, Staphylococcus epidermidis and Staphylococcus hominis, and was interpreted as distinct from the initial S. pettenkoferi episode. Vancomycin was introduced for MR-CoNS coverage, whereas ceftazidime was used for concurrent empiric Gram-negative coverage in the ICU setting.
Key Clinical Events, Microbiological Findings, and Antimicrobial Adjustments are Summarized Below
Initial hospital presentation: The patient developed sudden nausea, projectile vomiting, and right-sided limb weakness. Initial non-contrast brain CT showed left thalamic/basal ganglia hemorrhage with intraventricular extension.
Before transfer to the ICU: Repeat brain CT confirmed left thalamic hemorrhage with intraventricular extension and no significant midline shift. Chest CT showed posterior patchy pulmonary opacities and focal cystic or bullous changes, supporting clinically suspected aspiration-related pulmonary infection.
Day 0, immediately after ICU admission: Two sets of peripheral blood cultures were obtained and peripheral-blood mNGS was performed before neurosurgical intervention or placement of any intracranial drainage device and before escalation of antimicrobial therapy. Empiric ampicillin/sulbactam was initiated after the initial blood samples had been collected.
Day 1, within 24 h: Blood mNGS detected Staphylococcus pettenkoferi.
Day 3, 72 h: Both sets of peripheral blood cultures yielded S. pettenkoferi; antimicrobial therapy was escalated to piperacillin plus ertapenem as empiric broad-spectrum therapy in the setting of persistent fever and clinically suspected aspiration-related pulmonary infection.
Approximately week 2: A later, separate healthcare-associated MR-CoNS bloodstream infection was identified, involving Staphylococcus epidermidis and Staphylococcus hominis. Vancomycin was introduced for MR-CoNS coverage, whereas ceftazidime was used for concurrent empiric Gram-negative coverage in the ICU setting.
Follow-up: Body temperature declined, inflammatory markers improved, and subsequent blood cultures became negative. Follow-up brain CT showed absorption of the hemorrhage and reduced ventricular blood density, and follow-up chest CT demonstrated improvement in pulmonary consolidation.
During treatment, follow-up brain CT showed absorption of the hemorrhage and reduced ventricular blood density (Figure 3). Follow-up chest CT demonstrated improvement in pulmonary consolidation (Figure 4). After approximately one month of treatment and supportive care, the patient’s vital signs stabilized, respiratory function improved, and he was transferred to a secondary hospital for ongoing care.
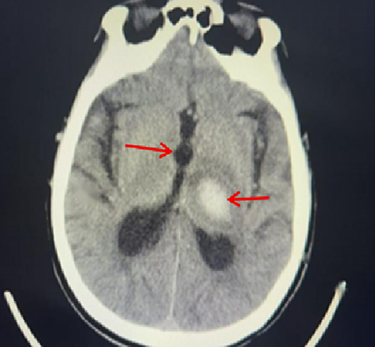 |
Figure 3 Follow-up brain CT after treatment. The scan shows absorption of the left thalamic hemorrhage and clearance of intraventricular blood. The red arrows indicate the regions of reduced hematoma density and decreased intraventricular blood compared with the initial CT. |
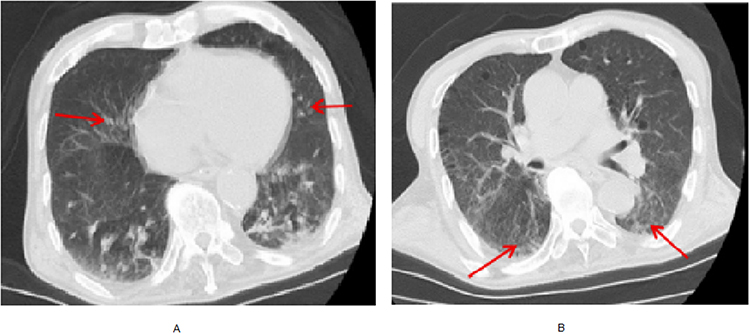 |
Figure 4 Follow-up chest CT after treatment. (A) No progression of the pre-existing scattered cystic changes. The red arrows indicate residual cystic or bullous changes. (B) Decreased posterior pulmonary opacities, consistent with radiographic improvement. The red arrows indicate the improved posterior pulmonary opacities. |
Discussion
Bloodstream infection remains a major cause of morbidity and mortality worldwide, particularly in critically ill patients, in whom delayed recognition and inappropriate early antimicrobial treatment may worsen outcomes.18,19 In time-sensitive settings, broad-spectrum therapy is sometimes initiated before the microbiological diagnosis is established. However, unnecessary antimicrobial escalation may complicate subsequent management and contribute to antimicrobial resistance. Antimicrobial decisions should therefore be reassessed continuously according to the clinical course and microbiological evidence.20,21
In this case, the initial episode also required cautious source attribution. As described in the Case Presentation, aspiration-related pulmonary infection was clinically suspected, but no respiratory specimen confirmed S. pettenkoferi as a pulmonary pathogen and no direct microbiological link between the pulmonary findings and bloodstream infection was established. Therefore, the respiratory tract was considered a presumed rather than confirmed source. This distinction is important because the main diagnostic issue was not to prove a respiratory source, but to determine whether an uncommon CoNS recovered from blood represented clinically significant infection rather than contamination.
Staphylococcus pettenkoferi is a relatively recently described coagulase-negative staphylococcal species with phenotypic overlap with other CoNS, which may lead to misidentification when specific identification methods are not used.11,12 Although its clinical spectrum remains incompletely defined, previous reports have described S. pettenkoferi bacteremia and device-associated infection, supporting its pathogenic potential in selected clinical contexts.16–18 When CoNS are recovered from blood, established interpretive frameworks emphasize compatible clinical features, repeated recovery of the same organism from two or more blood specimens collected on separate occasions, and exclusion of a more plausible alternative explanation such as contamination.12,22 The IDSA guideline for catheter-related bloodstream infection also recommends careful interpretation of CoNS recovered from blood and assessment of possible device-related sources when catheter-related infection is suspected.23
In the present case, these principles were applied cautiously rather than as a rigid diagnostic rule. S. pettenkoferi was detected early by peripheral-blood mNGS and was subsequently recovered from two separate sets of peripheral blood cultures. Together with the clinical presentation and repeated recovery from peripheral blood, these concordant findings supported clinically significant bloodstream infection rather than simple contamination. However, because no respiratory specimen confirmed S. pettenkoferi as a pulmonary pathogen, the source of bacteremia could not be confirmed microbiologically. Because the initial samples were obtained before neurosurgical intervention or intracranial device placement, a neurosurgical device-related source was considered unlikely for the initial S. pettenkoferi bloodstream infection.
Previously reported S. pettenkoferi infections have been clinically heterogeneous. Published cases and series have included fatal ICU bloodstream infection, ICU-associated bacteremia, peripheral line-associated bacteremia, catheter-related bacteremia, prosthetic joint infection, and rare central nervous system infection with meningoencephalitis and brain abscess.16–18,24–28 These reports suggest that S. pettenkoferi should not be interpreted solely on the basis of organism rarity, because its clinical significance depends strongly on host status, repeated microbiological recovery, antimicrobial susceptibility, and the presence or absence of intravascular catheters, prosthetic material, or other plausible infection foci. Park et al also showed that blood isolates of S. pettenkoferi may represent true infection, contamination, or catheter colonization, further supporting the need for careful microbiological interpretation.27 Management strategies reported in the literature have therefore varied according to clinical severity, antimicrobial susceptibility, and presumed source. Compared with these reports, the present case is distinctive because S. pettenkoferi was detected early by peripheral-blood mNGS and then confirmed by two peripheral blood culture sets obtained before neurosurgical intervention or intracranial device placement, whereas the presumed respiratory source remained microbiologically unconfirmed.
Before routine blood culture results became available, peripheral-blood mNGS provided early etiologic support, but it was not interpreted as definitive evidence on its own. Because mNGS detects microbial nucleic acids rather than viable organisms, it cannot reliably distinguish infection from contamination or colonization and does not provide phenotypic antimicrobial susceptibility data. Therefore, mNGS findings should be interpreted together with specimen type, sampling conditions, clinical findings, and conventional microbiology.23 In this case, concordant recovery of the same organism from two peripheral blood culture sets provided culture-based confirmation and susceptibility information, whereas mNGS mainly helped narrow etiologic suspicion earlier in the disease course.
The later MR-CoNS episode is mentioned only to complete the clinical course and to distinguish it from the initial S. pettenkoferi bloodstream infection. It occurred after approximately two weeks of ICU care, involved different CoNS species, Staphylococcus epidermidis and Staphylococcus hominis, and followed invasive supportive management and device exposure. It was therefore interpreted as a separate healthcare-associated episode rather than persistence or relapse of the initial infection. Vancomycin was used as the anti-staphylococcal agent, whereas ceftazidime was used for concurrent empiric Gram-negative coverage in the ICU setting and was not intended to treat MR-CoNS. Because no catheter-tip culture or other device-specific microbiological evidence confirmed a source, we avoided attributing this later episode to a specific device.
This case adds to the limited clinical literature on S. pettenkoferi bloodstream infection by illustrating a scenario in which an uncommon CoNS was detected early by peripheral-blood mNGS and subsequently confirmed by two peripheral blood culture sets. Its main contribution is not to establish a new treatment strategy or a definitive source of infection, but to emphasize a cautious interpretive approach when uncommon CoNS are recovered from blood. In this case, repeated recovery from peripheral blood, concordance across diagnostic methods, compatibility with the clinical course, and careful assessment of alternative explanations, including contamination and device-related infection, supported clinical significance. Because this is a single case, broader conclusions regarding typical infection sources, optimal antimicrobial therapy, or the routine role of mNGS in S. pettenkoferi bloodstream infection should be avoided.
Conclusion
This case adds to the limited evidence that Staphylococcus pettenkoferi can be associated with clinically significant bloodstream infection when supported by repeated blood culture recovery, concordant diagnostic findings, and compatible clinical features. In this patient, peripheral-blood mNGS provided early etiologic support, whereas conventional blood culture remained essential for confirmation and susceptibility testing. The respiratory tract was considered a presumed rather than microbiologically confirmed source. This case highlights the need for cautious interpretation of uncommon CoNS recovered from blood and underscores the need to avoid broad conclusions regarding typical infection sources or optimal antimicrobial therapy from a single case.
Data Sharing Statement
The data supporting the findings of this case report are available from the corresponding authors, Xia Li and Feipeng Zhao, upon reasonable request, subject to institutional requirements and patient privacy considerations.
Ethics Statement
This case report was reviewed and approved for publication by the Ethics Committee of Daqing People’s Hospital. Institutional approval was required for publication of the case details and accompanying images, and this approval was obtained from the Ethics Committee of Daqing People’s Hospital. Written informed consent for publication of the case details and any accompanying images was obtained directly from the patient after recovery. All patient information was anonymized to protect patient confidentiality.
Acknowledgments
We thank the ICU, neurosurgery, radiology, and clinical microbiology laboratory teams for their contributions to the patient’s care, microbiological identification, antimicrobial susceptibility testing, and diagnostic work-up.
Funding
This work was supported by Mudanjiang Medical University Doctoral Research Initiation Grant 2025-MYBSKY-001.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Underwood J, Griffiths R, Gillespie D, Akbari A, Ahmed H. All-cause and infection-attributable mortality amongst adults with bloodstream infection: a population-based study. Open Forum Infect Dis. 2024;11(5):ofae126. doi:10.1093/ofid/ofae126
2. Kadri SS, Lai YL, Warner S, et al. Inappropriate empirical antibiotic therapy for bloodstream infections based on discordant in-vitro susceptibilities: a retrospective cohort analysis of prevalence, predictors, and mortality risk in US hospitals. Lancet Infect Dis. 2021;21(2):241–9. doi:10.1016/S1473-3099(20)30477-1
3. Chen J, Huang H, Zhang R, et al. Risk factors associated with mortality and pathogen characteristics of bloodstream infection-induced severe sepsis in the pediatric intensive care unit: a retrospective cohort study. Front Cell Infect Microbiol. 2025;15:1492208. doi:10.3389/fcimb.2025.1492208
4. Iba T, Maier CL, Tanigawa T, Levy JH. Risk stratification utilizing sequential organ failure assessment (SOFA) score, antithrombin activity, and demographic data in sepsis-associated disseminated intravascular coagulation (DIC). Sci Rep. 2023;13:22502. doi:10.1038/s41598-023-49855-y
5. Gu W, Miller S, Chiu CY. Clinical metagenomic next-generation sequencing for pathogen detection. Clin Infect Dis. 2019;68(12):2062–2068. doi:10.1093/cid/ciy1049
6. Chiu CY, Miller SA. Clinical metagenomics. Nat Rev Genet. 2019;20(6):341–355. doi:10.1038/s41576-019-0113-7
7. Rodino KG, Simner PJ. Status check: next-generation sequencing for infectious-disease diagnostics. J Clin Invest. 2024;134(4):e178003. doi:10.1172/JCI178003
8. Zhao Y, Zhang W, Zhang X. Application of metagenomic next-generation sequencing in the diagnosis of infectious diseases. Front Cell Infect Microbiol. 2024;14:1458316. doi:10.3389/fcimb.2024.1458316
9. Hall KK, Lyman JA. Updated review of blood culture contamination. Clin Microbiol Rev. 2006;19(4):788–802. doi:10.1128/CMR.00062-05
10. Narayana Iyengar S, Dietvorst J, Ferrer-Vilanova A, Guirado G, Muñoz-Berbel X, Russom A. Toward rapid detection of viable bacteria in whole blood for early sepsis diagnostics and susceptibility testing. ACS Sens. 2021;6(9):3357–3366. doi:10.1021/acssensors.1c01219
11. Trülzsch K, Grabein B, Schumann P, et al. Staphylococcus pettenkoferi sp. nov. a novel coagulase-negative staphylococcal species isolated from human clinical specimens. Int J Syst Evol Microbiol. 2007;57(Pt 7):1543–1548. doi:10.1099/ijs.0.64381-0
12. Loïez C, Wallet F, Pischedda P, et al. First case of Staphylococcus pettenkoferi isolated in a human clinical specimen. J Clin Microbiol. 2007;45(3):1061–1063.
13. Mammina C, Bonura C, Vella MA, Fasciana T, Palma DM. A fatal bloodstream infection by Staphylococcus pettenkoferi in an intensive care unit patient. Case Rep Crit Care. 2011;2011:612732. doi:10.1155/2011/612732
14. Strong C, Csiako M, Cabezas M, Barwatt JW, Tillekeratne LG. Staphylococcus pettenkoferi bacteremia in an American intensive care unit. Case Rep Infect Dis. 2021;2021. doi:10.1155/2021/5235691
15. Gisriel SD, Jacobs JW. The first reported case of Staphylococcus pettenkoferi prosthetic joint infection. Microbes Infect. 2022;24(6–7):104978. doi:10.1016/j.micinf.2022.104978
16. Zahar JR, Lesprit P, Ruckly S, et al. Predominance of healthcare-associated cases among episodes of community-onset bacteraemia due to extended-spectrum β-lactamase-producing Enterobacteriaceae. Int J Antimicrob Agents. 2017;49(1):67–73. doi:10.1016/j.ijantimicag.2016.09.032
17. Caceres DH, Rivera SM, Armstrong PA, et al. Case-case comparison of Candida auris versus other Candida species bloodstream infections: results of an outbreak investigation in Colombia. Mycopathologia. 2020;185(5):917–923. doi:10.1007/s11046-020-00478-1
18. Cekin ZK, Oncul A, Bayraktar B. Bloodstream infections caused by multidrug resistant bacteria: clinical and microbiological features and mortality. Sisli Etfal Hastan Tip Bul. 2023;57:416–425. doi:10.14744/SEMB.2023.31697
19. Vucelić V, Klobučar I, Đuras-Cuculić B, et al. Sepsis and septic shock: an observational study of the incidence, management, and mortality predictors in a medical intensive care unit. Croat Med J. 2020;61:429–439. doi:10.3325/cmj.2020.61.429
20. Clinical Microbiology Group of Chinese Society of Laboratory Medicine, Clinical Microbiology Group of Chinese Society of Microbiology and Immunology, Society of Clinical Microbiology and Infection of China International Exchange and Promotion Association for Medical and Healthcare. Chinese expert consensus on metagenomics next-generation sequencing application on pathogen detection of infectious diseases. Chin J Lab Med. 2021;44(2):107–120.
21. Mandell LA, Niederman MS. Aspiration pneumonia. N Engl J Med. 2019;380(7):651–663. doi:10.1056/NEJMra1714562
22. Centers for Disease Control and Prevention. Laboratory Confirmed Bloodstream Infection (LCBI) checklist. National Healthcare Safety Network; 2024. Available from: https://www.cdc.gov/nhsn/pdfs/checklists/Laboratory-Confirmed-Bloodstream-Infection-LCBI-Checklist.pdf.
23. Mermel LA, Allon M, Bouza E, et al. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 update by the infectious diseases society of America. Clin Infect Dis. 2009;49(1):1–45. doi:10.1086/599376
24. Hashi AA, Delport JA, Elsayed S, Silverman MS. Staphylococcus pettenkoferi bacteremia: a case report and review of the literature. Can J Infect Dis Med Microbiol. 2015;26(6):319–322. doi:10.1155/2015/748154
25. Hadano Y, Hijikata T, Miura A, Fujii S, Awaya Y. Staphylococcus pettenkoferi bacteremia in a tertiary care hospital in Japan: report of three cases. J Infect Chemother. 2022;28(10):1424–1426. doi:10.1016/j.jiac.2022.06.009
26. Demiray EKD, Reyhanli G, Aydogdu O. How did that happen? Case report of a rarely heard bacteria Staphylococcus pettenkoferi and meningoencephalitis and brain abscess. Oman Med J. doi:10.5001/omj.2026.22
27. Park S, Chung HS, Lee M. Clinical and microbiological characteristics of six Staphylococcus pettenkoferi isolates from blood samples. Ann Lab Med. 2015;35(2):250–253. doi:10.3343/alm.2015.35.2.250
28. Kierzkowska M, Markowska K, Majewska A. Knowledge, attitude and practice regarding Staphylococcus pettenkoferi. Infect Dis Rep. 2022;14(1):112–120. doi:10.3390/idr14010015
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Diagnosis of Mycoplasma hominis Meningitis with Metagenomic Next-Generation Sequencing: A Case Report
Dong Y, He Y, Zhou X, Lv X, Huang J, Li Y, Qian X, Hu F, Zhu J
Infection and Drug Resistance 2022, 15:4479-4486
Published Date: 12 August 2022
Metagenomic Next-Generation Sequencing Assists in the Diagnosis of Mediastinal Aspergillus fumigatus Abscess in an Immunocompetent Patient: A Case Report and Literature Review
Deng W, Jiang Y, Qin J, Chen G, Lv Y, Lei Y, Luo J, Hong K, Huang B, Qin L, Tang X, Ye L, Dang Y, Wang C, Long F, Wang K, Kong J
Infection and Drug Resistance 2023, 16:1865-1874
Published Date: 30 March 2023
Metagenomic Next-Generation Sequencing Contributes to the Diagnosis of Pneumonia Caused by Chlamydia abortus in a Male Patient: Case Report and Literature Review
Gong F, Chen Z, Chang J, Liu J, Wang X, Mo W, Tan M, Jiang T
Infection and Drug Resistance 2023, 16:3463-3468
Published Date: 2 June 2023
Improving Blood Culture Quality with a Medical Staff Educational Program: A Prospective Cohort Study
Chen Y, Dai Y, Zhou Y, Huang Y, Jin Y, Geng Y, Ji B, Xu R, Zhu W, Hu S, Li Z, Liang J, Xiao Y
Infection and Drug Resistance 2023, 16:3607-3617
Published Date: 7 June 2023
Chlamydia Psittaci Pneumonia-Induced Myocarditis: A Case Report
Yang X, Liu Z, Liu X, Li Q, Huang H, Li R, He M
Infection and Drug Resistance 2023, 16:4259-4264
Published Date: 29 June 2023