Back to Journals » Drug Design, Development and Therapy » Volume 19
Minimum Effective Volume of Liposomal Bupivacaine for Interscalene Block in Arthroscopic Rotator Cuff Repair: A Prospective, Biased-Coin Up-and-Down Dose-Finding Study
Authors Wang HT, Xue Q, Li HJ, Zhao YY ![]() , Tian K, Yang JJ
, Tian K, Yang JJ ![]()
Received 3 August 2025
Accepted for publication 21 December 2025
Published 26 December 2025 Volume 2025:19 Pages 11789—11797
DOI https://doi.org/10.2147/DDDT.S558049
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Tamer Ibrahim
Hai-Tao Wang,1 Qiong Xue,1 Hui-Juan Li,1 Ying-Ying Zhao,1 Ke Tian,2 Jian-Jun Yang1
1Department of Anesthesiology, Pain and Perioperative Medicine, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, People’s Republic of China; 2Department of Orthopedics, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, People’s Republic of China
Correspondence: Jian-Jun Yang, Department of Anesthesiology, Pain and Perioperative Medicine, The First Affiliated Hospital of Zhengzhou University, No. 1 East Jianshe Road, Zhengzhou, People’s Republic of China, Email [email protected]
Background: Establishing the minimum effective volume (MEV90) of liposomal bupivacaine for ultrasound‑guided interscalene brachial plexus block (ISB) is essential to optimize postoperative analgesia and minimize local anesthetic–related side effects in patients undergoing arthroscopic rotator cuff repair. Determining this optimal volume provides a clinically meaningful reference for achieving consistent nerve block success while reducing unnecessary drug exposure and the risk of systemic toxicity. Therefore, the present study aimed to identify the MEV90 of liposomal bupivacaine for ISB in patients undergoing arthroscopic shoulder surgery.
Patients and Methods: This dose-finding study enrolled 51 patients scheduled for arthroscopic rotator cuff repair. Using a biased-coin up-and-down sequential design, patients received varying volumes of liposomal bupivacaine for ultrasound-guided ISB. The MEV90 was determined using centered isotonic regression. The occurrence of adverse events was systematically recorded for 72 hours.
Results: The MEV90 of liposomal bupivacaine for ISB was 10.0mL (90% CI, 9.3 to 12.5mL). A moderate positive correlation was identified between the time to first analgesic request and the volume of liposomal bupivacaine administered (r = 0.6, P < 0.001). Adverse events within 72 hours following the block included dizziness (7.8%), nausea and vomiting (9.8%), and chest discomfort (3.9%).
Conclusion: The MEV90 of liposomal bupivacaine for ultrasound-guided interscalene brachial plexus block in patients undergoing rotator cuff repair surgery was found to be 10.0 mL.
Keywords: bupivacaine, liposomes, brachial plexus blocks, rotator cuff tear arthropathy
Introduction
Arthroscopic rotator cuff repair is known to cause substantial postoperative pain, which, if inadequately managed, may delay early rehabilitation and adversely affect shoulder function recovery.1 Currently, multimodal analgesic regimens are recommended, with ultrasound-guided interscalene brachial plexus block (ISB) being the gold standard for perioperative analgesia in shoulder surgery due to its high success rate and opioid-sparing effect.2 However, conventional local anesthetics such as bupivacaine often provide limited analgesia duration of approximately 12–18 hours,3 necessitating supplemental analgesics which may increase opioid exposure and related adverse effects.
Liposomal bupivacaine (LB) is a novel long-acting formulation employing multivesicular liposome technology that allows sustained release of bupivacaine over 72 hours or longer.4,5 Randomized controlled trials have demonstrated that LB, when used in brachial plexus block, significantly prolongs analgesia and reduces postoperative opioid consumption compared to standard bupivacaine.6 These pharmacological advantages potentially address the need for extended duration analgesia during the peak pain period after rotator cuff repair, while limiting the total dose of local anesthetic and reducing the risk of local anesthetic systemic toxicity.
Although numerous dose‑finding studies of plain local anesthetics for ISB have been published, their MEV estimates vary considerably due to differences in drug concentration, methodology, endpoints, injection technique, and patient populations.7,8 By contrast, well‑designed investigations of liposomal bupivacaine in this block are lacking, and its MEV—particularly MEV90—remains undefined, with current practice relying largely on empirical volumes extrapolated from conventional bupivacaine.9
Given the variability in existing evidence and the clinical relevance of optimizing LB dosing, we conducted a prospective, biased-coin up-and-down sequential allocation trial to determine the MEV90 of LB for ultrasound-guided ISB in patients undergoing arthroscopic rotator cuff repair. This study aims to provide evidence-based guidance for LB volume selection, with the goal of improving postoperative pain control and reducing opioid use in this patient population.
Materials and Methods
Participants
This was a prospective, biased-coin up-and-down sequential allocation dose-finding study. The study (2024-KY-0358-002) was approved by the Scientific Research and Clinical Trial Ethics Committee of the First Affiliated Hospital of Zhengzhou University in accordance with the Declaration of Helsinki and registered with the Chinese Clinical Trials Registry (ChiCTR2400085466). After obtaining written informed consent, patients scheduled for unilateral elective upper limb surgery between June 2024 and September 2024 were prospectively enrolled at the First Affiliated Hospital of Zhengzhou University, Zhengzhou, China.
Inclusion criteria included: (1) Patients scheduled for arthroscopic rotator cuff repair at the First Affiliated Hospital of Zhengzhou University; (2) ASA classification I or II; (3) Age 18–65 years, with no gender restrictions; (4) BMI 18–30 kg/m2; (5) Patients receiving nerve block and PCIA after surgery.
Exclusion criteria included: (1) Presence of nerve injury or disorders around the shoulder joint, such as thoracic outlet syndrome, multiple sclerosis, or cervical intervertebral disc disease with ipsilateral radiculopathy; (2) Abnormal sensory or motor function in the upper limbs; (3) Active infection at the puncture site or coagulation dysfunction (eg, hemophilia, von Willebrand disease, or INR > 2); (4) Severe respiratory disease or a history of significant cardiovascular or cerebrovascular disease; (5) Diabetes or nervous system dysfunction; (6) Inability to understand or cooperate with VAS raters; (7) History of shoulder surgery; (8) Failed nerve block; (9) History of local anesthetic allergy; (10) Long-term opioid use (≥ 3 months or ≥ 1 month with a daily dose of ≥ 5 mg morphine equivalent); (11) Operation time < 1 hour or > 3 hours.
Study Design
The doses were adjusted according to the biased-coin design.10 A successful block was defined as a resting NRS score of < 4, 24 hours after the block, without the need for rescue analgesia. The initial dose of 10 mL (133 mg) was determined following the manufacturer’s recommendation and literature on low-volume interscalene blocks,7 corroborated by our prior institutional experience of its stable analgesic effect.Subsequently, if a patient experienced an inadequate block, the volume was increased by 1 mL for the next participant. If a patient achieved a successful block, the next participant was randomized to receive either a reduced volume (with a decrement of 1 mL) with a probability of b = 0.11, or the same volume with a probability of 1-b = 0.89. A schematic representation of this dose-adjustment algorithm is provided in Figure 1.
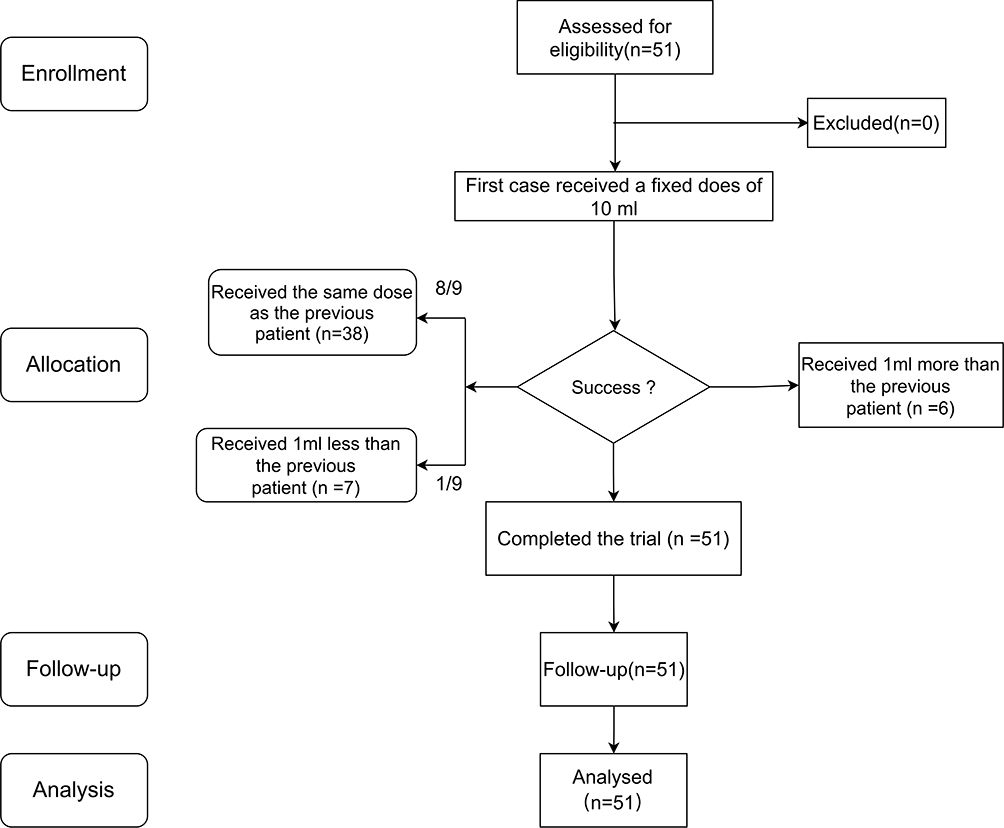 |
Figure 1 The CONSORT flow diagram. |
Ultrasound-Guided Interscalene Brachial Plexus Block
The interscalene brachial plexus blockade was performed in the anesthesia procedure room approximately 1 to 1.5 hours prior to the scheduled surgery. The brachial plexus was visualized using a 13–6 MHz linear transducer (SonoSite Edge, SonoSite, Bothell, Washington, USA) placed over the external jugular vein approximately 3 cm cranial to the clavicle, until the C5 and C6 nerve roots were distinctly visualized. A blunt-tip block needle (22 gauge cannula, 80 mm, Stimuplex D, B.Braun, Melsungen, Germany) was advanced using an “in-plane” approach from posterior to anterior towards the superior portion of the brachial plexus (C5-C6) at the standard level for the interscalene block, and 10 mL of liposomal bupivacaine was administered. If the spread was deemed inadequate, the needle tip was repositioned. Patients and personnel conducting the assessments were blinded to the volume of liposomal bupivacaine.
Block Evaluation
After 30 minutes of the nerve block, an examiner blinded to the volume of injectate assessed the presence of sensory blockade in the C5 and C6 territory. For the sensory function assessment, the subject’s sensitivity to cold in the deltoid area was assessed with their eyes closed during screening. The deltoid area was selected for testing the sensory block because the axillary nerve territory was deemed most relevant to the surgical model employed.11 Sensory function was recorded as either present or absent. If the cold sensation on the lateral side of the deltoid muscle was absent, the study proceeded to the next observation step. Otherwise, the subject was classified as withdrawn from the study.
Intraoperative Management
After 10 minutes of evaluation, standard vital sign monitors were applied, and oxygen was administered through a facemask. General anesthesia was induced using 2–2.5 mg/kg propofol, 0.2–0.3 mg/kg sufentanil, and 0.15 mg/kg cisatracurium. The airway was secured via tracheal intubation, and ventilation was maintained with 40% oxygen and a tidal volume of 6 mL/kg of ideal body weight. General anesthesia was maintained with 1–1.5% sevoflurane and 0.2–0.3 µg/kg/min remifentanil. After the surgical procedure, patients were transferred to the recovery room.
Outcome Measure
Patients were informed about the numeric rating scale for pain (0 to 10, where 0 indicates no pain and 10 indicates the worst imaginable pain) at rest and during movement, as well as the use of a 72-hour patient-controlled intravenous (i.v.) oxycodone infusion (0.5 mg/mL; 3 mg bolus as needed, no background infusion, and a lockout time of 5 minutes). Pain intensity scores were assessed by a research nurse, blinded to the volume of liposomal bupivacaine injected, at 6, 12, 24, 36, 48, and 72 hours following the liposomal bupivacaine injection. The date, time, and amount of rescue medication used were recorded over 72 hours.
The research nurse also recorded occurrences of vascular puncture, paraesthesia, hoarseness, local anesthetic systemic toxicity, Horner’s syndrome, dizziness, nausea and vomiting, and other complications within 72 hours following the nerve block.
Statistical Analysis
To estimate MEV90, a minimum of 45 successful blocks was required.12 The MEV90 with a 90% confidence interval (CI) was calculated using centered isotonic regression (CIR) for point and interval dose-response studies. CIR was chosen for the statistical calculation because it provides a substantial reduction in estimation error compared to isotonic regression when monotonicity violations occur.13 The CIR was performed using the R Statistical Software Package (R Foundation for Statistical Computing, Vienna, Austria; ISBN; http://www.Rproject.org). For continuous variables, the normality of the data was assessed using the Kolmogorov–Smirnov test. Data are presented as mean (SD or 95% CI) when normally distributed, and as median [IQR] when not normally distributed. Categorical variables are described as frequency, n (%). Pearson’s correlation coefficient (r) was also calculated to assess the association between the time to first analgesic request and the administered volume of liposomal bupivacaine.
Results
The study included 51 participants (Figure 1) with a mean age of 56.94 years. Patient characteristics and clinical parameters are summarized in Table 1. The mean NRS pain score during movement was 5.73, whereas the median NRS score at rest was 2. Regarding gender distribution, 64.71% of the participants were female (33 individuals), whereas 35.29% were male (18 individuals).
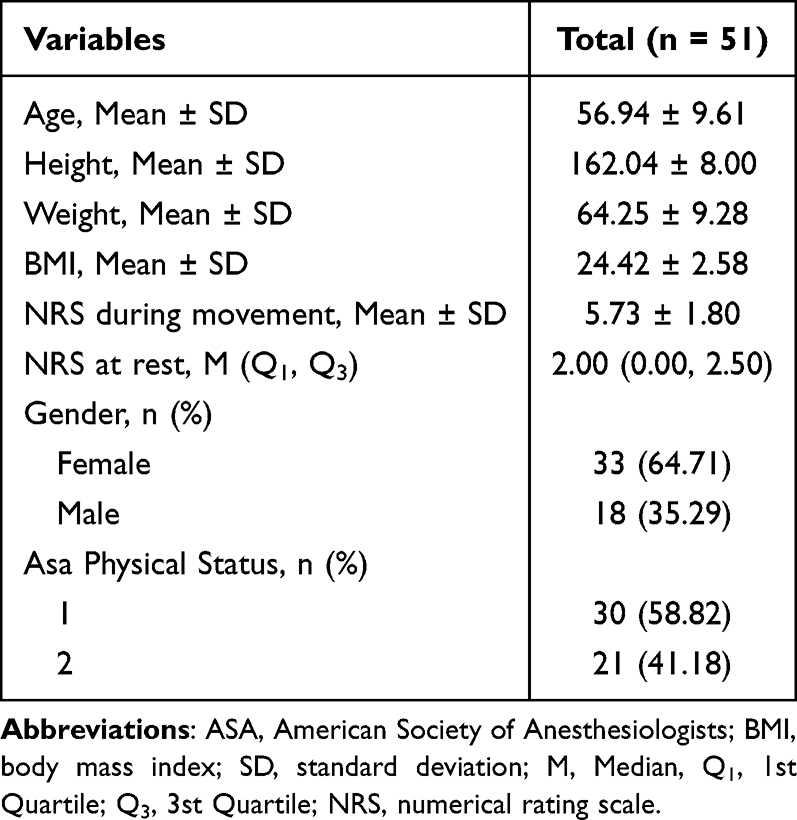 |
Table 1 Characteristics of 51 Patients. Values are Mean (SD) or Number (Proportion) |
The biased-coin design up-and-down sequence is illustrated in Figure 2a. Based on our criteria for successful blockade, six patients experienced block failure, whereas the remaining participants achieved successful blockade. The observed response rates for each volume of liposomal bupivacaine are shown in Table 2 and Figure 2b. The response rates adjusted by the pooled adjacent violators algorithm to generate monotonically non-decreasing response rates for the isotonic regression method are also shown. The MEV90 was found to be 10.0 mL (90% CI, 9.3 to 12.5 mL).
 |
Table 2 The Observed and PAVA-Adjusted Response Rates at Different Volumes of Liposomal Bupivacaine |
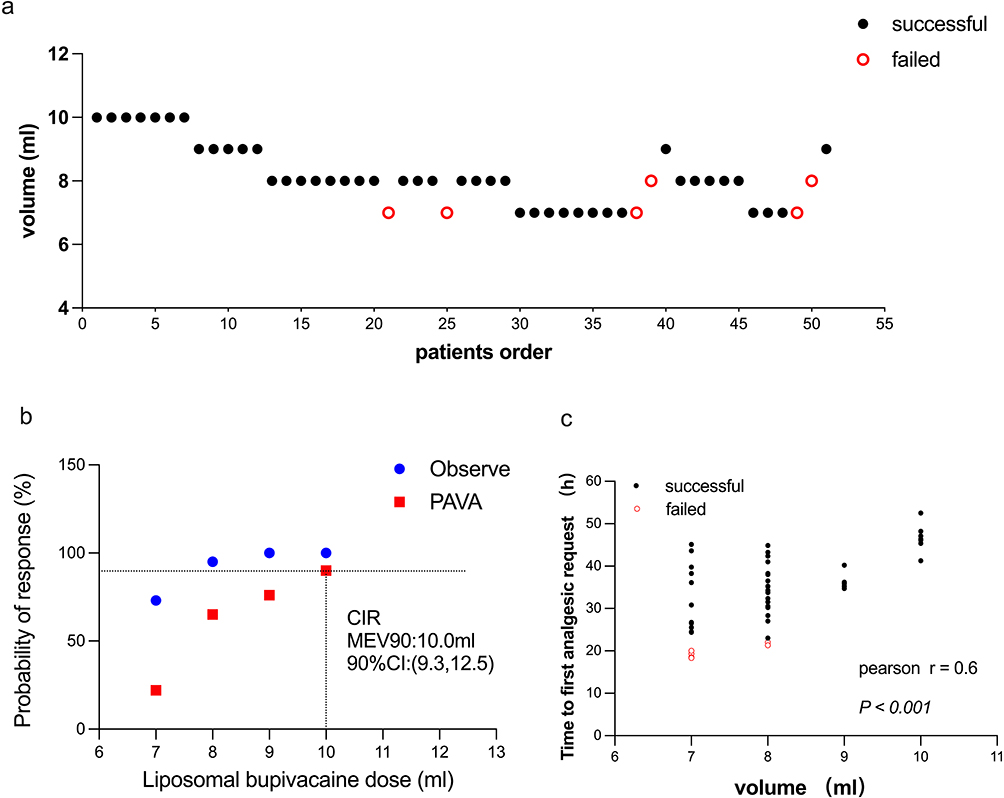 |
Figure 2 Volume-Dependent Efficacy of Liposomal Bupivacaine: Block Success Rates, MEV90 Determination, and Analgesia Duration. Notes: (a) Successful blocks (black solid dots) and failed blocks (red hollow circles) at different volumes of liposomal bupivacaine. (b) The observed response rates and the adjusted response rates calculated using the pooled adjacent violators algorithm at different volumes of liposomal bupivacaine. The vertical line is the calculated minimum effective volume of liposomal bupivacaine providing successful block in 90% of patients (MEV90) as estimated by centered isotonic regression (CIR). (c) Relationship between different doses of liposomal bupivacaine and the time to first rescue analgesia. Successful (black solid dots) and failed blocks (red hollow circles) with different liposomal bupivacaine volumes. |
A moderate positive correlation was identified between the time to first analgesic request and the volume of liposomal bupivacaine administered, with a Pearson correlation coefficient (r) of 0.6 (Figure 2c). This correlation was statistically significant (P < 0.001). In this study, seven patients received a 10 mL dose for brachial plexus blockade, with the time to first rescue analgesia averaging 46.71 ± 3.35 hours.
Within 72 hours following the interscalene brachial plexus blockade, adverse events were recorded, including dizziness in four patients, nausea and vomiting in five patients, and chest discomfort in two patients. No other significant adverse events were identified. Block-related complication data are reported in Table 3.
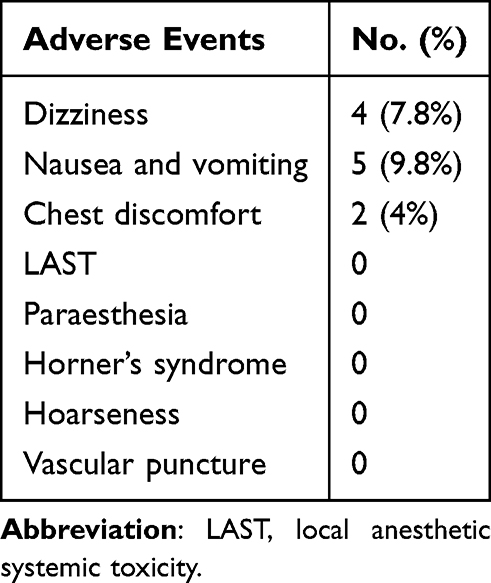 |
Table 3 Summary of Treatment-Emergent Adverse Events (TEAEs) |
Discussion
This study aimed to determine the MEV90 of liposomal bupivacaine for ISB in patients undergoing shoulder arthroscopy. We found the MEV90 for producing an effectives ISB using liposomal bupivacaine to be 10.0 mL (90% CI, 9.3 to 12.5mL). Traditionally, dose-finding studies in regional anesthesia have commonly relied on the Dixon and Massey up-and-down method to determine the 50% effective dose (ED50) or minimum effective volume (MEV50) of local anesthetics.11 Statistical tools, including maximum likelihood estimation and probit regression, were subsequently utilized to estimate higher, clinically relevant doses, such as ED90 or MEV90.14 However, these extrapolation methods have been criticized for their limited precision.10 The BCD method we utilized is relatively new in regional anesthesia, but several recent studies have employed it to determine the minimum effective volume (MEV90) of local anesthetics used in ultrasound-guided brachial plexus block techniques.15–17 In contrast to the Dixon and Massey approach, the BCD method’s simplified statistical framework enhances both transparency and accuracy, offering a more robust alternative for estimating the minimum effective volume (MEV90) in regional anesthesia.13 Furthermore, we adopted the CIR statistical method, a straightforward and theoretically grounded modification of isotonic regression. It offers significant improvements in estimation accuracy, even with small sample sizes, especially in cases of monotonicity violations.18
The minimum effective volume (MEV) for interscalene brachial plexus block varies widely due to differences in local anesthetic pharmacology, concentration, and study endpoints. Reported values range from 0.95 mL for 0.5% bupivacaine with epinephrine to 5 mL for 0.75% ropivacaine and 8.64 mL for 0.5% ropivacaine (MEV90).19–21 These discrepancies reflect enhanced potency at higher concentrations, adjuvant‑induced prolongation of effect, and the higher volumes needed to achieve MEV90 or surgical anesthesia endpoints. Liposomal bupivacaine requires greater initial spread to form a sustained‑release depot,4 which likely accounts for its MEV90 aligning with the upper range of conventional agents. Clinically, a 10 mL dose balances efficacy and safety—offering consistent block success, extended analgesia, and reduced opioid use while minimizing phrenic nerve involvement22 and systemic toxicity risk23—supporting its adoption as a standardized, evidence‑based volume in contemporary ultrasound‑guided regional anesthesia practice.
Our definition of a successful block is defined as a resting NRS score of < 4, 24 hours after the block, with no need for rescue analgesia. The definition of successful blockade is inherently subjective, and the success rate may vary depending on how researchers define success. Therefore, caution is warranted when applying these research findings to clinical practice.
A notable observation was the predominance of female patients, aligning with prior studies,24–26 suggesting that women, particularly those over 50 years old, are more susceptible to rotator cuff tears. This heightened vulnerability may result from hormonal changes, variations in muscle mass, and anatomical factors such as smaller humeral heads and narrower acromial spaces, which collectively contribute to tendon damage, especially in the context of repetitive overhead activities or trauma.27
Our study further demonstrated that patients with rotator cuff injuries exhibited elevated preoperative NRS pain scores during movement (5.73 ± 1.80). Shoulder pain can lead to and exacerbate upper limb dysfunction, a primary indication for rotator cuff surgery. Postoperative pain after rotator cuff repair is marked by its prolonged duration. Effective long-term analgesia is essential for promoting rapid recovery in patients after rotator cuff repair.28 Consequently, we conducted a correlation analysis to explore the relationship between different doses of bupivacaine liposomes and the time to the first analgesia requirement. A positive correlation was identified between the administered doses and the time to the first analgesia requirement (Pearson r = 0.6, p < 0.001). The ability of higher doses of bupivacaine liposomes to extend the time to first rescue analgesia was not the primary objective of this dose-ranging trial. Prospective clinical trials utilizing higher doses are necessary to confirm this.
Our study reported a postoperative incidence of dizziness at 3.9% and nausea and vomiting at 7.8%, consistent with the findings of Manish A. Patel et al,29 who reported a dizziness incidence of 2.9% and nausea and vomiting incidence of 5.8% in the 133 mg liposomal bupivacaine interscalene brachial plexus group. Their study also demonstrated that compared with the placebo group (dizziness 12.7%, nausea and vomiting 9.9%), the incidences of dizziness and nausea and vomiting were significantly lower, suggesting that liposomal bupivacaine is not the primary cause of these side effects. Two patients experienced chest discomfort; however, no respiratory distress or oxygen saturation decline was observed. In patients without underlying pulmonary conditions, this symptom is generally well-tolerated.30 Both patients’ symptoms resolved within 48 hours postoperatively.
Under the conditions of this study, there are several inherent limitations. First, all nerve blocks were performed by a single experienced anesthesiologist, which ensured consistency and effectiveness but may limit generalizability to broader clinical practice. Second, we utilized a fixed concentration of liposomal bupivacaine (133 mg/10 mL), varying only the volume. While this approach is standard in volume‑finding studies, it precludes conclusions regarding potential interactions between volume and concentration. Third, we did not use NRS pain scores during movement as transition criteria because all patients were required to use joint braces postoperatively, which may influence pain assessments in motion. Fourth, published literature indicates that the onset time of liposomal bupivacaine is approximately 30 minutes; in our study, the interscalene brachial plexus block was typically performed one hour prior to surgery, which may limit the applicability of our MEV90 data in clinical scenarios requiring faster operating room turnover. Finally, as a single‑centre study conducted in a relatively homogeneous elective shoulder surgery population using a standardized ultrasound‑guided interscalene technique, the findings may not be directly generalizable to other settings, patient groups, techniques, or endpoint definitions. Future multicentre trials involving multiple operators, varying anaesthetic concentrations, and broader patient inclusion criteria are warranted to enhance external validity and refine MEV estimates for LB.
Conclusion
In our study, the MEV90 of liposomal bupivacaine for ultrasound-guided interscalene brachial plexus blockade in patients undergoing rotator cuff repair surgery was determined to be 10.0mL (90% CI, 9.3 to 12.5mL).
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. Individual de-identified participant data—including baseline characteristics, surgical and anesthetic information, intervention details, postoperative pain scores, opioid consumption, adverse events, and protocol deviations—will be shared. The study protocol, statistical analysis plan, informed consent form, data dictionary, case report forms, and analysis code will also be accessible.
Researchers requesting access to the data are required to submit a methodologically sound proposal and to sign a data use agreement prior to obtaining the materials. Upon approval, the data will be provided through a secure, password-protected link.
Data will be available beginning at the time of publication and will remain accessible for five years thereafter.
Acknowledgments
We thank Dr.Chongyang Duan and Dr. Minggang Yin (Department of Biostatistics, School of Public Health, Southern Medical University) for their generous help with the statistical analysis.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Srikumaran U, Stein BE, Tan EW, Freehill MT, Wilckens JH. Upper-extremity peripheral nerve blocks in the perioperative pain management of orthopaedic patients: AAOS exhibit selection. J Bone Joint Surg Am. 2013;95(24):e197(1–13). doi:10.2106/JBJS.L.01745
2. Toma O, Persoons B, Pogatzki‐Zahn E, Van De Velde M, Joshi GP; the PROSPECT Working Group collaborators. PROSPECT guideline for rotator cuff repair surgery: systematic review and procedure‐specific postoperative pain management recommendations. Anaesthesia. 2019;74(10):1320–1331. doi:10.1111/anae.14796
3. Hussain N, Goldar G, Ragina N, Banfield L, Laffey JG, Abdallah FW. Suprascapular and interscalene nerve block for shoulder surgery: a systematic review and meta-analysis. Anesthesiology. 2017;127(6):998–1013. doi:10.1097/ALN.0000000000001894
4. Chahar P, Cummings KC. Liposomal bupivacaine: a review of a new bupivacaine formulation. J Pain Res. 2012;5:257–264. doi:10.2147/JPR.S27894
5. Ilfeld BM, Malhotra N, Furnish TJ, Donohue MC, Madison SJ. Liposomal bupivacaine as a single-injection peripheral nerve block: a dose-response study. Anesth Analg. 2013;117(5):1248–1256. doi:10.1213/ANE.0b013e31829cc6ae
6. Patel MA, Gadsden JC, Nedeljkovic SS, et al. Brachial plexus block with liposomal bupivacaine for shoulder surgery improves analgesia and reduces opioid consumption: results from a multicenter, randomized, double-blind, controlled trial. Pain Med. 2020;21(2):387–400. doi:10.1093/pm/pnz103
7. Abdallah FW, Halpern SH, Aoyama K, Brull R. Will the real benefits of single-shot interscalene block please stand up? A systematic review and meta-analysis. Anesthesia Analg. 2015;120(5):1114–1129. doi:10.1213/ANE.0000000000000688
8. Aliste J, Bravo D, Fernández D, Layera S, Finlayson RJ, Tran DQ. A randomized comparison between interscalene and small-volume supraclavicular blocks for arthroscopic shoulder surgery. Reg Anesth Pain Med. 2018;43(6):590–595. doi:10.1097/AAP.0000000000000767
9. Weller WJ, Azzam MG, Smith RA, Azar FM, Throckmorton TW. Liposomal bupivacaine mixture has similar pain relief and significantly fewer complications at less cost compared to indwelling interscalene catheter in total shoulder arthroplasty. J Arthroplasty. 2017;32(11):3557–3562. doi:10.1016/j.arth.2017.03.017
10. Saranteas T, Finlayson RJ, Tran DQH. Dose-finding methodology for peripheral nerve blocks. Reg Anesth Pain Med. 2014;39(6):550–555. doi:10.1097/AAP.0000000000000157
11. Vandepitte C, Gautier P, Xu D, Salviz EA, Hadzic A. Effective volume of ropivacaine 0.75% through a catheter required for interscalene brachial plexus blockade. Anesthesiology. 2013;118(4):863–867. doi:10.1097/ALN.0b013e3182850dc7
12. Tran DQH, Dugani S, Correa JA, Dyachenko A, Alsenosy N, Finlayson RJ. Minimum effective volume of lidocaine for ultrasound-guided supraclavicular block. Reg Anesth Pain Med. 2011;36(5):466–469. doi:10.1097/AAP.0b013e3182289f59
13. Oron AP, Souter MJ, Flournoy N. Understanding research methods: up-and-down designs for dose-finding. Anesthesiology. 2022;137(2):137–150. doi:10.1097/ALN.0000000000004282
14. Pace NL, Stylianou MP, Warltier DC. Advances in and limitations of up-and-down methodology: a précis of clinical use, study design, and dose estimation in anesthesia research. Anesthesiology. 2007;107(1):144–152. doi:10.1097/01.anes.0000267514.42592.2a
15. Fang G, Wan L, Mei W, Yu HH, Luo AL. The minimum effective concentration (MEC 90) of ropivacaine for ultrasound-guided supraclavicular brachial plexus block. Anaesthesia. 2016;71(6):700–705. doi:10.1111/anae.13445
16. Panchamia JK, Jagannathan R, Pulos BP, et al. The effects of shoulder arthroscopy on ultrasound image quality of the interscalene brachial plexus: a pre-procedure vs post-procedure comparative study. BMC Anesthesiol. 2021;21:187. doi:10.1186/s12871-021-01409-3
17. Wong MH, Karmakar MK, Mok LYH, Songthamwat B, Samy W. Minimum effective volume of 0.5% ropivacaine for ultrasound-guided costoclavicular brachial plexus block: a dose finding study. Eur J Anaesthesiol. 2020;37(9):780–786. doi:10.1097/EJA.0000000000001287
18. Oron AP, Flournoy N. Centered isotonic regression: point and interval estimation for dose–response studies. Stat Biopharm Res. 2017;9(3):258–267. doi:10.1080/19466315.2017.1286256
19. Falcão LFR, Perez MV, de Castro I, Yamashita AM, Tardelli MA, Amaral JLG. Minimum effective volume of 0.5% bupivacaine with epinephrine in ultrasound-guided interscalene brachial plexus block. Br J Anaesth. 2013;110(3):450–455. doi:10.1093/bja/aes419
20. Gautier P, Vandepitte C, Ramquet C, DeCoopman M, Xu D, Hadzic A. The minimum effective anesthetic volume of 0.75% ropivacaine in ultrasound-guided interscalene brachial plexus block. Anesth Analg. 2011;113(4):951–955. doi:10.1213/ANE.0b013e31822b876f
21. Mittal K, Janweja S, Prateek, Sangwan P, Agarwal D, Tak H. The estimation of minimum effective volume of 0.5% ropivacaine in ultrasound-guided interscalene brachial plexus nerve block: a clinical trial. J Anaesthesiol Clin Pharmacol. 2019;35(1):41–46. doi:10.4103/joacp.JOACP_70_18
22. Renard Y, Grape S, Gonvers E, Rossel JB, Goetti P, Albrecht E. Respiratory impact of local anaesthetic volume after interscalene brachial plexus block with extrafascial injection: a randomised controlled double-blinded trial. Br J Anaesth. 2025;134(4):1153–1160. doi:10.1016/j.bja.2024.12.010
23. Neal JM, Barrington MJ, Fettiplace MR, et al. The third American society of regional anesthesia and pain medicine practice advisory on local anesthetic systemic toxicity: executive summary 2017. Reg Anesth Pain Med. 2018;43(2):113–123. doi:10.1097/AAP.0000000000000720
24. Weber S, Chahal J. Management of rotator cuff injuries. J Am Acad Orthop Surg. 2020;28(5):e193. doi:10.5435/JAAOS-D-19-00463
25. White JJE, Titchener AG, Fakis A, Tambe AA, Hubbard RB, Clark DI. An epidemiological study of rotator cuff pathology using the health improvement network database. Bone Joint J. 2014;96-B(3):350–353. doi:10.1302/0301-620X.96B3.32336
26. Yamamoto A, Takagishi K, Osawa T, et al. Prevalence and risk factors of a rotator cuff tear in the general population. J Shoulder Elbow Surg. 2010;19(1):116–120. doi:10.1016/j.jse.2009.04.006
27. Longo UG, Mazzola A, Carotti S, et al. The role of estrogen and progesterone receptors in the rotator cuff disease: a retrospective cohort stud y. BMC Musculoskelet Disord. 2021;22(1):891. doi:10.1186/s12891-021-04778-5
28. Sgroi TA, Cilenti M. Rotator cuff repair: post-operative rehabilitation concepts. Curr Rev Musculoskelet Med. 2018;11(1):86–91. doi:10.1007/s12178-018-9462-7
29. Patel MA, Gadsden JC, Nedeljkovic SS, et al. Brachial plexus block with liposomal bupivacaine for shoulder surgery improves analgesia and reduces opioid consumption: results from a multicenter, randomized, double-blind, controlled trial. Pain Med. 2019:pnz103. doi:10.1093/pm/pnz103
30. Mak PHK, Irwin MG, Ooi CGC, Chow BFM. Incidence of diaphragmatic paralysis following supraclavicular brachial plexus block and its effect on pulmonary function. Anaesthesia. 2001;56(4):352–356. doi:10.1046/j.1365-2044.2001.01708-2.x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Liposomal Bupivacaine for Serratus Anterior Plane Block in Modified Radical Mastectomy: Protocol for a Randomized, Double-Blind Trial Evaluating Pain-Related and Early Recovery Outcomes
Wei M, Tong J, Pang Y, Zhou X, Qiu Y, Wang Z
Journal of Pain Research 2026, 19:617864
Published Date: 8 July 2026